
Multimodality Imaging in the Detection of Ischemic Heart Disease in Women
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
Background
2. Discussion
2.1. Etiologies
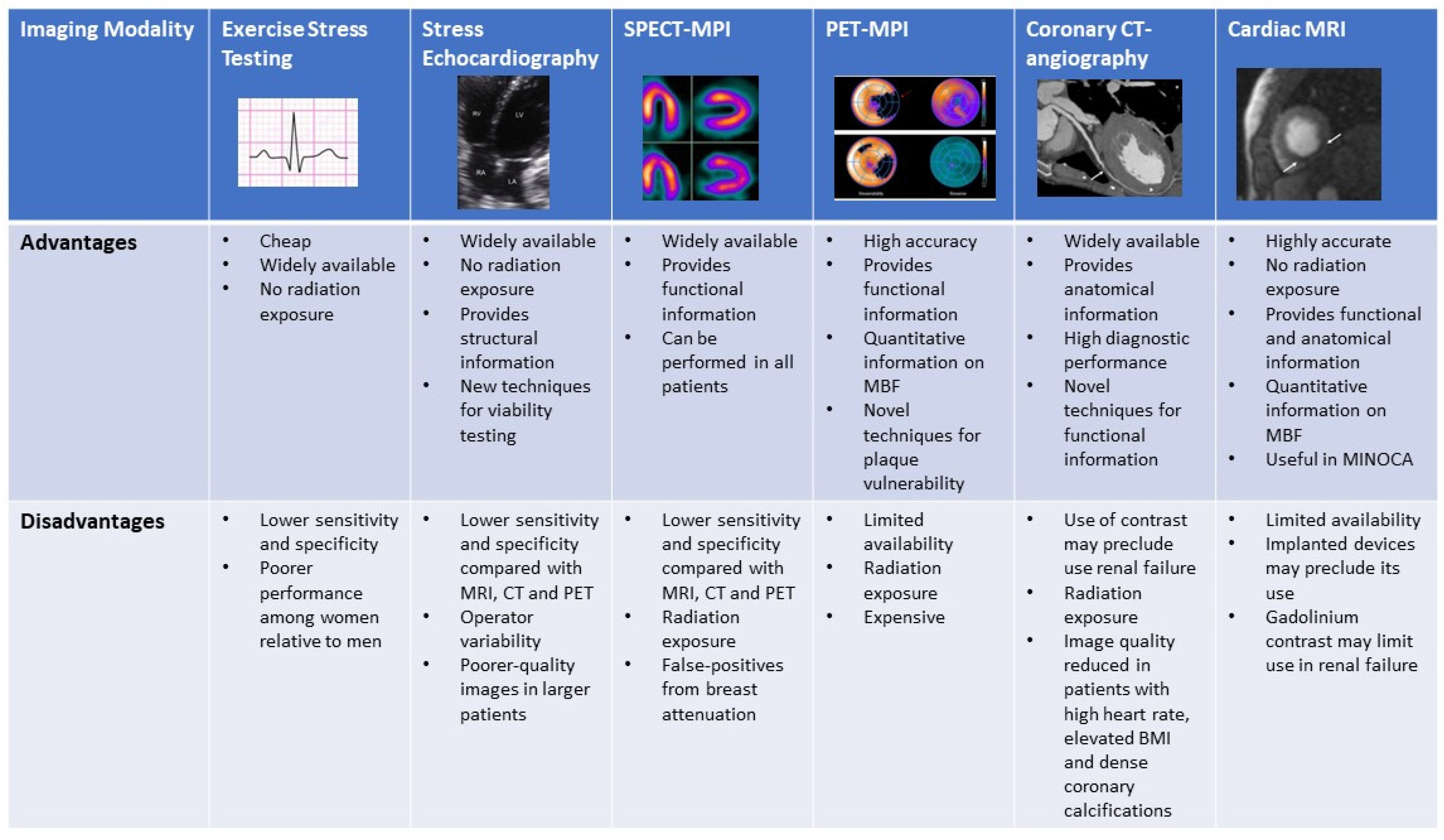
2.2. Noninvasive Imaging Modalities
2.3. Exercise Stress Testing
2.4. Exercise and Dobutamine Stress Echocardiography
2.5. SPECT- Myocardial Perfusion Imaging (Exercise and Pharmacological)
2.6. Stress Positron Emission Tomography
2.7. Coronary CT Angiography
2.8. Stress Cardiac Magnetic Resonance Imaging
2.9. Safety of Non-Invasive Imaging Modalities for Ischemia in Women and Pregnancy
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar]
- Hales, C.M.C.M.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity among Adults and Youth: United States, 2015–2016; NCHS Data Brief, No 288; National Center for Health Statistics: Hyattsville, MD, USA, 2017.
