
Cognitive Impairment in Acute Heart Failure: Narrative Review
by
 ,
,
Ioannis Ventoulis
1,* ,
,
Angelos Arfaras-Melainis
2,3,*,
John Parissis
2 and
Eftihia Polyzogopoulou
2 1
Department of Occupational Therapy, University of Western Macedonia, 50200 Ptolemaida, Greece
2
Heart Failure Unit and University Clinic of Emergency Medicine, Attikon University Hospital, National and Kapodistrian University of Athens Medical School, 12462 Athens, Greece
3
Jacobi Medical Center, Albert Einstein College of Medicine, Bronx, NY 10461, USA
*
Authors to whom correspondence should be addressed.
J. Cardiovasc. Dev. Dis. 2021, 8(12), 184; https://doi.org/10.3390/jcdd8120184
Submission received: 20 November 2021
/
Revised: 11 December 2021
/
Accepted: 12 December 2021
/
Published: 14 December 2021
(This article belongs to the Special Issue Understanding Heart Failure Management and Treatment)
Abstract
:Cognitive impairment (CI) represents a common but often veiled comorbidity in patients with acute heart failure (AHF) that deserves more clinical attention. In the AHF setting, it manifests as varying degrees of deficits in one or more cognitive domains across a wide spectrum ranging from mild CI to severe global neurocognitive disorder. On the basis of the significant negative implications of CI on quality of life and its overwhelming association with poor outcomes, there is a compelling need for establishment of detailed consensus guidelines on cognitive screening methods to be systematically implemented in the population of patients with heart failure (HF). Since limited attention has been drawn exclusively on the field of CI in AHF thus far, the present narrative review aims to shed further light on the topic. The underlying pathophysiological mechanisms of CI in AHF remain poorly understood and seem to be multifactorial. Different pathophysiological pathways may come into play, depending on the clinical phenotype of AHF. There is some evidence that cognitive decline closely follows the perturbations incurred across the long-term disease trajectory of HF, both along the time course of stable chronic HF as well as during episodes of HF exacerbation. CI in AHF remains a rather under recognized scientific field that poses many challenges, since there are still many unresolved issues regarding cognitive changes in patients hospitalized with AHF that need to be thoroughly addressed.
1. Introduction
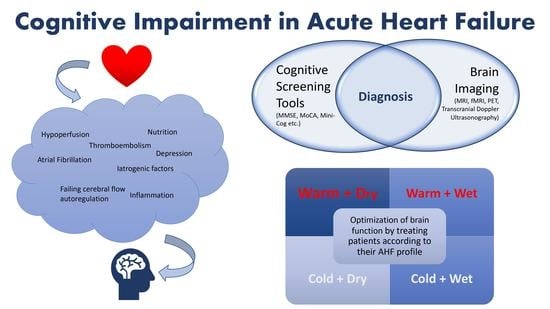
Acute heart failure (AHF) is a heterogeneous clinical syndrome characterized by abrupt onset or gradual deterioration of symptoms and signs of heart failure (HF), in contradiction to chronic HF which represents a state of a much more gradual onset of symptoms or an already established diagnosis of HF [1]. In most cases, AHF manifests as acute decompensated chronic HF and less frequently as de novo HF. On clinical grounds, four distinct phenotypes of AHF can be recognized based on the presence or absence of congestion and peripheral hypoperfusion, namely, warm and wet, cold and wet, warm and dry, and cold and dry [2,3]. AHF remains one of the most common causes of hospital admission in western societies accompanied by high readmission rates and accounting for considerable in-hospital and post-discharge mortality [3,4,5,6]. It constitutes a tremendous and growing public health issue which imposes a substantial economic burden on the healthcare systems worldwide [7,8,9].
AHF can lead to dysfunction, injury, and eventually failure of many vital organs, which in turn contributes to further increase in the observed mortality. The brain represents one of the target organs involved in this process [10]. The heart and the brain are closely linked and interact bidirectionally through numerous feedback pathways [11]. Owing to the complex pathophysiological interplay between the heart and the brain, the notion of the cardiocerebral syndrome in HF has emanated, along the lines of the cardiorenal and the cardiohepatic syndrome [12].
In fact, the close interaction between the heart and the brain has long been recognized, dating back to 1977 where the term ‘’cardiogenic dementia’’ was introduced to describe the cognitive deterioration observed in patients with heart disease [13]. Nowadays, cognitive impairment (CI) is a well-established entity among patients with HF, encountered across a wide range of clinical presentations, that is both acute and stable chronic HF with either reduced or preserved ejection fraction [14]. CI is an inclusive term used to describe any kind of deficit in one or more cognitive domains, the extent of which cannot be attributed to the expected normal decline due to aging. In the AHF setting, a wide spectrum of CI can be encountered, spanning from mild CI to severe global neurocognitive disorder [14,15,16,17].
The negative consequences of CI cannot be overstated, bearing in mind that CI has been linked to poor medical adherence [18], low abidance to recommended lifestyle behaviors [19], and deficits in self-care [20]. Even mild CI may have a significant negative impact on quality of life by affecting important aspects of everyday living and by interfering with self-care management, which is considered a crucial component for the successful treatment of HF [21,22,23]. Moreover, poor self-care has been shown to be an independent risk factor for cardiac events, HF hospitalizations, and increased length of hospital stay [24]. More importantly, in HF patients, CI has been associated with an increased risk of cardiovascular events [25]. In hospitalized patients with AHF, CI has proven to be an independent prognostic marker of in-hospital mortality, prompting approximately a 5-fold increase in mortality [26].
The majority of the research studies examining the scope of CI in HF have included stable HF patients, while the reviews on the topic have made no discrimination between chronic stable and acute HF. Studies dealing with CI in AHF are rather limited. Here, we focus on the association between AHF and CI, review the screening approach towards HF-induced brain injury, outline aspects of epidemiology, explore potential pathogenic mechanisms in AHF that may underlie and predispose to the development of CI, describe the dynamic changes of CI during an episode of AHF, highlight the role of brain imaging modalities in the assessment of CI, and propose a therapeutic approach.
2. Cognitive Screening Tools
During the application of a cognitive screening test, the patient is requested to carry out a series of tasks that assess one or more cognitive domains [27]. Commonly evaluated cognitive domains include memory (immediate and delayed, episodic and semantic), attention/concentration, working memory, visuospatial/constructional ability, executive function, perceptual motor function/psychomotor speed, learning, speech/language, orientation, and social cognition [27,28,29,30,31]. A vast array of brief screening tests for CI is available for use in different clinical settings. These include the Mini Mental State Examination (MMSE), the Montreal Cognitive Assessment (MoCA), the Mini-Cog Test, the Clock Drawing Test (CDT), the Abbreviated Mental Test (AMT), the Short Portable Mental Status Questionnaire (SPMSQ), the St. Louis University Mental Status Examination (SLUMS), the Memory Impairment Screen (MIS)/ MIS by Telephone (MIS-T), the Free and Cued Selective Reminding Test, the 7-Minute Screen (7MS), the Telephone Instrument for Cognitive Status (TICS), the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE), the 8-Item Informant Interview (AD8), the Functional Activities Questionnaire (FAQ), and others [27]. It has to be emphasized that the aforementioned cognitive tests serve as screening tools and are not intended for diagnostic purposes. Once a screening test turns out positive, further clinical assessment and comprehensive neuropsychological evaluation is warranted to formally confirm the diagnosis of CI [27,32]. Nevertheless, one should always keep in mind that when assessing cognitive status, a number of possible confounding factors should be taken into account, such as age, mood disorders, education, employment status, ethnicity, linguistic diversity, and cultural and socioeconomical background [33,34,35,36]. Subsequently, neurocognitive test batteries, even more so cognitive screening tests, need to compensate for possible confounders in order to be reliable and applicable in an evergrowing cross-cultural diverse population.
In HF studies, a variety of screening tools for CI have been utilized, none of which have been specifically devised for HF patients. The same screening tools have been used interchangeably in all HF clinical settings, that is, both inpatients and outpatients and both stable and acute HF. The most widely used screening instruments in HF literature are the MMSE and the MoCA [30,31,37,38]. Yet, the need for even briefer cognitive screening tests to be applied in a hectic clinical setting led to the development of the Mini-Cog [39,40] and the MoCA 5 min protocol (Mini-MoCA) [41,42]. Some of the most common and brief screening tools for the assessment of CI in HF are illustrated in Table 1.
The MMSE is an instrument measuring global cognition, as it covers several cognitive domains, such as orientation, memory (registration and recall), attention and calculation, language, and visuospatial/constructional skills. It consists of eleven questions or tasks and is based on a scoring system ranging from 0 to 30, with higher scores indicating better cognitive performance. It can be easily applied by lay personnel with very little training and requires about 5–10 min to administer [43]. Its performance is however confounded by age, educational level, literacy status, verbal IQ level, and cultural context [35,44,45,46,47]. It has been also criticized due to its reduced sensitivity to detect mild CI [35,47,48] as well as its limited ability to identify alterations in cognition relating to frontal subcortical executive functions and right hemispheric lesions [35,47,49].
