The Effect of Special Medical Examination for Night Shift Workers and Follow-Up Management Against Hypertension

 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
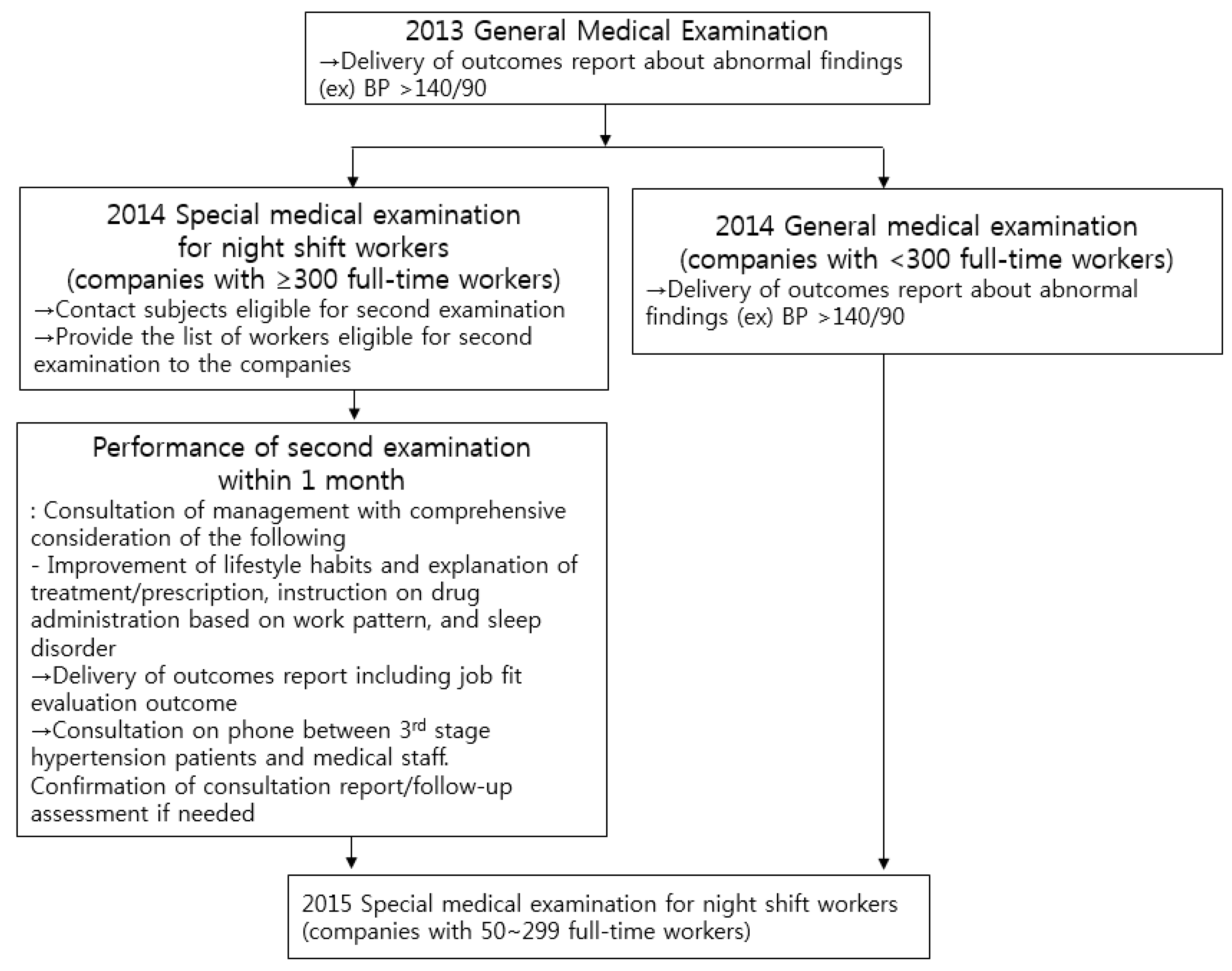
3.1. Follow-Up Management of the Subjects with Hypertension
3.2. Characteristics of Subjects with Hypertension in the Proper Management Group
3.3. Characteristics of the Subjects in Proper Management Group Based on the Size of Companies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Statistics Korea. 2017 Statistics on Causes of Mortalities; Statistics Korea: Daejeon, Korea, 2017. Available online: http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B34E01&conn_path=I2 (accessed on 21 January 2019). (In Korean)
- Kim, C.H.; Han, J.S. Hypertension and sodium intake. Korean J. Fam. Med. 2006, 27, 517–522. [Google Scholar]
- Yeom, J.H.; Sim, C.S.; Lee, J.; Yun, S.H.; Park, S.J.; Yoo, C.I.; Sung, J.H. Effect of shift work on hypertension: Cross sectional study. Ann. Occup. Environ. Med. 2017, 29, 11. [Google Scholar] [CrossRef] [PubMed]
- Costa, G. Shift work and occupational medicine: An overview. Occup. Med. 2003, 53, 83–88. [Google Scholar] [CrossRef]
- Knutsson, A. Methodological aspects of shift-work research. Chronobiol. Int. 2004, 21, 1037–1047. [Google Scholar] [CrossRef] [PubMed]
- Young, M.E. The circadian clock within the heart: Potential influence on myocardial gene expression, metabolism, and function. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H1–H16. [Google Scholar] [CrossRef] [PubMed]
- Knutsson, A. Health disorders of shift workers. Occup. Med. 2003, 53, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Government Legislation. Article 43 of Occupational Safety and Health Act. Available online: http://law.go.kr/engLsSc.do?tabMenuId=tab45&query=occupational%20safety%20and%20health%20act (accessed on 27 February 2019).
- Cho, B.; Lee, C.M. Current state of national health examination system in Korea. J. Korean Med. Assoc. 2011, 54, 666–669. [Google Scholar] [CrossRef]
- Kim, J. Management of drinking patients in primary care. Korean J. Fam. Pract. 2012, 2, 280–288. [Google Scholar]
- Korean Society for Preventive Medicine. Preventive Medicine and Public Health; GyeChuk Printing: Seoul, Korea, 2011; pp. 757–758. [Google Scholar]
- Noh, M.S. International Comparisons of Salary Difference Based on the Size of Companies and Its Implications, in KDI Focus; Korea Small Business Institute: Seoul, Korea, 2017. [Google Scholar]
- Ha, Y.M.; Park, H.J. Effect of job insecurity on job related depression and anxiety: Large- and small-sized company employees. Korean J. Occup. Health Nurs. 2016, 25, 329–339. [Google Scholar] [CrossRef]
