Preoperative Health-Related Quality of Life Predicts Minimal Clinically Important Difference and Survival after Surgical Resection of Hepatocellular Carcinoma

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
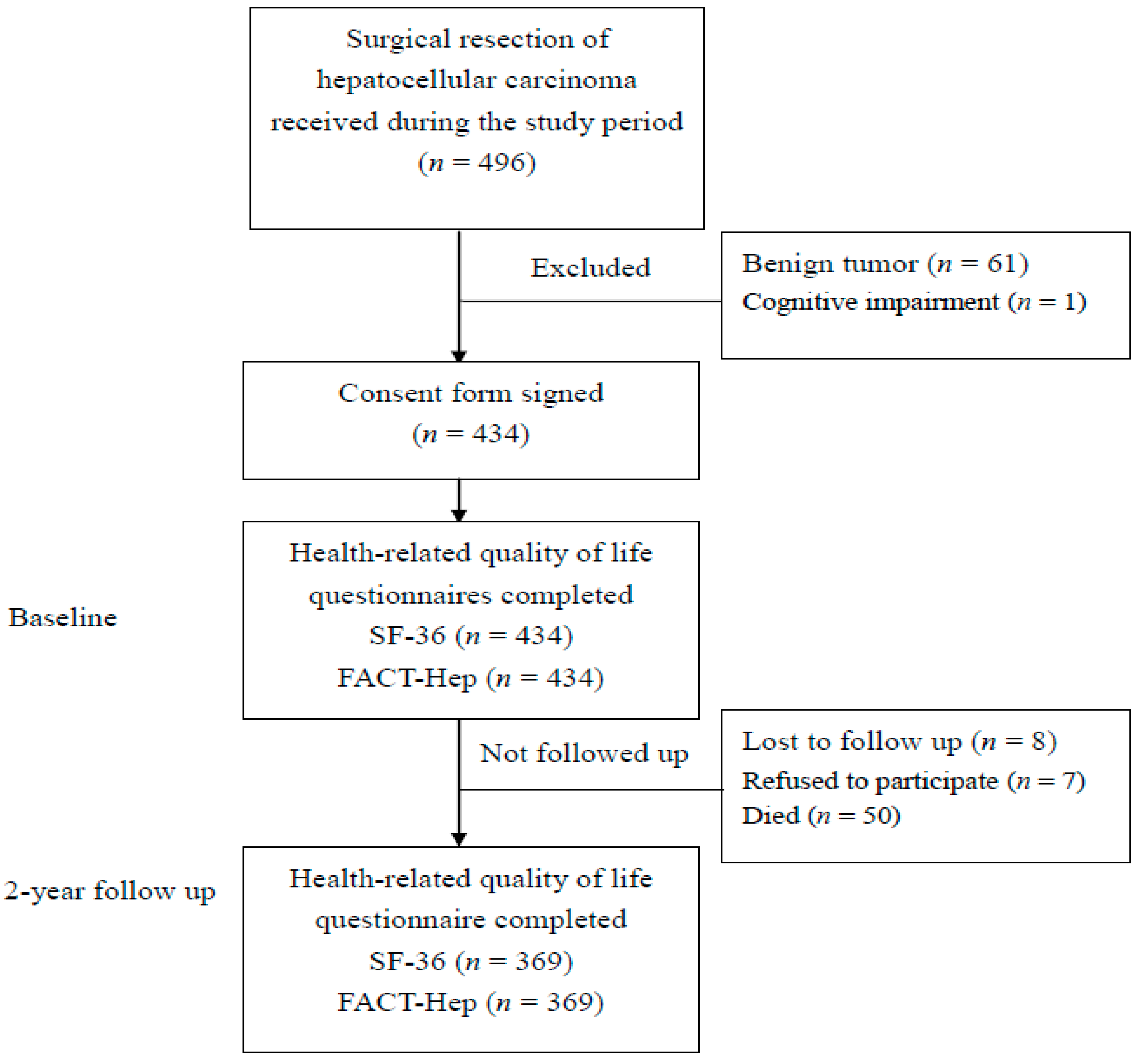
2.1. Subjects and Data Collection
2.2. Study Protocol
2.3. Measures of HRQoL
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. HRQoL Outcomes
3.3. Multivariable Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dhir, M.; Melin, A.A.; Douaiher, J.; Lin, C.; Zhen, W.K.; Hussain, S.M.; Geschwind, J.F.; Doyle, M.B.; Abou-Alfa, G.K.; Are, C. A Review and update of treatment options and controversies in the management of hepatocellular carcinoma. Ann. Surg. 2016, 263, 1112–1125. [Google Scholar] [CrossRef]
- Robertson, F.P.; Fuller, B.J.; Davidson, B.R. An evaluation of ischaemic preconditioning as a method of reducing ischaemia reperfusion injury in liver surgery and transplantation. J. Clin. Med. 2017, 6, 69. [Google Scholar] [CrossRef] [PubMed]
- Glantzounis, G.K.; Paliouras, A.; Stylianidi, M.C.; Milionis, H.; Tzimas, P.; Roukos, D.; Pentheroudakis, G.; Felekouras, E. The role of liver resection in the management of intermediate and advanced stage hepatocellular carcinoma. A systematic review. Eur. J. Surg. Oncol. 2018, 44, 195–208. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Health-related quality of life after treatment for bladder cancer in England. J. Clin. Med. 2018, 7, 553. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.C.; Lee, K.T.; Wang, J.J.; Sun, D.P.; Lee, H.H.; Shi, H.Y. Health-related quality of life before and after surgical resection of hepatocellular carcinoma: A prospective study. Asian Pac. J. Cancer Prev. 2018, 19, 65–72. [Google Scholar]
- Shapiro, C.L. Highlights of recent findings on quality-of-life management for patients with cancer and their survivors. JAMA Oncol. 2016, 2, 1401–1402. [Google Scholar] [CrossRef]
- Costa, D.S. Reflective, causal, and composite indicators of quality of life: A conceptual or an empirical distinction? Qual. Life Res. 2015, 24, 2057–2065. [Google Scholar] [CrossRef]
- Heffernan, N.; Cella, D.; Webster, K.; Odom, L.; Martone, M.; Passik, S.; Bookbinder, M.; Fong, Y.; Jarnagin, W.; Blumgart, L. Measuring health-related quality of life in patients with hepatobiliary cancers: The functional assessment of cancer therapy-hepatobiliary questionnaire. J. Clin. Oncol. 2002, 20, 2229–2239. [Google Scholar] [CrossRef] [PubMed]
- Jayadevappa, R.; Cook, R.; Chhatre, S. Minimal important difference to infer changes in health-related quality of life-a systematic review. Clin. Epidemiol. 2017, 89, 188–198. [Google Scholar] [CrossRef]
