
Blood Pressure Increase following COVID-19 Vaccination: A Systematic Overview and Meta-Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
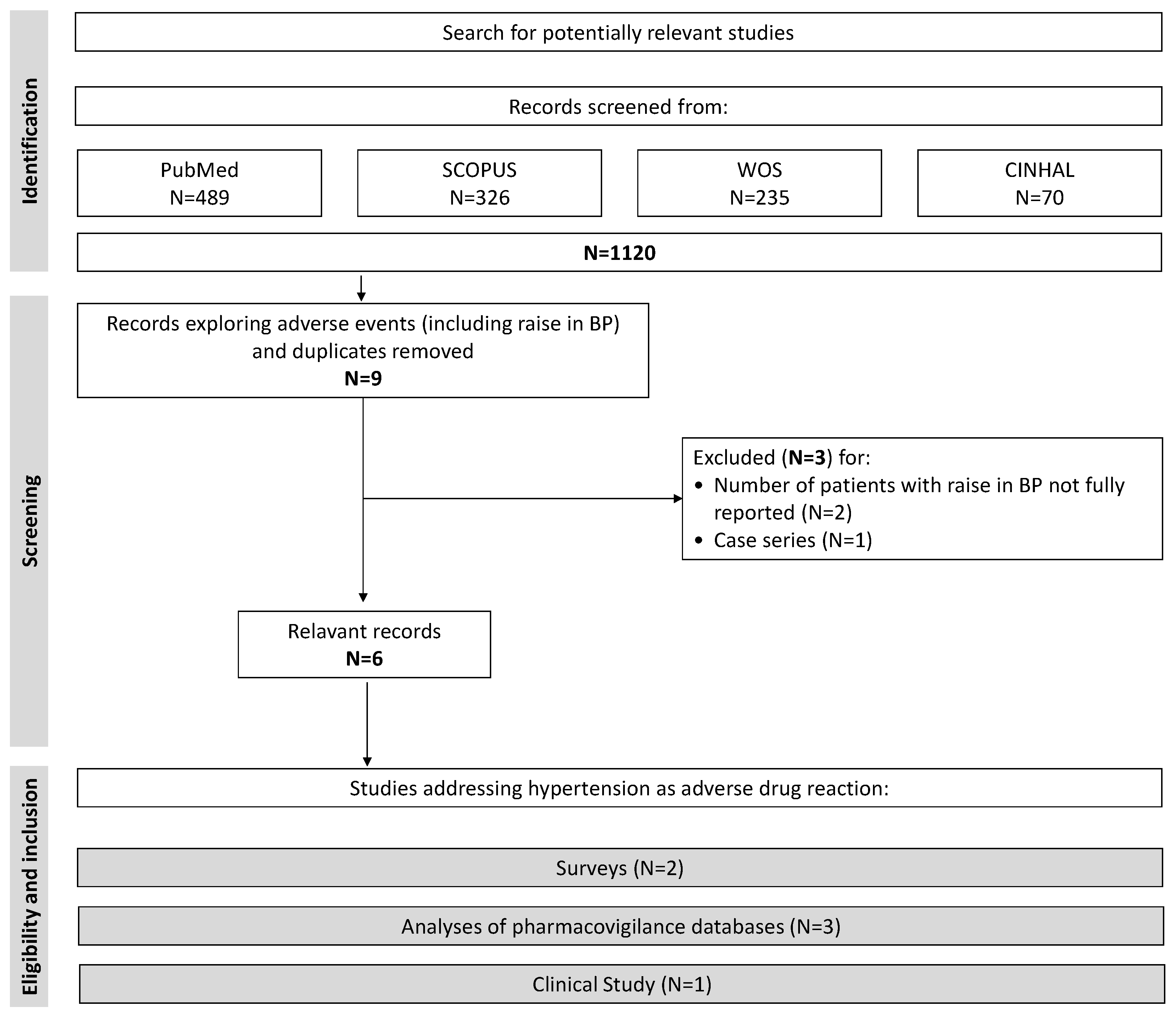
2.1. Study Selection and Outcome Measures
2.2. Data Sources and Searches
2.3. Data Synthesis
2.4. Data Analysis
3. Results
3.1. Excluded Studies
3.2. Included Studies
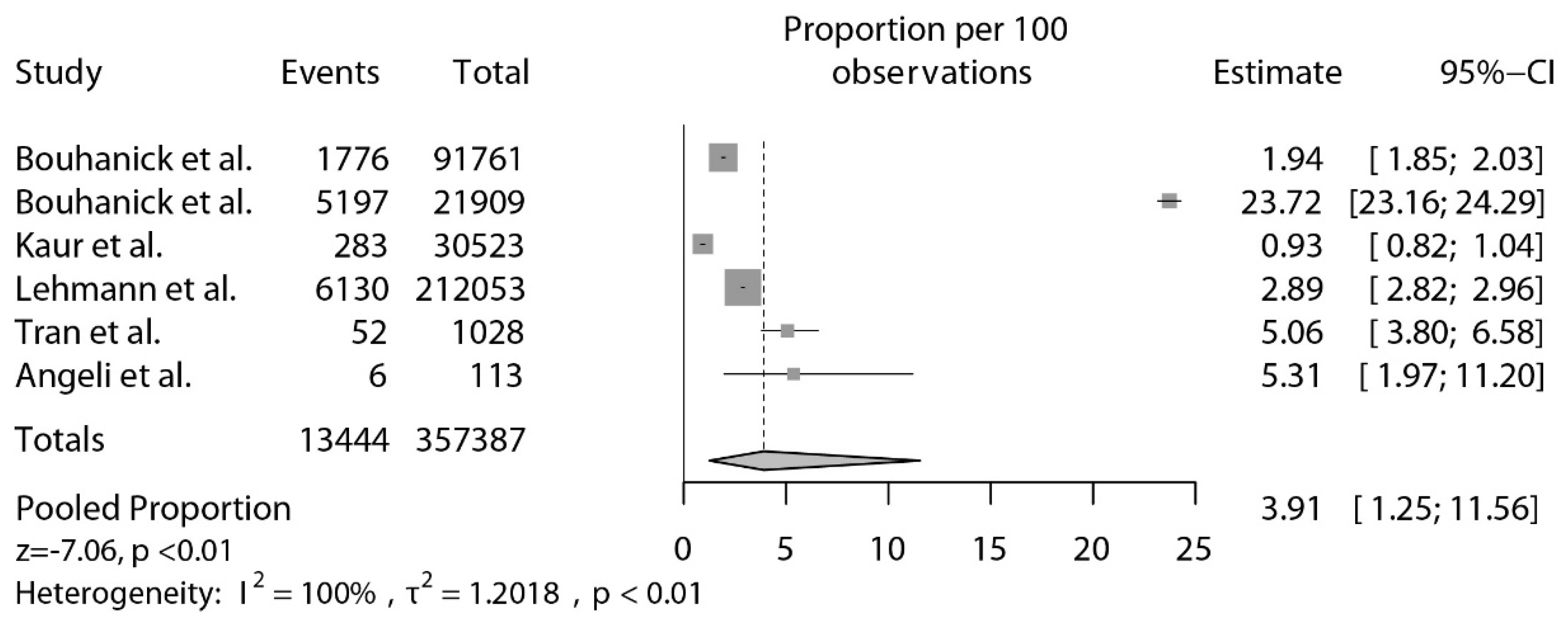
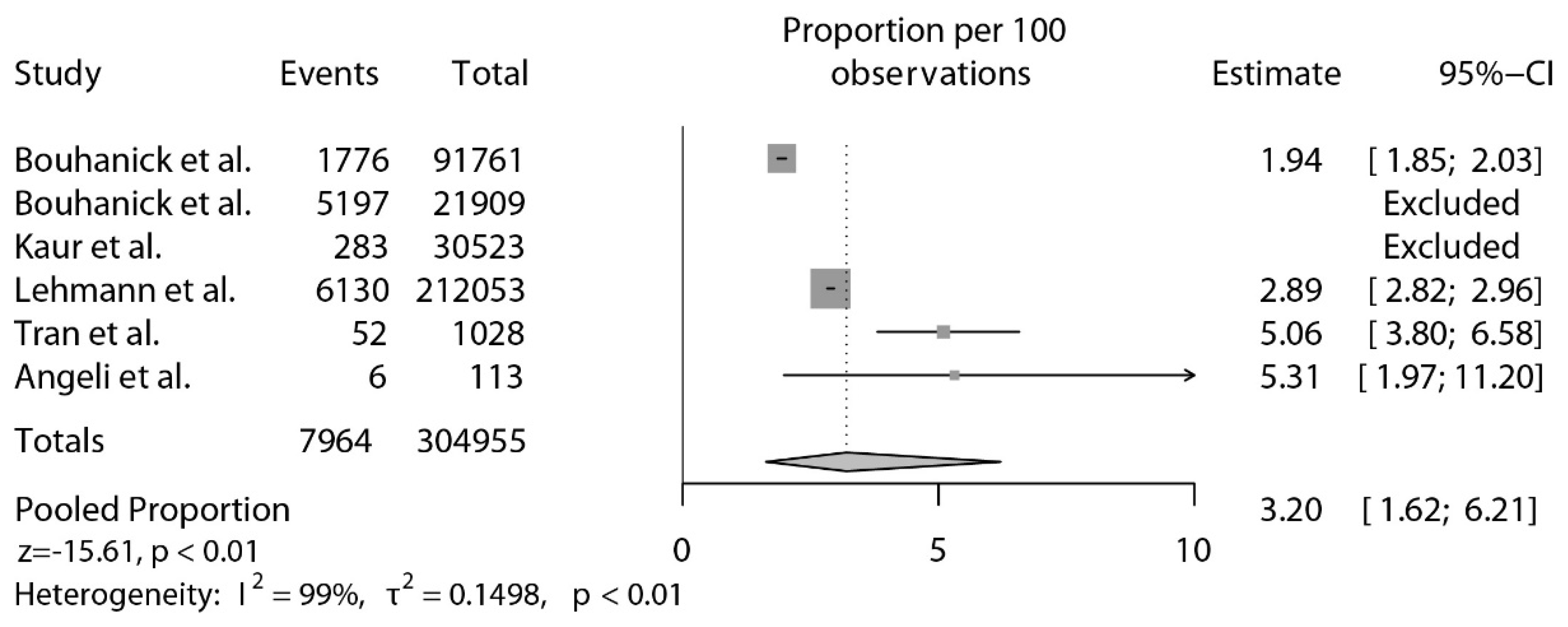
3.3. Pooled Analyzses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Angeli, F.; Reboldi, G.; Verdecchia, P. SARS-CoV-2 Infection and ACE2 Inhibition. J. Hypertens 2021, 39, 1555–1558. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Spanevello, A.; Reboldi, G.; Visca, D.; Verdecchia, P. SARS-CoV-2 vaccines: Lights and shadows. Eur. J. Intern. Med. 