Effects of Osteopathic Visceral Treatment in Patients with Gastroesophageal Reflux: A Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Participants
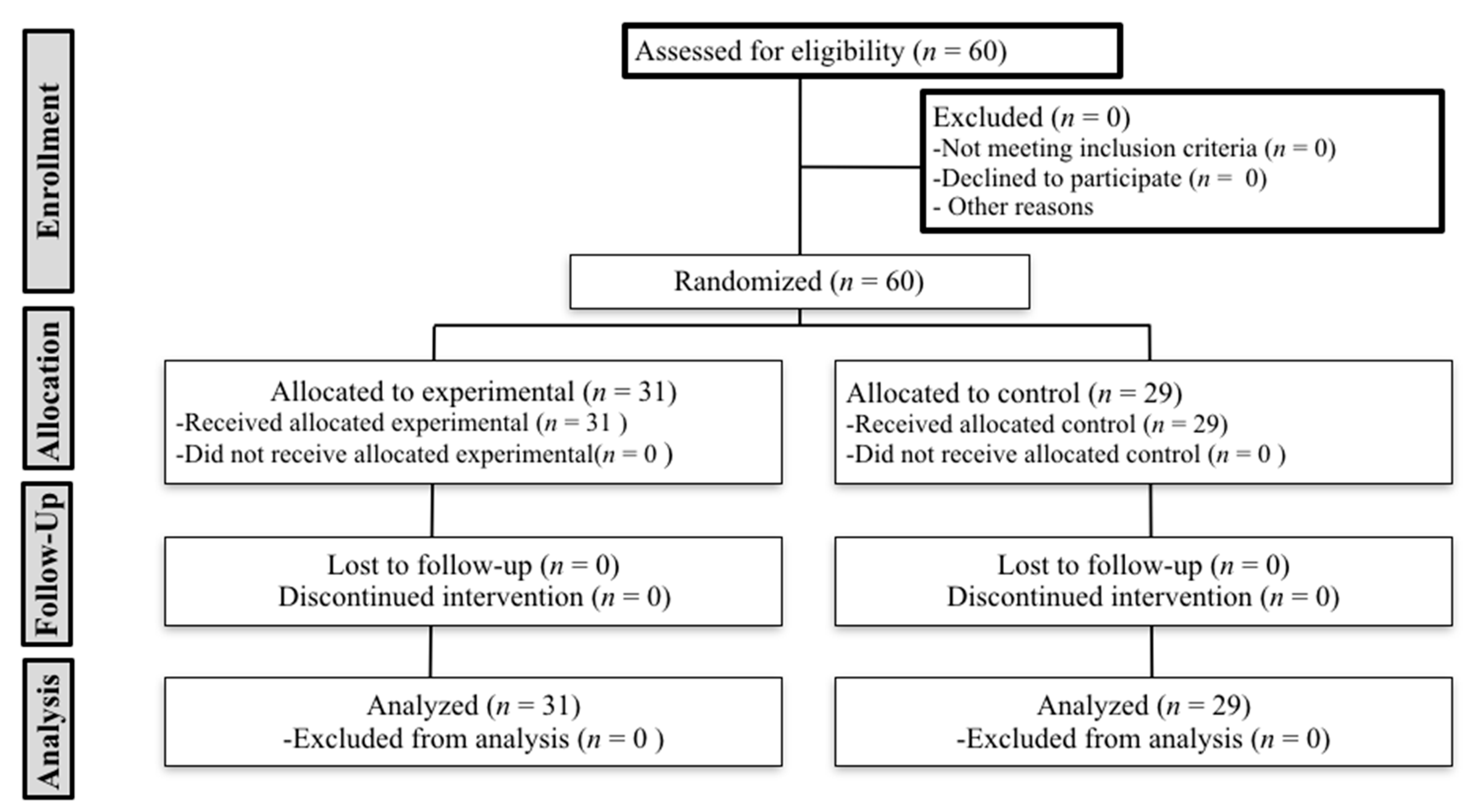
2.3. Randomization, Blinding and Allocation
2.4. Study Protocol
2.5. Primary Outcome: GERDQ Test
2.6. Secondary Outcome: PPT and Cervical Mobility
2.7. Statistical Analysis
2.8. Ethical Considerations and Data Protection
3. Results
3.1. Sample
3.2. Outcome Variables
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- El-Serag, H.B.; Sweet, S.; Winchester, C.C.; Dent, J. Update on the epidemiology of gastro-oesophageal reflux disease: A systematic review. Gut 2014, 63, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Eusebi, L.H.; Ratnakumaran, R.; Yuan, Y.; Solaymani-Dodaran, M.; Bazzoli, F.; Ford, A.C. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: A meta-analysis. Gut 2018, 67, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.E.; Rubenstein, J.H. Presentation and Epidemiology of Gastroesophageal Reflux Disease. Gastroenterology 2018, 154, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, N.J.; Hansen, R.A.; Morgan, D.R.; Gangarosa, L.M.; Ringel, Y.; Thiny, M.T.; Russo, M.W.; Sandler, R.S. The burden of gastrointestinal and liver diseases, 2006. Am. J. Gastroenterol. 2006, 101, 2128–2138. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.P. Barrett’s Esophagus and Esophageal Adenocarcinoma: How Common Are They Really? Dig. Dis. Sci. 2018, 63, 1988–1996. [Google Scholar] [CrossRef]