- Pandya, A.; Gaziano, T.A.; Weinstein, M.C.; Cutler, D. More Americans Living Longer with Cardiovascular Disease Will Increase Costs While Lowering Quality Of Life. Health Aff. 2013, 32, 1706–1714. [Google Scholar] [CrossRef] [Green Version]
- Blomkalns, A.L.; Chen, A.Y.; Hochman, J.S.; Peterson, E.D.; Trynosky, K.; Diercks, D.B.; Brogan, G.X.; Boden, W.E.; Roe, M.T.; Ohman, E.M.; et al. Gender disparities in the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: Large-scale observations from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the American College of Cardiology/American Heart Association Guidelines) National Quality Improvement Initiative. J. Am. Coll. Cardiol. 2005, 45, 832–837. [Google Scholar]
- Daugherty, S.L.; Peterson, P.N.; Magid, D.J.; Ho, P.M.; Bondy, J.; Hokanson, J.E.; Ross, C.A.; Rumsfeld, J.S.; Masoudi, F.A. The relationship between gender and clinical management after exercise stress testing. Am. Hear. J. 2008, 156, 301–307. [Google Scholar] [CrossRef]
- Vaccarino, V.; Rathore, S.S.; Wenger, N.K.; Frederick, P.D.; Abramson, J.L.; Barron, H.V.; Manhapra, A.; Mallik, S.; Krumholz, H.M. Sex and Racial Differences in the Management of Acute Myocardial Infarction, 1994 through 2002. N. Engl. J. Med. 2005, 353, 671–682. [Google Scholar] [CrossRef] [Green Version]
- Strong, J.P.; Malcom, G.T.; Newman, W.P.; Oalmann, M.C. Early Lesions of Atherosclerosis in Childhood and Youth: Natural History and Risk Factors. J. Am. Coll. Nutr. 1992, 11 (Suppl. 1), S51–S54. [Google Scholar] [CrossRef]
- Pasupathy, S.; Tavella, R.; Beltrame, J.F. Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA). Circulation 2017, 135, 1490–1493. [Google Scholar] [CrossRef]
- Tamis-Holland, J.E.; Jneid, H.; Reynolds, H.R.; Agewall, S.; Brilakis, E.S.; Brown, T.M.; Lerman, A.; Cushman, M.; Kumbhani, D.J.; Arslanian-Engoren, C.; et al. Contemporary Diagnosis and Management of Patients with Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation 2019, 139, e891–e908. [Google Scholar] [CrossRef]
- Safdar, B.; Spatz, E.S.; Dreyer, R.P.; Beltrame, J.F.; Lichtman, J.H.; Spertus, J.A.; Reynolds, H.R.; Geda, M.; Bueno, H.; Dziura, J.D.; et al. Presentation, Clinical Profile, and Prognosis of Young Patients with Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): Results From the VIRGO Study. J. Am. Heart. Assoc. 2018, 7, e009174. [Google Scholar] [CrossRef] [Green Version]
- Dreyer, R.P.; Tavella, R.; Curtis, J.P.; Wang, Y.; Pauspathy, S.; Messenger, J.; Rumsfeld, J.S.; Maddox, T.M.; Krumholz, H.M.; Spertus, J.A.; et al. Myocardial infarction with non-obstructive coronary arteries as compared with myocardial infarction and obstructive coronary disease: Outcomes in a Medicare population. Eur. Heart J. 2020, 41, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Merz, C.N.B.; Pepine, C.J.; Walsh, M.N.; Fleg, J.L. Ischemia and No Obstructive Coronary Artery Disease (INOCA): Developing Evidence-Based Therapies and Research Agenda for the Next Decade. Circulation 2017, 135, 1075–1092. [Google Scholar] [CrossRef] [PubMed]
- Kenkre, T.S.; Malhotra, P.; Johnson, B.D.; Handberg, E.M.; Thompson, D.V.; Marroquin, O.C.; Rogetrs, W.J.; Pepine, C.J.; Merz, C.N.B.; Kelsey, S.F. Ten-Year Mortality in the WISE Study (Women’s Ischemia Syndrome Evaluation). Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003863. [Google Scholar] [CrossRef] [PubMed]
- Ferencik, M.; Mayrhofer, T.; Bittner, D.O.; Emami, H.; Puchner, S.B.; Lu, M.T.; Meyersohn, N.M.; Ivanov, A.V.; Adami, E.C.; Patel, M.R.; et al. Use of High-Risk Coronary Atherosclerotic Plaque Detection for Risk Stratification of Patients with Stable Chest Pain: A Secondary Analysis of the PROMISE Randomized Clinical Trial. JAMA Cardiol. 2018, 3, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Gan, L.M.; Svedlund, S.; Wittfeldt, A.; Eklund, C.; Gao, S.; Matejka, G.; Jetppsson, A.; Albertsson, P.; Omerovic, E.; Lerman, A. Incremental Value of Transthoracic Doppler Echocardiography-Assessed Coronary Flow Reserve in Patients with Suspected Myocardial Ischemia Undergoing Myocardial Perfusion Scintigraphy. J. Am. Heart Assoc. 2017, 6, e004875. [Google Scholar] [CrossRef] [Green Version]
- Tjoe, B.; Barsky, L.; Wei, J.; Samuels, B.; Azarbal, B.; Merz, C.N.B.; Shufelt, C. Coronary microvascular dysfunction: Considerations for diagnosis and treatment. Clevel. Clin. J. Med. 2021, 88, 561–571. [Google Scholar] [CrossRef]
- Herscovici, R.; Sedlak, T.; Wei, J.; Pepine, C.J.; Handberg, E.; Bairey Merz, C.N. Ischemia and No Obstructive Coronary Artery Disease (INOCA): What Is the Risk? J. Am. Heart Assoc. 2018, 7, e008868. [Google Scholar] [CrossRef]