2021, 88, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Reboldi, G.; Verdecchia, P. Ageing, ACE2 deficiency and bad outcome in COVID-19. Clin. Chem. Lab. Med. 2021, 59, 1607–1609. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Verdecchia, P.; Balestrino, A.; Bruschi, C.; Ceriana, P.; Chiovato, L.; Dalla Vecchia, L.A.; Fanfulla, F.; La Rovere, M.T.; Perego, F.; et al. Renin Angiotensin System Blockers and Risk of Mortality in Hypertensive Patients Hospitalized for COVID-19: An Italian Registry. J. Cardiovasc. Dev. Dis. 2022, 9, 15. [Google Scholar] [CrossRef]
- Angeli, F.; Verdecchia, P.; Reboldi, G. RAAS Inhibitors and Risk of Covid-19. N. Engl. J. Med. 2020, 383, 1990–1991. [Google Scholar] [CrossRef]
- Verdecchia, P.; Angeli, F.; Reboldi, G. Angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers and coronavirus. J. Hypertens 2020, 38, 1190–1191. [Google Scholar] [CrossRef]
- Kaur, S.P.; Gupta, V. COVID-19 Vaccine: A comprehensive status report. Virus Res. 2020, 288, 198114. [Google Scholar] [CrossRef]
- Connors, M.; Graham, B.S.; Lane, H.C.; Fauci, A.S. SARS-CoV-2 Vaccines: Much Accomplished, Much to Learn. Ann. Intern. Med. 2021, 174, 687–690. [Google Scholar] [CrossRef]
- Bakhiet, M.; Taurin, S. SARS-CoV-2: Targeted managements and vaccine development. Cytokine Growth Factor Rev. 2021, 58, 16–29. [Google Scholar] [CrossRef]
- ChAdOx1 nCoV-19/AZD1222. Available online: https://www.astrazeneca.com/content/astraz/media-centre/press-releases/2021/azd1222-us-phase-iii-primary-analysis-confirms-safety-and-efficacy.html (accessed on 8 April 2021).
