1. Introduction
Calcineurin inhibitors (CNIs) are currently the standard immunosuppressive therapy after renal transplantation. Their introduction into clinical practice has improved short-term outcomes dramatically. Unfortunately, the rate of late allograft loss has not significantly improved [
1] and it is generally accepted that CNI nephrotoxicity contributes to this problem. Thus, multiple studies have investigated the impact of CNI-free immunosuppression on renal allograft function and patient and graft survival. The use of mammalian target of rapamycin inhibitors (mTORi) is impeded by drop-out rates of up to 40% due to side effects [
2] and furthermore is associated with higher allograft rejection rates [
3].
Belatacept inhibits T-cell activation by blocking a co-stimulatory signal by binding to CD80/CD86 on antigen presenting cells [
4]. It is currently approved for the de novo immunosuppression of renal allograft recipients in combination with mycophenolic acid and steroids. Studies have demonstrated an improved allograft survival over several years when compared to cyclosporine A-based immunosuppression [
5,
6]. Furthermore, a protocol for switching patients from CNIs to Belatacept has been published [
7,
8]. This conversion improved kidney function relative to the baseline and was safe concerning risk of death or transplant loss. Finally, it has been proposed that Belatacept-based regimens might have beneficial effects, especially in patients at high cardiovascular (CV) risk (reviewed by [
9]). One mechanism might be a reduction of pulse wave velocity in patients treated with Belatacept compared to CNI-treated patients [
10,
11]. However, “real world” data on renal outcomes and especially safety in the latter individuals are sparse.
Thus, we conducted a retrospective cohort study in renal allograft recipients at high CV risk and compared the efficacy and safety of Belatacept treatment in 34 patients to the outcomes of 150 patients treated with CNI (mainly tacrolimus) based immunosuppression.
2. Materials and Methods
2.1. Patient Population
Belatacept has been used in 42 renal transplant recipients at our center since 2010 and in this retrospective cohort study, all patients at high cardiovascular risk (definition see below) have been included (n = 34). Eighteen patients were treated de novo and 16 were converted at a median of 1.6 months (interquartile range (IQR), 0.6–4.2 months) after transplantation, mainly due to biopsy confirmed or clinically suspected renal CNI toxicity. No patient in this group was returned to CNI therapy thereafter. As we were interested in studying the efficacy and safety in patients on either CNI or Belatacept therapy, the day of conversion was taken as the baseline in these individuals and all clinical endpoints were adjudicated to the Belatacept group. Due to the early conversion, we excluded the time on CNI from any calculation. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Medical University Innsbruck (Project-ID: 1137/2019).
The median observation duration on Belatacept was 35 months, no patient was lost for follow-up and the total period on therapy analysed was 1194 months. All renal allograft recipients (n = 309) on CNI-based immunosuppression that received their transplant between 1 January, 2010 and 31 December, 2012 formed the control cohort. Of these, 150 also fulfilled the criteria for high cardiovascular risk. No patients were lost for follow-up, the median follow-up was 48 months and the total analysed period of months on therapy was 7309. High cardiovascular risk was defined by the presence of any significant pre-transplant coronary artery disease (CAD) confirmed on angiography, a history of myocardial infarction, peripheral artery disease (PAD) (cardiovascular disease) or stroke (cerebrovascular disease) or the presence of diabetes mellitus in combination with arterial hypertension.
2.2. Endpoints
Efficacy endpoints were renal allograft function as assessed by a change of eGFR on therapy, number of rejection episodes (either confirmed by biopsy or clinically based on an improvement of allograft function after anti-rejection therapy) or graft loss. The estimated glomerular filtration rate (eGFR) was calculated using the abbreviated MDRD formula. ΔeGFR was calculated by dividing the difference between eGFR at last follow-up and the baseline by the number of follow-up years. The safety endpoints were de novo cardiovascular events (new myocardial infarction, newly diagnosed CAD of any stage, newly diagnosed peripheral artery disease), severe infections (defined as infection leading to the admission of the patient to hospital), cytomegalo virus (CMV) reactivation (diagnosed by PCR with or without a clinical CMV infection), BKV reactivation (as determined by PCR in serum and/or urine), de novo malignancy and death. All efficacy and safety endpoints were identified using patients’ records.
