(Pro)renin Receptor Expression Increases throughout the Colorectal Adenoma—Adenocarcinoma Sequence and It Is Associated with Worse Colorectal Cancer Prognosis


Abstract
:1. Introduction
2. Results
2.1. Patients Clinical and Pathological Parameters
2.2. PRR Protein Expression in Human Colonic Tissues
2.2.1. PRR Expression According to the Gender and Age of the CRC Patients
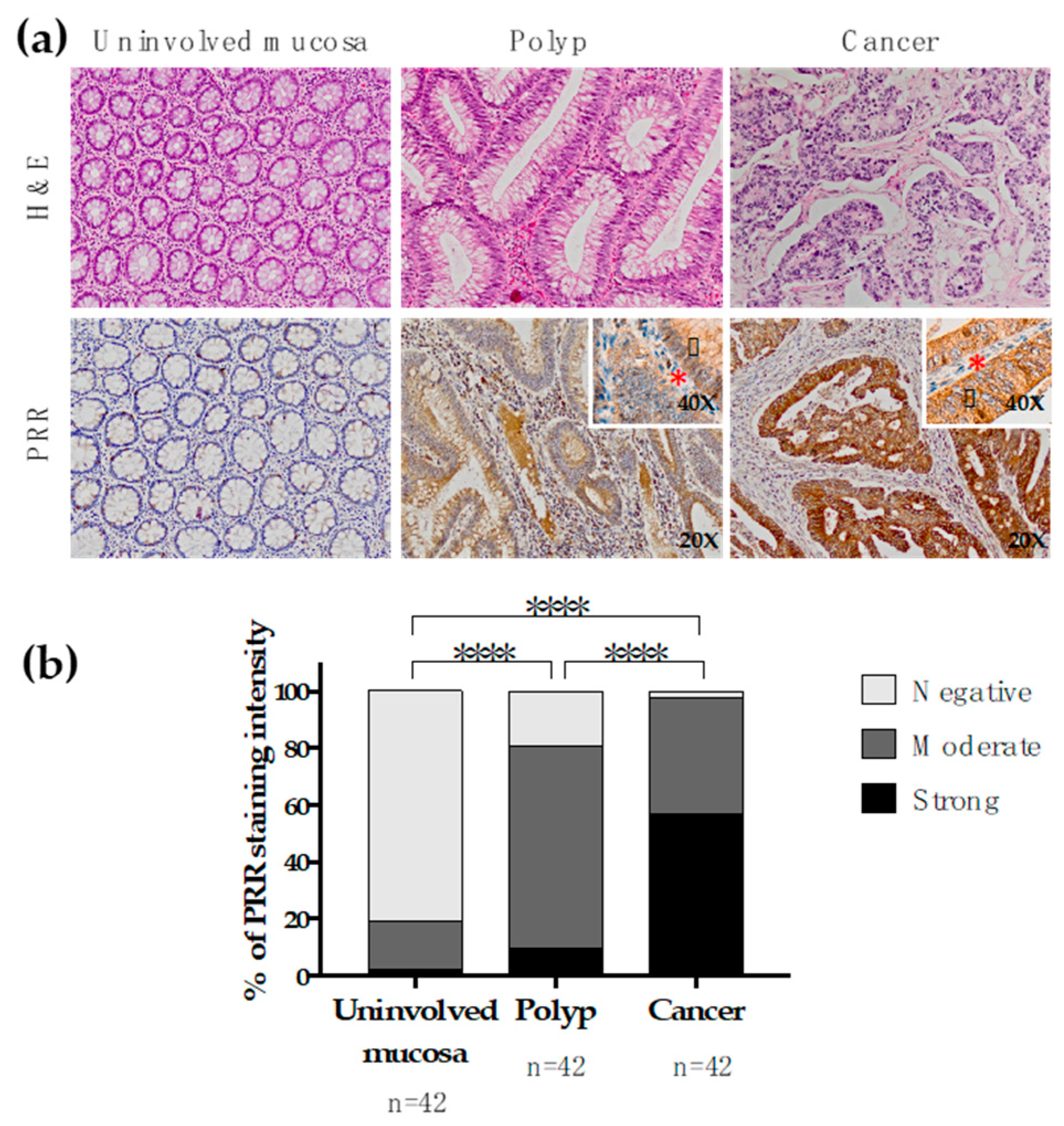
2.2.2. PRR Expression along the Polyp-Cancer Sequence
2.2.3. PRR Expression According to the Histologic Subtype
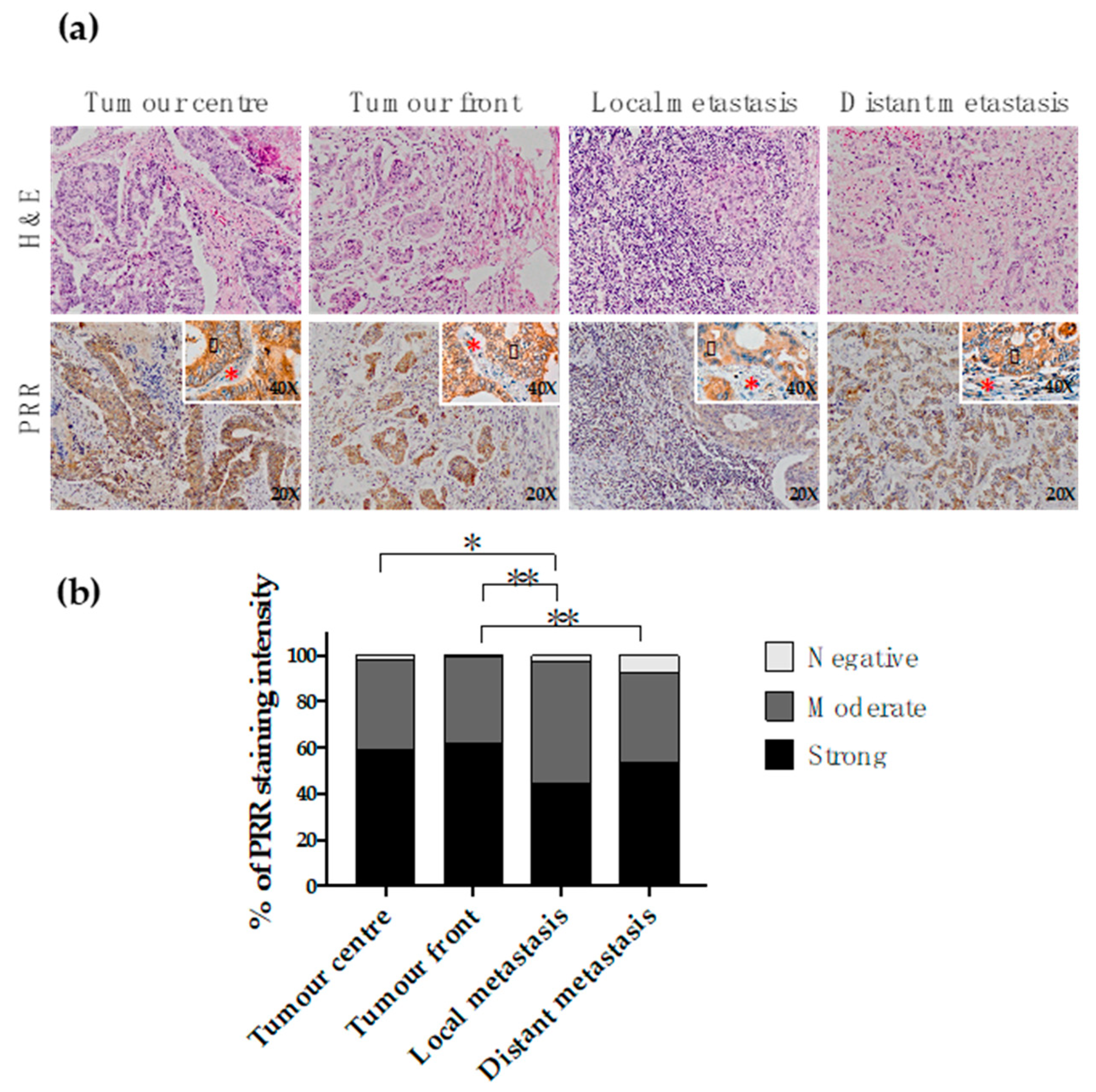
2.2.4. PRR Expression along the Conversion of the Primary Tumour into Metastasis
2.2.5. PRR Expression According to CRC Aggressiveness
2.2.6. PRR Expression According to the Overall Survival of CRC Patients
2.2.7. PRR Expression According to Disease-Free Survival of CRC Patients
2.2.8. PRR Expression According to the Tumour Budding
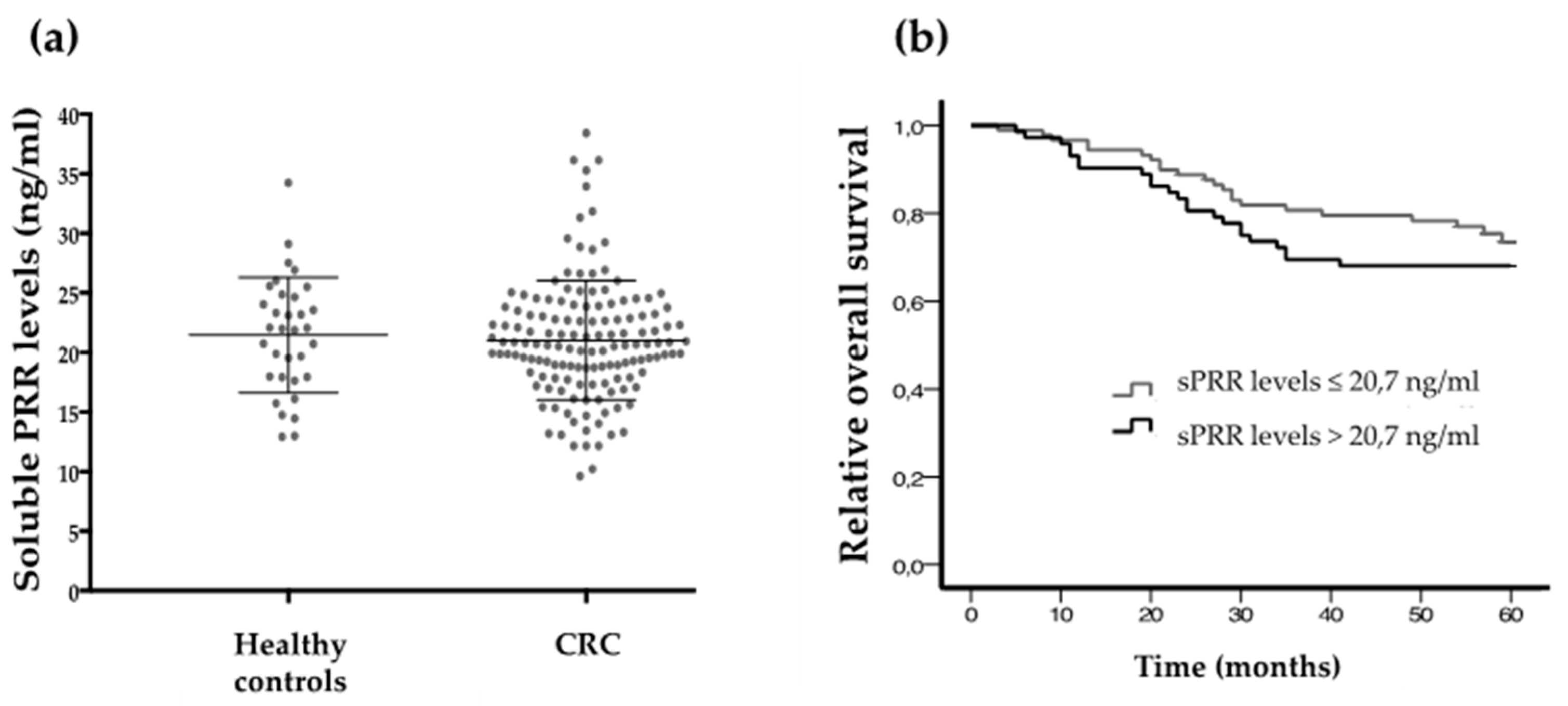
2.3. Soluble PRR Concentration According to CRC Aggressiveness and Patients Survival
3. Discussion
4. Materials and Methods
4.1. Immunohistochemistry
4.2. ELISA Assays
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, G.; Delarue, F.; Burcklé, C.; Bouzhir, L.; Giller, T.; Sraer, J.D. Pivotal role of the renin/prorenin receptor in angiotensin II production and cellular responses to renin. J. Clin. Investig. 2002, 109, 1417–1427. [Google Scholar] [CrossRef] [PubMed]
- Peach, M.J. Renin–angiotensin system: Biochemistry and mechanisms of action. Physiol. Rev. 1977, 57, 313–370. [Google Scholar] [CrossRef] [PubMed]
- Crowley, S.D.; Coffman, T.M. Recent advances involving the renin–angiotensin system. Exp. Cell Res. 2012, 318, 1049–1056. [Google Scholar] [CrossRef] [PubMed]
- Dzau, V.J.; Re, R. Tissue angiotensin system in cardiovascular medicine. A paradigm shift? Circulation 1994, 89, 493–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, A.J.; Thomas, W.G.; Hannan, R.D. The renin–angiotensin system and cancer: Old dog, new tricks. Nat. Rev. Cancer 2010, 10, 745–759. [Google Scholar] [CrossRef]
- Dolley–Hitze, T.; Jouan, F.; Martin, B.; Mottier, S.; Edeline, J.; Moranne, O.; Le Pogamp, P.; Belaud–Rotureau, M.A.; Patard, J.J.; Rioux–Leclercq, N.; et al. Angiotensin–2 receptors (AT1–R and AT2–R), new prognostic factors for renal clear–cell carcinoma? Br. J. Cancer 2010, 103, 1698–1705. [Google Scholar] [CrossRef]
- Han, C.D.; Ge, W.S. Up–regulation of Angiotensin–Converting Enzyme (ACE) enhances cell proliferation and predicts poor prognosis in laryngeal cancer. Med. Sci. Monit. 2016, 22, 4132–4138. [Google Scholar] [CrossRef]
- Shirotake, S.; Miyajima, A.; Kosaka, T.; Tanaka, N.; Maeda, T.; Kikuchi, E.; Oya, M. Angiotensin II type 1 receptor expression and microvessel density in human bladder cancer. Urology 2011, 77, 1009.e19–1009.e25. [Google Scholar] [CrossRef]
