1. Introduction
Arrhythmia is a potentially life-threatening condition; it is defined as an irregular heartbeat or abnormal heart rhythm [
1]. Cardiac arrhythmia occurs in 11%–58% of the population, of which the most common type is atrial fibrillation [
2]. The major determinant of prevalence of arrhythmia is aging of the population [
2]. The etiology of cardiac arrhythmia includes abnormalities of the sinoatrial node, atrioventricular node, His-Purkinje system, myocardial remodeling, ionic imbalances, dysfunctional ion channels, and clinical presentations range from asymptomatic to sudden cardiac death [
3]. The mechanism of normal aging for arrhythmia is associated with the apoptosis and subsequent fibrofatty infiltration of the myocardial cells, which affects the neighboring conduction system [
4]. In addition to normal aging, studies have reported that coronary artery disease [
5], air pollution [
6], and alteration of the autonomic nervous system [
7] (ANS), age, gender, smoking, and races [
8], are risk markers of cardiac arrhythmia.
Franciosi et al. found that alterations in levels of neuronal growth factors during ANS development can lead to cardiac arrhythmias [
9]. Furthermore, Shen et al. determined that the ANS mechanism involved in triggering arrhythmia could be arrhythmogenic or antiarrhythmic: sympathetic activity and parasympathetic activity are triggers for atrial fibrillation whereas sympathetic activation and parasympathetic activation are arrhythmogenic and antiarrhythmic for ventricular fibrillation, respectively [
10].
The cervical spine harbors the cervical ganglia, which are the paravertebral ganglia of the sympathetic nervous system [
10]. The sympathetic nerves of the right heart are predominantly from the right middle cervical ganglion and the sympathetic nerves of left heart is predominantly from the left middle cervical ganglion, while the remaining sympathetic innervation is from satellite ganglion, the distribution of which is more prominent in the left heart than right heart [
10]. Cardiac parasympathetic innervation is through the vagusnerve [
10].
Previous research into the effects of ANS alterations has focused on triggers of sympathetic neuronal activity and blocking agents, and most of these studies have used animal models [
11,
12,
13]. Degenerative disease of cervical spine, naming cervical spondylosis (CS), might cause compression of spinal canal and irritation of ANS [
14]. Cervical spondylosis is prevalent among people older than 50 years [
14]. Most common clinical signs of CS are pain and motor function impairment [
14]. Peng et al. have described two cases of cervical spondylosis that had secondary hypertension and successfully treated the two cases with anterior cervical discectomy and fusion [
