1. Introduction
Infections with helminths (e.g.,
Ascaris lumbricoides,
Trichuris trichiura and hookworm) and intestinal protozoa (e.g.,
Cryptosporidium and
Giardia intestinalis) are global public health threats and are closely associated with poverty, unsafe water and inadequate sanitation and hygiene [
1]. More than one billion people worldwide are infected with one or more species of soil-transmitted helminths (STH), of which over 267 million pre-school children and over 568 million school children are considered at risk of morbidity, especially in less developed countries [
1,
2,
3]. STH infections fall within the grouping termed as neglected tropical diseases (NTDs), and nearly 70% of the global burden it causes occurs in Asia [
4,
5]. Infections can cause diarrhea, abdominal pain, malnutrition, physical and intellectual growth retardations [
1]. Cryptosporidiosis is a major cause of diarrheal disease in developing and developed countries, and epidemiological studies have shown that
Cryptosporidium is more prevalent in developing countries (5% or higher) than in developed countries (3% or less) [
6].
Cryptosporidium was identified to be the second only to rotavirus as a cause of moderate-to-severe diarrhea in children during the first two years of life [
7]. Infection with
Cryptosporidium can lead to self-limiting diarrhea in immunocompetent individuals but life-threatening and prolonged diarrhea in immunocompromised ones such as people infected with HIV [
8].
Cryptosporidium infection is also associated with malnutrition and growth deficits in children. The types of organisms, risk factors and routes of transmission of the three infectious diseases are different, but their transmission is related to poor sanitation conditions and sanitary practices (
Table 1) [
9].
Historically, infections of
A. lumbricoides and
T. trichiura, along with other intestinal helminth parasites, have been a major public health problem in China. There have been two national surveys of parasitic diseases conducted in China. The prevalence of infection was 47.0% for
A. lumbricoides and 18.8% for
T. trichiura in the first national survey of parasitic diseases (1988–1992), which dropped dramatically to 12.7% and 6.1% at the second national survey (2001–2004) [
10]. Although, the prevalence of STH infections continuously decreased according to national surveillance data,
A. lumbricoides and
T. trichiura infections remain high in several underdeveloped regions in China [
11,
12,
13,
14]. A review of South and Southeast Asia demonstrates that school children have higher infection risks of
A. lumbricoides (25%, 95% CI: 16–31%) and
T. trichiura (22%, 95% CI: 14–34%) than the general population [
15]. However,
Cryptosporidium infection had been largely neglected and few studies had been conducted in the Yi ethnicity in SW China. Similarly, there are few studies on the epidemiology of STH infections and risk factors for infection in primary school children. Studies of
A. lumbricoides,
T. trichiura and
Cryptosporidium in children are relevant to the control of these three infectious diseases because primary school children are an important reservoir of infection and at risk of morbidity. The aim of the present study was to assess the prevalence of infection for
A. lumbricoides,
T. trichiura and
Cryptosporidium, and associated risk factors among elementary school children in this region, to provide a scientific basis for the formulation of government health policies and the promotion of school health education to reduce the prevalence of the three parasitic diseases in school-age children.
4. Results
There were a total of 348 eligible participants in the study. After exclusion of participants who did not provide feces or complete the questionnaires, 321 (92.2%) participants were included in the analysis. Demographic data showed similar distributions for those included and not included in the analysis (
Table 2).
Table 3 shows the prevalence of
A. lumbricoides,
T. trichiura,
Cryptosporidium and coinfections by age group. The prevalence of infection was 10.0% (95% CI: 6.9–13.8%) for
A. lumbricoides, 25.2% (95% CI: 20.6–30.4%) for
T. trichiura and 2.4% (95% CI: 1.1–4.9%) for
Cryptosporidium. The prevalence of co-infection was 3.7% (95% CI: 1.9–6.4%) for
A. lumbricoides/
T. trichiura, 0.3% (95% CI: 0–1.7%) for
A. lumbricoides/
Cryptosporidium and 0.9% (95% CI: 0.2–2.7%) for
T. trichiura/
Cryptosporidium. No triple infection was found in our study. The prevalence of
A. lumbricoides infection differed among the age groups and was the lowest among children over 13 years of age (
p = 0.04), while
T. trichiura and
Cryptosporidium infections and all the co-infections were not significantly different among the age groups (
Table 3).