- Lang, J.; Cluff, L.; Rineer, J.; Brown, D.; Jones-Jack, N. Building capacity for workplace health promotion: Findings from the Work@Health® Train-the-Trainer program. Health Promot. Prac. 2017, 18, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Federal Association of Company Health Insurance Funds European Information Centre. Report on the Current Status of Workplace Health Promotion in Small and Medium-Sized Enterprises; Federal Association of Company Health Insurance Funds European Information Centre: Essen, Germany, 2001. [Google Scholar]
- Gwon, B.H. Strategy for workers’ health protection in small sized company. Ind. Health 2016, 2335, 38–43. [Google Scholar]
- Paulsen, M.S.; Andersen, M.; Thomsen, J.L.; Schroll, H.; Larsen, P.V.; Lykkegaard, J.; Jacobsen, I.A.; Larsen, M.L.; Christensen, B.; Sondergaard, J. Multimorbidity and blood pressure control in 37,651 hypertensive patients from Danish general practice. J. Am. Heart Assoc. 2012, 2, e004531. [Google Scholar] [PubMed]
- Lee, H.M.; Kim, Y.M.; Lee, C.H.; Shin, J.H.; Kim, M.K.; Choi, B.Y. Awareness, treatment and control of hypertension and related factors in the jurisdictional areas of primary health care posts in a rural community of Korea. J. Prev. Med. Public Health 2011, 44, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Tada, Y.; Kawano, Y.; Maeda, I.; Yoshizaki, T.; Sunami, A.; Yokoyama, Y.; Matsumoto, H.; Hida, A.; Komatsu, T.; Togo, F. Association of body mass index with lifestyle and rotating shift work in Japanese female nurses. Obesity 2014, 22, 2489–2493. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Son, K.H.; Park, H.Y.; Choi, D.J.; Yoon, C.H.; Lee, H.Y.; Cho, E.Y.; Cho, M.C. Association between shift work and obesity among female nurses: Korean Nurses’ Survey. BMC Public Health 2013, 13, 1204. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.J.; Kim, K.; Kim, S.Y.; Kim, J.H.; Suh, C.; Son, B.C.; Lee, C.K.; Choi, J. Effects of shift work on abdominal obesity among 20–39-year-old female nurses: A 5-year retrospective longitudinal study. Ann. Occup. Environ. Med. 2016, 28, 69. [Google Scholar] [CrossRef] [PubMed]
- Zhao, I.; Bogossian, F.; Turner, C. A cross-sectional analysis of the association between night-only or rotating shift work and overweight/obesity among female nurses and midwives. J. Occup. Environ. Med. 2012, 54, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Fujino, Y.; Nakamura, T.; Kunimoto, M.; Tabata, H.; Tsuchiya, T.; Kadowaki, K.; Odoi, H.; Oyama, I.; Matsuda, S. An industry-based cohort study of the association between weight gain and hypertension risk among rotating shift workers. J. Occup. Environ. Med. 2013, 55, 1041–1045. [Google Scholar] [CrossRef] [PubMed]