15]. To our knowledge, no clinical research has investigated whether spondylosis of the spine is associated with a risk of arrhythmia, and the association between CS and arrhythmia is thus unknown.
This study, therefore, used the National Health Insurance Research Database (NHIRD) [
15], which represents the Taiwanese population, to test the hypothesis that patients with CS have an increased risk of arrhythmia.
3. Results
The case group comprised 22,236 subjects with CS and the control group comprised 22,236 subjects (
Table 1).
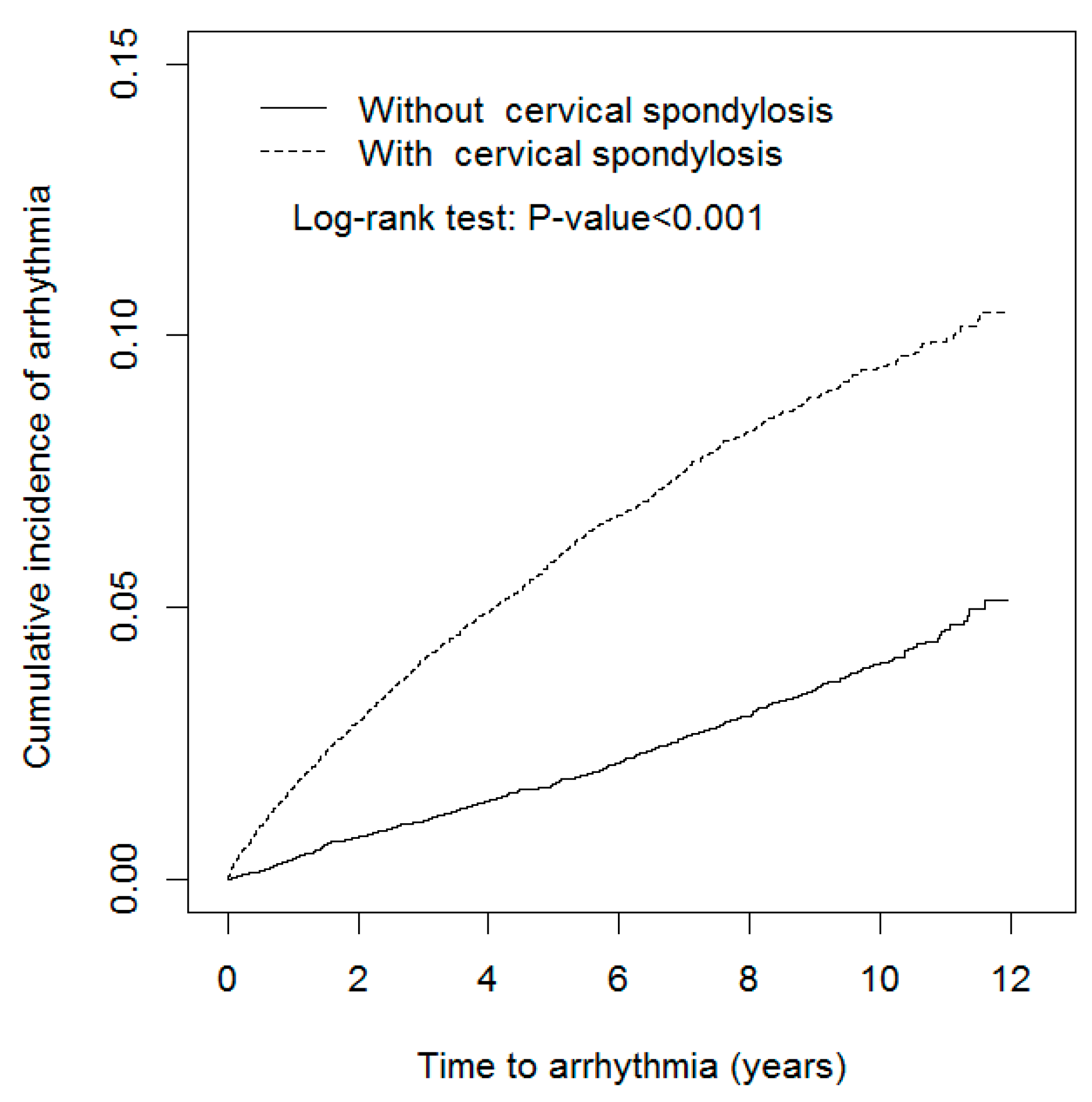
There were more women and younger individuals (mean age of 54.3 (SD 13.3) years) in the case group than in the control group (mean age of 54.4 (SD 13.4) years). The mean frequency of medical visits was higher in the case group (15.8 ± 13.9 medical visits per year) than in the control group (15.1 ± 13.9 medical visits per year). Nearly 50% of subjects worked in a white-collar profession (51.4% vs. 51.3% in the case and control groups, respectively) and most individuals lived in an urbanized area (63.4% vs. 63.6% in the case and control groups, respectively). The major comorbidity in both cohorts was hypertension (38.1% vs. 38.6%), followed by hyperlipidemia (30.5% vs. 31.0%), and COPD (13.7% vs. 13.9%). The percentage of patients taking NSAIDs was 34.3% vs. 34.4%. The mean follow-up period was shorter in the case group (5.86 ± 3.26 years) than in the control group (6.18 ± 3.15 years). The Kaplan–Meier plot revealed that the cumulative incidence of arrhythmia in the case group was approximately 5.44% higher than in the control group (log-rank test
p < 0.001,
Figure 1) after the 12-year follow-up.
The overall incidence density rates of arrhythmia were 11.1 and 3.91 per 1,000 person-years in the case and control groups, respectively (
Table 2). The adjusted HRs (aHRs) of arrhythmia were 3.10 (95% CI = 2.80–3.42) in the case group relative to the control group, after controlling for age, sex, frequency of medical visits/per year, occupation, urbanization level, comorbidity of diabetes, hypertension, hyperlipidemia, CAD, stroke, CKD or ESRD, COPD, cancer, CHF, and medications of NSAID, beta blocker, propranolol, carvedilol, and bisoprolol. The risk of arrhythmia increased with age, with aHRs of 1.86 (95% CI = 1.64–2.11) and 2.68 (95% CI = 2.33–3.10) for the two older age groups. Compared with patients who worked in a white-collar profession, those with a blue-collar profession (aHR = 1.11, 95% CI = 1.00–1.23) and those working in other professions (aHR = 1.22, 95% CI = 1.07–1.39) had a higher risk of developing arrhythmia. The risk of developing arrhythmia was higher for individuals with hypertension (aHR = 1.75, 95% CI = 1.55–1.97), hyperlipidemia (aHR = 1.44, 95% CI = 1.30–1.59), CAD (aHR = 1.94, 95% CI = 1.74–2.17), COPD (aHR = 1.42, 95% CI = 1.27–1.60), and CHF (aHR = 1.24, 95%CI = 1.00–1.54).