2.3. Statistics
The reported values represent either medians and interquartile ranges (IQR) or the number of patients and percentages of the respective cohort. Proportions were compared using the Chi2 or Fisher exact tests. Non-parametric tests were used to compare continuous variables. The factors potentially associated with the eGFR, the eGFR-slope (eGFR), and efficacy and safety parameters were assessed using a Cox regression analysis. In particular, those factors were: Belatacept treatment, recipient age, male gender of the recipient, recipient BMI, a CMV high risk mismatch (D+/R-), the presence of diabetes mellitus or arterial hypertension, the presence of cerebrovascular or cardiovascular disease, the time on renal replacement therapy (RRT) before renal transplantation (RTx), number of previous RTx, number of HLA mismatches, intraoperative urine production (initial diuresis), number of post-operative (PO)—meaning after renal transplantation—hemodialysis sessions (HDs), the absence or presence of steroids at discharge, the presence of serum-creatinine at discharge, the absence or presence of steroids at the last follow-up, the extended criteria donor (ECD) organ, the male sex of the donor, and donor age. A history of rejection was also included, with an exception for the endpoint rejection episodes. Variables with a p-value < 0.05 in univariate analysis were included in the multivariate analysis, where again a p-value < 0.05 was considered statistically significant. The analysis was performed using SPSS Version 24.
4. Discussion
We conducted a retrospective cohort study of renal allograft recipients at high cardiovascular risk either treated with a Belatacept- or CNI-based immunosuppressive regimen. eGFR improved with Belatacept treatment, but slightly decreased during CNI therapy and, in the multivariate analysis, Belatacept treatment was the only significant factor for the improvement of ΔeGFR. This is in line with the BENEFIT and BENEFIT-EXT studies, which also demonstrated an increase of GFR over a follow-up of seven years [
12,
13,
14]. However, the CNI comparator cohort consisted of cyclosporine A-treated patients only, whereas our group was mainly treated with tacrolimus (68% of patients). Our recipients were of a similar age (56 years) to recipients in BENEFIT-EXT, but older compared to BENEFIT (43 years). Additionally, our CV high risk cohorts consisted of more diabetic patients (CNI group: 57%, Belatacept group: 32% vs. BENEFIT: 15%, BENEFIT-EXT: 16%) and had worse donor characteristics (living donors: CNI group 4%, Belatacept group 15% vs. BENEFIT 58%, BENEFIT-EXT not reported). Furthermore, the BENEFIT studies did not report the number of patients suffering from established cardiovascular disease, which was substantial in our Belatacept (94%) and CNI patients (75%). Nevertheless, and although Belatacept patients had inferior renal allograft function at the time of discharge after transplantation, serum creatinine levels and eGFR were similar at follow-up in this high CV risk cohort compared to CNI-treated patients. Bertrand et al. [
15] and Le Meur et al. [
16] reported similar results in 17 and 25 patients treated with Belatacept, because of vascular damage and CNI intolerance.
Belatacept was not associated with an increased risk of rejection in our patients. BENEFIT-EXT [
17] reported a higher risk in Belatacept-treated patients, whereas BENEFIT [
18] found no significant difference. However, our CNI cohort was mainly treated with tacrolimus, which is generally accepted to have a slightly higher immunosuppressive potential, rather than cyclosporine A as in the BENEFIT(-EXT) studies. Belatacept was not a risk factor for graft loss in our cohort (HR 0.987, 95%CI 0.283–3.417,
p = 0.980), which is in line with the literature [
17,
18].
