1. Introduction
Artisanal and small-scale gold mining (ASGM) has recently been identified as the largest contributor to global anthropogenic mercury (Hg) in the atmosphere [
1]. Eighty to 100 million people are estimated to depend on ASGM for their livelihoods or be indirectly involved [
2,
3], and 10 to 15 million people are directly employed by ASGM globally [
1,
4]. Mercury, a neurotoxicant, is used to isolate gold ore in the ASGM process [
5]. There are two forms of Hg: organic and inorganic, which can be elemental (Hg) or inorganic salts (e.g., HgS, HgCl
2, Hg
+, Hg
+2). ASGM utilizes elemental Hg, which poses a risk for human health and environmental contamination as Hg is a potent neurotoxicant [
6,
7].
Gold deposits are ubiquitous in Ghana and have resulted in ASGM and large-scale gold mining across the country, making Ghana the ninth largest gold-producing country in the world [
8]. ASGM has grown tremendously in recent years with the rising price of gold, deregulation of gold mining, chronic unemployment, and increasing poverty [
9]. ASGM accounts for 35% of Ghana’s national gold production and employs 500,000 to 1 million people directly or indirectly [
8,
10]. In the Upper East Region of Ghana, where ASGM has grown rapidly, it is estimated that over 10,000 people are employed directly by ASGM in the Talensi-Nabdam District alone (now separate Talensi and Nabdam Districts) [
11].
In Ghanaian ASGM, gold ore is excavated from surface and shallow underground mining, and panning in streams [
7]. Ore is generally milled in a grinding machine and screened manually. The fine fraction is mixed with water and gold is concentrated in a wooden sluice box covered with carpets where gold and other heavy minerals are retained. The concentrate is panned with Hg in a rubber pan to form a gold amalgam. The amalgam is heated with a blowtorch to volatize the Hg and leave behind the gold ore with some residual Hg. Large amounts of Hg vapor is deposited locally and can be re-emitted from water and soil surfaces or can be methylated, bioaccumulate, and biomagnify in food chains [
1,
12]. Surface soils, water bodies, and sediments are the major biospheric sinks for Hg [
13].
Exposure to organic Hg, mainly methylmercury (MeHg), is primarily through consuming fish and seafood, although this varies in ASGM communities [
14]. Hair Hg concentrations generally reflect MeHg exposures from blood Hg concentrations at the time of hair growth, which grows at an average of one centimeter per month [
5,
15]. Elemental Hg, used in ASGM, has a half-life of approximately 56–58 days in the whole body and kidneys and can be measured in urine to assess medium-term exposure [
5,
16]. Urine and hair biological markers are used to assess elemental and MeHg exposures, respectively [
5,
17].
Soil ingestion is not thought of as a significant pathway of exposure to Hg, but may be of concern if Hg concentrations are high and people ingest significant quantities of soil. In 2010, approximately 400 children were killed and thousands adversely affected from lead poisoning at an ASGM community in northwestern Nigeria, Zamfara [
18,
19]. In this tragic case, the gold-rich ore also contained lead sulfide (galena), and thus processing the ore lead to extreme contamination of local soil and edible plants with lead. Ingestion of lead-contaminated soils and inhaled dust were determined to be the dominant exposure pathways, while contaminated water and foodstuff consumption were lesser but still notable exposure pathways [
