Connections and Divergence between Public Health and Built Environment—A Scoping Review



1
School of Architecture, Planning and Preservation, University of Maryland, College Park, MD 20742, USA
2
School of Public Health, University of Maryland, College Park, MD 20742, USA
*
Author to whom correspondence should be addressed.
Urban Sci. 2020, 4(1), 12; https://doi.org/10.3390/urbansci4010012
Submission received: 13 January 2020
/
Revised: 23 February 2020
/
Accepted: 2 March 2020
/
Published: 5 March 2020
{kind=link}
Abstract
:Public health and built environment design have a long-intertwined history of promoting a healthy quality of life. They emerged with the common goal of preventing infectious disease outbreaks in urban areas and improving occupants’ living conditions. In recent years, however, the two disciplines have become less engaged and with each developing a distinct focus. To respond to this disconnection, a systematic review was conducted to identify the connection and divergence between public health and built environment design and planning. This paper aims to establish a context for understanding the connections, synergies, and divergence between public health and built environment design disciplines. Further, the four main health factors in the built environment are identified and explained: physical, physiological, biological, and psychological factors. Finally, future trends to reconnect public health with build environment design are then outlined.
1. Introduction
The fields of public health and built environment emerged with the common goal of preventing infectious disease outbreaks in urban areas and improving occupants’ living condition. This long, intertwined tradition can be traced back to centuries ago [1,2]. The broad concept that built environments have an impact on people, both physically and psychologically, is understood. There is a longstanding recognition of the built environment as an important determinant of health, particularly housing [3]. However, despite the common historical origins and an existing interest in built environment planning, urban design, and public health, the two different fields have shifted away from each other, with only some overlaps existing between them today [3]. As the American Planning Association (APA) stated on their website: “Planning in the United States originated with a public health purpose…. The planning and public health professions were joined by a shared focus on urban reform…. Throughout the course of the 20th century and into the 21st century, however, planning diverged from its common roots with public health….” There are still intersections between the two fields in academic research, and a variety of green building rating systems have incorporated healthy design features and include occupants’ health and wellbeing as critical components; however, a greater role for public health in built environment design has not been prioritized. To date, sustainable buildings have mainly focused on energy conservation and material selection. The health co-benefits of sustainable building have not been fully realized yet. The transformation from a sustainable building to a healthy building could present a transformative tool to improve public health, and in the future, enhancing public health could become the primary benefit of sustainable design. To this extent, the aim of this scoping review is to (1) map the evidence of connections and divergences between developments in public health and the built environment design and planning field; (2) identify the main concepts, theories, and knowledge gaps; and (3) outline the future trends and potential to reconnect public health research and built environment design and planning.
2. Methodology
The method was a combination of scoping review [4] and inductive content analysis [5]. Authors first defined clearly formulated questions and a systematic way to select, filter, and evaluate each research paper. The questions we used to guide the review were: (1) What are the historical connections between the fields of public health and built environment design? (2) What are the built environment’s primary factors influencing public health? (3) What are the causes for the disconnections? A search of databases for public health, preventive medicine, planning, environmental health, and other “design” literature was conducted; the databases were Web of Science, Scopus, and PubMed. The keywords used were “public health”, “built environment”, “buildings”, “factors”, “connections”, and “gaps.” The search period spanned 1800 to 2019. The reason we started in the 1800s is because modern public health began in the nineteenth century, and the first attempt to establish public health legislation related to the built environment was in 1848: The Public Health Act [6]. The search resulted in a total of 428 papers relevant to built environment design and public health. Those references were then assessed for the inclusion of our in-depth review using content analysis. Content analysis is one of most commonly used and important research methodologies dealing with complex subjects in the social science field [7]. The contents were categorized into four key domains in the built environment that affect human health: (1) physical; (2) physiological; (3) biological; and (4) psychological. These domains address the major factors of human health across multiple disciplines including public health, urban planning, engineering, environmental engineering, sociology, environmental psychology, architecture design, medicine, and other human sciences. Based on the content analysis, we identified the 10 most cited papers in each of those categories; altogether, 40 papers were reviewed and analyzed closely to draw the findings and conclusion.
3. Findings
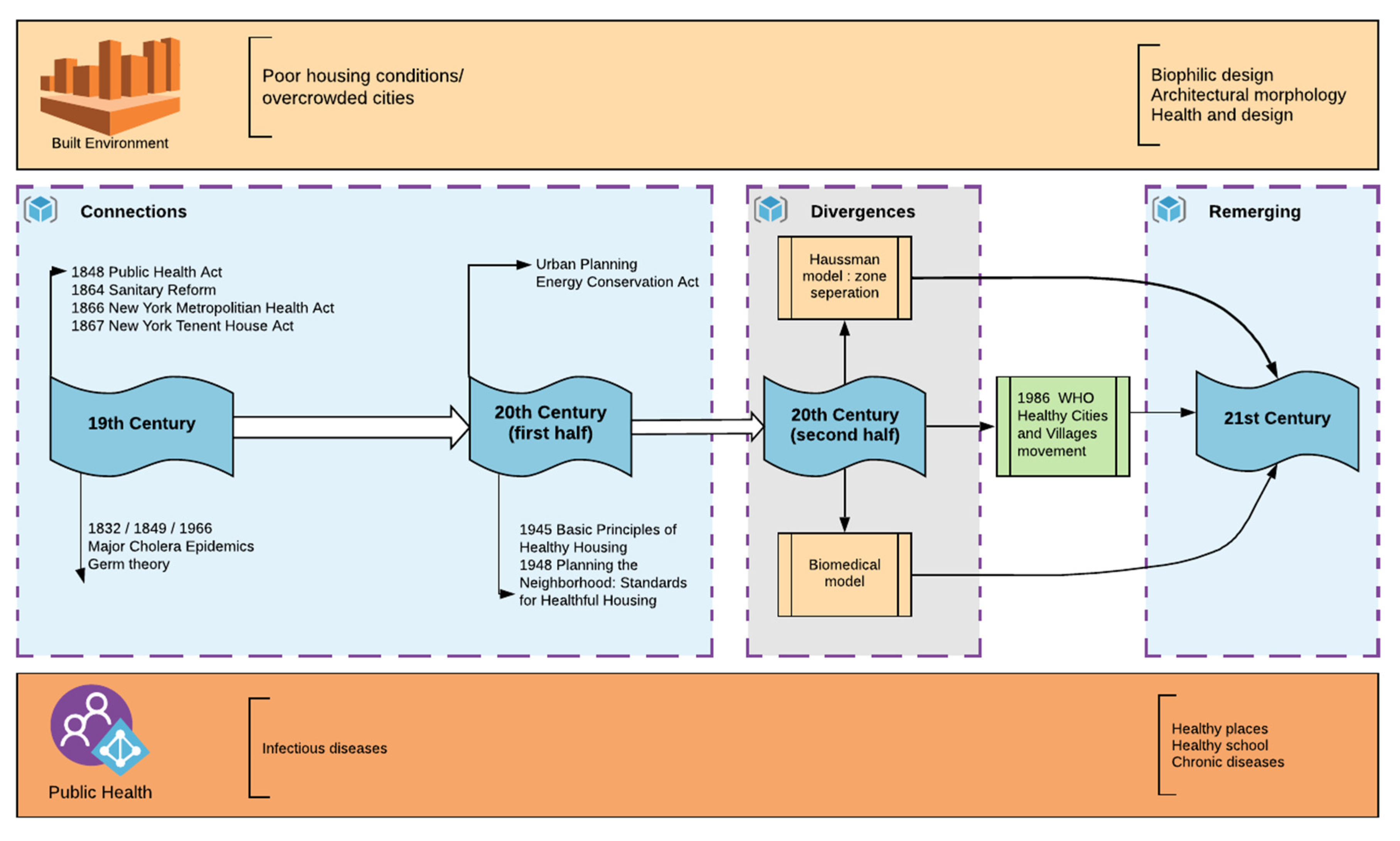
Figure 1 illustrates the connections, divergences, and remerging between public health and built environment within the 19th century onward. In the following sections, the authors discuss these three aspects separately following the same time span.