- Quinten, C.; Martinelli, F.; Coens, C.; Sprangers, M.A.; Ringash, J.; Gotay, C.; Bjordal, K.; Greimel, E.; Reeve, B.B.; Maringwa, J.; et al. A global analysis of multitrial data investigating quality of life and symptoms as prognostic factors for survival in different tumor sites. Cancer 2014, 120, 302–311. [Google Scholar] [CrossRef]
- Quinten, C.; Coens, C.; Mauer, M.; Comte, S.; Sprangers, M.A.; Cleeland, C.; Osoba, D.; Bjordal, K.; Bottomley, A.; EORTC Clinical Groups. Baseline quality of life as a prognostic indicator of survival: A meta-analysis of individual patient data from EORTC clinical trials. Lancet Oncol. 2009, 10, 865–871. [Google Scholar] [CrossRef]
- Grande, G.E.; Farquhar, M.C.; Barclay, S.I.; Todd, C.J. Quality of life measures (EORTC QLQ-C30 and SF-36) as predictors of survival in palliative colorectal and lung cancer patients. Palliat. Support. Care 2009, 7, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Dunne, D.F.; Jack, S.; Jones, R.P.; Jones, L.; Lythgoe, D.T.; Malik, H.Z.; Poston, G.J.; Palmer, D.H.; Fenwick, S.W. Randomized clinical trial of prehabilitation before planned liver resection. Br. J. Surg. 2016, 103, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Quinten, C.; Maringwa, J.; Gotay, C.C.; Martinelli, F.; Coens, C.; Reeve, B.B.; Flechtner, H.; Greimel, E.; King, M.; Osoba, D.; et al. Patient self-reports of symptoms and clinician ratings as predictors of overall cancer survival. J. Natl. Cancer Inst. 2011, 103, 1851–1858. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.W.J.; Eisenberg, D.F.; Cella, D.; Zhao, N.; de Boer, C.; DeWitte, M. The prognostic significance of patient-reported outcomes in cancer clinical trials. J. Clin. Oncol. 2008, 26, 1355–1363. [Google Scholar]
- Lin, S.; Hoffmann, K.; Schemmer, P. Treatment of hepatocellular carcinoma: A systematic review. Liver Cancer 2012, 1, 144–158. [Google Scholar] [CrossRef] [PubMed]
- Pompili, C.; Salati, M.; Refai, M.; Berardi, R.; Onofri, A.; Mazzanti, P.; Brunelli, A. Preoperative quality of life predicts survival following pulmonary resection in stage I non-small-cell lung cancer. Eur. J. Cardiothorac. Surg. 2013, 43, 905–910. [Google Scholar] [CrossRef]
- Ware, J.E.J.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Huang, I.C.; Wu, A.W.; Frangakis, C. Do the SF-36 and WHOQOL-BREF measure the same constructs? Evidence from the Taiwan population. Qual. Life Res. 2006, 5, 15–24. [Google Scholar] [CrossRef]
