Acute Severe Asthma in Adolescent and Adult Patients: Current Perspectives on Assessment and Management

 ,
,
Abstract
:1. Introduction
2. Definition of Acute Severe Asthma
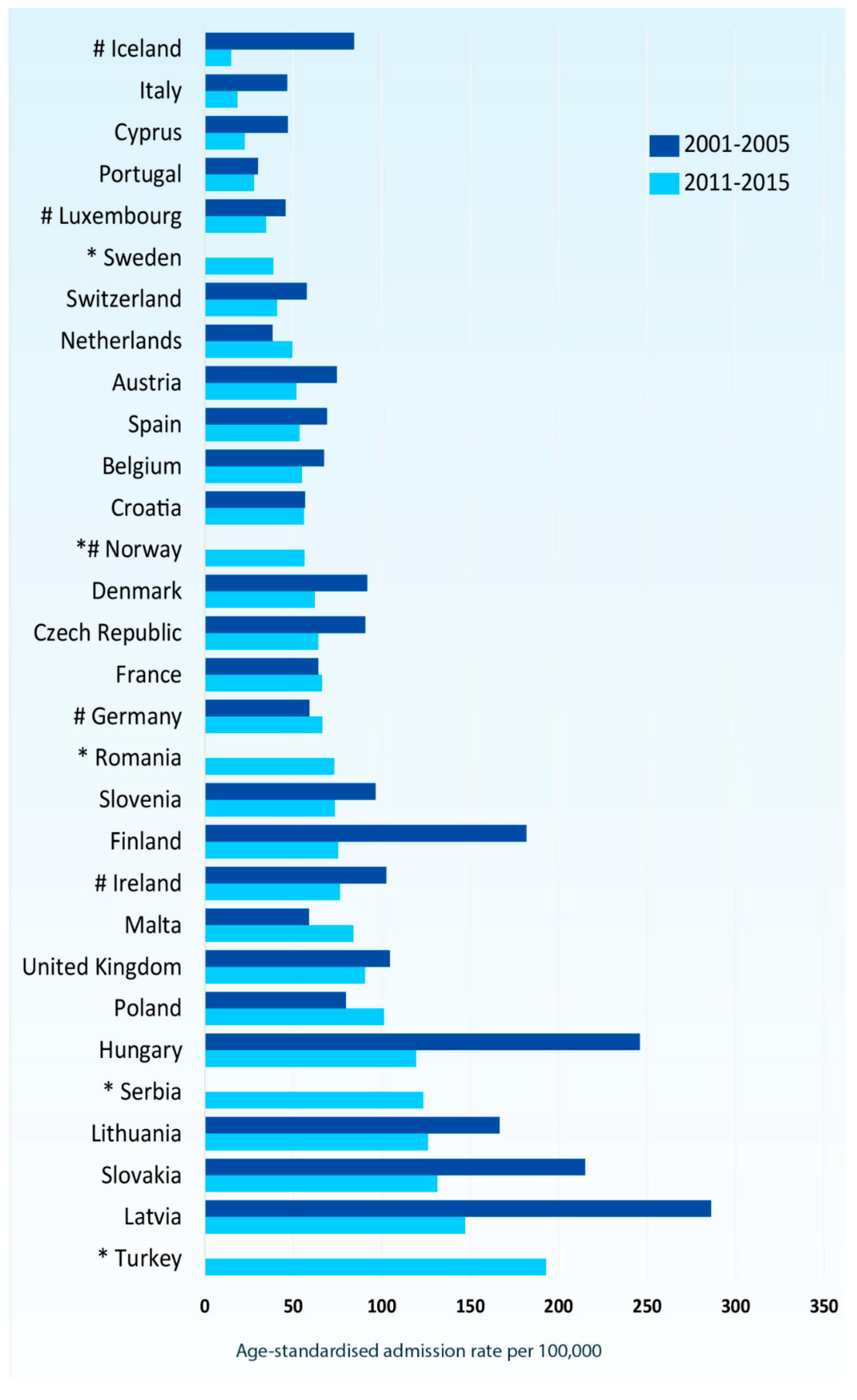
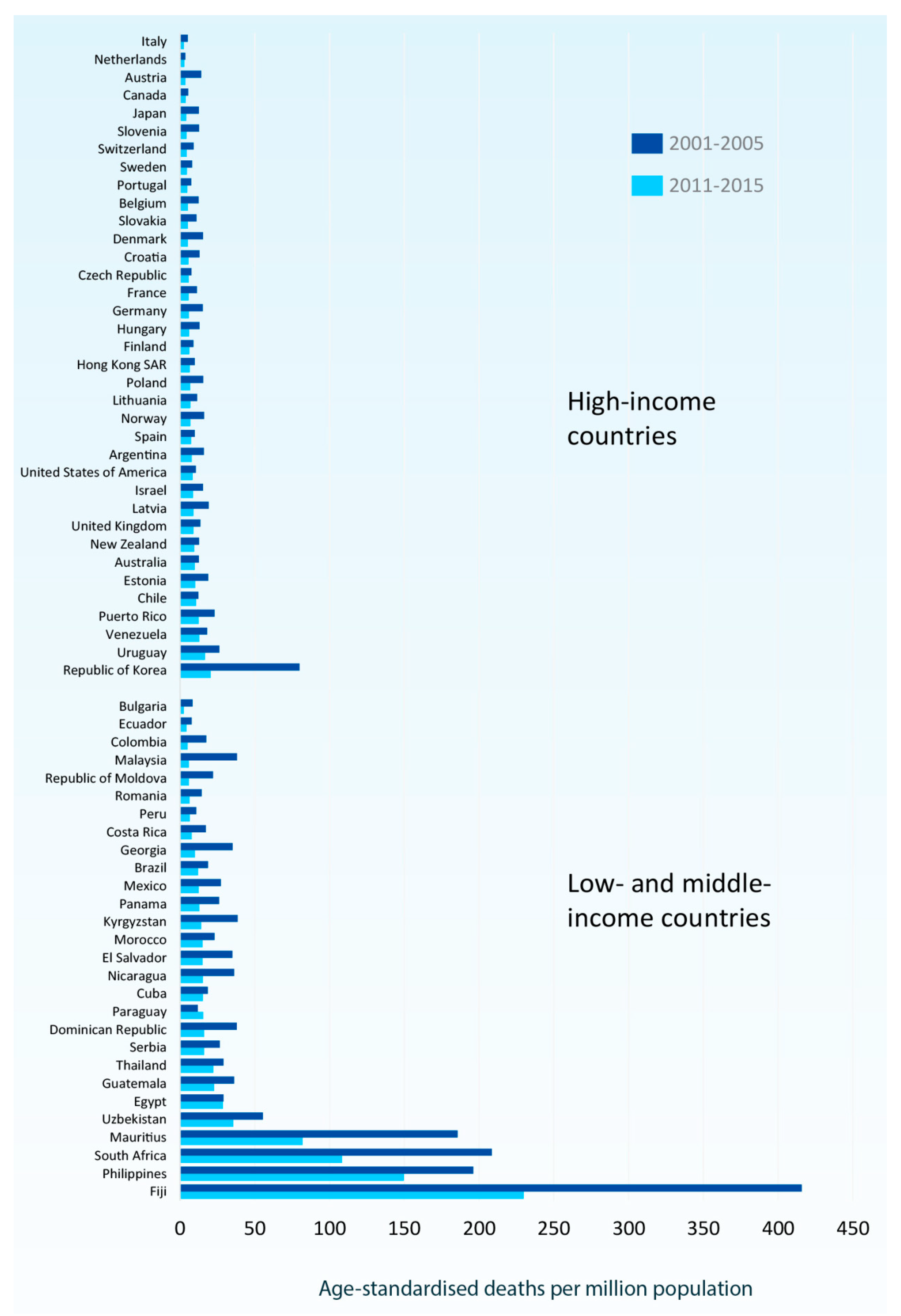
3. Epidemiology
4. Risk Factors for Asthma Exacerbations
5. Factors that Trigger Asthma Exacerbations
5.1. Respiratory Pathogens
5.2. Allergen Sensitization and Viral Infections
5.3. Allergen Exposure, Tobacco Smoke, and Environmental Pollutants
6. Genetic Associations with Asthma Exacerbations
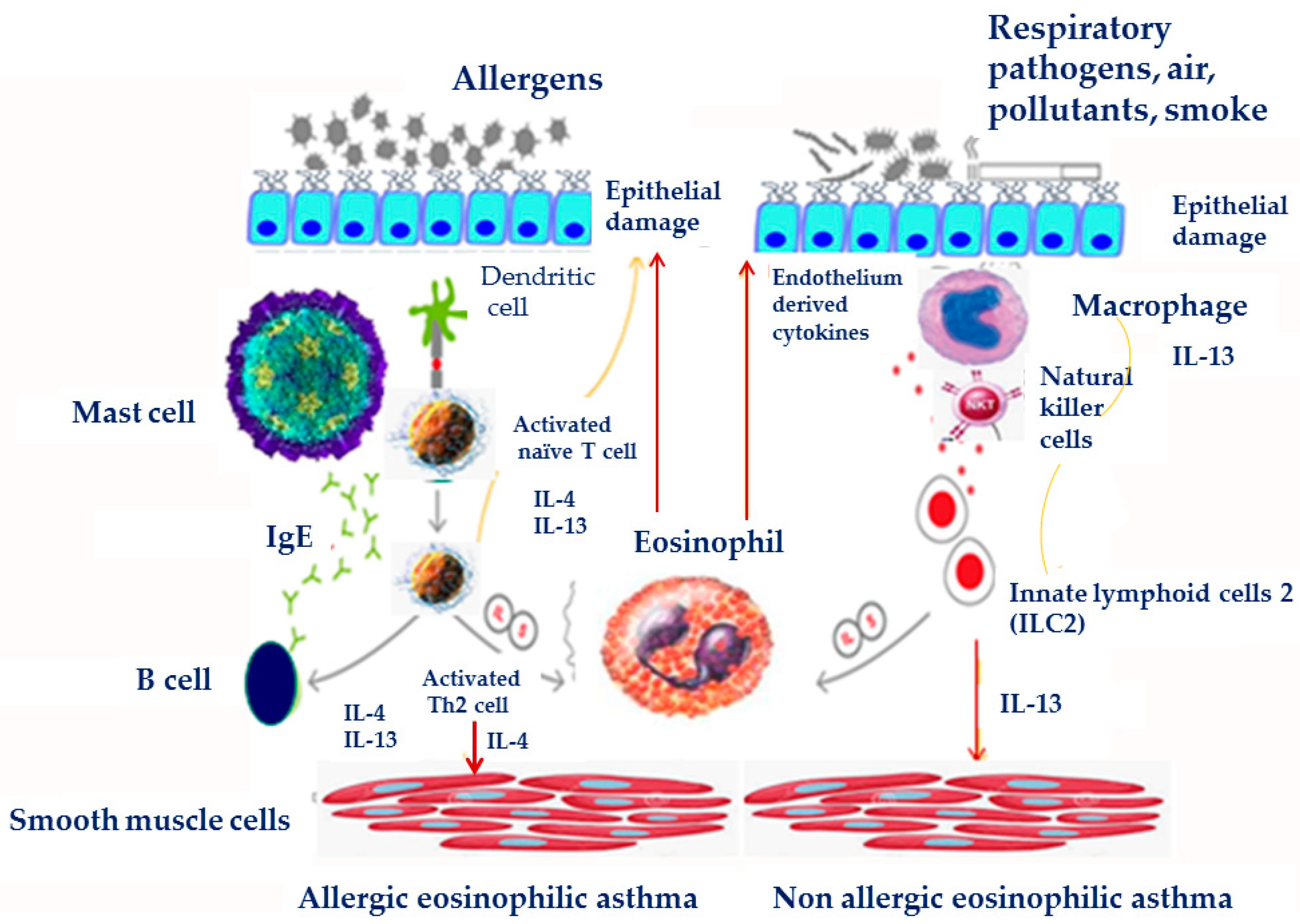
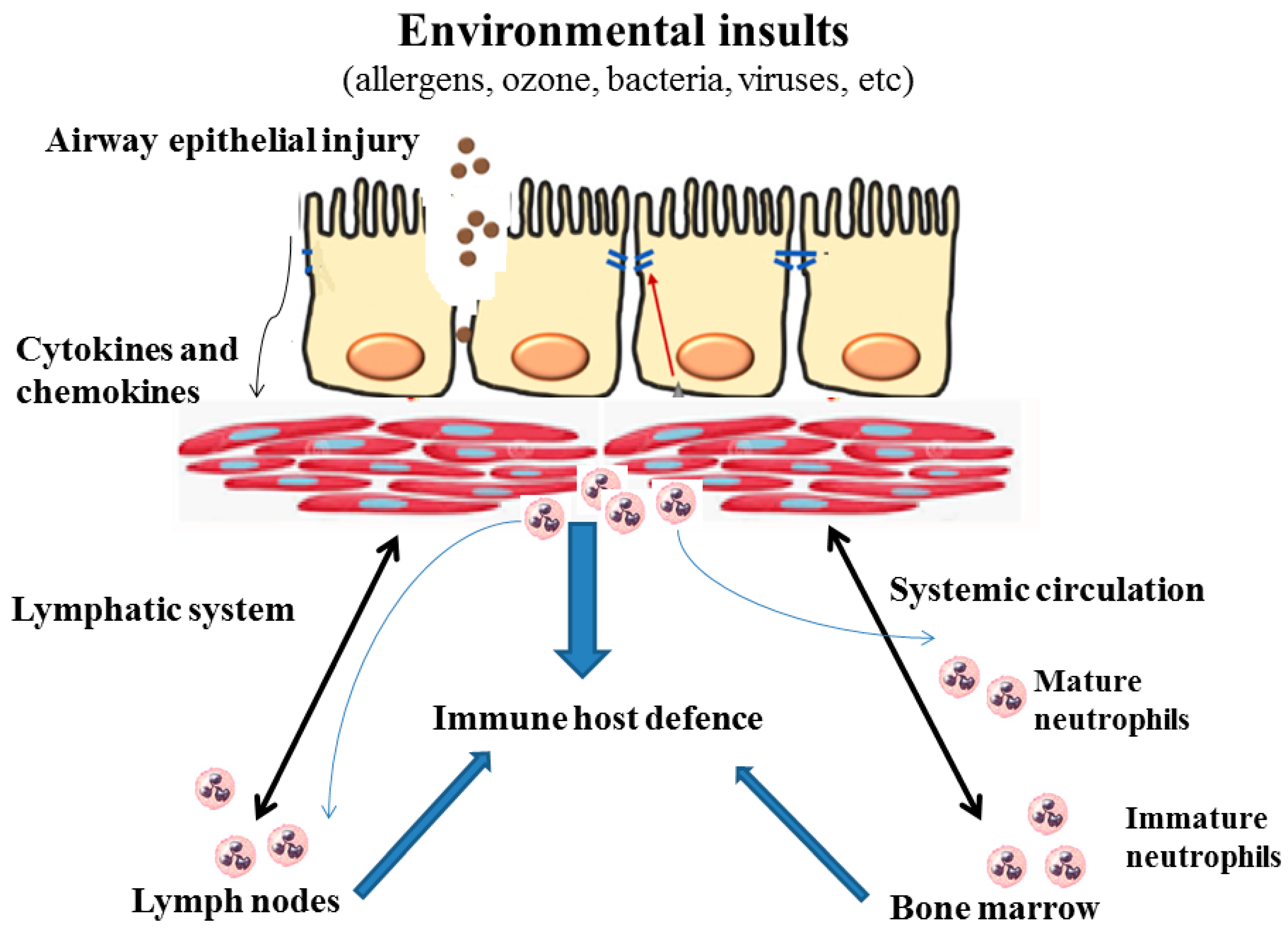
7. Pathogenesis-Immunobiology
8. Biomarkers Correlating with Risk of Asthma Exacerbations
9. Pathophysiology
10. Clinical Assessment
11. Pharmacological and Non-Pharmacological Management
11.1. β2-Adrenergic Receptor Agonists
11.2. Anticholinergics
11.3. Corticosteroids
11.4. Magnesium Sulfate
11.5. Methylxanthines
11.6. Leukotriene Modulators
11.7. Oxygen Supply
11.8. Heliox
11.9. Ketamine
11.10. Antibiotics
11.11. Non-Invasive Mechanical Ventilation
11.12. Invasive Mechanical Ventilation
11.13. Goals of Mechanical Ventilation
11.14. Permissive Hypercapnia
11.15. Additional and Unconventional Therapies for Acute Severe Asthma
11.15.1. Oxygen Delivery by High Flow Nasal Canula
11.15.2. Extracorporeal Life Support (ECLS)
11.15.3. Anesthetic Agents
11.15.4. Enoximone
12. Prognosis
13. Prevention and Risk Reduction
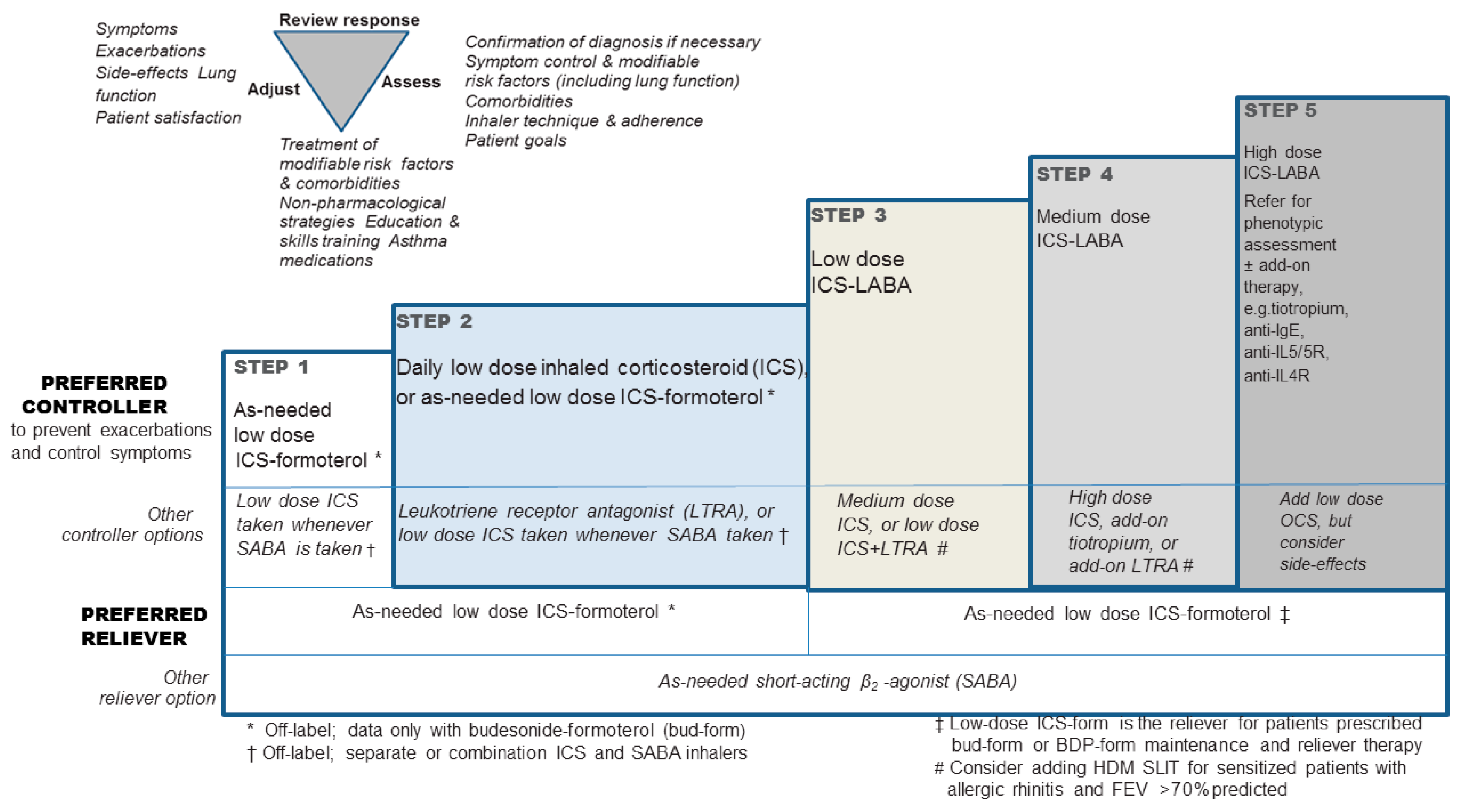
- Requirement for treatment with high-dose inhaled corticosteroids (ICS) and a second controller (and/or systemic corticosteroids) to maintain control.
- Refractory to the treatment mentioned above.
- Incomplete management of comorbidities such as severe sinus disease or obesity.
14. Conclusions
Author Contributions
Conflicts of Interest
References
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention (2019 Update). Available online: http://search.ebscohost.com/login.aspx?direct=true&db=cin20&A.N.=118972966&site=ehost-live (accessed on 6 August 2019).
- Teach, S.J.; Gill, M.A.; Togias, A.; Sorkness, C.A.; Arbes, S.J., Jr.; Calatroni, A.; Wildfire, J.J.; Gergen, P.J.; Cohen, R.T.; Pongracic, J.A.; et al. Preseasonal treatment with either omalizumab or an inhaled corticosteroid boost to prevent fall asthma exacerbations. J. Allergy Clin. Immunol. 2015, 136, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Trasande, L.; Thurston, G.D. The role of air pollution in asthma and other pediatric morbidities. J. Allergy Clin. Immunol. 2005, 115, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Rosser, F.; Brehm, J.M.; Forno, E.; Acosta-Pérez, E.; Kurland, K.; Canino, G.; Celedón, J.C. Proximity to a major road, vitamin D insufficiency, and severe asthma exacerbations in Puerto Rican children. Am. J. Respir. Crit. Care Med. 2014, 190, 1190–1193. [Google Scholar] [CrossRef] [PubMed]
- Shmool, J.L.; Kubzansky, L.D.; Newman, O.D.; Spengler, J.; Shepard, P.; Clougherty, J.E. Social stressors and air pollution across New York City communities: A spatial approach for assessing correlations among multiple exposures. Environ. Health 2014, 13, 91. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.L.; Pattemore, P.K.; Sanderson, G.; Smith, S.; Lampe, F.; Josephs, L.; Symington, P.; O’Toole, S.; Myint, S.H.; Tyrrell, D.A.J.; et al. Community study of role of viral infections in exacerbations of asthma in 9–11 year old children. BMJ 1995, 310, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.J.; Johnston, S.L. The role of viruses in acute exacerbations of asthma. J. Allergy Clin. Immunol. 2010, 125, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Jayasinghe, H.; Kopsaftis, Z.; Carson, K. Asthma Bronchiale and Exercise-Induced Bronchoconstriction. Respiration 2015, 89, 505–512. [Google Scholar] [CrossRef] [PubMed]
- D’Amato, M.; Molino, A.; Calabrese, G.; Cecchi, L.; Annesi-Maesano, I.; D’Amato, G. The impact of cold on the respiratory tract and its consequences to respiratory health. Clin. Transl. Allergy 2018, 8, 20. [Google Scholar] [CrossRef]
- Berns, S.H.; Halm, E.A.; Sampson, H.A.; Sicherer, S.H.; Busse, P.J.; Wisnivesky, J.P. Food allergy as a risk factor for asthma morbidity in adults. J. Asthma 2007, 44, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Vogel, N.M.; Katz, H.T.; Lopez, R.; Lang, D.M. Food allergy is associated with potentially fatal childhood asthma. J. Asthma 2008, 45, 862–866. [Google Scholar] [CrossRef]
- Williams, W.R. Asthma exacerbation by aspirin and chemical additives: Use of a nucleotide template model to investigate potential mechanisms. Gen. Physiol. Biophys. 2018, 37, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Ye, Y.M.; Kim, S.H.; Ban, G.Y.; Kim, S.C.; Kim, J.H.; Shin, Y.S.; Park, H.S. Identification of phenotypic clusters of nonsteroidal anti-inflammatory drugs exacerbated respiratory disease. Allergy 2017, 72, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Ledford, D.K.; Wenzel, S.E.; Lockey, R.F. Aspirin or other nonsteroidal inflammatory agent exacerbated asthma. J. Allergy Clin. Immunol. Pract. 2014, 2, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Plourde, A.; Lavoie, K.L.; Raddatz, C.; Bacon, S.L. Effects of acute psychological stress induced in laboratory on physiological responses in asthma populations: A systematic review. Respir. Med. 2017, 127, 21–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavoie, K.L.; Cartier, A.; Labrecque, M.; Bacon, S.L.; Lemière, C.; Malo, J.L.; Lacoste, G.; Barone, S.; Verrier, P.; Ditto, B. Are psychiatric disorders associated with worse asthma control and quality of life in asthma patients? Respir. Med. 2005, 99, 1249–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Byrne, P.M.; Inman, M.D. Bronchial hyperresponsiveness. Chest 2003, 123, 411S–416S. [Google Scholar] [CrossRef] [PubMed]
