1. Introduction
Quality of life (QoL) perception represents one of the most important aspects in the area of non-communicable chronic degenerative diseases (NCCD), especially regarding long-term life expectancy [
1]. Literature supports the role of physical activity in the improvement of QoL perception in many diseases. Among these, the most commonly considered are hypertension, diabetes, obesity and post-transplant syndrome [
2]. Recently cancer has also been considered in this context, thanks to the positive effect on QoL of exercise as a prescription program [
3,
4]. Meta-analyses in this area have even supported the use of QoL as a prognostic indicator of survival in some patients with cancer [
5,
6]. Individually programmed regular physical activity (PA) is already well known for its long-term advantages for overall cardiovascular risks factors. Few data are, however, available regarding physical exercises prescribed following an “unsupervised” exercise model with cancer patients in particular [
7]. Literature currently supports the importance of regular PA, especially at a moderate level, in this area [
8]. It has reduced comorbidities, enhanced mental well-being and particularly improved QoL [
9].
QoL is a complex term including several parameters: the perception of pain, of cognitive status, of state of the health of one’s role, one’s emotional state and one’s vitality. The study reports a clinical study carried out at the Sports Medicine and Exercise Unit of the University of Florence, Italy, in collaboration with the Regional Reference Center for the Critical Relational Area of Sports Psychology. The aim of this research is to verify the influence of exercise prescription programs on QoL perception parameters in a cohort of surviving cancer patients. The patients were prescribed an exercise program and followed up for at least six months.
2. Materials and Method
A group of 14 surviving cancer patients (nine females with breast cancer and five males with colon cancer) aged 63 ± 15, in stable clinical condition and regularly followed up at the Sports Medicine and Exercise Unit of the University of Florence, were enrolled in the study. This quality of life sub-study was part of a larger study (n = 37) investigating the benefits of a lifestyle intervention in cancer survivors. Among them, five female breast cancer survivors had received on average one line of chemotherapy, in adjuvant or in palliative setting. Four had received a cardiotoxic chemotherapy agent (anthracyclines or trastuzumab) for an average of three cycles of the same chemotherapy treatment (CT). The colon cancer patients had received 5-Fluorulacil or oxaliplatin for at least three cycles of therapy. At the onset of this study all patients were completely free of disease. All patients were between two and four years of treatment. Before being accepted and starting the prescribed exercise program, they were examined by oncologists who evaluated their clinical condition. Following evaluation, eligible patients were further evaluated at the Sports Medicine Center where this specific program has been promoted.
The protocol was approved by the local ethics committee. All subjects gave oral and written consent to participate. They were prescribed the exercise program composed of aerobic and resistance exercises. The aerobic component was of moderate intensity, in general fast walking, established at 70% of the patient’s maximal effort. One resistance exercise in the program was also allowed three times a week. It consisted of exercises of moderate level of intensity, involving at least 8 groups of the body’s main muscles. All mixed exercises were individually established in agreement with the American College of Sports Medicine (ACSM) guidelines [
10]. They were prescribed for unsupervised use at home (i.e., outside the gym and without the presence of specialized trainers). The program included at least three exercise sessions a week to be carried out for six months. This model, previously tested in subjects with similar chronic disease, had been validated [
11]. Adherence to the program was monitored and confirmed by a psychologist through weekly telephone contact with the patients as well as by administration of the SF36 questionnaire in which there is a question regarding the weekly amount of physical exercise carried out. None of the patients enrolled followed a specific diet. However, they were advised to follow normal Mediterranean nutritional habits that include at least two daily portions of fruit and three of vegetables as well as fish three times a week and two portions of cereals weekly. Aerobic and resistance exercises were individually prescribed taking into consideration the data that emerged from a patient’s first medical examination (T0). The exercise prescription was adapted after six months of training if considered necessary. All subjects underwent cardiovascular evaluation and specific strength and flexibility tests. The intensity of the aerobic exercise was established by the six-minute walking test (6MWT) on the basis of the maximal heart rate reached at the end of the test. The chair test and hand grip strength tests for the evaluation of upper and lower limbs were performed to establish the amount of the resistance exercise. In order to check whether patients adhered constantly to the protocol, to advice on diet and eating habits, they were periodically contacted by the psychologist through mobile phone. In addition the following anthropometric parameters were also evaluated: body mass index (BMI) calculated from height and weight data [
12], skin fold and hydration status. To investigate QoL perception a special questionnaire was administered at the beginning of the study and after six months. It consisted in an SF36 validated model [
13] in which all the QoL parameters are included and interpreted on the basis of the specific score model. The investigation offers information on perception of the level of physical activity, mental health, emotional status, health perception, pain perception. At the same time nutritional habits were also evaluated by another specific and validated questionnaire regarding adherence to the Mediterranean diet [
14]. This questionnaire is normally used to predict the prevalence of hypertension, hypercholesterolemia, diabetes and obesity. It is therefore considered fundamental in the present study, to complete the investigation. All data of cancer patients obtained at the beginning of the study were compared with the values found after six months of constant adherence to the exercise program prescribed.
