Long-Term Cognitive Performance of Retired Athletes with Sport-Related Concussion: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Assessment of Risk of Bias
2.5. Synthesized Analysis
3. Results
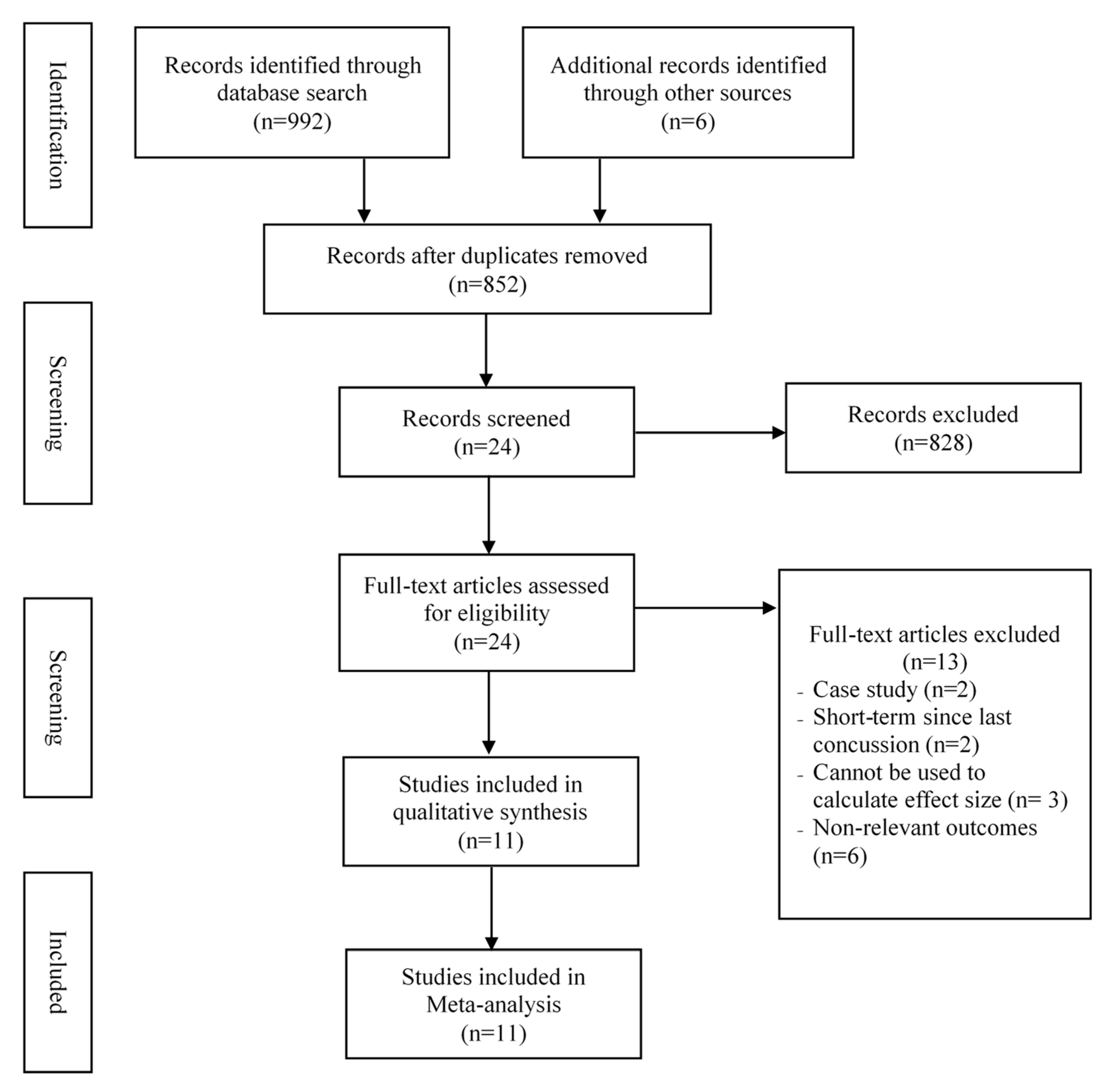
3.1. Search Results
3.2. Characteristics and Risk of Bias of Included Studies
3.3. Meta-Analysis of Cognitive Performance
3.4. Moderator Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McCrory, P.; Meeuwisse, W.H.; Aubry, M.; Cantu, R.C.; Dvorák, J.; Echemendia, R.J.; Engebretsen, L.; Johnston, K.M.; Kutcher, J.S.; Raftery, M.; et al. Consensus Statement on Concussion in Sport-The 4th International Conference on Concussion in Sport Held in Zurich, November 2012. PM R 2013, 5, 255–279. [Google Scholar] [CrossRef] [PubMed]
- Rice, S.M.; Parker, A.G.; Rosenbaum, S.; Bailey, A.; Mawren, D.; Purcell, R. Sport-Related Concussion and Mental Health Outcomes in Elite Athletes: A Systematic Review. Sport. Med. 2018, 48, 447–465. [Google Scholar] [CrossRef] [PubMed]
- Dougan, B.K.; Horswill, M.S.; Geffen, G.M. Athletes’ age, sex, and years of education moderate the acute neuropsychological impact of sports-related concussion: A meta-analysis. J. Int. Neuropsychol. Soc. 2014, 20, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Howell, D.; Osternig, L.; Van Donkelaar, P.; Mayr, U.; Chou, L.S. Effects of concussion on attention and executive function in adolescents. Med. Sci. Sports Exerc. 2013, 45, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Ledwidge, P.S.; Molfese, D.L. Long-Term Effects of Concussion on Electrophysiological Indices of Attention in Varsity College Athletes: An Event-Related Potential and Standardized Low-Resolution Brain Electromagnetic Tomography Approach. J. Neurotrauma 2016, 33, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Langlois, J.A.; Rutland-Brown, W.; Wald, M.M. The Epidemiology and Impact of Traumatic Brain Injury. J. Head Trauma Rehabil. 2009, 21, 375–378. [Google Scholar] [CrossRef]
- Daneshvar, D.H.; Nowinski, C.J.; McKee, A.C.; Cantu, R.C. The epidemiology of sport-related concussion. Clin. Sports Med. 2011, 30, 1–7. [Google Scholar] [CrossRef]
- Broglio, S.P.; Puetz, T.W. The effect of sport concussion on neurocognitive function, self-report symptoms and postural control: A meta-analysis. Sport. Med. 2008, 38, 53–67. [Google Scholar] [CrossRef]
- Henry, L.C.; Tremblay, S.; Boulanger, Y.; Ellemberg, D.; Lassonde, M. Neurometabolic Changes in the Acute Phase after Sports Concussions Correlate with Symptom Severity. J. Neurotrauma 2009, 27, 65–76. [Google Scholar] [CrossRef]
- Iverson, G.L.; Gaetz, M.; Lovell, M.R.; Collins, M.W. Cumulative effects of concussion in amateur athletes. Brain Inj. 2004, 18, 433–443. [Google Scholar] [CrossRef]
