
Effects of Exercise on Heart Failure with Preserved Ejection Fraction: An Updated Review of Literature

 , , , , , and
, , , , , and
Abstract
:1. Introduction
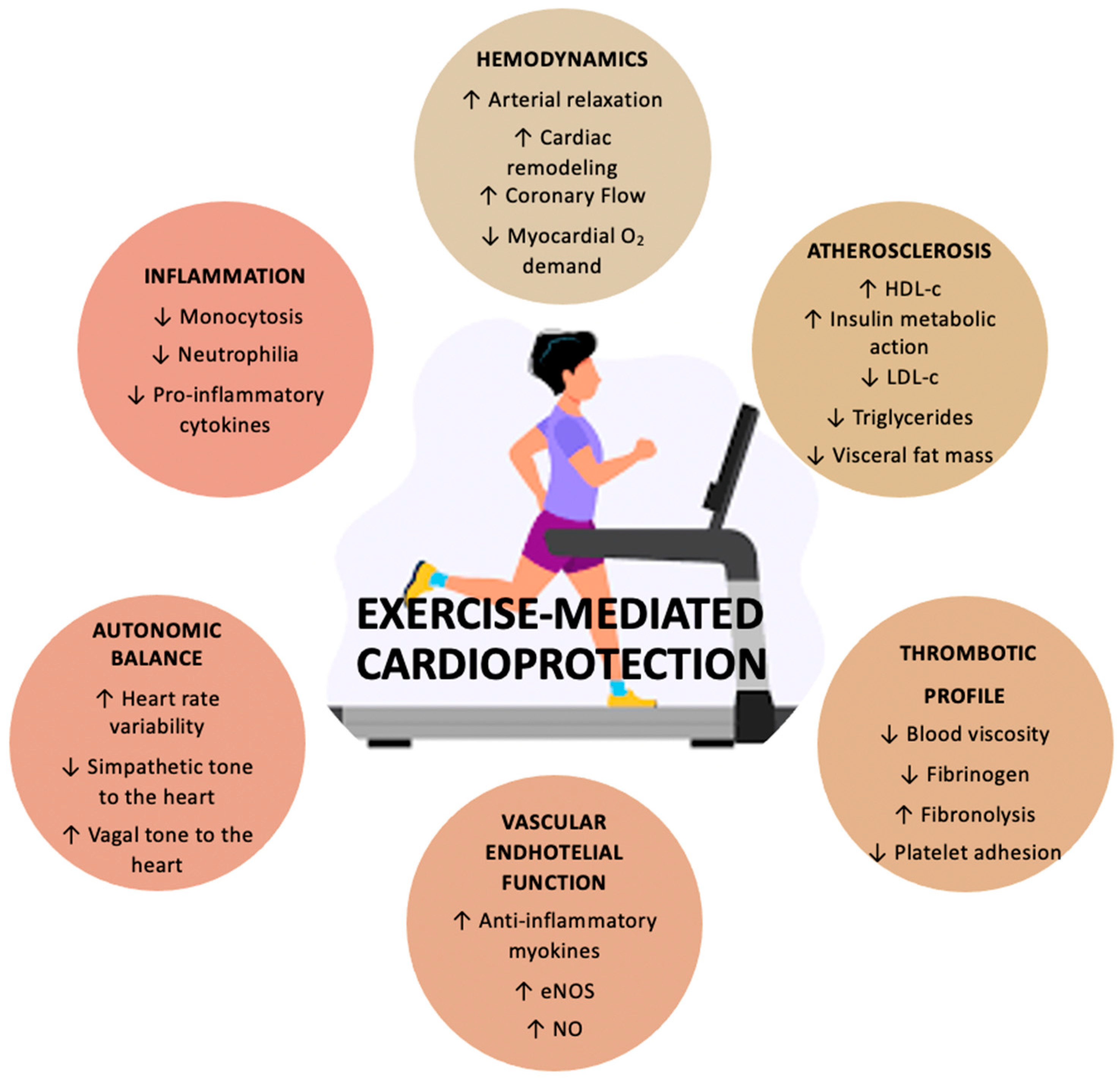
2. Cardiovascular Benefits of Exercise
2.1. Effects on Cardiovascular Risk Factors
2.2. Direct Cardiovascular Effects
2.3. Clinical Context
2.4. Effect of Exercise in Prevention of HFpEF
3. Evidence of Exercise in HFpEF
3.1. Cardiopulmonary Exercise Test
3.2. 6MWT
3.3. Echocardiography
3.4. Circulating Biomarkers
3.5. Quality of Life and Symptoms
3.6. Autonomic Dysfunction
3.7. Brachial Artery Flow-Mediated Dilation (FMD)
4. Clinical Impact and Future Perspectives
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [PubMed]
- Bozkurt, B.; Coats, A.J.S.; Tsutsui, H.; Abdelhamid, C.M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur. J. Heart Fail. 2021, 23, 352–380. [Google Scholar] [PubMed]
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Groenewegen, A.; Rutten, F.H.; Mosterd, A.; Hoes, A.W. Epidemiology of heart failure. Eur. J. Heart Fail. 2020, 22, 1342–1356. [Google Scholar] [CrossRef]
- Cho, D.H.; Yoo, B.S. Current Prevalence, Incidence, and Outcomes of Heart Failure with Preserved Ejection Fraction. Heart Fail. Clin. 2021, 17, 315–326. [Google Scholar] [CrossRef]
- Arcopinto, M.; Schiavo, A.; Salzano, A.; Bossone, E.; D’Assante, R.; Marsico, F.; Demelo-Rodriguez, P.; Baliga, R.R.; Cittadini, A.; Marra, A.M. Metabolic Syndrome in Heart Failure: Friend or Foe? Heart Fail. Clin. 2019, 15, 349–358. [Google Scholar] [CrossRef]
- Cittadini, A.; Salzano, A.; Iacoviello, M.; Triggiani, M.; Rengo, G.; Cacciatore, F.; Maiello, C.; Limongelli, G.; Masarone, D.; Perticone, F.; et al. Mutliple hormonal and metabolic deficiency syndrome predicts outcome in heart failure: The T.O.S.CA. Registry. Eur. J. Prev. Cardiol. 2021, 28, 1691–1700. [Google Scholar] [CrossRef]
- Streng, K.W.; Nauta, J.F.; Hillege, H.L.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; Filippatos, G.; Lang, C.C.; Metra, M.; Ng, L.L.; et al. Non-cardiac comorbidities in heart failure with reduced, mid-range and preserved ejection fraction. Int. J. Cardiol. 2018, 271, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Salzano, A.; Israr, M.Z.; Yazaki, Y.; Heaney, L.M.; Kanagala, P.; Singh, A.; Arnold, J.R.; Gulsin, G.S.; Squire, I.B.; McCann, G.P.; et al. Combined use of trimethylamine N-oxide with BNP for risk stratification in heart failure with preserved ejection fraction: Findings from the DIAMONDHFpEF study. Eur. J. Prev. Cardiol. 2019, 27, 2159–2162. [Google Scholar] [CrossRef] [Green Version]
- Salzano, A.; Marra, A.M.; Ferrara, F.; Arcopinto, M.; Bobbio, E.; Valente, P.; Polizzi, R.; De Vincentiis, C.; Matarazzo, M.; Saldamarco, L.; et al. Multiple hormone deficiency syndrome in heart failure with preserved ejection fraction. Int. J. Cardiol. 2016, 225, 1–3. [Google Scholar] [CrossRef]
- Salzano, A.; D’Assante, R.; Iacoviello, M.; Triggiani, V.; Rengo, G.; Cacciatore, F.; Maiello, C.; Limongelli, G.; Masarone, D.; Sciacqua, A.; et al. Progressive right ventricular dysfunction and exercise impairment in patients with heart failure and diabetes mellitus: Insights from the T.O.S.CA. Registry. Cardiovasc. Diabetol. 2022, 21, 108. [Google Scholar] [CrossRef] [PubMed]
- Pieske, B.; Tschope, C.; de Boer, R.A.; Fraser, A.G.; Anker, S.D.; Donal, E.; Edelmann, F.; Fu, M.; Guazzi, M.; Lam, C.S.P.; et al. How to diagnose heart failure with preserved ejection fraction: The HFA-PEFF diagnostic algorithm: A consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. Heart J. 2019, 40, 3297–3317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salzano, A.; De Luca, M.; Israr, M.Z.; Crisci, G.; Eltayeb, M.; Debiec, R.; Ranieri, B.; D’Assante, R.; Rega, S.; D’Agostino, A.; et al. Exercise Intolerance in Heart Failure with Preserved Ejection Fraction. Heart Fail. Clin. 2021, 17, 397–413. [Google Scholar] [CrossRef]
- Nocon, M.; Hiemann, T.; Mueller-Riemenschneider, F.; Thalau, F.; Roll, S.; Willich, S.N. Association of physical activity with all-cause and cardiovascular mortality: A systematic review and meta-analysis. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Tikkanen, E.; Gustafsson, S.; Ingelsson, E. Associations of Fitness, Physical Activity, Strength, and Genetic Risk With Cardiovascular Disease Longitudinal Analyses in the UK Biobank Study. Circulation 2018, 137, 2583–2591. [Google Scholar] [CrossRef]