- Hayes, S.N.; Tweet, M.S.; Adlam, D.; Kim, E.S.H.; Gulati, R.; Price, J.E.; Rose, C.H. Spontaneous Coronary Artery Dissection. J. Am. Coll. Cardiol. 2020, 76, 961–984. [Google Scholar] [CrossRef]
- Saw, J.; Starovoytov, A.; Humphries, K.; Sheth, T.; So, D.; Minhas, K.; Brass, N.; Lavoie, A.; Bishop, H.; Lavi, S.; et al. Canadian spontaneous coronary artery dissection cohort study: In-hospital and 30-day outcomes. Eur. Heart J. 2019, 40, 1188–1197. [Google Scholar] [CrossRef] [Green Version]
- Brieger, D.; Eagle, K.A.; Goodman, S.G.; Steg, P.G.; Budaj, A.; White, K.; Montalescot, G. Acute Coronary Syndromes without Chest Pain, An Underdiagnosed and Undertreated High-Risk Group: Insights From The Global Registry of Acute Coronary Events. Chest 2004, 126, 461–469. [Google Scholar] [CrossRef] [Green Version]
- Khan, N.A. Sex Differences in Acute Coronary Syndrome Symptom Presentation in Young Patients. JAMA Intern. Med. 2013, 173, 1863–1871. [Google Scholar] [CrossRef]
- Murthy, V.L.; Naya, M.; Taqueti, V.R.; Foster, C.R.; Gaber, M.; Hainer, J.; Dorbala, S.; Blankstein, R.; Rimoldi, O.; Camici, P.G.; et al. Effects of Sex on Coronary Microvascular Dysfunction and Cardiac Outcomes. Circulation 2014, 129, 2518–2527. [Google Scholar] [CrossRef]
- Kligfield, P.; Lauer, M.S. Exercise Electrocardiogram Testing. Circulation 2006, 114, 2070–2082. [Google Scholar] [CrossRef]
- Lewis, J.F.; McGorray, S.; Lin, L.; Pepine, C.J.; Chaitman, B.; Doyle, M.; Etdmundowicz, D.; Sharaf, B.L.; Merz, C.N.B. Exercise treadmill testing using a modified exercise protocol in women with suspected myocardial ischemia: Findings from the National Heart, Lung and Blood Institute–sponsored Women’s Ischemia Syndrome Evaluation (WISE). Am. Heart J. 2005, 149, 527–533. [Google Scholar] [CrossRef]
- Kwok, Y.; Kim, C.; Grady, D.; Segal, M.; Redberg, R. Meta-analysis of exercise testing to detect coronary artery disease in women. Am. J. Cardiol. 1999, 83, 660–666. [Google Scholar] [CrossRef]
- Linhart, J.W.; Laws, J.G.; Satinsky, J.D. Maximum Treadmill Exercise Electrocardiography in Female Patients. Circulation 1974, 50, 1173–1178. [Google Scholar] [CrossRef] [Green Version]
- Hlatky, M.A.; Pryor, D.B.; Harrell, F.E.; Califf, R.M.; Mark, D.B.; Rosati, R.A. Factors affecting sensitivity and specificity of exercise electrocardiography: Multivariable analysis. Am. J. Med. 1984, 77, 64–71. [Google Scholar] [CrossRef]
- Weiner, D.A.; Ryan, T.J.; McCabe, C.H.; Kennedy, J.W.; Schloss, M.; Tristani, F.; Chaitman, B.R.; Fisher, L.D. Exercise Stress Testing. N. Engl. J. Med. 1979, 301, 230–235. [Google Scholar] [CrossRef]
- Blankstein, R.; Ahmed, W.; Bamberg, F.; Rogers, I.S.; Schlett, C.L.; Nasir, K.; Fontes, J.D.; Tawakol, A.; Brady, T.J.; Nagurney, J.T.; et al. Comparison of Exercise Treadmill Testing with Cardiac Computed Tomography Angiography Among Patients Presenting to the Emergency Room with Chest Pain. Circ. Cardiovasc. Imaging 2012, 5, 233–242. [Google Scholar] [CrossRef] [Green Version]
- Shaw, L.J.; Mieres, J.H.; Hendel, R.H.; Boden, W.E.; Gulati, M.; Veledar, E.; Hachamovitch, R.; Arrighi, J.A.; Merz, C.N.B.; Gibbons, R.J.; et al. Comparative Effectiveness of Exercise Electrocardiography with or without Myocardial Perfusion Single Photon Emission Computed Tomography in Women with Suspected Coronary Artery Disease. Circulation 2011, 124, 1239–1249. [Google Scholar] [CrossRef] [Green Version]
- Smiseth, O.A.; Torp, H.; Opdahl, A.; Haugaa, K.H.; Urheim, S. Myocardial strain imaging: How useful is it in clinical decision making? Eur. Heart J. 2016, 37, 1196–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, R.; Altiok, E.; Heussen, N.; Hanrath, P.; Nowak, B.; Kaiser, H.-J.; Büll, U.; Kühl, H. Strain rate measurement by doppler echocardiography allows improvedassessment of myocardial viability inpatients with depressed left ventricular function. J. Am. Coll. Cardiol. 2002, 39, 443–449. [Google Scholar] [CrossRef]
- Pellikka, P.A.; Arruda-Olson, A.; Chaudhry, F.A.; Chen, M.H.; Marshall, J.E.; Porter, T.R.; Sawada, S.G. Guidelines for Performance, Interpretation, and Application of Stress Echocardiography in Ischemic Heart Disease: From the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2020, 33, 1–41.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.; Kwok, Y.S.; Heagerty, P.; Redberg, R. Pharmacologic stress testing for coronary disease diagnosis: A meta-analysis. Am. Heart J. 2001, 142, 934–944. [Google Scholar] [CrossRef]