- Pandolfino, J.E.; Zhang, Q.G.; Ghosh, S.K.; Han, A.; Boniquit, C.; Kahrilas, P.J. Transient lower esophageal sphincter relaxations and reflux: Mechanistic analysis using concurrent fluoroscopy and high-resolution manometry. Gastroenterology 2006, 131, 1725–1733. [Google Scholar] [CrossRef]
- de Mezerville Cantillo, L.; Cabas Sánchez, J.; Contreras, F.; Castellanos García, L.; Dondis, J.C.; Galdámez, J.; García-Maradiaga, R.; Grullón Dickson, F.; Jerez González, L.E.; Mayo DiBello, M. Guía Práctica de la Asociación Centroamericana y del Caribe de Gastroenterología y Endoscopía Digestiva (ACCGED) para el manejo de la Enfermedad por Reflujo Gastroesofágico (ERGE). Acta Gastroenterol. Latinoam. 2014, 44, 138–153. [Google Scholar]
- Gyawali, C.P.; Fass, R. Management of Gastroesophageal Reflux Disease. Gastroenterology 2018, 154, 302–318. [Google Scholar] [CrossRef]
- Chen, C.H.; Lin, C.L.; Kao, C.H. Gastroesophageal reflux disease with proton pump inhibitor use is associated with an increased risk of osteoporosis: A nationwide population-based analysis. Osteoporos Int. 2016, 27, 2117–2126. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Kandulski, A.; Venerito, M. Proton-pump inhibitors: Understanding the complications and risks. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 697–710. [Google Scholar] [CrossRef]
- Vaucher, P.; Macdonald, R.J.D.; Carnes, D. The role of osteopathy in the Swiss primary health care system: A practice review. BMJ Open. 2018, 8, e023770. [Google Scholar] [CrossRef] [PubMed]
- Organization WHOBfTiOWH. 2010. Available online: http://wwwwhoint/medicines/areas/traditional/BenchmarksforTraininginOsteopathypdf (accessed on 25 May 2019).
