Revealing Associations between Diagnosis Patterns and Acupoint Prescriptions Using Medical Data Extracted from Case Reports

Abstract
:1. Introduction
2. Methods
2.1. Experimental Design
2.2. Data Collection and Pre-Processing
2.3. Network Analysis of Diagnosis Patterns and Prescribed Acupoints
2.4. Associations Between Diagnosis Patterns Acupoint Prescriptions
3. Results
3.1. Characteristics of Diagnosis Patterns and Acupoints Based on Virtual Diagnoses
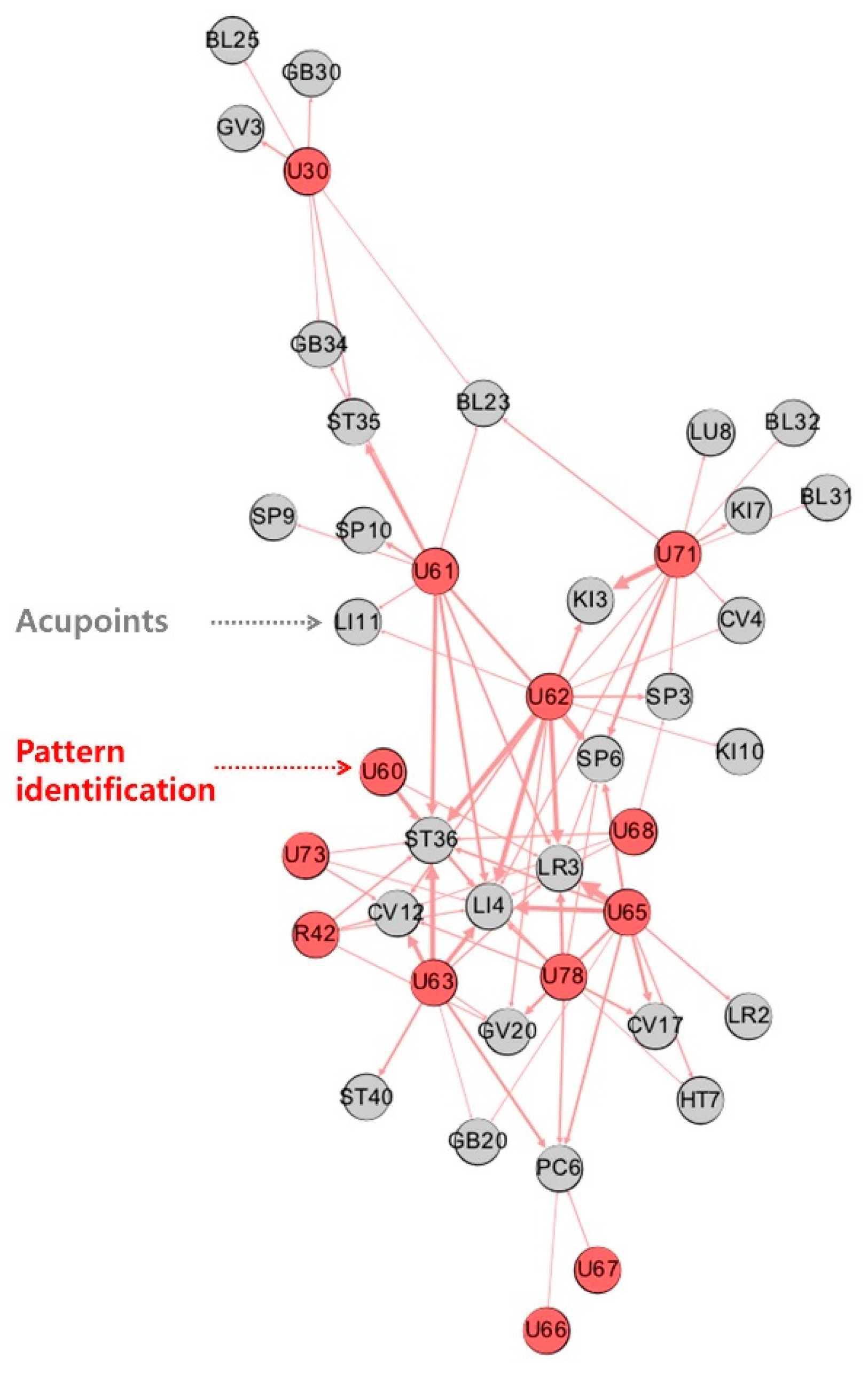
3.2. Network Analysis of Diagnosis Pattern Prescribed Acupoint Pairs
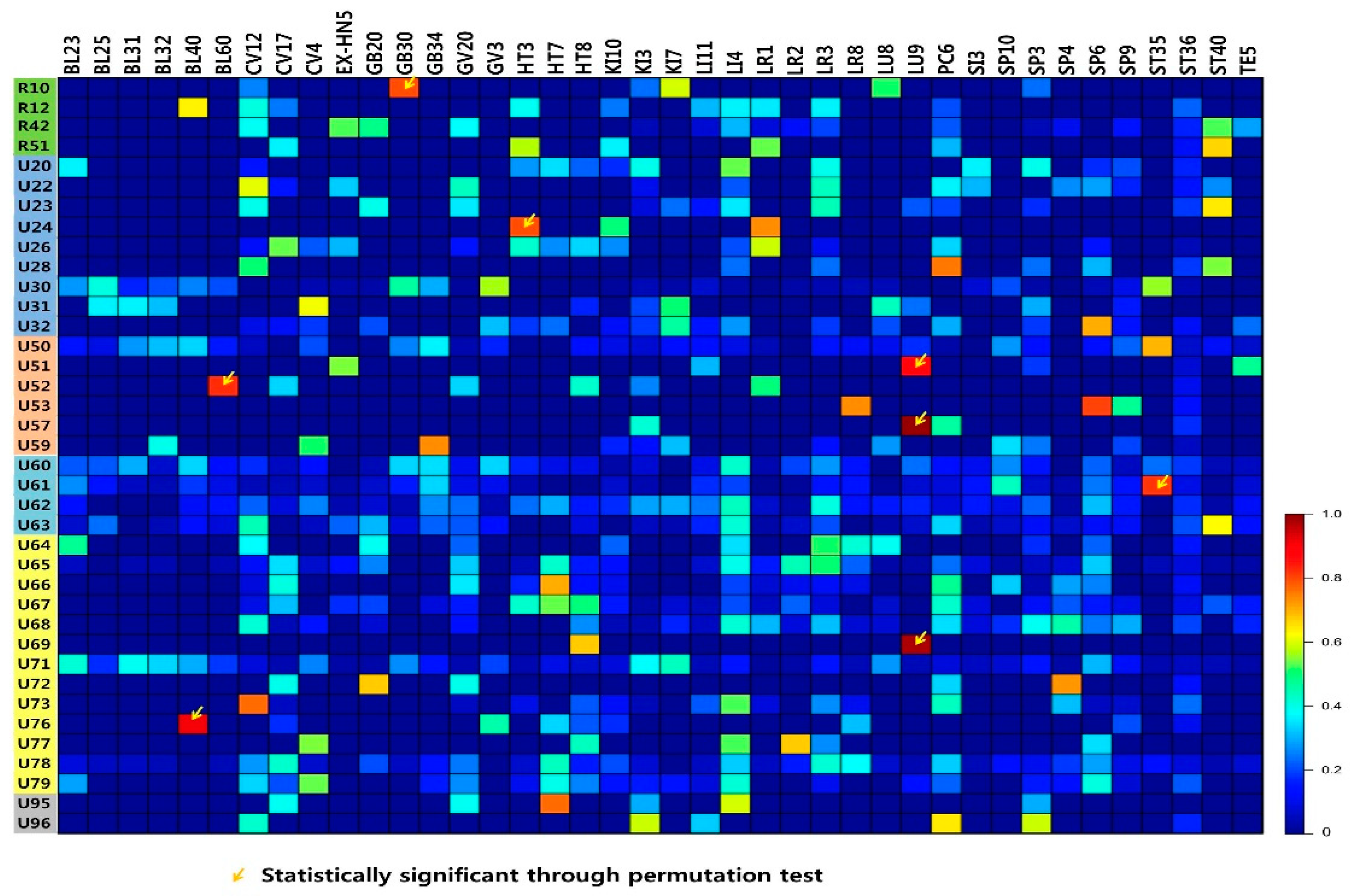
3.3. Associations Between Diagnosis Patterns and Prescribed Acupoints
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Sherman, K.J.; Cherkin, D.C.; Hogeboom, C.J. The Diagnosis and Treatment of Patients with Chronic Low-Back Pain by Traditional Chinese Medical Acupuncturists. J. Altern. Complement. Med. 2001, 7, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Alraek, T. Designing clinical studies that take into account traditional East Asian medicine’s systems and methods—with focus on pattern identification. Chin. J. Integr. Med. 2014, 20, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Napadow, V.; Liu, J.; Kaptchuk, T.J. A systematic study of acupuncture practice: Acupoint usage in an outpatient setting in Beijing, China. Complement. Ther. Med. 2004, 12, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.-M.; Lee, I.-S.; Wallraven, C.; Ryu, Y.-H.; Park, H.-J.; Chae, Y. Cortical Activation Patterns of Bodily Attention triggered by Acupuncture Stimulation. Sci. Rep. 2015, 5, 12455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.-Y.; Lin, F.; Jiang, Z.-L. Pattern of acupoint selection based on complex network analysis technique. Zhongguo Zhen Jiu Chin. Acupunct. Moxibustion 2011, 31, 85–88. [Google Scholar]
