
In Vivo Analysis of Intraoral Scanner Precision Using Open-Source 3D Software

 , ,
, ,  , and
, and
Abstract
:1. Introduction
- (1)
- There are no differences in the measures (set of values) caught in the successive digital impressions.
- (2)
- No significant differences in each scan expressed as clinically acceptable when considering a threshold of <0.3 mm [19].
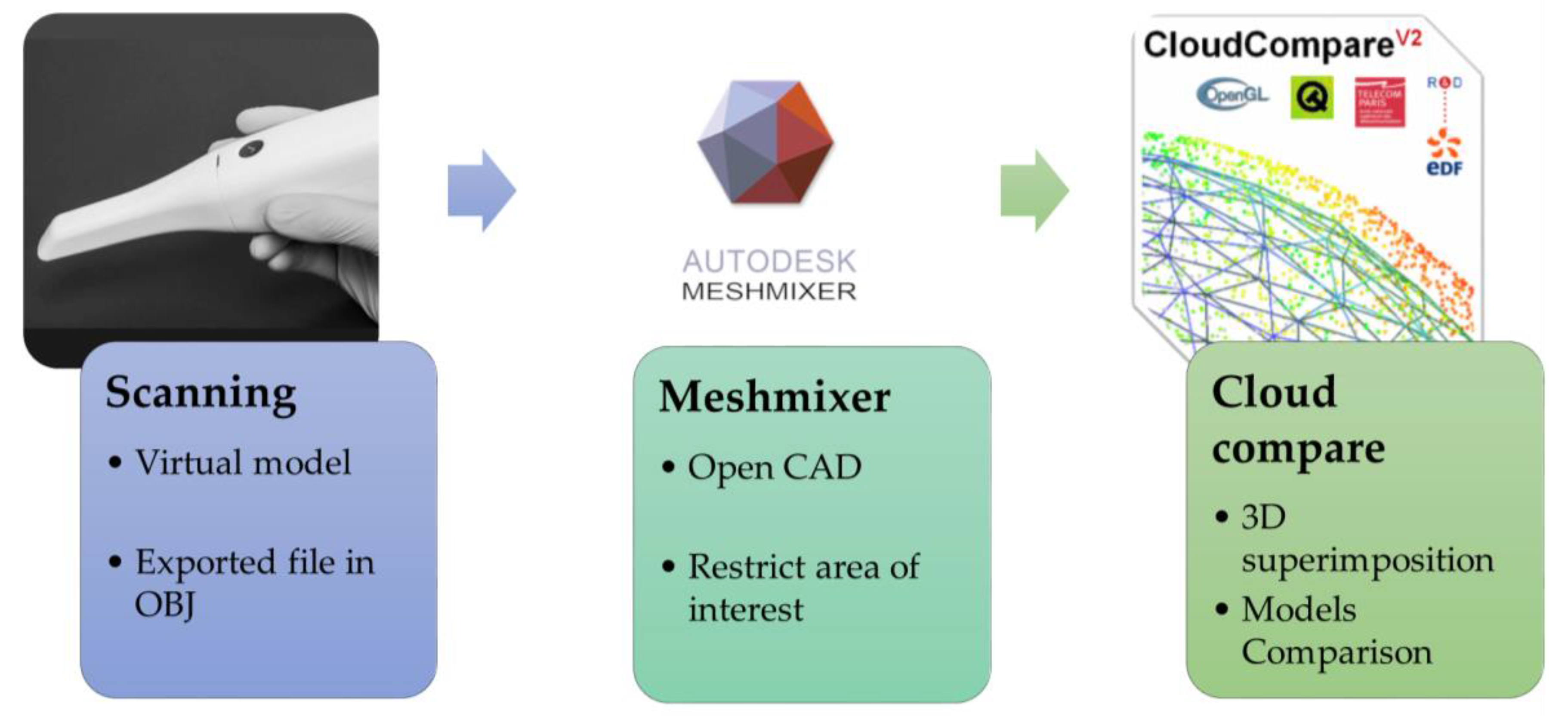
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mörmann, W.H. The evolution of the CEREC system. J. Am. Dent. Assoc. 2006, 137, 7S–13S. [Google Scholar] [CrossRef] [PubMed]
- Pradíes, G.; Zarauz, C.; Valverde, A.; Ferreiroa, A.; Martínez-Rus, F. Clinical evaluation comparing the fit of all-ceramic crowns obtained from silicone and digital intraoral impressions based on wavefront sampling technology. J. Dent. 2015, 43, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Giachetti, L.; Sarti, C.; Cinelli, F.; Russo, D.S. Accuracy of digital impressions in fixed prosthodontics: A systematic review of clinical studies. Int. J. Prosthodont. 2020, 33, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implant. Res. 2013, 24, 111–115. [Google Scholar] [CrossRef]
- Ting-Shu, S.; Jian, S. Intraoral digital impression technique: A review: Intraoral digital impression review. J. Prosthodont. 2015, 24, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.; Lim, Y.; Kim, B.; Kim, M.; Kwon, H.; Baek, Y. Effect of scanning-aid agents on the scanning accuracy in specially designed metallic models: A laboratory study. PLoS ONE 2022, 17, e0267742. [Google Scholar] [CrossRef]
- Logozzo, S.; Zanetti, E.M.; Franceschini, G.; Kilpelä, A.; Mäkynen, A. Recent advances in dental optics—Part I: 3D intraoral scanners for restorative dentistry. Opt. Lasers Eng. 2014, 54, 203–221. [Google Scholar] [CrossRef]
- Cucinotta, F.; Raffaele, M.; Salmeri, F. A Topology Optimization of a Motorsport Safety Device. Lect. Notes Mech. Eng. 2020, 400–409. [Google Scholar]
- Taneva, E.; Kusnoto, B.; Evans, C.A. 3D Scanning, Imaging, and Printing in Orthodontics; Chapter 9 Issues in Contemporary Orthodontics; IntechOpen: London, UK, 2015; pp. 147–188. [Google Scholar]
- Tsirogiannis, P.; Reissmann, D.R.; Heydecke, G. Evaluation of the marginal fit of single-unit, complete-coverage ceramic restorations fabricated after digital and conventional impressions: A systematic review and meta-analysis. J. Prosthet. Dent. 2016, 116, 328–335.e2. [Google Scholar] [CrossRef]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef]
- Imburgia, M.; Logozzo, S.; Hauschild, U.; Veronesi, G.; Mangano, C.; Mangano, F.G. Accuracy of four intraoral scanners in oral implantology: A comparative in vitro study. BMC Oral Health 2017, 17, 1–13. [Google Scholar] [CrossRef]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [Green Version]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.C.; Fages, M.; Ducret, M. Intraoral Scanner Tech-nologies: A Review to Make a Successful Impression. J. Healthc. Eng. 2017, 8427595, 1–9. [Google Scholar] [CrossRef]
- Kwon, M.; Cho, Y.; Kim, D.-W.; Kim, M.; Kim, Y.-J.; Chang, M. Full-arch accuracy of five intraoral scanners: In vivo analysis of trueness and precision. Korean J. Orthod. 2021, 51, 95–104. [Google Scholar] [CrossRef]
- Goracci, C.; Franchi, L.; Vichi, A.; Ferrari, M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impres-sions: A systematic review of the clinical evidence. Eur. J. Orthod. 2016, 38, 422–428. [Google Scholar] [CrossRef] [Green Version]