- Van Dun, P.L.; Nicolaie, M.A.; Van Messem, A. State of affairs of osteopathy in the Benelux: Benelux Osteosurvey 2013. Int. J. Osteopath. Med. 2016, 20, 3–17. [Google Scholar] [CrossRef]
- Attali, T.V.; Bouchoucha, M.; Benamouzig, R. Treatment of refractory irritable bowel syndrome with visceral osteopathy: Short-term and long-term results of a randomized trial. J. Dig. Dis. 2013, 14, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Molins-Cubero, S.; Rodriguez-Blanco, C.; Oliva-Pascual-Vaca, A.; Heredia-Rizo, A.M.; Bosca-Gandia, J.J.; Ricard, F. Changes in pain perception after pelvis manipulation in women with primary dysmenorrhea: A randomized controlled trial. Pain Med. 2014, 15, 1455–1463. [Google Scholar] [CrossRef] [PubMed]
- Pang, R.; Wang, S.; Tian, L.; Lee, M.C.; Do, A.; Cutshall, S.M.; Li, G.; Bauer, B.A.; Thomley, B.S.; Chon, T.Y. Complementary and Integrative Medicine at Mayo Clinic. Am. J. Chin. Med. 2015, 43, 1503–1513. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Vaca, A.O.; Punzano-Rodriguez, R.; Escriba-Astaburuaga, P.; Fernandez-Dominguez, J.C.; Ricard, F.; Franco-Sierra, M.A.; Rodríguez-Blanco, C. Short-Term Changes in Algometry, Inclinometry, Stabilometry, and Urinary pH Analysis After a Thoracolumbar Junction Manipulation in Patients with Kidney Stones. J. Altern. Complement. Med. 2017, 23, 639–647. [Google Scholar] [CrossRef]
- Xing, L.; Qu, L.; Chen, H.; Gao, S. Clinical effect of traditional Chinese spinal orthopedic manipulation in treatment of Functional Abdominal Pain Syndrome. Complement. Ther. Med. 2017, 32, 19–24. [Google Scholar] [CrossRef]
- Zhu, J.; Guo, Y.; Liu, S.; Su, X.; Li, Y.; Yang, Y.; Hou, L.; Wang, G.; Zhang, J.; Chen, J.; et al. Acupuncture for the treatment of gastro-oesophageal reflux disease: A systematic review and meta-analysis. Acupunct. Med. 2017, 35, 316–323. [Google Scholar] [CrossRef]
- Martinez-Ochoa, M.J.; Fernandez-Dominguez, J.C.; Morales-Asencio, J.M.; Gonzalez-Iglesias, J.; Ricard, F.; Oliva-Pascual-Vaca, A. Effectiveness of an Osteopathic Abdominal Manual Intervention in Pain Thresholds, Lumbopelvic Mobility, and Posture in Women with Chronic Functional Constipation. J. Altern. Complement. Med. 2018, 24, 816–824. [Google Scholar] [CrossRef]
- Martinez-Hurtado, I.; Arguisuelas, M.D.; Almela-Notari, P.; Cortes, X.; Barrasa-Shaw, A.; Campos-Gonzalez, J.C.; Lisón, J.F. Effects of diaphragmatic myofascial release on gastroesophageal reflux disease: A preliminary randomized controlled trial. Sci. Rep. 2019, 9, 7273. [Google Scholar] [CrossRef]
- Da Silva, R.C.; de Sa, C.C.; Pascual-Vaca, A.O.; de Souza Fontes, L.H.; Herbella Fernandes, F.A.; Dib, R.A.; Blanco, C.R.; Queiroz, R.A.; Navarro-Rodriguez, T. Increase of lower esophageal sphincter pressure after osteopathic intervention on the diaphragm in patients with gastroesophageal reflux. Dis. Esophagus 2013, 26, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Diniz, L.R.; Nesi, J.; Curi, A.C.; Martins, W. Qualitative evaluation of osteopathic manipulative therapy in a patient with gastroesophageal reflux disease: A brief report. J. Am. Osteopath. Assoc. 2014, 114, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Rotter, G.; Brinkhaus, B. Osteopathie bei gastroosophagealem Reflux mit Hiatushernie: Ein Fallbericht gemass der CARE-Leitlinie. Complement. Med. Res. 2017, 24, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Yang, G.; Wang, S.; Zheng, X.; Zhang, W.; Li, Y. The Most Commonly Treated Acupuncture Indications in the United States: A Cross-Sectional Study. Am. J. Chin. Med. 2018, 103, 212–215. [Google Scholar] [CrossRef]