- Liu, M.; Hu, W.; Xie, S.; Zhang, J.; Zhao, Z.; Liu, M.; Chang, X. Characteristics and laws of acupoint selection in treatment of hyperlipidemia with acupuncture and moxibustion. Zhongguo Zhen Jiu Chin. Acupunct. Moxibustion 2015, 35, 512–516. [Google Scholar]
- Kang, H.; Zhao, Y.; Li, C.; Chen, Y.; Tang, K.; Yang, L.; Ma, C.; Peng, J.; Zhu, R.; Liu, Q.; et al. Integrating Clinical Indexes into Four-Diagnostic Information Contributes to the Traditional Chinese Medicine (TCM) Syndrome Diagnosis of Chronic Hepatitis B. Sci. Rep. 2015, 5, 9395. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, K.A.; Abbas, E.; Zhang, J.; Guo, Z.-X.; Luo, R.; Bensoussan, A.; Komesaroff, P.A. An Investigation into the Reliability of Chinese Medicine Diagnosis According to Eight Guiding Principles and Zang-Fu Theory in Australians with Hypercholesterolemia. J. Altern. Complement. Med. 2009, 15, 259–266. [Google Scholar] [CrossRef]
- Kleinert, R.; Heiermann, N.; Plum, P.S.; Wahba, R.; Chang, D.-H.; Maus, M.; Chon, S.-H.; Hoelscher, A.H.; Stippel, D.L.; Zhu, E.; et al. Web-Based Immersive Virtual Patient Simulators: Positive Effect on Clinical Reasoning in Medical Education. J. Med. Internet Res. 2015, 17, e263. [Google Scholar] [CrossRef]
- Lee, T.; Jung, W.-M.; Lee, I.-S.; Lee, Y.-S.; Lee, H.; Park, H.-J.; Kim, N.; Chae, Y. Data Mining of Acupoint Characteristics from the Classical Medical Text: DongUiBoGam of Korean Medicine. Evid. Based Complement. Altern. Med. 2014, 2014, 329563. [Google Scholar] [CrossRef]
- Jung, W.-M.; Lee, T.; Lee, I.-S.; Kim, S.; Jang, H.; Kim, S.-Y.; Park, H.-J.; Chae, Y. Spatial Patterns of the Indications of Acupoints Using Data Mining in Classic Medical Text: A Possible Visualization of the Meridian System. Evid. Based Complement. Altern. Med. 2015, 2015, 457071. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.M.; Lee, S.H.; Lee, Y.S.; Chae, Y. Exploring spatial patterns of acupoint indications from clinical data: A STROBE-compliant article. Medicine (Baltimore) 2017, 96, e6768. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.-M.; Park, I.-S.; Lee, Y.-S.; Kim, C.-E.; Lee, H.; Hahm, D.-H.; Park, H.-J.; Jang, B.-H.; Chae, Y. Characterization of hidden rules linking symptoms and selection of acupoint using an artificial neural network model. Front. Med. 2018, 13, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; CARE Group; Allaire, A.; Aronson, J.; Carpenter, J.; et al. The CARE guidelines: Consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Eom, Y.-J.; Lee, Y.-S.; Nam, D.; Chae, Y. The Current Status of Quality of Reporting in Acupuncture Treatment Case Reports: An Analysis of the Core Journal in Korea. Evid. Based Complement. Altern. Med. 2017, 2017, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-S.; Lee, Y.-R.; Chae, Y.; Park, S.-Y.; Oh, I.-H.; Jang, B.-H. Translation of Korean Medicine Use to ICD-Codes Using National Health Insurance Service-National Sample Cohort. Evid. Based Complement. Altern. Med. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, A. An information-theoretic perspective of tf–idf measures. Inf. Process. Manag. 2003, 39, 45–65. [Google Scholar] [CrossRef]
- Lee, Y.-S.; Ryu, Y.; Jung, W.-M.; Kim, J.; Lee, T.; Chae, Y. Understanding Mind-Body Interaction from the Perspective of East Asian Medicine. Evid. Based Complement. Altern. Med. 2017, 2017. [Google Scholar] [CrossRef]
- Gu, P.; Chen, H. Modern bioinformatics meets traditional Chinese medicine. Brief. Bioinform. 2014, 15, 984–1003. [Google Scholar] [CrossRef]
- Lu, A.; Jiang, M.; Zhang, C.; Chan, K. An integrative approach of linking traditional Chinese medicine pattern classification and biomedicine diagnosis. J. Ethnopharmacol. 2012, 141, 549–556. [Google Scholar] [CrossRef]