The MoCA is a cognitive screening instrument originally designed to detect mild CI. It assesses eight cognitive domains, namely, attention, concentration, working memory, short-term memory (delayed recall), executive function, language, visuospatial ability, and orientation. It utilizes a scoring system spanning from 0 to 30 and requires approximately 10 min to complete. The higher scores are suggestive of better global cognition. To allow for discrepancies in the educational level, the total final score is adjusted by adding 1 point for those with 12 years of formal education or less [50]. A basic feature of the MoCA is that it incorporates an explicit component of executive function assessment (modified Trail making B task, phonemic fluency task, similarities task through two-item verbal abstraction), which the MMSE lacks [50,51]. However, it has a relatively poor specificity, which renders it of limited use in clinical settings characterized by low base rates of mild CI [52,53].
In head-to-head comparison studies examining the performance of MMSE and MoCA in both HF outpatients [36] and inpatients [54], MoCA outperformed MMSE in terms of identifying early cognitive changes indicative of subtle CI. Subsequently, Hawkins et al. examined the performance of MoCA and MMSE against a comprehensive neuropsychological battery of tests, which assess attention, executive function, memory, and visuospatial ability, in a population of 106 HF outpatients aged 50–85 years. They observed that a MoCA cut-off of <25 yielded 64% sensitivity and 66% specificity, while a cut-off of <28 for the MMSE attained 70% sensitivity and 66% specificity. They concluded that application of both tests led to correct identification of the majority of patients with and without multi-domain CI, albeit both of them failed to properly classify approximately one third of the HF patients [55].
The magnitude and clinical consequences of CI in HF have long been appreciated, considering the fact that the Heart Failure Society of America (HFSA) incorporated in their 2010 practice guidelines the general recommendation to assess patients’ cognitive status and provide additional support in case of CI as part of disease management [56]. The 2016 ESC (European Society of Cardiology) guidelines for the diagnosis and treatment of acute and chronic HF moved a step forward by stating that ‘’Cognitive function can be assessed using the Mini-Mental State Examination or the Montreal cognitive assessment’’, while encouraging patient’s support by a multidisciplinary HF team including a specialist in neurocognitive disorders, along with family and caregivers, in order to optimize HF management and facilitate self-care [2].
To date, there is no disease-specific cognitive measure tool for identifying CI in HF patients. Virtues of an ideal screening measure for CI would be high sensitivity and specificity combined with brevity, reliability, simplicity, ease of administration in routine clinical practice, and ability to capture even mild CI affecting either a single or multiple cognitive domains. Although the most suitable screening tool for CI with optimal sensitivity and specificity, validated in HF populations and tailored for use in clinical practice is yet to be identified, it is imperative for clinicians to be aware of the high prevalence of CI in AHF and its implications and systematically screen for cognitive deficits.
3. Epidemiology
The reported prevalence of CI in AHF varies considerably. Figures ranging from 16% to 80% have been reported in the literature. This observed wide fluctuation in prevalence is attributed to many factors, such as varying definitions of CI, different screening tests deployed, disparate thresholds applied, non-homogeneity of the HF population studied (in terms of age, severity, and type of HF), sample sizes and diverse study design characteristics.
Early reports indicated that the prevalence of CI (determined by MMSE scores <24) in 50 patients ≥60 years old with decompensated HF was 54%, while almost three thirds of the patients seemed to experience signs of CI when a cut-off of CAMCOG score <80 was applied [57]. At the same time, data from an Italian multicenter survey, having enrolled more than 1100 patients admitted to the hospital with HF, revealed that CI, assessed by the Hodkinson Abbreviated Mental Test, was evident in 35% of the patients [26,58]. Later on, Debette et al. reported that some degree of CI was observed in two thirds of the overall population (83) of patients with decompensated HF included in their study. They showed that 61% of them had mild CI (defined as MMSE score ≤28 or ≤26 depending on their educational level), while 31% exhibited overt CI (defined as MMSE score ≤24) [59].
Meanwhile, in a prospective cohort study of 282 patients (mean age 80 years) hospitalized for AHF, CI was present in 46.8% of the overall sample with 25.2% meeting criteria for mild CI (MMSE score 21–24) and 21.6% for moderate–severe CI (MMSE score ≤20) [60]. Similar rates (45%) of at least mild CI (MoCA ≤ 22) were recorded by an Australian study following 565 patients with decompensated HF and a median age of 74 years [61], while the Vanderbilt Inpatient Cohort Study (VICS) reported a comparable degree (53%) of any level of CI (defined as an SPMSQ score ≥1) in 883 patients with AHF and a median age of 60 years [62]. Furthermore, in a study examining the effect of CI on 30-day readmission rates in a population of 241 elderly hospitalized patients (>70 years old), 121 of whom were admitted for HF as the primary diagnosis, it was found that 67.7% of the HF patients had CI defined as Mini-Cog scores of less than 4 [63]. In contrast, the first study to have used the Mini-Cog in 720 patients hospitalized for HF reported a 23% prevalence of CI by using a different cut-off score of ≤2 [39].
A much higher prevalence of CI (79%) in at least one cognitive domain was reported by Hajduk et al. in a cohort of 577 older (average age 71 years) patients with decompensated HF, who were evaluated in three cognitive domains with the use of standardized measures. Specifically, deficits in memory, mental processing speed, and executive function were noted in 33.3%, 40%, and 56% of the HF patients, respectively [64]. An equally high prevalence (80%) of CI was noted in at least one of the three cognitive domains (memory, executive function, processing speed) assessed in a study of 744 patients with acute decompensated HF and a mean age of 72 years. In particular, 32% of the patients demonstrated CI in only one domain, 31% in two domains, and 17% in three domains. Patients exhibited primarily deficits in executive function (59%) and in processing speed (51%) and to a lesser extent in memory (35%) [65].
Recent studies still continue to show discrepancy in the reported rates of CI prevalence. As a matter of fact, a Swedish prospective cohort study including 281 patients hospitalized for HF with an average age of 74 years reported that 29% of them displayed signs of CI based on MoCA scores <23 [66]. Even more so, data from the RICA registry indicated that, amongst 3845 patients (mean age 79 years) hospitalized for decompensated HF, 16% had significant CI (14% moderate and 2% severe CI). In this study, cognitive status was assessed by means of the Short Portable Mental Status Questionnaire (SPMSQ) and the patients were categorized into three groups based on their performance on the particular test: 0–3 errors were considered as no CI or mild CI, 4–7 as moderate CI, and 8–10 as severe CI. By using these cut-offs, there was no discrimination between intact cognition and mild CI and only the prevalence of moderate and severe CI was determined, hence the low prevalence reported by the investigators [67]. On the other hand, the REHAB-HF trial recorded a CI prevalence of 78% among 198 older (≥60 years old) hospitalized patients with acute decompensated HF when a MoCA score <26 was used. Of note, only 2% of these patients were clinically recognized as cognitively impaired [68].
Regardless of the conflicting estimates of its prevalence, CI represents a veiled comorbidity in patients with AHF that deserves more clinical attention, as it is intertwined with significant clinical ramifications and poor health outcomes.
4. Pathophysiology
The pathophysiology behind the induced brain injury in AHF still awaits to be elucidated as the underlying mechanisms are not well understood and seem to be multifactorial. Different pathophysiological mechanisms responsible for the observed brain changes in AHF could be proposed. Depending on the clinical phenotype of AHF, diverse pathophysiological pathways may come into play and exert synergistic effects, since no single mechanism can fully explain the cognitive changes that occur in AHF.
Under normal conditions, cerebral blood flow remains rather stable during wide fluctuations of the mean arterial blood pressure owing to inherent properties that the central nervous system possesses to activate and maintain elaborate vascular and neurohumoral mechanisms of autoregulation [69,70]. However, in HF states, these cerebral neuroprotective autoregulatory mechanisms are blunted, thus compromising cerebral blood flow and jeopardizing the brain’s integrity [71]. Cerebrovascular reactivity is also impaired in HF, as evidenced by the diminished response of the cerebral vasculature to hypercapneic conditions [72].