3.1. Connections
In following the tradition from Greek and Roman ages, an overlap between building codes, planning regulations, and public health policy can be found in 19th century built environment and medical literature. The connection between public health and built environment originated from the era of infectious disease epidemiology. The overcrowded filthy city centers, inadequate sanitation efforts, and horrific workers’ housing conditions, together with multiple major cholera epidemics in 1832, 1849, and 1866 [8], aroused great concern from professionals in the fields of public health, city planning, building design, engineering, and social reform. Together, they joined efforts to reduce the harmful effects of rapid industrialization and urbanization [9,10]. They focused on the sanitary conditions of housing, working places, and city streets. During this period, planning and public health research and practices were regularly influenced by the miasma (bad air) theory and contagions—the major explanatory concept in the understanding of the disease process [11]. The miasma theory is an obsolete medical theory that claimed “bad air” or “night air” caused deadly diseases [11]; it was the predominate medical theory before the nineteenth century. Accordingly, a variety of design solutions through the control of air movement and limitation of sewage and trash exposures were provided to prevent the spread of disease [12]. Planners also used the power of the state to isolate populations suspected of causing diseases [10] or to separate the functions that were suspected of causing disease by creating single-use land zoning. However, the miasma theory failed to explain other aspects of public health issues and epidemics. Some isolated epidemics occurred only sporadically in certain urban areas, regardless of the ubiquitous filth present in most urban areas [10]. Consequently, the unexplained spread of disease activated further research on how the built environment influenced public health and furthered collaboration between the two disciplines during the 1940s and 1950s.
There were two highly influential documents produced during that time. In 1945, the American Public Health Association (APHA), under the leadership of renowned public health researcher and practitioner, Charles-Edward Amory Winslow (also the founder of Yale University, School of Public Health), produced a document titled Basic Principles of Healthy Housing (BPHH) to promote physical, mental, and social health in housing. Thirty principles were identified that covered people’s physiological and psychological needs and their protection against contagions and accidents. There were many detailed quantitative measurements and requirements that are still applicable in today’s housing design, and some have even been integrated into building codes, such as the stair riser and tread dimensions [3]. Five principles under the physiological category have become the primary performance indicators for today’s healthy buildings: (1) thermal environment, (2) indoor air environment, (3) daylight and lighting environment, (4) noise, and (5) safety (for space). This might have been the first time that existing housing conditions could be appraised in objective terms [3]. The latest version was published in 2018 as the National Healthy Housing Standard [13]. However, in the later revisions, many of the original requirements were removed, to the extent that one can no longer recognize the original intent. Now, the main focus is on the physical and physiological needs—such as safety and personal security, lighting, thermal comfort, ventilation, and moisture control—with the psychological needs completely excluded. The psychological needs originally outlined were needed for protection and to support social interactions.
Furthermore, in 1948, the APHA also produced a set of standards to address design and planning issues that supported the creation of a healthy living neighborhood, titled Planning the Neighborhood: Standards for Healthful Housing (PNSHH) [14]. PNSHH could be viewed as a companion publication to BPHH, which painted a comprehensive and broad picture of a healthy built environment. It was produced by the same committee under APHA: The Committee on the Hygiene of Housing (COHH). COHH clearly stated the following: “The present report, on standards for the environment of residential areas, deals with the physical setting in which homes should be located. An attempt is made to bring into focus the basic health criteria which should guide the planning of residential neighborhood environment….” [14]. PNSHH was intended to be used as a guiding principle and reference by the design team to test the adequacy of design proposals based on their impact on health [15]. The essential physical characteristics of the site that should be considered to build healthy buildings were soil and subsoil conditions; ground water and drainage; and flooding, exposure to the sun, circulation, hazardous conditions, power, fire, and safety. It even provided detailed guidelines for the size of public facilities (schools, playgrounds, parks, shopping centers, and other community facilities). This publication might be the first comprehensive document to outline the requirements and recommendations for healthful buildings in a large urban context. Certain principles included in the PNSHH need to be reinvestigated and examined, such as the preference of one or two single-family houses versus apartment buildings; however, the systematic understanding and measurement of buildings’ health quality in an urban context is still applicable.
Following the initial peak interest in increased built environment quality through public health improvements, the interest continued for decades, although with less of a concentration. Yet, in the late 1980s, an interest in urban environment reemerged—this time with a more defined and broader agenda. The World Health Organization (WHO) initiated the Healthy Cities and Villages movement in 1986, with the release of the report Health Cities: Promoting Health in the Urban Context [16,17]. The Healthy Cities and Villages movement served as a precursor to later movements, such as the smart growth and new urbanism movements.
Regarding the built environment design side, during early traditions, pre-Christianity, and the Renaissance, the health of building conditions was primarily focused in the realm of philosophy and humanity. Those early design guidelines were not easy to understand or follow, due to their abstract descriptions. The notion that the individual was responsible for his/her own health problems was too firmly entrenched, and many people believed that physical illnesses were related to one’s morals [18], with the influence of physical built environment factors treated as secondary. Beginning in the early 19th century, the assumptions started to shift, and people began to recognize the important role the built environment played in human health as a growing number of built environments were constructed. In 1842, British researcher Edwin Chatwick published Report on the Sanitary Condition of the Labouring Population of Great Britain while employed by a royal commission. This report studied built environment conditions contributing to population health [19,20] following a serious typhus outbreak in 1838. The report essentially led to the Britain Public Health Act of 1848 [17]. Chatwick argued that poor health conditions were caused by the physical built environments among living and working communities, and not by vice and immorality [20].
Chatwick’s work on sanitary reform rapidly generated great interest in the United States. The promotion of modern plumbing fixtures and sewage systems represented a large part of the United States’ sanitary reform movement since 1864 [21,22,23], and public health professionals, physicians, public officials, and engineers collectively joined the movement. Going beyond the sanitary system, they educated the public about hygiene and sought to eliminate overcrowding and poor ventilation, an impure water supply, and unwholesome food [3,24]. Those efforts lead to the United States’ first set of health and housing laws (the New York Metropolitan Health Act, 1866, and the New York Tenement House Act, 1867). The design solutions included requiring windows that opened to outside air in place of air shafts, separate toilet for each apartment, functional fire escapes, adequate lighting in hallways, proper sewage connections, and regular waste removal [3]. Along with the large interest in providing a higher quality built environment for improving public health, industrialization brought about the heyday of technological advancements. At the building scale, engineers and architects invented a variety of systems that could produce a consistent indoor environment, so that relatively healthy living conditions could be attained and maintained through the help of mechanical systems [24]. At the urban scale, design and technology-based engineering solutions were invented to remove waste and unsanitary items off the streets, such as a modern sewerage system and garbage collection [25]. Pest and rodent control were also included in the housing regulations [26].
