Low-Dose Aspirin for the Primary Prevention of Cardiovascular Disease in Diabetic Individuals: A Meta-Analysis of Randomized Control Trials and Trial Sequential Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Data Sources and Searches
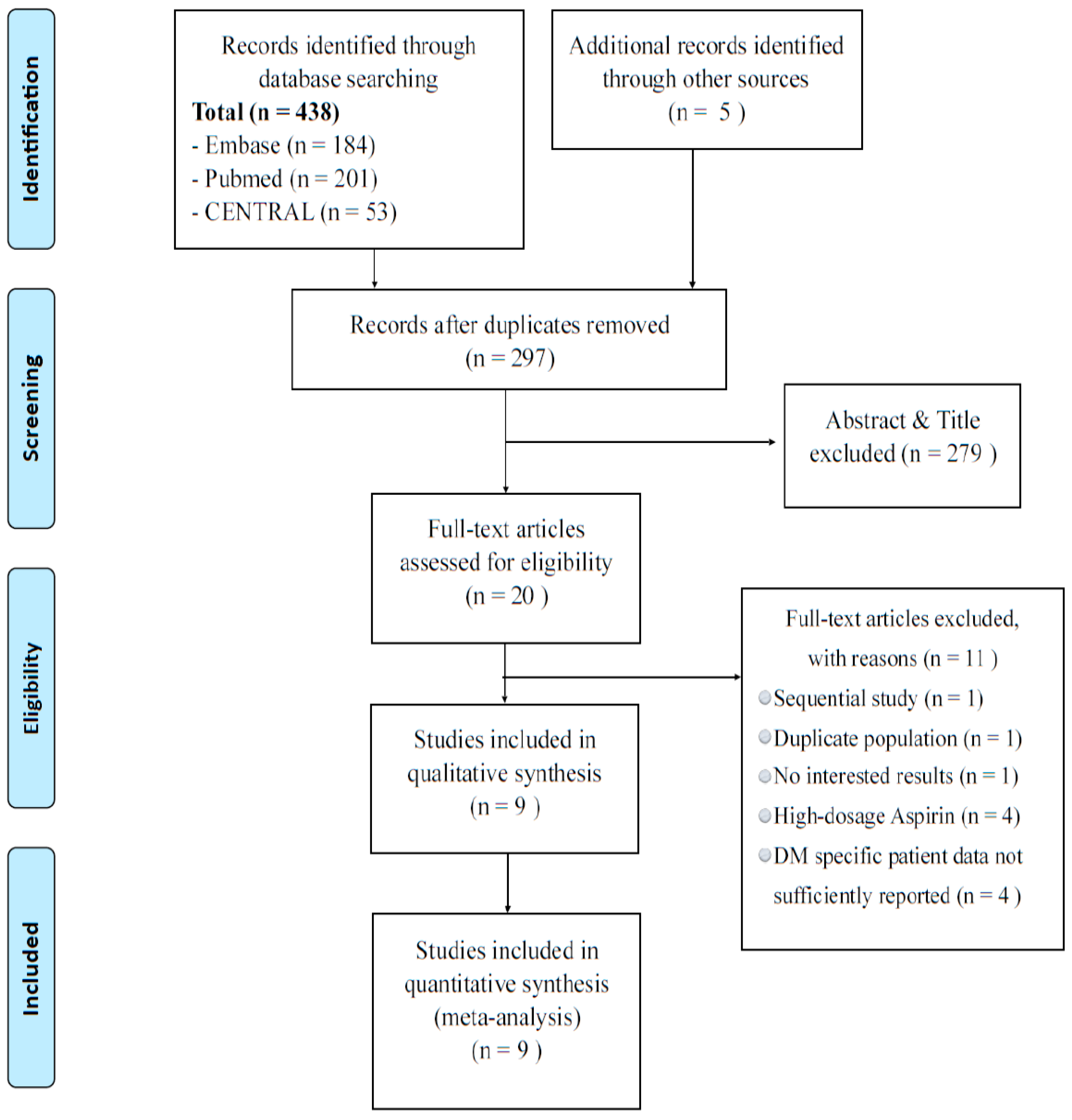
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
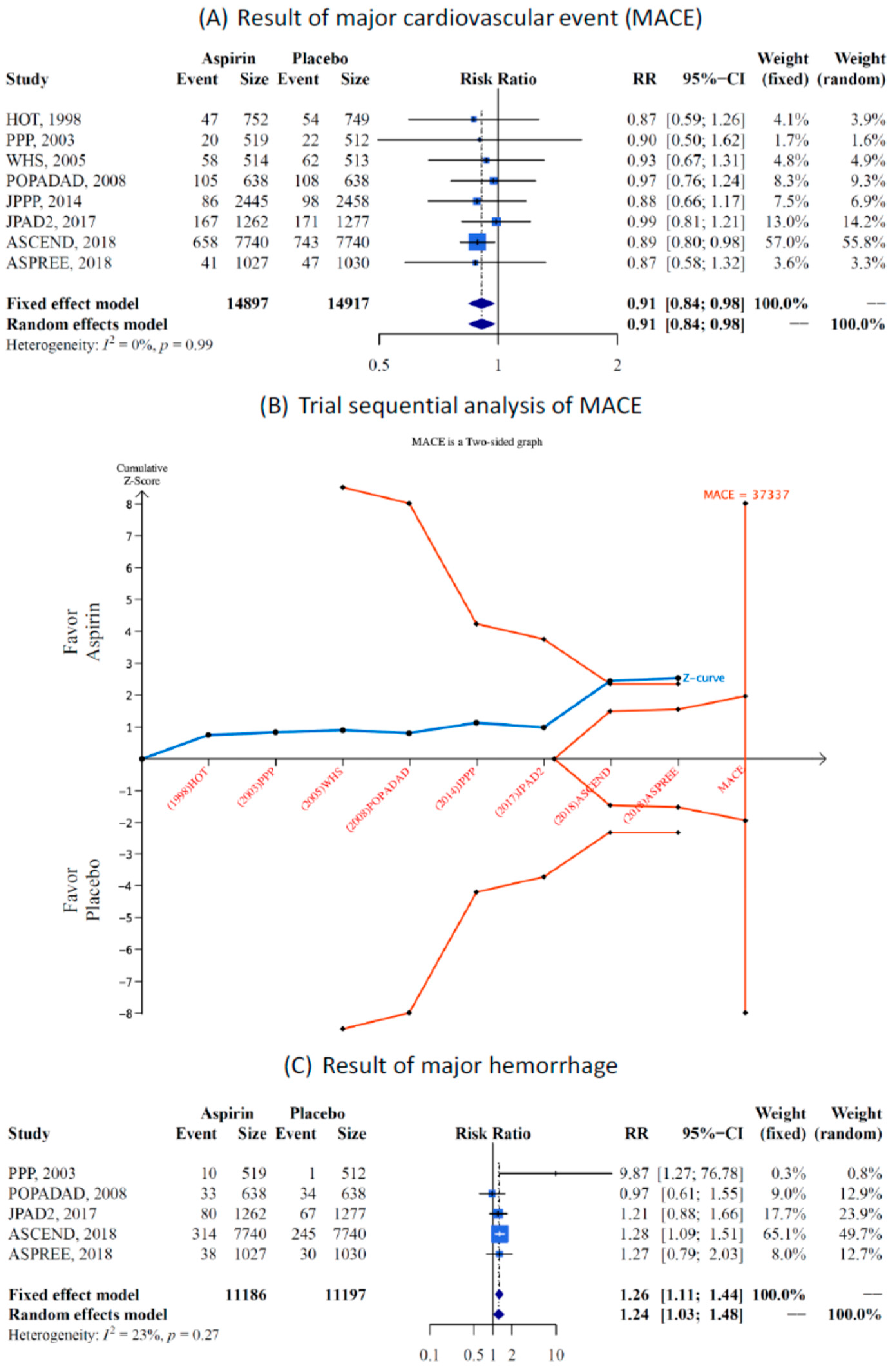
3.1. Major Adverse Cardiovascular Event and Major Hemorrhage
3.2. Efficacy and Safety End Point
3.3. Sensitivity Tests and Publication Bias
4. Discussion
4.1. Comparison of Previous Published Meta-Analysis
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Emerging Risk Factors Collaboration; Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [PubMed]
- Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002, 324, 71–86. [Google Scholar] [CrossRef] [Green Version]
- Campbell, C.L.; Smyth, S.; Montalescot, G.; Steinhubl, S.R. Aspirin dose for the prevention of cardiovascular disease: A systematic review. JAMA 2007, 297, 2018–2024. [Google Scholar] [CrossRef]
- Capodanno, D.; Angiolillo, D.J. Aspirin for primary cardiovascular risk prevention and beyond in diabetes mellitus. Circulation 2016, 134, 1579–1594. [Google Scholar] [CrossRef]
- Pignone, M.; Alberts, M.J.; Colwell, J.A.; Cushman, M.; Inzucchi, S.E.; Mukherjee, D.; Rosenson, R.S.; Williams, C.D.; Wilson, P.W.; Kirkman, M.S. Aspirin for primary prevention of cardiovascular events in people with diabetes: A position statement of the American Diabetes Association, a scientific statement of the American Heart Association, and an expert consensus document of the American College of Cardiology Foundation. Diabetes Care 2010, 33, 1395–1402. [Google Scholar] [PubMed]