19]. The quantity of soil and dust ingested in rural ASGM communities in Ghana are unknown, but there is evidence of the practice of geophagy (habitual, intentional ingestion) in some studies of Ghana and Sub-Saharan Africa, particularly among pregnant women [
20]. The species of Hg in soil in ASGM communities is unknown, and may be elemental Hg, which is used in ASGM, or oxidized inorganic or organic species. This practice has been observed among the Ewe in Ghana at a prevalence of 13.9% among adult males (ingestion of 13,000 mg soil/day), and 46.4% among adult females (30,000 mg/day; 150,000 mg/day in upper limit cases) [
21], and thought to be an exposure pathway for helminth (roundworms) for women in the Ashanti Region [
22]. Fifty percent of pregnant women practiced geophagy in Nigeria [
20]. In a northwestern Tanzanian ASGM community, geophagy was prevalent in 45.6% of pregnant women (62,500 mg/day) [
23].
An earlier study by our group in Ghana’s Talensi District observed elevated Hg exposure among ASGM miners based on analyses of urine and hair samples [
24]. To increase understanding of exposure as well as address continued community concerns, our team conducted a series of follow-up cross sectional studies that were broader in scope to assess Hg exposure in human (urine and hair from ASGM workers and community members) and ecological (household soil, sediment, ore, and fish) samples to provide a more holistic understanding of contamination and exposures. Spurred by the case of lead poisoning in an ASGM community in Nigeria, the work was also utilized to better understand soil Hg contamination (in households situated within an ASGM community as well as in an urban environment near a refinery) as one potential exposure pathway. Spatial methods were used to map key ASGM activities and households, as well as estimate Hg contamination in soil and urinary Hg throughout the ASGM community. We hypothesized that ASGM community participants and ASG miners in particular would have higher hair, urine, and household soil Hg levels than non-ASGM community participants and ASGM community non-miners.
2. Materials and Methods
2.1. Sampling Strategy and Study Populations
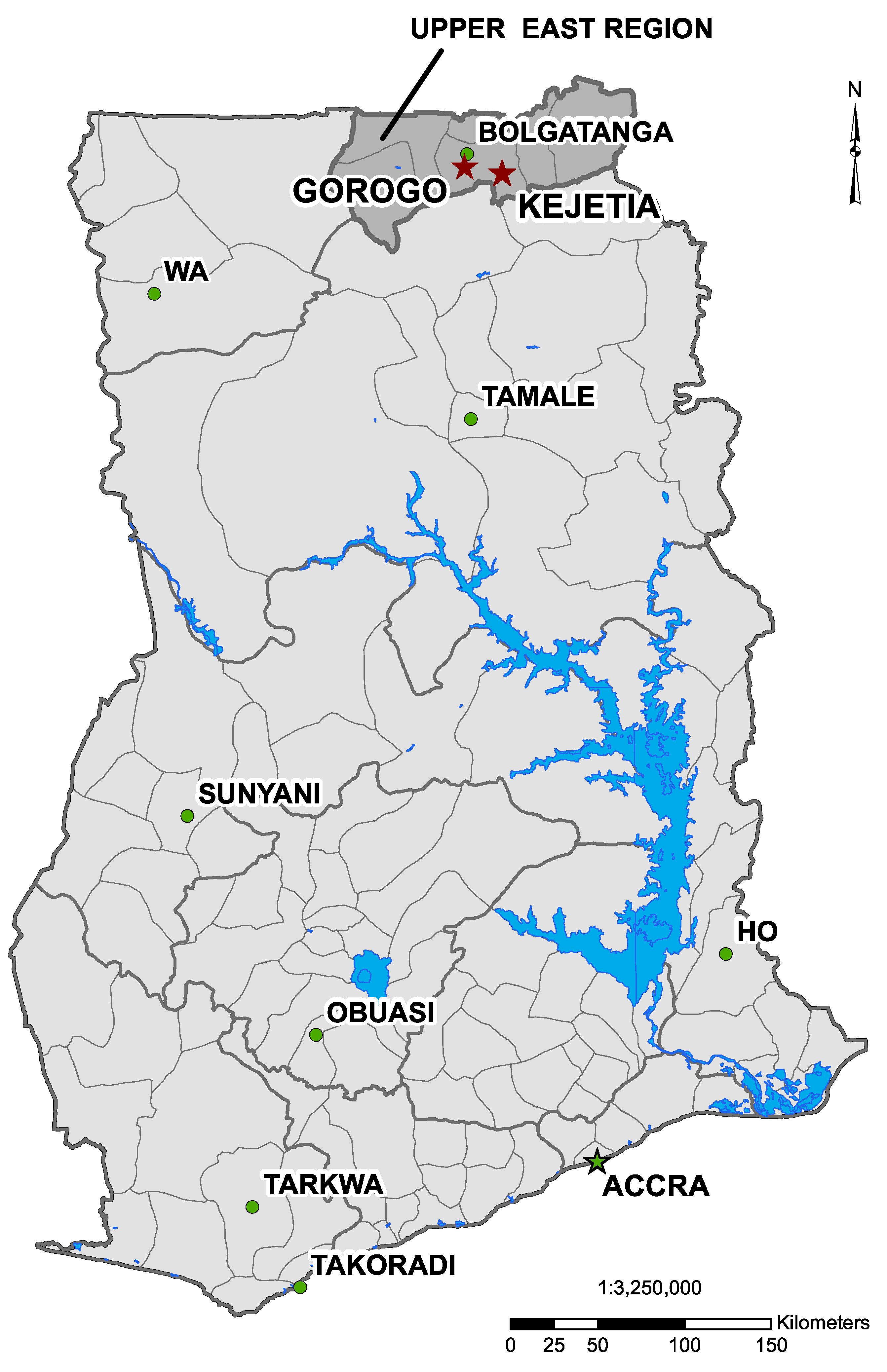
Data were collected from two communities in the Upper East Region of Ghana, in the prior Talensi-Nabdam District (
Figure 1), which has since split into separate Talensi and Nabdam Districts. A small-scale gold mining community, Kejetia (
Figure 2), was selected from a prior study of ASGM miners in the area [
24]. Kejetia is a community of approximately 2500 people that developed around ASGM in 1995 [
11,
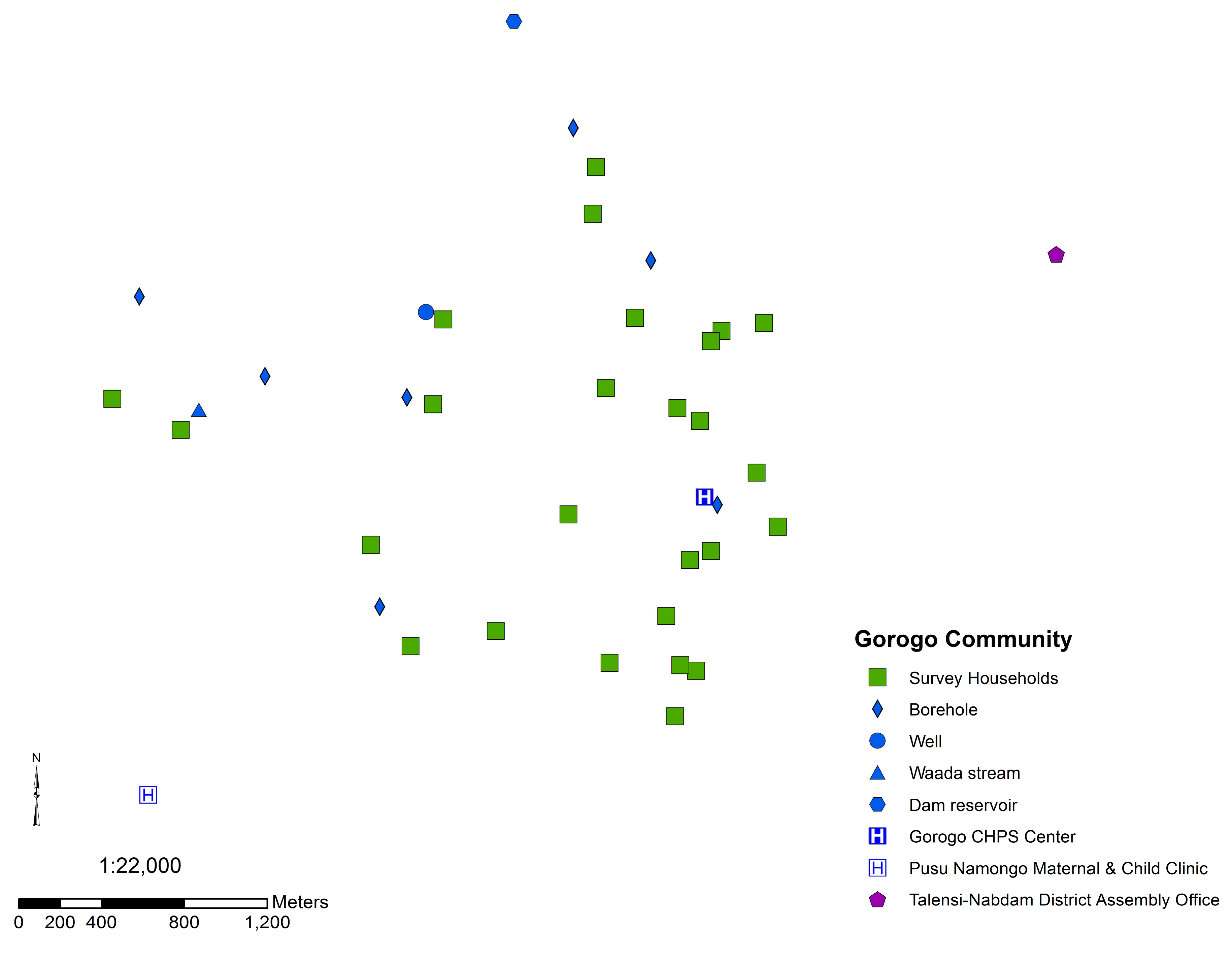
25]. Gorogo, a nearby, upstream, non-mining community, was selected for comparison (
Figure S1). Permission to work with the communities was granted by each community’s traditional chief and assemblyperson in Gorogo, and Institutional Review Board (IRB) approval was obtained through the University of Michigan (HUM00028444).
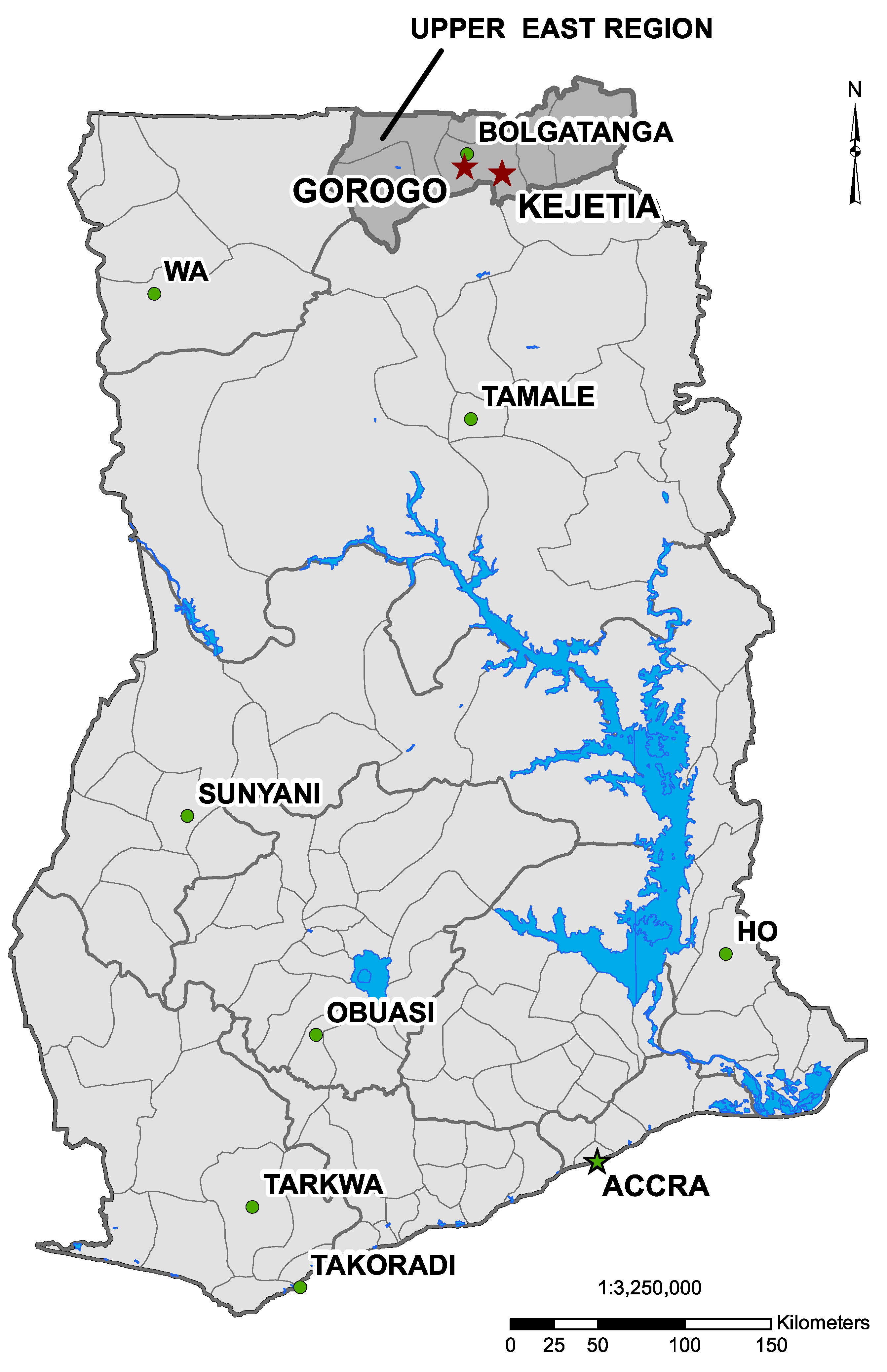
Figure 1.
Map of Ghana indicating Kejetia and Gorogo (two red stars), the two research communities, and the municipal capital, Bolgatanga (green circle), in the Upper East Region. (Map produced from data provided by the National Renewable Energy Laboratory [NREL], by Mozhgon Rajaee, June 2012 [
26]).
Figure 1.
Map of Ghana indicating Kejetia and Gorogo (two red stars), the two research communities, and the municipal capital, Bolgatanga (green circle), in the Upper East Region. (Map produced from data provided by the National Renewable Energy Laboratory [NREL], by Mozhgon Rajaee, June 2012 [
26]).