In the hypoperfused AHF states, the most plausible mechanism seems to be the decreased cerebral blood flow as a result of the reduced cardiac output, leading to inadequate blood supply to the brain and subsequent brain ischaemia [73,74,75]. The effect of the ischaemic assault to the brain is further magnified by the combination of transient mechanisms of hypoperfusion, whereby impaired cardiac performance manifested as low cardiac output acts synergistically with concurrent hypotension to yield a state of cardiogenic shock, which may be particularly detrimental to the brain. Furthermore, it is already known, based on the work of Gheorghiade et al., that systolic blood pressure at admission is an independent prognostic marker of morbidity and mortality in patients hospitalized with AHF and moreover low systolic blood pressure is associated with worse survival [76]. Zuccalà et al. reported that lower levels of systolic blood pressure were independently correlated with CI among older patients hospitalized with HF [77], while Hoth et al. found that systemic hypoperfusion indicated by low EF and low cardiac index was associated with deficits in several cognitive domains among HF patients [78]. Furthermore, other investigators reported a non-linear association between EF and cognitive performance, which became more pronounced at lower levels of EF and was further strengthened in the presence of concomitant hypotension [79]. Studies demonstrating significant cognitive improvement in post-heart transplant patients seem to confirm the hypothesis that systemic hypoperfusion due to impaired cardiac function is a principal causative factor of CI in HF [80,81]. Similarly, other studies noted that amelioration of cardiac function after cardiac resynchronization therapy was accompanied with improvements in cerebral blood flow and cognition [82,83]. Additionally, a study conducted in geriatric cardiac patients revealed that depressed cardiac output was associated with poorer cognitive performance in the domain of executive function [84]. Further support for the role of hypoperfusion in the pathophysiology of CI in HF is provided by imaging methods. Early reports exist even from the previous century stating that cerebral blood flow (estimated by the intravenous 133xenon injection method) is reduced in patients with severe HF [85]. Likewise, in patients with severe HF who were candidates for cardiac transplantation, cerebral blood flow estimated by single-photon emission computed tomography was decreased by approximately 30% at baseline, but interestingly it was restored within one month after heart transplantation [86]. A more recent study in HF patients, using transcranial Doppler ultrasound and brain magnetic resonance imaging, showed that reduced cerebral blood flow was associated with a greater degree of white matter hyperintensities and poorer cognitive performance [87].
Atrial fibrillation, which often complicates AHF, can further exacerbate CI. Indeed, atrial fibrillation can compromise cerebral perfusion by reducing systemic cardiac output via increased heart rate and reduced left ventricular systolic performance. It can also induce CI through alternative mechanisms, such as cerebral thromboembolism or cerebral microbleeds [88]. The phenomenon of the ischaemic insult to the brain may be further aggravated by the presence of multiple risk factors often found in HF patients and adding to the total cardiovascular risk burden. These risk factors include advanced age [89], arterial hypertension [90,91], diabetes mellitus [91,92], smoking [93], and obstructive sleep apnea [94], among others. Hyperhomocysteinaemia has also been associated with an increased risk for major neurocognitive disorders [95].
From a cellular point of view, cerebral hypoperfusion reduces the delivery of glucose and oxygen to the central nervous system. The deprivation of the brain’s main energy substrate and the resultant hypoxia lead to structural cellular changes of the neurons, alterations in the neuronal metabolism and disruption of the continuity of the blood–brain barrier. The energy shortage along with the established hypoxic conditions render the neurons susceptible to oxidative stress, inducing increased production of free radicals, ineffective protein handling, neuronal dysfunction, increased permeability of the blood–brain barrier, and oedema [96,97,98].
In the setting of hypertensive AHF, the elevated blood pressure results in an abrupt increase in cerebral blood flow, which cannot be effectively counterbalanced by appropriate constriction of the central nervous system’s vasculature due to the compromised autoregulatory mechanisms of the brain and the dysfunctional cerebrovascular reactivity [99,100,101]. Once the upper limit of cerebral autoregulation is exceeded, cerebral blood flow can no longer be maintained at a constant level and becomes directly proportional to the mean arterial pressure or, in other words, becomes pressure-passive [101]. When this breakthrough point is reached, segments of vasodilated vessels with alternating areas of vasoconstricted arterioles will be observed, since the loss of cerebrovascular autoregulation will lead to forced dilatation of certain arteriolar segments, while other portions of arterioles will remain physiologically constricted owing to the fact that the autoregulatory mechanism in these specific areas is still intact [101,102,103]. Accordingly, the unopposed abrupt rise in cerebral blood flow and pressure can disrupt the integrity of the endothelium of the brain vessels as well as the function of the blood–brain barrier, potentially leading to cerebral oedema [101,104].
In instances where congestion is the predominant clinical profile of AHF, it could be postulated that venous congestion in the brain may contribute to the development of CI through several different mechanisms. In detail, systemic congestion leads to increased central venous pressure which may then be transmitted backwards to the brain circulation, causing elevated cerebral venous pressure [105]. The phenomenon may be further aggravated by concomitant jugular venous reflux, which was found to be associated with CI when combined with high right atrial pressure [106]. The resultant retrograde increase in the cerebral venous pressure exerts adverse effects on cerebral haemodynamics by impeding cerebral venous return, promoting blood stasis in the brain, and elevating intracranial pressure, thus causing dysregulation of the cerebral perfusion pressure and cerebral blood flow. Moreover, increased cerebral venous pressure may account for the development of cerebral microhemorrhages of venous origin, the genesis of cerebral microinfarcts, the impaired function of the glymphatic system, alterations in the homeostasis of the cerebrospinal fluid, and the development of white matter hyperintensities [105]. In an experimental model of increased cerebral venous pressure, cerebral venous congestion was shown to disrupt the blood–brain barrier, impair blood flow, and promote neuroinflammation via activation of microglia and upregulation of proinflammatory mediators [107]. In other words, increased cerebral venous pressure induces a cascade of processes which have been implicated in the genesis of neuronal dysfunction and the development of CI.
Thromboembolism represents another mechanism through which HF can induce impaired cerebral perfusion. It can manifest either as ischaemic stroke or occult cerebral infarction. HF constitutes a hypercoagulable state, characterized by blood stasis, increased plasma viscosity, enhanced platelet aggregation, increased production of thrombogenic factors, reduced fibrinolysis, and impaired endothelial function. The compromised cardiac performance, in concert with the deranged haemorheological conditions that prevail in HF, promote thrombus formation through activation of the coagulation cascade, ultimately leading to cerebral infarction [108,109].
Apart from the aforementioned haemodynamic mechanisms, several other factors could also contribute to the development of CI in AHF. It is widely accepted that AHF is characterized by a state of excessive activation of the sympathetic nervous system and imbalance of the neurohormonal axis with overproduction of catecholamines and cortisol. Concordantly, there is an exaggerated expression of inflammatory mediators [10]. The undue activation of the neurohormonal system together with the overflow of proinflammatory cytokines exert deleterious effects on the neuronal cells, leading to an energy crisis and metabolic derangement of the neurons [98,110,111]. At the same time, a neurotoxic cascade is triggered, effectuating alterations in the cerebral beta-amyloid metabolism, which in turn generate additive effects by causing further brain insult [98,112].
The role of nutritional deficiencies has also been put forward as a potential mechanism for CI in HF, taking into account the fact that HF commonly induces a state characterized by insufficiency of nutrients via malabsorption, dietary restrictions, and use of certain medications (e.g., diuretics) [113]. As a matter of fact, thiamine deficiency induces oxidative stress and selective neuronal loss, while it has been linked to brain atrophy and white matter changes [114,115]. Along the same lines, iron deficiency, a very common HF comorbidity, has a negative impact on cognitive performance and should thus be treated accordingly [116]. Furthermore, low levels of serum albumin, which is a common finding in HF patients, especially in those with cachexia, have been associated with CI [58].
Moreover, depression seems to be tightly entangled with CI in HF patients and this correlation appears to be bidirectional and cumulative, as the presence of the former appears to deteriorate the latter and vice versa [33]. It has been reported that HF patients with depression have higher levels of proinflammatory cytokines, which have been implicated in the development of CI [117].
Lastly, iatrogenic factors should also not be overlooked. For instance, during treatment of hypertensive AHF, an inadvertent rapid decline in blood pressure could potentially provoke detrimental injury to the brain [118]. Moreover, in patients presenting with AHF, a plethora of factors can predispose the patient to an altered cognitive status, inducing even acute delirium. Such predisposing factors include deteriorating hypoxia [97,98], hypercapnia [119], electrolyte imbalances (e.g., hyponatraemia) [58,120], hypo- or hyper-glycaemia [121], anemia [122], renal [122] or hepatic failure [123], and drugs with anticholinergic properties [124].
5. Trajectory of CI over the Time Course of HF
Recently, a group of investigators attempted to estimate the prevalence of CI among 436 patients with incident HF (mean age 70 years) who were recruited in a prospective longitudinal cohort study (Regards study) evaluating participants at six-month intervals. Cognition was assessed with the Six-Item Screener (SIS) and scores ≤4 indicated CI. Interestingly, cognitive assessment was conducted prior to the incident HF diagnosis, thus reflecting cognition upon initial diagnosis of HF and minimizing any bias of clinical deterioration on cognition induced by the course of HF itself. The prevalence of CI in patients with incident HF (defined as the first hospitalization for HF without a previous history of HF) was 14.9%, being similar to that of a non-HF matched cohort (13.4%). Given the similar rates of CI prevalence between the two studied groups and taking into account the reported prevalence of CI in patients with already existing chronic HF (25–80%), the authors concluded that the highest burden of CI in HF develops after the HF diagnosis during the progression of the disease itself [125].