- Vanhees, L.; De Sutter, J.; Geladas, N.; Doyle, F.; Prescott, E.; Cornelissen, V.; Kouidi, E.; Dugmore, D.; Vanuzzo, D.; Borjesson, M.; et al. Importance of characteristics and modalities of physical activity and exercise in defining the benefits to cardiovascular health within the general population: Recommendations from the EACPR (Part I). Eur. J. Prev. Cardiol. 2012, 19, 670–686. [Google Scholar] [CrossRef]
- Giannuzzi, P.; Mezzani, A.; Saner, H.; Björnstad, H.; Fioretti, P.; Mendes, M.; Cohen-Solal, A.; Dugmore, L.; Hambrecht, R.; Hellemans, I.; et al. Physical activity for primary and secondary prevention. Position paper of the Working Group on Cardiac Rehabilitation and Exercise Physiology of the European Society of Cardiology. Eur. J. Cardiovasc. Prev. Rehabil. 2003, 10, 319–327. [Google Scholar] [CrossRef]
- Fiuza-Luces, C.; Santos-Lozano, A.; Joyner, M.; Carrera-Bastos, P.; Picazo, O.; Zugaza, J.L.; Izquierdo, M.; Ruilope, L.M.; Lucia, A. Exercise benefits in cardiovascular disease: Beyond attenuation of traditional risk factors. Nat. Rev. Cardiol. 2018, 15, 731–743. [Google Scholar] [CrossRef]
- Shaw, K.; Gennat, H.; O’Rourke, P.; Del Mar, C. Exercise for overweight or obesity. Cochrane Database Syst. Rev. 2006, 2006, CD003817. [Google Scholar] [CrossRef] [Green Version]
- Zomer, E.; Gurusamy, K.; Leach, R.; Trimmer, C.; Lobstein, T.; Morris, S.; James, W.P.T.; Finer, N. Interventions that cause weight loss and the impact on cardiovascular risk factors: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Kraus, W.E.; Houmard, J.A.; Duscha, B.D.; Knetzger, K.J.; Wharton, M.B.; McCartney, J.S.; Bales, C.W.; Henes, S.; Samsa, G.P.; Otvos, J.D.; et al. Effects of the amount and intensity of exercise on plasma lipoproteins. N. Engl. J. Med. 2002, 347, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Henson, J.; Edwardson, C.L.; Davies, M.J.; Gill, J.M.R.; Heaney, L.M.; Khunti, K.; Ng, L.; Sattar, N.; Zaccardi, F.; Yates, T. Physical activity and lipidomics in a population at high risk of type 2 diabetes mellitus. J. Sports Sci. 2020, 38, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- de Barcelos, G.T.; Heberle, I.; Coneglian, J.C.; Vieira, B.A.; Delevatti, R.S.; Gerage, A.M. Effects of Aerobic Training Progression on Blood Pressure in Individuals With Hypertension: A Systematic Review With Meta-Analysis and Meta-Regression. Front. Sports Act. Living 2022, 4, 719063. [Google Scholar] [CrossRef] [PubMed]
- Carpes, L.; Costa, R.; Schaarschmidt, B.; Reichert, T.; Ferrari, R. High-intensity interval training reduces blood pressure in older adults: A systematic review and meta-analysis. Exp. Gerontol. 2022, 158, 111657. [Google Scholar] [CrossRef]
- Dassanayake, S.; Sole, G.; Wilkins, G.; Gray, E.; Skinner, M. Effectiveness of Physical Activity and Exercise on Ambulatory Blood Pressure in Adults with Resistant Hypertension: A Systematic Review and Meta-Analysis. High Blood Press. Cardiovasc. Prev. 2022, 29, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Umpierre, D.; Ribeiro, P.A.B.; Kramer, C.K.; Leitao, C.B.; Zucatti, A.T.N.; Azevedo, M.J.; Gross, J.L.; Ribeiro, J.P.; Schaan, B.D. Physical Activity Advice Only or Structured Exercise Training and Association With HbA(1c) Levels in Type 2 Diabetes A Systematic Review and Meta-analysis. JAMA J. Am. Med. Assoc. 2011, 305, 1790–1799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of hyperglycaemia in type 2 diabetes, 2015: A patient-centred approach. Update to a Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2015, 58, 429–442. [Google Scholar] [CrossRef]
- Heaps, C.L.; Robles, J.C.; Sarin, V.; Mattox, M.L.; Parker, J.L. Exercise Training-Induced Adaptations in Mediators of Sustained Endothelium-Dependent Coronary Artery Relaxation in a Porcine Model of Ischemic Heart Disease. Microcirculation 2014, 21, 388–400. [Google Scholar] [CrossRef]
- Ashor, A.W.; Lara, J.; Siervo, M.; Celis-Morales, C.; Oggioni, C.; Jakovljevic, D.G.; Mathers, J.C. Exercise Modalities and Endothelial Function: A Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials. Sports Med. 2015, 45, 279–296. [Google Scholar] [CrossRef]
- Haskell, W.L.; Sims, C.; Myll, J.; Bortz, W.M.; Stgoar, F.G.; Alderman, E.L. Coronary-Artery Size And Dilating Capacity In Ultradistance Runners. Circulation 1993, 87, 1076–1082. [Google Scholar] [CrossRef] [Green Version]