- Li, G.-Z.; Sun, S.; You, M.; Wang, Y.-L.; Liu, G.-P. Inquiry diagnosis of coronary heart disease in Chinese medicine based on symptom-syndrome interactions. Chin. Med. 2012, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.; Deng, F.; Wang, Y.; Xu, Z.; Liu, G.; Xu, J.; Gewiss, H. (Eds.) Classification Research on Syndromes of TCM Based on SVM. In Proceedings of the 2009 2nd International Conference on Biomedical Engineering and Informatics, Tianjin, China, 17–19 October 2009. [Google Scholar]
- Li, G.-Z.; Yan, S.-X.; You, M.; Sun, S.; Ou, A. Intelligent ZHENG Classification of Hypertension Depending on ML-kNN and Information Fusion. Evid. Based Complement. Altern. Med. 2012, 2012, 837245. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.X.; Xu, J.; Yan, J.J.; Wang, Y.Q.; Guo, R.; Liu, G.P.; Yan, H.X.; Qian, P.; Hong, Y.J. Analysis of the diagnostic consistency of Chinese medicine specialists in cardiovascular disease cases and syndrome identification based on the relevant feature for each label learning method. Chin. J. Integr. Med. 2015, 21, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, X.; Lv, B.; Yang, F.; Hong, Y. Reliable Multi-Label Learning via Conformal Predictor and Random Forest for Syndrome Differentiation of Chronic Fatigue in Traditional Chinese Medicine. PLoS ONE 2014, 9, e99565. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.; Zhou, C. (Eds.) An Approach to Syndrome Differentiation in Traditional Chinese Medicine based on Neural Network. In Proceedings of the Third International Conference on Natural Computation (ICNC 2007), Haikou, China, 24–27 August 2007. [Google Scholar]
- Liu, G.-P.; Yan, J.-J.; Wang, Y.-Q.; Zheng, W.; Zhong, T.; Lu, X.; Qian, P. Deep Learning Based Syndrome Diagnosis of Chronic Gastritis. Comput. Math. Methods Med. 2014, 2014, 938350. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Case | Diagnosis | % | |
|---|---|---|---|
| 1 | U63 | Fluid and humour | 40.6 |
| 2 | U73 | Stomach disease | 28.5 |