- Mieres, J.H.; Shaw, L.J.; Arai, A.; Budoff, M.J.; Flamm, S.D.; Hundley, W.G.; Marwick, T.H.; Mosca, L.; Patel, A.; Quinones, M.A.; et al. Role of Noninvasive Testing in the Clinical Evaluation of Women with Suspected Coronary Artery Disease. Circulation 2005, 111, 682–696. [Google Scholar] [CrossRef] [Green Version]
- Roger, V.L.; Pellikka, P.A.; Bell, M.R.; Chow, C.W.H.; Bailey, K.R.; Seward, J.B. Sex and Test Verification Bias. Circulation 1997, 95, 405–410. [Google Scholar] [CrossRef]
- Dionisopoulos, P.N.; Collins, J.D.; Smart, S.C.; Knickelbine, T.A.; Sagar, K.B. The value of dobutamine stress echocardiography for the detection of coronary artery disease in women. J. Am. Soc. Echocardiogr. 1997, 10, 811–817. [Google Scholar] [CrossRef]
- Arruda-Olson Adelaide, M.; Juracan Eldyn, M.; Mahoney Douglas, W.; McCully Robert, B.; Roger Veronique, L.; Pellikka Patricia, A. Prognostic value of exercise echocardiographyin 5798 patients: Is there a gender difference? J. Am. Coll. Cardiol. 2002, 39, 625–631. [Google Scholar] [CrossRef] [Green Version]
- Woodward, W.; Dockerill, C.; McCourt, A.; Upton, R.; O’Driscoll, J.; Balkhausen, K.; Chandrasekaran, B.; Firoozan, S.; Kardos, A.; Wong, K.; et al. Real-world performance and accuracy of stress echocardiography: The EVAREST observational multi-centre study. Eur. Heart J.-Cardiovasc. Imaging 2022, 23, 689–698. [Google Scholar] [CrossRef]
- Gowd, B.M.P.; Heller, G.V.; Parker, M.W. Stress-only SPECT myocardial perfusion imaging: A review. J. Nucl. Cardiol. 2014, 21, 1200–1212. [Google Scholar] [CrossRef]
- Santana-Boado, C.; Candell-Riera, J.; Castell-Conesa, J.; Aguadé-Bruix, S. Diagnostic accuracy of technetium-99m-MIBI myocardial SPECT in women and men. J. Nucl. Med. 1998, 39, 751. [Google Scholar] [PubMed]
- Kong, B.A.; Shaw, L.; Miller, D.D.; Chaitman, B.R. Comparison of accuracy for detecting coronary artery disease and side-effect profile of dipyridamole thallium-201 myocardial perfusion imaging in women versus men. Am. J. Cardiol. 1992, 70, 168–173. [Google Scholar] [CrossRef]
- Amanullah, A.M.; Berman, D.S.; Hachamovitch, R.; Kiat, H.; Kang, X.; Friedman, J.D. Identification of Severe or Extensive Coronary Artery Disease in Women by Adenosine Technetium-99m Sestamibi SPECT. Am. J. Cardiol. 1997, 80, 132–137. [Google Scholar] [CrossRef]
- Iskandar, A.; Limone, B.; Parker, M.W.; Perugini, A.; Kim, H.; Jones, C.; Calamari, B.; Coleman, C.; Heller, G.V. Gender differences in the diagnostic accuracy of SPECT myocardial perfusion imaging: A bivariate meta-analysis. J. Nucl. Cardiol. 2013, 20, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Hachamovitch, R.; Berman, D.S.; Kiat, H.; Bairey Merz, C.N.B.; Cohen, I.; Cabico, J.; Friedman, J.; Germano, G.; Van Train, K.F.; Dialmond, G.A. Effective risk stratification using exercise myocardial perfusion SPECT in women: Gender-related differences in prognostic nuclear testing. J. Am. Coll. Cardiol. 1996, 28, 34–44. [Google Scholar] [CrossRef] [Green Version]
- Sharir, T.; Germano, G.; Kavanagh, P.B.; Lai, S.; Cohen, I.; Lewin, H.C.; Frietdman, J.D.; Zellweger, M.J.; Bermaln, D.S. Incremental Prognostic Value of Post-Stress Left Ventricular Ejection Fraction and Volume by Gated Myocardial Perfusion Single Photon Emission Computed Tomography. Circulation 1999, 100, 1035–1042. [Google Scholar] [CrossRef] [Green Version]
- Mieres, J. A report of the American Society of Nuclear Cardiology Task Force on Women and Heart Disease (writing group on perfusion imaging in women). J. Nucl. Cardiol. 2003, 10, 95–101. [Google Scholar] [CrossRef]
- Taqueti, V.R.; Dorbala, S.; Wolinsky, D.; Abbott, B.; Heller, G.V.; Bateman, T.M.; Mietres, J.H.; Phillips, L.M.; Wenger, N.K.; Shaw, L.J. Myocardial perfusion imaging in women for the evaluation of stable ischemic heart disease—State-of-the-evidence and clinical recommendations. J. Nucl. Cardiol. 2017, 24, 1402–1426. [Google Scholar] [CrossRef] [Green Version]
- Berrington De Gonzalez, A.; Kim, K.-P.; Smith-Bindman, R.; McAreavey, D. Myocardial Perfusion Scans. Circulation 2010, 122, 2403–2410. [Google Scholar] [CrossRef]
- Murthy, V.L.; Bateman, T.M.; Beanlands, R.S.; Berman, D.S.; Borges-Neto, S.; Chareonthaitawee, P.; Cerqueira, M.D.; deKemp, R.A.; DePuey, E.G.; Dilsizian, V.; et al. Clinical Quantification of Myocardial Blood Flow Using PET: Joint Position Paper of the SNMMI Cardiovascular Council and the ASNC. J. Nucl. Cardiol. 2018, 25, 269–297. [Google Scholar] [CrossRef] [Green Version]