- Wills-Karp, M. Immunologic basis of antigen-induced airway hyperresponsiveness. Annu. Rev. Immunol. 1999, 17, 255–281. [Google Scholar] [CrossRef] [PubMed]
- Gauvreau, G.M.; El-Gammal, A.I.; O’Byrne, P.M. Allergen-induced airway responses. Eur. Respir. J. 2015, 46, 819–831. [Google Scholar] [CrossRef]
- Laprise, C.; Laviolette, M.; Boutet, M.; Boulet, L.P. Asymptomatic airway hyperresponsiveness: Relationships with airway inflammation and remodelling. Eur. Respir. J. 1999, 14, 63–73. [Google Scholar] [CrossRef]
- Leigh, R.; Ellis, R.; Wattie, J.; Southam, D.S.; De Hoogh, M.; Gauldie, J.; O’Byrne, P.M.; Inman, M.D. Dysfunction and remodeling of the mouse airway persist after resolution of acute allergen-induced airway inflammation. Am. J. Respir. Cell Mol. Biol. 2002, 27, 526–535. [Google Scholar] [CrossRef]
- Southam, D.S.; Ellis, R.; Wattie, J.; Inman, M.D. Components of airway hyperresponsiveness and their associations with inflammation and remodeling in mice. J. Allergy Clin. Immunol. 2007, 119, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Leigh, R.; Ellis, R.; Wattie, J.N.; Hirota, J.A.; Matthaei, K.I.; Foster, P.S.; O’Byrne, P.M.; Inman, M.D. Type 2 cytokines in the pathogenesis of sustained airway dysfunction and airway remodeling in mice. Am. J. Respir. Crit. Care Med. 2004, 169, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Brożek, J.L.; Bousquet, J.; Agache, I.; Agarwal, A.; Bachert, C.; Bosnic-Anticevich, S.; Brignardello-Petersen, R.; Canonica, G.W.; Casale, T.; Chavannes, N.H.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines-2016 revision. J. Allergy Clin. Immunol. 2017, 140, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Dixon, A.E.; Kaminsky, D.A.; Holbrook, J.T.; Wise, R.A.; Shade, D.M.; Irvin, C.G. Allergic rhinitis and sinusitis in asthma: Differential effects on symptoms and pulmonary function. Chest 2006, 130, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Rivera, C.; Crespo, A.; Pinedo-Sierra, C.; García-Rivero, J.L.; Pallarés-Sanmartín, A.; Marina-Malanda, N.; Pascual-Erquicia, S.; Padilla, A.; Mayoralas-Alises, S.; Plaza, V.; et al. Mucus hypersecretion in asthma is associated with rhinosinusitis, polyps and exacerbations. Respir. Med. 2018, 135, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayres, J.G.; Miles, J.F. Oesophageal reflux and asthma. Eur. Respir. J. 1996, 9, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Pereira Vega, A.; Sánchez Ramos, J.L.; Maldonado Pérez, J.A.; Alvarez Gutierrez, F.J.; Ignacio García, J.M.; Vázquez Oliva, R.; Romero, P.P.; Bravo, N.J.M.; Sánchez, R.I.; Gil, M.F. Variability in the prevalence of premenstrual asthma. Eur. Respir. J. 2010, 35, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Moragón, E.; Plaza, V.; Serrano, J.; Picado, C.; Galdiz, J.B.; López-Viña, A.; Sanchis, J. Near-fatal asthma related to menstruation. J. Allergy Clin. Immunol. 2004, 113, 242–244. [Google Scholar] [CrossRef]
- Cohen, J.M.; Bateman, B.T.; Huybrechts, K.F.; Mogun, H.; Yland, J.; Schatz, M.; Wurst, K.E.; Hernandez-Diaz, S. Poorly Controlled Asthma During Pregnancy Remains Common in the United States. J. Allergy Clin. Immunol. Pract 2019. [Google Scholar] [CrossRef]
- To, T.; Feldman, L.Y.; Zhu, J.; Gershon, A.S. Asthma health services utilisation before, during and after pregnancy: A population-based cohort study. Eur. Respir. J. 2018, 51, 1800209. [Google Scholar] [CrossRef]
- British Thoracic Society; Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma-QRG; Royal College of Physicians: London, UK, 2003. [Google Scholar]
- Reddel, H.K.; Taylor, D.R.; Bateman, E.D.; Boulet, L.; Boushey, H.A.; Busse, W.W.; Casale, T.B.; Chanez, P.; Enright, P.L.; Gibson, P.G.; et al. American Thoracic Society Documents an Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations. Am. J. Respir. Crit. Care Med. 2009, 180, 59–99. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, N.; Zeki, A.; Albertson, T.E.; Louie, S. Definition of Critical Asthma Syndromes. Clin. Rev. Allergy Immunol. 2015, 48, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bel, E.H.; Sousa, A.; Fleming, L.; Bush, A.; Chung, K.F.; Versnel, J.; Wagener, A.H.; Wagers, S.S.; Sterk, P.J.; Compton, C.H.; et al. Diagnosis and definition of severe refractory asthma: An international consensus statement from the Innovative Medicine Initiative (IMI). Thorax 2011, 66, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Saltoun, C.A. Acute severe asthma (status asthmaticus). Allergy Asthma Proc. 2012, 33, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef]
- Eurostat (Version Dated November 2017). Available online: www.ec.europa.eu/Eurostat/web/health/health-care/data/database (accessed on 6 August 2019).