3.2. Divergence
The closely intertwined relation between built environment design and public health practice shifted its direction around the 20th century. Beginning in the 1850s, the driving ideology in public health shifted from the miasma theory to the germ theory [10]. This fundamental concept shift was accompanied by later changes in public health and planning practice. In the public health field, the focus changed from investigating ways to improve urban infrastructure to laboratory investigations of microbes [11] since the “bad air” could not explain or answer all public health questions. The physicians, not the planners, emerged as the new class of public health professionals [27,28]. In the planning field, the land separation/zoning changed from its original health concern to uncertainty regarding efficient land use [29]. Planners focused on functionality and spatial planning and a hierarchical ordering of land use following the German-inspired Haussman model [10]. This Haussman model represented the concept of dividing an entire city into residential and industrial zones [30,31,32]. It was invented by German social reformers in the 1870s and 1880s, and was extremely well-received in the United States in the early 1990s. American planners eventually emulated parts of the model, including the idea of basing the districts on land use [30], with zoning aimed at “immunizing” urban populations by separating land use. Although architects and engineers had tried to integrate health considerations into the basic building codes as a way to prevent hazardous conditions at the building design level, the resulting focus was on prevention, rather than health promoting. The design solutions were mainly technological and system-driven, such as air conditioning, mechanical systems, ventilation systems, and building infrastructure.
The latter half of the 20th century, around the 1960s, saw another shift in the public health field. This shift moved toward addressing the “hosts,” or diseased individuals [10]. Consequently, the research and practices progressed further inward, instead of studying the outside world. Social dimensions were ignored, and lifestyle, gender, and class were not taken into consideration [33]. Representing another major change, the public health profession moved from the germ theory to the biomedical model. The biomedical model is the predominant model used by physicians diagnosing diseases [34]; however, this model is based on the belief that health issues/phenomena can be reduced to their constituent parts (organs, body, legs, etc.), measured, and then causal relationships deduced [34]. It is a linear model that tends to overlook the interaction between the built environment and human health, and the interactional impact on both physical and psychological health. As the biomedical model became mainstream, researchers and practitioners also recognized its limitations. Afterward, in the late 1990s, some countries, such as Canada and Australia, saw a public health revival. A new public health practice and research approach reconciled the biomedical model with social science and provided a hybrid quantitative and qualitative method to not only examine the direct health factors, but also the latent factors in the built environment [35]. This revival was not fully developed in the United States, partially because of the idea that diseases could be explained at the molecular level, which had been scientifically proven, promoted and was deeply rooted. Moreover, this new revival could be not reconciled with the philosophy adopted throughout the United States, a philosophy where the individual was responsible for his or her own health, and individual health was largely determined by morality—not the surrounding environment (See Section 3.1). There were some areas where the built environment was studied and examined in relation to people’s physical activities and their influence on health, such as diabetes. Even though evidence had been found, the research impact of the public health field on urban design and planning practices was less obvious.
In the discipline of built environment design and planning, in the late 20th century, the concern for public health had become mainly physical and physiological, with the minimal requirements of air quality and thermal comfort representing the highest standards to pursue. Planning professionals turned to promoting economic development through large infrastructure and transportation projects [36], which were much needed after two world wars. Built environment planning and design shifted from attempting to protect human health in densely populated urban areas to promoting suburban economic development [36]. Health-related requirements and concerns gradually disappeared from the center stage of the planning practice. Instead, urban planning transferred its focus toward environmental health by adopting the Environmental Impact Assessment (EIA) process [10]. This process still represents the predominant method and has been perceived as the gold standard. At the same time, the building industry’s primary concern for a sustainable and healthy community began to center around resource efficiency and cost-effectiveness. By the late 20th century, the fields of urban planning, building design, and public health were largely disconnected from their initial social reform mission [10,37].
3.3. Remerging
In recent years, there have been emerging transdisciplinary attempts to connect public health to built environment design, particularly biophilic design. Biophilic design originated from the concept of biophilia. The theory of biophilia was proposed by biologist E.O. Wilson in 1984, who suggested that humans have an innate biological need to be connected to nature [38]. Afterward, design professionals, psychologists, and physicians have conducted studies on the health benefits of biophilic design, with most based on self-assessment [39,40,41]. More precisely, they examined the psychological and physical effects of biophilic design on inhabitants of a built environment. Another area of interest is the impact of architectural morphology on human health, which studies a building’s form, height, and massing and the related health implications. Continuing research from the 1970s related to social isolation associated with high-rise buildings [42]. Baqar et al. (2008) studied the social and psychological well-being of black elderly residents in high-rise buildings and found those residents to have higher rates in stress, depression, and schizophrenia [43]. Gifford found in Singapore, as high-rise buildings increased from 9% to 51% city-wide, the per capita rate of suicide increased fourfold [44]. These types of transdisciplinary studies and design interest have been reconnecting built environmental design and public health based on new data and empirical evidence, thus presenting a significant collaborative research potential.
Biophilic design primarily focuses on the indoor environment and interior of buildings, while architectural morphology studies the building typology. A focus restricted to individual buildings is not adequate to address the broad health impacts of the built environment. Consequently, beginning in the 2000s, there has been a re-emerging interest in the built environment’s impact on an urban scale. One of the most influential publications, Making Healthy Places, published in 2012, detailed the impact of community design on health and strategies for creating healthy places [45]. Furthermore, in 2014, the American Institute of Architects worked together with public health researchers and professionals to launch a design and health initiative. This generated six evidence-based approaches that designers can use to promote health and well-being: (1) environmental quality; (2) natural systems; (3) physical activity; (4) safety; (5) sensory environments; and (6) social connectedness [46]. These six approaches established a platform for the reconnection between public health and built environment design on a large scale. Moreover, in recent years, the use of big data from the medical sector has provided a possible entry point to address complex health outcomes linked to the built environment [47]. The study of medical and public health data, together with urban development patterns, has provided insight on the potential of design strategies to enhance urban health.
3.4. Existing Factors of Health Issues in the Build Environment
Based on the existing literature, the built environment condition affects health in multiple dimensions [48], with a variety of built environment hazards categorized into four primary factors to human health: (1) physical; (2) physiological; (3) biological; and (4) psychological factors.
3.4.1. Physical Factors
Physical factors are directly related to design and planning. One of the most important design concerns is ensuring occupant safety by preventing injuries both indoors and outdoors, especially related to the reduction of falls [49]. Many of the building design features and materials used influence the risk of injuries, such as slippery floors and insufficiently lighted stairs [50], unprotected upper-story windows, and low sill heights [51]. In Britain, more than a third of all adult accidents occur in the home [50], and residents who reside in high-rise buildings are more prone to falls from windows and balconies [52]. According to the WHO, each year, an estimated 646,000 individuals die from falls globally, of which over 80% are in low- and middle-income countries [53]. Besides the dangers of falling, violence and fire hazards are two other direct structural factors impacting human health that can be controlled and mitigated through good planning and design. Paul Stollard wrote a book proposing the concept that design measures could play a significant role in crime reduction [54]. Occupants’ experiences can differ radically from the designers’ intentions as their concerns and thinking differ [55], and the appropriate design could enhance their perception of safety as well as “designing out” hidden places to prevent opportunities for crime [53]. Well-designed fire protection and suppression features are critical for protecting occupants from fire. For instance, residential fires most often start in the kitchen, so installing a fire alarm could reduce the risk. Also, the basic building structure and materials need to be designed to minimize the danger of accidents due to the collapse of buildings and potential injuries—even death.