- Uemura, H.; Hasumi, H.; Ishiguro, H.; Teranishi, J.; Miyoshi, Y.; Kubota, Y. Renin-angiotensin system is an important factor in hormone refractory prostate cancer. Prostate 2006, 66, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, O.; Villarreal-Garza, C.; Vizcaíno, G.; Pineda, B.; Hernández-Pedro, N.; Guevara-Salazar, P.; Wegman-Ostrosky, T.; Villanueva–Rodríguez, G.; Gamboa–Domínguez, A. Association between AT1 and AT2 angiotensin II receptor expression with cell proliferation and angiogenesis in operable breast cancer. Tumour Biol. 2015, 36, 5627–5634. [Google Scholar] [CrossRef] [PubMed]
- Olschewski, D.N.; Hofschröer, V.; Nielsen, N.; Seidler, D.G.; Schwab, A.; Stock, C. The angiotensin II type 1 receptor antagonist losartan affects NHE1–dependent melanoma cell behavior. Cell. Physiol. Biochem. 2018, 45, 2560–2576. [Google Scholar] [CrossRef] [PubMed]
- Romero, C.A.; Orias, M.; Weir, M.R. Novel RAAS agonists and antagonists: Clinical applications and controversies. Nat. Rev. Endocrinol. 2015, 11, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Childers, W.K. Interactions of the renin–angiotensin system in colorectal cancer and metastasis. Int. J. Colorectal. Dis. 2015, 30, 749–752. [Google Scholar] [CrossRef] [PubMed]
- Faust, P.L.; Chirgwin, J.M.; Kornfeld, S. Renin, a secretory glycoprotein, acquires phosphomannosyl residues. J. Cell Biol. 1987, 105, 1947–1955. [Google Scholar] [CrossRef] [PubMed]
- Krop, M.; Danser, A.H.J. Circulating versus tissue renin–angiotensin system: on the origin of (pro)renin. Curr. Hypertens. Rep. 2008, 10, 112–118. [Google Scholar] [CrossRef]
- Huang, Y.; Wongamorntham, S.; Kasting, J.; McQuillan, D.; Owens, R.T.; Yu, L.; Noble, N.A.; Border, W. Renin increases mesangial cell transforming growth factor–beta1 and matrix proteins through receptor–mediated, angiotensin II–independent mechanisms. Kidney Int. 2006, 69, 105–113. [Google Scholar] [CrossRef]
- Huang, Y.; Noble, N.A.; Zhang, J.; Xu, C.; Border, W.A. Renin–stimulated TGF–beta1 expression is regulated by a mitogen–activated protein kinase in mesangial cells. Kidney Int. 2007, 72, 45–52. [Google Scholar] [CrossRef]
- Kaneshiro, Y.; Ichihara, A.; Takemitsu, T.; Sakoda, M.; Suzuki, F.; Nakagawa, T.; Hayashi, M.; Inagami, T. Increased expression of cyclooxygenase–2 in the renal cortex of human prorenin receptor gene–transgenic rats. Kidney Int. 2006, 70, 641–646. [Google Scholar] [CrossRef]
- Sakoda, M.; Ichihara, A.; Kaneshiro, Y.; Takemitsu, T.; Nakazato, Y.; Nabi, A.H.; Nakagawa, T.; Suzuki, F.; Inagami, T.; Itoh, H. (Pro)renin receptor-mediated activation of mitogen-activated protein kinases in human vascular smooth muscle cells. Hypertens. Res. 2007, 30, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Schefe, J.H.; Menk, M.; Reinemund, J.; Effertz, K.; Hobbs, R.M.; Pandolfi, P.P.; Ruiz, P.; Unger, T.; Funke–Kaiser, H. A novel signal transduction cascade involving direct physical interaction of the renin/prorenin receptor with the transcription factor promyelocytic zinc finger protein. Circ. Res. 2006, 99, 1355–1366. [Google Scholar] [CrossRef] [PubMed]