- Green, D.J.; Hopman, M.T.E.; Padilla, J.; Laughlin, M.H.; Thijssen, D.H.J. Vascular Adaptation To Exercise In Humans: Role Of Hemodynamic Stimuli. Physiol. Rev. 2017, 97, 495–528. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Mikami, Y.; Murayama, T.; Yokode, M.; Fujita, M.; Kita, T.; Kishimoto, C. Atherosclerotic plaques induced by marble-burying behavior are stabilized by exercise training in experimental atherosclerosis. Int. J. Cardiol. 2011, 151, 284–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, N.L.; Ribeiro, F.; Alves, A.J.; Teixeira, M.; Miranda, F.; Oliveira, J. Heart rate variability in myocardial infarction patients: Effects of exercise training. Rev. Port. De Cardiol. 2013, 32, 687–700. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Arena, R.; Swift, D.L.; Johannsen, N.M.; Sui, X.; Lee, D.-C.; Earnest, C.P.; Church, T.S.; O’Keefe, J.H.; Milani, R.V.; et al. Exercise and the cardiovascular system: Clinical science and cardiovascular outcomes. Circ Res. 2015, 117, 207–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosetti, M.; Abreu, A.; Corra, U.; Davos, C.H.; Hansen, D.; Frederix, I.; Iliou, M.C.; Pedretti, R.F.E.; Schmid, J.P.; Vigorito, C.; et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 460–495. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, G.F.; Landolfo, C.; Niebauer, J.; Ozemek, C.; Arena, R.; Lavie, C.J. Promoting Physical Activity and Exercise JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1622–1639. [Google Scholar] [CrossRef] [PubMed]
- Soares-Miranda, L.; Siscovick, D.S.; Psaty, B.M.; Longstreth, W.T.; Mozaffarian, D. Physical Activity and Risk of Coronary Heart Disease and Stroke in Older Adults The Cardiovascular Health Study. Circulation 2016, 133, 147–155. [Google Scholar] [CrossRef]
- Manson, J.E.; Greenland, P.; LaCroix, A.Z.; Stefanick, M.L.; Mouton, C.P.; Oberman, A.; Perri, M.G.; Sheps, D.S.; Pettinger, M.B.; Siscovick, D.S. Walking compared with vigorous exercise for the prevention of cardiovascular events in women. N. Engl. J. Med. 2002, 347, 716–725. [Google Scholar] [CrossRef] [Green Version]
- Wagner, A.; Simon, C.; Evans, A.; Ferrieres, J.; Montaye, M.; Ducimetiere, P.; Arveiler, D.; Grp, P.S. Physical activity and coronary event incidence in Northern Ireland and France—The Prospective Epidemiological Study of Myocardial Infarction (PRIME). Circulation 2002, 105, 2247–2252. [Google Scholar] [CrossRef] [Green Version]
- Florido, R.; Kwak, L.; Lazo, M.; Nambi, V.; Ahmed, H.M.; Hegde, S.M.; Gerstenblith, G.; Blumenthal, R.S.; Ballantyne, C.M.; Selvin, E.; et al. Six-Year Changes in Physical Activity and the Risk of Incident Heart Failure ARIC Study. Circulation 2018, 137, 2142–2151. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Back, M.; Borjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthelemy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Abreu, A.; Albus, C.; Ambrosetti, M.; Brotons, C.; Catapano, A.L.; Corra, U.; Cosyns, B.; Deaton, C.; Graham, I.; et al. Update on cardiovascular prevention in clinical practice: A position paper of the European Association of Preventive Cardiology of the European Society of Cardiology. Eur. J. Prev. Cardiol. 2020, 27, 181–205. [Google Scholar] [CrossRef] [Green Version]
- Oldridge, N.B.; Guyatt, G.H.; Fischer, M.E.; Rimm, A.A. Cardiac Rehabilitation After Myocardial-Infarction—Combined Experience Of Randomized Clinical-Trials. JAMA J. Am. Med. Assoc. 1988, 260, 945–950. [Google Scholar] [CrossRef]
- Lawler, P.R.; Filion, K.B.; Eisenberg, M.J. Efficacy of exercise-based cardiac rehabilitation post-myocardial infarction: A systematic review and meta-analysis of randomized controlled trials. Am. Heart J. 2011, 162, 571–584. [Google Scholar] [CrossRef]
- Kondamudi, N.; Haykowsky, M.; Forman, D.E.; Berry, J.D.; Pandey, A. Exercise Training for Prevention and Treatment of Heart Failure. Prog. Cardiovasc. Dis. 2017, 60, 115–120. [Google Scholar] [CrossRef]
- Pandey, A.; LaMonte, M.; Klein, L.; Ayers, C.; Psaty, B.M.; Eaton, C.B.; Allen, N.B.; de Lemos, J.A.; Carnethon, M.; Greenland, P.; et al. Relationship Between Physical Activity, Body Mass Index, and Risk of Heart Failure. J. Am. Coll. Cardiol. 2017, 69, 1129–1142. [Google Scholar] [CrossRef]