| 3 | U65 | Liver excess | 27.8 |
| 4 | U61 | Blood disorder | 40.3 |
| 5 | U62 | Qi-blood-yin-yang deficiency | 23.8 |
| 6 | U71 | Kidney disease | 38.6 |
| 7 | U65 | Liver excess | 30.7 |
| 8 | U30 | Diseases of the musculoskeletal system and connective tissue | 33.8 |
| 9 | U61 | Blood disorder | 19.9 |
| 10 | U62 | Qi-blood-yin-yang deficiency | 39.7 |
| Diagnosis Pattern Code Frequency (n) | Acupoints Frequency (%) | ||||
|---|---|---|---|---|---|
| U61 | ST36 | ST35 | LI4 | SP6 | SP10 |
| 460 | 32 (7.0%) | 27 (5.9%) | 26 (5.7%) | 25 (5.4%) | 21 (4.6%) |
| U62 | LI4 | ST36 | LR3 | KI3 | SP6 |
| 432 | 38 (8.8%) | 37 (8.6%) | 36 (8.3%) | 25 (5.8%) | 21 (4.9%) |
| U71 | KI3 | SP6 | KI7 | BL23 | LI4 |
| 424 | 40 (9.4%) | 25 (5.9%) | 18 (4.2%) | 16 (3.8%) | 15 (3.5%) |
| U65 | LR3 | LI4 | CV17 | GV20 | SP6 |
| 397 | 49 (12.3%) | 38 (9.6%) | 26 (6.5%) | 24 (6.0%) | 24 (6.0%) |
| U63 | ST36 | LI4 | CV12 | PC6 | ST40 |
| 378 | 39 (10.3%) | 33 (8.7%) | 32 (8.5%) | 24 (6.3%) | 21 (5.6%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.-H.; Yoon, D.-E.; Lee, Y.-S.; Jung, W.-M.; Kim, J.-H.; Chae, Y. Revealing Associations between Diagnosis Patterns and Acupoint Prescriptions Using Medical Data Extracted from Case Reports. J. Clin. Med. 2019, 8, 1663. https://doi.org/10.3390/jcm8101663
Kim C-H, Yoon D-E, Lee Y-S, Jung W-M, Kim J-H, Chae Y. Revealing Associations between Diagnosis Patterns and Acupoint Prescriptions Using Medical Data Extracted from Case Reports. Journal of Clinical Medicine. 2019; 8(10):1663. https://doi.org/10.3390/jcm8101663
Chicago/Turabian StyleKim, Cheol-Han, Da-Eun Yoon, Ye-Seul Lee, Won-Mo Jung, Joo-Hee Kim, and Younbyoung Chae. 2019. "Revealing Associations between Diagnosis Patterns and Acupoint Prescriptions Using Medical Data Extracted from Case Reports" Journal of Clinical Medicine 8, no. 10: 1663. https://doi.org/10.3390/jcm8101663