- American Diabetes Association. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42, S103–S123. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [PubMed]
- The ASCEND Study Collaborative Group. Effects of aspirin for primary prevention in persons with diabetes mellitus. N. Engl. J. Med. 2018, 379, 1529–1539. [Google Scholar]
- McNeil, J.J.; Wolfe, R.; Woods, R.L.; Tonkin, A.M.; Donnan, G.A.; Nelson, M.R.; Reid, C.M.; Lockery, J.E.; Kirpach, B.; Storey, E. Effect of aspirin on cardiovascular events and bleeding in the healthy elderly. N. Engl. J. Med. 2018, 379, 1509–1518. [Google Scholar] [CrossRef]
- Saito, Y.; Okada, S.; Ogawa, H.; Soejima, H.; Sakuma, M.; Nakayama, M.; Doi, N.; Jinnouchi, H.; Waki, M.; Masuda, I.; et al. Low-Dose Aspirin for Primary Prevention of Cardiovascular Events in Patients with Type 2 Diabetes Mellitus: 10-Year Follow-Up of a Randomized Controlled Trial. Circulation 2017, 135, 659–670. [Google Scholar] [CrossRef]
- De Berardis, G.; Sacco, M.; Strippoli, G.F.; Pellegrini, F.; Graziano, G.; Tognoni, G.; Nicolucci, A. Aspirin for primary prevention of cardiovascular events in people with diabetes: Meta-analysis of randomised controlled trials. BMJ 2009, 339, b4531. [Google Scholar] [CrossRef] [PubMed]