- Berry, J.D.; Pandey, A.; Gao, A.; Leonard, D.; Farzaneh-Far, R.; Ayers, C.; DeFina, L.; Willis, B. Physical fitness and risk for heart failure and coronary artery disease. Circ. Heart Fail. 2013, 6, 627–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, A.; Garg, S.; Khunger, M.; Darden, D.; Ayers, C.; Kumbhani, D.J.; Mayo, H.G.; de Lemos, J.A.; Berry, J.D. Dose-Response Relationship Between Physical Activity and Risk of Heart Failure: A Meta-Analysis. Circulation 2015, 132, 1786–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinker, S.K.; Pandey, A.; Ayers, C.R.; Barlow, C.E.; DeFina, L.F.; Willis, B.L.; Radford, N.B.; Farzaneh-Far, R.; de Lemos, J.A.; Drazner, M.H.; et al. Association of cardiorespiratory fitness with left ventricular remodeling and diastolic function: The Cooper Center Longitudinal Study. JACC Heart Fail. 2014, 2, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Shah, S.J.J.; Butler, J.; Kellogg, D.L.; Lewis, G.D.; Forman, D.E.; Mentz, R.J.; Borlaug, B.A.; Simon, M.A.; Chirinos, J.A.; et al. Exercise Intolerance in Older Adults With Heart Failure With Preserved Ejection Fraction JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 78, 1166–1187. [Google Scholar] [CrossRef] [PubMed]
- Del Buono, M.G.; Arena, R.; Borlaug, B.A.; Carbone, S.; Canada, J.M.; Kirkman, D.L.; Garten, R.; Rodriguez-Miguelez, P.; Guazzi, M.; Lavie, C.J.; et al. Exercise Intolerance in Patients With Heart Failure. J. Am. Coll. Cardiol. 2019, 73, 2209–2225. [Google Scholar] [CrossRef]
- Borlaug, B.A.; Melenovsky, V.; Russell, S.D.; Kessler, K.; Pacak, K.; Becker, L.C.; Kass, D.A. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation 2006, 114, 2138–2147. [Google Scholar] [CrossRef] [Green Version]
- Borlaug, B.A.; Olson, T.P.; Lam, C.S.P.; Flood, K.S.; Lerman, A.; Johnson, B.D.; Redfield, M.M. Global Cardiovascular Reserve Dysfunction in Heart Failure With Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2010, 56, 845–854. [Google Scholar] [CrossRef] [Green Version]
- Haykowsky, M.J.; Kouba, E.J.; Brubaker, P.H.; Nicklas, B.J.; Eggebeen, J.; Kitzman, D.W. Skeletal Muscle Composition and Its Relation to Exercise Intolerance in Older Patients With Heart Failure and Preserved Ejection Fraction. Am. J. Cardiol. 2014, 113, 1211–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haykowsky, M.J.; Brubaker, P.H.; John, J.M.; Stewart, K.P.; Morgan, T.M.; Kitzman, D.W. Determinants of Exercise Intolerance in Elderly Heart Failure Patients With Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2011, 58, 265–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhakal, B.P.; Malhotra, R.; Murphy, R.M.; Pappagianopoulos, P.P.; Baggish, A.L.; Weiner, R.B.; Houstis, N.E.; Eisman, A.S.; Hough, S.S.; Lewis, G.D. Mechanisms of Exercise Intolerance in Heart Failure With Preserved Ejection Fraction The Role of Abnormal Peripheral Oxygen Extraction. Circ. Heart Fail. 2015, 8, 286–294. [Google Scholar] [CrossRef] [Green Version]
- Reddy, Y.N.V.; Andersen, M.J.; Obokata, M.; Koepp, K.E.; Kane, G.C.; Melenovsky, V.; Olson, T.P.; Borlaug, B.A. Arterial Stiffening With Exercise in Patients With Heart Failure and Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2017, 70, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Adams, V.; Conraads, V.; Halle, M.; Mezzani, A.; Vanhees, L.; Arena, R.; Fletcher, G.F.; Forman, D.E.; Kitzman, D.W.; et al. Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations. Circulation 2012, 126, 2261–2274. [Google Scholar] [CrossRef] [PubMed]
- Pane, C.; Salzano, A.; Trinchillo, A.; Del Prete, C.; Casali, C.; Marcotulli, C.; Defazio, G.; Guardasole, V.; Vastarella, R.; Giallauria, F.; et al. Safety and feasibility of upper limb cardiopulmonary exercise test in Friedreich ataxia. Eur. J. Prev. Cardiol. 2020, 29, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Saccà, F.; Puorro, G.; Marsili, A.; Antenora, A.; Pane, C.; Casali, C.; Marcotulli, C.; Defazio, G.; Liuzzi, D.; Tatillo, C.; et al. Long-term effect of epoetin alfa on clinical and biochemical markers in friedreich ataxia. Mov. Disord. 2016, 31, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Parashar, A.; Kumbhani, D.J.; Agarwal, S.; Garg, J.; Kitzman, D.; Levine, B.D.; Drazner, M.; Berry, J.D. Exercise Training in Patients With Heart Failure and Preserved Ejection Fraction Meta-Analysis of Randomized Control Trials. Circ. Heart Fail. 2015, 8, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Kitzman, D.W.; Brubaker, P.H.; Herrington, D.M.; Morgan, T.M.; Stewart, K.P.; Hundley, W.G.; Abdelhamed, A.; Haykowsky, M.J. Effect of Endurance Exercise Training on Endothelial Function and Arterial Stiffness in Older Patients With Heart Failure and Preserved Ejection Fraction A Randomized, Controlled, Single-Blind Trial. J. Am. Coll. Cardiol. 2013, 62, 584–592. [Google Scholar] [CrossRef]