The characteristics of the participants are described in
Table 4. The mean age of participants was 12.6 years (SD: 2.0). Among 321 children recruited, 62.93% were male; 98.75% were Yi people; 89.10% lived on campus and had their three meals of week days at the school canteen. At homes of the 321 participants recruited, 85.98% of the drinking water came from mountain springs, 60% of household lavatories were simple, and 30% were triple compartment or biogas pools.
Table 5 and
Table 6 show the results of risk factors associated with
A. lumbricoides,
T. trichiura and
Cryptosporidium infections. Children from households using well or river water were at a greater risk of
A. lumbricoides infection (aOR = 2.67, 95% CI: 1.15–6.20). Having a household lavatory was negatively associated with
T. trichiura infection (aOR = 0.50, 95% CI: 0.30–0.84). Children having their three meals at the school canteen were at a lower risk of
Cryptosporidium infection (aOR = 0.06, 95% CI: 0.01–0.40). Similarly, living on campus was also a protective factor for
Cryptosporidium infection (cOR = 0.11, 95% CI: 0.03–0.46). Using spring water as water source was a protective factor for any intestinal infection (aOR = 0.52, 95% CI: 0.28–0.99).
5. Discussion
This study reported the prevalence of
A. lumbricoides,
T. trichiura and
Cryptosporidium infections in the elementary school children. The prevalence of
Cryptosporidium infections in our study (2.40%) was comparable to the provincial estimate (2.96%) in Sichuan Province, China [
15]. The prevalence of
A. lumbricoides infection (10.0%), was similar to the national prevalence (12.7%) of the second national important parasitic disease survey from 2001 to 2004, but was lower than those of Guizhou Province (42.0%) and Sichuan Province (27.7%) [
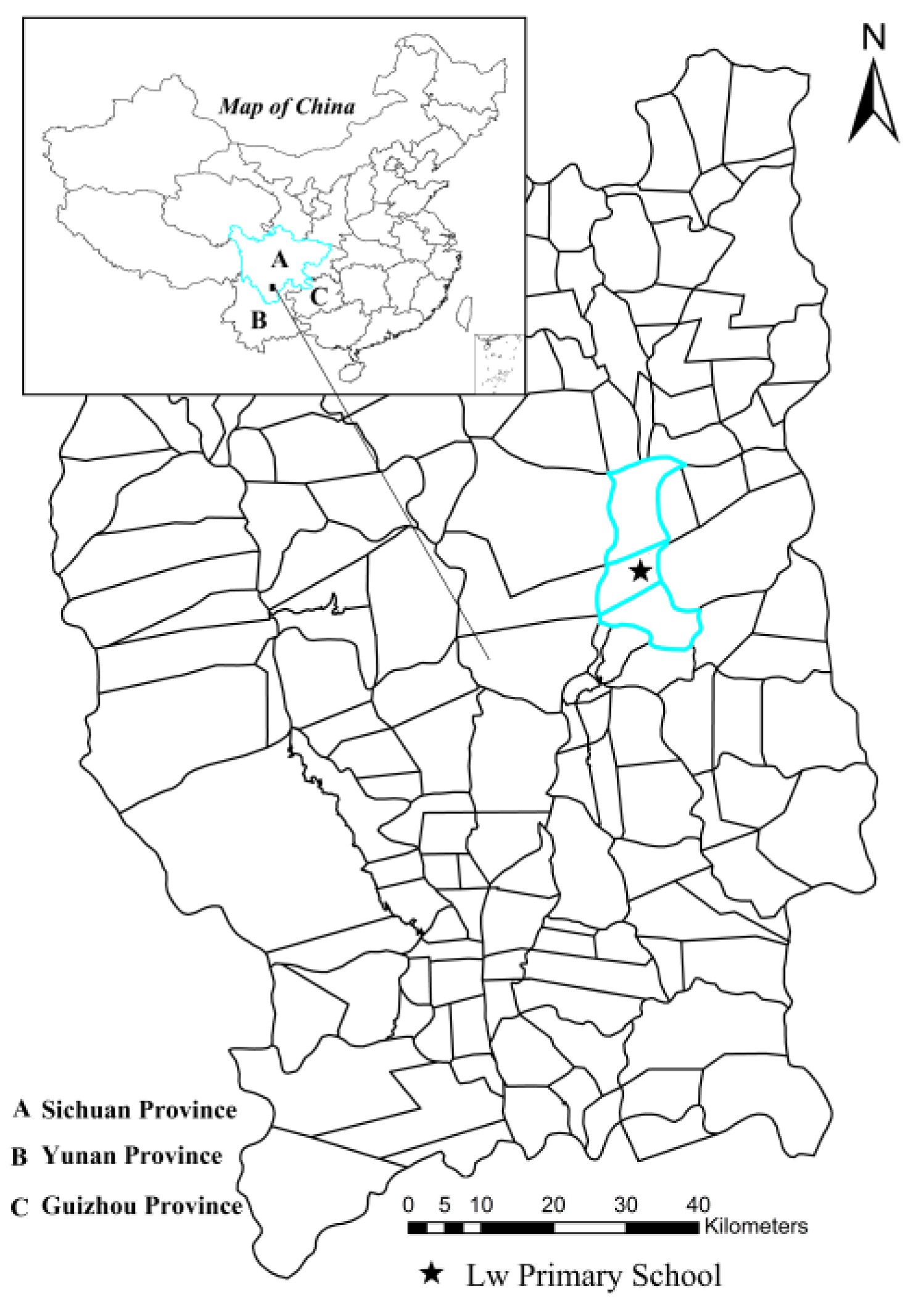
13]. Our study area is located in the southwestern of Sichuan Province, close to Yunnan and Guizhou Province (
Figure 1). The reduced prevalence of
A. lumbricoides infections may be related to the government’s deworming treatment of