- Cruciat, C.M.; Ohkawara, B.; Acebron, S.P.; Karaulanov, E.; Reinhard, C.; Ingelfinger, D.; Boutros, M.; Niehrs, C. Requirement of prorenin receptor and vacuolar H+-ATPase–mediated acidification for Wnt signaling. Science 2010, 327, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Bienz, M.; Clevers, H. Linking colorectal cancer to Wnt signaling. Cell 2000, 103, 311–320. [Google Scholar] [CrossRef]
- Clevers, H. The intestinal crypt, a prototype stem cell compartment. Cell 2013, 154, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, J.; Kerscher, S.; Brandt, U.; Pfeiffer, K.; Getlawi, F.; Apps, D.K.; Schägger, H. Identification and characterization of a novel 9.2–kDa membrane sector–associated protein of vacuolar proton–ATPase from chromaffin granules. J. Biol. Chem. 1998, 273, 10939–10947. [Google Scholar] [CrossRef]
- Stransky, L.; Cotter, K.; Forgac, M. The function of V–ATPases in cancer. Physiol. Rev. 2016, 96, 1071–1091. [Google Scholar] [CrossRef] [PubMed]
- Cousin, C.; Bracquart, D.; Contrepas, A.; Corvol, P.; Muller, L.; Nguyen, G. Soluble form of the (pro)renin receptor generated by intracellular cleavage by furin is secreted in plasma. Hypertension 2009, 53, 1077–1082. [Google Scholar] [CrossRef]
- Ichihara, A.; Sakoda, M.; Kurauchi–Mito, A.; Narita, T.; Kinouchi, K.; Murohashi–Bokuda, K.; Itoh, H. Possible roles of human (pro)renin receptor suggested by recent clinical and experimental findings. Hypertens. Res. 2010, 33, 177–180. [Google Scholar] [CrossRef]
- Yoshikawa, A.; Aizaki, Y.; Kusano, K.; Kishi, F.; Susumu, T.; Iida, S.; Ishiura, S.; Nishimura, S.; Shichiri, M.; Senbonmatsu, T. The (pro)renin receptor is cleaved by ADAM19 in the Golgi leading to its secretion into extracellular space. Hypertens. Res. 2011, 34, 599–605. [Google Scholar] [CrossRef] [Green Version]
- Arundhathi, A.; Chuang, W.H.; Chen, J.K.; Wang, S.E.; Shyr, Y.M.; Chen, J.Y.; Liao, W.N.; Chen, H.W.; Teng, Y.M.; Pai, C.C.; et al. Prorenin receptor acts as a potential molecular target for pancreatic ductal adenocarcinoma diagnosis. Oncotarget 2016, 7, 55437–55448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delforce, S.J.; Lumbers, E.R.; de Meaultsart, C.C.; Wang, Y.; Proietto, A.; Otton, G.; Scurry, J.; Verrills, N.M.; Scott, R.J.; Pringle, K.G. Expression of renin-angiotensin system (RAS) components in endometrial cancer. Endocr. Connect. 