- Vieira, E.; Alvaro, P.; Rodrigo, A.C.; Regina, A.; Fernandes, F.L.A.; Barreto, M.L.; Stelmach, R. Urbanization is associated with increased asthma morbidity and mortality in Brazil. Clin. Respir. J. 2018, 12, 410–417. [Google Scholar]
- Krishnan, V.; Diette, G.B.; Rand, C.S.; Bilderback, A.L.; Merriman, B.; Hansel, N.N.; Krishnan, J.A. Mortality in Patients Hospitalized for Asthma Exacerbations in the United States. Am. J. Respir. Crit. Care Med. 2006, 174, 633–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zein, J.G.; Udeh, B.L.; Teague, W.G.; Koroukian, S.M.; Schlitz, N.K.; Bleecker, E.R.; Busse, W.B.; Calhoun, W.J.; Castro, M.; Count, S.A.; et al. Impact of Age and Sex on Outcomes and Hospital Cost of Acute Asthma in the United States, 2011–2012. PLoS ONE 2016, 11, e0157301. [Google Scholar] [CrossRef] [PubMed]
- Sekiya, K.; Nakatani, E.; Fukutomi, Y.; Kaneda, H.; Iikura, M.; Yoshida, M.; Takahashi, K.; Tomii, K.; Nishikawa, M.; Kaneko, N.; et al. Severe or life-threatening asthma exacerbation: Patient heterogeneity identified by cluster analysis. Clin. Exp. Allergy 2016, 46, 1043–1055. [Google Scholar] [CrossRef] [PubMed]
- Yii, A.; Tan, J.; Lapperre, T. Long-term future risk of severe exacerbations: Distinct 5-year trajectories of problematic asthma. Allergy 2017, 72, 1398–1405. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.G.; Woodruff, P.G.; Clark, S.; Camargo, C.A. Sudden-onset asthma exacerbations: Clinical features, response to therapy, and 2-week follow-up. Eur. Respir. J. 2000, 15, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Ramnath, V.R.; Clark, S.; Camargo, C.A.J. Multicenter Study of Clinical Features of Sudden-Onset Versus Slower-Onset Asthma Exacerbations Requiring Hospitalization. Respir. Care 2007, 52, 1013–1020. [Google Scholar] [PubMed]
- Skobeloff, E.M.; Spivey, W.H.; St Clair, S.S.; Schoffstall, J.M. The influence of age and sex on asthma admissions. JAMA 1992, 268, 3437–3440. [Google Scholar] [CrossRef]
- Tattersfield, A.E.; Postma, D.S.; Barnes, P.J.; Svensson, K.; Bauer, C.A.; O’Byrne, P.M.; Lofdahl, C.G.; Pauwels, R.A.; Ullman, A. Exacerbations of asthma: A descriptive study of 425 severe exacerbations. Am. J. Respir. Crit. Care Med. 1999, 160, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Borish, L.; Chipps, B.; Deniz, Y.; Gujrathi, S.; Zheng, B.; Dolan, C.M.; TENOR Study Group. Total serum IgE levels in a large cohort of patients with severe or difficult-to-treat asthma. Ann. Allergy Asthma Immunol. 2005, 95, 247–253. [Google Scholar] [CrossRef]
- Leynaert, B.; Sunyer, J.; Garcia-Esteban, R.; Svanes, C.; Jarvis, D.; Cerveri, I.; Dratva, J.; Gislason, T.; Heinrich, J.; Janson, C.; et al. Gender differences in prevalence, diagnosis and incidence of allergic and nonallergic asthma: A population-based cohort. Thorax 2012, 67, 625–631. [Google Scholar] [CrossRef]
- Redmond, A.M.; James, A.W.; Nolan, S.H.; Self, T.H. Premenstrual asthma: Emphasis on drug therapy options. J. Asthma 2004, 41, 687–693. [Google Scholar] [CrossRef]
- Guy, E.S.; Kirumaki, A.; Hanania, N.A. Acute asthma in pregnancy. Crit. Care Clin. 2004, 20, 731–745. [Google Scholar] [CrossRef]
- Moore, W.C.; Meyers, D.A.; Wenzel, S.E.; Teague, W.G.; Li, H.; Li, X.; D’Agostino, R., Jr.; Castro, M.; Curran-Everett, D.; Fitzpatrick, A.M.; et al. Identification of asthma phenotypes using cluster analysis in the Severe Asthma Research Program. Am. J. Respir. Crit. Care Med. 2010, 181, 315–323. [Google Scholar] [CrossRef]
- Peters, U.; Dixon, A.E.; Forno, E. Obesity and asthma. J. Allergy Clin. Immunol. 2018, 141, 1169–1179. [Google Scholar] [CrossRef] [Green Version]
- Eisner, M.D.; Katz, P.P.; Yelin, E.H.; Shiboski, S.C.; Blanc, P.D. Risk factors for hospitalization among adults with asthma: The influence of sociodemographic factors and asthma severity. Respir. Res. 2001, 2, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Griswold, S.K.; Nordstrom, C.R.; Clark, S.; Gaeta, T.J.; Price, M.L.; Camargo, C.A., Jr. Asthma exacerbations in North American adults: Who are the ‘frequent fliers’ in the emergency department? Chest 2005, 127, 1579–1586. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Hennessey, P.A.; Formica, M.A.; Cox, C.; Walsh, E.E. Respiratory syncytial virus infection in elderly and high-risk adults. N. Engl. J. Med. 2005, 352, 1749–1759. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.K.; Kim, T.S.; Hufford, M.M.; Braciale, T.J. Viral infection of the lung: Host response and sequelae. J. Allergy Clin. Immunol. 2013, 132, 1263–1276. [Google Scholar] [CrossRef] [PubMed]
- Rumpel, J.A.; Ahmedani, B.K.; Peterson, E.L.; Wells, K.E.; Yang, M.; Levin, A.M.; Yang, J.J.; Kumar, R.; Burchard, E.G.; Williams, L.K. Genetic ancestry and its association with asthma exacerbations among African American subjects with asthma. J. Allergy Clin. Immunol. 2012, 130, 1302–1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddel, H.; Ware, S.; Marks, G.; Salome, C.; Jenkins, C.; Woolcock, A. Differences between asthma exacerbations and poor asthma control. Lancet 1999, 353, 364–369. [Google Scholar] [CrossRef]
- Pauwels, R.A.; Pedersen, S.; Busse, W.W.; Tan, W.C.; Chen, Y.Z.; Ohlsson, S.V.; Ullman, A.; Lamm, C.J.; O’Byrne, P.M.; START Investigators Group. Early intervention with budesonide in mild persistent asthma: A randomised, double-blind trial. Lancet 2003, 361, 1071–1076. [Google Scholar] [CrossRef]
- Rodrigo, G.J. Anticholinergics for asthma. Curr. Opin. Allergy Clin. Immunol. 2018, 18, 38–43. [Google Scholar] [CrossRef]
- Kirkland, S.; Vandenberghe, C.; Voaklander, B. Combined inhaled beta-agonist and anticholinergic agents for emergency management in adults with asthma (Review). Cochrane Database Syst. Rev. 2017, 1, CD001284. [Google Scholar]
- Gottlieb, M.; Kuhns, M.J. Do Inhaled Anticholinergic Agents in Addition to β; -Agonists Improve Outcomes in Acute Asthma Exacerbations? Ann. Emerg. Med. 2017, 70, 421–422. [Google Scholar] [CrossRef]
- Bobrovitz, N.; Heneghan, C.; Onakpoya, I.; Fletcher, B.; Collins, D.; Tompson, A.; Lee, J.; Nunan, D.; Fisher, R.; Scott, B.; et al. Medications that reduce emergency hospital admissions: An overview of systematic reviews and prioritisation of treatments. BMC Med. 2018, 16, 115. [Google Scholar] [CrossRef] [PubMed]
- Suissa, S.; Ernst, P. Inhaled corticosteroids: Impact on asthma morbidity and mortality. J. Allergy Clin. Immunol. 2001, 107, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.K.; Lee, J.H.; Miller, D.P.; Wenzel, S.E. Recent asthma exacerbations: A key predictor of future exacerbations. Respir. Med. 2007, 101, 481–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Covar, R.A.; Szefler, S.J.; Zeiger, R.S.; Sorkness, C.A.; Moss, M.; Mauger, D.T.; Boehmer, S.J.; Strunk, R.C.; Martinez, F.D.; Taussig, L.M.; et al. Factors associated with asthma exacerbations during a long-term clinical trial of controller medications in children. J. Allergy Clin. Immunol. 2008, 122, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Haselkorn, T.; Fish, J.E.; Chipps, B.E.; Miller, D.P.; Chen, H.; Weiss, S.T. Effect of weight change on asthma related health outcomes in patients with severe or difficult-to-treat asthma. Respir. Med. 2009, 103, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Chipps, B.E.; Zeiger, R.S.; Borish, L.; Wenzel, S.E.; Yegin, A.; Hayden, M.L.; Miller, D.P.; Bleecker, E.R.; Simons, F.E.R.; Szefler, S.J.; et al. Key findings and clinical implications from The Epidemiology and Natural History of Asthma: Outcomes and Treatment and Treatment Regimens (TENOR) study. J. Allergy Clin. Immunol. 2012, 130, 332–342. [Google Scholar] [CrossRef]
- Wenzel, S. Severe asthma: From characteristics to phenotypes to endotypes. Clin. Exp. Allergy 2012, 42, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, S.E. Asthma phenotypes: The evolution from clinical to molecular approaches. Nat. Med. 2012, 18, 716–725. [Google Scholar] [CrossRef] [PubMed]
- Killian, K.J.; Watson, R.; Otis, J.; St Amand, T.A.; O’Byrne, P.M. Symptom perception during acute bronchoconstriction. Am. J. Respir. Crit. Care Med. 2000, 162, 490–496. [Google Scholar] [CrossRef]
- Magadle, R.; Berar-Yanay, N.; Weiner, P. The risk of hospitalization and near-fatal and fatal asthma in relation to the perception of dyspnea. Chest 2002, 121, 329–333. [Google Scholar] [CrossRef]
- Hancox, R.J.; Cowan, J.O.; Flannery, E.M.; Herbison, G.P.; McLachlan, C.R.; Taylor, D.R. Bronchodilator tolerance and rebound bronchoconstriction during regular inhaled beta-agonist treatment. Respir. Med. 2000, 94, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Stanford, R.H.; Shah, M.B.; D’Souza, A.O.; Dhamane, A.D.; Schatz, M. Short-acting β-agonist use and its ability to predict future asthma related outcomes. Ann. Allergy Asthma Immunol. 2012, 109, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Suissa, S.; Ernst, P.; Benayoun, S.; Baltzan, M.; Cai, B. Low-dose inhaled corticosteroids and the prevention of death from asthma. N. Engl. J. Med. 2000, 343, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Adolescents and Adults with Difficult-to-Treat and Severe Asthma. Available online: http://search.ebscohost.com/login.aspx?direct=true&db=cin20&A.N.=118972966&site=ehost-live (accessed on 6 August 2019).