2.1. SF36 Questionnaire
Health-related QoL was assessed through the Italian version of the Short Form Health Survey (SF36) questionnaire. This tool has been validated in several experimental and observational studies regarding different chronic diseases. It has been widely used in clinical studies involving Italian subjects since 1990 and is a validated questionnaire used throughout Italy [
15]. This questionnaire can be self administered. It is auto-multidimensional and consists of 36 items combined into eight scaled scores including eight health domains: PF—physical functioning (ten questions), RP—role physical—limitations due to impaired physical health (four questions), RE—role emotional—limitations due to emotional problems (three questions), BP—physical Body-Pain (two questions), GH—perception of general health (five questions), VT—vitality (four questions), SF—social functioning (two questions), MH—mental health (five questions) and a single question on change in health status.
2.2. Statistical Analysis
The anthropometrics and nutritional data are expressed as mean ± SD. The data of the QoL parameters were derived from the SF36 questionnaire and reported as mean values. The scores were recoded, recalibrated, and converted into 0–100 scores. The summary scores were computed using the Italian population normative values for the same age, and Z-score was also calculated. The correlation coefficient (r) between the dietary habits and QoL perception parameters was also evaluated. A p-value < 0.05 was considered statistically different.
3. Results
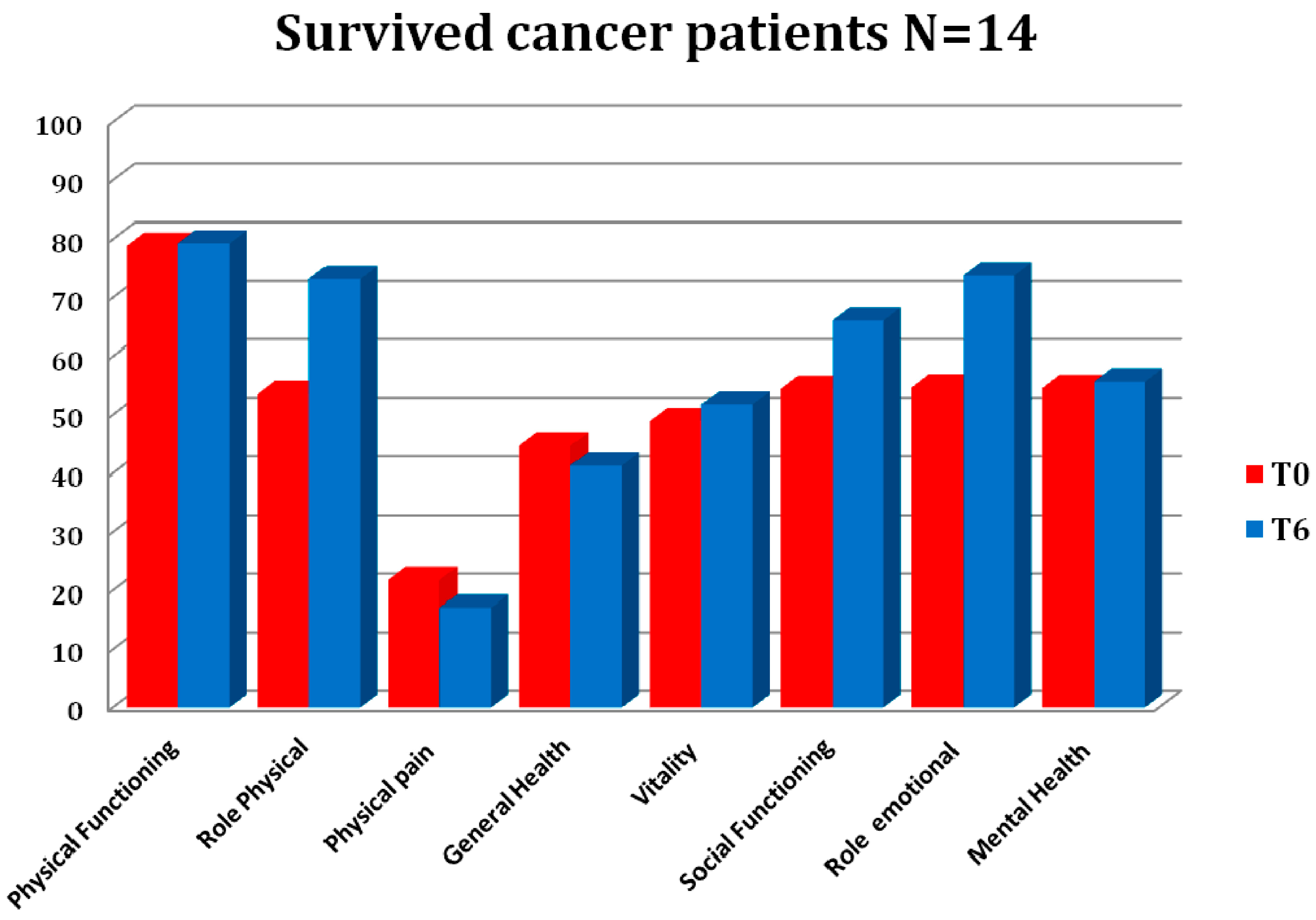
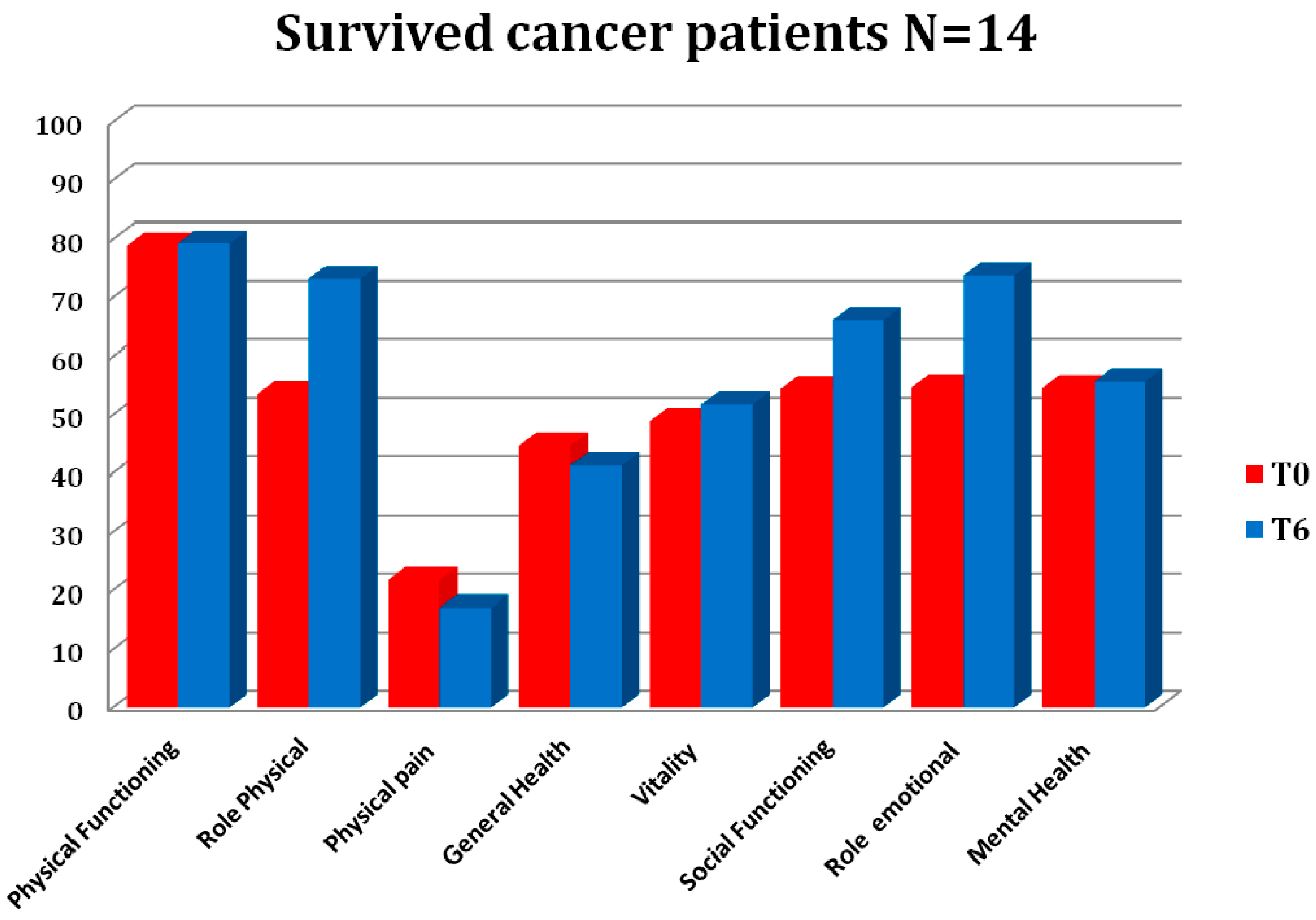
Weekly phone calls to monitor protocol adherence revealed that all the 14 patients (100%) enrolled were constantly adherent to the protocol, despite the females being more convinced in general than the men. They were very satisfied to maintain contact with the sports medicine center by phone calls and none of them had abandoned the program. Considering the importance of controlling this aspect, we constantly took care to regularly update this aspect. A significant improvement in QoL parameters was found in the group analyzed after exercise training, as reported in
Table 1 and
Figure 1. A significant reduction of pain and an increase of RP were observed. The PF (physical functioning) level perception increased significantly after six months (T0: 78.9; T6: 79.2;
p < 0.05) as well as the mental health (T0: 54.6; T6: 55.7;