- Fujimoto, N.; Prasad, A.; Hastings, J.L.; Bhella, P.S.; Shibata, S.; Palmer, D.; Levine, B.D. Cardiovascular effects of 1 year of progressive endurance exercise training in patients with heart failure with preserved ejection fraction. Am. Heart J. 2012, 164, 869–877. [Google Scholar] [CrossRef] [Green Version]
- Haykowsky, M.J.; Brubaker, P.H.; Stewart, K.P.; Morgan, T.M.; Eggebeen, J.; Kitzman, D.W. Effect of endurance training on the determinants of peak exercise oxygen consumption in elderly patients with stable compensated heart failure and preserved ejection fraction. J. Am. Coll. Cardiol. 2012, 60, 120–128. [Google Scholar] [CrossRef] [Green Version]
- Maldonado-Martin, S.; Brubaker, P.H.; Eggebeen, J.; Stewart, K.P.; Kitzman, D.W. Association Between 6-Minute Walk Test Distance and Objective Variables of Functional Capacity After Exercise Training in Elderly Heart Failure Patients With Preserved Ejection Fraction: A Randomized Exercise Trial. Arch. Phys. Med. Rehabil. 2017, 98, 600–603. [Google Scholar] [CrossRef]
- Edelmann, F.; Gelbrich, G.; Dungen, H.D.; Frohling, S.; Wachter, R.; Stahrenberg, R.; Binder, L.; Topper, A.; Lashki, D.J.; Schwarz, S.; et al. Exercise Training Improves Exercise Capacity and Diastolic Function in Patients With Heart Failure With Preserved Ejection Fraction Results of the Ex-DHF (Exercise training in Diastolic Heart Failure) Pilot Study. J. Am. Coll. Cardiol. 2011, 58, 1780–1791. [Google Scholar] [CrossRef] [Green Version]
- Brubaker, P.H.; Avis, T.; Rejeski, W.J.; Mihalko, S.E.; Tucker, W.J.; Kitzman, D.W. Exercise Training Effects on the Relationship of Physical Function and Health-Related Quality of Life Among Older Heart Failure Patients With Preserved Ejection Fraction. J. Cardiopulm. Rehabil. Prev. 2020, 40, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.C.; Yang, N.I.; Wang, C.H.; Cherng, W.J.; Chou, S.L.; Pan, T.L.; Wang, J.S. Aerobic Interval Training Elicits Different Hemodynamic Adaptations Between Heart Failure Patients with Preserved and Reduced Ejection Fraction. Am. J. Phys. Med. Rehabil. 2016, 95, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Kitzman, D.W.; Brubaker, P.; Morgan, T.; Haykowsky, M.; Hundley, G.; Kraus, W.E.; Eggebeen, J.; Nicklas, B.J. Effect of Caloric Restriction or Aerobic Exercise Training on Peak Oxygen Consumption and Quality of Life in Obese Older Patients With Heart Failure With Preserved Ejection Fraction A Randomized Clinical Trial. JAMA J. Am. Med. Assoc. 2016, 315, 36–46. [Google Scholar] [CrossRef]
- Smart, N.A.; Haluska, B.; Jeffriess, L.; Leung, D. Exercise training in heart failure with preserved systolic function: A randomized controlled trial of the effects on cardiac function and functional capacity. Congest. Heart Fail. 2012, 18, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Angadi, S.S.; Mookadam, F.; Lee, C.D.; Tucker, W.J.; Haykowsky, M.J.; Gaesser, G.A. High-intensity interval training vs. moderate-intensity continuous exercise training in heart failure with preserved ejection fraction: A pilot study. J. Appl. Physiol. 2015, 119, 753–758. [Google Scholar] [CrossRef] [PubMed]
- da Silveira, A.D.; de Lima, J.B.; Piardi, D.D.; Macedo, D.D.; Zanini, M.; Nery, R.; Laukkanen, J.A.; Stein, R. High-intensity interval training is effective and superior to moderate continuous training in patients with heart failure with preserved ejection fraction: A randomized clinical trial. Eur. J. Prev. Cardiol. 2020, 27, 1733–1743. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.; Winzer, E.B.; Duvinage, A.; Gevaert, A.B.; Edelmann, F.; Haller, B.; Pieske-Kraigher, E.; Beckers, P.; Bobenko, A.; Hommel, J.; et al. Effect of High-Intensity Interval Training, Moderate Continuous Training, or Guideline-Based Physical Activity Advice on Peak Oxygen Consumption in Patients With Heart Failure With Preserved Ejection Fraction A Randomized Clinical Trial. JAMA J. Am. Med. Assoc. 2021, 325, 542–551. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Brubaker, P.H.; Morgan, T.M.; Stewart, K.P.; Little, W.C. Exercise Training in Older Patients With Heart Failure and Preserved Ejection Fraction A Randomized, Controlled, Single-Blind Trial. Circ. Heart Fail. 2010, 3, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Alves, A.J.; Ribeiro, F.; Goldhammer, E.; Rivlin, Y.; Rosenschein, U.; Viana, J.L.; Duarte, J.A.; Sagiv, M.; Oliveira, J. Exercise Training Improves Diastolic Function in Heart Failure Patients. Med. Sci. Sports Exerc. 2012, 44, 776–785. [Google Scholar] [CrossRef]