- Shahnawaz, M.; van der Westhuizen, L.R.; Gledhill, R.F. Episodic cervical dystonia associated with gastro-oesophageal reflux. A case of adult-onset Sandifer syndrome. Clin. Neurol. Neurosurg. 2001, 103, 212–215. [Google Scholar] [CrossRef]
- Kabakus, N.; Kurt, A. Sandifer Syndrome: A continuing problem of misdiagnosis. Pediatr. Int. 2006, 48, 622–625. [Google Scholar] [CrossRef]
- Kostakis, A.; Manjunatha, N.P.; Kumar, A.; Moreland, E.S. Abnormal head posture in a patient with normal ocular motility: Sandifer syndrome. J. Pediatr. Ophthalmol. Strabismus 2008, 45, 57–58. [Google Scholar] [CrossRef]
- Flanagin, B.A.; Mitchell, M.T.; Thistlethwaite, W.A.; Alverdy, J.C. Diagnosis and treatment of atypical presentations of hiatal hernia following bariatric surgery. Obes. Surg. 2010, 20, 386–392. [Google Scholar] [CrossRef]
- Rana, A.Q.; Yousuf, M.S.; Joian, S. A chronic case of adult-onset Sandifer syndrome. Neurol. Sci. 2013, 34, 405–406. [Google Scholar] [CrossRef]
- Rouzade, M.L.; Fioramonti, J.; Bueno, L. A model for evaluation of gastric sensitivity in awake rats. Neurogastroenterol. Motil. 1998, 10, 157–163. [Google Scholar] [CrossRef]
- Ozaki, N.; Bielefeldt, K.; Sengupta, J.N.; Gebhart, G.F. Models of gastric hyperalgesia in the rat. Am. J. Physiol Gastrointest. Liver Physiol. 2002, 283, G666–G676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loukas, M.; Du Plessis, M.; Louis, R.G.; Tubbs, R.S., Jr.; Wartmann, C.T.; Apaydin, N. The subdiaphragmatic part of the phrenic nerve - morphometry and connections to autonomic ganglia. Clin. Anat. 2016, 29, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.C.O.; Biasotto-Gonzalez, D.A.; Oliveira, F.H.M.; Andrade, A.O.; Gomes, C.; Lanza, F.C.; Amorim, C.F.; Politti, F. Effect of Osteopathic Visceral Manipulation on Pain, Cervical Range of Motion, and Upper Trapezius Muscle Activity in Patients with Chronic Nonspecific Neck Pain and Functional Dyspepsia: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. Evid. Based Complement. Alternat. Med. 2018, 2018, 4929271. [Google Scholar] [CrossRef] [PubMed]
- Fraser, A.; Delaney, B.; Moayyedi, P. Symptom-based outcome measures for dyspepsia and GERD trials: A systematic review. Am. J. Gastroenterol. 2005, 100, 442–452. [Google Scholar] [CrossRef]
- Chess, L.E.; Gagnier, J. Risk of bias of randomized controlled trials published in orthopaedic journals. BMC Med. Res. Methodol. 2013, 13, 76. [Google Scholar] [CrossRef]
- De Coster, M.; Pollaris, A. Osteopatía Visceral; Paidotribo: Barcelona, Spain, 2001. [Google Scholar]
- Jones, R.; Junghard, O.; Dent, J.; Vakil, N.; Halling, K.; Wernersson, B.; Lind, T. Development of the GerdQ, a tool for the diagnosis and management of gastro-oesophageal reflux disease in primary care. Aliment. Pharmacol. Ther. 2009, 30, 1030–1038. [Google Scholar] [CrossRef]
- Dent, J.; Vakil, N.; Jones, R.; Bytzer, P.; Schoning, U.; Halling, K.; Junghard, O.; Lind, T. Accuracy of the diagnosis of GORD by questionnaire, physicians and a trial of proton pump inhibitor treatment: The Diamond Study. Gut 2010, 59, 714–721. [Google Scholar] [CrossRef]
- Jonasson, C.; Moum, B.; Bang, C.; Andersen, K.R.; Hatlebakk, J.G. Randomised clinical trial: A comparison between a GerdQ-based algorithm and an endoscopy-based approach for the diagnosis and initial treatment of GERD. Aliment. Pharmacol. Ther. 2012, 35, 1290–1300. [Google Scholar] [CrossRef]