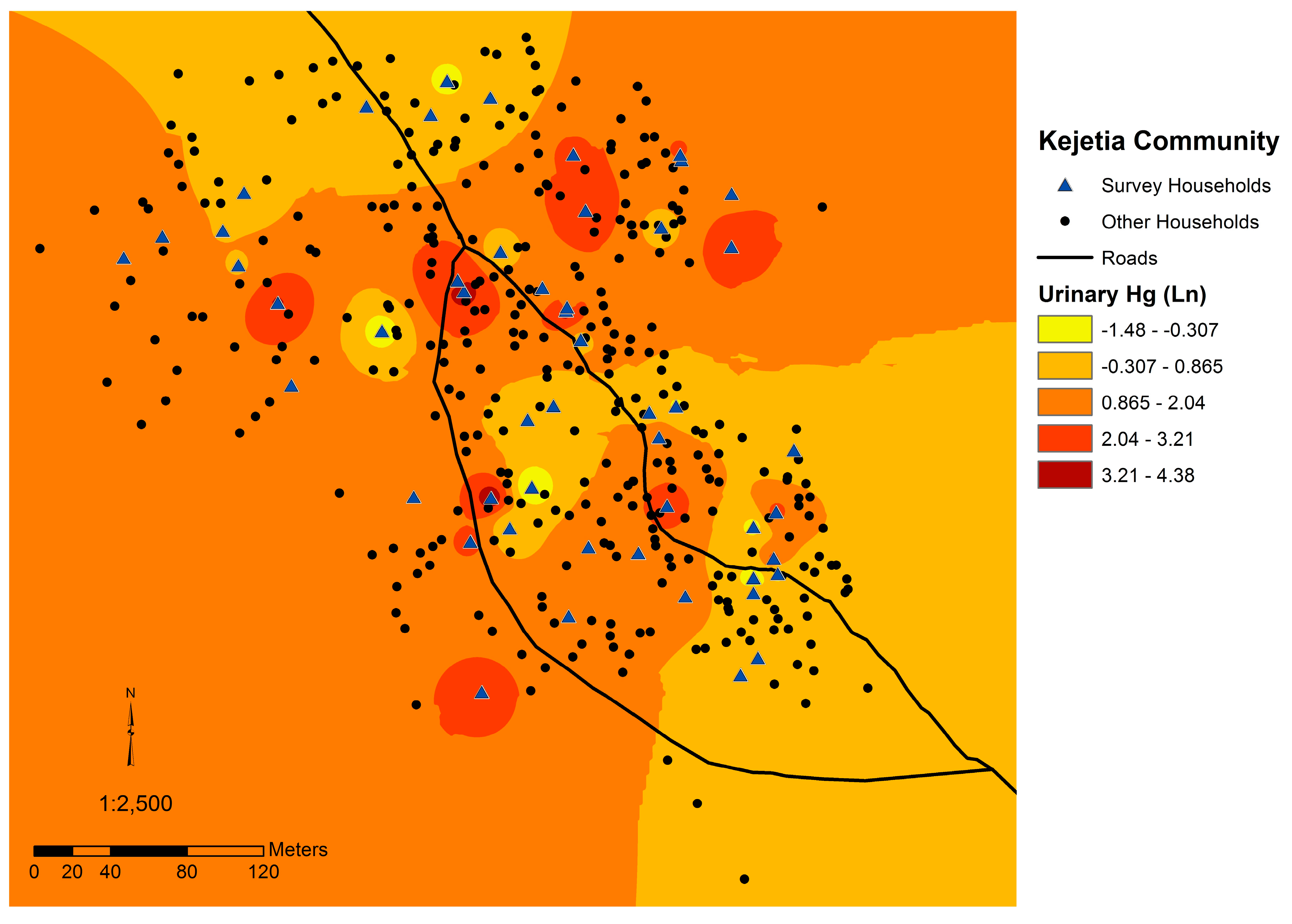
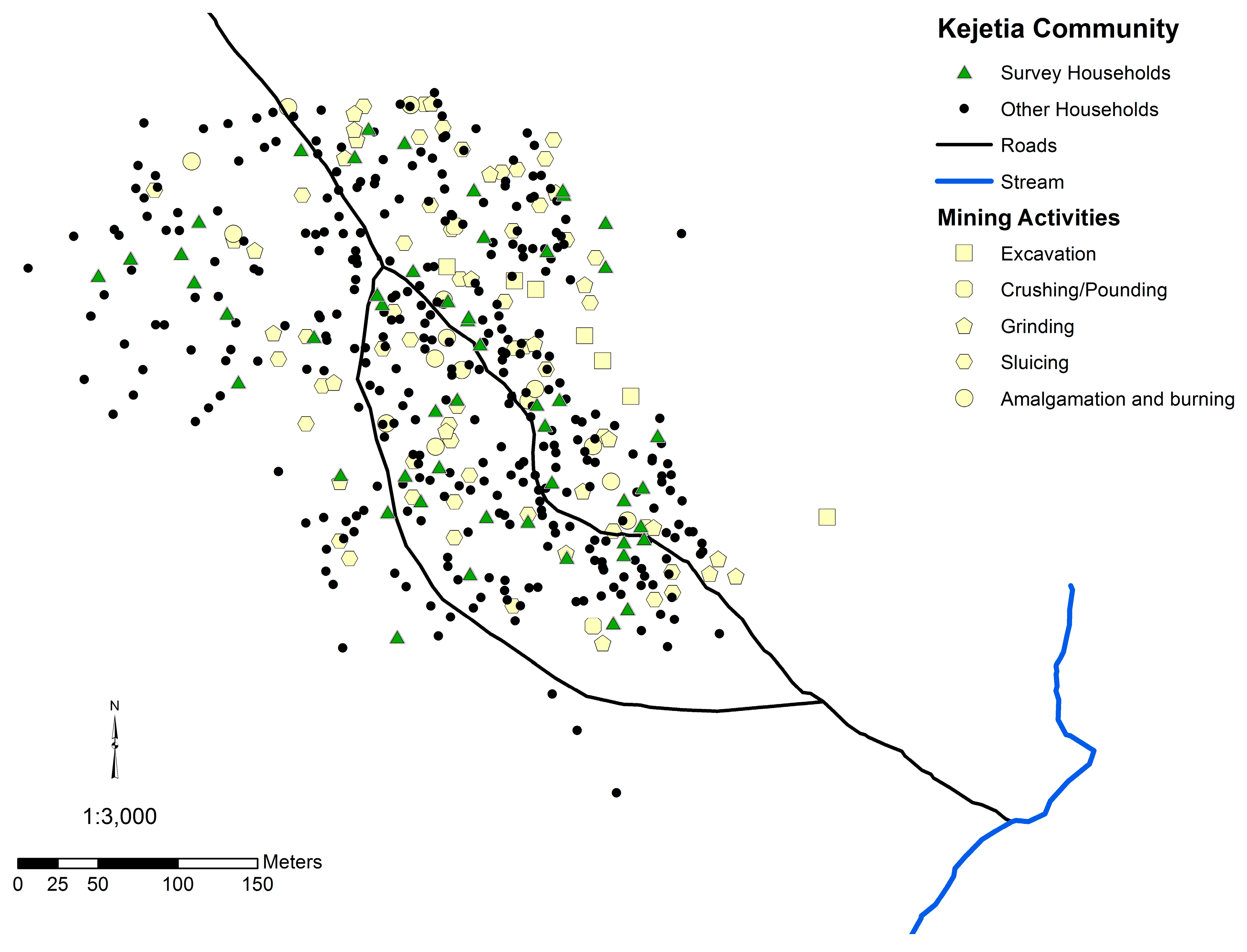
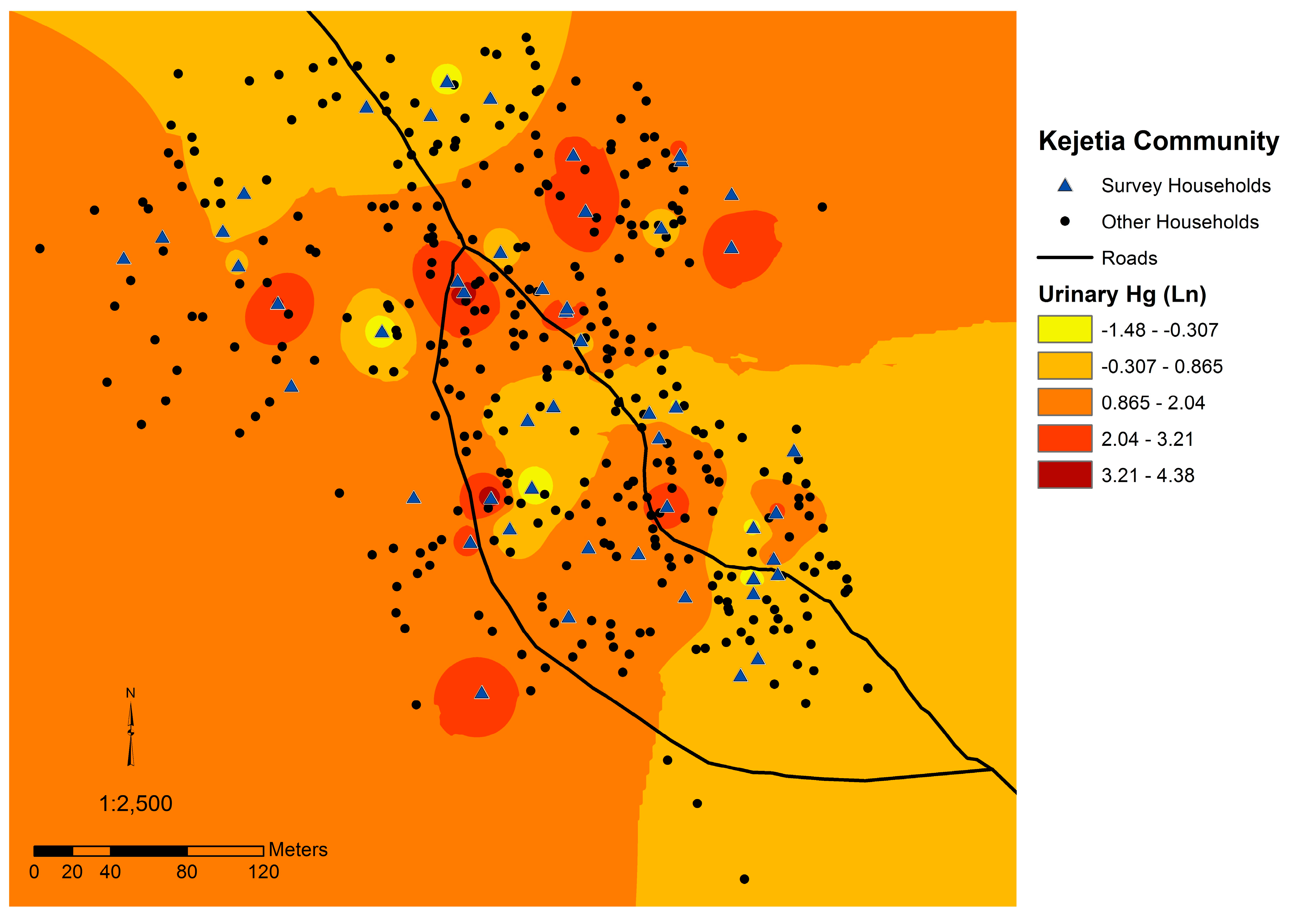
Figure 2.