3.4.2. Physiological Factors
Physiological factors are the factors in the built environment that stimulate the occupant’s physical bodily changes, consequently affecting occupant health or comfort. For example, when the room temperature is too high or low, this type of deviation from the acceptable temperature range could be associated with an increased risk of cardiovascular disease [56]. The physiological factors that are closely associated with the building design are temperature [57], humidity [56], ventilation [52], air quality [58], illuminance level [59], and acoustic level [60], and these factors comprise the indoor environmental quality (IEQ). A 2011 study [61] of 42 office buildings showed that mechanical ventilated buildings (sealed buildings) had more sick building symptoms (SBS) than naturally ventilated buildings (non-sealed buildings). However, more recent research indicated opposing results, with the prevalence of SBS in non-sealed buildings being higher than in sealed buildings [58]. Regardless of the varied findings, the majority of research and case studies support concerns regarding the linkage between the sealed indoor environment and biological factors that contribute to SBS.
Ample evidence connects a building’s indoor environment quality and characters to respiratory issues and lung conditions. These diseases have been proven to be linked to cold (indoor temperature) and damp (excessive indoor humidity) environments [62]. Furthermore, dampness and mold have been found to be associated with aches and pains in the human body [63]. Exposure to indoor toxic substances released from the building’s materials or paint can result in chronic headaches, itchy eyes, asthma, and lung disease [64]. A higher level of exposure to carbon monoxide results in acute intoxication [65]. Other exposures, such as lead [66], asbestos [67], and radon [68], and their related deleterious health impacts, including death, have been well studied and understood.
Inadequate indoor lighting affects both vision and the photobiological needs of synchronizing circadian rhythm, which impacts sleep and depression [69]. Well-designed lighting is one of the most important design elements to support an occupant’s ability to perform daily tasks and decrease the level of disability associated with these impairments [68]. Research results consistently show that acoustic quantity and quality have physiological impacts on occupants. Also, indoor noise has been proven to have a strong association with high blood pressure levels, and the noise level is influenced by the room orientation and adjacency to windows [70]. The interference and health impact from noise are found in schools, offices, and health care facilities located in different countries, such as Nigeria [65], South Africa [71], Hong Kong [72], and the United States [73].
3.4.3. Biological Factors
Biological contributors are associated with indoor mold, fungi, and other insect/mite conditions that can endanger an occupant’s health and well-being. The growth of biological factors inside a building could be caused by the unhealthy and inappropriate use of building materials, inadequate ventilation as indoor dampness is related to false design and construction, and inadequate repair and maintenance [74,75]. Constant exposure to such factors can result in reoccurring health-related issues, including respiratory diseases and allergies [76,77]. Recently, a new subfield has emerged, the “microbiology of the built environment,” which studies the communities of microorganisms found in human-constructed environments. Its potential will be analyzed in Section 4.
3.4.4. Psychological Factors
Psychological factors go beyond basic human health, aimed at promoting or undermining an occupant’s optimal physiological, mental, and social performance. A large number of physiological factors are intertwined with psychological factors; for instance, lighting and sound. Hwang and Kim studied 2744 healthy occupants for 1.5 years to investigate the effects of indoor lighting on occupants’ visual comfort and eye health [78]. The studies produced multiple findings. A significant correlation between the occupants’ visual comfort and the lighting conditions and luminance distribution of windows was observed; further, it was found that daylight improved the occupants’ psychological health and productivity [79]. So far, the number of existing studies with a focus on psychological factors to occupant social performance and mental health is relatively limited [79]. Results from the existing body of studies have suggested that residents’ perceptions of their homes are associated with their self-rated health status [80]. The concern of substandard housing conditions and fear of deteriorating indoor quality, especially in public housing projects, have been reported to contribute to psychosocial stress and can lead to mental health issues [3].
Overall, the four factors are often interrelated and are difficult to be extrapolated. For instance, excessive noise levels caused by insufficient acoustic insulation in the partition wall is a physical factor, but it also leads to sleep deprivation, which essentially could cause psychological stress and activation of the hypothalamic-pituitary-adrenal axis and sympathetic nervous system [3]. Indoor pollution can cause discomfort and impact productivity through influencing cognitive functions [81]. Among the four factors, the psychological and biological factors to human health have been less explored.
4. Future Trends: Reconnecting Public Health and Built Environment Planning and Design
In the past several decades, the leading factors of death in the built environment, particularly in developed countries, have shifted from infectious disease to chronic conditions [16]. A new set of challenges emerged, along with a different trend calling for new and multidisciplinary/multifactor solutions. This section outlines three future trends that may guide to reestablish the connection between built environment planning/design and public health.
4.1. Multidisciplinary: Human Ecology, Biology, Psychology, and Neurology
While existing attributes and factors that have a psychological and biological impact have been difficult to measure and monitor, building physical and physiological factors have received more research attention. Introducing human ecology into the equation will help to further our understanding of the lesser-known factors. Human ecology itself is a transdisciplinary field that has strong roots in biology, geography, and sociology. It studies the interaction between humans and the natural and built environments [15]. The term “human ecology” was first proposed by engineer and environmental chemist Ellen Henrietta Swallow Richard, who described it as “the study of the surroundings of human beings in the effects they produce on the lives of men” [81]. It was later adopted by sociological research [82] and interpreted as part of the works of the Chicago School [83]. Since the 1970s, studies in human ecology have found that the levels of stimulation from the built environment are capable of moderating and optimizing human behavior and functions. A lack of stimulation can lead to boredom and sensory deprivation [84], and overstimulation can cause focus and attention deprivation [85]. Built environment stimulation includes visual, acoustic, and other sensory stimuli. The level of stimulation is influenced and sometimes determined by design features, such as light level, noise level, color contrast, urban density, openness of the space, and other spatial characteristics. Exposure to visual and acoustic stimulation is strongly influenced by architectural layout [82], and the design layout includes the space size, shape, volume, geometry, and orientation.
The second new discipline that should be integrated is microbiology, which is particularly useful to understand how architectural design could influence the diversity and structure of the built environment microbiome [86]. In recent years, the research community has intensively focused on the microbiome in buildings, with findings indicating that indoor spaces often harbor unique microbial communities [87]. Furthermore, the difference between buildings is greater than the difference between seasons [88] and locations (site and climate condition), demonstrating the point that each individual building has a predominate effect on human health through cultivating different microbiome communities. This field represents a very interesting and promising research direction. For instance, Lax and colleagues found that, even in the same location, individual homes all have different bacterial communities [89], and the indoor microbiology environment is quite different from that of outdoors. This distinguished microbiome environment is induced by several factors. Firstly, indoor bacterial communities often originate from indoor sources [90,91], mainly from building materials and human bodies; secondly, the physical and chemical properties of building surfaces and materials in the built environment are, for the most part, very different compared with materials and surfaces in the natural environment [92]. The uniqueness of bacterial sources and the growing environment make the microbiological environment in buildings a crucial factor to occupant health. Studies have shown that building design and operation can influence indoor microbial communities [88]. More open and connected spatial layouts/designs contained a unique collection of bacteria compared to more closed and less connected spaces [88]. The buildings’ conditions are also important, as indicated in studies of buildings with prior moisture and dampness conditions. Indoor fungal communities often differ from those in non-damp buildings, for buildings with the same function and location [88]. The observed relationship between building design and bacterial diversity suggests that architectural and engineering design could alter the indoor microbiome [87,93]. Moreover, not all bacteria are harmful, as exposure to the “right” amount and kind of microbes may be beneficial for human health [88]. In addition, architectural design has been shown to influence the types of indoor bacterial accumulation, in part because building form variations and interior spatial arrangement can influence the occupants’ use of space [94]. In general, this relatively new field has provided some knowledge regarding the microbiome of the built environment, and disease vulnerability has also initiated certain experimental research on how microorganisms can be transferred to occupants’ cutaneous or mucosal membranes, potentially increasing or decreasing the risk of inflammation-induced psychiatric conditions [95].