- Nakazato, R.; Berman, D.S.; Alexanderson, E.; Slomka, P. Myocardial perfusion imaging with PET. Imaging Med. 2013, 5, 35–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bateman, T.M.; Heller, G.V.; McGhie, A.I.; Friedman, J.D.; Case, J.A.; Bryngelson, J.R.; Hertenstein, G.K.; Moutray, K.L.; Reid, K.; Cullom, S.J. Diagnostic accuracy of rest/stress ECG-gated Rb-82 myocardial perfusion PET: Comparison with ECG-gated Tc-99m sestamibi SPECT. J. Nucl. Cardiol. 2006, 13, 24–33. [Google Scholar] [CrossRef]
- Cerqueira, M.D.; Allman, K.C.; Ficaro, E.P.; Hansen, C.L.; Nichols, K.J.; Thompson, R.C.; Van Decker, W.A.; Yakovlevitch, M. Recommendations for reducing radiation exposure in myocardial perfusion imaging. J. Nucl. Cardiol. 2010, 17, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Sampson Uchechukwu, K.; Dorbala, S.; Limaye, A.; Kwong, R.; Di Carli Marcelo, F. Diagnostic Accuracy of Rubidium-82 Myocardial Perfusion Imaging with Hybrid Positron Emission Tomography/Computed Tomography in the Detection of Coronary Artery Disease. J. Am. Coll. Cardiol. 2007, 49, 1052–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nandalur, K.R.; Dwamena, B.A.; Choudhri, A.F.; Nandalur, S.R.; Reddy, P.; Carlos, R.C. Diagnostic Performance of Positron Emission Tomography in the Detection of Coronary Artery Disease: A Meta-analysis. Acad. Radiol. 2008, 15, 444–451. [Google Scholar] [CrossRef]
- Sdringola, S.; Nakagawa, K.; Nakagawa, Y.; Yusuf, S.W.; Boccalandro, F.; Mullani, N.; Haynie, M.; Hess, M.J.; Gould, K.L. Combined intense lifestyle and pharmacologic lipid treatment further reduce coronary events and myocardial perfusion abnormalities compared with usual-care cholesterol-lowering drugs in coronary artery disease. J. Am. Coll. Cardiol. 2003, 41, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Figueroa, A.L.; Subramanian, S.S.; Cury, R.C.; Truong, Q.A.; Gardecki, J.A.; Tearney, G.J.; Hoffmann, U.; Brady, T.J.; Tawakol, A. Distribution of inflammation within carotid atherosclerotic plaques with high-risk morphological features: A comparison between positron emission tomography activity, plaque morphology, and histopathology. Circ. Cardiovasc. Imaging 2012, 5, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarkin, J.M.; Joshi, F.R.; Evans, N.R.; Chowdhury, M.M.; Figg, N.L.; Shah, A.V.; Starks, L.T.; Martin-Garrido, A.; Manavaki, R.; Yu, E.; et al. Detection of Atherosclerotic Inflammation by 68Ga-DOTATATE PET Compared to [18F]FDG PET Imaging. J. Am. Coll. Cardiol. 2017, 69, 1774–1791. [Google Scholar] [CrossRef]
- Joshi, N.V.; Vesey, A.T.; Williams, M.C.; Shah, A.S.V.; Calvert, P.A.; Craighead, F.H.M.; Yeoh, S.E.; Wallace, W.; Salter, D.; Fletcher, A.M.; et al. 18F-fluoride positron emission tomography for identification of ruptured and high-risk coronary atherosclerotic plaques: A prospective clinical trial. Lancet 2014, 383, 705–713. [Google Scholar] [CrossRef] [Green Version]
- Joseph, P.; Tawakol, A. Imaging atherosclerosis with positron emission tomography. Eur. Heart J. 2016, 37, 2974–2980. [Google Scholar] [CrossRef] [Green Version]
- Bhalla, S. Coronary Computed Tomography Angiography of Spontaneous Coronary Artery Dissection: A Case Report and Review of the Literature. Am. J. Case Rep. 2015, 16, 130–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Truong, Q.A.; Rinehart, S.; Abbara, S.; Achenbach, S.; Berman, D.S.; Bullock-Palmer, R.; Carrascosa, P.; Chinnaiyan, K.M.; Dey, D.; Ferencik, M.; et al. Coronary computed tomographic imaging in women: An expert consensus statement from the Society of Cardiovascular Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2018, 12, 451–466. [Google Scholar] [CrossRef]
- Abdelrahman Khaled, M.; Chen Marcus, Y.; Dey Amit, K.; Virmani, R.; Finn Aloke, V.; Khamis Ramzi, Y.; Choi, A.D.; Min, J.K.; Williams, M.C.; Buckler, A.J.; et al. Coronary Computed Tomography Angiography From Clinical Uses to Emerging Technologies. J. Am. Coll. Cardiol. 2020, 76, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Haase, R.; Schlattmann, P.; Gueret, P.; Andreini, D.; Pontone, G.; Alkadhi, H.; Hausleiter, J.; Garcia, M.J.; Leschka, S.; Meijboom, W.B.; et al. Diagnosis of obstructive coronary artery disease using computed tomography angiography in patients with stable chest pain depending on clinical probability and in clinically important subgroups: Meta-analysis of individual patient data. BMJ 2019, 365, l1945. [Google Scholar] [CrossRef] [Green Version]