p < 0.05). RP and RE improved (T0: 54.7; T6: 73.8;
p < 0.05), and pain perception was reduced (T0: 21.8; T6: 17.1;
p < 0.05), while vitality and social SF36 parameters increased significantly as reported in
Table 1. From the analysis of food diaries, a significant improvement of the mean frequency of meals per day (T0: 3.08 ± 0.48; T6: 3.69 ± 0.63;
p < 0.05) and a very significant reduction in quantity of food intake as demonstrated by calorie intake (T0: 1893.23 ± 315.59; T6: 1660 ± 182.8;
p < 0.01) were observed. In addition, among the anthropometric parameters, the triceps folds were also significantly reduced (T0: 18.96 ± 6.31; T6: 17.66 ± 6.4;
p < 0.05) as well as the waist circumferences expressed in cm (T0: 90.11 ± 10.2; T6: 88.60 ± 10.44), although not significantly. The BMI remained stable (T0: 25.33 ± 2.7; T0: 25.10 ± 2.6). The data of QoL correlated negatively with dietary habits (
r = −0.647;
p < 0.05). The PA level perception correlated also significantly with the frequency of meals (
r = 0.706;
p < 0.01) and with the role of emotional behavior (
r = 0.746;
p < 0.01). The PA correlated negatively with pain perception (
r = −0.593;
p < 0.05) and with vitality (
r = 0.690;
p < 0.01).