- McCrea, M.; Guskiewicz, K.M.; Marshall, S.W.; Barr, W.; Randolph, C.; Cantu, R.C.; Onate, J.A.; Yang, J.; Kelly, J.P. Acute Effects and Recovery Time Following Concussion in Collegiate Football Players: The NCAA Concussion Study. J. Am. Med. Assoc. 2003, 290, 2556–2563. [Google Scholar] [CrossRef] [PubMed]
- Sufrinko, A.; Pearce, K.; Elbin, R.J.; Covassin, T.; Johnson, E.; Collins, M.; Kontos, A.P. The effect of preinjury sleep difficulties on neurocognitive impairment and symptoms after sport-related concussion. Am. J. Sports Med. 2015, 43, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Matser, J.T.; Kessels, A.G.H.; Lezak, M.D.; Troost, J. A Dose-Response Relation of Headers and Concussions With Cognitive Impairment in Professional Soccer Players. J. Clin. Exp. Neuropsychol. 2003, 23, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Belanger, H.G.; Vanderploeg, R.D. The neuropsychological impact of sports-related concussion: A meta-analysis. J. Int. Neuropsychol. Soc. 2005, 11, 345–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAllister, T.W.; Flashman, L.A.; Maerlender, A.; Greenwald, R.M.; Beckwith, J.G.; Tosteson, T.D.; Crisco, J.J.; Brolinson, P.G.; Duma, S.M.; Duhaime, A.-C.; et al. Cognitive effects of one season of head impacts in a cohort of collegiate contact sport athletes. Neurology 2012, 78, 1777–1784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martini, D.N.; Broglio, S.P. Long-term effects of sport concussion on cognitive and motor performance: A review. Int. J. Psychophysiol. 2018, 132, 25–30. [Google Scholar] [CrossRef]
- McAllister, T.; McCrea, M. Long-Term Cognitive and Neuropsychiatric Consequences of Repetitive Concussion and Head-Impact Exposure. J. Athl. Train. 2017, 52, 309–317. [Google Scholar] [CrossRef]
- Guskiewicz, K.M.; Marshall, S.W.; Bailes, J.; McCrea, M.; Cantu, R.C.; Randolph, C.; Jordan, B.D. Association between recurrent concussion and late-life cognitive impairment in retired professional football players. Neurosurgery 2005, 57, 719–726. [Google Scholar] [CrossRef]
- Hinton, P.S.; Johnstone, B.; Blaine, E.; Bodling, A. Effects of current exercise and diet on late-life cognitive health of former college football players. Phys. Sportsmed. 2011, 39, 11–22. [Google Scholar] [CrossRef]
- Montenigro, P.H.; Alosco, M.L.; Martin, B.M.; Daneshvar, D.H.; Mez, J.; Chaisson, C.E.; Nowinski, C.J.; Au, R.; McKee, A.C.; Cantu, R.C.; et al. Cumulative Head Impact Exposure Predicts Later-Life Depression, Apathy, Executive Dysfunction, and Cognitive Impairment in Former High School and College Football Players. J. Neurotrauma 2017, 34, 328–340. [Google Scholar] [CrossRef]
- Brainard, L.L.; Beckwith, J.G.; Chu, J.J.; Crisco, J.J.; McAllister, T.W.; Duhaime, A.C.; Maerlender, A.C.; Greenwald, R.M. Gender differences in head impacts sustained by collegiate ice hockey players. Med. Sci. Sports Exerc. 2012, 44, 297–304. [Google Scholar] [CrossRef]
