The Hazards of a Biomedical Exercise Paradigm: Exploring the Praxis of Exercise Professionals

{kind=link}
Abstract
:1. Introduction
A few times I said to the personal trainer I was finding it tough and I didn’t know if I could carry on. ‘But he encouraged me to dig deep to do the best possible. As he was the professional. I did as he asked. I thought no pain, no gain’.
2. Issues of Scientism in Medicine
- Disease is defined as a deviation from a statistical norm and measurable level of biological functioning.
- Each defined disease is a specific and individual ‘entity’; generic regardless of culture and context.
- Medicine is a neutral, objective science without recourse to relational, metaphysical or existential considerations.
- Medicine allows for an ontological foundation of mind-body dualism.
The ACSM [American College of Sports Medicine] promotes and integrates scientific research, education and practical applications of sports medicine and exercise science to maintain and enhance physical performance, fitness, health and quality of life.[36], (p. 24)
A new form of exercise may allegedly produce significant results, but if it is not supported by scientific research, it becomes a questionable trend.[37], (p. 8)
3. Evidence for a Biomedical Scientism in Exercise Praxis
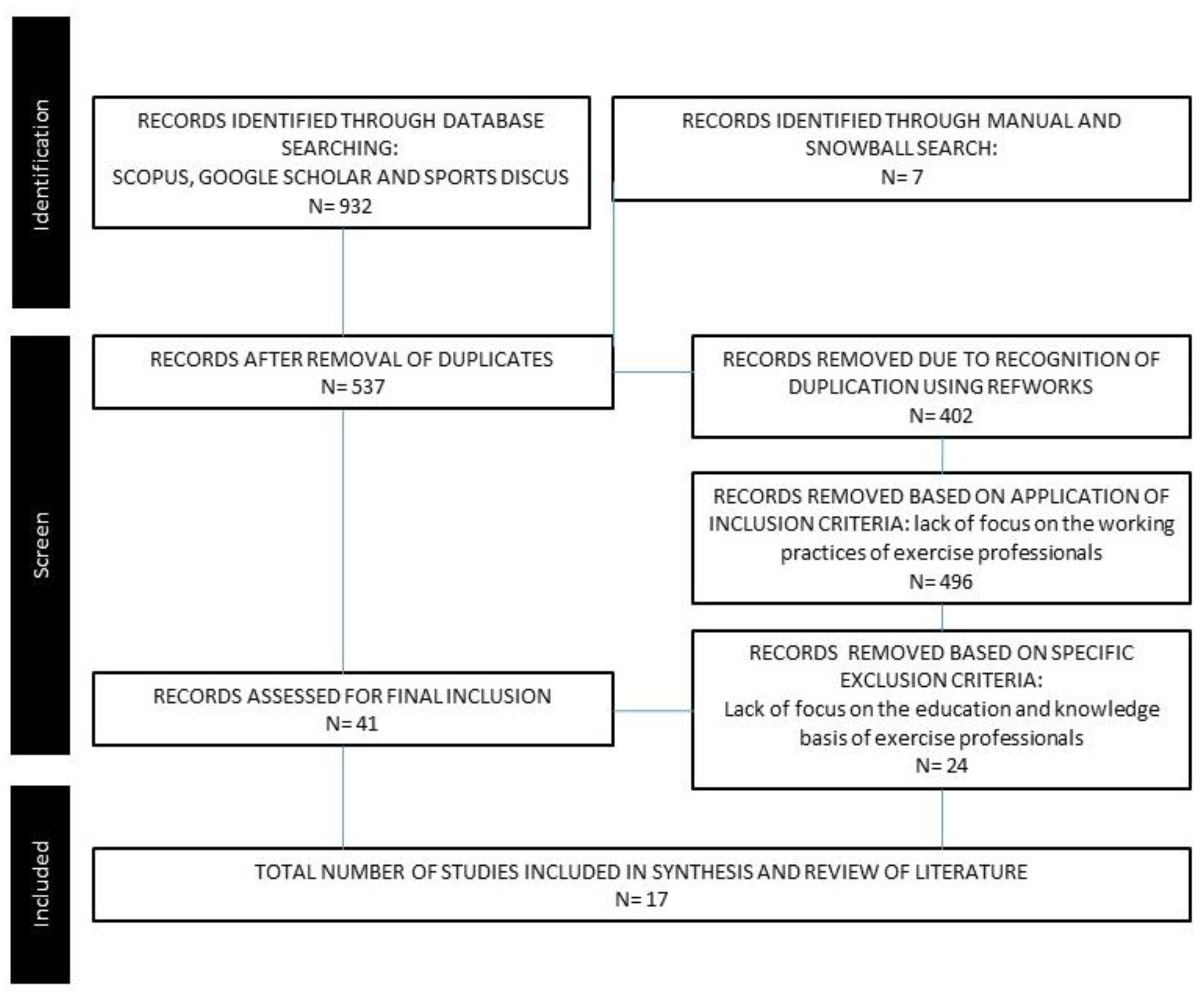
3.1. Method
3.2. Analysis
3.2.1. Epistemology
3.2.2. Ontology
3.2.3. Axiology
“…even in its simplest forms on the animal level, play is more than a mere physiological phenomenon or a psychological reflex. It goes beyond the confines of purely physical or purely biological activity. It is a significant function…In play there is something ‘at play’ which transcends the immediate needs of life and imparts meaning to the action.”[68], (p. 19)
4. Discussion
5. Conclusions
- Exercise professional education should be structured in a manner which highlights the need for praxis. Professionals should be made aware of both the strengths and limits of a techno-rational process and its scientific foundations.
- Exercise professional education should consider a greater holistic definition of professional knowledge beyond biomedical propositional concepts and theory.
- Exercise professionals should be exposed to axiological notions of exercise beyond the linearity of medical data. The values of existential wellbeing and notions of play should be explicitly introduced into the educational process.
- Exercise professional education should place greater emphasis on pedagogies which explore the issues of ethical programming, individualized physical activity, and client relationships. Consequently research should be undertaken into the appropriateness of utilizing online, digital and blended learning technologies within future education.
Funding
Acknowledgments
Conflicts of Interest
References
- Greene, L. ‘Fit’ to Be Tried—$1.1M Workout Lawsuit. New York Post. 23 March 2004. Available online: https://nypost.com/2004/03/23/fit-to-be-tried-1-1m-workout-lawsuit (accessed on 15 July 2019).