- Jordan, K. Assessment of published reliability studies for cervical spine range-of-motion measurement tools. J. Manip. Physiol. Ther. 2000, 23, 180–195. [Google Scholar] [CrossRef]
- Zavala-Gonzales, M.A.; Azamar-Jacome, A.A.; Meixueiro-Daza, A.; De La Medina, A.R. Validation and diagnostic usefulness of gastroesophageal reflux disease questionnaire in a primary care level in Mexico. J. Neurogastroenterol. Motil. 2014, 20, 475–482. [Google Scholar] [CrossRef]
- Ferragut-Garcias, A.; Plaza-Manzano, G.; Rodriguez-Blanco, C.; Velasco-Roldan, O.; Pecos-Martin, D.; Oliva-Pascual-Vaca, J.; Llabrés-Bennasar, B.; Oliva-Pascual-Vaca, Á. Effectiveness of a Treatment Involving Soft Tissue Techniques and/or Neural Mobilization Techniques in the Management of Tension-Type Headache: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2017, 98, 211–219.e2. [Google Scholar] [CrossRef] [PubMed]
- Walton, D.M.; Macdermid, J.C.; Nielson, W.; Teasell, R.W.; Chiasson, M.; Brown, L. Reliability, standard error, and minimum detectable change of clinical pressure pain threshold testing in people with and without acute neck pain. J. Orthop. Sports Phys. Ther. 2011, 41, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Heredia-Rizo, A.M.; Oliva-Pascual-Vaca, A.; Rodriguez-Blanco, C.; Torres-Lagares, D.; Albornoz-Cabello, M.; Pina-Pozo, F.; Luque-Carrasco, A. Craniocervical posture and trigeminal nerve mechanosensitivity in subjects with a history of orthodontic use: A cross-sectional study. Cranio 2013, 31, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Heredia Rizo, A.M.; Pascual-Vaca, A.O.; Cabello, M.A.; Blanco, C.R.; Pozo, F.P.; Carrasco, A.L. Immediate effects of the suboccipital muscle inhibition technique in craniocervical posture and greater occipital nerve mechanosensitivity in subjects with a history of orthodontia use: A randomized trial. J. Manip. Physiol. Ther. 2012, 35, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.P.; Bandy, W.D. Intrarater reliability of CROM measurement of cervical spine active range of motion in persons with and without neck pain. J. Orthop. Sports Phys. Ther. 2008, 38, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Audette, I.; Dumas, J.P.; Cote, J.N.; De Serres, S.J. Validity and between-day reliability of the cervical range of motion (CROM) device. J. Orthop. Sports Phys. Ther. 2010, 40, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Allison, G.T.; Singer, K.P. Reliability of the spin-T cervical goniometer in measuring cervical range of motion in an asymptomatic Indian population. J. Manip. Physiol. Ther. 2005, 28, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Hall, T.M.; Robinson, K.W.; Fujinawa, O.; Akasaka, K.; Pyne, E.A. Intertester reliability and diagnostic validity of the cervical flexion-rotation test. J. Manip. Physiol Ther. 2008, 31, 293–300. [Google Scholar] [CrossRef]
- Casanova-Mendez, A.; Oliva-Pascual-Vaca, A.; Rodriguez-Blanco, C.; Heredia-Rizo, A.M.; Gogorza-Arroitaonandia, K.; Almazan-Campos, G. Comparative short-term effects of two thoracic spinal manipulation techniques in subjects with chronic mechanical neck pain: A randomized controlled trial. Man. Ther. 2014, 19, 331–337. [Google Scholar] [CrossRef]
- Krleza-Jeric, K.; Lemmens, T. 7th revision of the Declaration of Helsinki: Good news for the transparency of clinical trials. Croat. Med. J. 2009, 50, 105–110. [Google Scholar] [CrossRef]
- 15/1999 OL. December 13, Personal Data Protection: B.O.E. number 298;1999. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-1999-23750 (accessed on 18 February 2019).