- Fields, L.; Didehbani, N.; Hart, J.; Cullum, C.M. No Linear Association Between Number of Concussions or Years Played and Cognitive Outcomes in Retired NFL Players. Arch. Clin. Neuropsychol. 2019, 1–7. [Google Scholar] [CrossRef]
- Casson, I.R.; Viano, D.C.; Haacke, E.M.; Kou, Z.; LeStrange, D.G. Is There Chronic Brain Damage in Retired NFL Players? Neuroradiology, Neuropsychology, and Neurology Examinations of 45 Retired Players. Sports Health 2014, 6, 384–395. [Google Scholar] [CrossRef] [Green Version]
- Manley, G.; Gardner, A.J.; Schneider, K.J.; Guskiewicz, K.M.; Bailes, J.; Cantu, R.C.; Castellani, R.J.; Turner, M.; Jordan, B.D.; Randolph, C.; et al. A systematic review of potential long-term effects of sport-related concussion. Br. J. Sports Med. 2017, 51, 969–977. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodologi. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Cohen, J. The Statistical Power of Abnormal-Social Psychological Research: A Review. J. Abnorm. Soc. Psychol. 1962, 65, 145–153. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- De Beaumont, L.; Thoret, H.; Mongeon, D.; Messier, J.; Leclerc, S.; Tremblay, S.; Ellemberg, D.; Lassonde, M. Brain function decline in healthy retired athletes who sustained their last sports concussion in early adulthood. Brain 2009, 132, 695–708. [Google Scholar] [CrossRef] [Green Version]
- Hume, P.A.; Theadom, A.; Lewis, G.N.; Quarrie, K.L.; Brown, S.R.; Hill, R.; Marshall, S.W. A Comparison of Cognitive Function in Former Rugby Union Players Compared with Former Non-Contact-Sport Players and the Impact of Concussion History. Sport. Med. 2017, 47, 1209–1220. [Google Scholar] [CrossRef]
- McMillan, T.M.; McSkimming, P.; Wainman-Lefley, J.; Maclean, L.M.; Hay, J.; McConnachie, A.; Stewart, W. Long-Term health outcomes after exposure to repeated concussion in elite level: Rugby union players. J. Neurol. Neurosurg. Psychiatry 2017, 88, 505–511. [Google Scholar] [CrossRef]
- Misquitta, K.; Dadar, M.; Tarazi, A.; Hussain, M.W.; Alatwi, M.K.; Ebraheem, A.; Multani, N.; Khodadadi, M.; Goswami, R.; Wennberg, R.; et al. The relationship between brain atrophy and cognitive-behavioural symptoms in retired Canadian football players with multiple concussions. NeuroImage Clin. 2018, 19, 551–558. [Google Scholar] [CrossRef]
- Multani, N.; Goswami, R.; Khodadadi, M.; Ebraheem, A.; Davis, K.D.; Tator, C.H.; Wennberg, R.; Mikulis, D.J.; Ezerins, L.; Tartaglia, M.C. The association between white-matter tract abnormalities, and neuropsychiatric and cognitive symptoms in retired professional football players with multiple concussions. J. Neurol. 2016, 263, 1332–1341. [Google Scholar] [CrossRef]
- Pearce, A.J.; Rist, B.; Fraser, C.L.; Cohen, A.; Maller, J.J. Neurophysiological and cognitive impairment following repeated sports concussion injuries in retired professional rugby league players. Brain Inj. 2018, 32, 498–505. [Google Scholar] [CrossRef]