- Blondel, B.; Schwab, F.; Ungar, B.; Smith, J.; Bridwell, K.; Glassman, S.; Shaffrey, C.; Farcy, J.P.; Lafage, V. Impact of magnitude and percentage of global sagittal plane correction on health-related quality of life at 2-years follow-up. Neurosurgery 2012, 71, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Doll, K.M.; Snavely, A.C.; Kalinowski, A.; Irwin, D.E.; Bensen, J.T.; Bae-Jump, V.; Boggess, J.F.; Soper, J.T.; Brewster, W.R.; Gehrig, P.A. Preoperative quality of life and surgical outcomes in gynecologic oncology patients: A new predictor of operative risk? Gynecol. Oncol. 2014, 133, 546–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steel, J.L.; Eton, D.T.; Cella, D.; Olek, M.C.; Carr, B.I. Clinically meaningful changes in health-related quality of life in patients diagnosed with hepatobiliary carcinoma. Ann. Oncol. 2006, 17, 304–312. [Google Scholar] [CrossRef] [PubMed]
- McGlothlin, A.E.; Lewis, R.J. Minimal clinically important difference: Defining what really matters to patients. JAMA 2014, 312, 1342–1343. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | N (%) or Mean ± SD | |
|---|---|---|
| Gender | Male | 271 (73.4) |
| Female | 98 (26.6) | |
| Age, years | 60.2 ± 10.8 | |
| Marital status | Married | 335 (90.8) |
| Divorced or widowed | 34 (9.2) | |
| Education | 8.7 ± 3.6 | |
| No formal education | 26 (7.1) | |
| Primary school | 122 (33.1) | |
| Junior high school | 75 (20.3) | |
| Senior high school | 92 (24.9) | |
| College or above | 54 (14.6) | |
| Body mass index, kg/m2 | 25.0 ± 3.5 | |
| Normal (18.5~24.9 kg/m2) | 218 (59.1) | |
| Overweight (25.0~29.9 kg/m2) | 124 (33.6) | |
| Obese (≥30.0 kg/m2) | 27 (7.3) | |
| Charlson co-morbidity index, score | 1.6 ± 1.3 | |
| Co-residence with family | Yes | 358 (97.0) |
| No | 11 (3.0) | |
| Smoking | Yes | 71 (19.2) |
| No | 298 (80.8) | |
| Drinking | Yes | 78 (21.1) |
| No | 291 (78.8) | |
| Tumor stage | I | 216 (58.6) |
| II | 102 (27.6) | |
| III | 51 (13.8) | |
| Chemotherapy | Yes | 11 (3.0) |
| No | 358 (97.0) | |
| Radiotherapy | Yes | 5 (1.4) |
| No | 364 (98.6) | |
| Average length of stay, days | 13.0 ± 6.6 | |
| Variable | Preoperative | 2 Years Postoperative | 2 Years Postoperative-Preoperative | p Value |
|---|---|---|---|---|
| SF-36 PCS | 56.0 ± 8.7 | 61.7 ± 9.5 | 5.8 ± 7.2 | p < 0.001 |
| SF-36 MCS | 48.5 ± 8.1 | 57.1 ± 9.8 | 8.5 ± 8.4 | p < 0.001 |
| FACT-G total | 91.2 ± 10.4 | 98.7 ± 10.8 | 7.5 ± 10.9 | p < 0.001 |
| FACT-Hep total | 156.9 ± 14.2 | 165.6 ± 15.8 | 9.7 ± 13.3 | p < 0.001 |
| Variables | Odds Ratio (95% CI) | p Value |
|---|---|---|
| SF-36 PCS | ||
| Preoperative SF-36 PCS score | 0.90 (0.84, 0.96) | <0.001 |
| Age | 1.05 (1.01, 1.10) | 0.041 |
| Gender (male vs. female) | 0.31 (0.12, 0.83) | 0.019 |
| Education | 1.14 (1.01, 1.30) | 0.040 |
| Body mass index | 1.11 (1.09, 1.12) | 0.045 |
| SF-36 MCS | ||
| Preoperative SF-36 MCS score | 0.80 (0.73, 0.88) | <0.001 |
| Age | 1.01 (1.01, 1.02) | <0.001 |
| Body mass index | 0.91 (0.84, 0.99) | 0.034 |
| Charlson co-morbidity index | 1.53 (1.13, 1.94) | <0.001 |
| FACT-G total | ||
| Preoperative FACT-G total score | 0.92 (0.90, 0.95) | <0.001 |