Once HF develops, further cognitive decline ensues, which parallels the duration and severity of HF. In line with this, Hammond et al. conducted a longitudinal analysis in the Cardiovascular Health Study concerning the time course of CI after newly diagnosed HF. The study included 4864 participants aged ≥65 years with a long follow-up. During a mean follow-up of 6.4 years, 496 patients with incident HF were identified. Cognitive performance was assessed annually using the 100-point Modified Mini-Mental State Examination (3MSE) and model-predicted trajectories of mean 3MSE scores were formulated for both study groups (no history of HF and after incident HF) and for different age groups. The investigators noted that the rate of cognitive decline was markedly faster after incident HF, compared to subjects with no HF, and the deterioration in cognition was much more pronounced at older ages. Remarkably, the rate of cognitive decline after incident HF was not significantly affected neither by atrial fibrillation status nor by EF category [126].
Likewise, secondary data analysis from the ACTIVE study indicated that patients with HF exhibit more rapid decline in cognitive function longitudinally (over a five-year period), albeit limited only to the cognitive domain of reasoning [127]. Along the same lines, a prospective longitudinal study on cognitive changes over a 10-year period of follow-up among 702 octogenarians with and without HF detected greater rates of cognitive decline in the field of episodic memory over time in those with HF [128].
On the other hand, in another longitudinal study, despite observing relative decline in global cognitive function of stable HF patients over a time period of two years compared to healthy controls, the investigators considered these cognitive changes to be subtle and not specific to HF when comparing them to patients with coronary artery disease [129]. Similarly, the TIME-CHF trial following 611 HF patients aged ≥60 years failed to detect significant changes in cognitive function in relation to changes in HF severity over a period of 18 months, since the prevalence of severe CI (defined as Hodkinson Abbreviated Mental Test score ≤7) remained rather stable over time. Yet, it is noteworthy that there was a significant rate of patient drop out with approximately two-thirds of those with severe CI at baseline being unavailable for follow-up assessment, which should be considered a major confounder [130]. On top of this, other researchers actually reported modest improvement in certain cognitive fields of patients with HF followed for a period of 12 months, highlighting that cognitive dysfunction in HF is not necessarily universal and could be potentially modifiable. However, there may have been a selection bias in this survey by not covering the full spectrum of HF patients (mild forms of HF patients who most probably abide by their medical regimens may have predominated) and by excluding patients with MMSE < 24. Moreover, the sample of HF patients was relatively small with an intermediate-term follow-up [131].
In acute decompensated HF it would be intriguing to assess the changes in cognitive function during the time window immediately after admission to the hospital (acute phase) up to the time point where full compensation has been achieved (compensated phase). This issue was addressed by Kindermann et al. in the CogImpair-HF study which examined the cognitive performance of 20 patients with decompensated HF before (within 48 h after admission) and after (14 ± 7 days) compensation in comparison to 20 patients with stable HF and 20 healthy controls. As expected, initially, patients with decompensated HF performed substantially worse than the other two groups, especially in the domains of memory, executive control, and processing speed, but once the compensated phase was reached, improvements were noted in their cognitive performance approaching the level of patients with stable HF [132].
Despite the paucity of longitudinal studies with an extensive follow-up, some evidence exists that cognitive decline closely pursues the perturbations incurred across the long-term disease trajectory of HF. The presumed longitudinal relationship between CI and HF is graphically depicted in Figure 1.
6. Role of Brain Imaging Modalities
Neuroimaging studies conducted in HF patients have documented structural abnormalities in several brain regions involved in cognition. Morphologic cerebral abnormalities, including cortical atrophy, ventricular enlargement, and cerebral infarcts, have been recognized long ago through brain magnetic resonance imaging (MRI) in HF patients with idiopathic dilated cardiomyopathy and have been related to worse cognitive performance [133]. More recent studies in HF patients have demonstrated regional volume reductions across certain brain cognitive areas, such as the hippocampus [134], the mammillary bodies [135], and the putamen [136]. Furthermore, another study showed reduced regional cortical thickness across multiple brain sites that control various high-level and autonomic functions. The observed findings reflect loss of neurons and supporting glial cells and exhibit lateralization, with the cortical thinning being more pronounced on the left side [137]. Almeida et al. found that HF patients demonstrated a higher burden of grey matter lesions, which were more extensive but with a similar pattern of topographic distribution, compared to patients with ischaemic heart disease [138].
With the use of 99 mTc-single-photon emission computed tomography (SPECT), regional cerebral blood flow was evaluated in HF patients and, when compared to controls, blood flow was found reduced in certain posterior cortical areas and was directly correlated to the degree of CI [139]. Subsequently, the same investigators supported that the regional cerebral blood flow abnormalities detected in HF patients resemble the regional patterns of functional brain deficits depicted in positron emission tomography (PET) imaging studies of glucose metabolism or amyloid deposition at the early stages of Alzheimer’s disease [140].
The aforementioned finding of regional cerebral hypoperfusion is in accordance with another study of HF patients reporting a significant reduction in cerebral blood flow, as estimated by 133Xe-SPECT, pre-transplant, which was consequently reversed following transplantation [86]. Accordingly, Alosco et al. recruited 69 HF patients who underwent brain MRI, transcranial Doppler ultrasonography of the middle cerebral artery, and cognitive assessment via the MMSE. They found that reduced cerebral blood flow was associated with greater white matter hyperintensities in older adults with HF [87]. In an attempt to further differentiate white matter injury into axonal versus myelin lesions, other investigators applied an MRI technique called diffusion tensor imaging to HF patients and reported both axonal and myelin injury, as evidenced by increased axial and radial diffusivity, respectively. The injury, comprising of either loss of axonal integrity or myelin breakdown or a combination of both, was evident along several fiber pathways in the brain, including cognitive circuits, such as fibers projecting to the limbic system, the thalamus, and the basal ganglia [141].
In order to relate neuroanatomical alterations in the grey and white matter with cerebral metabolic changes that occur in certain cognitive areas of the brain, additional studies are warranted in HF patients, ideally with the application of more sophisticated imaging modalities, such as 18F-FDG PET, amyloid PET imaging, functional MRI, and magnetic resonance spectroscopy [142,143,144,145].
7. Therapeutic Strategy
Once CI has been recognized, every effort should be made to limit its consequences by applying therapies that minimize or reverse brain injury. The main pillar of our therapeutic strategy should aim at preventing any subsequent CI, while effectively managing AHF. Of paramount importance is the prompt restoration of central haemodynamics, which will allow the stabilization of the patient with AHF. Any underlying comorbidities should also be addressed accordingly. In the AHF setting, any reversible cause of altered mental status should be systematically sought and immediately corrected [146].
It needs to be emphasized that there is no particular therapeutic intervention available for prevention and management of CI in AHF. In order to provide and ensure brain protection, the currently suggested approach is to abide by the recommendations provided by the clinical practice HF guidelines [1]. For the time being, applying optimal evidence-based medical treatment specifically tailored to each clinical profile of AHF, as per guidelines, should suffice. The proposed therapeutic approach, targeted at preventing CI and protecting the brain, depends on the AHF clinical phenotype and is presented in Figure 2.
8. Conclusions
While the exact pathophysiological mechanisms remain poorly understood and still need to be clarified, the evidence regarding the presence and burden of CI in AHF has been well established. Caution must be exercised given the fact that CI in AHF patients often goes unrecognized in the clinical setting. Most of the time, cognitive changes are subtle and may easily be overlooked by the clinician unless routinely scrutinized. Considering the overwhelming association of CI with poor outcomes, screening for CI has been recommended by HF guidelines, but unfortunately the scientific committees still omit to specify when and how to screen. Consequently, it is more than obvious that there is a compelling need for establishment of detailed consensus guidelines on cognitive screening methods to be systematically implemented in the population of patients with HF in the context of a more integrated approach.