- Shih, Y.S.; Tsai, C.H.; Li, T.C.; Yu, C.J.; Chou, J.W.; Feng, C.L.; Wang, K.-T.; Lai, H.-C.; Hsieh, C.-L. Effect of wu chu yu tang on gastroesophageal reflux disease: Randomized, double-blind, placebo-controlled trial. Phytomedicine 2019, 56, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Rimmani, H.H.; Rustom, L.B.O.; Rahal, M.A.; Shayto, R.H.; Chaar, H.; Sharara, A.I. Dexlansoprazole is Effective in Relieving Heartburn during the Fasting Month of Ramadan. Dig. Dis. 2019, 37, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.Y.; Fang, D.C.; Fan, L.L.; Chang, H.; Wu, Z.L.; Cao, Y.; Lan, C.H. Efficacy and safety of esomeprazole with flupentixol/melitracen in treating gastroesophageal reflux disease patients with emotional disorders. J. Gastroenterol. Hepatol. 2014, 29, 1200–1206. [Google Scholar] [CrossRef] [PubMed]
- Reimer, C.; Lodrup, A.B.; Smith, G.; Wilkinson, J.; Bytzer, P. Randomised clinical trial: Alginate (Gaviscon Advance) vs. placebo as add-on therapy in reflux patients with inadequate response to a once daily proton pump inhibitor. Aliment. Pharmacol. Ther. 2016, 43, 899–909. [Google Scholar] [CrossRef]
- Cossentino, M.J.; Mann, K.; Armbruster, S.P.; Lake, J.M.; Maydonovitch, C.; Wong, R.K. Randomised clinical trial: The effect of baclofen in patients with gastro-oesophageal reflux—A randomised prospective study. Aliment. Pharmacol. Ther. 2012, 35, 1036–1044. [Google Scholar] [CrossRef]
- Pandolfino, J.E.; Kwiatek, M.A.; Kahrilas, P.J. The pathophysiologic basis for epidemiologic trends in gastroesophageal reflux disease. Gastroenterol. Clin. N. Am. 2008, 37, 827–843. [Google Scholar] [CrossRef]
- Polomsky, M.; Siddall, K.A.; Salvador, R.; Dubecz, A.; Donahue, L.A.; Raymond, D.; Jones, C.; Watson, T.J.; Peters, J.H. Association of kyphosis and spinal skeletal abnormalities with intrathoracic stomach: A link toward understanding its pathogenesis. J. Am. Coll Surg. 2009, 208, 562–569. [Google Scholar] [CrossRef]
- Imagama, S.; Hasegawa, Y.; Wakao, N.; Hirano, K.; Hamajima, N.; Ishiguro, N. Influence of lumbar kyphosis and back muscle strength on the symptoms of gastroesophageal reflux disease in middle-aged and elderly people. Eur. Spine J. 2012, 21, 2149–2157. [Google Scholar] [CrossRef] [Green Version]
- Welch, R.W.; Gray, J.E. Influence of respiration on recordings of lower esophageal sphincter pressure in humans. Gastroenterology 1982, 83, 590–594. [Google Scholar]
- Dieleman, E.M.; Senan, S.; Vincent, A.; Lagerwaard, F.J.; Slotman, B.J.; van Sornsen de Koste, J.R. Four-dimensional computed tomographic analysis of esophageal mobility during normal respiration. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 775–780. [Google Scholar] [CrossRef]
- Schulze, K.S. The imaging and modelling of the physical processes involved in digestion and absorption. Acta Physiol. 2015, 213, 394–405. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, G.; Cerritelli, F.; Cortelli, P. Sensitization and Interoception as Key Neurological Concepts in Osteopathy and Other Manual Medicines. Front. Neurosci. 2016, 10, 100. [Google Scholar] [CrossRef] [PubMed]