- Butalia, S.; Leung, A.A.; Ghali, W.A.; Rabi, D.M. Aspirin effect on the incidence of major adverse cardiovascular events in patients with diabetes mellitus: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2011, 10, 25. [Google Scholar] [CrossRef] [PubMed]
- Kokoska, L.A.; Wilhelm, S.M.; Garwood, C.L.; Berlie, H.D. Aspirin for primary prevention of cardiovascular disease in patients with diabetes: A meta-analysis. Diabetes Res. Clin. Pract. 2016, 120, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Sun, A.; Zhang, P.; Wu, C.; Zhang, S.; Fu, M.; Wang, K.; Zou, Y.; Ge, J. Aspirin for primary prevention of cardiovascular events in patients with diabetes: A meta-analysis. Diabetes Res. Clin. Pract. 2010, 87, 211–218. [Google Scholar] [CrossRef]
- Kunutsor, S.; Seidu, S.; Khunti, K. Aspirin for primary prevention of cardiovascular and all-cause mortality events in diabetes: Updated meta-analysis of randomized controlled trials. Diabet. Med. 2017, 34, 316–327. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. Available online: https://handbook-5-1.cochrane.org/ (accessed on 1 April 2019).
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series; Higgins, J.P.T., Green, S., Eds.; John Wiley & Sons: Chichester, UK, 2008; pp. 243–296. [Google Scholar]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Ntali, G.; Wass, J.A. Epidemiology, clinical presentation and diagnosis of non-functioning pituitary adenomas. Pituitary 2018, 21, 111–118. [Google Scholar] [CrossRef] [PubMed]
- GRADEpro Guideline Development Tool (Software). Available online: https://gradepro.org./ (accessed on 1 April 2019).