- Smith-Squire, A. One Hour with a Personal Trainer Put This Woman in Hospital for Four Days: Rebecca Suffered Rare Muscle Condition Brought on by Exercising Too Hard. Mail Online. 9 December 2013. Available online: https://www.dailymail.co.uk/health/article-2521007/Rebecca-Johnson-suffered-rare-muscle-condition-brought-exercising-hard.html (accessed on 15 July 2019).
- Branco, J. National Gym Chain, Personal Trainer Sued after Man Spends Week in Hospital. Brisbane Times. 10 July 2017. Available online: https://www.brisbanetimes.com.au/national/queensland/national-gym-chain-personal-trainer-sued-after-man-spends-week-in-hospital-20170709-gx7q1p.html (accessed on 15 July 2019).
- Sinert, R.; Kohl, L.; Rainone, T.; Scalea, T. Exercise-induced rhabdomyolysis. Ann. Emerg. Med. 1994, 23, 1301–1306. [Google Scholar] [CrossRef]
- Aalborg, C.; Rød-Larsen, C.; Leiro, I.; Aasebø, W. An increase in the number of admitted patients with exercise-induced rhabdomyolysis. Tidsskr. Nor. Laegeforen. Tidsskr. Prakt. Med. Raekke. 2016, 136, 1532–1536. [Google Scholar] [CrossRef] [PubMed]
- Khalil, M.A.; Saab, B.R. Resistance exercise-induced rhabdomyolysis: Need for immediate intervention and proper counselling. Aust. Fam. Physician. 2016, 45, 898–901. [Google Scholar] [PubMed]
- Eickhoff-Shemek, J.M. An analysis of 8 negligence lawsuits against personal fitness trainers: 3 major liability exposures revealed. ACSM’s Health Fit. J. 2010, 14, 34–37. [Google Scholar] [CrossRef]
- Ciccolella, M.E.; Moore, B.; VanNess, J.M.; Wyant, J. Exertional Rhabdomyolysis and the Law: A Brief Review. J. Exerc. Physiol. Online 2014, 17, 19–27. [Google Scholar]
- Pullen, E.; Malcolm, D. Assessing the effects of the exercise pill. Qual. Res. Sport Exerc. Health. 2018, 10, 493–504. [Google Scholar] [CrossRef]
- Cairney, J.; McGannon, K.R.; Atkinson, M. Exercise is medicine: Critical considerations in the qualitative research landscape. Qual. Res. Sport Exerc. Health. 2018, 10, 391–399. [Google Scholar] [CrossRef]
- Williams, T.L.; Hunt, E.R.; Papathomas, A.; Smith, B. Exercise is medicine? Most of the time for most; but not always for all. Qual. Res. Sport Exerc. Health. 2018, 10, 441–456. [Google Scholar] [CrossRef]
- Lessl, T.M. Naturalizing science: Two episodes in the evolution of a rhetoric of scientism. West. J. Commun. 1996, 60, 379–396. [Google Scholar] [CrossRef]
- Porter, R. The Cambridge History of Medicine; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Williams, S.J. Medicine and the Body; Sage: London, UK, 2003. [Google Scholar]
- Freund, P.E.; McGuire, M.B.; Podhurst, L.S. Health, Illness, and the Social Body: A Critical Sociology; Prentice Hall: Upper Saddle River, NJ, USA, 2003. [Google Scholar]
- Nicholson, D.J. The machine conception of the organism in development and evolution: A critical analysis. Stud. Hist. Philos. Sci. Part C Stud. Hist. Philos. Biol. Biomed. Sci. 2014, 48, 162–174. [Google Scholar] [CrossRef] [Green Version]
- Kontopodis, M. Biomedicine, psychology and the kindergarten: Children at risk and emerging knowledge practices. Sport Educ. Soc. 2013, 18, 475–493. [Google Scholar] [CrossRef]