- Alvarez, G.G.; FitzGerald, J.M. A systematic review of the psychological risk factors associated with near fatal asthma or fatal asthma. Respiration 2007, 74, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Foster, J.M.; McDonald, V.M.; Guo, M.; Reddel, H.K. “I have lost in every facet of my life”: The hidden burden of severe asthma. Eur. Respir. J. 2017, 50, 1700765. [Google Scholar] [CrossRef] [PubMed]
- Denlinger, L.C.; Phillips, B.R.; Ramratnam, S.; Ross, K.; Bhakta, N.R.; Cardet, J.C.; Castro, M.; Peters, S.P.; Phipatanakul, W.; Aujla, S.; et al. Inflammatory and Comorbid Features of Patients with Severe Asthma and Frequent Exacerbations. Am. J. Respir. Crit. Care Med. 2017, 195, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Grissell, T.V.; Powell, H.; Shafren, D.R.; Boyle, M.J.; Hensley, M.J.; Jones, P.D.; Whitehead, B.F.; Gibson, P.G. Interleukin-10 gene expression in acute virus-induced asthma. Am. J. Respir. Crit. Care Med. 2005, 172, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Libster, R.; Bugna, J.; Coviello, S.; Hijano, D.R.; Dunaiewsky, M.; Reynoso, N.; Cavalieri, M.L.; Guglielmo, M.C.; Areso, M.S.; Gilligan, T.; et al. Pediatric hospitalizations associated with 2009 pandemic influenza A (H1N1) in Argentina. N. Engl. J. Med. 2010, 362, 45–55. [Google Scholar] [CrossRef]
- O’Riordan, S.; Barton, M.; Yau, Y.; Read, S.E.; Allen, U.; Tran, D. Risk factors and outcomes among children admitted to hospital with pandemic H1N1 influenza. Cmaj 2010, 182, 39–44. [Google Scholar] [CrossRef]
- Winther, B.; Gwaltney, J.M.; Hendley, J.O. Respiratory virus infection of monolayer cultures of human nasal epithelial cells. Am. Rev. Respir. Dis. 1990, 141, 839–845. [Google Scholar] [CrossRef]
- Unger, B.L.; Ganesan, S.; Comstock, A.T.; Faris, A.N.; Hershenson, M.B.; Sajjan, U.S. Nod-like receptor X-1 is required for rhinovirus-induced barrier dysfunction in airway epithelial cells. J. Virol. 2014, 88, 3705–3718. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.E.; Lamson, D.M.; St George, K.; Walsh, T.J. Human rhinoviruses. Clin. Microbiol. Rev. 2013, 26, 135–162. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, A.I.; Jackson, D.J.; Edwards, M.R.; Johnston, S.L. Airway epithelial orchestration of innate immune function in response to virus infection. A focus on asthma. Ann. Am. Thorac. Soc. 2016, 13, S55–S63. [Google Scholar] [PubMed]
- Fensterl, V.; Sen, G.C. Interferons and viral infections. Biofactors 2009, 35, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Makris, S.; Johnston, S. Recent advances in understanding rhinovirus immunity. F1000Research 2018, 24, 7. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.K.; Hernandez, J.Z.; Wimmenauer, V.; Shepherd, B.E.; Hijano, D.; Libster, R.; Serra, M.E.; Bhat, N.; Batalle, J.P.; Mohamed, Y.; et al. A mechanistic role for type, III IFN-_1 in asthma exacerbations mediated by human rhinoviruses. Am. J. Respir. Crit. Care Med. 2012, 185, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.C.; Anderson, D.; Galbraith, S.; Fantino, E.; Gutierrez Cardenas, D.; Read, J.F.; Serralha, M.; Holt, B.J.; Strickland, D.H.; Sly, P.D.; et al. Personalised transcriptomics reveals heterogeneous immunophenotypes in children with viral bronchiolitis. Am. J. Respir. Crit. Care Med. 2019, 199, 1537–1549. [Google Scholar] [CrossRef] [PubMed]
- Khoo, S.K.; Read, J.; Franks, K.; Zhang, G.; Bizzintino, J.; Coleman, L.; McCrae, C.; Öberg, L.; Troy, N.M.; Prastanti, F.; et al. Upper airway cell transcriptomics identify a major new immune, logical phenotype with strong clinical correlates in young children with acute wheezing. J. Immunol. 2019, 202, 1845–1858. [Google Scholar] [CrossRef] [PubMed]
- Turi, K.N.; Shankar, J.; Anderson, L.J.; Rajan, D.; Gaston, K.; Gebretsadik, T.; Das, S.R.; Stone, C.; Larkin, E.K.; Rosas-Salazar, C.; et al. Infant viral respiratory infection nasal immune-response patterns and their association with subsequent childhood recurrent wheeze. Am. J. Respir. Crit. Care Med. 2018, 198, 1064–1073. [Google Scholar] [CrossRef] [PubMed]
- Fedele, G.; Schiavoni, I.; Nenna, R.; Pierangeli, A.; Frassanito, A.; Leone, P.; Petrarca, L.; Scagnolari, C.; Midulla, F. Analysis of the immune response in infants hospitalized with viral bronchiolitis shows different Th1/Th2 profiles associated with respiratory syncytial virus and human rhinovirus. Pediatr. Allergy Immunol. 2018, 29, 555–557. [Google Scholar] [CrossRef] [PubMed]
- Oliver, B.G.; Lim, S.; Wark, P.; Laza-Stanca, V.; King, N.; Black, J.L.; Roth, M.; Johnston, S.L. Rhinovirus exposure impairs immune responses to bacterial products in human alveolar macrophages. Thorax 2008, 63, 519–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harford, C.G.; Leidler, V.; Hara, M. Effect of the lesion due to influenza virus on the resistance of mice to inhaled pneumococci. J. Exp. Med. 1949, 89, 53–68. [Google Scholar] [CrossRef] [PubMed]
- Kloepfer, K.M.; Lee, W.M.; Pappas, T.E.; Kang, T.J.; Vrtis, R.F.; Evans, M.D.; Gangnon, R.E.; Bochkov, Y.A.; Jackson, D.J.; Lemanske, R.F., Jr.; et al. Detection of pathogenic bacteria during rhinovirus infection is associated with increased respiratory symptoms and asthma exacerbations. J. Allergy Clin. Immunol. 2014, 133, 1301–1307. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, N.G.; Stanciu, L.A.; Papi, A.; Holgate, S.T.; Johnston, S.L. Rhinovirus-induced alterations on peripheral blood mononuclear cell phenotype and costimulatory molecule expression in normal and atopic asthmatic subjects. Clin. Exp. Allergy 2002, 32, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.J.; Makrinioti, H.; Rana, B.M.; Shamji, B.W.; Trujillo-Torralbo, M.B.; Footitt, J.; Del-Rosario, J.; Telcian, A.G.; Nikonova, A.; Zhu, J.; et al. IL-33-dependent type 2 inflammation during rhinovirus-induced asthma exacerbations in vivo. Am. J. Respir. Crit. Care Med. 2014, 190, 1373–1382. [Google Scholar] [CrossRef] [PubMed]
- Beale, J.; Jayaraman, A.; Jackson, D.J.; Macintyre, J.D.R.; Edwards, M.R.; Walton, R.P.; Zhu, J.; Ching, Y.M.; Shamji, B.; Edwards, M.; et al. Rhinovirus-induced, IL-25 in asthma exacerbation drives type 2 immunity and allergic pulmonary inflammation. Sci. Transl. Med. 2014, 6, 256ra134. [Google Scholar] [CrossRef]
- Hong, J.Y.; Bentley, J.K.; Chung, Y.; Lei, J.; Steenrod, J.M.; Chen, Q.; Sajjan, U.S.; Hershenson, M.B. Neonatal rhinovirus induces mucous metaplasia and airways hyperresponsiveness through, IL-25 and type 2 innate lymphoid cells. J. Allergy Clin. Immunol. 2014, 134, 429–439. [Google Scholar] [CrossRef]
- Shariff, S.; Shelfoon, C.; Holden, N.S.; Traves, S.L.; Wiehler, S.; Kooi, C.; Proud, D.; Leigh, R. Human rhinovirus infection of epithelial cells modulates airway smooth muscle migration. Am. J. Respir. Cell Mol. Biol. 2017, 56, 796–803. [Google Scholar] [CrossRef]
- Leigh, R.; Oyelusi, W.; Wiehler, S.; Koetzler, R.; Zaheer, R.S.; Newton, R.; Proud, D. Human rhinovirus infection enhances airway epithelial cell production of growth factors involved in airway remodeling. J. Allergy Clin. Immunol. 2008, 121, 1238–1245. [Google Scholar] [CrossRef]
- Djukanovic, R.; Harrison, T.; Johnston, S.L.; Gabbay, F.; Wark, P.; Thomson, N.C.; Niven, R.; Singh, D.; Reddel, H.K.; Davies, D.E.; et al. The effect of inhaled, I.F.N-beta on worsening of asthma symptoms caused by viral infections. A randomized trial. Am. J. Respir. Crit. Care Med. 2014, 190, 145–154. [Google Scholar] [CrossRef]
- Sporik, R.; Holgate, S.T.; Platts-Mills, T.A.; Cogswell, J.J. Exposure to house-dust mite allergen (Der p I) and the development of asthma in childhood. A prospective study. N. Engl. J. Med. 1990, 323, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Zureik, M.; Neukirch, C.; Leynaert, B.; Liard, R.; Bousquet, J.; Neukirch, F. Sensitisation to airborne moulds and severity of asthma: Cross sectional study from European Community respiratory health survey. BMJ 2002, 325, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Message, S.D.; Laza-Stanca, V.; Mallia, P.; Parker, H.L.; Zhu, J.; Kebadze, T.; Contoli, M.; Sanderson, G.; Kon, O.M.; Papi, A.; et al. Rhinovirus-induced lower respiratory illness is increased in asthma and related to virus load and Th1/2 cytokine and, IL-10 production. Proc. Natl. Acad. Sci. USA 2008, 105, 13562–13567. [Google Scholar] [CrossRef] [PubMed]
- Rosas, I.; McCartney, H.A.; Payne, R.W.; Calderon, C.; Lacey, J.; Chapela, R.; Ruiz-Velazco, S. Analysis of the relationships between environmental factors (aeroallergens, air pollution, and weather) and asthma emergency admissions to a hospital in Mexico City. Allergy 1998, 53, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Mitakakis, T.Z.; Marks, G.B.; Car, N.G.; Belousova, E.G.; Leuppi, J.D.; Xuan, W.; Downie, S.R.; Tobias, A.; Peat, J.K.; et al. Clinical importance of Alternaria exposure in children. Am. J. Respir. Crit. Care Med. 2001, 164, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Donohue, K.M.; Al-alem, V.; Perzanowshi, M.S.; Chew, G.L.; Johnson, A.; Divjan, A.; Kelvin, E.A.; Hoepner, L.A.; Perera, F.P.; Miller, R.L. Anti-cockroach and anti-mouse IgE are associated with early wheeze and atopy inan inner-city birth cohort. J. Allergy Clin. Immunol. 2008, 122, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Ouyang, F.X.; Pongracic, J.A.; Fang, Y.P.; Wang, B.Y.; Liu, X.; Xing, H.; Caruso, D.; Liu, X.; Zhang, S.; et al. Dissociation between the prevalence of atopy and allergic disease in rural China among children and adults. J. Allergy Clin. Immunol. 2008, 122, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Salo, P.M.; Arbes, S.J.; Crockett, P.W.; Thorne, P.S.; Cohn, R.D.; Zeldin, D.C. Exposure to multiple indoor allergens in, U.S. homes and its relationship to asthma. J. Allergy Clin. Immunol. 2008, 121, 678–684. [Google Scholar] [CrossRef]
- Kanchongkittiphon, W.; Mendell, M.J.; Gaffin, J.M.; Wang, G.; Phipatanakul, W. Indoor environmental exposures and exacerbation of asthma: An update to the 2000 review by the Institute of Medicine. Environ. Health Perspect. 2015, 123, 6–20. [Google Scholar] [CrossRef]
- Matsui, E.C. Environmental exposures and asthma morbidity in children living in urban neighborhoods. Allergy 2014, 69, 553–558. [Google Scholar] [CrossRef]
- Yang, J.J.; Burchard, E.G.; Choudhry, S.; Johnson, C.C.; Ownby, D.R.; Favro, D.; Chen, J.; Akana, M.; Ha, C.; Kwok, P.-Y.; et al. Differences in allergic sensitization by self-reported race and genetic ancestry. J. Allergy Clin. Immunol. 2008, 122, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Thomson, N.C.; Chaudhuri, R.; Livingston, E. Asthma and cigarette smoking. Eur. Respir. J. 2004, 24, 822–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polosa, R.; Knoke, J.D.; Russo, C.; Piccillo, G.; Caponnetto, P.; Sarva, M.; Proietti, L.; Al-Delaimy, W.K. Cigarette smoking is associated with a greater risk of incident asthma in allergic rhinitis. J. Allergy Clin. Immunol. 2008, 121, 1428–1434. [Google Scholar] [CrossRef] [PubMed]
- Quinto, K.B.; Kit, B.K.; Lukacs, S.L.; Akinbami, L.J. Environmental tobacco smoke exposure in children aged 3–19 years with and without asthma in the United States, 1999–2010. NCHS Data Brief 2013, 126, 1–8. [Google Scholar]
- McCarville, M.; Sohn, M.W.; Oh, E.; Weiss, K.; Gupta, R. Environmental tobacco smoke and asthma exacerbations and severity: The difference between measured and reported exposure. Arch. Dis. Child. 2013, 98, 510–514. [Google Scholar] [CrossRef]
- Vargas, P.A.; Brenner, B.; Clark, S.; Boudreaux, E.D.; Camargo, C.A., Jr. Exposure to environmental tobacco smoke among children presenting to the emergency department with acute asthma: A multicenter study. Pediatr. Pulmonol. 2007, 42, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Hassanzad, M.; Khalilzadeh, S.; Eslampanah Nobari, S.; Bloursaz, M.; Sharifi, H.; Mohajerani, S.A.; Nejad, S.T.; Velayati, A.A. Cotinine level is associated with asthma severity in passive smoker children. Iran. J. Allergy Asthma Immunol. 2015, 14, 67–73. [Google Scholar]