2017, 6, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Ishizuka, E.T.; Kanda, A.; Kase, S.; Noda, K.; Ishida, S. Involvement of the receptor–associated prorenin system in the pathogenesis of human conjunctival lymphoma. Invest. Ophthalmol. Vis. Sci. 2014, 56, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Ohba, K.; Suzuki, T.; Nishiyama, H.; Kaneko, K.; Hirose, T.; Totsune, K.; Sasano, H.; Takahashi, K. Expression of (pro)renin receptor in breast cancers and its effect on cancercell proliferation. Biomed. Res. 2014, 35, 117–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sennoune, S.R.; Bermudez, L.E.; Lees, J.C.; Hirsch, J.; Filleur, S.; Martínez–Zaguilán, R. Vacuolar H+-ATPase is down–regulated by the angiogenesis–inhibitory pigment epithelium–derived factor in metastatic prostate cancer cells. Cell. Mol. Biol. 2014, 60, 45–52. [Google Scholar] [PubMed]
- Shibayama, Y.; Fujimori, T.; Nguyen, G.; Hirose, T.; Totsune, K.; Ichihara, A.; Kitada, K.; Nakano, D.; Kobori, H.; Kohno, M.; et al. (Pro)renin receptor is crucial for Wnt/β–catenin–dependent genesis of pancreatic ductal adenocarcinoma. Sci. Rep. 2015, 5, 8854. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Shibayama, Y.; Zhang, A.; Ohsaki, H.; Asano, E.; Suzuki, Y.; Kushida, Y.; Kobara, H.; Masaki, T.; Wang, Z.; et al. (Pro)renin receptor promotes colorectal cancer through the Wnt/beta–catenin signalling pathway despite constitutive pathway component mutations. Br. J. Cancer 2018, 120, 229–237. [Google Scholar] [CrossRef]
- Fenocchio, E.; Colombi, F.; Calella, M.G.; Filippi, R.; Depetris, I.; Chilà, G.; Lombardi, P.; Marino, D.; Cagnazzo, C.; Ferraris, R.; et al. Improvement of metastatic colorectal cancer patient survival: single institution experience. Cancers 2019, 11, 369. [Google Scholar] [CrossRef]
- Fearon, E.R. Molecular genetics of colorectal cancer. Annu. Rev. Pathol. 2011, 6, 479–507. [Google Scholar] [CrossRef]
- Fearon, E.R.; Vogelstein, B. A genetic model for colorectal tumorigenesis. Cell 1990, 61, 759–767. [Google Scholar] [CrossRef]
- Jass, J.R. Classification of colorectal cancer based on correlation of clinical, morphological and molecular features. Histopathology 2007, 50, 113–130. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Wang, L.; Wang, J. Developing proteomics–based biomarkers for colorectal neoplasms for clinical practice: opportunities and challenges. Proteom. Clin. Appl. 2013, 7, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Bosman, F.T.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO Classification of Tumours of the Digestive System; International Agency for Research on Cancer, Elsevier: Lyon, France, 2010. [Google Scholar]
- Odze, R.D.; Goldblum, J.R. Odze and Goldblum Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas E–Book; Elsevier Health Sciences: Philadelphia, PA, USA, 2014; ISBN 978-1-4557-3324-8. [Google Scholar]
- Koelzer, V.H.; Lugli, A. The tumor border configuration of colorectal cancer as a histomorphological prognostic indicator. Front. Oncol. 2014, 4, 29. [Google Scholar] [CrossRef] [PubMed]