The third discipline is psychology. Environmental psychology, in particular, has a long history of studying the influence of the built environment on human behavior and, consequently, health [96,97]. Since the early 1900s, there have been multiple theories invented to interpret the psychological impact of the built environment, such as personality and motivation theories. Personality theories advocate creating a work environment that reflects the occupant’s personality [98]. This theory created much ambiguity in understanding what the exact correlation was between the built environment, personality, and personal behavior; consequently, design challenges have been imposed that are not well-defined [97]. Motivation theories (Yerkes–Dodson Law) proposed an inverted U-shape relation between a person’s performance and their level of arousal from the built environmental stimulation [99]. In a recent German study, a correlation was found between space openness (view to outside) and occupant excitement; regarding the room proportion and occupant’s interest level, they found the optimized room ratio was actually near the golden ratio [99]. Although evidence exists in the field of environmental psychology of how visual images can induce certain emotions, there is still a lack of deep understanding of how specific visual properties (features) of the built environment contribute to this effect [100].
The fourth and most recently introduced discipline, neuroscience, could further such understanding by studying humans’ response to external stimulus [100] using advanced neuroimaging techniques, such as functional magnetic resonance imaging (fMRI) and electroencephalogram (EEG). With those technologies, researchers could record and study brain activity when exposed to different built environments. With a deep understanding of stimuli and their impact, the architect and designer could focus on designing an environment that can stimulate different brain responses, hence influencing activity, memory, and creativity.
4.2. Multilevel: Urban and Building Integration
Buildings exist in relation to urban context and social infrastructure; their effects on health not only are reflected at the individual level, but also extend to the urban level. In order to fully understand the health impact of buildings, the first step is to contextualize individual buildings within a community and neighborhood. Contextual urban characteristics could help to assess the impact of buildings that are multi-dimensional, and those dimensions can be defined by density [1,101], land-use mix [102,103,104], architectural/design features [95,96,97,98,99,100,101], and street characteristics (connectivity and accessibility) [99,100,101]. Density refers to housing, job, or population density, while land-use mix is often defined by the use and function of the land area or floor area. Architectural/design features include sidewalk coverage, architectural characteristics, aesthetic values, building setback or front porch coverage, and other physical variables [102,103]. Finally, street characteristics (connectivity and accessibility) are associated with street grids, block size, and different available transportation methods. There were several efforts in the early 20th century from the field of public health to assess the quality of healthy building within the urban context. In 1945, public health researcher C.E.A. Winslow, with colleagues, proposed an appraisal method for measuring the quality of housing in collaboration with the health department, housing authorities, and local planning professionals from New Haven, Connecticut. Their efforts were to devise a technique for inspecting and evaluating the health qualities of housing that were simple and objective [104].
4.3. Multifactor Assessment
A Smart Market report by Dodge Data & Analytics in 2016 indicated that investments in healthier buildings are poised to be a transformative trend in the design and construction industry [105]. Seventy-five percent of owners believe that having healthier and happier tenants or employees is one of the most important goals. The five important healthier building attributes chosen by building owners, architects, and engineers are air quality, thermal comfort, lighting and daylight exposure, biophilic design (close to nature), and enhanced tenants’ mood [103,104]. Those five major building attributes and other factors, together, define the health impact of buildings, with health interpreted as including physical, cognitive, and emotional well-being. Currently, the commonly used methods to assess a building’s impact on occupants are real estate property, housing, and individual building surveys. The real estate property survey typically concerns the property value, building location, and existing conditions. Local jurisdictions and property management companies all have their own assessments, which do not typically reflect the direct health impact of a building since the real estate value is not determined by health impact. The second assessment, the American Housing Survey: Housing Adequacy and Quality as Measured by the AHS (2013), was created based on the standards established by the Housing Act of 1949 [105] to determine whether a building has a suitable living environment. However, those measurements are not sufficient to quantify the quality of a healthy building since “adequacy” is a narrower concept than quality, and a building can suffer from various healthy deficiencies and still be considered as an adequate shelter [105]. The third method to assess a healthy building is the individual building inspection. Such inspections typically occur after a health complaint is filed; therefore, the assessments are typically reactive rather than proactive and cause- and solution-driven rather than enhancement- and promotion-driven. The inspection results are seldom designed to be useful to others besides the inspection agency, and are only related to that particular building or group of buildings. Lastly, larger urban environments, such as neighborhood environments, are usually disregarded in individual building surveys [105]. Overall, the current building impact assessment methods have been kept at a bare minimum, are solution-driven, and are based on a single factor. In order to assess impact from multiple factors, a comprehensive building and built environment quality assessment method should consider all the health factors mentioned in Section 3 and be based on the multidisciplinary approach mentioned in Section 4.1.
5. Conclusions
This paper has documented the connections and divergence between the built environment and public health. An overview of the literature highlighted four primary built environment factors (1) physical; (2) physiological; (3) biological; and (4) psychological) that are influential to human health. However, despite this influence a disconnect between the fields of built environment and public health has been recognized. In recent years, urban planning professionals have focused on planning for active living, emergency preparedness, environmental exposure, social cohesion, and mental health [106], which require higher and more strategic levels of planning that could have direct and indirect health impacts. Architects and engineers, in contrast, have focused on advancing the local built environment in order to improve health conditions at a detailed level. Due to the existing gap between built environment design and public health, this paper ultimately proses a multidisciplinary, multilevel, and multifactor framework to narrow the gap. Human ecology, biology, psychology, and neurology have been identified as additional fields that need to be integrated to establish a new and richer connection. Based on the literature, it is important that the built environment design community be reconnected to public health professionals. When built environment design and engineering and public health shared common goals, the results were not only vastly evolutional, but also tremendously beneficial to human health and well-being. Overall, this paper presents innovative knowledge on the relation between the built environment and public health. It outlines the four influential factorial categories and identifies three future research trends. Finally, this manuscript offers an important starting point for future researchers who want to close the gap and develop an integrated approach that either mitigates the negative impacts or promotes the positive impacts of the built environment on public health.
Author Contributions
Conceptualization, M.H. and J.D.R.; methodology, M.H. and J.D.R.; formal analysis, M.H. and J.D.R.; writing—original draft preparation, M.H.; writing—M.H. and J.D.R., X.X.; visualization, M.H.; project administration, M.H.; funding acquisition, M.H. and J.D.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by University of Maryland, Tier 1 research fund.