Map of the Kejetia community, indicating households surveyed, community markers, and locations of mining activities.
Figure 2.
Map of the Kejetia community, indicating households surveyed, community markers, and locations of mining activities.
Participants were recruited to participate in the survey by household. In accordance with cultural norms, households were defined as those who eat from the same “pot”. Lacking community maps and official population estimates, it was impossible to follow true random sampling. In June 2010, women of childbearing age (16 through 49 years) were surveyed from Kejetia through convenience sampling. From May through July 2011, sampling was done in Kejetia and Gorogo. In Kejetia, all households were assigned a set of coordinates using a handheld global positioning system (GPS; Oregon 450; Garmin International, Inc., Olathe, USA). Households were numbered and assigned to a cluster of approximately 20 households based on geographic proximity. Each day, a random number was selected from a bag to identify a household from up to three different clusters for participation. Two to three random households were sampled from each cluster to ensure geographic representation. If a household was not eligible or declined participation, another number from within the cluster was pulled from the bag until an appropriate household was found.
The community of Gorogo was much more geographically dispersed, making clustering infeasible. Households were selected from convenience sampling, by spinning a plastic bottle at the geographic middle of the community and selecting the house pointed to most closely [
27]. The bottle was then spun from each participating household to find the next household to be surveyed, and from other geographic locations throughout the community. If a household was not eligible or declined participation, re-spinning the bottle in the same location as the previous spin chose a replacement household.
2.2. Surveys
For each household surveyed, a household head and up to three other adults (18 years or older) were interviewed on household characteristics, and their occupational and medical histories. Questions were adapted from the Ghana Demographic and Health Survey (DHS) [
28] and the American Thoracic Society Epidemiology Standardization Project [
29], with responses being studied in other efforts by our team. English surveys were administered by a team of university students and verbally translated by local Ghanaian translators in the participant’s choice language (Talen, Nabt, Gurune, Twi, Dagbani, English, or Hausa). Translators were trained on appropriate medical terms and health outcomes in local languages prior to conducting the interviews.
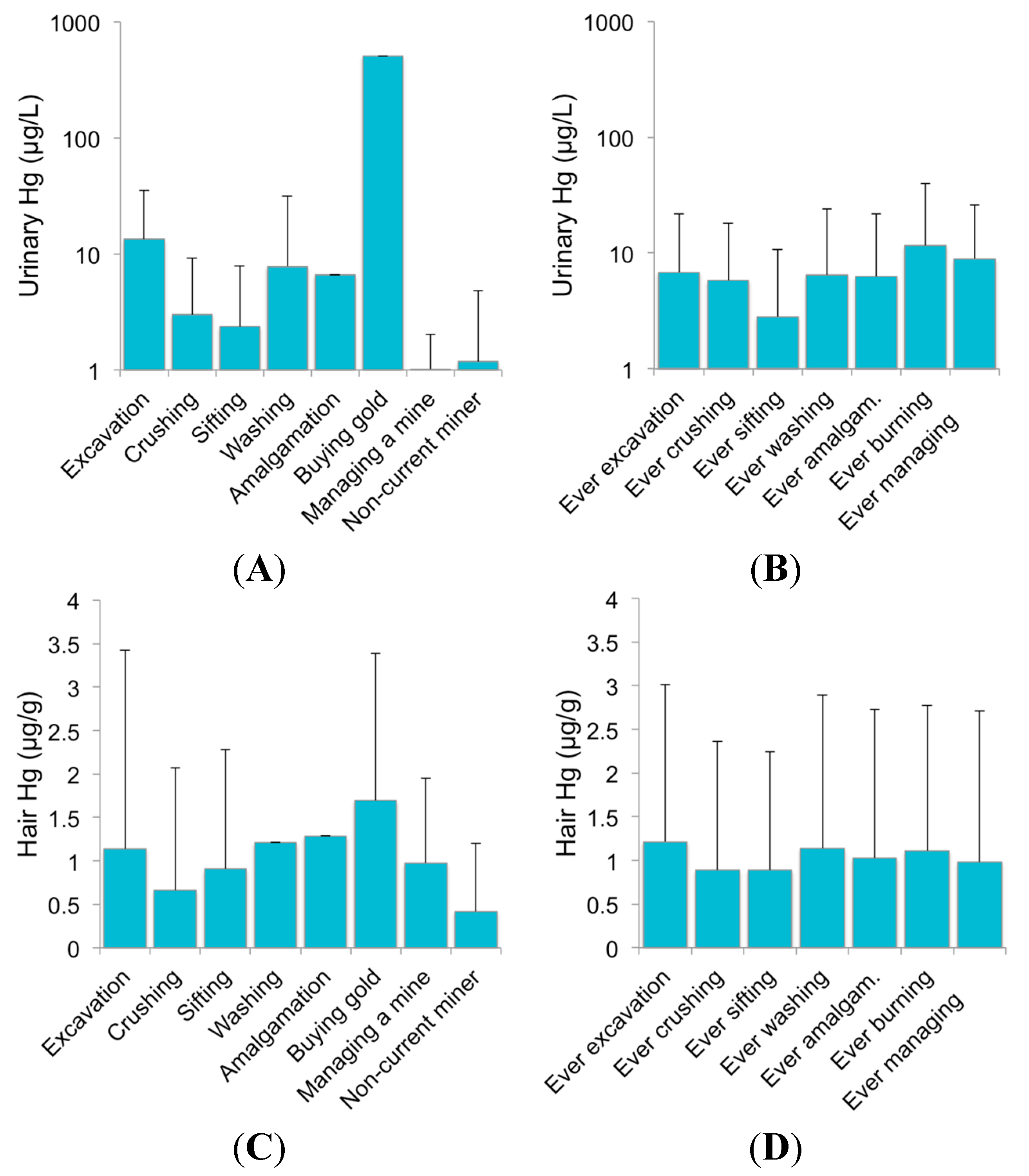
The head of household (HOH) or an identified alternative household participant knowledgeable about the individuals in the household completed a survey on demographics of people in the household, household characteristics and amenities, and a 24-h dietary survey. A maximum of four adults per household, including the HOH were administered a separate survey. In 2010, women were surveyed on prenatal care and birth, medical, and occupational histories. In 2011, this included questions on occupational, medical, and smoking histories; and spirometry was performed when feasible. In households with more than four adults, the HOH provided guidance on who to interview. ASGM activities were stratified as excavation, crushing (crushing, grinding, or pounding ore), sifting (“shanking”), washing (or sluicing), amalgamation, burning (or roasting), and owning or managing a mine. Since many participants engaged in multiple mining activities, each participant was surveyed about ever-involvement in each mining activity as well as the main activity performed in the three months preceding the survey.