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Fléjou, J.F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod. Pathol. 2017, 30, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Zennaro, C.; Palmisano, S.; Velkoska, E.; Sabato, N.; Toffoli, B.; Giacomel, G.; Buri, L.; Zanconati, F.; Bellini, G.; et al. Characterization and significance of ACE2 and Mas receptor in human colon adenocarcinoma. J. Renin Angiotensin Aldosterone Syst. 2012, 13, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Luo, Y.; Sato, S.; Tanabe, E.; Kitayoshi, M.; Fujiwara, R.; Sasaki, T.; Fujii, K.; Ohmori, H.; Kuniyasu, H. Role of two types of angiotensin II receptors in colorectal carcinoma progression. Pathobiology 2014, 81, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Larrinaga, G.; Perez, I.; Ariz, U.; Sanz, B.; Beitia, M.; Errarte, P.; Etxezarraga, C.; Candenas, M.L.; Pinto, F.M.; López, J.I. Clinical impact of aspartyl aminopeptidase expression and activity in colorectal cancer. Transl. Res. 2013, 162, 297–308. [Google Scholar] [CrossRef]
- Sanz, B.; Perez, I.; Beitia, M.; Errarte, P.; Fernández, A.; Blanco, L.; Estalella, I.; Loizate, A.; Irazusta, J.; López, J.I.; et al. Aminopeptidase N activity predicts 5–year survival in colorectal cancer patients. J. Investig. Med. 2015, 63, 740–746. [Google Scholar] [CrossRef]
- Beitia, M.; Solano–Iturri, J.D.; Errarte, P.; Sanz, B.; Perez, I.; Etxezarraga, C.; Loizate, A.; Asumedi, A.; Larrinaga, G. Altered expression of renin–angiotensin system receptors throughout colorectal adenoma–adenocarcinoma sequence. Int. J. Med. Sci. 2019, 16, 813–821. [Google Scholar] [CrossRef]
- Wegman–Ostrosky, T.; Soto–Reyes, E.; Vidal–Millán, S.; Sánchez–Corona, J. The renin–angiotensin system meets the hallmarks of cancer. J. Renin Angiotensin Aldosterone Syst. 2015, 16, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Osumi, H.; Matsusaka, S.; Wakatsuki, T.; Suenaga, M.; Shinozaki, E.; Mizunuma, N. Angiotensin II type–1 receptor blockers enhance the effects of bevacizumab-based chemotherapy in metastatic colorectal cancer patients. Mol. Clin. Oncol. 2015, 3, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, N.; Segawa, T.; Kinoshita, N.; Ichihara, A. Novel sandwich ELISA for detecting the human soluble (pro)renin receptor. Front. Biosci. 2013, 5, 583–590. [Google Scholar] [CrossRef]
- Zhu, Q.; Yang, T. Enzymatic sources and physio-pathological functions of soluble (pro)renin receptor. Curr. Opin. Nephrol. Hypertens. 2018, 27, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Palmirotta, R.; Lovero, D.; Cafforio, P.; Felici, C.; Mannavola, F.; Pellè, E.; Quaresmini, D.; Tucci, M.; Silvestris, F. Liquid biopsy of cancer: a multimodal diagnostic tool in clinical oncology. Ther. Adv. Med. Oncol. 2018, 10, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Marrugo–Ramírez, J.; Mir, M.; Samitier, J. Blood–based cancer biomarkers in liquid biopsy: A promising non–invasive alternative to tissue biopsy. Int. J. Mol. Sci. 2018, 19, 2877. [Google Scholar] [CrossRef] [PubMed]