- Arbab-Zadeh, A.; Di Carli, M.F.D.; Cerci, R.; George, R.T.; Chen, M.Y.; Dewey, M.; Niinuma, H.; Vavere, A.L.; Betoko, A.; Plotkin, M.; et al. Accuracy of Computed Tomographic Angiography and Single-Photon Emission Computed Tomography–Acquired Myocardial Perfusion Imaging for the Diagnosis of Coronary Artery Disease. Circ. Cardiovasc. Imaging 2015, 8, e003533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, B.J.; Abraham, A.; Wells, G.A.; Chen, L.; Ruddy, T.D.; Yam, Y.; Govas, N.; Galbraith, P.D.; Dennie, C.; Beanlands, R.S. Diagnostic accuracy and impact of computed tomographic coronary angiography on utilization of invasive coronary angiography. Circ. Cardiovasc. Imaging 2009, 2, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, M.C.; Moss, A.J.; Dweck, M.; Adamson, P.D.; Alam, S.; Hunter, A.; Shah, A.S.; Pawade, T.; Weir-McCall, J.R.; Roditi, G.; et al. Coronary Artery Plaque Characteristics Associated with Adverse Outcomes in the SCOT-HEART Study. J. Am. Coll. Cardiol. 2019, 73, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Neglia, D.; Rovai, D.; Caselli, C.; Pietila, M.; Teresinska, A.; Aguadé-Bruix, S.; Pizzi, M.N.; Todiere, G.; Gimelli, A.; Schroeder, S.; et al. Detection of Significant Coronary Artery Disease by Noninvasive Anatomical and Functional Imaging. Circ. Cardiovasc. Imaging 2015, 8, e002179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douglas, P.S.; Hoffmann, U.; Patel, M.R.; Mark, D.B.; Al-Khalidi, H.R.; Cavanaugh, B.; Cole, J.; Dolor, R.J.; Fordyce, C.B.; Huang, M.; et al. Outcomes of Anatomical versus Functional Testing for Coronary Artery Disease. N. Engl. J. Med. 2015, 372, 1291–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jug, B.; Gupta, M.; Papazian, J.; Li, D.N.; Tsang, J.; Bhatia, H.; Karlsbetrg, R.; Budoff, M. Diagnostic performance of 64-slice multidetector coronary computed tomographic angiography in women. J. Nucl. Cardiol. 2012, 19, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Nous, F.M.A.; Geisler, T.; Kruk, M.B.P.; Alkadhi, H.; Kitagawa, K.; Vliegenthart, R.; Hell, M.M.; Hausleiter, J.; Nguyen, P.K.; Budde, R.P.; et al. Dynamic Myocardial Perfusion CT for the Detection of Hemodynamically Significant Coronary Artery Disease. JACC Cardiovasc. Imaging 2022, 15, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.A.; Fonte, T.A.; Min, J.K. Computational Fluid Dynamics Applied to Cardiac Computed Tomography for Noninvasive Quantification of Fractional Flow Reserve. J. Am. Coll. Cardiol. 2013, 61, 2233–2241. [Google Scholar] [CrossRef] [PubMed]
- Nørgaard, B.L.; Leipsic, J.; Gaur, S.; Seneviratne, S.; Ko, B.S.; Ito, H.; Jensen, J.M.; Mauri, L.; De Bruyne, B.; Bezerra, H.; et al. Diagnostic Performance of Noninvasive Fractional Flow Reserve Derived From Coronary Computed Tomography Angiography in Suspected Coronary Artery Disease: The NXT Trial (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps). J. Am. Coll. Cardiol. 2014, 63, 1145–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Tang, X.; Peng, L.; Luo, Y.; Dong, R.; Liu, J. The diagnostic performance of CT-derived fractional flow reserve for evaluation of myocardial ischaemia confirmed by invasive fractional flow reserve: A meta-analysis. Clin. Radiol. 2015, 70, 476–486. [Google Scholar] [CrossRef] [PubMed]
- A Fairbairn, T.A.; Nieman, K.; Akasaka, T.; Nørgaard, B.L.; Berman, D.S.; Raff, G.; Hurwitz-Koweek, L.M.; Pontone, G.; Kawasaki, T.; Sand, N.P.; et al. Real-world clinical utility and impact on clinical decision-making of coronary computed tomography angiography-derived fractional flow reserve: Lessons from the ADVANCE Registry. Eur. Heart J. 2018, 39, 3701–3711. [Google Scholar] [CrossRef] [Green Version]
- Fairbairn, T.A.; Dobson, R.; Hurwitz-Koweek, L.; Matsuo, H.; Norgaard, B.L.; Rønnow Sand, N.P.; Nieman, K.; Bax, J.J.; Pontone, G.; Raff, G.; et al. Sex Differences in Coronary Computed Tomography Angiography–Derived Fractional Flow Reserve: Lessons From ADVANCE. JACC Cardiovasc. Imaging 2020, 13, 2576–2587. [Google Scholar] [CrossRef]
- Kim, H.-S.; Tonino, P.A.L.; De Bruyne, B.; Yong, A.S.C.; Tremmel, J.A.; Pijls, N.H.J.; Fearon, W.F. The Impact of Sex Differences on Fractional Flow Reserve–Guided Percutaneous Coronary Intervention: A FAME (Fractional Flow Reserve versus Angiography for Multivessel Evaluation) Substudy. JACC Cardiovasc. Interv. 2012, 5, 1037–1042. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.G.; Raju, R.; Blanke, P.; Yang, T.-H.; Mancini, G.B.J.; Budoff, M.J.; Norgaard, B.L.; Min, J.K.; Letipsic, J.A. Diagnostic accuracy and discrimination of ischemia by fractional flow reserve CT using a clinical use rule: Results from the Determination of Fractional Flow Reserve by Anatomic Computed Tomographic Angiography study. J. Cardiovasc. Comput. Tomogr. 2015, 9, 120–128. [Google Scholar] [CrossRef] [Green Version]