- Chruściel-Nogalska, M.; Smektała, T.; Tutak, M.; Sporniak-Tutak, K.; Olszewski, R. Open-source software in dentistry: A systematic review. Int. J. Technol. Assess. Health Care 2017, 33, 487–493. [Google Scholar] [CrossRef]
- Osnes, C.A.; Wu, J.H.; Venezia, P.; Ferrari, M.; Keeling, A.J. Full arch precision of six intraoral scanners in vitro. J. Prosthodont. Res. 2020, 64, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Güth, J.-F.; Keul, C.; Stimmelmayr, M.; Beuer, F.; Edelhoff, D. Accuracy of digital models obtained by direct and indirect data capturing. Clin. Oral Investig. 2013, 17, 1201–1208. [Google Scholar] [CrossRef]
- Boeddinghaus, M.; Breloer, E.S.; Rehmann, P.; Wöstmann, B. Accuracy of single-tooth restorations based on intraoral digital and conventional impressions in patients. Clin. Oral Investig. 2015, 19, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- de Andrade, G.S.; Pinto, A.B.A.; Tribst, J.P.M.; Chun, E.P.; Borges, A.L.S.; de Siqueira Ferreira Anzaloni Saavedra, G. Does overlay preparation design affect polymerization shrinkage stress distribution? A 3D FEA study. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 1026–1034. [Google Scholar] [CrossRef]
- Zarauz, C.; Valverde, A.; Martinez-Rus, F.; Hassan, B.; Pradies, G. Clinical evaluation comparing the fit of all-ceramic crowns obtained from silicone and digital introral impressions. Clin. Oral Investig. 2016, 20, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Vecsei, B.; Joós-Kovács, G.; Borbély, J.; Hermann, P. Comparison of the accuracy of direct and indirect three-dimensional digitizing processes for CAD/CAM systemsean in vitro study. J. Prosthodont. Res. 2017, 61, 177–184. [Google Scholar] [CrossRef]
- Arcas, L.P.B.; Tribst, J.P.M.; Baroudi, K.; Amaral, M.; da Silva-Concílio, L.R.; Vitti, R.P. Dimensional accuracy comparison of physical models generated by digital impression/3D-printing or analog impression/plaster methods. Int. J. Odontostomatol. 2021, 15, 562–568. [Google Scholar] [CrossRef]
- Moreno, A.; Gimenez, B.; Ozcan, M.; Pradies, G. A clinical protocol for intraoral digital impressions of screw-retained CAD/CAM framework on multipleimplants based on wavefront sampling technology. Implant. Dent. 2013, 22, 320–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gimenez, B.; Ozcan, M.; Martinez-Rus, F.; Pradies, G. Accuracy of a digital impression system based on parallel confocal la-ser technology for implants with consideration of operator experience and implant angulation ande depth. Int J. Oral Maxillofac. Implant. 2014, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Keeling, A.; Mandelli, F.; Lo Giudice, G.; Garcia-Godoy, F.; Joda, T. The ability of marginal detection using different intraoral scanning systems: A pilot randomized controlled trial. Am. J. Dent. 2018, 31, 272–276. [Google Scholar] [PubMed]
- Lee, J.H.; Yun, J.H.; Han, J.S.; Yeo, I.S.L.; Yoon, H.I. Repeatability of intraoral scanners for complete arch scan of partially eden-tulous dentitions: An in vitro study. J. Clin. Med. 2019, 8, 1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar]
- Ender, A.; Zimmermann, M.; Mehl, A. Accuracy of complete- and partial-arch impressions of actual intraoral scanning systems in vitro. Int. J. Comput. Dent. 2019, 22, 11–19. [Google Scholar]