- Perez, I.; Blanco, L.; Sanz, B.; Errarte, P.; Ariz, U.; Beitia, M.; Fernández, A.; Loizate, A.; Candenas, M.L.; Pinto, F.M.; et al. Altered activity and expression of cytosolic peptidases in colorectal cancer. Int. J. Med. Sci. 2015, 12, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Errarte, P.; Beitia, M.; Perez, I.; Manterola, L.; Lawrie, C.H.; Solano–Iturri, J.D.; Calvete–Candenas, J.; Unda, M.; López, J.I.; Larrinaga, G. Expression and activity of angiotensin–regulating enzymes is associated with prognostic outcome in clear cell renal cell carcinoma patients. PLoS ONE 2017, 12, e0181711. [Google Scholar] [CrossRef] [PubMed]
- Daryadel, A.; Bourgeois, S.; Figueiredo, M.F.L.; Gomes Moreira, A.; Kampik, N.B.; Oberli, L.; Mohebbi, N.; Lu, X.; Meima, M.E.; Danser, A.H.J.; et al. Colocalization of the (Pro)renin receptor/Atp6ap2 with H+-ATPases in mouse kidney but prorenin does not acutely regulate intercalated cell H+-ATPase activity. PLoS ONE 2016, 11, e0147831. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Rehman, A.U.; Zuo, C.; Sheehan, C.E.; Lee, E.C.; Lin, J.; Zhao, Z.; Choi, E.; Lee, H. A novel histologic grading scheme based on poorly differentiated clusters is applicable to treated rectal cancer and is associated with established histopathological prognosticators. Cancer Med. 2016, 5, 1510–1518. [Google Scholar] [CrossRef] [Green Version]
- Lee, V.W.K.; Chan, K.F. Tumor budding and poorly–differentiated cluster in prognostication in Stage II colon cancer. Pathol. Res. Pract. 2018, 214, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.; Murphy, J.; Jass, J.R.; Mochizuki, H.; Talbot, I.C. Tumour “budding” as an index to estimate the potential of aggressiveness in rectal cancer. Histopathology 2002, 40, 127–132. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Clinical and Pathological Data (n = 294) | Average (%) | |
|---|---|---|
| Age average (range) | 70 (29–93) | |
| Follow-up months (range) | 44 (0–188) | |
| Gender | Male | 203 (69%) |
| Female | 91 (31%) | |
| Histologic subtype | Intestinal-type Adenocarcinoma (AdC) | 231 (79%) |
| Mucinous carcinoma (MuC) | 50 (17%) | |
| Signet ring cell carcinoma (SrcC) | 13 (4%) | |
| Histologic grade (G) | G1 | 37 (13%) |
| G2 | 161 (55%) | |
| G3 | 95 (32%) | |
| Local invasion (pT) | pT1 | 2 (<1%) |
| pT2 | 13 (4%) | |
| pT3 | 178 (61%) | |
| pT4 | 101 (34%) | |
| Affected lymph nodes (N) | N0 | 37 (13%) |
| N1 | 161 (55%) | |
| N2 | 95 (32%) | |
| Distant metastases (M) | M0 | 182 (62%) |
| M1 | 112 (38%) | |
| Stage (TNM system) * | I | 7 (2%) |
| II | 25 (9%) | |
| III | 150 (51%) | |
| IV | 112 (38%) | |
| Heading | Negative Staining (%) | Moderate Staining (%) | Strong Staining (%) | Chi-square (p value) | |
|---|---|---|---|---|---|
| Tumour centre | Adenocarcinoma (AdC) | 2.2 | 39.0 | 58.8 | 9 × 10−6 a |
| Mucinous carcinoma (MuC) | 4.1 | 75.5 | 20.4 | ||
| Signet ring cell carcinoma (SrcC) | 0.0 | 76.9 | 23.1 | ||
| Tumour front | Adenocarcinoma (AdC) | 0.9 | 37.4 | 61.7 | 0.001 b |