- Ruiter, K.I.; Boshra, R.; Doughty, M.; Noseworthy, M.; Connolly, J.F. Disruption of function: Neurophysiological markers of cognitive deficits in retired football players. Clin. Neurophysiol. 2019, 130, 111–121. [Google Scholar] [CrossRef]
- Strain, J.F.; Womack, K.B.; Didehbani, N.; Spence, J.S.; Conover, H.; Hart, J.; Kraut, M.A.; Cullum, C.M. Imaging correlates of memory and concussion history in retired National Football League athletes. JAMA Neurol. 2015, 72, 773–780. [Google Scholar] [CrossRef]
- Tarazi, A.; Tator, C.H.; Wennberg, R.; Ebraheem, A.; Green, R.E.A.; Collela, B.; Saverino, C.; Khodadadi, M.; Misquitta, K.; Tartaglia, M.C. Motor Function in Former Professional Football Players with History of Multiple Concussions. J. Neurotrauma 2018, 35, 1003–1007. [Google Scholar] [CrossRef]
- Terry, D.P.; Miller, L.S. Repeated mild traumatic brain injuries is not associated with volumetric differences in former high school football players. Brain Imaging Behav. 2018, 12, 631–639. [Google Scholar] [CrossRef]
- Tremblay, S.; De Beaumont, L.; Henry, L.C.; Boulanger, Y.; Evans, A.C.; Bourgouin, P.; Poirier, J.; Théoret, H.; Lassonde, M. Sports concussions and aging: A neuroimaging investigation. Cereb. Cortex 2013, 23, 1159–1166. [Google Scholar] [CrossRef]
- Karr, J.E.; Areshenkoff, C.N.; Garcia-Barrera, M.A. The neuropsychological outcomes of concussion: A systematic review of meta-analyses on the cognitive sequelae of mild traumatic brain injury. Neuropsychology 2014, 28, 321–336. [Google Scholar] [CrossRef]
- Belanger, H.G.; Spiegel, E.; Vanderploeg, R.D. Neuropsychological performance following a history of multiple self-reported concussions: A meta-analysis. J. Int. Neuropsychol. Soc. 2010, 16, 262–267. [Google Scholar] [CrossRef]
- Shenton, M.E.; Hamoda, H.M.; Schneiderman, J.S.; Bouix, S.; Pasternak, O.; Rathi, Y.; Vu, M.A.; Purohit, M.P.; Helmer, K.; Koerte, I.; et al. A review of magnetic resonance imaging and diffusion tensor imaging findings in mild traumatic brain injury. Brain Imaging Behav. 2012, 6, 137–192. [Google Scholar] [CrossRef]


{kind=link}
| Study/Year | Participants | Sports Type and Level; Career Years | Time Since Last Concussion (Mean Year) | Cognitive Outcomes (Instrument) | Downs and Black Score; Quality | |||
|---|---|---|---|---|---|---|---|---|
| Reported Concussion | Mean Age (Concussed/Control) | Sample Size (Concussed/Control) n Times of Concussion Male (%) | Year of Education | |||||
| De Beaumont et al. (2009) [28] | Self-report and sports physician confirmed | 61; 59 | 19; 21 1–5 n.r | 18; 18 | Mix; C n.r | 34.74 | Immediate recall(RCFT) Delayed recall (RCFT) Visual ability (RCFT) | 11, moderate |