- Salzano, A.; D’Assante, R.; Israr, M.Z.; Eltayeb, M.; D’Agostino, A.; Bernieh, D.; De Luca, M.; Rega, S.; Ranieri, B.; Mauro, C.; et al. Biomarkers in Heart Failure: Clinical Insights. Heart Fail. Clin. 2021, 17, 223–243. [Google Scholar] [CrossRef]
- Israr, M.Z.; Salzano, A.; Yazaki, Y.; Voors, A.A.; Ouwerkerk, W.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; Metra, M.; Samani, N.J.; et al. Implications of serial measurements of natriuretic peptides in heart failure: Insights from BIOSTAT-CHF. Eur. J. Heart Fail. 2020, 22, 1486–1490. [Google Scholar] [CrossRef] [PubMed]
- Nolte, K.; Herrmann-Lingen, C.; Wachter, R.; Gelbrich, G.; Dungen, H.D.; Duvinage, A.; Hoischen, N.; von Oehsen, K.; Schwarz, S.; Hasenfuss, G.; et al. Effects of exercise training on different quality of life dimensions in heart failure with preserved ejection fraction: The Ex-DHF-P trial. Eur. J. Prev. Cardiol. 2015, 22, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.C.; Smith, K.; Wingham, J.; Eyre, V.; Greaves, C.J.; Warren, F.C.; Green, C.; Jolly, K.; Davis, R.C.; Doherty, P.J.; et al. A randomised controlled trial of a facilitated home-based rehabilitation intervention in patients with heart failure with preserved ejection fraction and their caregivers: The REACH-HFpEF Pilot Study. BMJ Open 2018, 8, e019649. [Google Scholar] [CrossRef]
- Murad, K.; Brubaker, P.H.; Fitzgerald, D.M.; Morgan, T.M.; Goff, D.C.; Soliman, E.Z.; Eggebeen, J.D.; Kitzman, D.W. Exercise training improves heart rate variability in older patients with heart failure: A randomized, controlled, single-blinded trial. Congest. Heart Fail. 2012, 18, 192–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, K.; Shimada, K.; Nishitani-Yokoyama, M.; Kunimoto, M.; Matsubara, T.; Matsumori, R.; Abulimiti, A.; Aikawa, T.; Ouchi, S.; Shimizu, M.; et al. Arterial Stiffness Index and Exercise Tolerance in Patients Undergoing Cardiac Rehabilitation. Int. Heart J. 2021, 62, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Bohm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Tucker, W.J.; Lijauco, C.C.; Hearon, C.M.; Angadi, S.S.; Nelson, M.D.; Sarma, S.; Nanayakkara, S.; La Gerche, A.; Haykowsky, M.J. Mechanisms of the Improvement in Peak VO2 With Exercise Training in Heart Failure With Reduced or Preserved Ejection Fraction. Heart Lung Circ. 2018, 27, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maddox, T.M.; Januzzi, J.L.; Allen, L.A.; Breathett, K.; Butler, J.; Davis, L.L.; Fonarow, G.C.; Ibrahim, N.E.; Lindenfeld, J.; Masoudi, F.A.; et al. 2021 Update to the 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2021, 77, 772–810. [Google Scholar] [CrossRef]


| Peak VO2 mL/kg/min | ET | Ctr | |||
|---|---|---|---|---|---|
| Baseline | Final | baseline | Final | p§ | |
| Kitzman 2010 [78] | 13.8 ± 2.5 | 16.1 ± 2.6 * | 12.8 ± 2.6 | 12.5 ± 3.4 | <0.001 |
| Edelmann 2011 [70] | 16.1 ± 4.9 | 18.7 ± 5.4 * | 16.7 ± 4.7 | 16.0 ± 6.0 | <0.001 |
| Smart 2012 [74] | 12.2 ± 3.6 | 15 ± 4.9 * | 14.1 ± 4.1 | 14.8 ± 4.6 | 0.06 |
| Kitzman 2013 [66] | 14.2 ± 2.8 | 15.8 ± 3.3 | 14.0 ± 3.2 | 13.8 ± 3.1 | 0.0001 |
| Maldonado-Martin 2017 [69] | 13.5 ± 2.3 | 16.0 ± 2.6 * | 12.7 ± 3.2 | 12.6 ± 3.4 | 0.01 |
| Brubaker 2020 [71] | 13.7 ± 2.8 | 15.2±6.3 * | 13.3 ± 3.0 | 13.0–14.0 | 0.001 |
| HIIT | MCT | ||||
| Baseline | final | baseline | Final | p§ | |
| Angadi 2015 [75] | 19.2 ± 5.2 | 21.0 ± 5.2 * | 16.9 ± 3.0 | 16.8 ± 4.0 | d: 0.94 vs. −1.63 |
| Donelli da Silveira 2020 [76] | 16.1 ± 3.3 | 19.6 ± 3.5 * | 17.6 ± 3.5 | 19.5 ± 3.7 * | <0.001 |
| Mueller 2021 [77] | 18.9 ± 5.4 | 20.2 ± 6.0 | 18.2 ± 5.1 | 19.8 ± 2.5 | 0.002 |
| VE/VCO2 Slope | ET | Ctr | |||
|---|---|---|---|---|---|
| Baseline | final | baseline | Final | p§ | |
| Kitzman 2010 [78] | 34 ± 6 | 35 ± 8 | 33 ± 5 | 34 ± 5 | n.s. |
| Smart 2012 [74] | 33.9 ± 3.3 | 29.6 ± 5.3 | 33.7 ± 3.0 | 33.8 ± 3.2 | n.s. |
| Kitzman 2013 [66] | 31.5 ± 4.4 | 32.2 ± 4.5 | 30.6 ± 3.6 | 30.2 ± 3.3 | n.s. |