- Quirke, V.; Gaudillière, J.P. The era of biomedicine: Science, medicine, and public health in Britain and France after the Second World War. Med Hist. 2008, 52, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Haack, S. Defending Science-Within Reason: Between Scientism and Cynicism; Prometheus Books: London, UK, 2011. [Google Scholar]
- Williams, R.N.; Robinson, D.N. Scientism: The New Orthodoxy; Bloomsbury Publishing: New York, NY, USA, 2014. [Google Scholar]
- Busfield, J. The concept of medicalization reassessed. Sociol. Health Illn. 2017, 39, 759–774. [Google Scholar] [CrossRef] [PubMed]
- Giddens, A. The Constitution of Society: Outline of the Theory of Structuration; University of California Press: Berkeley, CA, USA, 1984. [Google Scholar]
- Gray, J. The Soul of the Marionette: A Short Inquiry into Human Freedom; Farrar, Straus and Giroux: New York, NY, USA, 2015. [Google Scholar]
- Sorell, T. Scientism: Philosophy and the Infatuation with Science; Routledge: Abingdon, UK, 2013. [Google Scholar]
- Voegelin, E. Science, Politics and Gnosticism; ISI Books: Wilmington, DE, USA, 1968. [Google Scholar]
- Illich, I. Medical Nemesis: The Expropriation of Health; Pantheon Books: New York, NY, USA, 1974. [Google Scholar]
- Baron, R.J. Why Aren’t More Doctors Phenomenologists? In The Body in Medical Thought and Practice; Leder, D., Ed.; Springer: Dordrecht, The Netherlands, 1992. [Google Scholar]
- Pelligrino, E.D.; Thomasma, D.C. A Philosophical Basis of Medical Practice; Oxford University Press: Oxford, UK, 1981. [Google Scholar]
- Jewson, N.D. The disappearance of the sick-man from medical cosmology, 1770–1870. Int. J. Epidemiol. 2009, 38, 622–633. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, S. Medical Nemesis 40 years on: The enduring legacy of Ivan Illich. J. R. Coll. Physicians Edinb. 2016, 46, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Miles, A. From evidence-based to evidence-informed, from patient-focussed to person-centered—The ongoing “energetics” of health and social care discourse as we approach the Third Era of Medicine. J. Eval. Clin. Pract. 2017, 23, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Sallis, R.E. Exercise is medicine and physicians need to prescribe it! Br. J. Sports Med. 2009, 43, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Sallis, R.; Franklin, B.; Joy, L.; Ross, R.; Sabgir, D.; Stone, J. Strategies for promoting physical activity in clinical practice. Prog. Cardiovasc. Dis. 2015, 57, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Williams, O.; Gibson, K. Exercise as a poisoned elixir: Inactivity, inequality and intervention. Qual. Res. Sport Exerc. Health. 2018, 10, 412–428. [Google Scholar] [CrossRef]
- Neville, R.D. Exercise is medicine: Some cautionary remarks in principle as well as in practice. Med. Health Care Philos. 2013, 16, 615–622. [Google Scholar] [CrossRef]
- Bushman, B.A.; Battista, R.; Swan, P.; Ransdell, L.; Thompson, W.R. ACSM’s Resources for the Personal Trainer; Wolters Kluwer Health: New York, NY, USA, 2013. [Google Scholar]