| Hume et al. (2017) [29] | Self-report and doctor confirmed | 41.3; 44.9; 42.1 | 103; 198; 65 1+ 100% | n.r | Rugby; P, C 23 | 25 | Verbal memory (CNS-VS) Attention (CNS-VS) Reaction time (CNS-VS) Visual ability (CNS-VS) | 11, moderate |
| Mcmillan et al. (2016) [30] | Self-report and doctor confirmed | 53; 55 | 52; 29 14 100% | 16; 17.3 | Rugby; P 22.4 | 20 | Immediate recall (RAVLT) Delayed recall (RAVLT) Reaction time (SART) Attention (SDT) Visual ability (LOT ) | 11, moderate |
| Misquitta et al. (2018) [31] | Self-report and sports physician confirmed | 55.6; 50.8 | 53; 25 4 100% | 16; 16 | Football; P 9 | 15 | Immediate recall (RAVLT) Delayed recall (RAVLT) Verbal memory (RVDLT) | 11, moderate |
| Multani et al. (2016) [32] | Self-report and certified athletic trainer confirmed | 49.6; 46.7 | 18; 17 5.4 100% | 17.3; 16.4 | Football; P 7.8 | 16.2 | Immediate recall (RAVLT) Delayed recall (RAVLT) | 11, moderate |
| Pearce et al. (2018) [33] | Self-report and sports physician confirmed | 48.4; 48.8 | 25; 25 8.5 100% | 13.9; 14.8 | Rugby; P n.r | 18.8 | Verbal memory (CNT) Visual ability (CNT) Reaction time (CNT) | 11, moderate |
| Ruiter et al. (2019) [34] | Self-report and certified athletic trainer confirmed | 57.6; 53.7 | 19; 20 4 n.r | 16.7; 16 | Football; P 7.8 | 28 | Verbal Memory (ImPACT) Visual Memory (ImPACT) Attention (ImPACT) Reaction Time (ImPACT) | 11, moderate |
| Strain et al. (2015) [35] | Self-report and sports physician confirmed | 68; 59 | 20; 21 3.8 n. | 16.5; 15.9 | Football; P 8.9 | 20 | Verbal memory (CVLT) | 11, moderate |
| Tarazi et al. (2018) [36] | Self-report and sports physician confirmed | 53.4; 50 | 45; 25 5.07 100% | 16.13; 16.12 | Football; P 7.9 | 17.33 | Verbal memory (RAVLT) Immediate recall (RAVLT) Delayed recall (RAVLT) Attention (Trial B) | 11, moderate |
| Terry et al. (2018) [37] | Self-report and certified athletic trainer confirmed | 53.1; 50 | 20; 20 4.3 100% | 15.7; 15.3 | Football; H n,r | 36.7 | Immediate recall (RBANS) Delayed recall (RBANS) Verbal memory (RBANS) Attention (RBANS) Visual ability (RBANS) | 11, moderate |
| Tremblay et al. (2013) [38] | Self-report and sports physician confirmed | 60.9; 58.13 | 15; 15 2.08 100% | 16.67; 17.27 | Mix; C n.r | 24 | Verbal memory (RAVLT) Visual ability (TCFT) Attention (SDT) | 11, moderate |
| Outcomes | Number of Trials | SMD | 95% CI | I2 % | Between-Group Heterogeneity | Publication Bias | ||
|---|---|---|---|---|---|---|---|---|
| Q–Value | df(Q) | p–Value | Egger’s Test (p) | |||||
| Verbal memory | 6 | −0.29 * | −0.59 to −0.02 | 52.8% | 10.59 | 5 | 0.06 | 0.05 |
| Immediate recall | 6 | −0.20 | −0.46 to 0.07 | 27.9% | 6.94 | 5 | 0.23 | 0.24 |
| Delay recall | 7 | −0.30 * | −0.55 to −0.05 | 24.1% | 7.90 | 6 | 0.25 | 0.68 |
| Visuospatial ability | 9 | −0.11 | −0.28 to 0.05 | 12.5% | 9.14 | 8 | 0.33 | 0.68 |