- FDA Briefing Document. Janssen Ad26.COV2.S Vaccine for the Prevention of COVID-19. Vaccines and Related Biological Products Advisory Committee Meeting. 26 February 2021. Available online: https://www.fda.gov/media/146217/download (accessed on 8 April 2021).
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I.; et al. Interim Results of a Phase 1-2a Trial of Ad26.COV2.S Covid-19 Vaccine. N. Engl. J. Med. 2021, 384, 1824–1835. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Wise, J. Covid-19: European countries suspend use of Oxford-AstraZeneca vaccine after reports of blood clots. BMJ 2021, 372, n699. [Google Scholar] [CrossRef]
- Joint CDC and FDA Statement on Johnson & Johnson COVID-19 Vaccine. Available online: https://www.fda.gov/news-events/press-announcements/joint-cdc-and-fda-statement-johnson-johnson-covid-19-vaccine (accessed on 14 April 2021).
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef]
- Schultz, N.H.; Sorvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattor, T.H.; Tjonnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef]
- Shiravi, A.A.; Ardekani, A.; Sheikhbahaei, E.; Heshmat-Ghahdarijani, K. Cardiovascular Complications of SARS-CoV-2 Vaccines: An Overview. Cardiol. Ther. 2022, 11, 13–21. [Google Scholar] [CrossRef]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA Vaccine against SARS-CoV-2—Preliminary Report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef]
- Ostergaard, S.D.; Schmidt, M.; Horvath-Puho, E.; Thomsen, R.W.; Sorensen, H.T. Thromboembolism and the Oxford-AstraZeneca COVID-19 vaccine: Side-effect or coincidence? Lancet 2021, 397, 1441–1443. [Google Scholar] [CrossRef]
- Angeli, F.; Reboldi, G.; Trapasso, M.; Verdecchia, P. Hypertension after COVID-19 vaccination. G. Ital. Cardiol. 2022, 23, 10–14. [Google Scholar] [CrossRef]
- Meylan, S.; Livio, F.; Foerster, M.; Genoud, P.J.; Marguet, F.; Wuerzner, G.; Center, C.C.V. Stage III Hypertension in Patients After mRNA-Based SARS-CoV-2 Vaccination. Hypertension 2021, 77, e56–e57. [Google Scholar] [CrossRef]
- Zappa, M.; Verdecchia, P.; Spanevello, A.; Visca, D.; Angeli, F. Blood pressure increase after Pfizer/BioNTech SARS-CoV-2 vaccine. Eur. J. Intern. Med. 2021, 90, 111–113. [Google Scholar] [CrossRef]
- Gregoire, G.; Derderian, F.; Le Lorier, J. Selecting the language of the publications included in a meta-analysis: Is there a Tower of Babel bias? J. Clin. Epidemiol. 1995, 48, 159–163. [Google Scholar] [CrossRef]
- Haynes, R.B.; Wilczynski, N.; McKibbon, K.A.; Walker, C.J.; Sinclair, J.C. Developing optimal search strategies for detecting clinically sound studies in MEDLINE. J. Am. Med. Inform. Assoc. 1994, 1, 447–458. [Google Scholar] [CrossRef] [Green Version]
- McAuley, L.; Pham, B.; Tugwell, P.; Moher, D. Does the inclusion of grey literature influence estimates of intervention effectiveness reported in meta-analyses? Lancet 2000, 356, 1228–1231. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- McPheeters, M.L.; Kripalini, S.; Peterson, N.B.; Idowu, R.T. Quality Improvement Interventions To Address Health Disparities. Evidence Report/ technology Assessment. Rockville (MD): Agency for Healthcare Research and Quality (US). 2012. Available online: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0049222/pdf/TOC.pdf (accessed on 18 March 2022).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. 2011. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 28 February 2022).