- McGill, E.A.; Montel, I. NASM Essentials of Personal Fitness Training; Jones & Bartlett Learning: Burlington, MA, USA, 2017. [Google Scholar]
- McFee, G. Ethics, Knowledge and Truth in Sports Research: An Epistemology of Sport; Routledge: Abingdon, UK, 2010. [Google Scholar]
- Griffin, J. Client-Centered Exercise Prescription, 3E; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Nesti, M. Existential Psychology and Sport: Implications for Research and Practice; Routledge: London, UK, 2004. [Google Scholar]
- Corlett, J. Sophistry, Socrates and Sport Psychology. Sport Psychol. 1996, 10, 84–94. [Google Scholar] [CrossRef]
- Fahlberg, L.L.; Fahlberg, K.; Gates, W.K. Exercise and existence: Exercise behavior from an existential-phenomenological perspective. Sport Psychol. 1992, 6, 172–191. [Google Scholar] [CrossRef]
- Smith, A. Exercise is recreation not medicine. J. Sport Health Sci. 2016, 5, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Rejeski, W.J. Dose-response issues from a psychosocial perspective. In Physical Activity, Fitness and Health; Bouchard, C., Shephard, R.J., Stephens, T., Eds.; Human Kinetics: Champaign, IL, USA, 1994. [Google Scholar]
- De Lyon, A.T.; Neville, R.D.; Armour, K.M. The role of fitness professionals in public health: A review of the literature. Quest 2017, 69, 313–330. [Google Scholar] [CrossRef]
- Akerson, M. Investigating Personal Fitness Trainers’ Qualifications. Ph.D. Thesis, University of Central Florida, Orlando, FL, USA, 2014. Available online: https://stars.library.ucf.edu/cgi/viewcontent.cgi?referer=&httpsredir=1&article=4014&context=etd (accessed on 15 July 2019).
- Barnes, K.; Desbrow, B.; Ball, L. Personal trainers are confident in their ability to provide nutrition care: A cross-sectional investigation. Public Health 2016, 140, 39–44. [Google Scholar] [CrossRef]
- Bennie, J.A.; Wiesner, G.H.; van Uffelen, J.G.; Harvey, J.T.; Biddle, S.J. Sources of practice knowledge among Australian fitness trainers. Transl. Behav. Med. 2017, 7, 741–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bratland-Sanda, S.; Sundgot-Borgen, J. “I’m concerned—What Do I Do?” recognition and management of disordered eating in fitness center settings. Int. J. Eat. Disord. 2015, 48, 415–423. [Google Scholar] [CrossRef]
- Dietrich, J.; Keyzer, P.; Jones, V.; Norton, K.; Sekendiz, B.; Gray, S.; Finch, C. Train the trainers: Maintaining standards to minimise injuries and avoiding legal liability in the fitness industry. J. Sci. Med. Sport. 2014, 18, e3. [Google Scholar] [CrossRef]
- Gray, J.; Smith, A.; James, H. An Aristotelian investigation into personal training. Health Fit. J. Can. 2014, 7, 33–47. [Google Scholar]
- Keyzer, P.; Coyle, I.; Dietrich, J.; Norton, K.; Sekendiz, B.; Jones, V.; Finch, C.F. Legal Risk Management and Injury in the Fitness Industry: The Outcomes of Focus Group Research and a National Survey of Fitness Professionals. Available online: https://www.latrobe.edu.au/__data/assets/pdf_file/0004/589153/JLM-June-2014_Keyzer-et-al-article.pdf (accessed on 15 July 2019).