4. Discussion
There is some evidence in the literature that exercise is actually the best medicine for reducing anxiety, decreasing the negative effects of depression and effectively helping to manage stress, especially in non communicable chronic diseases (NCCD) [
14,
16,
17]. Particularly for surviving cancer patients’ QoL perception, exercise is one of the most important aspects. In these patients, a complete lifestyle intervention is often called for [
4,
18]. Although the literature mainly supports the role of supervised exercise, regular unsupervised prescribed PA should be considered for the positive effects that it demonstrates, in a short time, on many aspects of QoL that affect the social and relational life. Adherence to the type of exercise is the main limitation of planned PA. The possibility to adjust the PA programs to the characteristics of the individual, particularly those subjects with highly disabling diseases and consequently reduced exercise capacity, is, in our opinion, an important aspect in favor of such a program and its marked utility in cancer patients. For this reason we believe the program deserves to be divulged.
The necessity to go beyond the area of cardiovascular risk is now well known everywhere. It is important to extend the evaluation of QoL to more complex and consistent elements that are the basis of social relationships. This requires evaluating and controlling in terms of follow-up. On these terms the role of unsupervised exercise in diseases with long-term life expectancy should be considered, especially where the progressive improvement of the aim is to recover QoL. We suppose that the general health parameter, as a global health QoL perception, and therefore as a sort of the summary of the values of the single parameters, cannot show a significant improvement. We are aware that the inclusion of other data such as the physical component summary score (PCS) could be very helpful for a good interpretation, particularly in the case of a small sample. The normalization to a Z-score using normative Italian data did not show any significant variation. All parameters in the QoL investigation are therefore fundamental for pure well being.
The present investigation is limited to a restricted group of subjects, all of whom are very motivated to take part in the study. They consequently adhere closely to its aims. The data obtained cannot at this stage yield results common to all cancer patients. Although potentially important, this is, at the moment, preliminary data prompting further investigation into this field. The lack of SF36 summary scores (mental and physical component scores) for a complete analysis of QoL is a limitation of our study.
This accompanied by a general reduction in emotional distress and reduced perception of pain. In particular, there was a significant improvement of all the parameters related to QoL that are also positively correlated with eating habits, especially the frequency and distribution of daily meals and choice of food. All these data support the role of QoL investigation in identifying the parameters strongly related to cardiovascular risk. The present study nevertheless needs to be considered a pilot investigation. More complete, larger evaluations are necessary for confirming the data.
The PA exercise model can reveal the needs and improvements in the areas of metabolic chronic diseases, as long as adherence to the program is constant with only eventual minor discontinuity. Exercise programs are safe and effective for QoL and depression in breast cancer patients, whose treatment needs to be completed [
19]. This aspect could be particularly important considering that the prevention of cognitive dysfunction in cancer patients is one of the main targets in the context of the PA exercise model [
20].
The positive effects of regular PA interventions are more pronounced, with moderate or vigorous intensity, with respect to mild-intensity exercise programs, as can be observed in the case of the unsupervised program where the level of exercise can be easily maintained. This study can in fact be considered a pilot study because the PA model has been applied in an unsupervised form and in a small sample of cancer patients.
The results of the QoL analyzed must be interpreted cautiously and we reasonably believe that more and larger studies, preferably with a randomized design, will be necessary to confirm these data.
Acknowledgments
The study did not receive any grant or financial support. We wish to thank Susan Seeley for her revision of the English.