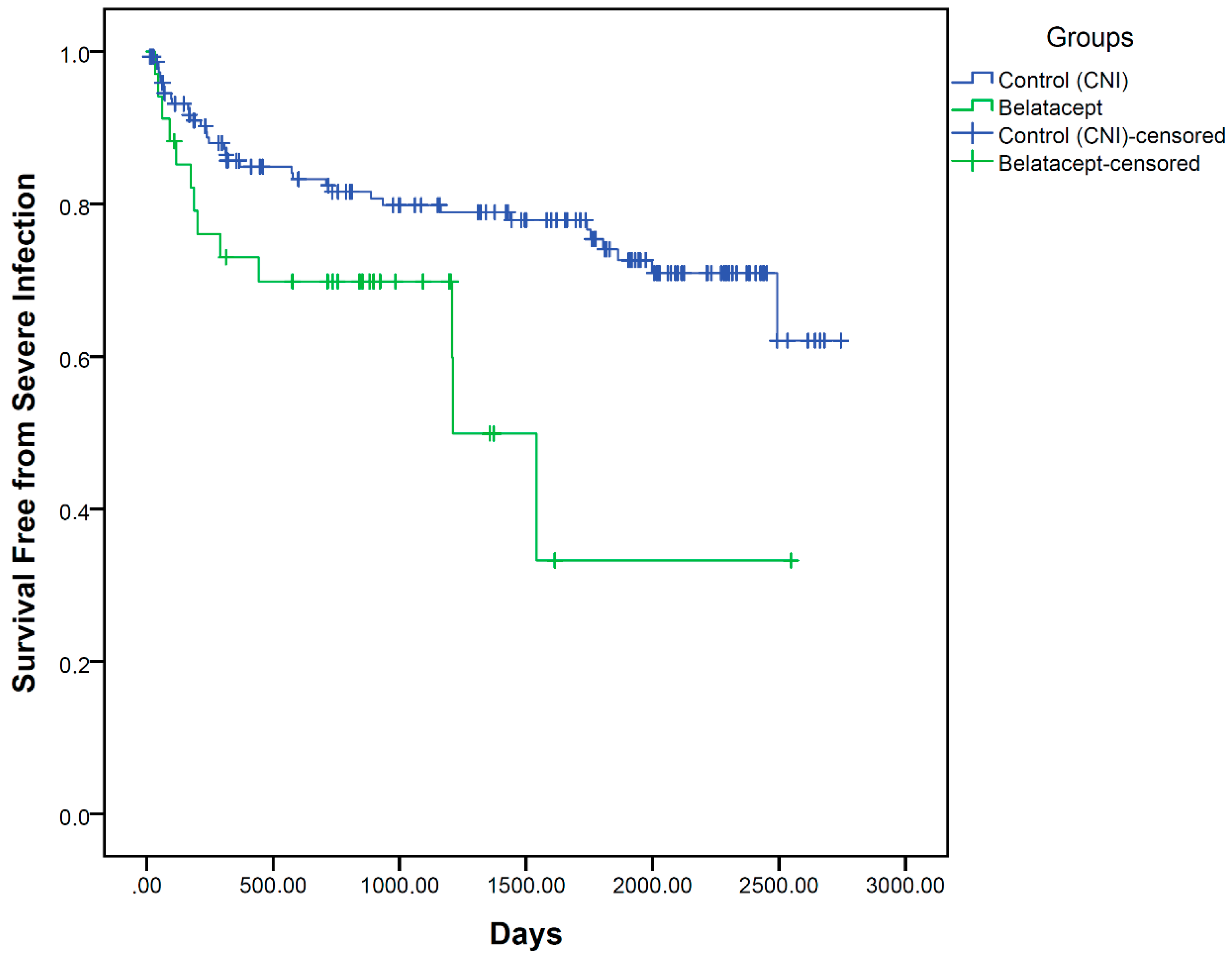
Concerning safety and in contrast to Florman et al. [
13], we found that Belatacept treatment was associated with an increased incidence of severe infections in the univariate Cox regression. The most obvious differences were higher event rates of diarrhoea, urinary tract infection and sepsis. Sepsis as an endpoint has not been reported in any previous studies of Belatacept patients. In line with our data, gastroenteritis and urinary tract infections were numerically higher in the switch studies [
7,
8,
19]. However, in the multivariate regression analysis, Belatacept treatment was not associated with an increase of this endpoint. One explanation for the higher incidence of gastroenteritis (diarrhoea) might be the more frequent use of mycophenlate in Belatacept patients (76.47 vs. 60.67%; 1.26–fold more), which is known to have such gastrointestinal side-effects. The reason for this is that physicians tend to prescribe the triple combination of mycophenolic acid, steroids and Belatacept, as only this regimen was approved for renal allograft recipients. However, it cannot be ruled out that some examples of mycophenolate-associated diarrhoea have been misdiagnosed as infectious diarrhoea, therefore increasing the proportion of diarrhoea in Belatacept patients compared to CNI patients, although the fold-change of diarrhoea (8.8 vs. 0.7%, 12.57-fold) substantially exceeds the use of mycophenlate in the Belatacept compared to the CNI group (1.26-fold, see above). Additionally, the proportion of mycophenolate-treated patients in the switch studies was almost identical between the groups (and higher compared to our data (approx. 94%)) [
7,
8,
19].