- McKean, M.R.; Slater, G.; Oprescu, F.; Burkett, B.J. Do the nutrition qualifications and professional practices of registered exercise professionals align? Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 154–162. [Google Scholar] [CrossRef]
- McKean, M.; Mitchell, L.; O’Connor, H.; Prvan, T.; Slater, G. Are exercise professionals fit to provide nutrition advice? An evaluation of general nutrition knowledge. J. Sci. Med. Sport. 2018, 22, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Waryasz, G.R.; Daniels, A.H.; Gil, J.A.; Suric, V.; Eberson, C.P. Personal trainer demographics, current practice trends and common trainee injuries. Orthop. Rev. 2016, 8, 6600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wojtowicz, A.E.; Alberga, A.S.; Parsons, C.G.; von Ranson, K.M. Perspectives of Canadian fitness professionals on exercise and possible anorexia nervosa. J. Eat. Disord. 2015, 3, 40. [Google Scholar] [CrossRef] [PubMed]
- Zenko, Z.; Ekkekakis, P. Knowledge of exercise prescription guidelines among certified exercise professionals. J. Strength Cond. Res. 2015, 29, 1422–1432. [Google Scholar] [CrossRef]
- Anderson, G.; Elliott, B.; Woods, N. The Canadian personal training survey. J. Exerc. Physiol. Online 2010, 13, 19–28. [Google Scholar]
- Andreasson, J.; Johansson, T. ‘Doing for group exercise what McDonald’s did for hamburgers’: Les Mills, and the fitness professional as global traveller. Sport Educ. Soc. 2016, 21, 148–165. [Google Scholar] [CrossRef]
- Barnes, K.; Ball, L.; Desbrow, B. Personal trainer perceptions of providing nutrition care to clients: A qualitative exploration. Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 186–193. [Google Scholar] [CrossRef]
- Dias, M.R.; Simão, R.F.; Saavedra, F.J.; Ratamess, N.A. Influence of a personal trainer on self-selected loading during resistance exercise. J. Strength Cond. Res. 2017, 31, 1925–1930. [Google Scholar] [CrossRef]
- Lyon, A.T.; Cushion, C.J. The acquisition and development of fitness trainers’ professional knowledge. J. Strength Cond. Res. 2013, 27, 1407–1422. [Google Scholar] [CrossRef]
- Fox, M.; Green, G.; Martin, P. Doing Practitioner Research; Sage: London, UK, 2007. [Google Scholar]
- Brown, T.C.; Fry, M.D. Motivational climate, staff and members’ behaviors, and members’ psychological well-being at a national fitness franchise. Res. Q. Exerc. Sport. 2014, 85, 208–217. [Google Scholar] [CrossRef]
- Campos, F.; Martins, F.; Simões, V.; Franco, S. Fitness participants perceived quality by age and practiced activity. J. Phys. Educ. Sport. 2017, 17, 698–704. [Google Scholar]
- Hart, S.L. Axiology—Theory of values. Philos. Phenomenol. Res. 1971, 32, 29–41. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Landolfo, C.; Niebauer, J.; Ozemek, C.; Arena, R.; Lavie, C.J. Promoting physical activity and exercise: JACC health promotion series. J. Am. Coll. Cardiol. 2018, 72, 1622–1639. [Google Scholar] [CrossRef] [PubMed]
- Huizinga, J. Homo Ludens: A Study of the Play Element in Culture; Temple Smith: London, UK, 1970. [Google Scholar]
- Nesti, M.S. Exercise for health: Serious fun for the whole person. J. Sport Health Sci. 2016, 5, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, H. The playful and the serious: An approximation to Huizinga’s Homo Ludens. Game Stud. 2006, 6, 1604–7982. [Google Scholar]
- Heyward, V.H.; Gibson, A. Advanced Fitness Assessment and Exercise Prescription, 7th ed.; Human Kinetics: Champagne, IL, USA, 2014. [Google Scholar]
- Hewa, S.; Hetherington, R.W. Specialists without spirit: Limitations of the mechanistic biomedical model. Theor. Med. 1985, 16, 129–139. [Google Scholar] [CrossRef]