- Tweet, M.S.; Akhtar, N.J.; Hayes, S.N.; Best, P.J.; Gulati, R.; Araoz, P.A. Spontaneous coronary artery dissection: Acute findings on coronary computed tomography angiography. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 467–475. [Google Scholar] [CrossRef]
- Tweet, M.S.; Gulati, R.; Williamson, E.E.; Vrtiska, T.J.; Hayes, S.N. Multimodality Imaging for Spontaneous Coronary Artery Dissection in Women. JACC Cardiovasc. Imaging 2016, 9, 436–450. [Google Scholar] [CrossRef]
- Min James, K.; Dunning, A.; Lin Fay, Y.; Achenbach, S.; Al-Mallah, M.; Budoff Matthew, J.; Cademartiri, F.; Callister, T.Q.; Chang, H.J.; Cheng, V.; et al. Age- and Sex-Related Differences in All-Cause Mortality Risk Based on Coronary Computed Tomography Angiography Findings. J. Am. Coll. Cardiol. 2011, 58, 849–860. [Google Scholar]
- Lu, M.T.; Douglas, P.S.; Udelson, J.E.; Adami, E.; Ghoshhajra, B.B.; Picard, M.H.; Roberts, R.; Lee, K.L.; Einstein, A.J.; Mark, D.B.; et al. Safety of coronary CT angiography and functional testing for stable chest pain in the PROMISE trial: A randomized comparison of test complications, incidental findings, and radiation dose. J. Cardiovasc. Comput. Tomogr. 2017, 11, 373–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vadvala, H.; Kim, P.; Mayrhofer, T.; Pianykh, O.; Kalra, M.; Hoffmann, U.; Ghoshhajra, B. Coronary CTA using scout-based automated tube potential and current selection algorithm, with breast displacement results in lower radiation exposure in females compared to males. Cardiovasc. Diagn. Ther. 2014, 4, 470–479. [Google Scholar]
- Patel, A.R.; Salerno, M.; Kwong, R.Y.; Singh, A.; Heydari, B.; Kramer, C.M. Stress Cardiac Magnetic Resonance Myocardial Perfusion Imaging: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2021, 78, 1655–1668. [Google Scholar] [CrossRef] [PubMed]
- Thomson, L.E.J.; Wei, J.; Agarwal, M.; Haft-Baradaran, A.; Shufelt, C.; Mehta, P.K.; Gill, E.B.; Johnson, B.D.; Kenkre, T.; Handberg, E.M.; et al. Cardiac Magnetic Resonance Myocardial Perfusion Reserve Index Is Reduced in Women with Coronary Microvascular Dysfunction. Circ. Cardiovasc. Imaging 2015, 8, e002481. [Google Scholar] [CrossRef] [Green Version]
- Woolen, S.A.; Shankar, P.R.; Gagnier, J.J.; Maceachern, M.P.; Singer, L.; Davenport, M.S. Risk of Nephrogenic Systemic Fibrosis in Patients with Stage 4 or 5 Chronic Kidney Disease Receiving a Group II Gadolinium-Based Contrast Agent. JAMA Intern. Med. 2020, 180, 223. [Google Scholar] [CrossRef]
- Schwitter, J.; Wacker, C.M.; Wilke, N.; Al-Saadi, N.; Sauer, E.; Huettle, K.; Schönberg, S.O.; Luchner, A.; Strohm, O.; Ahlstrom, H.; et al. MR-IMPACT II: Magnetic Resonance Imaging for Myocardial Perfusion Assessment in Coronary artery disease Trial: Perfusion-cardiac magnetic resonance vs. single-photon emission computed tomography for the detection of coronary artery disease: A comparative. Eur. Heart J. 2013, 34, 775–781. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, J.P.; Maredia, N.; Younger, J.F.; Brown, J.M.; Nixon, J.; Everett, C.C.; Bijsterveld, P.; Ridgway, J.P.; Radjenovic, A.; Dickinson, C.J.; et al. Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CE-MARC): A prospective trial. Lancet 2012, 379, 453–460. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, J.P.; Motwani, M.; Maredia, N.; Brown, J.M.; Everett, C.C.; Nixon, J.; Bijsterveld, P.; Dickinson, C.J.; Ball, S.G.; Plein, S. Comparison of Cardiovascular Magnetic Resonance and Single-Photon Emission Computed Tomography in Women with Suspected Coronary Artery Disease From the Clinical Evaluation of Magnetic Resonance Imaging in Coronary Heart Disease (CE-MARC) Trial. Circulation 2014, 129, 1129–1138. [Google Scholar] [CrossRef] [Green Version]
- Merkle, N.; Wöhrle, J.; Nusser, T.; Grebe, O.; Spiess, J.; Torzewski, J.; Hombach, V. Diagnostic performance of magnetic resonance first pass perfusion imaging is equally potent in female compared to male patients with coronary artery disease. Clin. Res. Cardiol. 2010, 99, 21–28. [Google Scholar] [CrossRef]