Acknowledgments
This work has been made possible with support from the United States National Science Foundation, through the founding of the workshop Health in Buildings for Today and Tomorrow: Making Connections. We also thank our colleagues at the University of Maryland, School of Architecture and School of Public Health who provided insights and expertise that greatly assisted this research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Frumkin, H. Healthy places: Exploring the evidence. Am. J. Public Health 2003, 93, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Pappas, G.; Kiriaze, I.J.; Falagas, M.E. Insights into infectious disease in the era of Hippocrates. Int. J. Infect. Dis. 2008, 12, 347–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieger, J.; Higgins, D.L. Housing and health: Time again for public health action. Am. J. Public Health 2002, 92, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elo, S.; Kääriäinen, M.; Kanste, O.; Pölkki, T.; Utriainen, K.; Kyngäs, H. Qualitative content analysis: A focus on trustworthiness. SAGE Open 2014, 4, 2158244014522633. [Google Scholar] [CrossRef]
- United Kingdom Parliament. Sunderland the Public Health Act. Available online: https://www.parliament.uk/about/living-heritage/transformingsociety/towncountry/towns/tyne-and-wear-case-study/about-the-group/public-administration/sunderland-and-the-public-health-act/ (accessed on 17 November 2019).
- Neuendorf, K.A. The Content Analysis Guidebook; Sage: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Rosenberg, C.E. The Cholera Years: The United States in 1832, 1849, and 1866; University of Chicago Press: Chicago, IL, USA, 2009. [Google Scholar]
- People, H. Healthy People in Healthy Communities: A Systematic Approach to Health Improvement; Report; US Department of Health and Human Services: Washington, DC, USA, 2000.
- Corburn, J. Confronting the challenges in reconnecting urban planning and public health. Am. J. Public Health 2004, 94, 541–546. [Google Scholar] [CrossRef]
- Vandenbroucke, J. Is ‘the causes of cancer’a miasma theory for the end of the twentieth century? Int. J. Epidemiol. 1998, 17, 708–709. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Boufford, J.I.; Pagán, J.A. Systems Science Simulation Modeling to Inform Urban Health Policy and Planning. In Smart City Networks; Springer: Berlin/Heidelberg, Germany, 2017; pp. 151–166. [Google Scholar]
- National Healthy Housing Standard. Available online: https://nchh.org/tools-and-data/housing-code-tools/national-healthy-housing-standard/ (accessed on 20 July 2018).
- Standards for Healthful Housing: Planning for the Neighborhood. Available online: https://babel.hathitrust.org/cgi/pt?id=mdp.39015007191813;view=1up;seq=5 (accessed on 20 July 2018).
- Ewing, R.; Clemente, O. Measuring Urban Design: Metrics for Livable Places; Island Press: Washington, DC, USA, 2013. [Google Scholar]
- Duhl, L.J.; Hancock, T. Promoting Health in the Urban Context; WHO Healthy Cities Project Office: Geneva, Switzerland, 1988. [Google Scholar]
- Abrams, R.F.; Malizia, E.; Wendel, A.; Sallis, J.; Millstein, R.A.; Carlson, J.A.; Cannuscio, C.; Glanz, K.; Samet, J.; Sleet, D.A.; et al. Making Healthy Places: Designing and Building for Health, Well-Being, and Sustainability; Island Press: Washington, DC, USA, 2012. [Google Scholar]
- Hamlin, C.; Sidley, P. Revolutions in public health: 1848, and 1998? BMJ 1998, 317, 587–591. [Google Scholar] [CrossRef] [Green Version]
- Hamlin, C. Edwin Chadwick and the engineers, 1842-1854: Systems and antisystems in the pipe-and-brick sewers war. Technol. Cult. 1992, 33, 680–709. [Google Scholar] [CrossRef] [Green Version]
- Finer, S.E. The Life and Times of Sir Edwin Chadwick; Routledge: London, UK, 2016. [Google Scholar]
- Brieger, G.H. Sanitary Reform in New York City: Stephen Smith and the Passage of the Metropolitan Health Bill. Bull. Hist. Med. 1966, 40, 407–429. [Google Scholar]
- Kramer, H.D. The beginnings of the public health movement in the United States. Bull. Hist. Med. 1947, 21, 352–376. [Google Scholar] [PubMed]
- Krueckeberg, D.A. Introduction to Planning History in the United States; Routledge: London, UK, 2018. [Google Scholar]
- Brucemann, R.; Prowler, D. 19th century mechanical system designs. J. Archit. Educ. 1977, 30, 11–15. [Google Scholar] [CrossRef]
- Rosen, G. A History of Public Health; JHU Press: Baltimore, MD, USA, 2015. [Google Scholar]
- Cretti, D.J. Permanently Installed Pest Extermination System; United States Patent and Tradeark Office: Washington, DC, USA, 1988.
- Krieger, N. Theories for social epidemiology in the 21st century: An ecosocial perspective. Int. J. Epidemiol. 2001, 30, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Porter, D. Health, Civilization and the State: A History of Public Health from Ancient to Modern Times; Routledge: London, UK, 2005. [Google Scholar]
- Planning & Zoning for Health in the Built Environment. Available online: https://www.planning.org/pas/infopackets/eip38/ (accessed on 20 July 2018).
- Liebmann, G. It’s Time to Reconsider Oppressive Zoning. USA TODAY N. Y. 1996, 125, 62–64. [Google Scholar]
- Platt, R.H. Land Use and Society, Revised Edition: Geography, law, and Public Policy; Island Press: Washington, DC, USA, 2004. [Google Scholar]
- Hirt, S. The devil is in the definitions: Contrasting American and German approaches to zoning. J. Am. Plan. Assoc. 2007, 73, 436–450. [Google Scholar] [CrossRef]
- Susser, M.; Susser, E. Choosing a future for epidemiology: I. Eras and paradigms. Am. J. Public Health 1996, 86, 668–673. [Google Scholar] [CrossRef] [Green Version]
- Baum, F. Researching public health: Behind the qualitative-quantitative methodological debate. Soc. Sci. Med. 1995, 40, 459–468. [Google Scholar] [CrossRef]
- Thomson, H.; Petticrew, M.; Morrison, D. Health effects of housing improvement: Systematic review of intervention studies. BMJ 2001, 323, 187–190. [Google Scholar] [CrossRef] [Green Version]
- Fishman, R. The American Planning Tradition: Culture and Policy; Woodrow Wilson Center Press: Washington, DC, USA, 2000. [Google Scholar]
- Duhl, L.J.; Sanchez, A.K.; World Health Organization. Healthy Cities and the City Planning Process: A Background Document on Links between Health and Urban Planning; WHO Regional Office for Europe: Copenhagen, Denmark, 1999. [Google Scholar]
- Li, W.; Keegan, T.H.; Sternfeld, B.; Sidney, S.; Quesenberry, C.P., Jr.; Kelsey, J.L. Outdoor falls among middle-aged and older adults: A neglected public health problem. Am. J. Public Health 2006, 96, 1192–1200. [Google Scholar] [CrossRef]
- Oakley, A.; Dawson, M.F.; Holland, J.; Arnold, S.; Cryer, C.; Doyle, Y.; Rice, J.; Hodgson, C.R.; Sowden, A.; Sheldon, T.; et al. Preventing falls and subsequent injury in older people. Qual. Health Care 1996, 5, 243. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatrics. Falls from heights: Windows, roofs, and balconies. Pediatrics 2001, 107, 1188–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falls. Available online: https://www.who.int/news-room/fact-sheets/detail/falls (accessed on 20 July 2018).