- Ferrante, G.; Simoni, M.; Cibella, F.; Liotta, G.; Malizia, V.; Corsello, G.; Viegi, G.; La Grutta, S. Third-hand smoke exposure and health hazards in children. Monaldi Arch. Chest Dis. 2013, 79, 38–43. [Google Scholar] [CrossRef]
- Samoli, E.; Nastos, P.T.; Paliatsos, A.G.; Katsouyanni, K.; Priftis, K.N. Acute effects of air pollution on pediatric asthma exacerbation: Evidence of association and effect modification. Environ. Res. 2011, 111, 418–424. [Google Scholar] [CrossRef]
- Gasana, J.; Dillikar, D.; Mendy, A.; Forno, E.; Ramos Vieira, E. Motor vehicle air pollution and asthma in children: A meta-analysis. Environ. Res. 2012, 117, 36–45. [Google Scholar] [CrossRef]
- Delfino, R.J.; Wu, J.; Tjoa, T.; Gullesserian, S.K.; Nickerson, B.; Gillen, D.L. Asthma morbidity and ambient air pollution: Effect modification by residential traffic-related air pollution. Epidemiology 2014, 25, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Moffatt, M.F.; Kabesch, M.; Liang, L.; Dixon, A.L.; Strachan, D.; Heath, S.; Depner, M.; von Berg, A.; Bufe, A.; Rietschel, E.; et al. Genetic variants regulating, ORMDL3 expression contribute to the risk of childhood asthma. Nature 2007, 448, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Portelli, M.A.; Hodge, E.; Sayers, I. Genetic risk factors for the development of allergic disease identified by genome-wide association. Clin. Exp. Allergy 2015, 45, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Du, R.; Litonjua, A.A.; Tantisira, K.G.; Lasky-Su, J.; Sunyaev, S.R.; Klanderman, B.J.; Celedon, J.C.; Avila, L.; Soto-Quiros, M.E.; Weiss, S.T.; et al. Genome-wide association study reveals class I M.H.C-restricted T cell-associated molecule gene (CRTAM) variants interact with vitamin D levels to affect asthma exacerbations. J. Allergy Clin. Immunol. 2012, 129, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Tavendale, R.; Macgregor, D.F.; Mukhopadhyay, S.; Palmer, C.N. A polymorphism controlling, ORMDL3 expression is associated with asthma that is poorly controlled by current medications. J. Allergy Clin. Immunol. 2008, 121, 860–863. [Google Scholar] [CrossRef] [PubMed]
- Tantisira, K.G.; Silverman, E.S.; Mariani, T.J.; Xu, J.; Richter, B.G.; Klanderman, B.J.; Litonjua, A.A.; Lazarus, R.; Rosenwasser, L.J.; Fuhlbrigge, A.L.; et al. FCER2: A pharmacogenetics basis for severe exacerbations in children with asthma. J. Allergy Clin. Immunol. 2007, 120, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Chupp, G.L.; Lee, C.G.; Jarjour, N.; Shim, Y.M.; Holm, C.T.; He, S.; Dziura, J.D.; Reed, J.; Coyle, A.J.; Kiener, P.; et al. A chitinase-like protein in the lung and circulation of patients with severe asthma. N. Engl. J. Med. 2007, 357, 2016–2027. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, J.; Basu, K.; Tavendale, R.; Palmer, C.N.; Smith, H.; Mukhopadhyay, S. The CHI3L1 rs4950928 poly morphism is associated with asthma-related hospital admissions in children and young adults. Ann. Allergy Asthma Immunol. 2011, 106, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.G.; Hartl, D.; Lee, G.R.; Koller, B.; Matsuura, H.; Da Silva, C.A.; Sohn, M.H.; Cohn, L.; Homer, R.J.; Kozhich, A.A.; et al. Role of breast regression protein 39 (BRP-39)/chitinase 3-like-1 in Th2 and, IL-13-induced tissue responses and apoptosis. J. Exp. Med. 2009, 206, 1149–1166. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Sun, Y.; Shi, Z.; Huang, H.; Fang, Z.; Chen, J.; Xiu, Q.; Li, B. YKL-40 induces, IL-8 expression from bronchial epithelium via, MAPK. (JNK and, ERK) and, NF-kB pathways, causing bronchial smooth muscle proliferation and migration. J. Immunol. 2013, 190, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.J.; Brightling, C. Pathogenesis of asthma: Implications for precision medicine. Clin. Sci. 2017, 131, 1723–1735. [Google Scholar] [CrossRef] [PubMed]
- Rovina, N.; Baraldo, S.; Saetta, M. Severe asthma: Inflammation. Pneumon 2011, 24, 306–313. [Google Scholar]
- Robinson, D.; Humbert, M.; Buhl, R.; Cruz, A.A.; Inoue, H.; Korom, S.; Hanania, N.A.; Nair, P. Revisiting Type 2-high and Type 2-low airway inflammation in asthma: Current knowledge and therapeutic implications. Clin. Exp. Allergy 2017, 47, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Santus, P.; Saad, M.; Damiani, G.; Patella, V.; Radovanovic, D. Current and future targeted therapies for severe asthma: Managing treatment with biologics based on phenotypes and biomarkers. Pharmacol. Res. 2019, 146, 104296. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, N.S.; Hollins, F.; Sutcliffe, A.; Saunders, R.; Shah, S.; Siddiqui, S.; Gupta, S.; Haldar, P.; Green, R.; Pavord, I.; et al. Eosinophil protein in airway macrophages: A novel biomarker of eosinophilic inflammation in patients with asthma. J. Allergy Clin. Immunol. 2010, 126, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2017, 391, 783–800. [Google Scholar] [CrossRef]
- Lambrecht, B.N.; Hammad, H. The immunology of asthma. Nat. Immunol. 2015, 16, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.; Gyles, S.L.; Wettey, F.R.; Gazi, L.; Townsend, E.; Hunter, M.G.; Pettipher, R. Prostaglandin D2 causes preferential induction of proinflammatory Th2 cytokine production through an action on chemoattractant receptor-like molecule expressed on Th2 cells. J. Immunol. 2005, 175, 6531–6536. [Google Scholar] [CrossRef] [PubMed]
- Doherty, T.A.; Broide, D.H. Group 2 innate lymphoid cells: New players in human allergic diseases. J. Investig. Allergol. ClinImmunol. 2015, 25, 1–11. [Google Scholar]
- Aron, J.L.; Akbari, O. Regulatory T cells and type 2 innate lymphoid cell-dependent asthma. Allergy 2017, 72, 1148–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sokolowska, M.; Chen, L.Y.; Liu, Y.; Martinez-Anton, A.; Logun, C.; Alsaaty, S.; Cuento, R.A.; Cai, R.; Sun, J.; Quehenberger, O.; et al. Dysregulation of lipidomic profile and antiviral immunity in response to hyaluronan in patients with severe asthma. J. Allergy Clin. Immunol. 2017, 139, 1379–1383. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Smith, S.G.; Salter, B.; El-Gammal, A.; Oliveria, J.P.; Obminski, C.; Watson, R.; O’Byrne, P.M.; Gauvreau, G.M.; Sehmi, R.; et al. Allergen-induced Increases in Sputum Levels of Group 2 Innate Lymphoid Cells in Subjects with Asthma. Am. J. Respir. Crit. Care Med. 2017, 196, 700–712. [Google Scholar] [CrossRef] [PubMed]
- Sugita, K.; Steer, C.A.; Martinez-Gonzalez, I.; Altunbulakli, C.; Morita, H.; Castro-Giner, F.; Kubo, T.; Wawrzyniak, P.; Ruckert, B.; Sudo, K.; et al. Type 2 innate lymphoid cells disrupt bronchial epithelial barrier integrity by targeting tight junctions through, IL-13 in asthmatic patients. J. Allergy Clin. Immunol. 2018, 141, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Wawrzyniak, P.; Wawrzyniak, M.; Wanke, K.; Sokolowska, M.; Bendelja, K.; Ruckert, B.; Globinska, A.; Jakiela, B.; Kast, J.I.; Idzko, M.; et al. Regulation of bronchial epithelial barrier integrity by type 2 cytokines and histone deacetylases in asthmatic patients. J. Allergy Clin. Immunol. 2017, 139, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Pascual, R.M.; Peters, S.P. Airway remodeling contributes to the progressive loss of lung function in asthma: An overview. J. Allergy Clin. Immunol. 2005, 116, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Doherty, T.; Broide, D. Cytokines and growth factors in airway remodeling in asthma. Curr. Opin. Immunol. 2007, 19, 676–680. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International, ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [PubMed]
- Strickland, D.H.; Holt, P.G. T regulatory cells in childhood asthma. Trends Immunol. 2011, 32, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Josefowicz, S.Z.; Niec, R.E.; Kim, H.Y.; Treuting, P.; Chinen, T.; Zheng, Y.; Umetsu, D.T.; Rudensky, A.Y. Extrathymically generated regulatory T cells control mucosal, TH2 inflammation. Nature 2012, 482, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Hartl, D.; Koller, B.; Mehlhorn, A.T.; Reinhardt, D.; Nicolai, T.; Schendel, D.J.; Griese, M.; Krauss-Etschmann, S. Quantitative and functional impairment of pulmonary, C.D.4+C.D.25hi regulatory T cells in pediatric asthma. J. Allergy Clin. Immunol. 2007, 119, 1258–1266. [Google Scholar] [CrossRef] [PubMed]
- Smyth, L.J.; Eustace, A.; Kolsum, U.; Blaikely, J.; Singh, D. Increased airway T reg-ulatory cells in asthmatic subjects. Chest 2010, 138, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Ling, E.M.; Smith, T.; Nguyen, X.D.; Pridgeon, C.; Dallman, M.; Arbery, J.; Carr, V.A.; Robinson, D.S. Relation of, CD4+CD25+ regulatory T-cell suppression of allergen-driven T-cell activation to atopic status and expression of allergic disease. Lancet 2004, 363, 608–615. [Google Scholar] [CrossRef]
- Nguyen, K.D.; Vanichsarn, C.; Fohner, A.; Nadeau, K.C. Selective deregulation in chemokine signaling pathways of, CD4+CD25(hi)C.D.127(lo)/(-) regulatory T cells in human allergic asthma. J. Allergy Clin. Immunol. 2009, 123, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Akdis, C.A.; Akdis, M. Mechanisms and treatment of allergic disease in the big picture of regulatory T cells. J. Allergy Clin. Immunol. 2009, 123, 735–746. [Google Scholar] [CrossRef] [PubMed]
- Kearley, J.; Barker, J.E.; Robinson, D.S.; Lloyd, C.M. Resolution of airway inflam-mation and hyperreactivity after in vivo transfer of, CD4+CD25+ regulatory T cells is interleukin 10 dependent. J. Exp. Med. 2005, 202, 1539–1547. [Google Scholar] [CrossRef]
- Xu, W.; Lan, Q.; Chen, M.; Chen, H.; Zhu, N.; Zhou, X.; Wang, J.; Fan, H.; Yan, C.-S.; Kuang, J.-L.; et al. Adoptive transfer of induced-Treg cells effectively attenuates murine airway allergic inflammation. PLoS ONE 2012, 7, e40314. [Google Scholar] [CrossRef] [PubMed]
- Kearley, J.; Robinson, D.S.; Lloyd, C.M. CD4+CD25+ regulatory T cells reverse established allergic airway inflammation and prevent airway remodeling. J. Allergy Clin. Immunol. 2008, 122, 617–624. [Google Scholar] [CrossRef]
- Bobolea, I.; Barranco, P.; Del Pozo, V.; Romero, D.; Sanz, V.; Lopez-Carrasco, V.; Canabal, J.; Villasante, C.; Quirce, S. Sputum periostin in patients with different severe asthma phenotypes. Allergy 2015, 70, 540–546. [Google Scholar] [CrossRef]
- Wu, W.; Bleecker, E.; Moore, W.; Busse, W.W.; Castro, M.; Chung, K.F.; Calhoun, W.J.; Erzurum, S.; Gaston, B.; Israel, E.; et al. Unsupervised phenotyping of Severe Asthma Research Program participants using expanded lung data. J. Allergy Clin. Immunol. 2014, 133, 1280–1288. [Google Scholar] [CrossRef] [Green Version]
- Moore, W.C.; Hastie, A.T.; Li, X.; Li, H.; Busse, W.W.; Jarjour, N.N.; Wenzel, S.E.; Peters, S.P.; Meyers, D.A.; Bleecker, E.R.; et al. Sputum neutrophil counts are associated with more severe asthma phenotypes using cluster analysis. J. Allergy Clin. Immunol. 2014, 133, 1557–1563. [Google Scholar] [CrossRef]
- Shaw, D.E.; Berry, M.A.; Hargadon, B.; McKenna, S.; Shelley, M.J.; Green, R.H.; Brightling, C.E.; Wardlaw, A.J.; Pavord, I.D. Association between neutrophilic airway inflammation and airflow limitation in adults with asthma. Chest 2007, 6, 1871–1875. [Google Scholar] [CrossRef] [PubMed]
- Douwes, J.; Gibson, P.; Pekkanen, J.; Pearce, N. Non-eosinophilic asthma: Importance and possible mechanisms. Thorax 2002, 57, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Berry, M.; Morgan, A.; Shaw, D.E.; Parker, D.; Green, R.; Brightling, C.; Bradding, P.; Wardlaw, A.J.; Pavord, I.D. Pathological features and inhaled corticosteroid response of eosinophilic and non-eosinophilic sthma. Thorax 2007, 62, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Bullens, D.M.; Truyen, E.; Coteur, L.; Dilissen, E.; Hellings, P.W.; Dupont, L.J.; Ceuppens, J.L. IL-17 mRNA in sputum of asthmatic patients: Linking T cell driven inflammation and granulo cytic influx? Respir. Res. 2006, 7, 135. [Google Scholar] [CrossRef] [PubMed]