2.3. Sample Collection
Urine and hair biological markers were collected to assess elemental and methylmercury exposure, respectively, from all participants when feasible [
5]. Spot urine samples (5–15 mL) were collected from participants mid-morning at the time of the interview, stored at room temperature in Bolgatanga, Ghana, and frozen at −20 °C until analysis in the U.S. Samples were thawed to 4 °C and vortexed prior to analysis. Hair was cut as close to the scalp as possible from the occipital region of the head and placed on a sticky-note and stored in a plastic bag until analysis. Only the 2 cm closest to the scalp was used for analysis. Hair samples were washed once with acetone and twice with deionized water, and dried for Hg analysis [
24,
30].
Household soil samples were collected in 2010 and 2011from Kejetia and in 2012 from a Bolgatanga refinery. Household surface soil was collected from a common area, designated by the HOH. Each household soil sample is a composite of five subsamples taken from the four corners and center of an approximate 30 cm
2 area [
31]. Samples were collected from the top 1–2 cm of soil into sealed WhirlPak bags. Ore samples were collected from miners within Kejetia from various stages throughout the ASGM process (crushing, grinding, and washing) in 2011. In 2012, soil samples were collected at a gold refinery in the regional urban center Bolgatanga (which processes the gold mined from Kejetia), at zero, three, and six meters from the roasting site, following the same collection protocol as household soil samples. Samples were stored at room temperature in Bolgatanga, Ghana at 4 °C until analysis in the U.S. All samples were dried at 110 °C for 16 h and soil sifted through a 2 mm polymer sieve to remove any detritus or stones.
In 2010, fish and sediment samples were collected from around Kejetia. Fish were caught from the adjacent stream and nearby reservoir and purchased from vendors in Kejetia. Samples were whole fish, but were not identified by species names. All fish samples were dried in Bolgatanga and stored at 4 °C until analysis in the U.S. Samples were dried again at 60 °C for 16 h in the laboratory. Whole fish were ground up for analyses to better reflect consumption habits in the Upper East Region.
2.4. Sample Mercury Analysis
Total Hg was measured using a Direct Mercury Analyzer-80 (DMA-80; Milestone, Inc., Shelton, CT, USA), following U.S. Environmental Protection Agency (EPA) Method 7473 [
32]. Certified reference materials (CRMs; urine: QMEQAS, Institut National de Santa Publique Quebec; hair: National Institute for Environmental Studies Japan; dogfish liver: DOLT-4, National Research Council Canada; soil: San Joaquin Soil 2709, U.S. National Institute of Standards and Technology) were analyzed approximately every ten samples, blanks every five samples and sample replicates at least every nine samples. All soil and sediment samples were run in duplicate and blanks every two samples (four replicates).
The average recovery of CRMs was 91%–92% for NIES hair and 94%–107% for DOLT-4, and 97%–98% for QMEQAS urine in urine, hair, soil, sediment, ore, and fish sample analyses. For San Joaquin soil CRM, the average recovery ranged from 85% to 101% in Gorogo and Kejetia, respectively. In Kejetia and Gorogo samples, within-day variation was <5% for NIES hair and QMEQAS urine, <10% for DOLT-4, and <20% for San Joaquin soil. The average within-day variation of replicates of participants’ samples was low for hair (<6%) and urine (<8.3%). Soil and sediment samples, analyzed in duplicate due to expected higher variation, had an average within-day variation of 6.7%–12.3%.
The average theoretical Hg detection limit (TMDL; 3 × standard deviation of the ng Hg of blanks + average ng Hg of blanks) for hair was 0.058 ng Hg in Kejetia in 2010, 0.126 ng Hg in Kejetia in 2011, and 0.044 ng Hg in Gorogo. No hair samples were below the TMDL. The average TMDL for urine was 0.090 ng Hg for Kejetia in 2010 (1 sample < TMDL), 0.136 ng Hg for Kejetia in 2011 (3 samples < TMDL), and 0.046 ng Hg for Gorogo (21 samples < TMDL). The average TMDL for household soil was 1.853 ng Hg for Kejetia in 2010, 3.030 ng Hg for Kejetia in 2011, and 0.083 ng Hg for Gorogo. The TMDL for Bolgatanga soil refinery samples was 3.987 ng Hg. The TMDL was high for ore samples (3.183 ng Hg), with 3 samples below the TMDL. Sediment samples also had a high TMDL of 1.853 ng Hg, as they were analyzed with household soil samples (11 samples < TMDL). No fish samples were below the TMDL (0.134 ng Hg).
Specific gravity (SG) was measured using a pocket refractometer (PAL-10S, Atago U.S.A., Inc., Tokyo, Japan) to adjust urine samples by urinary dilution using the mean urinary specific gravity (1.016) [
33,
34]. Specific gravity was used to adjust for urinary flow over creatinine, as it is less influenced by ethnicity, age, sex, and diet [
35,
36,
37]. The equation is as follows, where
p refers to a participant’s personal urinary Hg and urinary SG values, and the average urinary SG is 1.016:
2.5. Soil and Hg Ingestion
Soil and dust ingestion was assessed with three potential scenarios: inadvertent ingestion of small quantities of soil and dust; occasional, intentional ingestion of soil and dust (pica); and habitual, intentional ingestion of soil and dust (geophagy). Inadvertent soil and dust ingestion occurs from ingestion of house dust and hand-to-mouth and food contact. In rural northern Ghanaian communities, earthen floors, a long dry season, and mining activities may increase soil and dust ingestion for adults and children. Using estimates of ingestion from the U.S. EPA on average ingestion rates based on age for a general U.S. population and estimates from other studies used in Sub-Saharan Africa, scenarios were evaluated using a central tendency (median or mean) or worst-case scenario that was often the estimated 95% upper limit of ingestion. Despite best efforts, however, there have been no known studies to quantify soil or dust ingestion in Sub-Saharan Africa for non-geophagic adults or geophagic practices in northeast Ghana where our study was based. As such, we used existing estimates of soil and dust ingestion and the relevant calculations. A variety of scenarios were explored. The U.S. EPA estimates soil and dust ingestion for inadvertent ingestion, whereas estimates for pica and geophagy principally refer only to soil ingestion [
38].
Mercury ingestion from soil and dust was calculated per day by multiplying the household soil total Hg concentration (note, we did not speciate the soil Hg) with the quantity of soil and dust ingested per day estimated for various scenarios. For all scenarios, the estimated quantity of soil and dust ingested is equal for all participants, except for the inadvertent ingestion central tendency of 50 mg/day for adults ≥21 years and 110 mg/day for adults 18 to 21 years [
38]. Lacking a reference dose (RfD) for elemental Hg (which is likely to be the main form of Hg in the soil), Hg ingestion was evaluated with the U.S. EPA RfD for mercuric chloride of 0.3 µg Hg per kg of body weight-day and using participants’ body weight [
39]. To assess potential exposure for Bolgatanga residents living near the urban refinery, a set weight of 65 kg was used to determine an RfD. Although the average U.S. adult weight is 80 kg (>21 years) [
38], the average weight was 63.2 kg in Kejetia and 59.1 kg in Gorogo. Furthermore, we assumed 100% bioavailability of Hg following ingestion, and without Hg speciation data we used total soil Hg to compare to the RfD. Future studies should further explore these particular issues.
2.6. Statistical and Spatial Analyses
The data were analyzed using SPSS Statistical Software (v.22; IBM, Chicago, IL, USA). Since Hg biomarkers and household soil were not normally distributed, they were log-transformed for independent t-tests. Bivariate analyses were also performed non-parametrically (e.g., Spearman’s ρ). One-way analysis of variance (ANOVA) was used to assess bivariate correlations of Hg biomarkers and household soil with mining status, mining activities, sex, and education level. Correlations between ever-involvement in each mining activity were assessed through Chi-square tests. Statistical analyses were performed with specific gravity-adjusted and unadjusted urinary Hg. All results are reported with mean ± standard deviation, unless otherwise indicated.
Maps of households in each community were created using ArcGIS (v. 10.1; Esri, Redlands, CA, USA). GPS coordinates were measured at each participant’s household. We were unable to geocode three households due to logistical issues. These three households were exempted from geospatial analyses. This included two households from Kejetia and one from Gorogo. Global Moran’s I statistic was used to analyze spatial autocorrelation of Hg concentrations across the Kejetia community in urine and household soil. In each assessment, Euclidean distance and inverse distance weighting were used to account for Kejetia’s non-grid organization and to place a larger influence on nearby neighbor Hg concentrations than more distant Hg concentrations.