The incidence densities of arrhythmia, as stratified by sex, age, occupation category, urbanization level, and comorbidities, were all higher in the case group than in the control group (
Table 3). The aHRs of arrhythmia for the case group, as compared with the control group, were all significant for women, highest in patients aged ≤49 years, urbanization level 3, and patients with no comorbidities.
Further analysis revealed overall incidence density rates of arrhythmia of 10.8 and 11.5 per 1000 person-years for those in the case group without myelopathy and those in the case group with myelopathy, respectively, with aHRs of 2.87 (95% CI = 2.58–3.20) and 3.53 (95% CI = 3.13–3.97), respectively (
Table 4).
Table 5 shows the relative risk of an individual in the case group developing arrhythmia after receiving treatment and not receiving treatment, respectively. Compared with the control group, participants in the case group with no neurological signs had a 3.32-fold increased risk of developing arrhythmia (95% CI = 3.01–3.68), whereas those receiving rehabilitation and with neurological signs receiving spinal decompression had a 1.94-fold and 1.84-fold increased risk of arrhythmia, respectively. Compared to patients in the case group with no neurological signs, those in the case group receiving rehabilitation had a 0.61-fold decreased risk of developing arrhythmia (95% CI = 0.48–0.78), whereas those with neurological signs receiving spinal decompression exhibited had a 0.58-fold decreased risk of developing arrhythmia (95% CI = 0.42–0.79).
Table 6 shows the relative risks for different types of arrhythmias in the case group. There were 252 events of atrial fibrillation in CS cohort and 127 events of atrial fibrillation in non-CS cohort, 33 events of ventricular tachycardia in CS cohort and 12 events of ventricular tachycardia in non-CS cohort, 78 events of supraventricular tachycardia in CS cohort and 35 events of supraventricular tachycardia in non-CS cohort. Compared with the control group, subjects in the case group had 2.22-fold increased risk of developing atrial fibrillation (95% CI = 1.79–2.76), a 3.19-fold increased risk of developing ventricular tachycardia (95% CI = 1. 64–6.20), and a 2.54-fold increased risk of developing supraventricular tachycardia (95% CI = 1.70–3.79).
4. Discussion
The present study reveals that CS is associated with a 3.10-fold increase of arrhythmia risk compared to patients without cervical spondylosis, especially atrial fibrillation, ventricular and supraventricular tachycardia. ANS stimulation could explain the related mechanism of this finding. Clinical evidence had shown that CS can cause sympathetic nerve irritation and associated sympathetic symptoms [
27], and instability at the C4–C5 intervertebral space is the most-common type causing sympathetic symptoms [
28]. Recognized sympathetic symptoms of CS are vertigo, dizziness, tinnitus, headache, and palpitation [
29]. Previous electrophysiological studies have demonstrated that sympathetic activation has a proarrhythmic effect in enhancing automaticity, triggering re-entry, and reducing the threshold of refractoriness [
29,
30,
31]. Such studies have shown that an imbalance of the autonomic nervous system and stimulation of the sympathetic nervous system can trigger atrial fibrillation [
32], ventricular tachycardia [
33], and ventricular fibrillation [
34]. Such findings are thus similar to those of our study: CS is associated with a higher risk of developing atrial fibrillation, atrial flutter, and ventricular tachycardia. We supposed that a possible mechanism would be that cervical region trauma influences spinal sympathetic neurons because sympathetic control of heart originates from T1-5, thus the parasympathetic tone is unopposed. The increased vagal tone would be associated with atrial fibrillation. A reason for the insignificant risk of developing ventricular fibrillation shown in our study is possibly related to low event rate which only one event occurred in the study cohort and comparison cohort individually.