A. lumbricoides in high-risk populations. A survey of school-age children in 2010 also showed a reduction in the prevalence of
A. lumbricoides infection in rural southwestern China [
18]. For
T. trichiura infection, the prevalence in our study (25.2%) was higher than both second national survey (4.6% in China Mainland) and the survey of school-age children in southwestern China in 2010 (14.3% in Guizhou Province, and 2.2% in Sichuan Province) [
13,
18]. According to the WHO report, the prevalence of STH infection in China was estimated to be less than 20% [
22]. The prevalence of
T. trichiura infections in the study area remained high. The main reason may be the unsatisfactory efficacy of currently recommended drugs against
T. trichiura infection, especially when they are not regularly taken [
23]. Poor hygiene, especially at home, may be another reason for the high prevalence of
T. trichiura infection. Most children in the school drank unboiled water (84.42%) and ate raw food without washing (86.60%). Water, food, soil and hands are easily contaminated by worm eggs in the case of inadequate sanitation facilities and feces management, unsafe water and poor hygiene practices [
24]. Therefore, improving access to adequate water, sanitation and hygiene (WASH) at the household level and in school is essential to prevent infections of
T. trichiura [
25]. In addition, the climatic factors in Liangshan Prefecture are within the plausible limits of STH transmission [
5]. As expected, the prevalence of
A. lumbricoides infection varied by age. However, the age patterns of
T. trichiura and
Cryptosporidium infections showed little variation, which probably reflected a combination of behavioral and socioeconomic factors [
26]. Indeed, older students had more opportunities to receive health education and knowledge about infection prevention. Interestingly, although most hygiene habits tended to improve with age in our study, older students were prone to eating raw food. This finding emphasized the importance of continuing and strengthening health education programs targeting school children to reduce the intensity of parasites and the attendant morbidity [
12].