| Mucinous carcinoma (MuC) | 4.4 | 60.0 | 35.6 | ||
| Signet ring cell carcinoma (SrcC) | 0.0 | 81.8 | 18.2 | ||
| Local metastasis | Adenocarcinoma (AdC) | 2.8 | 52.3 | 44.9 | 0.024 c |
| Mucinous carcinoma (MuC) | 11.1 | 55.6 | 33.3 | ||
| Signet ring cell carcinoma (SrcC) | 0.0 | 84.6 | 15.4 | ||
| Distant metastasis | Adenocarcinoma (AdC) | 7.4 | 39.4 | 53.2 | 0.003 d |
| Mucinous carcinoma (MuC) | 15.8 | 73.7 | 10.5 | ||
| Signet ring cell carcinoma (SrcC) | 28.6 | 57.1 | 14.3 | ||
| Tumour Centre | Tumour Front | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Negative Staining (%) | Moderate Staining (%) | Strong Staining (%) | Chi-square (p value) | Negative Staining (%) | Moderate Staining (%) | Strong Staining (%) | Chi-square (p value) | ||
| Grade | 1 | 2.8 | 41.7 | 55.6 | 0.55 | 0 | 37.5 | 62.5 | 0.270 |
| 2 | 1.3 | 39.2 | 59.5 | 0.6 | 34.6 | 64.7 | |||
| 3 | 5.9 | 35.3 | 58.8 | 2.9 | 50 | 47.1 | |||
| pT | pT1–pT2 | 0 | 64.3 | 35.7 | 0.001 a | 0 | 71.4 | 28.6 | 0.051 b |
| pT3 | 0.7 | 44.7 | 54.7 | 1.4 | 37.2 | 61.4 | |||
| pT4 | 6.3 | 20.3 | 73.4 | 0 | 30.2 | 69.8 | |||
| N | N0 | 2.7 | 48.6 | 48.6 | 0.038 c | 2.8 | 41.7 | 55.6 | 0.564 |
| N1 | 0 | 43.5 | 56.5 | 0.9 | 37.7 | 61.3 | |||
| N2 | 4.8 | 28.9 | 66.3 | 0 | 35 | 65 | |||
| M | M0 | 3 | 47.8 | 49.3 | 0.002 | 0 | 45.4 | 54.6 | 0.005 |
| M1 | 1.1 | 26.6 | 72.3 | 2.2 | 26.1 | 71.7 | |||
| Stage | I-II | 4.2 | 62.5 | 33.3 | 0.004 d | 0 | 52.2 | 47.8 | 0.023 e |
| III | 2.7 | 44.5 | 52.7 | 0 | 43.9 | 56.1 | |||
| IV | 1.1 | 26.6 | 72.3 | 2.2 | 26.1 | 71.7 | |||
| PRR Protein Expression | Cut-off | Follow-up Time | n (%) | Log-Rank (p value) |
|---|---|---|---|---|
| Tumour centre | Moderate staining/Strong staining | 60 months | Alive 58 (26%) Dead 165 (74%) | 0.013 |
| 120 months | Alive 15 (7%) Dead 208 (93%) | 0.038 | ||
| Tumour front | Moderate staining/Strong staining | 60 months | Alive 58 (26%) Dead 162 (74%) | 0.051 |
| 120 months | Alive 15 (7%) Dead 205 (93%) | 0.062 | ||
| Local metastasis | Moderate staining/Strong staining | 60 months | Alive 41 (24%) Dead 130 (76%) | 0.029 |
| 120 months | Alive 14 (8%) Dead 157 (92%) | 0.038 | ||
| Distant metastasis | Moderate staining/Strong staining | 60 months | Alive 21 (24%) Dead 66 (76%) | 0.019 |
| 120 months | Alive 3 (3%) Dead 84 (97%) | 0.037 |
| Variables | Grade | pT | N | M | PRR | |
|---|---|---|---|---|---|---|
| Tumour Centre | p value | 0.032 | 3.9 × 10−4 | 0.777 | 6.4 × 10−5 | 0.599 |
| OR | 1.376 | 1.728 | 1.035 | 1.915 | 1.095 | |
| Inferior | 1.028 | 1.277 | 0.818 | 1.392 | 0.780 | |
| Superior | 1.841 | 2.337 | 1.308 | 2.633 | 1.537 | |
| Local Metastasis | p value | 0.087 | 0.002 | 0.903 | 2.6 × 10−4 | 0.089 |
| OR | 1.334 | 1.689 | 0.980 | 1.939 | 1.358 | |
| Inferior | 0.959 | 1.214 | 0.703 | 1.359 | 0.954 | |
| Superior | 1.855 | 2.351 | 1.365 | 2.768 | 1.933 | |
| Distant Metastasis | p value | 0.708 | 0.400 | 0.098 | 0.021 | 0.058 |