- McGlone, F.; Cerritelli, F.; Walker, S.; Esteves, J. The role of gentle touch in perinatal osteopathic manual therapy. Neurosci. Biobehav. Rev. 2017, 72, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banneheka, S. Morphological study of the ansa cervicalis and the phrenic nerve. Anat. Sci. Int. 2008, 83, 31–44. [Google Scholar] [CrossRef] [PubMed]
- McCoss, C.A.; Johnston, R.; Edwards, D.J.; Millward, C. Preliminary evidence of Regional Interdependent Inhibition, using a ‘Diaphragm Release’ to specifically induce an immediate hypoalgesic effect in the cervical spine. J. Bodyw. Mov. Ther. 2017, 21, 362–374. [Google Scholar] [CrossRef]
- McSweeney, T.P.; Thomson, O.P.; Johnston, R. The immediate effects of sigmoid colon manipulation on pressure pain thresholds in the lumbar spine. J. Bodyw. Mov. Ther. 2012, 16, 416–423. [Google Scholar] [CrossRef]
- Herregods, T.V.; Bredenoord, A.J.; Smout, A.J. Pathophysiology of gastroesophageal reflux disease: New understanding in a new era. Neurogastroenterol. Motil. 2015, 27, 1202–1213. [Google Scholar] [CrossRef]
- Farmer, A.D.; Ruffle, J.K.; Aziz, Q. The Role of Esophageal Hypersensitivity in Functional Esophageal Disorders. J. Clin. Gastroenterol. 2017, 51, 91–99. [Google Scholar] [CrossRef]
- Scott, D.; Jull, G.; Sterling, M. Widespread sensory hypersensitivity is a feature of chronic whiplash-associated disorder but not chronic idiopathic neck pain. Clin. J. Pain. 2005, 21, 175–181. [Google Scholar] [CrossRef]
- Coppieters, I.; De Pauw, R.; Kregel, J.; Malfliet, A.; Goubert, D.; Lenoir, D.; Cagnie, B.; Meeus, M. Differences Between Women With Traumatic and Idiopathic Chronic Neck Pain and Women Without Neck Pain: Interrelationships Among Disability, Cognitive Deficits, and Central Sensitization. Phys. Ther. 2017, 97, 338–353. [Google Scholar]
- Sa, S.; Silva, A.G. Repositioning error, pressure pain threshold, catastrophizing and anxiety in adolescents with chronic idiopathic neck pain. Musculoskelet. Sci. Pract. 2017, 30, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Cote, P.; Cassidy, J.D.; Carroll, L. The factors associated with neck pain and its related disability in the Saskatchewan population. Spine 2000, 25, 1109–1117. [Google Scholar] [PubMed]
- Moore, K.L.; Daley, A.F., II; Agur, A.M.R. Clinically Oriented Anatomy; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Control Group (n = 29) | Osteopathic Manual Group (n = 31) | p Value | ||
|---|---|---|---|---|---|
| Mean | SD (95%CI) | Mean | SD (95%CI) | ||
| Age | 49.45 | 13.77 (44.21–54.69) | 48.19 | 14.03 (43.05–53.34) | 0.728 |
| Sex | |||||
| Male | 14 | 48.3% | 15 | 48.4% | 0.599 |
| Female | 15 | 51.7% | 16 | 51.6% | |
| PPIs | |||||
| Yes | 8 | 27.6% | 14 | 45.2% | 0.188 |
| No | 21 | 72.4% | 17 | 54.8% | |
| Smoker | |||||
| Yes | 7 | 24.1% | 12 | 38.7% | 0.175 |
| No | 22 | 75.9% | 19 | 61.3% | |
| BMI | 24.81 | 3.84 (23.35–26.27) | 24.70 | 3.84 (23.30–26.11) | 0.706 |