- Medina-Sotomayor, P.; Agustín Pascual, M.; Isabel Camps, A. Accuracy of four digital scanners according to scanning strategy in complete-arch impressions. PLoS ONE 2018, 13, e0202916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passos, L.; Meiga, S.; Brigagão, V.; Street, A. Impact of different scanning strategies on the accuracy of two current intraoral scanning systems in complete-arch impressions: An in vitro study. Int. J. Comput. Dent. 2019, 22, 307–319. [Google Scholar] [PubMed]
- Son, K.; Jin, M.-U.; Lee, K.-B. Feasibility of using an intraoral scanner for a complete-arch digital scan, part 2: A comparison of scan strategies. J. Prosthet. Dent. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Klussmann, L.; Wöstmann, B.; Schlenz, M.A. Accuracy of digital and conventional full-arch impressions in patients: An update. J. Clin. Med. 2020, 9, 688. [Google Scholar] [CrossRef] [Green Version]
- Sanda, K.; Yasunami, N.; Okada, M.; Furuhashi, A.; Ayukawa, Y. Accuracy of the intra- and extra-oral scanning technique for transferring the intaglio surface of a pontic of provisional restorations to definitive restorations. Materials 2021, 14, 6489. [Google Scholar] [CrossRef]
- Braian, M.; Wennerberg, A. Trueness and precision of 5 intraoral scanners for scanning edentulous and dentate complete-arch mandibular casts: A comparative in vitro study. J. Prosthet. Dent. 2019, 122, 129–136.e2. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.C.; Park, S.-J. Digital intraoral scanners and alginate impressions in reproducing full dental arches: A comparative 3D assessment. Appl. Sci. 2020, 10, 7637. [Google Scholar] [CrossRef]
- Li, H.; Lyu, P.; Wang, Y.; Sun, Y. Influence of object translucency on the scanning accuracy of a powder-free intraoral scanner: A laboratory study. J. Prosthet. Dent. 2017, 117, 93–101. [Google Scholar] [CrossRef]
- Mangano, F.; Lerner, H.; Margiani, B.; Solop, I.; Latuta, N.; Admakin, O. Congruence between meshes and library files of implant scanbodies: An in vitro study comparing five intraoral scanners. J. Clin. Med. 2020, 9, 2174. [Google Scholar] [CrossRef]
- Troiano, A.; Lo Giudice, G.; de Luca, R.; Lo Giudice, F.; D’Amato, S.; Tartaro, G.; Colella, G. Salvage of dental implant located in mandibular odontogenic cyst. A conservative surgical treatment proposal. Dent. J. 2020, 8, 49. [Google Scholar] [CrossRef]
- Lee, S.J.; Kim, S.-W.; Lee, J.J.; Cheong, C.W. Comparison of intraoral and extraoral digital scanners: Evaluation of surface topography and precision. Dent. J. 2020, 8, 52. [Google Scholar] [CrossRef] [PubMed]
- Michelinakis, G.; Apostolakis, D.; Tsagarakis, A.; Kourakis, G.; Pavlakis, E. A comparison of accuracy of 3 intraoral scanners: A single-blinded in vitro study. J. Prosthet. Dent. 2020, 124, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Revell, G.; Simon, B.; Mennito, A.; Evans, Z.P.; Renne, W.; Ludlow, M.; Vág, J. Evaluation of complete-arch implant scanning with 5 different intraoral scanners in terms of trueness and operator experience. J. Prosthet. Dent. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/33832761/ (accessed on 23 September 2022). [CrossRef] [PubMed]
- Róth, I.; Czigola, A.; Joós-Kovács, G.L.; Dalos, M.; Hermann, P.; Borbély, J. Learning curve of digital intraoral scanning—An in vivo study. BMC Oral Health 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- ISO I. 5725-1: 1994; Accuracy (Trueness and Precision) of Measurement Methods and Results e Part 1: General Principles and Definitions. International Organization for Standardization: Geneva, Switzerland, 1994.