| HIIT | MCT | ||||
| Baseline | final | baseline | final | p§ | |
| Angadi 2015 [75] | 31.2 ± 11.5 | 31.6 ± 10.3 | 26.5 ± 2.4 | 26.7 ± 3.1 | n.s. |
| Donelli da Silveira2020 [76] | 39.4 ± 6.1 | 35.7 ± 4.7 | 36.8 ± 5.4 | 34.6 ± 5.1 | <0.001 |
| Mueller 2021 [77] | 34.5 ± 7.9 | 35.0 ± 9.8 | 34.2 ± 7.2 | 33.7 ± 6.8 | n.s. |
| Ventilatory Anaerobic Threshold (VAT) | ET | Ctr | |||
|---|---|---|---|---|---|
| Baseline | final | baseline | final | p§ | |
| Kitzman 2010 [78] (mL/min) | 746 ± 149 | 822 ± 180 * | 660 ± 174 | 618 ± 126 | <0.001 |
| Eldemann 2011 [70] (mL/min/kg) | 10.2 ± 3.0 | 12.7 ± 3.6 * | 10.3 ± 2.5 | 10.0 ± 3.2 | <0.001 |
| Smart 2012 [74] (mL/min/kg) | 7.8 ± 1.8 | 9.8 ± 2.6 | 9.1 ± 3.8 | 9.2 ± 5.3 | n.s. |
| Kitzman 2013 [66] (mL/min) | 699 ± 178 | 796 ± 163 * | 734 ± 189 | 702 ± 186 | 0.01 |
| Maldonado Martin 2017 [69] (mL/min/kg) | 9.3 ± 1.5 | 10.4 ± 1.4 | 8.3 ± 1.3 | 8.3 ± 2.2 | n.s. |
| Brubaker 2020 [71] (mL/min) | 721 ± 161 | 768.8 ± 846.2 * | 703 ± 184 | 636.5 ± 711.5 | 0.001 |
| HIIT | MCT | ||||
| Baseline | final | baseline | final | p | |
| Angadi 2015 [75] ml/min/kg | 12.2 ± 4.0 | 13.1 ± 3.5 | 11.1 ± 2.1 | 11.7 ± 2.4 | n.s. |
| 6MWT Distance (m) | ET | Ctr | |||
|---|---|---|---|---|---|
| baseline | final | baseline | final | p§ | |
| Kitzman 2010 [78] | 1494 ± 224 | 1659 ± 173 * | 1412 ± 382 | 1460 ± 411 | 0.002 |
| Edelmann 2011 [70] | 545 ± 86 | 569 ± 88 * | 551 ± 86 | 568 ± 80 | 0.63 |
| Kitzman 2013 [66] | 447 ± 107 | 486 ± 89 | 438 ± 79 | 448 ± 70 | 0.009 |
| Maldonado-Martin 2017 [69] | 455 ± 68 | 506 ± 53 * | 402 ± 142 | 430 ± 125 * | 0.028 |
| Brubaker 2020 [71] | 445 ± 88 | 474.5–504.1 * | 425 ± 117 | 434.4 ± 462.9 | <0.001 |
| ECHOCARDIOGRAPHY | ET | Ctr | |||
|---|---|---|---|---|---|
| Baseline | final | baseline | final | p§ | |
| Kitzman 2010 [78] | |||||
| EF (%) | 61 ± 5 | 57 ± 8 | 60 ± 10 | 55 ± 8 | ns |
| E/A | 0.90 ± 0.24 | 1.02 ± 0.28 | 1.02 ± 0.38 | 1.12 ± 0.36 | ns |
| DT | 220 ± 55 | 230 ± 40 | 227 ± 52 | 221 ± 52 | ns |
| Edelmann 2011 [70] | |||||
| EF (%) | 67 ± 7 | 66 ± 6 | 66 ± 7 | 67 ± 8 | ns |
| E/e’ | 12.8 ± 3.2 | 10.5 ± 2.5 * | 13.5 ± 4.6 | 14.1 ± 3.9 | 0.01 |
| LAVi mL/m2 | 27.9 ± 7.6 | 24.3 ± 6.5 * | 28.2 ± 8.8 | 28.6 ± 9.2 | 0.01 |
| Smart 2012 [74] | |||||
| EF (%) | 58 ± 13.2 | 61.3 ± 9.5 | 56.7 ±7.7 | 58.7 ±6.4 | ns |
| E/A | 0.87 ± 0.13 | 0.82 ± 0.17 | 0.94 ± 0.39 | 0.82 ± 0.22 | ns |
| DT | 276 ± 50 | 281 ± 54 | 245 ± 44 | 248 ± 36 | ns |
| E/e’ | 20.7 ± 12.8 | 25.1 ± 24 | 15.9 ± 6.8 | 15.9 ± 5.5 | ns |
| Alves 2012 [79] | |||||
| EF (%) | 56.4 | 57.7 * | 55.9 | 55.4 | 0.01 |
| E/A | 0.93 | 1.05 * | 1.01 | 1.04 | 0.01 |
| DT (sec) | 236.7 | 222.7 * | 216.9 | 214.8 | 0.01 |
| EDd (mm) | 51.5 | 51 | 51.7 | 51.9 | ns |
| ESd (mm) | 30.4 | 29.6 | 30.9 | 31.3 | ns |
| Fu 2016 [72] | |||||
| EF (%) | 57.6 ± 1.9 | 57.8 ± 1.7 | 56.5 ± 2.2 | 54.4 ± 3.3 | ns |
| E/A | 1.1 ± 0.2 | 0.9 ± 0.1 | 1.0 ± 0.3 | 0.8 ± 0.2 | ns |
| E/e’ | 21.0 ± 2.2 | 16.1 ± 1.8* | 19.2 ±1.5 | 17.8 ± 1.9 | ns |
| HIIT | MCT | ||||
| Angadi 2015 [75] | |||||
| EF (%) | 65 ± 5 | 63 ± 6 | 66 ± 4 | 61 ± 5 | ns |
| E/A | 1.3 ± 0.5 | 1.2 ± 0.5 | 1.2 ± 0.6 | 1.6 ± 1.1 | ns |
| DT | 194 ± 55 | 225 ± 40 * | 199 ± 71 | 220 ± 43 | ns |
| E/e’ | 14.6 ± 5.6 | 12.7 ± 4.7 | 17.7 ± 6.3 | 16.7 ± 5.2 | ns |
| LAVi (mL/m2) | 35.8 ± 3.0 | 32.4 ± 7.2 | 40.5 ± 9.3 | 46.3 ± 18.1 | ns |
| Donelli da Silveira 2020 [79] | |||||
| EF (%) | 65 ± 5 | 66 ± 4 | 65 ± 5 | 65 ± 5 | ns |
| E/A | 0.99 ± 0.2 | 0.91 0.2 | 1.05 ± 0.3 | 1.08 ± 0.3 | ns |
| DT | 233 ± 33 | 222 ± 27 | 214 ± 33 | 209 ± 37 | ns |
| E/e’ | 14.2 ± 4 | 11.6 ± 3 * | 13.3 ± 3 | 11.1 ± 2 * | ns |
| Mueller 2021 [77] | |||||
| E/e’ | 15.8 ± 3.7 | 14.2 ± 3.9 | 15.9 ± 4.1 | 15.6 ± 4.4 | ns |
| LAVi mL/m2 | 35.4 ± 9.0 | 37.4 ± 10.9 | 37.9 ± 13.0 | 36.6 ± 9.2 | ns |
| Brachial ArteryFlow-Mediated Dilation (%) | ET | Ctr | |||
|---|---|---|---|---|---|
| baseline | final | baseline | Final | p§ | |
| Kitzman 2013 [66] | 4.0 ± 2.0 | 3.8 ± 3.0 | 4.7 ± 3.5 | 4.3 ± 3.5 | ns |
| HIIT | MCT | ||||
| baseline | final | baseline | Final | ||
| Angadi 2015 [75] | 6.9 ± 3.7 | 7.0 ± 4.2 | 8.1 ± 4.1 | 3.4 ± 3.6 | ns |
| First Author; Year of Publication (Ref.) | Study Design; Duration (wk) | Type of Exercise | Patient; Age; Women (%) | Principal Outcomes Investigated and Main Findings |
|---|---|---|---|---|