4. Discussion
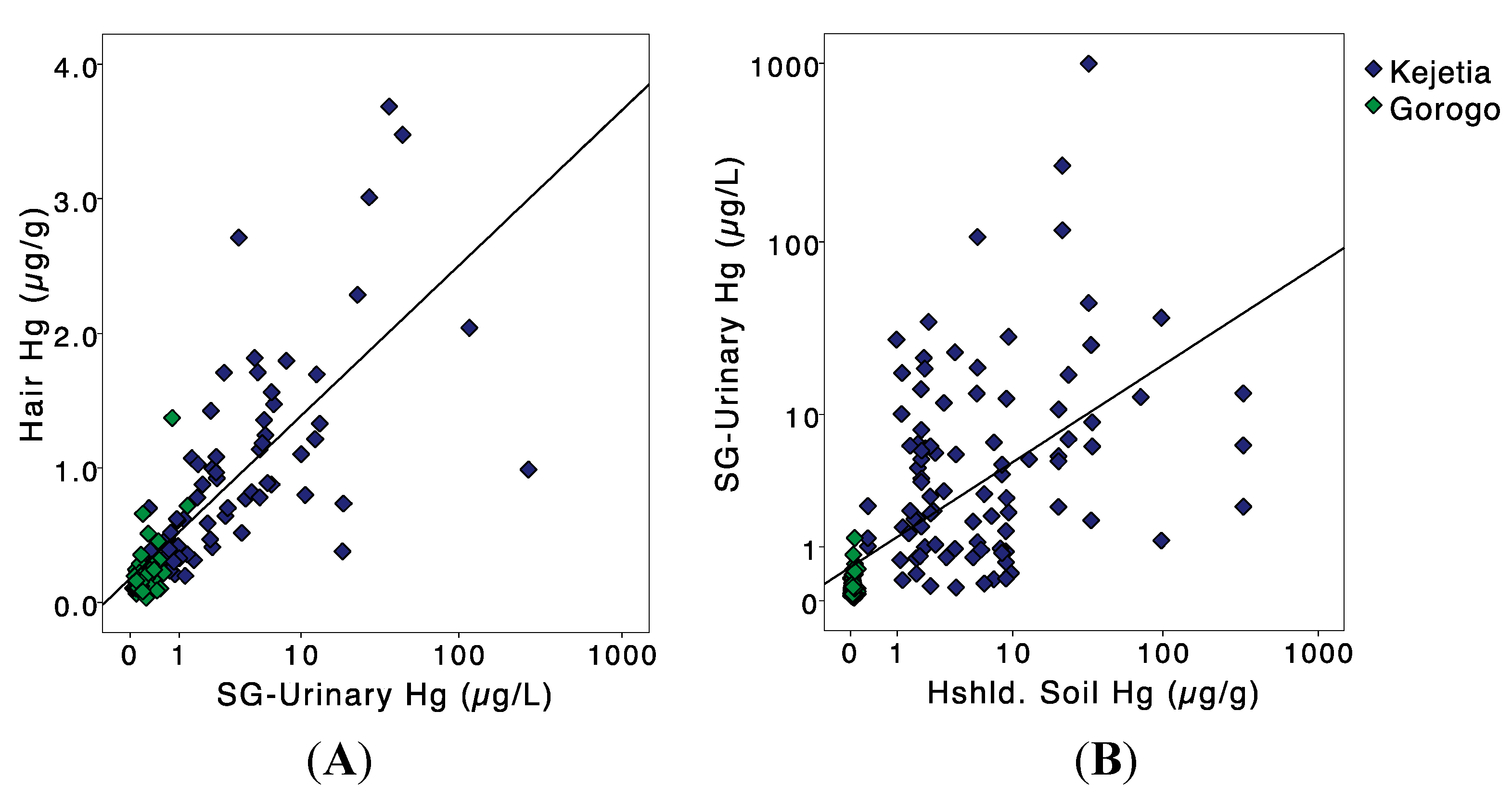
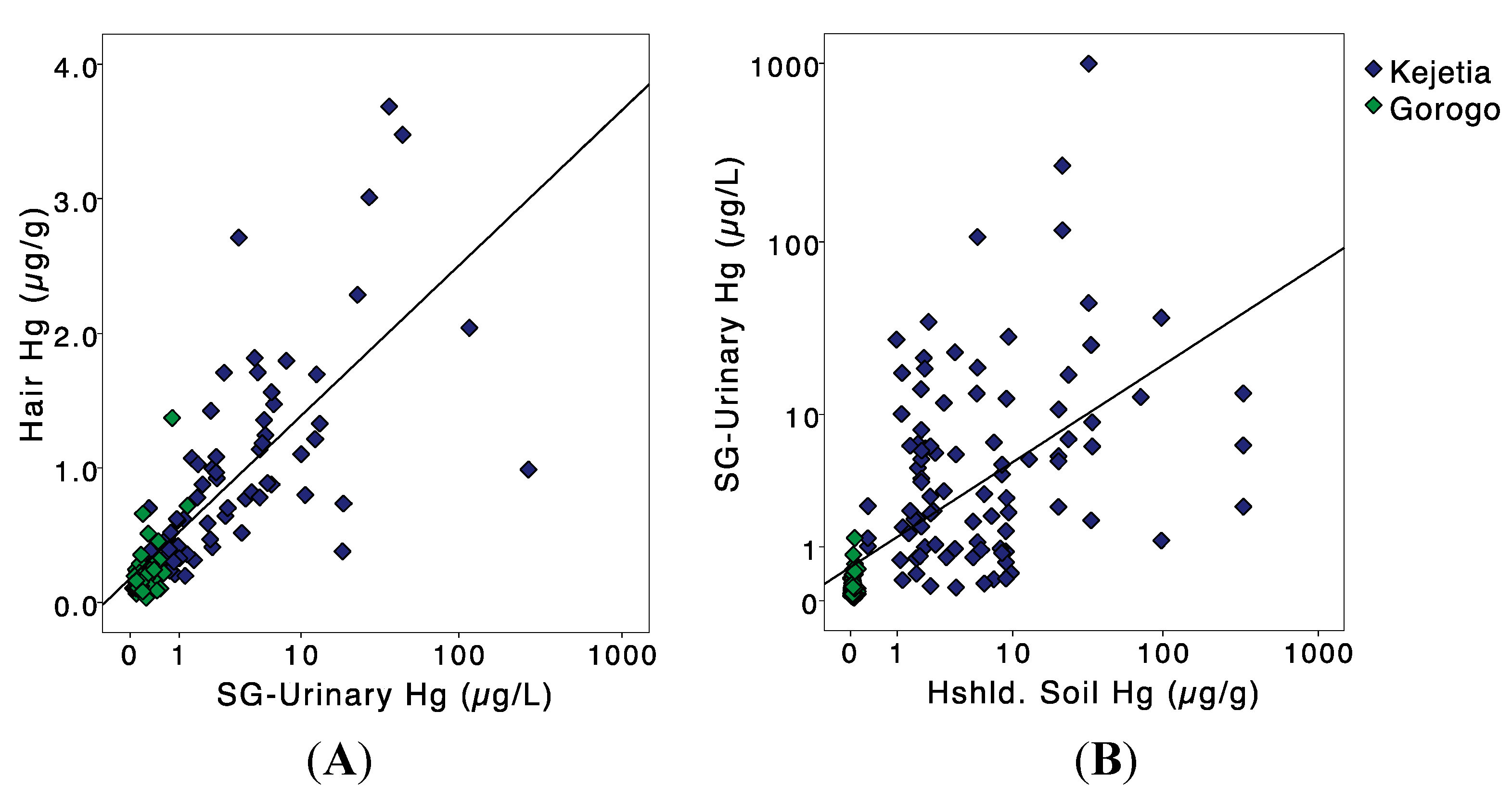
In Kejetia, like other ASGM communities, Hg contamination is of prominent concern. Our study assessed the Hg contamination of soil, sediment, and fish, and human exposure through multiple biomarker measures. Mining involvement and use of Hg was common in Kejetia—just over 50% of Kejetia 2011 participants performed amalgamation, indicating a potential for widespread contamination and exposures. Urinary and hair Hg biomarkers, which were positively correlated, were elevated among Kejetia and Gorogo participants.
Studies of other ASGM communities generally had higher mean hair Hg concentrations than in Kejetia (0.974 ± 0.748 µg/g), but this varied (means ranging from 0.62 to 4.27 µg/g) [
50,
51]. Kejetia miners (1.13 ± 0.809 µg/g) had similar hair Hg concentrations to Kejetia miners surveyed in 2009 (1.2 ± 1.4 µg/g) [
24] and to other ASG miners across Ghana (means ranging from 1.1 to 2.14 µg/g) [
24,
51,
52]. Most participants had hair Hg concentrations between 1 and 2 µg/g, a “normal level” [
41]. Mean hair Hg concentrations were lower in Gorogo (0.231 ± 0.202 µg/g) than observed in other non-mining populations in Ghana (means ranging from 0.717 to 2.35 µg/g) [
51,
52,
53,
54]. Other studies of non-miners have included more urban participants that may have a higher diet of fish contributing to higher hair Hg concentrations. In addition, our analysis of Hg in sediment and fish found that concentrations were low, as seen across Ghana [
7], which may partially explain our low hair Hg levels.