| PPT C4 | 30.49 | 8.44 (27.28–33.70) | 29.93 | 12.63 (25.30–34.56) | 0.304 |
| Cervical mobility | 328.65 | 62.22 (306.34–350.97) | 326.16 | 57.91 (304.57–347.74) | 0.873 |
| GerdQ test | 3.79 | 2.81 (2.73–4.86) | 5.13 | 3.91 (3.69–6.56) | 0.248 |
| Outcome | Time | Control Group (n = 29) | Osteopathic Manual Group (n = 31) | p Value | ||
|---|---|---|---|---|---|---|
| Mean | SD (95%CI) | Mean | SD (95%CI) | |||
| PPT C4 | Baseline | 30.49 | 8.44 (26.47–34.51) | 29.92 | 12.63 (26.04–33.81) | 0.034 a |
| Post-1st Treatment | 29.25 | 9.48 (25.09–33.41) | 29.36 | 12.57 (25.34–33.39) | ||
| Follow-up | 29.31 | 11.25 (23.15–35.46) | 34.06 | 20.28 (28.05–39.95) | ||
| Post-2nd Treatment | 29.61 | 11.14 (22.83–36.4) | 37.84 | 22.97 (31.28–44.40) | ||
| Cervical mobility | Baseline | 328.65 | 62.22 (306.34–350.97) | 326.16 | 57.91 (304.57–347.74) | <0.001 a |
| Post-1st Treatment | 319.55 | 60.56 (299.20–339.90) | 339.51 | 48.69 (319.83–359.19) | ||
| Follow-up | 309.20 | 59.96 (288.46–329.94) | 336.96 | 51.58 (316.91–357.02) | ||
| Post-2nd Treatment | 312.86 | 64.72 (291.56–3334.15) | 344.25 | 49.33 (323.66–364.85) | ||
| GerdQ test | Baseline | 3.79 | 2.81 (2.73 to 4.86) | 5.13 | 3.91 (3.69–6.56) | 0.005 b |
| Post 1 Week | 3.34 | 2.81 (2.27–4.42) | 3.19 | 3.37 (1.96–4.43) | ||
| Outcome | Time | Mean | 95% CI |
|---|---|---|---|
| GerdQ test | Baseline | 1.34 | −0.42–3.09 |
| Post 1 Week | 0.15 | −1.46–1.763 | |
| Difference Post 1 Week - Baseline | 1.49 | 0.47–2.49 | |
| PPT | Baseline | 0.56 | −5.03–6.15 |
| Post-1st Treatment | 0.11 | −5.67–5.90 | |
| Follow-up | 4.69 | −3.75–13.14 | |
| Post-2nd Treatment | 8.22 | −1.08–17.53 | |
| Difference Post 2nd Treatment - Baseline | 8.78 | 0.48–17.09 | |
| Cervical mobility | Baseline | 2.49 | −28.55–33.54 |
| Post-1st Treatment | 19.96 | −8.34–48.27 | |
| Follow-up | 27.76 | −1.09–56.61 | |
| Post-2nd Treatment | 31.39 | 1.77–61.02 | |
| Difference Post 2nd Treatment - Baseline | 33.89 | 15.17–52.61 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eguaras, N.; Rodríguez-López, E.S.; Lopez-Dicastillo, O.; Franco-Sierra, M.Á.; Ricard, F.; Oliva-Pascual-Vaca, Á. Effects of Osteopathic Visceral Treatment in Patients with Gastroesophageal Reflux: A Randomized Controlled Trial. J. Clin. Med. 2019, 8, 1738. https://doi.org/10.3390/jcm8101738
Eguaras N, Rodríguez-López ES, Lopez-Dicastillo O, Franco-Sierra MÁ, Ricard F, Oliva-Pascual-Vaca Á. Effects of Osteopathic Visceral Treatment in Patients with Gastroesophageal Reflux: A Randomized Controlled Trial. Journal of Clinical Medicine. 2019; 8(10):1738. https://doi.org/10.3390/jcm8101738
Chicago/Turabian StyleEguaras, Nuria, Elena Sonsoles Rodríguez-López, Olga Lopez-Dicastillo, M. Ángeles Franco-Sierra, François Ricard, and Ángel Oliva-Pascual-Vaca. 2019. "Effects of Osteopathic Visceral Treatment in Patients with Gastroesophageal Reflux: A Randomized Controlled Trial" Journal of Clinical Medicine 8, no. 10: 1738. https://doi.org/10.3390/jcm8101738