- Persily, A. Challenges in developing ventilation and indoor air quality standards: The story of ASHRAE Standard 62. Build. Environ. 2015, 91, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Stollard, P.; Stollard, P. Crime Prevention through Housing Design; Taylor & Francis: London, UK, 2003. [Google Scholar]
- Day, C. Places of the Soul: Architecture and Environmental Design as a Healing Art; Routledge: London, UK, 2017. [Google Scholar]
- Collins, K. Low indoor temperatures and morbidity in the elderly. Age Ageing 1986, 15, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Burge, S.; Hedge, A.; Wilson, S.; Bass, J.H.; Robertson, A. Sick building syndrome: A study of 4373 office workers. Ann. Occup. Hyg. 1987, 31, 493–504. [Google Scholar]
- Holmes, S.H.; Phillips, T.; Wilson, A. Overheating and passive habitability: Indoor health and heat indices. Build. Res. Inf. 2016, 44, 1–19. [Google Scholar] [CrossRef]
- Pitarma, R.; Marques, G.; Ferreira, B.R. Monitoring indoor air quality for enhanced occupational health. J. Med. Syst. 2017, 41, 23. [Google Scholar] [CrossRef]
- Figueiro, M.G.; Steverson, B.; Heerwagen, J.H.; Rea, M.S. Daylight in office buildings: Impact of building design on personal light exposures, sleep and mood. In Proceedings of the 28th Session of the CIE, Manchester, UK, 28 June–4 July 2015. [Google Scholar]
- Freihoefer, K.; Guerin, D.; Martin, C.; Kim, H.Y.; Brigham, J.K. Occupants’ satisfaction with, and physical readings of, thermal, acoustic, and lighting conditions of sustainable office workspaces. Indoor Built Environ. 2015, 24, 457–472. [Google Scholar] [CrossRef]
- Boechat, J.; Rios, J.; Ramos, M.; Luiz, R.; Neto, F.A.; Lapa e Silva, J.R. Sick Building Syndrome (SBS) Among Office Workers and Exposure to Indoor Fungal Allergens in Rio de Janeiro, Brazil. J. Allergy Clin. Immunol. 2011, 127, AB178. [Google Scholar] [CrossRef]
- Shaw, M. Housing and public health. Annu. Rev. Public Health 2004, 25, 397–418. [Google Scholar] [CrossRef] [Green Version]
- Bambra, C. Health Divides: Where You Live Can Kill You; Policy Press: Bristol, UK, 2016. [Google Scholar]
- Benveniste, G. Mastering the Politics of Planning: Crafting Credible Plans and Policies that Make a Difference; Jossey-Bass Inc Publiser: San Francisco, CA, USA, 1989. [Google Scholar]
- Jargowsky, P.A. Poverty and Place: Ghettos, Barrios, and the American City; Russell Sage Foundation: New York, NY, USA, 1997. [Google Scholar]
- Tesh, S.N. Uncertain Hazards: Environmental Activists and Scientific Proof; Cornell University Press: Ithaca, NY, USA, 2018. [Google Scholar]
- Heiman, M.K. Science by the people: Grassroots environmental monitoring and the debate over scientific expertise. J. Plan. Educ. Res. 1997, 16, 291–299. [Google Scholar] [CrossRef]
- Krieger, N. Questioning epidemiology: Objectivity, advocacy, and socially responsible science. Am. J. Public Health 1999, 89, 1151–1153. [Google Scholar] [CrossRef] [PubMed]
- Brawley, E.C. Enriching lighting design. NeuroRehabilitation 2009, 25, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Foraster, M.; Künzli, N.; Aguilera, I.; Rivera, M.; Agis, D.; Vila, J.; Bouso, L.; Deltell, A.; Marrugat, J.; Ramos, R.; et al. High blood pressure and long-term exposure to indoor noise and air pollution from road traffic. Environ. Health Perspect. 2014, 122, 1193–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seabi, J. An epidemiological prospective study of children’s health and annoyance reactions to aircraft noise exposure in South Africa. Int. J. Environ. Res. Public Health 2013, 10, 2760–2777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gou, Z.; Lau, S.S.-Y.; Shen, J. Indoor environmental satisfaction in two LEED offices and its implications in green interior design. Indoor Built Environ. 2012, 21, 503–514. [Google Scholar] [CrossRef]
- Lee, Y.S.; Kim, S.-K. Indoor environmental quality in LEED-certified buildings in the US. J. Asian Archit. Build. Eng. 2008, 7, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Johansson, P.; Svensson, T.; Ekstrand-Tobin, A. Validation of critical moisture conditions for mould growth on building materials. Build. Environ. 2013, 62, 201–209. [Google Scholar] [CrossRef] [Green Version]
- Pietrzyk, K. A systemic approach to moisture problems in buildings for mould safety modelling. Build. Environ. 2015, 86, 50–60. [Google Scholar] [CrossRef]
- Norbäck, D.; Zock, J.; Plana, E.; Heinrich, J.; Tischer, C.; Jacobsen Bertelsen, R.; Olivieri, M. Building dampness and mold in European homes in relation to climate, building characteristics and socio-economic status: The European Community Respiratory Health Survey ECRHS II. Indoor Air 2017, 27, 921–932. [Google Scholar] [CrossRef]
- Kielb, C.; Lin, S.; Muscatiello, N.; Hord, W.; Rogers-Harrington, J.; Healy, J. Building-related health symptoms and classroom indoor air quality: A survey of school teachers in New York State. Indoor Air 2015, 25, 371–380. [Google Scholar] [CrossRef]
- Hwang, T.; Kim, J.T. Effects of indoor lighting on occupants’ visual comfort and eye health in a green building. Indoor Built Environ. 2011, 20, 75–90. [Google Scholar] [CrossRef]
- Ghaffarianhoseini, A.; AlWaer, H.; Omrany, H.; Ghaffarianhoseini, A.; Alalouch, C.; Clements-Croome, D.; Tookey, J. Sick building syndrome: Are we doing enough? Archit. Sci. Rev. 2018, 61, 99–121. [Google Scholar] [CrossRef] [Green Version]
- Dunn, J.R.; Hayes, M.V. Social inequality, population health, and housing: A study of two Vancouver neighborhoods. Soc. Sci. Med. 2000, 51, 563–587. [Google Scholar] [CrossRef]
- MacNaughton, P.; Satish, U.; Laurent, J.G.C.; Flanigan, S.; Vallarino, J.; Coull, B.; Spengler, J.D.; Allen, J.G. The impact of working in a green certified building on cognitive function and health. Build. Environ. 2017, 114, 178–186. [Google Scholar] [CrossRef]
- Richards, E.H. Sanitation in Daily Life; Whitcomb & Barrows: Boston, MA, USA, 1910. [Google Scholar]
- Vaillancourt, J.G. Sociology of the environment: From human ecology to ecosociology. In Environmental Sociology: Theory and Practice; Captus Press: Concord, ON, Canada, 1995; pp. 3–32. [Google Scholar]
- Douglas, I.; James, P. Urban Ecology: An Introduction; Routledge: London, UK, 2014. [Google Scholar]
- Evans, G.W.; McCoy, J.M. When buildings don’t work: The role of architecture in human health. J. Environ. Psychol. 1998, 18, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Wohlwill, J.F. Human adaptation to levels of environmental stimulation. Hum. Ecol. 1974, 2, 127–147. [Google Scholar] [CrossRef]
- Kembel, S.W.; Jones, E.; Kline, J.; Northcutt, D.; Stenson, J.; Womack, A.M.; Bohannan, B.J.; Brown, G.Z.; Green, J.L. Architectural design influences the diversity and structure of the built environment microbiome. ISME J. 2012, 6, 1469. [Google Scholar] [CrossRef] [Green Version]