- Stijnen, T.; Hamza, T.H.; Ozdemir, P. Random effects meta-analysis of event outcome in the framework of the generalized linear mixed model with applications in sparse data. Stat. Med. 2010, 29, 3046–3067. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Erbert, D.D. Doing Meta-Analysis with R: A Hands-On Guide, 1st ed.; Chapman and Hall/CRC: New York, NY, USA, 2021. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouhanick, B.; Brusq, C.; Bongard, V.; Tessier, S.; Montastruc, J.L.; Senard, J.M.; Montastruc, F.; Herin, F. Blood pressure measurements after mRNA-SARS-CoV-2 tozinameran vaccination: A retrospective analysis in a university hospital in France. J. Hum. Hypertens 2022, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Bouhanick, B.; Montastruc, F.; Tessier, S.; Brusq, C.; Bongard, V.; Senard, J.M.; Montastruc, J.L.; Herin, F. Hypertension and Covid-19 vaccines: Are there any differences between the different vaccines? A safety signal. Eur. J. Clin. Pharmacol. 2021, 77, 1937–1938. [Google Scholar] [CrossRef] [PubMed]
- Ch’ng, C.C.; Ong, L.M.; Wong, K.M. Changes in Blood Pressure After Pfizer/Biontech Sars-Cov-2 Vaccination. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Kaur, R.J.; Dutta, S.; Charan, J.; Bhardwaj, P.; RTandon, A.; Yadav, D.; Islam, S.; Haque, M. Cardiovascular Adverse Events Reported from COVID-19 Vaccines: A Study Based on WHO Database. Int. J. Gen. Med. 2021, 14, 3909–3927. [Google Scholar] [CrossRef]
- Sanidas, E.; Anastasiou, T.; Papadopoulos, D.; Velliou, M.; Mantzourani, M. Short term blood pressure alterations in recently COVID-19 vaccinated patients. Eur. J. Intern. Med. 2022, 96, 115–116. [Google Scholar] [CrossRef]
- Tran, V.N.; Nguyen, H.A.; Le, T.T.A.; Truong, T.T.; Nguyen, P.T.; Nguyen, T.T.H. Factors influencing adverse events following immunization with AZD1222 in Vietnamese adults during first half of 2021. Vaccine 2021, 39, 6485–6491. [Google Scholar] [CrossRef]
- Lehmann, K. Suspected Cardiovascular Side Effects of two Covid-19 Vaccines. J. Biol. Today’s World 2021, 10, 1–6. [Google Scholar] [CrossRef]
- Angeli, F.; Masnaghetti, S.; Visca, D.; Rossoni, A.; Taddeo, S.; Biagini, F.; Verdecchia, P. Severity of COVID-19: The importance of being hypertensive. Monaldi Arch. Chest Dis. 2020, 90. [Google Scholar] [CrossRef]
- Kyriakidis, N.C.; Lopez-Cortes, A.; Gonzalez, E.V.; Grimaldos, A.B.; Prado, E.O. SARS-CoV-2 vaccines strategies: A comprehensive review of phase 3 candidates. NPJ Vaccines 2021, 6, 28. [Google Scholar] [CrossRef]
- Angeli, F.; Verdecchia, P.; Reboldi, G. Pharmacotherapy for hypertensive urgency and emergency in COVID-19 patients. Expert Opin. Pharm. 2022, 23, 235–242. [Google Scholar] [CrossRef]
- Angeli, F.; Zappa, M.; Reboldi, G.; Trapasso, M.; Cavallini, C.; Spanevello, A.; Verdecchia, P. The pivotal link between ACE2 deficiency and SARS-CoV-2 infection: One year later. Eur. J. Intern. Med. 2021, 93, 28–34. [Google Scholar] [CrossRef]
- Verdecchia, P.; Cavallini, C.; Spanevello, A.; Angeli, F. COVID-19: ACE2centric Infective Disease? Hypertension 2020, 76, 294–299. [Google Scholar] [CrossRef]
- Verdecchia, P.; Cavallini, C.; Spanevello, A.; Angeli, F. The pivotal link between ACE2 deficiency and SARS-CoV-2 infection. Eur. J. Intern. Med. 2020, 76, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, P.; Reboldi, G.; Cavallini, C.; Mazzotta, G.; Angeli, F. ACE-inhibitors, angiotensin receptor blockers and severe acute respiratory syndrome caused by coronavirus. G. Ital. Cardiol. 2020, 21, 321–327. [Google Scholar] [CrossRef]