- Manni, M.L.; Trudeau, J.B.; Scheller, E.V.; Mandalapu, S.; Elloso, M.M.; Kolls, J.K.; Wenzel, S.E.; Alcorn, J.F. The complex relationship between inflammation and lung function in severe asthma. Mucosal Immunol. 2014, 7, 1186–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besnard, A.G.; Togbe, D.; Couillin, I.; Tan, Z.; Zheng, S.G.; Erard, F.; Le Bert, M.; Quesniaux, V.; Ryffel, B. Inflammasome-IL-1-Th17 response in allergic lung inflammation. J. Mol. Cell Biol. 2012, 4, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Krishnaswamy, J.K.; Chu, T.; Eisenbarth, S.C. Beyond pattern recognition:NOD-like receptors in dendritic cells. Trends Immunol. 2013, 34, 224–233. [Google Scholar] [CrossRef]
- Bruijnzeel, P.L.; Uddin, M.; Koenderman, L. Targeting neutrophilic inflammation in severe neutrophilic asthma: Can we target the disease-relevant neutrophil phenotype? J. Leukoc. Biol. 2015, 4, 549–556. [Google Scholar] [CrossRef]
- Simpson, J.L.; Grissell, T.V.; Douwes, J.; Scott, R.J.; Boyle, M.J.; Gibson, P.G. Innate immune activation in neutrophilic asthma and bronchiectasis. Thorax 2007, 3, 211–218. [Google Scholar] [CrossRef]
- Petsky, H.L.; Cates, C.J.; Lasserson, T.J.; Li, A.M.; Turner, C.; Kynaston, J.A.; Chang, A.B. A systematic review and meta-analysis: Tailoring asthma treatment on eosinophilic markers (exhaled nitric oxide or sputum eosinophils). Thorax 2012, 67, 199–208. [Google Scholar] [CrossRef]
- Gaillard, E.A.; McNamara, P.S.; Murray, C.S.; Pavord, I.D.; Shields, M.D. Blood eosinophils as a marker of likely corticosteroid response in children with preschool wheeze: Time for an eosinophil guided clinical trial? Clin. Exp. Allergy 2015, 45, 1384–1395. [Google Scholar] [CrossRef] [PubMed]
- Bleecker, E.R.; FitzGerald, J.M.; Chanez, P.; Papi, A.; Weinstein, S.F.; Barker, P.; Sproule, S.; Gilmartin, G.; Aurivillius, M.; Werkstrom, V.; et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting beta2-agonists (SIROCCO): A randomised, multicentre, placebo-controlled phase 3 trial. Lancet 2016, 388, 2115–2127. [Google Scholar] [CrossRef]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; FitzGerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N. Engl. J. Med. 2014, 371, 1198–1207. [Google Scholar] [CrossRef] [PubMed]
- Ortega, H.G.; Yancey, S.W.; Mayer, B.; Gunsoy, N.B.; Keene, O.N.; Bleecker, E.R.; Brightling, C.E.; Pavord, I.D. Severe eosinophilic asthma treated with mepolizumab stratified by baseline eosinophil thresholds: A secondary analysis of the DREAM and MENSA studies. Lancet Respir. Med. 2016, 4, 549–556. [Google Scholar] [CrossRef]
- Katz, L.E.; Gleich, G.J.; Hartley, B.F.; Yancey, S.W.; Ortega, H.G. Blood eosinophil count is a useful biomarker to identify patients with severe eosinophilic asthma. Ann. Am. Thorac. Soc. 2014, 11, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Price, D.B.; Rigazio, A.; Campbell, J.D.; Bleecker, E.R.; Corrigan, C.J.; Thomas, M.; Wenzel, S.E.; Wilson, A.M.; Small, M.B.; Gopalan, G.; et al. Blood eosinophil count and prospective annual asthma disease burden: A UK cohort study. Lancet Respir. Med. 2015, 3, 849–858. [Google Scholar] [CrossRef]
- Zeiger, R.S.; Schatz, M.; Dalal, A.A.; Chen, W.; Sadikova, E.; Suruki, R.Y.; Kawatkar, A.A.; Qian, L. Blood eosinophil count and outcomes in severe uncontrolled asthma: A prospective study. J. Allergy Clin. Immunol. Pract. 2017, 5, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, P.G.; Modrek, B.; Choy, D.F.; Jia, G.; Abbas, A.R.; Ellwanger, A.; Koth, L.L.; Arron, J.R.; Fahy, J.V. T-helper type 2-driven inflammation defines major subphenotypes of asthma. Am. J. Respir. Crit. Care Med. 2009, 180, 388–395. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, J.M.; Bleecker, E.R.; Nair, P.; Korn, S.; Ohta, K.; Lommatzsch, M.; Ferguson, G.T.; Busse, W.W.; Barker, P.; Sproule, S.; et al. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2016, 388, 2128–2141. [Google Scholar] [CrossRef]
- Hanania, N.A.; Wenzel, S.; Rosen, K.; Hsieh, H.J.; Mosesova, S.; Choy, D.F.; Lal, P.; Arron, J.R.; Harris, J.M.; Busse, W. Exploring the effects of omalizumab in allergic asthma: An analysis of biomarkers in the EXTRA study. Am. J. Respir. Crit. Care Med. 2013, 187, 804–811. [Google Scholar] [CrossRef]
- Bjermer, L.; Alving, K.; Diamant, Z.; Magnussen, H.; Pavord, I.; Piacentini, G.; Price, D.; Roche, N.; Sastre, J.; Thomas, M.; et al. Current evidence and future research needs for FeNO measurement in respiratory diseases. Respir. Med. 2014, 108, 830–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dweik, R.A.; Sorkness, R.L.; Wenzel, S.; Hammel, J.; Curran-Everett, D.; Comhair, S.A.; Bleecker, E.; Busse, W.; Calhoun, W.J.; Castro, M.; et al. National Heart, Lung, and Blood Institute Severe Asthma Research Program. Use of exhaled nitric oxide measurement to identify a reactive, at-risk phenotype among patients with asthma. Am. J. Respir. Crit. Care Med. 2010, 181, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Gemicioglu, B.; Musellim, B.; Dogan, I.; Guven, K. Fractional exhaled nitric oxide (FeNo) in different asthma phenotypes. Allergy Rhinol. 2014, 5, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Sippel, J.M.; Holden, W.E.; Tilles, S.A.; O’Hollaren, M.; Cook, J.; Thukkani, N.; Priest, J.; Nelson, B.; Osborne, M.L. Exhaled nitric oxide levels correlate with measures of disease control in asthma. J. Allergy Clin. Immunol. 2000, 106, 645–650. [Google Scholar] [CrossRef] [PubMed]
- van Veen, I.H.; Ten Brinke, A.; Sterk, P.J.; Sont, J.K.; Gauw, S.A.; Rabe, K.F.; Bel, E.H. Exhaled nitric oxide predicts lung function decline in difficult-to-treat asthma. Eur. Respir. J. 2008, 32, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, S.L.; Kittelson, J.; Cowan, J.O.; Flannery, E.M.; Hancox, R.J.; McLachlan, C.R.; Taylor, D.R. The predictive value of exhaled nitric oxide measurements in assessing changes in asthma control. Am. J. Respir. Crit. Care Med. 2001, 164, 738–743. [Google Scholar] [CrossRef] [PubMed]
- Van Vliet, D.; Alonso, A.; Rijkers, G.; Heynens, J.; Rosias, P.; Muris, J.; Jobsis, Q.; Dompeling, E. Prediction of asthma exacerbations in children by innovative exhaled inflammatory markers: Results of a longitudinal study. PLoS ONE 2015, 10, e0119434. [Google Scholar] [CrossRef] [PubMed]
- Van der Valk, R.J.; Baraldi, E.; Stern, G.; Frey, U.; de Jongste, J.C. Daily exhaled nitric oxide measurements and asthma exacerbations in children. Allergy 2012, 67, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Robroeks, C.M.; van Vliet, D.; Jobsis, Q.; Braekers, R.; Rijkers, G.T.; Wodzig, W.K.; Bast, A.; Zimmermann, L.; Dompeling, E. Prediction of asthma exacerbations in children: Results of a one-year prospective study. Clin. Exp. Allergy 2012, 42, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Song, J.S.; You, J.S.; Jeong, S.I.; Yang, S.; Hwang, I.T.; Im, Y.G.; Baek, H.S.; Kim, H.Y.; Suh, D.I.; Lee, H.B.; et al. Serum periostin levels correlate with airway hyper-responsiveness to methacholine and mannitol in children with asthma. Allergy 2015, 70, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Wedes, S.H.; Wu, W.; Comhair, S.A.; McDowell, K.M.; DiDonato, J.A.; Erzurum, S.C.; Hazen, S.L. Urinary bromotyrosine measures asthma control and predicts asthma exacerbations in children. J. Pediatr. 2011, 159, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Suzuki, M.; Konno, S.; Nishimura, M.; Bobolea, I.; Barranco, P.; Del Pozo, V.; Romero, D.; Sanz, V.; López-Carrasco, V.; et al. Sputum periostin in patients with different severe asthma phenotypes. Allergy 2015, 70, 884–885. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, M.; Ohtawa, J.; Akitsu, K. Association of airway wall thickness with serum periostin in steroid-naive asthma. Allergy Asthma Proc. 2016, 37, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Sabiner, U.; Birben, E.; Erzurum, S. Oxidative Stress in Asthma: Part of the puzzle. Pediatr. Allergy Immunol. 2018, 29, 789–800. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Roisin, R. Acute severe asthma: Pathophysiology and pathobiology of gas exchange abnormalities. Eur. Respir. J. 1997, 10, 1359–1371. [Google Scholar] [CrossRef] [PubMed]
- Brochard, L. Intrinsic (or auto-) PEEP. during controlled mechanical ventilation. Intensive Care Med. 2012, 28, 1376–1378. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.Y.; Sutter, M.E.; Albertson, T.E. The patient with asthma in the emergency department. Clin. Rev. Allergy Immunol. 2012, 43, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Pepe, P.E.; Marini, J.J. Occult Positive End-Expiratory Pressure in Mechanically Ventilated, PA tients with Airflow Obstruction. Am. Rev. Respir. Dis. 1982, 126, 166–170. [Google Scholar] [PubMed]
- Brenner, B.; Corbridge, T.; Kazzi, A. Intubation and mechanical ventilation of the asthmatic patient in respiratory failure. J. Emerg. Med. 2009, 37, S23–S34. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, G.G.; Schulzer, M.; Jung, D.; Fitzgerald, J. A systematic review of risk factors associated with near-fatal and fatal asthma. Can. Respir. J. 2005, 12, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Suissa, S.; Blais, L.; Ernst, P. Patterns of increasing beta-agonist use and the risk of fatal or near-fatal asthma. Eur. Respir. J. 1994, 7, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, J.M.; Tavakoli, H.; Lynd, L.D.; Al Efraij, K.; Sadatsafavi, M. The impact of inappropriate use of short acting beta agonists in asthma. Respir. Med. 2017, 131, 135–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodder, R.; Lougheed, M.D.; Rowe, B.H.; FitzGerald, J.M.; Kaplan, A.G.; McIvor, R.A. Management of acute asthma in adults in the emergency department: Nonventilatory management. CMAJ 2010, 182, E55–E67. [Google Scholar] [CrossRef] [PubMed]
- Fergeson, J.E.; Patel, S.S.; Lockey, R.F. Acute asthma, prognosis, and treatment. J. Allergy Clin. Immunol. 2017, 139, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Lockey, R.F.; Ledford, D.K. Asthma: Comorbidities, Coexisting Conditions, and Differential Diagnosis; Oxford University Press: Oxford, UK, 2014; pp. 231–367. [Google Scholar]
- Fretzayas, A.; Moustaki, M.; Loukou, I.; Douros, K. Differentiating vocal cord dysfunction from asthma. J. Asthma Allergy 2017, 10, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Keeley, D.; Osman, L. Dysfunctional breathing and asthma. It is important to tell the difference. BMJ 2001, 322, 1075–1076. [Google Scholar] [CrossRef]
- Carruthers, D.M.; Harrison, B.D. Arterial blood gas analysis or oxygen saturation in the assessment of acute asthma? Thorax 1995, 50, 186–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasileiadis, I.; Alevrakis, E.; Ampelioti, S.; Vagionas, D.; Rovina, N.; Koutsoukou, A. Acid-Base Disturbances in Patients with Asthma: A Literature Review and Comments on Their Pathophysiology. J. Clin. Med. 2019, 8, 563. [Google Scholar] [CrossRef]
- Cates, C.; Welsh, E.; Rowe, B. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma (Review). Cochrane Database Syst. Rev. 2013, 13, CD000052. [Google Scholar]
- Rodrigo, G.J.; Rodrigo, C. Continuous vs intermittent beta-agonists in the treatment of acute adult asthma: A systematic review with meta-analysis. Chest 2002, 122, 160–165. [Google Scholar] [CrossRef]
- Camargo, C.J.; Spooner, C.; Rowe, B. Continuous versus intermittent beta-agonists for acute asthma (Review). Cochrane Database Syst. Rev. 2003, 4, CD001115. [Google Scholar]