| Age | 1.04 (1.01, 1.07) | 0.007 |
| Education | 1.12 (1.04, 1.21) | 0.002 |
| Body mass index | 1.19 (1.09, 1.29) | <0.001 |
| FACT-Hep total | ||
| Preoperative FACT-Hep total score | 0.97 (0.95, 0.98) | <0.001 |
| Age | 1.05 (1.02, 1.07) | 0.001 |
| Education | 1.11 (1.03, 1.19) | 0.007 |
| Body mass index | 1.09 (1.01, 1.18) | 0.020 |
| Variable | HR (95% CI) | p Value |
|---|---|---|
| Preoperative SF-36 PCS score | 1.05 (1.03, 1.08) | <0.001 |
| Preoperative SF-36 MCS score | 1.03 (1.01, 1.05) | <0.001 |
| Preoperative SF-36 physical function | 1.06 (1.01, 1.10) | <0.001 |
| Preoperative SF-36 role physical | 1.03 (1.00, 1.05) | <0.001 |
| Preoperative SF-36 bodily pain | 1.02 (1.01, 1.03) | 0.008 |
| Preoperative SF-36 general health | 1.07 (1.01, 1.14) | <0.001 |
| Preoperative SF-36 vitality | 1.02 (1.01, 1.04) | 0.001 |
| Preoperative SF-36 social function | 1.02 (1.01, 1.03) | 0.003 |
| Preoperative SF-36 role emotional | 1.04 (1.01, 1.06) | <0.001 |
| Preoperative SF-36 mental health | 1.03 (1.00, 1.05) | <0.001 |
| Preoperative FACT physical well-being | 1.04 (1.00, 1.07) | <0.001 |
| Preoperative FACT social/family well-being | 1.01 (1.01, 1.02) | 0.010 |
| Preoperative FACT functional well-being | 1.03 (1.01, 1.06) | <0.001 |
| Preoperative FACT emotional well-being | 1.03 (1.01, 1.05) | <0.001 |
| Preoperative FACT additional concerns | 1.02 (1.00, 1.04) | <0.001 |
| Preoperative FACT-G total score | 1.07 (1.01, 1.14) | <0.001 |
| Preoperative FACT-Hep total score | 1.10 (1.02, 1.19) | <0.001 |
| Education | 1.10 (1.02, 1.18) | 0.012 |
| Body mass index | 1.02 (1.01, 1.04) | 0.002 |
| Charlson co-morbidity index | 0.83 (0.70, 0.99) | 0.040 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, C.-C.; Lee, K.-T.; Wang, J.-J.; Sun, D.-P.; Lee, H.-H.; Huang, C.-C.; Shi, H.-Y. Preoperative Health-Related Quality of Life Predicts Minimal Clinically Important Difference and Survival after Surgical Resection of Hepatocellular Carcinoma. J. Clin. Med. 2019, 8, 576. https://doi.org/10.3390/jcm8050576
Chiu C-C, Lee K-T, Wang J-J, Sun D-P, Lee H-H, Huang C-C, Shi H-Y. Preoperative Health-Related Quality of Life Predicts Minimal Clinically Important Difference and Survival after Surgical Resection of Hepatocellular Carcinoma. Journal of Clinical Medicine. 2019; 8(5):576. https://doi.org/10.3390/jcm8050576
Chicago/Turabian StyleChiu, Chong-Chi, King-Teh Lee, Jhi-Joung Wang, Ding-Ping Sun, Hao-Hsien Lee, Chien-Cheng Huang, and Hon-Yi Shi. 2019. "Preoperative Health-Related Quality of Life Predicts Minimal Clinically Important Difference and Survival after Surgical Resection of Hepatocellular Carcinoma" Journal of Clinical Medicine 8, no. 5: 576. https://doi.org/10.3390/jcm8050576