Author Contributions
Laura Stefani conceived and wrote the paper; Mattia Rotelli and Angelica Frulli analyzed and elaborated all the data; Luca Amoroso, Laura Belloni and Giorgio Galanti revised and approved the final version of the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [PubMed]
- Galanti, G.; Stefani, L.; Mascherini, G.; Petri, C.; Corsani, I.; Francini, L.; Cattozzo, A.; Gianassi, M.; Minetti, E.; Pacini, A.; et al. Short term perspective study of prescribed physical activity in kidney transplant recipients. Intern. Emerg. Med. 2016, 11, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Galanti, G.; Stefani, L.; Gensini, G.F. Exercise as a prescription therapy for breast and colon cancer survivors. Int. J. Gen. Med. 2013, 6, 245–251. [Google Scholar] [PubMed]
- Stefani, L.; Mascherini, G.; Petri, C.; Galanti, G. Lifestyle intervention in surviving cancer patients. J. Funct. Morphol. Kinesiol. 2016, 1, 48–53. [Google Scholar] [CrossRef]
- Quinten, C.; Coens, C.; Mauer, M.; Comte, S.; Sprangers, M.A.G.; Cleeland, C.; Osoba, D.; Bjordal, K.; Bottomley, A. Base line quality of life as a prognostic indicator of survival: A meta-analysis of individual patient data from EORTC clinical trials. Lancet Oncol. 2009, 10, 865–871. [Google Scholar] [CrossRef]
- Montazeri, A. Quality of life data as prognostic indicators of survival in cancer patients: An overview of the literature from 1982 to 2008. Health Qual. Life Outcomes 2009, 7. [Google Scholar] [CrossRef] [PubMed]
- Karvinen, K.H.; Courneya, K.S.; North, S.; Venner, P. Associations between exercise and quality of life in bladder cancer survivors: A population-based study. Cancer Epidemiol. Biomark. Prev. 2007, 16, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Winters-Stone, K.; Lee, A.; Schmitz, K.S. Cancer, physical activity, and exercise. Compr. Physiol. 2012, 2, 2775–2809. [Google Scholar] [PubMed]
- King, S.; Green, H.J. Psychological intervention for improving cognitive function in cancer survivors: A literature review and randomized controlled trial. Front. Oncol. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; Available online: http://www.acsm.org (accessed on 1 July 2013).
- Brocki, B.C.; Andreasen, J.; Nielsen, L.R.; Nekrasas, V.; Gorst-Rasmussen, A.; Westerdahl, E. Short and long-term effects of supervised versus unsupervised exercise training on health-related quality of life and functional outcomes following lung cancer surgery—A randomized controlled trial. Lung Cancer 2014, 83, 102–108. [Google Scholar] [CrossRef] [PubMed]
- FAO/WHO/UNU. Human Energy Requirements: Report of a Joint FAO/WHO/UNU Expert Consultation, Rome 17–24 October 2001; FAO: Rome, Italy, 2004. [Google Scholar]
- McHorney, C.A.; Ware, J.E.; Raczek, A.E. The MOS 36-Itern Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Arvaniti, F.; Stefanadis, C. Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the MedDietScore. Prev. Med. 2007, 44, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Apolone, G.; Mosconi, P.; Ware, J.E. Questionario sullo Stato di Salute SF-36. Manuale d’uso e Guida All’Interpretazione dei Risultati; Milano Edizioni Angelo Guerini Associati SpA: Milano, Italy, 1997. [Google Scholar]
- Sechi, A.; Deroma, L.; Paci, S.; Lapolla, A.; Carubbi, F.; Burlina, A.; Rigoldi, M.; di Rocco, M. Quality of life in adult patients with glycogen storage disease type I: Results of a multicenter Italian study. JIMD Rep. 2014, 14, 47–53. [Google Scholar] [PubMed]
- Adams, T.; Moore, M.; Dye, J. The relationship between physical activity and mental health in a national sample of college females. Women Health 2007, 45, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Adlard, P.; Cotman, C. Voluntary exercise protects against stress-induced decreases in brain-derived neurotrophic factor protein expression. Neuroscience 2004, 124, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Sabiston, C.M.; McDonough, M.H.; Crocker, P.R. Psychosocial experiences of breast cancer survivors involved in a dragon boat program: Exploring links to positive psychological growth. J. Sport Exerc. Psychol. 2007, 29, 419–438. [Google Scholar] [CrossRef] [PubMed]
- Hassmen, P.; Koivula, N. Physical exercise and psychological well-being: A population study in Finland. Prev. Med. 2001, 30, 17–25. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}