- Wilkinson, M.; Bulloch, B.; Garcia-Filion, P.; Keahey, L. Efficacy of racemic albuterol versus levalbuterol used as a continuous nebulization for the treatment of acute asthma exacerbations: A randomized, double-blind, clinical trial. J. Asthma 2011, 48, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Nowak, R.; Emerman, C.; Hanrahan, J.P.; Parsey, M.V.; Hanania, N.A.; Claus, R.; Schaefer, K.; Baumgartner, R.A.; XOPENEX Acute Severe Asthma Study Group. A comparison of levalbuterol with racemic albuterol in the treatment of acute severe asthma exacerbations in adults. Am. J. Emerg. Med. 2006, 24, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Tobin, A. Intravenous salbutamol: Too Much of a Good Thing? Crit. Care Resusc. 2005, 7, 119–127. [Google Scholar] [PubMed]
- Travers, A.H.; Milan, S.J.; Jones, A.P.; Camargo, C.A., Jr.; Rowe, B.H. Addition of intravenous β2 -agonists to inhaled β2 -agonists for acute asthma. Cochrane Database Syst. Rev. 2012, 12, CD010179. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.H.; Scott, S.J. Continuous infusions of terbutaline in asthma—A review. J. Asthma 2011, 48, 753–756. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, G.J.; Nannini, L.J. Comparison between nebulized adrenaline and β2 agonists for the treatment of acute asthma. A meta-analysis of randomized trials. Am. J. Emerg. Med. 2006, 24, 217–222. [Google Scholar] [CrossRef]
- Gosens, R.; Gross, N. The mode of action of anticholinergics in asthma. Eur. Respir. J. 2018, 52, 1701247. [Google Scholar] [CrossRef]
- Vogelberg, C. Anticholinergics in asthma: Are we utilizing asthma therapies effectively? Ther Clin Risk Manag. 2019, 15, 405–408. [Google Scholar] [CrossRef]
- Edmonds, M.; Milan, S.; Camargo, C.A., Jr.; Pollack, C.V.; Rowe, B.H. Early use of inhaled corticosteroids in the emergency department treatment of acute asthma (Review). Cochrane Database Syst. Rev. 2012, 12, CD002308. [Google Scholar]
- Rowe, B.H.; Vethanayagam, D. The role of inhaled corticosteroids in the management of acute asthma. Eur. Respir. J. 2007, 30, 1035–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, S.; Kuan, W.S.; Kelly, A.M.; Van Meer, O.; Motiejunaite, J.; Keijzers, G.; Jones, P.; Body, R.; Karamercan, M.A.; Klim, S.; et al. Treatment and outcome of adult patients with acute asthma in emergency departments in Australasia, South East Asia and Europe: Are guidelines followed? AANZDEM/EuroDEM study. Emerg. Med. Australas. 2019. (Epub ahead of print). [Google Scholar] [CrossRef] [PubMed]
- Rowe, B.H.; Edmonds, M.L.; Spooner, C.H.; Diner, B.; Camargo, C.A. Corticosteroid therapy for acute asthma. Respir. Med. 2004, 98, 275–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulco, P.P.; Lone, A.A.; Pugh, C.B. Intravenous versus oral corticosteroids for treatment of acute asthma exacerbations. Ann. Pharmacother. 2002, 36, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, S.; Campbell, S.; Villa-Roel, C.; Rowe, B. Intramuscular versus oral corticosteroids to reduce relapses following discharge from the emergency department for acute asthma (Review). Cochrane Database Syst. Rev. 2018, 2018, CD012629. [Google Scholar]
- Normansell, R.; Kew, K.; Mansour, G. Different oral corticosteroid regimens for acute asthma (Review). Cochrane Database Syst. Rev. 2016, 5, CD011801. [Google Scholar]
- Rowe, B.; Bretzlaff, J.; Bourdon, C.; Bota, G.; Blitz, S.; Camargo, C.A., Jr. Magnesium sulfate for treating exacerbations of acute asthma in the emergency department. Cochrane Database Syst. Rev. 2000, 2, CD001490. [Google Scholar]
- Kew, K.; Kirtchuk, L.; Michell, C. Intravenous magnesium sulfate for treating adults with acute asthma in the emergency department (Review). Cochrane Database Syst. Rev. 2014, 5, CD010909. [Google Scholar] [CrossRef]
- Green, R.H. Asthma in adults (acute): Magnesium sulfate treatment. BMJ Clin. Evid. 2016, 1, 1513. [Google Scholar]
- Knightly, R.; Milan, S.; Hughes, R.; Knopp-sihota, J.; Rowe, B.; Normansell, R.; Powell, C. Inhaled magnesium sulfate in the treatment of acute asthma (Review). Cochrane Database Syst. Rev. 2017, 11, CD003898. [Google Scholar]
- Javor, E.; Grle, S.P. Limitations of the results from randomized clinical trials involving intravenous and nebulised magnesium sulphate in adulta with severe acute asthma. Pulm. Pharmacol. Ther. 2019, 55, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, S.; Cohen, J.; Bradburn, M.; Stevens, J.; Gray, A.; Benger, J.; Coats, T.; 3Mg Research Team. The 3Mg trial: A randomised controlled trial of intravenous or nebulised magnesium sulphate versus placebo in adults with acute severe asthma. Health Technol. Assess. 2014, 18, 1–168. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.; Milan, S.; Rowe, B. Addition of intravenous aminophylline to inhaled β2—Agonists in adults with acute asthma (Review). Cochrane Database Syst. Rev. 2012, 12, CD002742. [Google Scholar] [PubMed]
- Mahemuti, G.; Zhang, H.; Li, J. Efficacy and side effects of intravenous theophylline in acute asthma: A systematic review and meta-analysis. Drug Des. Dev. Ther. 2018, 12, 99–120. [Google Scholar] [CrossRef] [PubMed]
- Silverman, R.A.; Chen, Y.; Bonuccelli, C.M.; Simonson, S.G. Zafirlukast improves emergency department outcomes after an acute asthma episode. Ann. Emerg. Med. 1999, 34, S1. [Google Scholar] [CrossRef]
- Camargo, C.A.J.; Smithline, H.A.; Malice, M.-P.; Green, S.A.; Reiss, T.F. A randomized controlled trial of intravenous montelukast in acute asthma. Am. J. Respir. Crit. Care Med. 2003, 167, 528–533. [Google Scholar] [CrossRef]
- Watts, K.; Chavasse, R. Leukotriene receptor antagonists in addition to usual care for acute asthma in adults and children (Review). Cochrane Database Syst. Rev. 2012, 5, CD006100. [Google Scholar]
- Perrin, K.; Wijesinghe, M.; Healy, B.; Wadsworth, K.; Bowditch, R.; Bibby, S.; Baker, T.; Weatherall, M.; Beasley, R. Randomised controlled trial of high concentration versus titrated oxygen therapy in severe exacerbations of asthma. Thorax 2011, 66, 937–941. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, G.J.; Verde, M.R.; Peregalli, V. Effects of Short-term 28% and 100% Oxygen on Pa, CO2 and Peak Expiratory Flow Rate in Acute Asthma—A randomized trial. Chest 2003, 124, 1312–1317. [Google Scholar] [CrossRef]
- Inwald, D.; Roland, M.; Kuitert, L.; Mckenzie, S.A.; Petros, A.; Inwald, D. Oxygen treatment for acute severe asthma. BMJ 2001, 323, 98–100. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, G.J.; Castro-Rodriguez, J.A. Heliox-driven β2 -agonists nebulization for children and adults with acute asthma: A systematic review with meta-analysis. Ann. Allergy Asthma Immunol. 2014, 112, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, G.J.; Rodrigo, C.; Pollack, C.V.; Rowe, B.; Em, C. Use of Helium-Oxygen Mixtures in the Treatment of Acute Asthma a Systematic Review. Chest 2003, 123, 891–896. [Google Scholar] [CrossRef] [PubMed]
- El-Khatib, M.; Jamaleddine, G.; Kanj, N. Effect of Heliox- and Air-Driven Nebulized Bronchodilator Therapy on Lung Function in Patients with Asthma. Lung 2014, 192, 377–383. [Google Scholar] [CrossRef] [PubMed]
- L’Hommedieu, C.S.; Arens, J.J. The use of ketamine for the emergency intubation of patients with status asthmaticus. Ann. Emerg. Med. 1987, 16, 568–571. [Google Scholar] [CrossRef]
- Goyal, S.; Agrawal, A. Ketamine in status asthmaticus: A review. Indian J. Crit. Care Med. 2013, 17, 154–161. [Google Scholar] [PubMed]
- Esmailian, M.; Esfahani, M.K.; Heydari, F. The Effect of Low-Dose Ketamine in Treating Acute Asthma Attack; A Randomized Clinical Trial. Emergency 2018, 6, e21. [Google Scholar] [PubMed]
- Stefan, M.S.; Shieh, M.S.; Spitzer, K.A.; Pekow, P.S.; Krishnan, J.A.; Au, D.H.; Lindenauer, P.K. Association of Antibiotic Treatment with Outcomes in Patients Hospitalized for an Asthma Exacerbation Treated with Systemic Corticosteroids. JAMA Intern. Med. 2019, 179, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Lindenauer, P.K.; Stefan, M.S.; Feemster, L.C. Use of antibiotics among patients hospitalized for exacerbations of asthma. JAMA Intern. Med. 2016, 176, 1397–1400. [Google Scholar] [CrossRef] [PubMed]
- Stefan, M.S.; Nathanson, B.H.; Lagu, T.; Priya, A.; Pekow, P.S.; Steingrub, J.S.; Hill, N.S.; Goldberg, R.J.; Kent, D.M.; Lindenauer, P.K. Outcomes of Noninvasive and Invasive Veltilation in Patients Hospitalized with Asthma Exacerbation. Ann. Am. Thorac. Soc. 2016, 13, 1096–1104. [Google Scholar] [CrossRef]
- Pallin, M.; Naughton, M.T. Noninvasive ventilation in acute asthma. J. Crit. Care 2014, 29, 586–593. [Google Scholar] [CrossRef]
- Burns, K.E.A.; Meade, M.O.; Premji, A. Noninvasive ventilation as a weaning strategy for mechanical ventilation in adults with respiratory failure: A Cochrane systematic review. CMAJ 2014, 186, E112–E122. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.S.C.; Wu, K.C.; Wong, T.K.M.; Tsai, Y.H.; Cheng, R.K.S.; Bishop, M.J.; Tan, P.P. Effects of fenoterol and ipratropium on respiratory resistance of asthmatics after tracheal intubation. Br. J. Anaesth. 2000, 84, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Davidson, C.; Banham, S.; Elliott, M. BTS/ICS Guideline for the Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults. Thorax 2016, 71, ii1–ii35. [Google Scholar] [CrossRef] [PubMed]
- Davidson, C.; Banham, S.; Elliott, M.; Kennedy, D.; Gelder, C.; Glossop, A.; Church, A.C.; Creagh-Brown, B.; Dodd, J.W.; Felton, T.; et al. Guideline for the ventilatory management of acute hypercapnic respiratory failure in adults. BMJ Open Respir Res. 2016, 14, e000133. [Google Scholar]
- Davis, D.P.; Hwang, J.Q.; Dunford, J.V. Rate of decline in oxygen saturation at various pulse oximetry values with prehospital rapid sequence intubation. Prehosp. Emerg. Care 2008, 12, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Eames, W.; Rooke, G.; Wu, R.; Bishop, M. Comparison of the effects of Etomidate, Propofol, and Thiopental on respiratory resistance asther tracheal intubation. Anesthesiology 1996, 84, 1307–1311. [Google Scholar] [CrossRef] [PubMed]
- Laher, A.; Buchanan, S. Mechanically Ventilating the Severe Asthmatic Mechanically Ventilating the Severe Asthmatic. J. Intensive Care Med. 2018, 33, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Laghi, F.; Goyal, A. Auto-PEEP in respiratory failure. Minerva Anestesiol. 2012, 78, 201–221. [Google Scholar] [PubMed]
- Williams, T.J.; Tuxen, D.; Scheinkestel, C.D.; Czarny, D.; Bowes, G. Risk Factors for Morbidity in Mechanically Ventilated Patients with Acute Severe Asthma 1, 2. Am. Rev. Respir. Dis. 1992, 146, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Leatherman, J. Mechanical ventilation for severe asthma. Chest 2015, 147, 1671–1680. [Google Scholar] [CrossRef]
- Kollef, M.H. Lung hyperinflation caused by inappropriate ventilation resulting in electromechanical dissociation: A case report. Heart Lung 1992, 21, 74–77. [Google Scholar]
- Riker, R.R.; Shehabi, Y.; Bokesch, P.M.; Ceraso, D.; Wisemandle, W.; Whitten, P.; Margolis, B.D.; Byrne, D.W.; Ely, E.W.; Rocha, M.G.; et al. Dexmedetomidine vs Midazolam for Sedation of Critically Ill Patients. JAMA 2009, 301, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Burburan, S.M.; Xisto, D.G.; Rocco, P.R.M. Anaesthetic management in asthma. Minerva Anestesiol. 2007, 73, 357–365. [Google Scholar] [PubMed]
- Behbehani, N.A.; Al-Mane, F.; D’yachkova, Y.; Pare, P.; FitzGerald, J.M. Myopathy following mechanical ventilation for acute severe asthma: The role of muscle relaxants and corticosteroids. Chest 1999, 115, 1627–1631. [Google Scholar] [CrossRef] [PubMed]