- Animut, Y.; Assefa, A.T.; Lemma, D.G. Blood pressure control status and associated factors among adult hypertensive patients on outpatient follow-up at University of Gondar Referral Hospital, northwest Ethiopia: A retrospective follow-up study. Integr. Blood Press. Control 2018, 11, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Foguet-Boreu, Q.; Violan, C.; Lopez Jimenez, T.; Pons-Vigues, M.; Rodriguez-Blanco, T.; Valderas, J.M.; Guisado Clavero, M.; Pujol-Ribera, E. Pharmacological control of diabetes and hypertension comorbidity in the elderly: A study of “real world” data. Prim. Care Diabetes 2017, 11, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Xu, X.; Yan, J.; Yu, W.; Tang, X.; Wu, H.; Parkin, C.L. Analysis on associated factors of uncontrolled hypertension among elderly hypertensive patients in Southern China: A community-based, cross-sectional survey. BMC Public Health 2014, 14, 903. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.L.; Cheung, B.M.; Man, Y.B.; Lau, C.P.; Lam, K.S. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999–2004. Hypertension 2007, 49, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.D.; Tsang, P.P.; Li, W.T.; Wang, H.H.; Liu, K.Q.; Griffiths, S.M.; Wong, M.C. Determinants of medication adherence and blood pressure control among hypertensive patients in Hong Kong: A cross-sectional study. Int. J. Cardiol. 2015, 182, 250–257. [Google Scholar] [CrossRef] [PubMed]
- The Korean Society Hypertension (KSH); Hypertension Epidemiology Research Working Group; Kim, H.C.; Cho, M.-C. Korea hypertension fact sheet 2018. Clin. Hyprtens. 2018, 24, 13. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Maintained | Improved | Not Improved | |
|---|---|---|---|
| Drinking | - | Adequate level on the second-year survey | Excessive drinking on the second-year survey |
| Exercise | - | Adequate level on the second-year survey | Lacking exercise on the second-year survey |
| Smoking | - | Non-smoker or previous smoker on the second-year survey | Current smoker on the second-year survey |
| Comorbidities | |||
| Diabetes | Not diagnosed with diabetes on either first- or second-year examination | Second examination outcomes in the first year showing fasting blood sugar level of ≥126 mg/dL or HbA1c level of ≥6.5%, but blood test in the second-year examination showing fasting blood sugar level of <126 mg/dL or HbA1c level of <6.5% or the patient was currently under anti-diabetic medications | Second examination outcomes in both first and second years showing fasting blood sugar level of ≥126 mg/dL or HbA1c level of ≥6.5% |