- Schünemann, H.J.; Oxman, A.D.; Higgins, J.P.T.; Vist, G.E.; Glasziou, P.; Guyatt, G.H. Chapter 11: Presenting resultsand ’Summary of findings’ tables. In Cochrane Handbook for Systematic Reviewsof Interventions Version 5.1.0 (Updated March 2011); Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Wetterslev, J.; Thorlund, K.; Brok, J.; Gluud, C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J. Clin. Epidemiol. 2008, 61, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Thorlund, K.; Imberger, G.; Walsh, M.; Chu, R.; Gluud, C.; Wetterslev, J.; Guyatt, G.; Devereaux, P.J.; Thabane, L. The number of patients and events required to limit the risk of overestimation of intervention effects in meta-analysis—A simulation study. PLoS ONE 2011, 6, e25491. [Google Scholar] [CrossRef] [PubMed]
- Brok, J.; Thorlund, K.; Gluud, C.; Wetterslev, J. Trial sequential analysis reveals insufficient information size and potentially false positive results in many meta-analyses. J. Clin. Epidemiol. 2008, 61, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Whitehead, A.; Simmonds, M. Sequential methods for random-effects meta-analysis. Stat. Med. 2011, 30, 903–921. [Google Scholar] [CrossRef] [PubMed]
- Wetterslev, J.; Engstrøm, J.; Gluud, C.; Thorlund, K. Trial sequential analysis: Methods and software for cumulative meta-analyses. Cochrane Methods Cochrane Database Syst. Rev. Suppl. 2012, 1, 29–31. [Google Scholar]
- Medical Research Council’s General Practice Research Framework. Thrombosis prevention trial: Randomised trial of low-intensity oral anticoagulation with warfarin and low-dose aspirin in the primary prevention of ischaemic heart disease in men at increased risk. Lancet 1998, 351, 233–241. [Google Scholar] [CrossRef]
- Hansson, L.; Zanchetti, A.; Carruthers, S.G.; Dahlöf, B.; Elmfeldt, D.; Julius, S.; Ménard, J.; Rahn, K.H.; Wedel, H.; Westerling, S. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: Principal results of the Hypertension Optimal Treatment (HOT) randomised trial. Lancet 1998, 351, 1755–1762. [Google Scholar] [CrossRef]
- Sacco, M.; Pellegrini, F.; Roncaglioni, M.C.; Avanzini, F.; Tognoni, G.; Nicolucci, A. Primary prevention of cardiovascular events with low-dose aspirin and vitamin E in type 2 diabetic patients: Results of the Primary Prevention Project (PPP) trial. Diabetes Care 2003, 26, 3264–3272. [Google Scholar] [CrossRef]
- Ridker, P.M.; Cook, N.R.; Lee, I.-M.; Gordon, D.; Gaziano, J.M.; Manson, J.E.; Hennekens, C.H.; Buring, J.E. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N. Engl. J. Med. 2005, 352, 1293–1304. [Google Scholar] [CrossRef] [PubMed]
- Belch, J.; MacCuish, A.; Campbell, I.; Cobbe, S.; Taylor, R.; Prescott, R.; Lee, R.; Bancroft, J.; MacEwan, S.; Shepherd, J. The prevention of progression of arterial disease and diabetes (POPADAD) trial: Factorial randomised placebo controlled trial of aspirin and antioxidants in patients with diabetes and asymptomatic peripheral arterial disease. BMJ 2008, 337, a1840. [Google Scholar] [CrossRef]
- Ikeda, Y.; Shimada, K.; Teramoto, T.; Uchiyama, S.; Yamazaki, T.; Oikawa, S.; Sugawara, M.; Ando, K.; Murata, M.; Yokoyama, K. Low-dose aspirin for primary prevention of cardiovascular events in Japanese patients 60 years or older with atherosclerotic risk factors: A randomized clinical trial. JAMA 2014, 312, 2510–2520. [Google Scholar] [CrossRef]