| Reaction time | 5 | −0.08 | −0.40 to 0.23 | 64.5% | 11.25 | 4 | 0.02 | 0.08 |
| Attention | 4 | −0.33 * | −0.59 to −0.06 | 0% | 2.36 | 3 | 0.50 | 0.94 |
| Outcomes | Continuous Predictors | Number of Trials | β | 95% CI | Q–Value | df(Q) | p–Value |
|---|---|---|---|---|---|---|---|
| Verbal memory | Time between testing and last concussion | 6 | –0.03681 | –0.06974 to –0.00387 | 4.80 | 1 | 0.03 * |
| n times of concussion | 6 | –0.04266 | –0.08715 to 0.00182 | 3.53 | 1 | 0.06 | |
| Career years | 5 | 0.02435 | –0.00204 to 0.05075 | 3.27 | 1 | 0.07 | |
| Age | 6 | –0.03767 | –0.06506 to –0.01027 | 7.26 | 1 | 0.01 * | |
| Immediate recall | Time between testing and last concussion | 6 | –0.01184 | –0.03596 to 0.01229 | 0.92 | 1 | 0.34 |
| n times of concussion | 6 | –0.01554 | –0.06829 to 0.03720 | 0.33 | 1 | 0.56 | |
| Career years | 3 | –0.02751 | –0.53642 to 0.04140 | 2.82 | 1 | 0.09 | |
| age | 6 | –0.08684 | –0.16033 to –0.01336 | 5.37 | 1 | 0.02 * | |
| Reaction time | Time between testing and last concussion | 5 | –0.04295 | –0.10872 to 0.02282 | 1.64 | 1 | 0.20 |
| n times of concussion | 5 | –0.03419 | –0.07068 to 0.00230 | 3.37 | 1 | 0.07 | |
| Career years | 4 | –0.02752 | –0.07109 to 0.01604 | 1.53 | 1 | 0.22 | |
| Age | 5 | 0.03489 | –0.00052 to 0.07030 | 3.73 | 1 | 0.053 | |
| Delay recall | Time between testing and last concussion | 7 | –0.01113 | –0.03488 to 0.01262 | 0.84 | 1 | 0.36 |
| n times of concussion | 7 | –0.03056 | –0.08352 to 0.02240 | 1.28 | 1 | 0.26 | |
| Career years | 4 | –0.03861 | –0.07783 to 0.00061 | 3.72 | 1 | 0.054 | |
| Age | 7 | –0.07432 | –0.13650 to –0.01214 | 5.48 | 1 | 0.02 * | |
| Visual spatial recall | Time between testing and last concussion | 9 | –0.00021 | –0.02251 to 0.02209 | 0.00 | 1 | 0.98 |
| n times of concussion | 9 | –0.00275 | –0.03785 to 0.03232 | 0.02 | 1 | 0.88 | |
| Career years | 5 | 0.00684 | –0.02268 to 0.03635 | 0.21 | 1 | 0.65 | |
| Age | 9 | –0.01296 | –0.03713 to 0.01121 | 1.10 | 1 | 0.29 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Ma, Y.; Chen, S.; Liu, X.; Kang, H.J.; Nelson, S.; Bell, S. Long-Term Cognitive Performance of Retired Athletes with Sport-Related Concussion: A Systematic Review and Meta-Analysis. Brain Sci. 2019, 9, 199. https://doi.org/10.3390/brainsci9080199
Zhang Y, Ma Y, Chen S, Liu X, Kang HJ, Nelson S, Bell S. Long-Term Cognitive Performance of Retired Athletes with Sport-Related Concussion: A Systematic Review and Meta-Analysis. Brain Sciences. 2019; 9(8):199. https://doi.org/10.3390/brainsci9080199
Chicago/Turabian StyleZhang, Yanjie, Yongzhi Ma, Shihui Chen, Xiaolei Liu, Hye Jung Kang, Siera Nelson, and Samantha Bell. 2019. "Long-Term Cognitive Performance of Retired Athletes with Sport-Related Concussion: A Systematic Review and Meta-Analysis" Brain Sciences 9, no. 8: 199. https://doi.org/10.3390/brainsci9080199