In our cohort, Belatacept treatment was not a risk factor for CMV reactivation, malignancy or death. This is in line with the published data cited above. Additionally, Belatacept treatment was not a risk factor for BKV reactivations either in patients’ serum or urine. Unfortunately, data on these endpoints were not reported in the BENEFIT and BENEFIT-EXT studies. Nevertheless, our data is in line with the phase II studies, which showed only slightly increased cumulative incidence rates (0.85 vs. 0 [
19]) and events (4 vs. 0% [
8] and 2 vs. 0% [
7]) in Belatacept patients. Unfortunately, no statistics were calculated in these studies.
Published data suggest a beneficial impact of Belatacept on arterial stiffness and metabolic parameters (e.g., arterial hypertension and lipid profile) or post-transplant diabetes mellitus. The authors concluded that this could improve kidney transplant recipients’ survival by reducing events related to those factors [
9,
17,
18,
20]. However, available data from the long-term outcomes of these studies do not show a significant difference in severely adverse events (including cardiac or vascular disorders) [
12,
14]. Concerning patients with high cardiovascular risk, the only study that has been published so far was a post-hoc analysis of patients with pre-existing diabetes of the BENEFIT and BENEFIT-EXT cohorts. Patient survival and renal function were numerically but not significantly higher in Belatacept patients at 12 months’ follow-up and, unfortunately, cardiovascular events were not reported [
8]. Hence, to the best of our knowledge, this is the first report on cardiovascular events in Belatacept compared to CNI-treated patients. We found no difference between Belatacept- and CNI-treated patients concerning de novo cardiovascular events with a cumulative follow-up of 1194 months in Belatacept (
n = 35) and 7309 months in CNI patients (
n = 150).
Our study has limitations. Firstly, this is a retrospective study, which by nature does not provide the same data quality as a prospective design. Secondly, the size of the study population is relatively small, as we included only 34 Belatacept patients and 150 CNI patients as a comparator. Thirdly, the baseline characteristics of time on RRT, primary renal disease, diabetes, cardiovascular disease and arterial hypertension were different between our two populations (
Table 1) and it is possible that statistical methods were not able to correct appropriately for this issue. Fourthly, the median time of follow-up was longer in CNI patients (Belatacept: 1054 vs. CNI: 1462 days) but not statistically significant (
p = 0.084). From our point of view, the duration of follow-up is still significant, although one might argue that a longer follow-up would have been beneficial, especially for the end point “cardiovascular event”. However, the number of studies that have published data of renal allograft recipients on Belatacept-based immunosuppression is generally limited. In total, until the end of 2014, the data of 521 Belatacept patients, which were compared to CNI-treated controls, were published [
21]. Recently, one study of 17 Belatacept patients matched to 18 control patients, and two studies of 25 and 6 cases that were converted from CNI to Belatacept without a control population, were published [
15,
16,
22]. The randomized controlled trials BENEFIT [
18], BENEFIT-EXT [
17] and the switch study [
8] originally reported one-year results of 181, 129 and 81 belatacept patients compared to a CNI-treated cohort of similar size. Hence, we believe that our cohort size and follow-up period is considerable and contributes information in a real world setting.
In conclusion, we believe that Belatacept is an efficient, beneficial and safe option for renal allograft recipients at high cardiovascular risk. In our cohort, Belatacept treatment was associated with a superior graft function compared to a CNI-treated cohort and was not a risk factor for renal allograft rejection, -loss, severe infection, CMV- or BKV-reactivation, malignancy or death.

 ,
, 

{kind=link}