- Rubenstein, R.E. Aristotle’s Children; Harcourt Inc.: Oakland, CA, USA, 2003. [Google Scholar]
- Bergdolt, K. Wellbeing: A Cultural History of Healthy Living; Polity: Cambridge, UK, 2008. [Google Scholar]
- Robbins, B.D. The Medicalized Body and Anaesthetic Culture. In The Medicalized Body and Anesthetic Culture; Robbins, B.D., Ed.; Palgrave Macmillan: New York, NY, USA, 2018. [Google Scholar]
- Louis-Courvoisier, M.; Mauron, A. He found me very well; for me, I was still feeling sick’: The strange worlds of physicians and patients in the 18th and 21st centuries. Med. Humanit. 2002, 28, 9–13. [Google Scholar] [CrossRef]
- Baron, R.J. An introduction to medical phenomenology: I can’t hear you while I’m listening. Ann. Intern. Med. 1985, 103, 606–611. [Google Scholar] [CrossRef]
- Markula, P.; Chikinda, J. Group fitness instructors as local level health promoters: A Foucauldian analysis of the politics of health/fitness dynamic. Int. J. Sport Policy Politics 2016, 8, 625–646. [Google Scholar] [CrossRef]
- Rawson, E.S.; Clarkson, P.M.; Tarnopolsky, M.A. Perspectives on exertional rhabdomyolysis. Sports Med. 2017, 47, 33–49. [Google Scholar] [CrossRef]
- Schön, D.A. The Reflective Practitioner: How Professionals Think in Action; Basic Book Inc.: New York, NY, USA, 1983. [Google Scholar]
- Eraut, M. Developing Professional Knowledge and Competence; Routledge: London, UK, 2002. [Google Scholar]
- Kavanagh, J.M.; Szweda, C. A crisis in competency: The strategic and ethical imperative to assessing new graduate nurses’ clinical reasoning. Nurs. Educ. Perspect. 2017, 38, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Eastwood, J.L.; Koppelman-White, E.; Mi, M.; Wasserman, J.A.; Krug, E.F., III; Joyce, B. Epistemic cognition in medical education: A literature review. Int. J. Med. Educ. 2017, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Schraw, G.; Brownlee, J.L.; Olafson, L.; Brye, M.V.V. Teachers’ Personal Epistemologies: Evolving Models for Informing Practice; IAP: Charlotte, NC, USA, 2017. [Google Scholar]
- Renedo, A.; Komporozos-Athanasiou, A.; Marston, C. Experience as evidence: The dialogic construction of health professional knowledge through patient involvement. Sociology 2018, 52, 778–795. [Google Scholar] [CrossRef]
- McNamee, M. Positivism, Popper and Paradigms: An introductory essay in the philosophy of science. In Philosophy and the Sciences of Exercise, Health and Sport: Critical Perspectives on Research Methods; McNamee, M., Ed.; Routledge: London, UK, 2005. [Google Scholar]
| 1 | Websites accessed 15/07/19. |
| 2 | Google search “online pt courses uk“ undertaken 23/07/19 https://www.google.co.uk/search?source=hp&ei=8sg2XcKhKK2GjLsPlpa_kAQ&q=online+pt+courses+UK&oq=online+pt+courses+UK&gs_l=psy-ab.3..0j0i22i30l5.958.5348..5572...0.0..0.182.1322.19j2......0....1..gws-wiz.....0..35i39j0i131.PtOJ_zpOPD8&ved=0ahUKEwjC4uKd08rjAhUtA2MBHRbLD0IQ4dUDCAo&uact=5. |

© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gray, J. The Hazards of a Biomedical Exercise Paradigm: Exploring the Praxis of Exercise Professionals. Philosophies 2019, 4, 54. https://doi.org/10.3390/philosophies4030054
Gray J. The Hazards of a Biomedical Exercise Paradigm: Exploring the Praxis of Exercise Professionals. Philosophies. 2019; 4(3):54. https://doi.org/10.3390/philosophies4030054
Chicago/Turabian StyleGray, John. 2019. "The Hazards of a Biomedical Exercise Paradigm: Exploring the Praxis of Exercise Professionals" Philosophies 4, no. 3: 54. https://doi.org/10.3390/philosophies4030054
APA StyleGray, J. (2019). The Hazards of a Biomedical Exercise Paradigm: Exploring the Praxis of Exercise Professionals. Philosophies, 4(3), 54. https://doi.org/10.3390/philosophies4030054