| OR | 1.091 | 1.214 | 1.344 | 1.888 | 1.683 | |
| Inferior | 0.692 | 0.772 | 0.947 | 1.100 | 0.982 | |
| Superior | 1.720 | 1.909 | 1.909 | 3.242 | 2.882 |
| Multiple Logistic Regresssion | Final Step of the Wald Method | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Grade | pT | N | PRR | PRR | pT | |
| Tumour centre | p value | 0.55 | 0.09 | 0.58 | 0.003 | 0.002 | 0.09 |
| B | 0.24 | 1.36 | 0.25 | 0.87 | 0.92 | 1.35 | |
| OR | 1.28 | 3.9 | 1.28 | 2.39 | 2.5 | 3.85 | |
| Inferior | 0.57 | 0.78 | 0.53 | 1.33 | 1.4 | 0.82 | |
| Superior | 2.8 | 19.3 | 3.1 | 4.3 | 4.46 | 18.03 | |
| Tumour front | p value | 0.69 | 0.15 | 0.45 | 0.01 | 0.005 | - |
| B | 0.16 | 1.17 | 0.34 | 0.76 | 0.83 | - | |
| OR | 1.18 | 3.23 | 1.41 | 2.14 | 2.28 | - | |
| Inferior | 0.53 | 0.66 | 0.58 | 1.18 | 1.28 | - | |
| Superior | 2.61 | 15.8 | 3.43 | 3.89 | 4.08 | - | |
| Patients’ Clinical and Pathological Sata (n = 161) | Average (%) | sPRR Levels (ng/mL) | p value | |
|---|---|---|---|---|
| Follow-up months (range) | 50 (3–84) | |||
| Age average (range) | 70 (34–93) | |||
| Gender | Male | 103 (72%) | ||
| Female | 41 (28%) | |||
| Histologic subtype | Intestinal-type adenocarcinoma (AdC) | 128 (89%) | 21.12 | 0.331 |
| Mucinous carcinoma (MuC) | 16 (11%) | 20.22 | ||
| Histologic grade (G) | G1 | 6 (4%) | 19.49 | 0.676 |
| G2 | 119 (83%) | 21.16 | ||
| G3 | 19 (13%) | 20.60 | ||
| Local invasion (pT) | pT2 | 36 (25%) | 20.59 | 0.561 |
| pT3 | 94 (65%) | 20.99 | ||
| pT4 | 14 (10%) | 22.29 | ||
| Affected lymph nodes (N) | N0 | 82 (57%) | 21.25 | |
| N1 | 48 (33%) | 20.61 | 0.781 | |
| N2 | 14 (10%) | 21.07 | ||
| Stage (TNM system) | I | 28 (19%) | 20.69 | |
| II | 53 (37%) | 21.35 | ||
| III | 59 (41%) | 21.18 | 0.296 | |
| IV | 4 (3%) | 16.49 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beitia, M.; Solano-Iturri, J.D.; Errarte, P.; Calvete-Candenas, J.; Loizate, A.; Etxezarraga, M.C.; Sanz, B.; Larrinaga, G. (Pro)renin Receptor Expression Increases throughout the Colorectal Adenoma—Adenocarcinoma Sequence and It Is Associated with Worse Colorectal Cancer Prognosis. Cancers 2019, 11, 881. https://doi.org/10.3390/cancers11060881
Beitia M, Solano-Iturri JD, Errarte P, Calvete-Candenas J, Loizate A, Etxezarraga MC, Sanz B, Larrinaga G. (Pro)renin Receptor Expression Increases throughout the Colorectal Adenoma—Adenocarcinoma Sequence and It Is Associated with Worse Colorectal Cancer Prognosis. Cancers. 2019; 11(6):881. https://doi.org/10.3390/cancers11060881
Chicago/Turabian StyleBeitia, Maider, Jon Danel Solano-Iturri, Peio Errarte, Julio Calvete-Candenas, Alberto Loizate, Mari Carmen Etxezarraga, Begoña Sanz, and Gorka Larrinaga. 2019. "(Pro)renin Receptor Expression Increases throughout the Colorectal Adenoma—Adenocarcinoma Sequence and It Is Associated with Worse Colorectal Cancer Prognosis" Cancers 11, no. 6: 881. https://doi.org/10.3390/cancers11060881