| Dyslipidemia | Not diagnosed with dyslipidemia on either first- or second-year examination (blood test) | Second examination outcomes (blood test) in the first year showing LDL cholesterol level of ≥160 mg/dL or triglyceride level of ≥500 mg/dL or total cholesterol level of ≥240 mg/dL, but blood test in the second year showing the levels below the standard of dyslipidemia or the patient currently under treatment improved | Second examination outcomes on both first- and second-years showing LDL cholesterol level of ≥160 mg/dL or triglyceride level of ≥500 mg/dL or total cholesterol level of ≥240 mg/dL |
| BMI * | Normal BMI on both first and second years (<23) | BMI in the second year decreased compared with BMI in the first-year examination | BMI in the second year increased compared with BMI in the first-year examination |
| Waist circumference * | Normal waist circumference on both first- and second-year examinations (<90 cm for men and <85 cm for women) | Waist circumference measured in the second year decreased compared with waist circumference measured in the first-year examination | Waist circumference measured in the second-year examination increased compared with waist circumference measured in the first-year examination |
| Improper, N (%) (n = 567 (27.4%)) | Proper, N (%) (n = 1503 (72.6%)) | p-Value * | |
|---|---|---|---|
| Age * | <0.0001 | ||
| ≤20 s | 63 (11.1) | 125 (8.3) | |
| 30 s | 198 (34.9) | 360 (24.0) | |
| 40 s | 174 (30.7) | 507 (33.7) | |
| ≥50 s | 132 (23.3) | 511 (34.0) | |
| Sex * | 0.0156 | ||
| Male | 532 (93.8) | 1360 (90.5) | |
| Female | 35 (6.2) | 143 (9.5) | |
| Size of companies † | 0.0004 | ||
| ≥300 | 278 (49.0) | 867 (57.7) | |
| 50–299 | 289 (51.0) | 636 (42.3) | |
| Work period | 0.0093 | ||
| <2 years | 68 (12.1) | 129 (8.7) | |
| 2–5 years | 167 (29.7) | 420 (28.3) | |
| 5–12 years | 144 (25.6) | 348 (23.4) | |
| ≥12 years | 183 (32.6) | 589 (39.6) | |
| Exercising | 0.4766 | ||
| Improved | 307 (54.1) | 840 (55.9) | |
| Not improved | 260 (45.9) | 663 (44.1) | |
| Drinking habit | 0.5237 | ||
| Improved | 365 (64.4) | 990 (65.9) | |
| Not improved | 202 (35.6) | 513 (34.1) | |
| Smoking habit * | 0.0179 | ||
| Improved | 341 (60.1) | 988 (65.7) | |
| Not improved | 226 (39.9) | 515 (34.3) | |
| Diabetes | <0.0001 | ||
| Maintained | 552 (97.4) | 1399 (93.1) | |
| Improved | 7 (1.2) | 94 (6.3) | |
| Not improved | 8 (1.4) | 10 (0.7) | |
| Dyslipidemia | <0.0001 | ||
| Maintained | 561 (98.9) | 1428 (95.0) | |
| Improved | 3 (0.5) | 67 (4.5) | |
| Not improved | 3 (0.5) | 8 (0.5) | |
| BMI * | <0.0001 | ||
| Normal | 58 (10.2) | 252 (16.8) | |
| Improved | 186 (32.8) | 563 (37.5) | |
| Maintained | 48 (8.5) | 102 (6.8) | |
| Not improved | 275 (48.5) | 586 (39.0) | |
| Waist circumference | <0.0001 | ||
| Normal | 252 (44.4) | 870 (57.9) | |