Undoubtedly, more well-designed trials are needed to precisely delineate the longitudinal effects that HF exerts on cognitive function both over the time course of stable chronic HF as well as during episodes of HF exacerbation. There are still many unresolved issues regarding cognitive changes in patients hospitalized with AHF that need to be thoroughly addressed in the future. CI in AHF remains a rather undiscovered and under recognized scientific field that poses many challenges and awaits to be unraveled by future investigators.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Kurmani, S.; Squire, I. Acute Heart Failure: Definition, Classification and Epidemiology. Curr. Hear. Fail. Rep. 2017, 14, 385–392. [Google Scholar] [CrossRef] [Green Version]
- Arrigo, M.; Jessup, M.; Mullens, W.; Reza, N.; Shah, A.M.; Sliwa, K.; Mebazaa, A. Acute heart failure. Nat. Rev. Dis. Primers 2020, 6, 16. [Google Scholar] [CrossRef]
- Sinnenberg, L.; Givertz, M.M. Acute heart failure. Trends Cardiovasc. Med. 2020, 30, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Alla, F.; Zannad, F.; Filippatos, G. Epidemiology of acute heart failure syndromes. Hear. Fail. Rev. 2007, 12, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.C.; Ikonomidis, J.S.; Khavjou, O.; Konstam, M.A.; Maddox, T.M.; et al. Forecasting the impact of heart failure in the United States: A policy statement from the American Heart Association. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [CrossRef] [Green Version]
- Weintraub, N.L.; Collins, S.P.; Pang, P.S.; Levy, P.D.; Anderson, A.S.; Arslanian-Engoren, C.; Gibler, W.B.; McCord, J.K.; Parshall, M.B.; Francis, G.S.; et al. Acute heart failure syndromes: Emergency department presentation, treatment, and disposition: Current approaches and future aims: A scientific statement from the American Heart Association. Circulation 2010, 122, 1975–1996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N.; et al. The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef]
- Harjola, V.-P.; Mullens, W.; Banaszewski, M.; Bauersachs, J.; Brunner-La Rocca, H.P.; Chioncel, O.; Collins, S.P.; Doehner, W.; Filippatos, G.S.; Flammer, A.J.; et al. Organ dysfunction, injury and failure in acute heart failure: From pathophysiology to diagnosis and management. A review on behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2017, 19, 821–836. [Google Scholar] [CrossRef] [PubMed]
- Scherbakov, N.; Doehner, W. Heart–brain Interactions in Heart Failure. Card. Fail. Rev. 2018, 4, 87–91. [Google Scholar] [CrossRef]
- Havakuk, O.; King, K.; Grazette, L.; Yoon, A.J.; Fong, M.; Bregman, N.; Elkayam, U.; Kloner, R.A. Heart Failure-Induced Brain Injury. J. Am. Coll. Cardiol. 2017, 69, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Cardiogenic Dementia. Lancet 1977, 1, 27–28. [CrossRef]
- Alagiakrishnan, K.; Mah, D.; Ahmed, A.; Ezekowitz, J. Cognitive decline in heart failure. Hear. Fail. Rev. 2016, 21, 661–673. [Google Scholar] [CrossRef]
- Knopman, D.S.; Petersen, R.C. Mild Cognitive Impairment and Mild Dementia: A Clinical Perspective. Mayo Clin. Proc. 2014, 89, 1452–1459. [Google Scholar] [CrossRef] [Green Version]
- Uthamalingam, S.; Gurm, G.S.; Daley, M.; Flynn, J.; Capodilupo, R. Usefulness of Acute Delirium as a Predictor of Adverse Outcomes in Patients >65 Years of Age with Acute Decompensated Heart Failure. Am. J. Cardiol. 2011, 108, 402–408. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Hawkins, L.A.; Kilian, S.; Firek, A.; Kashner, T.M.; Firek, C.J.; Silvet, H. Cognitive impairment and medication adherence in outpatients with heart failure. Hear. Lung 2012, 41, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Alosco, M.L.; Spitznagel, M.B.; van Dulmen, M.; Raz, N.; Cohen, R.; Sweet, L.H.; Colbert, L.H.; Josephson, R.; Hughes, J.; Rosneck, J.; et al. Cognitive Function and Treatment Adherence in Older Adults With Heart Failure. Psychosom. Med. 2012, 74, 965–973. [Google Scholar] [CrossRef] [Green Version]
- Currie, K.; Rideout, A.; Lindsay, G.; Harkness, K. The Association Between Mild Cognitive Impairment and Self-care in Adults With Chronic Heart Failure: A Systematic Review and Narrative Synthesis. J. Cardiovasc. Nurs. 2015, 30, 382–393. [Google Scholar] [CrossRef] [Green Version]
- Cameron, J.; Worrall-Carter, L.; Page, K.; Riegel, B.; Lo, S.K.; Stewart, S. Does cognitive impairment predict poor self-care in patients with heart failure? Eur. J. Hear. Fail. 2010, 12, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Harkness, K.; Heckman, G.; Akhtar-Danesh, N.; Demers, C.; Gunn, E.; McKelvie, R.S. Cognitive function and self-care management in older patients with heart failure. Eur. J. Cardiovasc. Nurs. 2014, 13, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Hjelm, C.M.; Broström, A.; Riegel, B.; Årestedt, K.; Strömberg, A. The association between cognitive function and self-care in patients with chronic heart failure. Hear. Lung 2015, 44, 113–119. [Google Scholar] [CrossRef]
- Kato, N.P.; Kinugawa, K.; Nakayama, E.; Tsuji, T.; Kumagai, Y.; Imamura, T.; Maki, H.; Shiga, T.; Hatano, M.; Yao, A.; et al. Insufficient Self-Care Is an Independent Risk Factor for Adverse Clinical Outcomes in Japanese Patients With Heart Failure. Int. Hear. J. 2013, 54, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Gelow, J.M.; Mudd, J.O.; Chien, C.V.; Lee, C.S. Usefulness of Cognitive Dysfunction in Heart Failure to Predict Cardiovascular Risk at 180 Days. Am. J. Cardiol. 2015, 115, 778–782. [Google Scholar] [CrossRef] [Green Version]
- Zuccalà, G.; Pedone, C.; Cesari, M.; Onder, G.; Pahor, M.; Marzetti, E.; Monaco, R.L.; Cocchi, A.; Carbonin, P.; Bernabei, R. The effects of cognitive impairment on mortality among hospitalized patients with heart failure. Am. J. Med. 2003, 115, 97–103. [Google Scholar] [CrossRef]
- Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W., Jr.; Kubik, M.; Landefeld, C.S.; et al. Screening for Cognitive Impairment in Older Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2020, 323, 757–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leto, L.; Feola, M. Cognitive impairment in heart failure patients. J. Geriatr. Cardiol. 2014, 11, 316–328. [Google Scholar] [CrossRef] [PubMed]
- Dardiotis, E.; Giamouzis, G.; Mastrogiannis, D.; Vogiatzi, C.; Skoularigis, J.; Triposkiadis, F.; Hadjigeorgiou, G.M. Cognitive Impairment in Heart Failure. Cardiol. Res. Pract. 2012, 2012, 1–9. [Google Scholar] [CrossRef]
- Davis, K.K.; Allen, J.K. Identifying cognitive impairment in heart failure: A review of screening measures. Hear. Lung 2013, 42, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Bauer, L.C.; Johnson, J.K.; Pozehl, B.J. Cognition in heart failure: An overview of the concepts and their measures. J. Am. Acad. Nurse Pract. 2011, 23, 577–585. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Sohani, Z.N.; Samaan, Z. Does depression impact cognitive impairment in patients with heart failure? Cardiol. Res. Pract. 2012, 2012, 524325. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.C.; Moore, T.M.; Stein, D.J.; Pretorius, A.; Zingela, Z.; Nagdee, M.; Ngqengelele, L.; Campbell, M.; Sibeko, G.; King, M.C.; et al. Adaptation and validation of a computerized neurocognitive battery in the Xhosa of South Africa. Neuropsychology 2021, 35, 581–594. [Google Scholar] [CrossRef]
- Devenney, E.; Hodges, J.R. The Mini-Mental State Examination: Pitfalls and limitations. Pract. Neurol. 2017, 17, 79–80. [Google Scholar] [CrossRef]
- Athilingam, P.; King, K.B.; Burgin, S.W.; Ackerman, M.; Cushman, L.A.; Chen, L. Montreal Cognitive Assessment and Mini-Mental Status Examination compared as cognitive screening tools in heart failure. Hear. Lung 2011, 40, 521–529. [Google Scholar] [CrossRef]