External contamination is a major challenge in using hair as a biomarker for MeHg in ASGM communities. Sherman
et al. [
14] examined Hg stable isotopes in urine and hair to assess their validity as biomarkers for elemental and MeHg. The study used hair and urinary Hg from Kejetia miners collected in our 2010 and 2011 study. Total urinary Hg had Hg isotope ratios similar to those found in ore deposits, and accurately reflect exposure to inorganic elemental Hg used in ASGM. Hair Hg, however, had a low percentage of MeHg as total Hg (7.6–29%), suggesting that the majority of hair Hg was exogenously adsorbed elemental Hg [
14]. It is likely that hair Hg overestimates exposure to MeHg from fish and seafood consumption in these ASGM communities [
14]. The one outlier from 2010 (92.6 µg/g hair Hg) may be an example of high exogenously adsorbed elemental Hg on hair. Our hair samples were washed with acetone and deionized water, but other studies have found that these procedures do not remove adsorbed, external Hg contamination [
17]. It is possible to analyze hair samples for MeHg specifically, but this requires a larger mass of hair, and sample quantities are often limited as many Ghanaians had hair <2 cm. Thus, hair samples from Kejetia and ASGM sites likely do not represent merely MeHg as is often found in populations not exposed to elemental or inorganic Hg.
Kejetia 2011 participants had higher mean urinary Hg concentrations (30.9 µg/L) than observed in most other studies of ASGM communities in southern Ghana (means ranging from 2.6 to 34.2 µg/L) [
50,
55]. Slight differences in the ASGM process and practices, such as communities built solely around ASGM, may lead to higher exposures in the Upper East Region than in southern Ghana where people may not live as close to mining activities. Kejetia miners from our study had similar, but slightly elevated, urinary Hg levels from a 2009 study of Kejetia miners (mean: 38.9 ± 95.7 µg/L) [
24], and other studies of ASGM miners in Ghana (means ranging from 0.56 to 17.0 µg/L) [
24,
52,
55,
56]. Mean urinary Hg in Gorogo (0.161 µg/L) was lower than observed in other non-ASGM communities (means ranging from 0.69 to 3.1 µg/L) [
52,
55].
Mercury is a known toxicant with numerous adverse health effects. Hg is especially dangerous as it is able to pass the blood-brain and blood-placental barrier, posing additional risks to an unborn fetus and young children [
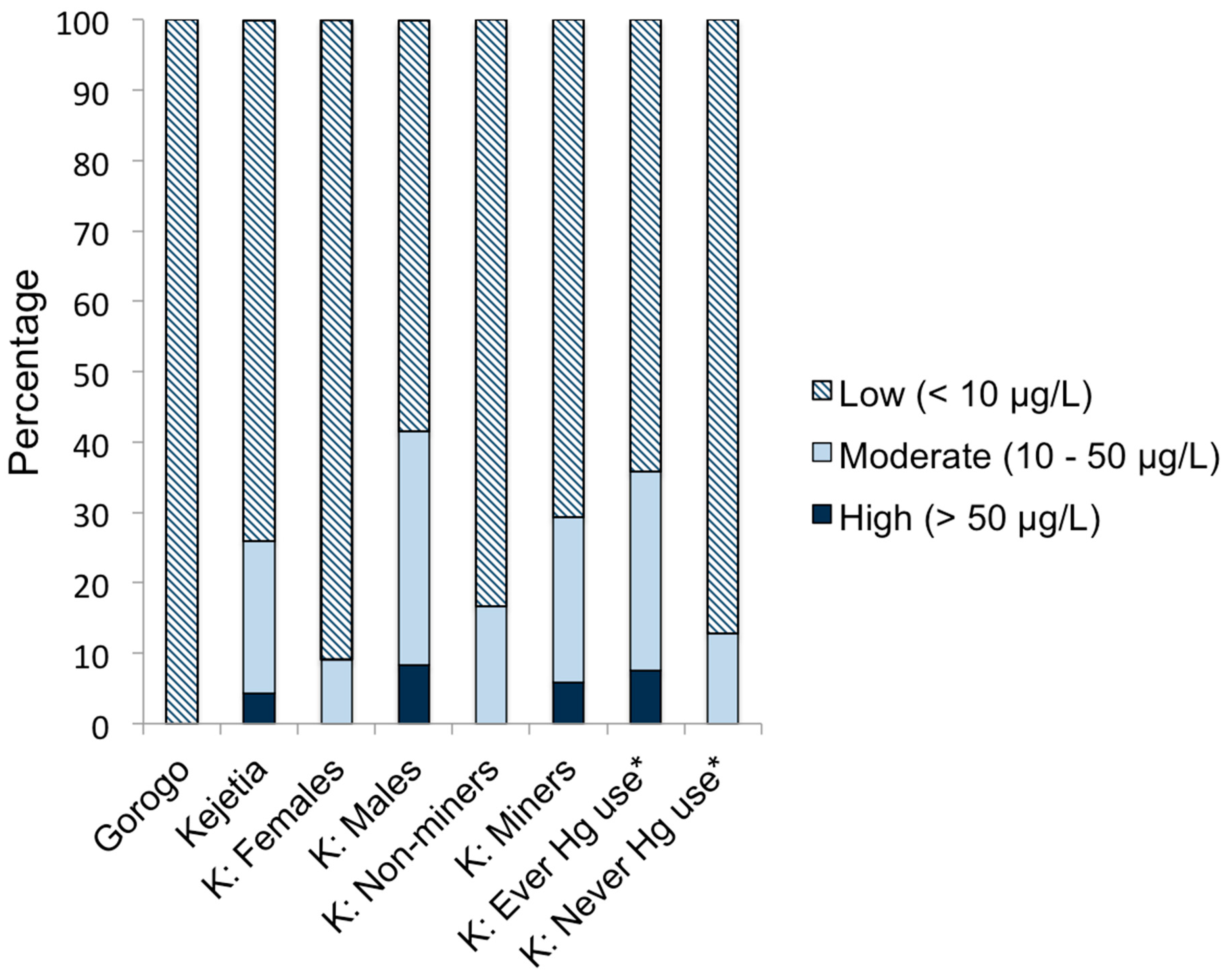
5]. Evidence in Kejetia and elsewhere show that its use is common in ASGM communities, posing potential risks for miners and community residents. While <10 µg/L Hg is expected to be asymptomatic [
40], women of childbearing age are recommended to be exposed to as little Hg as possible [
5]. The 24 Kejetia 2011 participants with SG-adjusted urinary Hg concentrations >10 µg/L may be at risk for Hg-induced toxicity [
5,
45]. Almost 17% of non-mining participants in Kejetia had urinary Hg concentrations >10 µg/L, suggesting that living within the community exposes residents to Hg vapor, even without engaging in mining directly. This may result from inhalation of directly burned elemental Hg or inhalation of volatilized soil Hg. This is particularly important for pregnant women and young children that also reside in these communities and are more vulnerable to the impacts of Hg exposure [
5].