- Ogawa, H.; Nakayama, M.; Morimoto, T.; Uemura, S.; Kanauchi, M.; Doi, N.; Jinnouchi, H.; Sugiyama, S.; Saito, Y.; Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD) Trial Investigators. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: A randomized controlled trial. JAMA 2008, 300, 2134–2141. [Google Scholar] [CrossRef] [PubMed]
- Lai, K.C.; Lam, S.K.; Chu, K.M.; Wong, B.C.; Hui, W.M.; Hu, W.H.; Lau, G.K.; Wong, W.M.; Yuen, M.F.; Chan, A.O. Lansoprazole for the prevention of recurrences of ulcer complications from long-term low-dose aspirin use. N. Engl. J. Med. 2002, 346, 2033–2038. [Google Scholar]
- Stavrakis, S.; Stoner, J.A.; Azar, M.; Wayangankar, S.; Thadani, U. Low-dose aspirin for primary prevention of cardiovascular events in patients with diabetes: A meta-analysis. Am. J. Med. Sci. 2011, 341, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Younis, N.; Williams, S.; Ammori, B.; Soran, H. Role of aspirin in the primary prevention of cardiovascular disease in diabetes mellitus: A meta-analysis. Expert Opin. Pharmacother. 2010, 11, 1459–1466. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Lee, S.; Kim, J.H. Real-world Evidence versus Randomized Controlled Trial: Clinical Research Based on Electronic Medical Records. J. Korean Med. Sci. 2018, 33, e213. [Google Scholar] [CrossRef] [PubMed]
- De Berardis, G.; Sacco, M.; Evangelista, V.; Filippi, A.; Giorda, C.B.; Tognoni, G.; Valentini, U.; Nicolucci, A. Aspirin and Simvastatin Combination for Cardiovascular Events Prevention Trial in Diabetes (ACCEPT-D): Design of a randomized study of the efficacy of low-dose aspirin in the prevention of cardiovascular events in subjects with diabetes mellitus treated with statins. Trials 2007, 8, 21. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Source | Trial Design | Country (Study Name) | Population (DM) | Case (Mean Age) | Males | Aspirin Dosage | Mean Follow up (Completion Rate) |
|---|---|---|---|---|---|---|---|
| MRC 1998 [27] | PC, RCT | UK (TPT) | Patients at high risk of IHD (type 1 and 2) | 68 (57.3 years *) | 100.0 | 75 mg/daily | 6.7 years/98.9 |
| Hansson et al. 1998 [28] | DB, RCT | Globally (HOT) | Participants with hypertension (type 1 and 2) | 1501 (61.5 years) | NR | 75 mg/daily | 3.8 years/97.4 |
| Sacco et al. 2003 [29] | MC, OP, RCT, 2 × 2 factorial design | Italy (PPP) | Participants > 50 years with > one cardiovascular risk factor (type 2) | 1031 (64.2 years) | 48.2 | 100 mg/daily | 3.6 years/99.3 |
| Ridker et al. 2005 [30] | MC, DB, RCT, 2 × 2 factorial design | USA (WHS) | Healthy women (NA) | 1027 (54.6 years *) | 0 | 100 mg/every other day | 10.1 years/99.4 |
| Belch et al. 2008 [31] | DB, RCT, 2 × 2 factorial design | UK (POPADAD) | Patients aged ≥ 40 years plus ABP ≤ 0.99 (type 1 and 2) | 1276 (60 years) | 44.1 | 100 mg/daily | 6.7 years/99.5 |
| Ikeda et al. 2014 [32] | OP, RCT | Japan (JPPP) | Elderly with multiple atherosclerotic risk factors (NR) | 4903 (70.6 years *) | NR | 100 mg/daily | 5.0 years/98.7 |
| Saito et al. 2017 [10] | MC, OP, RCT | Japan (JPAD2) | Patients with Type 2 Diabetes (type 2) | 2160 (64.4 years) | 55.5 | 81 or 100 mg/daily | 10.3 years/63.8 |
| ASCEND group 2018 [8] | DB, RCT | UK (ASCEND) | Patients with diabetes (type 1 and 2) | 15,800 (63.3 years) | 62.6 | 100 mg/daily | 7.4 years/99.1 |