- Cameron, J.; Kure, C.E.; Pressler, S.J.; Ski, C.F.; Clark, A.M.; Thompson, D.R. Diagnostic Accuracy of Cognitive Screening Instruments in Heart Failure: A Systematic Review. J. Cardiovasc. Nurs. 2016, 31, 412–424. [Google Scholar] [CrossRef] [PubMed]
- Cameron, J.; Gallagher, R.; Pressler, S.J. Detecting and Managing Cognitive Impairment to Improve Engagement in Heart Failure Self-Care. Curr. Hear. Fail. Rep. 2017, 14, 13–22. [Google Scholar] [CrossRef]
- Patel, A.; Parikh, R.; Howell, E.H.; Hsich, E.; Landers, S.H.; Gorodeski, E.Z. Mini-cog performance: Novel marker of post discharge risk among patients hospitalized for heart failure. Circ. Heart Fail. 2015, 8, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Borson, S.; Scanlan, J.; Brush, M.; Vitaliano, P.; Dokmak, A. The mini-cog: A cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int. J. Geriatr. Psychiatry 2000, 15, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Nyenhuis, D.; Black, S.E.; Law, L.S.; Lo, E.S.; Kwan, P.W.; Au, L.; Chan, A.Y.; Wong, L.K.; Nasreddine, Z.; et al. Montreal Cognitive Assessment 5-Minute Protocol Is a Brief, Valid, Reliable, and Feasible Cognitive Screen for Telephone Administration. Stroke 2015, 46, 1059–1064. [Google Scholar] [CrossRef] [Green Version]
- Cameron, J.D.; Gallagher, R.; Pressler, S.J.; McLennan, S.N.; Ski, C.F.; Tofler, G.; Thompson, D.R. Sensitivity and Specificity of a Five-Minute Cognitive Screening Test in Patients With Heart Failure. J. Card. Fail. 2016, 22, 99–107. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Anthony, J.C.; LeResche, L.; Niaz, U.; Von Korff, M.R.; Folstein, M.F. Limits of the ‘Mini-Mental State’ as a screening test for dementia and delirium among hospital patients. Psychol. Med. 1982, 12, 397–408. [Google Scholar] [CrossRef]
- O’connor, D.W.; Pollitt, P.A.; Hyde, J.B.; Fellows, J.L.; Miller, N.D.; Brook, C.P.B.; Reiss, B.B. The reliability and validity of the Mini-Mental State in a British community survey. J. Psychiatr. Res. 1989, 23, 87–96. [Google Scholar] [CrossRef]
- Brayne, C. The mini-mental state examination, will we be using it in 2001? Int. J. Geriatr. Psychiatry 1998, 13, 285–290. [Google Scholar] [CrossRef]
- Naugle, R.I.; Kawczak, K. Limitations of the Mini-Mental State Examination. Clevel. Clin. J. Med. 1989, 56, 277–281. [Google Scholar] [CrossRef]
- Mitchell, A.J. A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J. Psychiatr. Res. 2009, 43, 411–431. [Google Scholar] [CrossRef]
- Folstein, M. Mini-mental and son. Int. J. Geriatr. Psychiatry 1998, 13, 290–294. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Ismail, Z.; Rajji, T.K.; Shulman, K.I. Brief cognitive screening instruments: An update. Int. J. Geriatr. Psychiatry 2010, 25, 111–120. [Google Scholar] [CrossRef]
- McLennan, S.; Mathias, J.; Brennan, L.; Stewart, S. Validity of the Montreal Cognitive Assessment (MoCA) as a Screening Test for Mild Cognitive Impairment (MCI) in a Cardiovascular Population. J. Geriatr. Psychiatry Neurol. 2011, 24, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Coen, R.F.; Cahill, R.; Lawlor, B.A. Things to watch out for when using the Montreal cognitive assessment (MoCA). Int. J. Geriatr. Psychiatry 2011, 26, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Cameron, J.; Worrall-Carter, L.; Page, K.N.; Stewart, S.; Ski, C. Screening for mild cognitive impairment in patients with heart failure: Montreal Cognitive Assessment versus Mini Mental State Exam. Eur. J. Cardiovasc. Nurs. 2013, 12, 252–260. [Google Scholar] [CrossRef]
- Hawkins, M.A.; Gathright, E.C.; Gunstad, J.; Dolansky, M.A.; Redle, J.D.; Josephson, R.; Moore, S.M.; Hughes, J.W. The MoCA and MMSE as screeners for cognitive impairment in a heart failure population: A study with comprehensive neuropsychological testing. Hear. Lung 2014, 43, 462–468. [Google Scholar] [CrossRef] [Green Version]
- Lindenfeld, J.; Albert, N.M.; Boehmer, J.P.; Collins, S.P.; Ezekowitz, J.A.; Givertz, M.M.; Katz, S.D.; Klapholz, M.; Moser, D.K.; Rogers, J.G.; et al. HFSA 2010 Comprehensive Heart Failure Practice Guideline. J. Card. Fail. 2010, 16, e1–e194. [Google Scholar] [CrossRef]
- Almeida, O.P.; Tamai, S. Congestive heart failure and cognitive functioning amongst older adults. Arq. De Neuro-Psiquiatr. 2001, 59, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Zuccalà, G.; Marzetti, E.; Cesari, M.; Monaco, M.R.L.; Antonica, L.; Cocchi, A.; Carbonin, P.; Bernabei, R. Correlates of cognitive impairment among patients with heart failure: Results of a multicenter survey. Am. J. Med. 2005, 118, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Debette, S.; Bauters, C.; Leys, D.; Lamblin, N.; Pasquier, F.; de Groote, P. Prevalence and Determinants of Cognitive Impairment in Chronic Heart Failure Patients. Congest. Hear. Fail. 2007, 13, 205–208. [Google Scholar] [CrossRef]
- Dodson, J.A.; Truong, T.-T.N.; Towle, V.R.; Kerins, G.; Chaudhry, S.I. Cognitive Impairment in Older Adults with Heart Failure: Prevalence, Documentation, and Impact on Outcomes. Am. J. Med. 2013, 126, 120–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huynh, Q.; Negishi, K.; Blizzard, L.; Saito, M.; De Pasquale, C.; Hare, J.L.; Leung, D.; Stanton, T.; Sanderson, K.; Venn, A.J.; et al. Mild cognitive impairment predicts death and readmission within 30 days of discharge for heart failure. Int. J. Cardiol. 2016, 221, 212–217. [Google Scholar] [CrossRef]
- Sterling, M.R.; Safford, M.M.; Goggins, K.; Nwosu, S.K.; Schildcrout, J.S.; A Wallston, K.; Mixon, A.S.; Rothman, R.L.; Kripalani, S. Numeracy, Health Literacy, Cognition, and 30-Day Readmissions among Patients with Heart Failure. J. Hosp. Med. 2018, 13, 145–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, K.S.; Kazim, R.; Xu, J.; Borson, S.; Taffet, G.E. Unrecognized Cognitive Impairment and Its Effect on Heart Failure Readmissions of Elderly Adults. J. Am. Geriatr. Soc. 2016, 64, 2296–2301. [Google Scholar] [CrossRef]
- Hajduk, A.M.; Lemon, S.C.; McManus, D.D.; Lessard, D.M.; Gurwitz, J.H.; A Spencer, F.; Goldberg, R.J.; Saczynski, J.S. Cognitive impairment and self-care in heart failure. Clin. Epidemiol. 2013, 5, 407–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, S.N.; Hajduk, A.M.; McManus, D.D.; Darling, C.E.; Gurwitz, J.H.; Spencer, F.A.; Goldberg, R.J.; Saczynski, J.S. Cognitive status in patients hospitalized with acute decompensated heart failure. Am. Hear. J. 2014, 168, 917–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holm, H.; Bachus, E.; Jujic, A.; Nilsson, E.D.; Wadström, B.; Molvin, J.; Minthon, L.; Fedorowski, A.; Nägga, K.; Magnusson, M. Cognitive test results are associated with mortality and rehospitalization in heart failure: Swedish prospective cohort study. ESC Hear. Fail. 2020, 7, 2948–2955. [Google Scholar] [CrossRef] [PubMed]
- Bruñén, J.M.G.; Echeverria, M.P.; Díez-Manglano, J.; Manzano, L.; Trullàs, J.C.; Requena, J.M.R.; Bautista, M.P.S.; Franco, Á.G.; Rodrigo, J.M.C.; Montero-Pérez-Barquero, M.; et al. Cognitive impairment in patients hospitalized for congestive heart failure: Data from the RICA Registry. Intern. Emerg. Med. 2021, 16, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Pastva, A.M.; Hugenschmidt, C.E.; Kitzman, D.W.; Nelson, M.B.; Brenes, G.A.; Reeves, G.R.; Mentz, R.J.; Whellan, D.J.; Chen, H.; Duncan, P.W. Cognition, Physical Function, and Quality of Life in Older Patients With Acute Decompensated Heart Failure. J. Card. Fail. 2021, 27, 286–294. [Google Scholar] [CrossRef]