- Watanabe, Y.; Mendonca, L.; Allen, E.R.; Howe, A.; Lee, M.; Allen, J.D.; Chawla, H.; Pulido, D.; Donnellan, F.; Davies, H.; et al. Native-like SARS-CoV-2 spike glycoprotein expressed by ChAdOx1 nCoV-19/AZD1222 vaccine. ACS Cent. Sci. 2021, 7, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Deshotels, M.R.; Xia, H.; Sriramula, S.; Lazartigues, E.; Filipeanu, C.M. Angiotensin II mediates angiotensin converting enzyme type 2 internalization and degradation through an angiotensin II type I receptor-dependent mechanism. Hypertension 2014, 64, 1368–1375. [Google Scholar] [CrossRef] [Green Version]
- Simoes e Silva, A.C.; Silveira, K.D.; Ferreira, A.J.; Teixeira, M.M. ACE2, angiotensin-(1–7) and Mas receptor axis in inflammation and fibrosis. Br. J. Pharm. 2013, 169, 477–492. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Vaccine | Developer | Platform | Doses |
|---|---|---|---|
| BNT162b2 * | Pfizer/BioNTech | mRNA | 2 |
| mRNA-1273 * | Moderna | mRNA | 2 |
| Ad26.COV2.S * | Janssen/Johnson & Johnson | DNA Adenovirus vector | 1 |
| CVnCoV | CureVAC | mRNA | 2 |
| ChAdOx1nCoV-19 * | AstraZeneca/University of Oxford/Serum Institute of India | DNA Adenovirus vector | 2 |
| NVX-CoV2373 * | Novavax | Recombinant protein | 2 |
| Gam-COVID-Vac (Sputnik V) | Gamaleya Institute | DNA Adenovirus vectors | 2 |
| Study | Source | Cohort (N) | Year | Vaccine | Outcome | Severe Increase in BP * (N) | |
|---|---|---|---|---|---|---|---|
| Definition | N | ||||||
| Bouhanick et al. [36] | Pharmacovigilance database | 91,761 | 2021 | BNT162b2, ChAdOx1nCoV-19, Ad26.COV2.S | Abnormal BP | 1776 | - |
| Bouhanick et al. [35] | Patients and healthcare workers | 21,909 | 2022 | BNT162b2 | Persistent BP ≥ 140/90 (15 min after vaccination) | 5197 | 709 |
| Kaur et al. [38] | Pharmacovigilance database | 30,523 | 2021 | BNT162b2, ChAdOx1nCoV-19, mRNA-1273 | Abnormal BP | 283 | 36 |
| Lehmann et al. [41] | Pharmacovigilance database | 212,053 | 2021 | BNT162b2, ChAdOx1nCoV-19, Ad26.COV2.S, mRNA-1273 | Abnormal BP | 6130 | 551 |
| Tran et al. [40] | Cross-sectional online survey | 1028 | 2021 | ChAdOx1nCoV-19 | Self reported hypertension | 52 | - |
| Angeli et al. [25] | Cross-sectional online survey | 113 | 2021 | BNT162b2 | Raise in home BP > 10 mmHg | 6 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angeli, F.; Reboldi, G.; Trapasso, M.; Santilli, G.; Zappa, M.; Verdecchia, P. Blood Pressure Increase following COVID-19 Vaccination: A Systematic Overview and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2022, 9, 150. https://doi.org/10.3390/jcdd9050150
Angeli F, Reboldi G, Trapasso M, Santilli G, Zappa M, Verdecchia P. Blood Pressure Increase following COVID-19 Vaccination: A Systematic Overview and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2022; 9(5):150. https://doi.org/10.3390/jcdd9050150
Chicago/Turabian StyleAngeli, Fabio, Gianpaolo Reboldi, Monica Trapasso, Gabriella Santilli, Martina Zappa, and Paolo Verdecchia. 2022. "Blood Pressure Increase following COVID-19 Vaccination: A Systematic Overview and Meta-Analysis" Journal of Cardiovascular Development and Disease 9, no. 5: 150. https://doi.org/10.3390/jcdd9050150