| Kitzman2010 [78] | Randomized, prospective, attention-controlled, single-blind study 16 wk | 1 h ET (warm-up, stimulus, and cool-down phases), 3 times/wk | ET UC |
|
| N = 26 N = 27 | ||||
| 70 ± 6 y 69 ± 5 y | ||||
| 83% 91% | ||||
| Edelmann2011 [70] | Prospective, randomized 2:1 controlled trial 12 wk | Endurance/resistance training | ET UC |
|
| N = 44 N = 20 | ||||
| 64± 8 y 65 ± 6 y | ||||
| 55% 60% | ||||
| Smart2012 [74] | Randomized, controlled trial 16 wk | Cycle ergometer exercise training at 60 rpm | ET UC |
|
| N = 12 N = 13 | ||||
| 67 ± 5.8 y 61.9 ± 6.9 y | ||||
| 42% 53% | ||||
| Murad2012 [84] | Randomized, controlled, single-blinded design 16 wk | 1 h ET (warm-up, stimulus, and cool-down phases), 3 times/wk | ET UC |
|
| N = 35 N = 31 | ||||
| 70.1 ± 5.6 y 68.0 ± 4.8 y | ||||
| 63% 64.5% | ||||
| Alves2012 [79] | Randomized controlled trial 24 wk | Interval training | ET UC |
|
| N = 20 N = 11 | ||||
| Overall | ||||
| 63 ± 11 y | ||||
| 29% | ||||
| Haykowsky2012 [68] | Randomized, single-blind trial 16 wk | Endurance exercise training | ET UC |
|
| N = 22 N = 18 | ||||
| 70 ± 6 y 68 ± 5 y | ||||
| 82 % 94% | ||||
| Fujimoto2012 [67] | Randomized controlled trial 54 wk | Endurance exercise training | ET UC |
|
| N = 7 N = 13 | ||||
| 74.9 ± 6 y 70.2 ± 4 y | ||||
| 57% 38% | ||||
| Kitzman2013 [66] | Randomized, controlled, single-blind trial 16 wk | Walking, arm, and leg ergometry | ET UC |
|
| N = 32 N = 31 | ||||
| 70 ± 7 y 70 ± 7 y | ||||
| 72% 80% | ||||
| Angadi2015 [75] | Randomized comparison trial/pilot study 4 wk | HIIT vs. MI-ACT | HIIT MCT |
|
| N = 9 N = 6 | ||||
| 69.0 ± 6.1 y 71.5 ± 11.7 y | ||||
| 11% 33% | ||||
| Nolte2015 [83] | Prospective, randomized, controlled trial 12 wk | Endurance/resistance training | ET UC |
|
| N = 44 N = 20 | ||||
| overall | ||||
| 65 ± 7 y | ||||
| 56% | ||||
| Kitzman2016 [73] | Randomized, attention- controlled, 2 × 2 factorial trail 20 wk | Walking exercise 3 times/wk | ET Diet group |
|
| N = 26 N = 24 | ||||
| ET + Diet group UC | ||||
| N = 25 N = 25 | ||||
| Overall | ||||
| 67 ± 5 y | ||||
| 81% | ||||
| Fu2016 [72] | Randomized, controlled trial 12 wk | Aerobic interval training | ET UC |
|
| N = 30 N = 30 | ||||
| 60.5 ± 2.7 y 63.1 ± 2.6 y | ||||
| 33% 40% | ||||
| Maldonado-Martin2017 [69] | Prospective, randomized, single-blinded trial 16 wk | Cycling and walking at 50% to 70% of VO2 peak intensity | ET UC |
|
| N = 23 N = 24 | ||||
| >65 y | ||||
| 87% | ||||
| Lang2018 [83] | Randomized controlled trial 12 wk | Home-based comprehensive self-management rehabilitation program | ET UC |
|
| N = 25 N = 25 | ||||
| 71.8 ± 9.9 y 76 ± 6.6 y | ||||
| 64% 44% | ||||
| Donelli da Silveira2020 [76] | Single-blinded, parallel randomized clinical trial 3 d per wk 12 wk | HIIT vs. MCT | HIIT MCT |
|
| N = 10 N = 9 | ||||
| 60 ± 10 y 60 ± 9 y | ||||
| 70% 56% | ||||
| Brubaker2020 [71] | Randomized controlled trial 16 wk | ≤60 min of moderate-intensity endurance exercise training 3 time/wk | ET UC |
|
| N = 58 N = 58 | ||||
| 70.3 ± 6.7 69.2 ± 6.2 | ||||
| 76% 86% | ||||
| Mueller2021 [77] | Randomized controlled trial 3 mo supervised followed by 9 mo of telemedical monitored home-based training | HIIT vs. MCT vs. UC | HIIT MCT UC |
|
| N = 58 N = 58 N = 60 | ||||
| 70 ± 7 y 70 ± 8 y 69 ±10 y | ||||
| 71% 60% 68% |


{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crisci, G.; De Luca, M.; D’Assante, R.; Ranieri, B.; D’Agostino, A.; Valente, V.; Giardino, F.; Capone, V.; Chianese, S.; Rega, S.; et al. Effects of Exercise on Heart Failure with Preserved Ejection Fraction: An Updated Review of Literature. J. Cardiovasc. Dev. Dis. 2022, 9, 241. https://doi.org/10.3390/jcdd9080241
Crisci G, De Luca M, D’Assante R, Ranieri B, D’Agostino A, Valente V, Giardino F, Capone V, Chianese S, Rega S, et al. Effects of Exercise on Heart Failure with Preserved Ejection Fraction: An Updated Review of Literature. Journal of Cardiovascular Development and Disease. 2022; 9(8):241. https://doi.org/10.3390/jcdd9080241
Chicago/Turabian StyleCrisci, Giulia, Mariarosaria De Luca, Roberta D’Assante, Brigida Ranieri, Anna D’Agostino, Valeria Valente, Federica Giardino, Valentina Capone, Salvatore Chianese, Salvatore Rega, and et al. 2022. "Effects of Exercise on Heart Failure with Preserved Ejection Fraction: An Updated Review of Literature" Journal of Cardiovascular Development and Disease 9, no. 8: 241. https://doi.org/10.3390/jcdd9080241