- Paulson, O.B.; Strandgaard, S.; Edvinsson, L. Cerebral autoregulation. Cerebrovasc. Brain Metab. Rev. 1990, 2, 161–192. [Google Scholar] [PubMed]
- Vavilala, M.S.; A Lee, L.; Lam, A.M. Cerebral blood flow and vascular physiology. Anesthesiol. Clin. N. Am. 2002, 20, 247–264. [Google Scholar] [CrossRef]
- Sila, C.A. Cognitive impairment in chronic heart failure. Clevel. Clin. J. Med. 2007, 74, S132–S137. [Google Scholar] [CrossRef]
- Georgiadis, D.; Sievert, M.; Cencetti, S.; Uhlmann, F.; Krivokuca, M.; Zierz, S.; Werdan, K. Cerebrovascular reactivity is impaired in patients with cardiac failure. Eur. Hear. J. 2000, 21, 407–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraser, K.S.; Heckman, G.A.; McKelvie, R.S.; Harkness, K.; Middleton, L.E.; Hughson, R.L. Cerebral hypoperfusion is exaggerated with an upright posture in heart failure: Impact of depressed cardiac output. JACC Heart Fail. 2015, 3, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Loncar, G.; Bozic, B.; Lepić, T.; Dimkovic, S.; Prodanovic, N.; Radojicic, Z.; Cvorovic, V.; Markovic, N.; Brajović, M.; Despotovic, N.; et al. Relationship of reduced cerebral blood flow and heart failure severity in elderly males. Aging Male 2011, 14, 59–65. [Google Scholar] [CrossRef]
- Choi, B.-R.; Kim, J.S.; Yang, Y.J.; Park, K.-M.; Lee, C.W.; Kim, Y.-H.; Hong, M.-K.; Song, J.-K.; Park, S.-W.; Park, S.-J.; et al. Factors Associated With Decreased Cerebral Blood Flow in Congestive Heart Failure Secondary to Idiopathic Dilated Cardiomyopathy. Am. J. Cardiol. 2006, 97, 1365–1369. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Abraham, W.T.; Albert, N.M.; Greenberg, B.H.; O’Connor, C.M.; She, L.; Stough, W.G.; Yancy, C.W.; Young, J.B.; Fonarow, G.C.; et al. Systolic Blood Pressure at Admission, Clinical Characteristics, and Outcomes in Patients Hospitalized With Acute Heart Failure. JAMA 2006, 296, 2217–2226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuccala, G.; Onder, G.; Pedone, C.; Carosella, L.; Pahor, M.; Bernabei, R.; Cocchi, A. Hypotension and cognitive impairment: Selective association in patients with heart failure. Neurology 2001, 57, 1986–1992. [Google Scholar] [CrossRef] [PubMed]
- Hoth, K.F.; Poppas, A.; Moser, D.J.; Paul, R.H.; Cohen, R.A. Cardiac Dysfunction and Cognition in Older Adults With Heart Failure. Cogn. Behav. Neurol. 2008, 21, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, R.F.; Grega, M.A.; Bailey, M.M.; Zeger, S.L.; Baumgartner, W.A.; McKhann, G.M.; Selnes, O.A. Association between hypotension, low ejection fraction and cognitive performance in cardiac patients. Behav. Neurol. 2010, 22, 63–71. [Google Scholar] [CrossRef]
- Bornstein, R.A.; Starling, R.C.; Myerowitz, P.D.; Haas, G.J. Neuropsychological function in patients with end-stage heart failure before and after cardiac transplantation. Acta Neurol. Scand. 1995, 91, 260–265. [Google Scholar] [CrossRef]
- Roman, D.D.; Kubo, S.H.; Ormaza, S.; Francis, G.S.; Bank, A.J.; Shumway, S.J. Memory improvement following cardiac transplantation. J. Clin. Exp. Neuropsychol. 1997, 19, 692–697. [Google Scholar] [CrossRef] [PubMed]
- van Bommel, R.J.; Marsan, N.A.; Koppen, H.; Delgado, V.; Borleffs, C.J.; Ypenburg, C.; Bertini, M.; Schalij, M.J.; Bax, J.J. Effect of cardiac resynchronization therapy on cerebral blood flow. Am. J. Cardiol. 2010, 106, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Dixit, N.K.; Vazquez, L.D.; Cross, N.J.; Kuhl, E.A.; Serber, E.R.; Kovacs, A.; Dede, D.E.; Conti, J.B.; Sears, S.F. Cardiac Resynchronization Therapy: A Pilot Study Examining Cognitive Change in Patients Before and After Treatment. Clin. Cardiol. 2010, 33, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, A.L.; Poppas, A.; Paul, R.H.; Cohen, R.A. Systemic hypoperfusion is associated with executive dysfunction in geriatric cardiac patients. Neurobiol. Aging 2007, 28, 477–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajagopalan, B.; Raine, A.E.; Cooper, R.; Ledingham, J.G. Changes in cerebral blood flow in patients with severe congestive cardiac failure before and after captopril treatment. Am. J. Med. 1984, 76, 86–90. [Google Scholar] [CrossRef]
- Gruhn, N.; Larsen, F.S.; Boesgaard, S.; Knudsen, G.M.; Mortensen, S.A.; Thomsen, G.; Aldershvile, J. Cerebral Blood Flow in Patients With Chronic Heart Failure Before and After Heart Transplantation. Stroke 2001, 32, 2530–2533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alosco, M.L.; Brickman, A.M.; Spitznagel, M.B.; Garcia, S.L.; Narkhede, A.; Griffith, E.Y.; Raz, N.; Cohen, R.; Sweet, L.H.; Colbert, L.H.; et al. Cerebral perfusion is associated with white matter hyperintensities in older adults with heart failure. Congest. Hear. Fail. 2013, 19, E29–E34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madhavan, M.; Graff-Radford, J.; Piccini, J.P.; Gersh, B.J. Cognitive dysfunction in atrial fibrillation. Nat. Rev. Cardiol. 2018, 15, 744–756. [Google Scholar] [CrossRef] [PubMed]
- de la Torre, J.C. Hemodynamic Instability in Heart Failure Intensifies Age-Dependent Cognitive Decline. J. Alzheimers Dis. 2020, 76, 63–84. [Google Scholar] [CrossRef] [PubMed]
- Alosco, M.L.; Brickman, A.M.; Spitznagel, M.B.; van Dulmen, M.; Raz, N.; Cohen, R.; Sweet, L.H.; Colbert, L.H.; Josephson, R.; Hughes, J.; et al. The independent association of hypertension with cognitive function among older adults with heart failure. J. Neurol. Sci. 2012, 323, 216–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchistiakova, E.; Anderson, N.; Greenwood, C.E.; MacIntosh, B. Combined effects of type 2 diabetes and hypertension associated with cortical thinning and impaired cerebrovascular reactivity relative to hypertension alone in older adults. NeuroImage Clin. 2014, 5, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strachan, M.W.J.; Deary, I.J.; E Ewing, F.M.; Frier, B.M. Is Type II Diabetes Associated With an Increased Risk of Cognitive Dysfunction?: A critical review of published studies. Diabetes Care 1997, 20, 438–445. [Google Scholar] [CrossRef]
- Campos, M.W.; Serebrisky, D.; Castaldelli-Maia, J.M. Smoking and Cognition. Curr. Drug Abus. Rev. 2016, 9, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Knecht, K.M.; Alosco, M.L.; Spitznagel, M.B.; Cohen, R.; Raz, N.; Sweet, L.; Colbert, L.H.; Josephson, R.; Hughes, J.; Rosneck, J.; et al. Sleep Apnea and Cognitive Function in Heart Failure. Cardiovasc. Psychiatry Neurol. 2012, 2012, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Hjelm, C.; Broström, A.; Dahl, A.; Johansson, B.; Fredrikson, M.; Strömberg, A. Factors Associated With Increased Risk for Dementia in Individuals Age 80 Years or Older With Congestive Heart Failure. J. Cardiovasc. Nurs. 2014, 29, 82–90. [Google Scholar] [CrossRef] [Green Version]
- de la Torre, J.C. Are Major Dementias Triggered by Poor Blood Flow to the Brain? Theoretical Considerations. J. Alzheimers Dis. 2017, 57, 353–371. [Google Scholar] [CrossRef] [PubMed]
- Engelhardt, S.; Al-Ahmad, A.J.; Gassmann, M.; Ogunshola, O.O. Hypoxia selectively disrupts brain microvascular endothelial tight junction complexes through a hypoxia-inducible factor-1 (HIF-1) dependent mechanism. J. Cell Physiol. 2014, 229, 1096–1105. [Google Scholar] [CrossRef] [PubMed]
- Ampadu, J.; Morley, J.E. Heart failure and cognitive dysfunction. Int. J. Cardiol. 2015, 178, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Immink, R.V.; Born, B.-J.H.V.D.; van Montfrans, G.A.; Koopmans, R.P.; Karemaker, J.M.; van Lieshout, J.J. Impaired Cerebral Autoregulation in Patients With Malignant Hypertension. Circulation 2004, 110, 2241–2245. [Google Scholar] [CrossRef] [Green Version]