- Tuxen, D.; Lane, S. The Effects of Ventilatory Pattern on Hyperinflation, Airway Pressures, and Circulation in Mechanical Ventilation of Patients with Severe Air-Flow. Am. Rev. Respir. Dis. 1987, 136, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Tuxen, D.V. Detrimental Effects of Positive End-expiratory Pressure during Controlled Mechanical Ventilation of Patients with Severe Airflow Obstruction. Am. Rev. 1989, 140, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Caramez, M.; Borges, J.; Tucci, M.; Okamoto, V. Paradoxical responses to positive end-expiratory pressure in patients with airway obstruction during controlled ventilation. Crit. Care Med. 2005, 33, 1519–1528. [Google Scholar] [CrossRef] [PubMed]
- Stather, D.R.; Stewart, T.E. Clinical review: Mechanical ventilation in severe asthma. Crit. Care 2005, 9, 581–587. [Google Scholar] [CrossRef] [Green Version]
- Baudin, F.; Buisson, A.; Vanel, B.; Massenavette, B.; Pouyau, R.; Javouhey, E. Nasal high flow in management of children with status asthmaticus: A retrospective observational study. Ann. Intensive Care 2017, 7, 55. [Google Scholar] [CrossRef]
- Pilar, J.; Modesto, I.; Alapont, V.; Lopez-Fernandez, Y.M.; Lopez-Macias, O.; Garcia-Urabayen, D.; Amores-Hernandez, I. High-flow nasal cannula therapy versus non-invasive ventilation in children with severe acute asthma exacerbation: An observational cohort study. Med. Intensiva 2017, 41, 418–424. [Google Scholar] [CrossRef]
- Chang, C.L.; Yates, D.H. Use of Early Extra-Corporeal Membrane Oxygenation (E.C.M.O.) for Severe Refractory Status Asthmaticus. J. Med. Cases 2011, 2, 124–126. [Google Scholar]
- Alzeer, A.H.; Otair, H.A.A.; Khurshid, S.M.; Badrawy, S.E.; Bakir, B.M. Case Report A case of near fatal asthma: The role of ECMO as rescue therapy. Ann. Thorac. Med. 2015, 10, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, M.E.; Woo, Y.J.; Sager, J.S.; Fuchs, B.D.; Christie, J.D. Outcomes using extracorporeal life support for adult respiratory failure due to status asthmaticus. ASAIO J. 2009, 55, 47. [Google Scholar] [CrossRef] [PubMed]
- Yeo, H.J.; Kim, D.; Jeon, D.; Kim, Y.S.; Rycus, P.; Cho, W.H. Extracorporeal membrane oxygenation for life-threatening asthma refractory to mechanical ventilation: Analysis of the Extracorporeal Life Support Organization registry. Crit. Care 2017, 21, 297. [Google Scholar] [CrossRef] [PubMed]
- Di Lascio, G.; Prifti, E.; Messai, E.; Peris, A.; Harmelin, G.; Xhaxho, R.; Fico, A.; Sani, G.; Bonacchi, M. Extracorporeal membrane oxygenation support for life-threatening acute severe status asthmaticus. Perfusion 2017, 32, 157. [Google Scholar] [CrossRef] [PubMed]
- Lobaz, S.; Carey, M. Case reports Rescue of acute refractory hypercapnia and acidosis secondary to life-threatening asthma with extracorporeal carbon dioxide removal (ECCO2R) Case report. J. Intensive Care Soc. 2011, 12, 140–142. [Google Scholar] [CrossRef]
- Brenner, K.; Abrams, D.C.; Agerstrand, C.L.; Brodie, D. Extracorporeal carbon dioxide removal for refractory status asthmaticus: Experience in distinct exacerbation phenotypes. Perfusion 2014, 29, 26–28. [Google Scholar] [CrossRef]
- Schneider, T.; Bence, T.; Brettner, F. “Awake” ECCO2R superseded intubation in a near-fatal asthma attack. J. Intensive Care 2017, 5, 53. [Google Scholar] [CrossRef]
- Tobias, J.D. Inhalational Anesthesia: Basic Pharmacology, End Organ Effects, and Applications in the Treatment of Status Asthmaticus. J. Intensive Care Med. 2009, 24, 361–371. [Google Scholar] [CrossRef]
- Vaschetto, R.; Bellotti, E.; Turucz, E.; Gregoretti, C.; Corte, F.D.; Navalesi, P. Inhalational Anesthetics in Acute Severe Asthma. Curr. Drug Targets 2009, 10, 826–832. [Google Scholar] [CrossRef]
- Rosseel, P.; Lauwers, L.F.; Baute, L.; Care, I.; Stuivenberg, A.Z. Halothane treatment in life-threatening asthma. Intensive Care Med. 1985, 11, 241–246. [Google Scholar] [CrossRef]
- Bierman, M.; Brown, M.; Muren, O. Prolonged isoflurane anesthesia in status asthmaticus. Crit. Care Med. 1986, 14, 832–833. [Google Scholar] [CrossRef] [PubMed]
- Schutte, D.; Zwitserloot, A.M.; Houmes, R.; Hoog, M.D.; Draaisma, J.M.; Lemson, J. Sevoflurane therapy for life-threatening asthma in children. Br. J. Anaesth. 2013, 111, 967–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, E.; Fahimi, J.; Hern, H. Sevoflurane administration initiated out of the, ED for life-threatening status asthmaticus. Am. J. Emerg. Med. 2015, 33, e3–e6. [Google Scholar] [CrossRef] [PubMed]
- Ruszkai, Z.; Bokretas, G.; Bartha, P. Sevoflurane therapy for life-threatening acute severe asthma: A case report. Can. J. Anesth. 2014, 61, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Beute, J. Emergency treatment of status asthmaticus with enoximone. Br. J. Anaesth. 2014, 112, 1105–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanchal, R.; Kumar, G.; Majumdar, T.; Taneja, A.; Patel, J.; Dagar, G.; Jacobs, E.R.; Whittle, J. Utilization of mechanical ventilation for asthma exacerbations: Analysis of a national database. Respir. Care 2014, 59, 644–653. [Google Scholar] [CrossRef]
- Marquette, C.H.; Saulnier, F.; Leroy, O.; Wallaert, B.; Chopin, C.; Demarcq, J.M.; Durocher, A.; Tonnel, A.B. Long-term prognosis of near-fatal asthma. A 6-year follow-up study of 145 asthmatic patients who underwent mechanical ventilation for a near-fatal attack of asthma. Am. Rev. Respir. Dis. 1992, 146, 76–81. [Google Scholar] [CrossRef]
- Yellowlees, P.M.; Ruffin, R.E. Psychological defenses and coping styles in patients following a life-threatening attack of asthma. Chest 1989, 95, 1298–1303. [Google Scholar] [CrossRef]
- Lemmetyinen, R.E.; Karjalainen, J.V.; But, A.; Renkonen, R.L.O.; Pekkanen, J.R.; Toppila-Salmi, S.K.; Haukka, J.K. Higher mortality of adults with asthma: A 15-year follow-up of a population-based cohort. Allergy 2018, 73, 1479–1488. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A History of Near Fatal Asthma Requiring Intubation and Mechanical Ventilation |
|---|
| Hospitalization or emergency care visits for asthma in the past year |
| Currently using or having recently stopped using oral steroids |
| Not currently using inhaled steroids |
| SABA over-use (more than one canister of salbutamol/month (or equivalent)) |
| History of psychiatric disease or psychosocial problems |
| Female Sex |
| Age > 40 years |
| Smoking history |
| Poor perception of airflow limitation |
| Hyperinflation in chest radiograph |
| Poor adherence with asthma medications and/or poor adherence |
| (or lack of) with a written asthma action plan |
| Food allergy |
| Medication | Dosing | References |
|---|---|---|
| Salbutamol (albuterol) solution for nebulization: single dose 2.5 mg/2.5 mL | Continuous nebulization for an hour and re-assess clinical response | [214,215,216,217,218,219,220,221,223] |
| Ipratropium bromide | Nebulization of 0.5 mg/2.5 mL/4–6 h in combination with salbutamol (same nebulizer) | [61,62,63,224] |
| Corticosteroids | Methylprednisolone iv infusion of 40 mg or hydrocortisone iv, 200 mg or oral prednisone 40 mg | [65,225,226,227,228,229,230,231,232] |
| Magnesium sulfate | Single iv infusion of 2 gr/20 min | [233,234,235,236,237,238] |
| Methylxanthines | Not recommended as first line; poor response and potential serious adverse events | [239,240] |
| Leukotriene receptor antagonists | Single iv infusion of 7–14 mg over 5 min | [241,242,243] |
| Epinephrine (adrenaline) | 0.3–0.4 mL sc of a 1:1000 (1 mg/mL) solution/20 min for 3 doses in case of no response | [222] |
| Terbutaline (1 mg/mL) | 0.25 mg sc/20 min for 3 doses in case of no response (preferred in pregnancy) | [221,223] |
| Heliox | Helium/oxygen mixture in a 80:20 or 70:30 ratio | [247,248,249] |
| Medication | Dosing | Side Effects | References |
|---|---|---|---|
| Midazolam | 0.03–0.1 mg/kg bolus iv infusion, followed by an infusion of 3–10 mg/h | Hypotension | [268,269] |
| Propofol | Infusion of 60–80 mg/min initially, up to 2 mg/kg. Continue with iv infusion of 5–10 mg/kg/h as needed, and for sedation on mechanical ventilation 1–4 mg/kg/h | Hypotension, seizures, hyperlipidemia | [262,268] |
| Fentanyl | 50–100 μg/kg bolus iv infusion, followed by infusion of 50–100 μg/h | Bradycardia, histamine release | [268,269] |
| Remifentanyl | Initial dose of 1 μg/kg iv infusion, followed by an infusion of 0.25–0.5 μg/kg/min (up to 2 μg/kg/min) | Bradycardia, hypotension | [268,269] |
| Ketamine | 1 mg/mL bolus iv infusion, followed by a maintenance infusion of 0.1–0.5 mg/min | Sympatheticomimetic effects, delirium | [250,251,252] |
| Dexmedetomidine | Initial loading dose of 1 μg/kg, iv over 10–30 min, followed by a maintenance infusion of 0.2–0.7 μg/kg/h | Hypotension, bradycardia | [68,269] |
| Cis-atracurium | 0.1–0.2 mg/kg bolus iv infusion, followed by infusion in a rate of 3 μg/kg/min (up to 10 μg/mL/min) | Bronchospasm | [269,270] |
| Mode | Settings |
|---|---|
| Tidal volume | 6 mL/kg ideal bodyweight |
| Respiratory rate | 8–10/min |
| Minute ventilation | <10 L/min |
| Inspiratory flow rate | 60–80 L/min |
| Inspiratory to expiratory ratio | >1:3 |
| Inspiratory wave form | Decelerated waveform |
| Expiratory time | 4–5 s |
| Plateau pressure | <30 cm H2O |
| PEEP | 0 cm H2O |
| FiO2 | 100% initially and titrate to maintain SaO2 > 90% |
| Risk Factor | Treatment Strategy | Evidence |
|---|---|---|
| Any patient with 1 risk factor for exacerbations (including poor symptom control) |
| A |
| A | |
| A | |
| A | |
| ≥1 severe exacerbation in last year |
| A |
| A | |
| C | |
| Exposure to tobacco smoke |
| A |
| B | |
| Low FEV1, especially if <60% predicted |
| B |
| D | |
| D | |
| Obesity |
| B |
| D | |
| Major psychological problems |
| D |
| D | |
| Major socioeconomic problems |
| D |
| Confirmed food allergy |
| A |
| Allergen exposure if sensitized |
| C |
| D | |
| B | |
| Allergen exposure if sensitized |
| A |
| Medication | Use | Adverse Effects |
|---|---|---|
| Anti-IgE (omalizumab, SC, ≥6 years) | An add-on option for patients with severe allergic asthma uncontrolled on high dose ICS-LABA. elf-administration may be permitted | Reactions at the site of injection are common but minor. Anaphylaxis is rare. |
| Anti-IL5/anti-IL5R (anti-IL5 mepolizumab (SC, ≥12 or ≥6 years), reslizumab (IV, ≥18 years) or anti-IL5 receptor benralizumab (SC, ≥12 years)) | Add-on options for patients with severe eosinophilic asthma uncontrolled on high dose ICS-LABA | Headache and reactions at injection site are common but minor. |
| Anti-IL4R (dupilumab, SC, ≥12 years) | An add-on option for patients with severe eosinophilic/Type 2 asthma uncontrolled on high dose ICS-LABA, or requiring maintenance OCS. It is also approved for treatment of moderate-severe atopic dermatitis. Self-administration may be permitted | Reactions at injection site are common but minor. Blood eosinophilia occurs in 4–13% of patients. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostakou, E.; Kaniaris, E.; Filiou, E.; Vasileiadis, I.; Katsaounou, P.; Tzortzaki, E.; Koulouris, N.; Koutsoukou, A.; Rovina, N. Acute Severe Asthma in Adolescent and Adult Patients: Current Perspectives on Assessment and Management. J. Clin. Med. 2019, 8, 1283. https://doi.org/10.3390/jcm8091283
Kostakou E, Kaniaris E, Filiou E, Vasileiadis I, Katsaounou P, Tzortzaki E, Koulouris N, Koutsoukou A, Rovina N. Acute Severe Asthma in Adolescent and Adult Patients: Current Perspectives on Assessment and Management. Journal of Clinical Medicine. 2019; 8(9):1283. https://doi.org/10.3390/jcm8091283
Chicago/Turabian StyleKostakou, Eirini, Evangelos Kaniaris, Effrosyni Filiou, Ioannis Vasileiadis, Paraskevi Katsaounou, Eleni Tzortzaki, Nikolaos Koulouris, Antonia Koutsoukou, and Nikoletta Rovina. 2019. "Acute Severe Asthma in Adolescent and Adult Patients: Current Perspectives on Assessment and Management" Journal of Clinical Medicine 8, no. 9: 1283. https://doi.org/10.3390/jcm8091283