- Klem, I.; Greulich, S.; Heitner, J.F.; Kim, H.; Vogelsberg, H.; Kispert, E.-M.; Ambati, S.R.; Bruch, C.; Parker, M.; Judd, R.M.; et al. Value of Cardiovascular Magnetic Resonance Stress Perfusion Testing for the Detection of Coronary Artery Disease in Women. JACC Cardiovasc. Imaging 2008, 1, 436–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danad, I.; Szymonifka, J.; Twisk, J.W.R.; Norgaard, B.L.; Zarins, C.K.; Knaapen, P.; Min, J.K. Diagnostic performance of cardiac imaging methods to diagnose ischaemia-causing coronary artery disease when directly compared with fractional flow reserve as a reference standard: A meta-analysis. Eur. Heart J. 2016, 38, 991–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho-Filho Otavio, R.; Seabra Luciana, F.; Mongeon, F.-P.; Abdullah Shuaib, M.; Francis Sanjeev, A.; Blankstein, R.; Di Carli, M.F.; Jerosch-Herold, M.; Kwong, R.Y. Stress Myocardial Perfusion Imaging by CMR Provides Strong Prognostic Value to Cardiac Events Regardless of Patient’s Sex. JACC Cardiovasc. Imaging 2011, 4, 850–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smilowitz, N.R.; Mahajan, A.M.; Roe, M.T.; Hellkamp, A.S.; Chiswell, K.; Gulati, M.; Reynolds, H.R. Mortality of Myocardial Infarction by Sex, Age, and Obstructive Coronary Artery Disease Status in the ACTION Registry-GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry-Get with the Guidelines). Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003443. [Google Scholar] [CrossRef]
- Pasupathy, S.; Air, T.; Dreyer, R.P.; Tavella, R.; Beltrame, J.F. Systematic Review of Patients Presenting with Suspected Myocardial Infarction and Nonobstructive Coronary Arteries. Circulation 2015, 131, 861–870. [Google Scholar] [CrossRef] [Green Version]
- Gudenkauf, B.; Hays, A.G.; Tamis-Holland, J.; Trost, J.; Ambinder, D.I.; Wu, K.C.; Arbab-Zadeth, A.; Blumenthal, R.S.; Sharma, G. Role of Multimodality Imaging in the Assessment of Myocardial Infarction with Nonobstructive Coronary Arteries: Beyond Conventional Coronary Angiography. J. Am. Heart Assoc. 2022, 11, e022787. [Google Scholar] [CrossRef]
- Reynolds, H.R.; Srichai, M.B.; Iqbal, S.N.; Slater, J.N.; Mancini, G.B.J.; Feit, F.; Pena-Sing, I.; Axel, L.; Attubato, M.; Yatskar, L.; et al. Mechanisms of Myocardial Infarction in Women without Angiographically Obstructive Coronary Artery Disease. Circulation 2011, 124, 1414–1425. [Google Scholar] [CrossRef]
- Gerbaud, E.; Arabucki, F.; Nivet, H.; Barbey, C.; Cetran, L.; Chassaing, S.; Seguy, B.; Lesimple, A.; Cochet, H.; Montaudon, M.; et al. OCT and CMR for the Diagnosis of Patients Presenting with MINOCA and Suspected Epicardial Causes. JACC Cardiovasc. Imaging 2020, 13, 2619–2631. [Google Scholar] [CrossRef]
- Barker, D.; Mason, G.; Schlosshan, D.; McLoughlin, H.; Tan, L.-B. Maximal exercise testing can be safely used to assess pregnant cardiac patients. Am. J. Obstet. Gynecol. 2005, 193, S80. [Google Scholar] [CrossRef]
- Colletti, P.M.; Lee, K.H.; Elkayam, U. Cardiovascular imaging of the pregnant patient. AJR Am. J. Roentgenol. 2013, 200, 515–521. [Google Scholar] [CrossRef]
- Dorbala, S.; Di Carli, M.F.; Delbeke, D.; Abbara, S.; DePuey, E.G.; Dilsizian, V.; Forrester, J.; Janowitz, W.; Kaufmann, P.A.; Mahmarian, J.; et al. SNMMI/ASNC/SCCT guideline for cardiac SPECT/CT and PET/CT 1.0. J. Nucl. Med. 2013, 54, 1485–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groen, R.S.; Bae, J.Y.; Lim, K.J. Fear of the unknown: Ionizing radiation exposure during pregnancy. Am. J. Obstet. Gynecol. 2012, 206, 456–462. [Google Scholar] [CrossRef]
- Tremblay, E.; Thérasse, E.; Thomassin-Naggara, I.; Trop, I. Quality Initiatives: Guidelines for Use of Medical Imaging during Pregnancy and Lactation. Radiographics 2012, 32, 897–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb, J.A.W.; Thomsen, H.S.; Morcos, S.K. The use of iodinated and gadolinium contrast media during pregnancy and lactation. Eur. Radiol. 2005, 15, 1234–1240. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaine, S.P.; Sharma, G.; Tower-Rader, A.; Botros, M.; Kovell, L.; Parakh, A.; Wood, M.J.; Harrington, C.M. Multimodality Imaging in the Detection of Ischemic Heart Disease in Women. J. Cardiovasc. Dev. Dis. 2022, 9, 350. https://doi.org/10.3390/jcdd9100350
Gaine SP, Sharma G, Tower-Rader A, Botros M, Kovell L, Parakh A, Wood MJ, Harrington CM. Multimodality Imaging in the Detection of Ischemic Heart Disease in Women. Journal of Cardiovascular Development and Disease. 2022; 9(10):350. https://doi.org/10.3390/jcdd9100350
Chicago/Turabian StyleGaine, Sean Paul, Garima Sharma, Albree Tower-Rader, Mina Botros, Lara Kovell, Anushri Parakh, Malissa J. Wood, and Colleen M. Harrington. 2022. "Multimodality Imaging in the Detection of Ischemic Heart Disease in Women" Journal of Cardiovascular Development and Disease 9, no. 10: 350. https://doi.org/10.3390/jcdd9100350