- Braian, M.; De Bruyn, H.; Fransson, H.; Christersson, C.; Wennerberg, A. Tolerance measurements on internal- and external-hexagon implants. Int. J. Oral Maxillofac. Implant. 2014, 29, 846–852. [Google Scholar] [CrossRef] [Green Version]
- Tribst, J.P.M.; Dal Piva, A.M.d.O.; Lo Giudice, R.; Borges, A.L.S.; Bottino, M.A.; Epifania, E.; Ausiello, P. The Influence of Custom-Milled Framework Design for an Implant-Supported Full-Arch Fixed Dental Prosthesis: 3D-FEA Study. Int. J. Environ. Res. Public Health 2020, 17, 4040. [Google Scholar] [CrossRef]
- Giudice, R.L.; Famà, F. Health care and health service digital revolution. Int. J. Environ. Res. Public Health 2020, 17, 4913. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pairs of Scans | Deviation < 0.01 mm | Deviation < 0.05 mm | Deviation < 0.1 mm | Deviation < 0.2 mm | Deviation < 0.3 mm | Deviation < 0.4 mm |
|---|---|---|---|---|---|---|
| 1 vs. 2 | 2.9% | 48.5% | 77.9% | 96.2% | 99.8% | 100.0% |
| 1 vs. 3 | 2.4% | 49.2% | 82.1% | 94.8% | 98.4% | 99.4% |
| 1 vs. 4 | 3.5% | 79.5% | 97.5% | 99.6% | 99.9% | 100.0% |
| 1 vs. 5 | 2.3% | 46.0% | 75.6% | 97.2% | 100.0% | 100.0% |
| 2 vs. 3 | 2.3% | 36.2% | 67.2% | 92.3% | 97.0% | 99.1% |
| 2 vs. 4 | 2.5% | 59.4% | 82.9% | 97.0% | 99.5% | 99.7% |
| 2 vs. 5 | 6.6% | 78.7% | 96.1% | 99.6% | 99.9% | 100.0% |
| 3 vs. 4 | 1.9% | 42.0% | 77.7% | 93.4% | 97.3% | 98.9% |
| 3 vs. 5 | 1.2% | 29.4% | 59.9% | 90.1% | 95.9% | 98.4% |
| 4 vs. 5 | 2.8% | 55.6% | 83.0% | 98.6% | 100.0% | 100.0% |
| Mean | 2.8% | 52.4% | 80.0% | 95.9% | 98.8% | 99.6% |
| Standard dev. | 1.4% | 15.6% | 10.9% | 3.0% | 1.4% | 0.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Giudice, R.; Galletti, C.; Tribst, J.P.M.; Melenchón, L.P.; Matarese, M.; Miniello, A.; Cucinotta, F.; Salmeri, F. In Vivo Analysis of Intraoral Scanner Precision Using Open-Source 3D Software. Prosthesis 2022, 4, 554-563. https://doi.org/10.3390/prosthesis4040045
Lo Giudice R, Galletti C, Tribst JPM, Melenchón LP, Matarese M, Miniello A, Cucinotta F, Salmeri F. In Vivo Analysis of Intraoral Scanner Precision Using Open-Source 3D Software. Prosthesis. 2022; 4(4):554-563. https://doi.org/10.3390/prosthesis4040045
Chicago/Turabian StyleLo Giudice, Roberto, Cosimo Galletti, João Paulo Mendes Tribst, Laia Perez Melenchón, Marco Matarese, Alessandra Miniello, Filippo Cucinotta, and Fabio Salmeri. 2022. "In Vivo Analysis of Intraoral Scanner Precision Using Open-Source 3D Software" Prosthesis 4, no. 4: 554-563. https://doi.org/10.3390/prosthesis4040045