| Improved | 125 (22.1) | 280 (18.6) | |
| Maintained | 37 (6.5) | 64(4.3) | |
| Not improved | 153 (27.0) | 289(19.2) |
| Variables | Before Adjustment | * After Adjustment | |||
|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | ||
| Age | |||||
| ≤20 s | 1.00 | 1.00 | |||
| 30 s | 0.92 | 0.64–1.30 | 0.82 | 0.56–1.19 | |
| 40 s | 1.47 | 1.03–2.08 | 1.13 | 0.76–1.67 | |
| ≥50 s | 1.95 | 1.36–2.79 | 1.44 | 0.96–2.15 | |
| Sex | |||||
| Male | 1.00 | 1.00 | |||
| Female | 1.60 | 1.10–2.38 | 1.34 | 0.90–2.05 | |
| Work period | |||||
| 2 years | 1.00 | 1.00 | |||
| 5 years | 1.33 | 0.94–1.87 | 1.30 | 0.90–1.86 | |
| 12 years | 1.27 | 0.89–1.81 | 1.25 | 0.85–1.81 | |
| 12 years | 1.70 | 1.21–2.37 | 1.36 | 0.93–1.96 | |
| Size of companies † | |||||
| ≥300 | 1.00 | 1.00 | |||
| 50–299 | 0.71 | 0.58–0.86 | 0.68 | 0.55–0.83 | |
| Exercising | |||||
| Not improved | 1.00 | 1.00 | |||
| Improved | 1.07 | 0.88–1.30 | 1.02 | 0.83–1.25 | |
| Drinking | |||||
| Not improved | 1.00 | 1.00 | |||
| Improved | 1.07 | 0.87–1.31 | 0.97 | 0.78–1.21 | |
| Smoking | |||||
| Not improved | 1.00 | 1.00 | |||
| Improved | 1.27 | 1.04–1.55 | 1.04 | 0.84–1.30 | |
| Diabetes | |||||
| Not improved | 1.00 | 1.00 | |||
| Improved | 10.74 | 3.25–37.32 | 4.55 | 2.21–11.03 | |
| Maintained | 2.03 | 0.77–5.17 | 0.52 | 0.19–1.43 | |
| Dyslipidemia | |||||
| Not improved | 1.00 | 1.00 | |||
| Improved | 8.37 | 1.36–52.65 | 6.97 | 2.54–28.86 | |
| Maintained | 0.96 | 0.21–3.31 | 0.98 | 0.26–4.69 | |
| BMI | |||||
| Not improved | 1.00 | 1.00 | |||
| Maintained | 1.00 | 0.69–1.46 | 0.89 | 0.60–1.32 | |
| Improved | 1.42 | 1.14–1.77 | 1.35 | 1.06–1.72 | |
| Maintained normal | 2.04 | 1.49–2.83 | 1.48 | 1.04–2.12 | |
| Waist circumference | |||||
| Not improved | 1.00 | 1.00 | |||
| Maintained | 0.92 | 0.59–1.45 | 0.84 | 0.52–1.34 | |
| Improved | 1.19 | 0.89–1.58 | 1.10 | 0.80–1.52 | |
| Maintained normal | 1.83 | 1.44–2.32 | 1.61 | 1.23–2.12 | |
| ≥300 (N = 1145) | 50–299 (N = 925) | |||
|---|---|---|---|---|
| Unadjusted | Adjusted * | Unadjusted | Adjusted * | |
| Age | ||||
| ≤20 s | 1.00 | 1.00 | 1.00 | 1.00 |
| 30 s | 1.16 (0.70–1.89) | 1.22 (0.73–2.00) | 0.63 (0.38–1.04) | 0.56 (0.33–0.93) |
| 40 s | 1.39 (0.84–2.25) | 1.33 (0.80–2.19) | 1.47 (0.88–2.42) | 1.24 (0.73–2.09) |
| ≥50 s | 1.55 (0.92–2.59) | 1.46 (0.85–2.50) | 2.45 (1.48–4.02) | 2.04 (1.19–3.47) |
| Sex | ||||
| Males | 1.00 | 1.00 | 1.00 | 1.00 |
| Females | 1.18 (0.72–1.99) | 1.11 (0.67–1.94) | 2.31 (1.32–4.35) | 1.87 (1.02–3.65) |
| Work period | ||||
| <2 years | 1 | 1 | 1 | 1 |
| 2–5 years | 1.54 (0.85–2.73) | 1.58 (0.85–2.86) | 1.09 (0.70–1.67) | 1.21 (0.76–1.92) |
| 5–12 years | 1.03 (0.57–1.81) | 1.01 (0.54–1.83) | 1.45 (0.91–2.32) | 1.65 (0.99–2.76) |