- Stephens, B. What have we learned about the microbiomes of indoor environments? MSystems 2016, 1, e00083-16. [Google Scholar] [CrossRef] [Green Version]
- Rintala, H.; Pitkäranta, M.; Toivola, M.; Paulin, L.; Nevalainen, A. Diversity and seasonal dynamics of bacterial community in indoor environment. BMC Microbiol. 2008, 8, 56. [Google Scholar] [CrossRef] [Green Version]
- Lax, S.; Smith, D.P.; Hampton-Marcell, J.; Owens, S.M.; Handley, K.M.; Scott, N.M.; Gibbons, S.M.; Larsen, P.; Shogan, B.D.; Weiss, S.; et al. Longitudinal analysis of microbial interaction between humans and the indoor environment. Science 2014, 345, 1048–1052. [Google Scholar] [CrossRef] [Green Version]
- Dunn, R.R.; Fierer, N.; Henley, J.B.; Leff, J.W.; Menninger, H.L. Home life: Factors structuring the bacterial diversity found within and between homes. PLoS ONE 2013, 8, e64133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hospodsky, D.; Qian, J.; Nazaroff, W.W.; Yamamoto, N.; Bibby, K.; Rismani-Yazdi, H.; Peccia, J. Human occupancy as a source of indoor airborne bacteria. PLoS ONE 2012, 7, e34867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, J.A.; Stephens, B. Microbiology of the built environment. Nat. Rev. Microbiol. 2018, 16, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.-S.; Chun, J.; Kim, B.-S. Identification of household bacterial community and analysis of species shared with human microbiome. Curr. Microbiol. 2013, 67, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Brown, G.; Kline, J.; Mhuireach, G.; Northcutt, D.; Stenson, J. Making microbiology of the built environment relevant to design. Microbiome 2016, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Hoisington, A.J.; Brenner, L.A.; Kinney, K.A.; Postolache, T.T.; Lowry, C.A. The microbiome of the built environment and mental health. Microbiome 2015, 3, 60. [Google Scholar] [CrossRef] [Green Version]
- Canter, D.V.; Craik, K.H. Environmental psychology. J. Environ. Psychol. 1981, 1, 1–11. [Google Scholar] [CrossRef]
- Oseland, N. The impact of psychological needs on office design. J. Corp. Real Estate 2009, 11, 244–254. [Google Scholar] [CrossRef]
- Cohen, R.A. Yerkes–Dodson Law. Encycl. Clin. Neuropsychol. 2011, 2737–2738. Available online: https://link.springer.com/referenceworkentry/10.1007%2F978-0-387-79948-3_1340 (accessed on 3 March 2020).
- Franz, G. Space, color, and perceived qualities of indoor environments. In Proceedings of the 19th International Association for People-Environment Studies Conference (IAPS 2006), Seattle, WA, USA, 11–16 September 2006; Hogrefe & Huber: Seattle, WA, USA, 2006. [Google Scholar]
- Nanda, U.; Pati, D.; Ghamari, H.; Bajema, R. Lessons from neuroscience: Form follows function, emotions follow form. Intell. Build. Int. 2013, 5, 61–78. [Google Scholar] [CrossRef]
- Brownson, R.C.; Fielding, J.E.; Maylahn, C.M. Evidence-based public health: A fundamental concept for public health practice. Annu. Rev. Public Health 2009, 30, 175–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, M.; Thompson, J.; de Sá, T.H.; Ewing, R.; Mohan, D.; McClure, R.; Roberts, I.; Tiwari, G.; Giles-Corti, B.; Sun, X.; et al. Land use, transport, and population health: Estimating the health benefits of compact cities. Lancet 2016, 388, 2925–2935. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.; Xiao, W.; Wen, M.; Wei, R. Walkability, land use and physical activity. Sustainability 2016, 8, 65. [Google Scholar] [CrossRef] [Green Version]
- Knuiman, M.W.; Christian, H.E.; Divitini, M.L.; Foster, S.A.; Bull, F.C.; Badland, H.M.; Giles-Corti, B. A longitudinal analysis of the influence of the neighborhood built environment on walking for transportation: The RESIDE study. Am. J. Epidemiol. 2014, 180, 453–461. [Google Scholar] [CrossRef] [Green Version]
- Larice, M.; Macdonald, E. The Urban Design Reader; Routledge: London, UK, 2013. [Google Scholar]
- Jackson, R.J.; Dannenberg, A.L.; Frumkin, H. Health and the built environment: 10 years after. Am. J. Public Health 2013, 103, 1542–1544. [Google Scholar] [CrossRef]
- Wolch, J.R.; Byrne, J.; Newell, J.P. Urban green space, public health, and environmental justice: The challenge of making cities ‘just green enough’. Landsc. Urban Plan. 2014, 125, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Koohsari, M.J.; Badland, H.; Giles-Corti, B. (Re) Designing the built environment to support physical activity: Bringing public health back into urban design and planning. Cities 2013, 35, 294–298. [Google Scholar] [CrossRef]
- Koohsari, M.J.; Mavoa, S.; Villanueva, K.; Sugiyama, T.; Badland, H.; Kaczynski, A.T.; Owen, N.; Giles-Corti, B. Public open space, physical activity, urban design and public health: Concepts, methods and research agenda. Health Place 2015, 33, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Kaczynski, A.T.; Koohsari, M.J.; Stanis, S.A.W.; Bergstrom, R.; Sugiyama, T. Association of street connectivity and road traffic speed with park usage and park-based physical activity. Am. J. Health Promot. 2014, 28, 197–203. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Bull, F.; Knuiman, M.; McCormack, G.; Van Niel, K.; Timperio, A.; Christian, H.; Foster, S.; Divitini, M.; Middleton, N.; et al. The influence of urban design on neighbourhood walking following residential relocation: Longitudinal results from the RESIDE study. Soc. Sci. Med. 2013, 77, 20–30. [Google Scholar] [CrossRef] [Green Version]
- The Drive towards Healthier Buildings 2016. Available online: https://www.worldgbc.org/sites/default/files/Drive%20Toward%20Healthier%20Buildings%202016_ffff.pdf (accessed on 20 July 2018).
- Nelbach, P. An Appraisal Method for Measuring the Quality of Housing: A Yardstick for Health Officers, Housing Officials and Planners. Part III. Appraisal of Neighborhood Environment; American Public Health Association: Washington, DC, USA, 1950. [Google Scholar]
- American Housing Survey: A Measure of (Poor) Housing Quality. Available online: https://www.census.gov/programs-surveys/ahs/research/publications/PoorHousingQuality.html (accessed on 20 July 2018).
- American Planning Association. Planning for Public Health. Available online: https://www.planning.org/research/publichealth/ (accessed on 1 May 2019).
Figure 1.
Connections, divergences, and remerging between public health and the built environment.

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hu, M.; Roberts, J.D. Connections and Divergence between Public Health and Built Environment—A Scoping Review. Urban Sci. 2020, 4, 12. https://doi.org/10.3390/urbansci4010012
AMA Style
Hu M, Roberts JD. Connections and Divergence between Public Health and Built Environment—A Scoping Review. Urban Science. 2020; 4(1):12. https://doi.org/10.3390/urbansci4010012
Chicago/Turabian StyleHu, Ming, and Jennifer D. Roberts. 2020. "Connections and Divergence between Public Health and Built Environment—A Scoping Review" Urban Science 4, no. 1: 12. https://doi.org/10.3390/urbansci4010012