Another possible pathway is regional hyper innervation of the sympathetic nerves of the heart [
35]. Although an increased nerve fiber density, and thus increased arrhythmia susceptibility, are most commonly seen in heart failure [
36] and acute myocardial infarction [
37], injury of the spinal cord is also one of the causes of hyper innervation [
38]. We therefore hypothesize that CS could contribute to the possible irritation and injury of the spinal cord, which therefore causes hyper innervation of the heart. Electrophysiological evidence is therefore required to clarify the possible link between CS and hyper innervation of the sympathetic nerves. Our data also showed that beta-blockers bisoprolol and carvedilol was associated with lower risk of arrhythmia, while propranolol is associated with higher risk of arrythmia. Although these medications were all beta-receptor antagonists, we suppose that the difference would be that propranolol is widely used for anxiety beyond the range of cardiovascular system and its duration is short-acting [
39,
40]. Bisoprolol is a selective beta-1 receptor antagonist and carvedilol is a comprehensive beta (1)-, beta (2)-, and alpha (1)-adrenoreceptor blocker [
41,
42]. The lower risk of arrhythmia in users of bisoprolol and carvedilol might strengthen our supposed commonality mechanism that higher risk of arrhythmia cervical spondylosis patients is associated with hyperactive sympathetic tones in cervical spondylosis patients.
One interesting finding of this study is that CS patients who had received rehabilitation or surgical decompression had a lower risk of arrhythmia events compared with who had mild cervical spondylosis with no signs. A possible reason for this is that patients receiving surgical decompression were in relatively better physical health than those not receiving such an intervention; however, this is unlikely in this study as the prevalence of all possible comorbidities were comparable between the case group and the control group. Nevertheless, this study provides evidence supporting the use of rehabilitation and surgical decompression to protect against future arrhythmias, and the use of a detailed animal model is suggested to clarify the decompression effect on the cervical spinal cord with respect to arrhythmia.
This study has several limitations: first, information relating to smoking habits, alcohol consumption, caffeine intake, body mass index, and physical activity were unavailable from the NHIRD. Second, several confounders that could also cause arrhythmia, such as heart surgery, thoracic surgery, congenital heart anomaly, valvar heart disease, prolongation of QT interval, and thyroid disease were not considered in this study; this structural heart disease would be arrhythmogenic [
43,
44]. However, they were not frequently observed in people with cervical spondylosis, then this is less of a concern. Several other ECG markers of arrhythmia risk such as
P wave duration, QRS duration and fragmentation, ST segment depression and elevation, Tpeak-Tend interval or premature ventricular contractions were also insufficient. Though other major comorbidities that could predispose to the development of arrhythmia were adjusted and matched to alleviate the bias, their associated therapy might influence arrhythmia risk were not considered. Third, the occurrence of arrhythmia was based on the diagnostic code registered in NHIRD; therefore, validation of an accurate arrhythmia diagnosis is lacking. Fourth, CS is common in the population and is likely to be underdiagnosed; therefore, a bias for CS prevalence is present in our case and control groups. Nevertheless, this bias is common in population-based studies, and we have included intervention procedures used for CS, such as surgical decompression and rehabilitation, to reinforce our findings. Furthermore, this study is retrospective-based and if subjects in the control group had undiagnosed CS, the risk of arrhythmia would therefore be underestimated in the case group, which thus strengthens the findings of this study: the risk of arrhythmia is increased in the CS population. Fifth, although we have considered occupation, we have no information about night shift conditions of each participant. Night shift is reported to be associated with prolong QT and Tpeak-Tend intervals, which increases ventricular arrhythmia risk [
45]. Finally, the different types of arrhythmia, such as atrial fibrillation, atrioventricular node block, QT prolongation, and sick sinus syndrome, were not differentiated in this study. Nevertheless, because the objective of this study was to evaluate the association between CS and the risk of developing arrhythmia, the limitations presented here do not affect the value of the findings.
In summary, this study demonstrated that CS is associated with an increased risk of developing arrhythmia. As arrhythmia is linked to the risk of sudden death and strokes, this study should prompt clinical awareness of the higher risk of arrhythmia in patients with CS. The finding of this study might arouse the alertness of clinicians that CS is associated with arrhythmia, especially those who had symptoms of myelopathy. Thus, electrocardiogram would be needed in those CS presented with sympathetic symptoms or those who had several identified risk markers of arrhythmia. Primary prevention with anti-coagulations or anti-arrhythmic medications for fatal arrhythmia or ischemia stroke would be beneficial. This study has several inherent limitations; thus, large prospective studies are required to examine the direct causal relationship between CS and the occurrence of arrhythmia.





{kind=link}