| McNeil et al. 2018 [9] | DB, RCT | USA/Australia (ASPREE) | Health older (NR) | 2057 (74 years *) | 44 | 100 mg/daily | 4.7 years/97.2 |
| Outcome Assessment | No. of Trials (Patients) | Anticipated Absolute Effects (95% CI) | Risk Ratio (95% CI) Random-Effect Estimate | p-Value Random-Effect Estimate | Heterogeneity I2(%) Cochrane Q p-Value | Certainty of Evidence (GRADE) † | |
|---|---|---|---|---|---|---|---|
| Risk with Placebo | Risk with Aspirin | ||||||
| MACE | 8 (29,814) | 87 per 1000 | 80 per 1000 (73 to 86) | 0.91 (0.84–0.98) | 0.018 * | 0.0% p = 1.00 | ⨁⨁⨁◯ MODERATE |
| MACE with age ≥ 60 years | 5 (18,664) | 111 per 1000 | 101 per 1000 (92 to 108) | 0.91 (0.83–0.98) | 0.023 * | 0.0% p = 1.00 | ⨁⨁◯◯ LOW |
| MACE with age < 60 years | 3 (7212) | 90 per 1000 | 91 per 1000 (65 to 124) | 1.00 (0.73–1.39) | 0.973 | 67.2% p = 0.0476 | ⨁◯◯◯ Very LOW |
| Myocardial infarction | 6 (22,854) | 31 per 1000 | 32 per 1000 (26 to 38) | 1.01 (0.84–1.22) | 0.891 | 21.1% p = 0.275 | ⨁⨁◯◯ LOW |
| Fatal myocardial infarction | 3 (19,295) | 15 per 1000 | 14 per 1000 (9 to 23) | 0.98 (0.60–1.60) | 0.942 | 44.1% p = 0.166 | ⨁◯◯◯ Very LOW |
| Stroke | 7 (22,922) | 36 per 1000 | 31 per 1000 (27 to 35) | 0.84 (0.73–0.97) | 0.017 * | 0.0% p = 0.645 | ⨁⨁⨁◯ MODERATE |
| Fatal stroke | 3 (19,025) | 5 per 1000 | 6 per 1000 (4 to 9) | 1.20 (0.82–1.77) | 0.349 | 0.0% p = 0.773 | ⨁◯◯◯ Very LOW |
| Coronary heart disease | 6 (22,923) | 48 per 1000 | 45 per 1000 (40 to 50) | 0.94 (0.84–0.1.06) | 0.323 | 0.0% p = 0.864 | ⨁⨁◯◯ LOW |
| Major hemorrhage | 5 (22,383) | 34 per 1000 | 42 per 1000 (35 to 50) | 1.24 (1.03–1.48) | 0.0221 * | 22.9% p = 0.2687 | ⨁⨁◯◯ LOW |
| Major intracranial hemorrhage | 5 (21,353) | 6 per 1000 | 7 per 1000 (5 to 9) | 1.08 (0.77–1.50) | 0.654 | 0.0% p = 0.666 | ⨁⨁◯◯ LOW |
| Major Gl bleeding | 4 (20,326) | 14 per 1000 | 20 per 1000 (13 to 32) | 1.43 (0.92–2.22) | 0.117 | 56.7% p = 0.074 | ⨁⨁◯◯ LOW |
| All-cause death | 6 (23,884) | 87 per 1000 | 84 per 1000 (78 to 92) | 0.97 (0.90–1.06) | 0.537 | 0.0% p = 0.457 | ⨁⨁◯◯ LOW |
| Cardiovascular death | 5 (21,827) | 18 per 1000 | 17 per 1000 (14 to 21) | 0.94 (0.77–1.14) | 0.517 | 0.0% p = 0.545 | ⨁⨁◯◯ LOW |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, M.-H.; Lee, C.-H.; Lin, C.; Zou, Y.-F.; Lu, C.-H.; Hsieh, C.-H.; Lee, C.-H. Low-Dose Aspirin for the Primary Prevention of Cardiovascular Disease in Diabetic Individuals: A Meta-Analysis of Randomized Control Trials and Trial Sequential Analysis. J. Clin. Med. 2019, 8, 609. https://doi.org/10.3390/jcm8050609
Lin M-H, Lee C-H, Lin C, Zou Y-F, Lu C-H, Hsieh C-H, Lee C-H. Low-Dose Aspirin for the Primary Prevention of Cardiovascular Disease in Diabetic Individuals: A Meta-Analysis of Randomized Control Trials and Trial Sequential Analysis. Journal of Clinical Medicine. 2019; 8(5):609. https://doi.org/10.3390/jcm8050609
Chicago/Turabian StyleLin, Ming-Hsun, Chien-Hsing Lee, Chin Lin, Yi-Fen Zou, Chieh-Hua Lu, Chang-Hsun Hsieh, and Cho-Hao Lee. 2019. "Low-Dose Aspirin for the Primary Prevention of Cardiovascular Disease in Diabetic Individuals: A Meta-Analysis of Randomized Control Trials and Trial Sequential Analysis" Journal of Clinical Medicine 8, no. 5: 609. https://doi.org/10.3390/jcm8050609