A recent meta-analysis of the effects of water, sanitation, and hygiene (WASH) on STH infections reported that access to piped water and proper water treatment was associated with lower risks of
A. lumbricoides and
T. trichiura infections [
27]. Our study found that using river or well water was associated with an increased risk of
A. lumbricoides infection. In the study area, the main sources of drinking water in the study area were mountain springs (far from human living areas, piped after extensive precipitation and filtration), followed by wells or rivers (both close to living areas and susceptible to fecal pollution). Moreover, some students’ homes (14.33%) used river or well water as the source of drinking water and 84.42% of school children were in the habit of drinking unboiled water. The drinking water is rarely disinfected and is often contaminated by untreated infectious human excreta, which puts the local residents at great risk of intestinal parasitic infections. Safer drinking water is an urgent need in the rural regions of Liangshan Prefecture. Having a household lavatory was negatively associated with
T. trichiura infection, which was similar to previous findings [
19,
27,
28,
29]. In order to reduce intestinal infectious diseases, the local government promoted and constructed triple compartment toilets or biogas digesters that can fully ferment feces to kill the eggs and ensure that human waste is safely separated from human contact in some rural areas [
30,
31]. But many families only have simple lavatories that pile up human stools and urine as a direct fertilizer. A cluster-randomized trial undertaken in Kenya demonstrated that school hygiene and sanitation reduced the re-infections of STH after school-based deworming [
2]. A recent meta-analysis has shown that adequate sanitation is associated with the reduction of STH transmission risk (between 40% and 50% reduced infection rates) [
28]. There is no doubt that improvements to water, sanitation, and hygiene (WASH) lead to a significant reduction in STH infection. Schools are available platforms, not only for health education but for sanitation improvements. School-age children are more likely to receive health education and tend to integrate new health behaviors into their daily lives [
32].
Soil-transmitted helminthiasis, a group of NTDs, is thought to be associated with malnutrition and iron deficiency anemia, and has a negative impact on children’s physical and cognitive development [
33]. Hence, reducing risk factors and regular deworming become important strategies for controlling STH [
34]. Effective control of STH can have a positive outcome on students’ education, as chronic helminth infection impedes cognitive development and leads to growth delays, thus delaying enrollment and grade progression [
35].
Cryptosporidium is typically transmitted by fecal-oral routes, through ingestion of human or domestic animal fecal-contaminated food or untreated water. In our study, students having meals at the school canteen or living on campus had lower odds of obtaining
Cryptosporidium infection. Students who live on campus (89.10%) ate three meals at the school canteen. The elementary school we selected was basically a boarding school. The majority of the students stayed in the school dormitories for 5 days per week and returned home during holidays and weekends. One possible reason for the association of
Cryptosporidium infection with eating in the school cafeteria was less chance of contact with domestic animals. Raising domestic animals is known as a risk factor for
Cryptosporidium infection [
36,
37]. Another possible reason was that schools had better sanitation facilities and safer water, protecting those students who did not have access to these facilities at home [
14,
32,
38]. The local government has been concerned about the safety of school drinking water. At Lw Primary School, improved water and sanitation facilities, including basic tap water, were available to the students. Tap water was used for handwashing without soap. A recent review showed that diarrhea and gastrointestinal diseases decreased as schools had access to adequate sanitation [
39]. Improper waste disposal and unsafe water, especially at home, will increase the chance of transmission of fecal-oral diseases [
14,
40].
We recognize a number of limitations in our study. The diagnoses of three intestinal parasitic infections were based on a single stool sample and underestimation of the infection rates might be possible. There was also a lack of data on helminth infection intensities and
Cryptosporidium genotypes. Further research is needed to determine the infection intensities of
A. lumbricoides and
T. trichiura and also the routes of transmission of
Cryptosporidium among school children in this region. To truly understand the motivators for behavior and exposure to infection, further studies might be needed to systematically assess risk factors of intestinal parasites by using a combination of quantitative and qualitative methods including water quality monitoring and WASH spot checks [
40]. The sample size is not enough for more accurate statistical analysis. In view of these limitations, the findings should be interpreted discreetly.

 ,
, 

{kind=link}