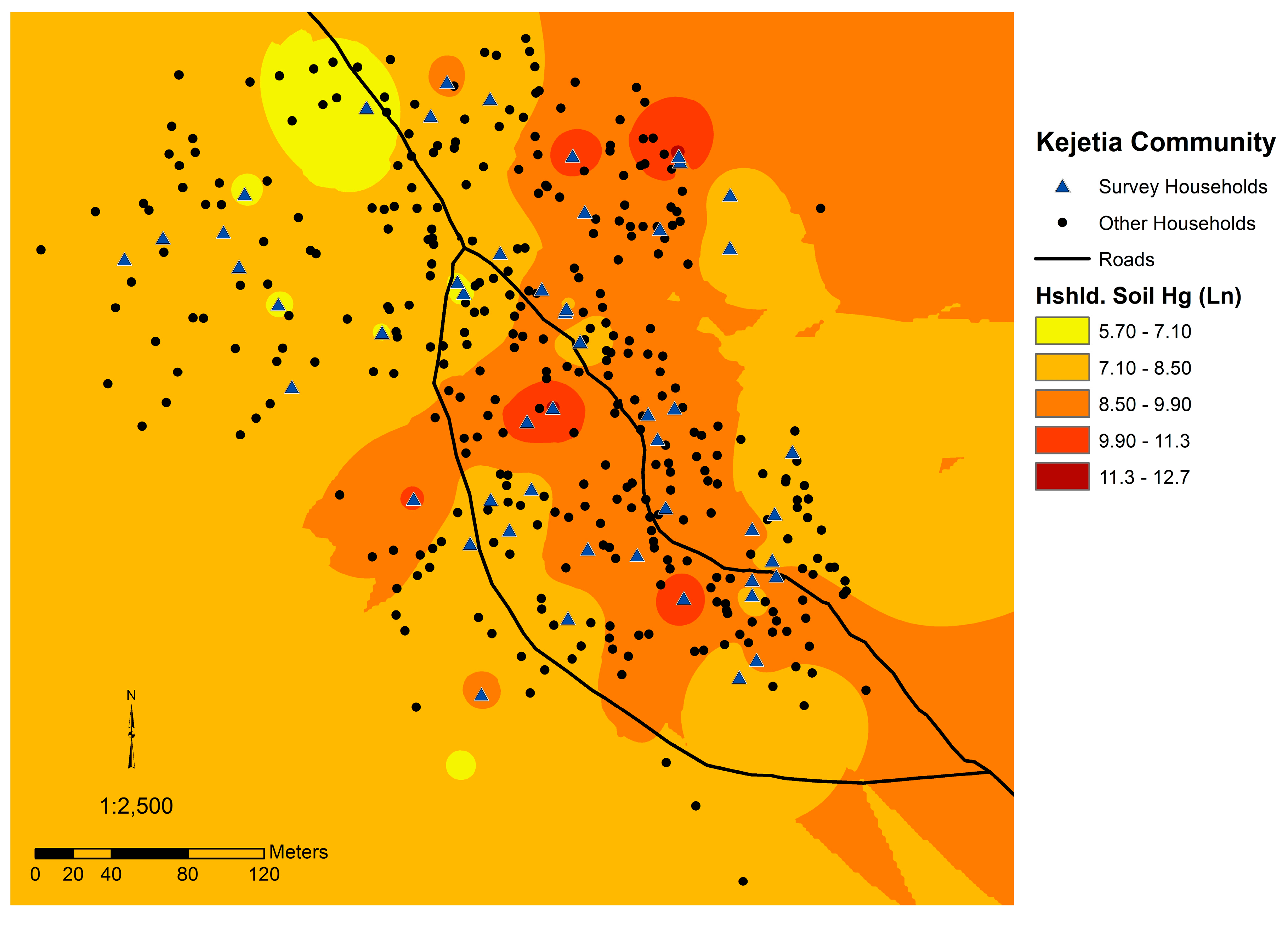
Household soil Hg concentrations were significantly higher in Kejetia than Gorogo. Household soil Hg was spatially autocorrelated and positively correlated to whether Kejetia participants were current miners and if they had ever burned Hg. Soil Hg in Kejetia (medians in 2010 and 2011, respectively: 2.16 and 3.05 µg/g; range: 0.096–330 µg/g), were similar to soil Hg levels from two ASGM villages in Zamfara, Nigeria (medians: 2.4 and 2.9 µg/g; range: 0.7–15.2 µg/g) [
19]. Mean Kejetia household soil Hg (15.55 µg/g) in 2011 was higher than measured in studies of 19 other ASGM areas across Ghana except for one study of four sites in the Western and Central Regions, which measured soil from active amalgamation and burning sites and found mean soil Hg levels of 0.93, 6.09, 21.6, and 185.93 µg/g [
7,
57]. Our study, however, focused on common areas where people spent their time to more appropriately reflect personal exposures for community residents. In other studies across Ghana, 21 out of 25 (84%) ASGM sampling sites measured mean soil levels below the Canadian Soil Quality Guideline for residential areas at 6.6 µg/g Hg, and 3 out of 25 (12%) were below 0.1 µg/g Hg [
7,
51,
57,
58,
59,
60,
61,
62,
63,
64,
65]. Household soil Hg in Gorogo (0.041 ± 0.023 µg/g) was lower than observed in other non-ASGM areas (means ranging from 0.099 to 0.170 µg/g) [
7,
51,
64].
High household soil Hg concentrations exceeding the Canadian Soil Quality Guideline for residential areas, which is set to protect human and environmental health, indicate an additional concern [
42]. One-third of 2011 Kejetia household soil Hg concentrations were above the Canadian Soil Quality Guideline of 6.6 µg/g Hg [
42,
45]. Kejetia household soil Hg was significantly correlated to urinary Hg in 2011, suggesting that Hg burning is occurring at or around participants’ homes and may be locally depositing in the community. The spatial autocorrelation of household soil and participants’ urinary Hg in Kejetia further supports this hypothesis. The correlation of urinary Hg and household soil may also be in indication of inhalation of evaporated elemental Hg from contaminated household soil. As seen in
Figure 2, mining activities occur throughout the community, which may explain why contamination and exposures are widespread in Kejetia.
Mean and median soil Hg concentrations from samples collected at the Bolgatanga refinery were higher than at Kejetia, Zamfara (Nigeria), and most other studies of ASGM sites in Ghana [
7,
19]. This is of concern given that such refineries are common across countries with active ASGM industries and are often situated outside the ASGM community in larger urban centers where few have explored Hg exposure issues. Concentrations of Hg from ore samples were relatively low compared to soil samples, but were greater than measured in Gorogo or other non-ASGM sites across Ghana [
7]. Sediment and fish samples were quite low, and all fell below guideline values except for one sediment sample [
43,
44].
Ingestion of soil, particularly through the practice of geophagy and pica, may be an additional pathway of exposure to Hg that is perhaps understudied in ASGM communities. The dusty environment in northern Ghana combined with the mining activities may also result in higher inadvertent soil ingestion. People may ingest soil and dust through hand-to-mouth contact, the air, and from soil and dust on skin, clothing, inanimate objects, and food. Although the prevalence of the practice of geophagy in northern Ghana is unknown, Vermeer’s study indicates it was common in the Volta Region in the 1970s (prevalent in 46.4% of adult females), and is still common in many Sub-Saharan African countries [
20,
21]. Vermeer also found that pica was common in 73.6% of adult females and 13.9% of adult males [
21]. The fractionation of Hg in household soil is unknown, however, and total Hg concentrations may not accurate reflect bioavailability.
Any Kejetia adults practicing geophagy and upper limit pica may be at risk of exceeding the U.S. EPA RfD for Hg ingestion, and still others may ingest quantities of Hg greater than the RfD in inadvertent ingestion. Children and youth, who ingest higher quantities of soil and dust and have greater hand-to-mouth contact, may have a larger burden of Hg exposure from soil and dust than adults. In geophagy, soil and clays may be purchased at markets from elsewhere, or be locally sourced from walls of houses, termite mounts, and ground soil [
21,
23]. Geophagic consumption of local or distant soils and involvement in ASGM would greatly influence Hg exposure. High soil concentrations around the refinery in Bolgatanga stress the important of studying urban areas where gold is refined, in addition to traditional ASGM areas where ore is processed.
As the share of global anthropogenic Hg from ASGM grows, there is increasing worldwide concern about its use. The Minamata Convention on Mercury is a global treaty working to reduce Hg emissions and mining with a particular focus on regulating the ASGM sector [
66]. Convention signatories, such as Ghana, are expected to take initiatives to reduce and when feasible eliminate the use of Hg and to develop a national action plan (Article 7, Annex C) including various elements such as reduction targets and baseline estimates of Hg used in ASGM [
66]. Studies such as this one provide necessary support for the Minamata Convention’s assessment of baseline Hg use and pollution in ASGM, particularly filling a knowledge gap in northern Ghana, since most studies have focused on southern Ghana.
Limitations
There are a number of limitations to consider for this study. Data on air Hg concentrations in homes and throughout the community would provide a more complete picture of exposure pathways. High household soil Hg concentrations may be a source of Hg vapor in homes and an additional inhalational exposure. The Canadian guideline values for Hg in soil and sediment are for non-tropical environments and do not include Hg speciation [
42,
43]. Owing to inconsistent practices, recipes, and meal sharing, and a lack of knowledge of fish species and origins, it is difficult to adequately quantify fish consumption for rural Ghanaians. An estimate of MeHg ingestion from fish consumption would help to better estimate the fraction of MeHg in ASGM community participants’ hair samples. However, utilizing Sherman
et al.’s study [
14], we have a suitable estimation of the proportion of MeHg in ASGM miners’ hair.
Many of the soil and dust ingestion scenarios from US-based assumptions of inadvertent ingestion and pica are inadequate for West Africans with different dietary habits, earthen floor housing, climate, local environments, and other factors [
19]. It is unclear what appropriate soil and dust ingestion rates are for rural northern Ghanaians, but the dusty conditions during the long dry season from October through April anecdotally imply higher ingestion rates [
67]. ASGM areas may also have higher ingestion rates as people work and live in close proximity to ore processing [
48]. Soil ingestion rates from Tanzanian studies reflect only soil ingestion, and may significantly underestimate total soil and dust ingestion in dusty conditions. Estimations of Hg ingestion from soil were based on household soil concentrations, although we do not have information on the source of soil for geophagy. In northeast Ghana and in a mining community in particular, individuals practicing geophagy may also intentionally obtain soils from outside their community, in community spaces, or from their homes.
The toxicity of Hg depends greatly on its speciation, which is unknown for Kejetia. A site contaminated with mercuric nitrate and elemental Hg in Tennessee, USA, measured total Hg from 0.5 to 3000 µg/g in floodplain soil [
68]. Only 0.01% was found to be organic Hg (MeHg), 6% was elemental Hg, and 91% was inorganic (primarily HgS) [
68]. A follow-up study at the same site 15 years later measured elemental Hg in 10%–30% of total Hg [
69]. At both time points, the soluble and bioavailable fractions were relatively small portions of the total Hg [
68,
69]. The presence of certain types of bacteria in the soil (e.g., sulfate-reducing bacteria), which is largely unknown for Ghana, can also influence the speciation in soil [
68]. In the absence of data on Hg speciation and fractionation in Kejetia, we rely on total Hg concentrations and must also include some uncertainty in our analyses. Further studies on the bioavailability of Hg from soil and dust and ingestion rates in rural, West African communities would aid in clarifying this exposure pathway. Additionally, the U.S. EPA RfD is for mercuric chloride and may not adequately assess risks from elemental Hg ingestion.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}