| ≥12 years | 1.58 (0.89–2.73) | 1.43 (0.77–2.57) | 1.54 (0.99–2.41) | 1.37 (0.84–2.24) |
| Exercising | ||||
| Not improved | 1.00 | 1.00 | 1.00 | 1.00 |
| Improved | 1.06 (0.81–1.39) | 1.02 (0.77–1.35) | 1.09 (0.82–1.44) | 0.97 (0.72–1.31) |
| Drinking | ||||
| Not improved | 1.00 | 1.00 | 1.00 | 1.00 |
| Improved | 0.90 (0.68–1.19) | 0.81 (0.61–1.08) | 1.40 (1.04–1.89) | 1.15 (0.84–1.58) |
| Smoking | ||||
| Not improved | 1.00 | 1.00 | 1.00 | 1.00 |
| Improved | 1.22 (0.92–1.61) | 1.17 (0.87–1.58) | 1.29 (0.97–1.71) | 0.90 (0.65–1.24) |
| Diabetes | ||||
| Not improved | 1.00 | 1.00 | 1.00 | 1.00 |
| Improved | <0.001(7.85)) | 3.62(1.25–15.37) | 22.80(5.41–116.02) | 5.16 (2.02–17.49) |
| Maintained normal | <0.001(1.41) | >999.999(0.48) | 3.32(1.10–11.06) | 0.35 (0.10–1.14) |
| Dyslipidemia | ||||
| Not improved | 1.00 | 1.00 | 1.00 | 1.00 |
| Improved | 6.67 (0.24–184.72) | 13.35(2.83–238.69) | 13.50 (1.16–189.52) | 3.90 (1.09–24.96) |
| Maintained normal | 0.50 (0.03–2.92) | 1.94 (0.31–37.42) | 2.13 (0.25–17.82) | 0.62 (0.07–5.70) |
| BMI | ||||
| Not improved | 1.00 | 1.00 | 1.00 | 1.00 |
| Maintained | 0.93 (0.56–1.58) | 0.85 (0.50–1.47) | 1.09 (0.64–1.88) | 0.94 (0.54–1.68) |
| Improved | 1.35 (1.00–1.83) | 1.37 (0.99–1.91) | 1.48 (1.08–2.04) | 1.33 (0.93–1.91) |
| Maintained normal | 2.07 (1.32–3.35) | 1.57 (0.96–2.64) | 2.06 (1.34–3.25) | 1.48 (0.91–2.46) |
| Waist circumference | ||||
| Not improved | 1.00 | 1.00 | 1.00 | 1.00 |
| Maintained | 0.85 (0.47–1.60) | 0.85 (0.46–1.61) | 1.02 (0.52–2.01) | 0.80 (0.39–1.63) |
| Improved | 0.95 (0.64–1.43) | 0.85 (0.55–1.31) | 1.61 (1.06–2.44) | 1.48 (0.93–2.37) |
| Maintained normal | 1.73 (1.24–2.40) | 1.51 (1.05–2.16) | 2.05 (1.43–2.92) | 1.41 (0.93–2.11) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, W.S.; Lee, J.-W.; Lee, J.Y.; Kim, K.Y.; Myong, J.-P.; Lee, W.-C. The Effect of Special Medical Examination for Night Shift Workers and Follow-Up Management Against Hypertension. Int. J. Environ. Res. Public Health 2019, 16, 719. https://doi.org/10.3390/ijerph16050719
Choi WS, Lee J-W, Lee JY, Kim KY, Myong J-P, Lee W-C. The Effect of Special Medical Examination for Night Shift Workers and Follow-Up Management Against Hypertension. International Journal of Environmental Research and Public Health. 2019; 16(5):719. https://doi.org/10.3390/ijerph16050719
Chicago/Turabian StyleChoi, Won Seon, Ji-Won Lee, Jae Yong Lee, Kyeong Yeon Kim, Jun-Pyo Myong, and Won-Chul Lee. 2019. "The Effect of Special Medical Examination for Night Shift Workers and Follow-Up Management Against Hypertension" International Journal of Environmental Research and Public Health 16, no. 5: 719. https://doi.org/10.3390/ijerph16050719