- Skinhoj, E.; Strandgaard, S. Pathogenesis of hypertensive encephalopathy. Lancet 1973, 1, 461–462. [Google Scholar] [CrossRef]
- Gardner, C.J.; Lee, K. Hyperperfusion Syndromes: Insight into the Pathophysiology and Treatment of Hypertensive Encephalopathy. CNS Spectr. 2007, 12, 35–42. [Google Scholar] [CrossRef]
- MacKenzie, E.T.; Strandgaard, S.; I Graham, D.; Jones, J.V.; Harper, A.M.; Farrar, J.K. Effects of acutely induced hypertension in cats on pial arteriolar caliber, local cerebral blood flow, and the blood-brain barrier. Circ. Res. 1976, 39, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Auer, L. The Sausage-String Phenomenon in Acutely Induced Hypertension—Arguments Against the Vasospasm Theory in the Pathogenesis of Acute Hypertensive Encephalopathy. Eur. Neurol. 1978, 17, 166–173. [Google Scholar] [CrossRef]
- Johansson, B. Regional Cerebral Blood Flow in Acute Experimental Hypertension. Acta Neurol. Scand. 1974, 50, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Fulop, G.A.; Tarantini, S.; Yabluchanskiy, A.; Molnar, A.; Prodan, C.I.; Kiss, T.; Csipo, T.; Lipecz, A.; Balasubramanian, P.; Farkas, E.; et al. Role of age-related alterations of the cerebral venous circulation in the pathogenesis of vascular cognitive impairment. Am. J. Physiol. Circ. Physiol. 2019, 316, H1124–H1140. [Google Scholar] [CrossRef]
- Sung, S.-H.; Lee, C.-W.; Wang, P.-N.; Lee, H.-Y.; Chen, C.-H.; Chung, C.-P. Cognitive functions and jugular venous reflux in severe mitral regurgitation: A pilot study. PLoS ONE 2019, 14, e0207832. [Google Scholar] [CrossRef] [PubMed]
- Fulop, G.A.; Ahire, C.; Csipo, T.; Tarantini, S.; Kiss, T.; Balasubramanian, P.; Yabluchanskiy, A.; Farkas, E.; Toth, A.; Nyúl-Tóth, Á.; et al. Cerebral venous congestion promotes blood-brain barrier disruption and neuroinflammation, impairing cognitive function in mice. GeroScience 2019, 41, 575–589. [Google Scholar] [CrossRef]
- Kim, M.-S.; Kim, J.-J. Heart and Brain Interconnection—Clinical Implications of Changes in Brain Function During Heart Failure. Circ. J. 2015, 79, 942–947. [Google Scholar] [CrossRef] [Green Version]
- Doehner, W.; Ural, D.; Haeusler, K.G.; Čelutkienė, J.; Bestetti, R.; Cavusoglu, Y.; Peña-Duque, M.A.; Glavas, D.; Iacoviello, M.; Laufs, U.; et al. Heart and brain interaction in patients with heart failure: Overview and proposal for a taxonomy. A position paper from the Study Group on Heart and Brain Interaction of the Heart Failure Association. Eur. J. Hear. Fail. 2017, 20, 199–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Athilingam, P.; A Moynihan, J.; Chen, L.; D’Aoust, R.; Groer, M.; E Kip, K. Elevated Levels of Interleukin 6 and C-Reactive Protein Associated With Cognitive Impairment in Heart Failure. Congest. Hear. Fail. 2013, 19, 92–98. [Google Scholar] [CrossRef]
- McAfoose, J.; Baune, B. Evidence for a cytokine model of cognitive function. Neurosci. Biobehav. Rev. 2009, 33, 355–366. [Google Scholar] [CrossRef] [Green Version]
- Hong, X.; Bu, L.; Wang, Y.; Xu, J.; Wu, J.; Huang, Y.; Liu, J.; Suo, H.; Yang, L.; Shi, Y.; et al. Increases in the Risk of Cognitive Impairment and Alterations of Cerebral β-amyloid Metabolism in Mouse Model of Heart Failure. PLoS ONE 2013, 8, e63829. [Google Scholar] [CrossRef]
- Hanninen, S.A.; Darling, P.B.; Sole, M.J.; Barr, A.; Keith, M.E. The Prevalence of Thiamin Deficiency in Hospitalized Patients With Congestive Heart Failure. J. Am. Coll. Cardiol. 2006, 47, 354–361. [Google Scholar] [CrossRef] [Green Version]
- Calingasan, N.Y.; Chun, W.J.; Park, L.C.; Uchida, K.; Gibson, G.E. Oxidative Stress Is Associated with Region-Specific Neuronal Death During Thiamine Deficiency. J. Neuropathol. Exp. Neurol. 1999, 58, 946–958. [Google Scholar] [CrossRef]
- Langlais, P.J.; Savage, L.M. Thiamine deficiency in rats produces cognitive and memory deficits on spatial tasks that correlate with tissue loss in diencephalon, cortex and white matter. Behav. Brain Res. 1995, 68, 75–89. [Google Scholar] [CrossRef]
- Yavuz, B.B.; Cankurtaran, M.; Haznedaroglu, I.C.; Halil, M.; Ulger, Z.; Altun, B.; Ariogul, S. Iron deficiency can cause cognitive impairment in geriatric patients. J. Nutr. Health Aging 2012, 16, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Parissis, J.T.; Adamopoulos, S.; Rigas, A.; Kostakis, G.; Karatzas, D.; Venetsanou, K.; Kremastinos, D.T. Comparison of circulating proinflammatory cytokines and soluble apoptosis mediators in patients with chronic heart failure with versus without symptoms of depression. Am. J. Cardiol. 2004, 94, 1326–1328. [Google Scholar] [CrossRef]
- Cotter, G.; Metra, M.; Davison, B.A.; Jondeau, G.; Cleland, J.G.; Bourge, R.C.; Milo, O.; O’Connor, C.M.; Parker, J.D.; Torre-Amione, G.; et al. Systolic blood pressure reduction during the first 24 h in acute heart failure admission: Friend or foe? Eur. J. Hear. Fail. 2017, 20, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Cleutjens, F.A.; Janssen, D.J.; Ponds, R.W.; Dijkstra, J.B.; Wouters, E.F. COgnitive-pulmonary disease. Biomed. Res. Int. 2014, 2014, 697825. [Google Scholar] [CrossRef] [Green Version]
- Nowak, K.L.; Yaffe, K.; Orwoll, E.S.; Ix, J.H.; You, Z.; Barrett-Connor, E.; Hoffman, A.R.; Chonchol, M. Serum Sodium and Cognition in Older Community-Dwelling Men. Clin. J. Am. Soc. Nephrol. 2018, 13, 366–374. [Google Scholar] [CrossRef]
- Kumari, M.; Brunner, E.; Fuhrer, R. Minireview: Mechanisms by Which the Metabolic Syndrome and Diabetes Impair Memory. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2000, 55, B228–B232. [Google Scholar] [CrossRef] [Green Version]
- Pulignano, G.; Del Sindaco, D.; Di Lenarda, A.; Tinti, M.D.; Tarantini, L.; Cioffi, G.; Tolone, S.; Pero, G.; Minardi, G. Chronic renal dysfunction and anaemia are associated with cognitive impairment in older patients with heart failure. J. Cardiovasc. Med. 2014, 15, 481–490. [Google Scholar] [CrossRef]
- Hadjihambi, A.; Arias, N.; Sheikh, M.; Jalan, R. Hepatic encephalopathy: A critical current review. Hepatol. Int. 2018, 12, 135–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinohara, M.; Yamada, M. Drug-induced Cognitive Impairment. Brain Nerve 2016, 68, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Sterling, M.R.; Jannat-Khah, D.; Bryan, J.; Banerjee, S.; McClure, L.A.; Wadley, V.G.; Unverzagt, F.W.; Levitan, E.B.; Goyal, P.; Peterson, J.C.; et al. The Prevalence of Cognitive Impairment Among Adults With Incident Heart Failure: The “Reasons for Geographic and Racial Differences in Stroke” (REGARDS) Study. J. Card. Fail. 2019, 25, 130–136. [Google Scholar] [CrossRef]
- Hammond, C.A.; Blades, N.J.; Chaudhry, S.I.; Dodson, J.A.; Longstreth, W.T., Jr.; Heckbert, S.R.; Psaty, B.M.; Arnold, A.M.; Dublin, S.; Sitlani, C.M.; et al. Long-Term Cognitive Decline After Newly Diagnosed Heart Failure: Longitudinal Analysis in the CHS (Cardiovascular Health Study). Circ. Heart Fail. 2018, 11, e004476. [Google Scholar] [CrossRef] [PubMed]
- Alwerdt, J.; Edwards, J.D.; Athilingam, P.; O’Connor, M.L.; Valdes, E. Longitudinal Differences in Cognitive Functioning Among Older Adults With and Without Heart Failure. J. Aging Health 2013, 25, 1358–1377. [Google Scholar] [CrossRef]
- Hjelm, C.; Dahl, A.; Broström, A.; Mårtensson, J.; Johansson, B.; Strömberg, A. The influence of heart failure on longitudinal changes in cognition among individuals 80 years of age and older. J. Clin. Nurs. 2011, 21, 994–1003. [Google Scholar] [CrossRef] [Green Version]
- Almeida, O.P.; Beer, C.; Lautenschlager, N.T.; Arnolda, L.; Alfonso, H.; Flicker, L. Two-year course of cognitive function and mood in adults with congestive heart failure and coronary artery disease: The Heart-Mind Study. Int. Psychogeriatr. 2012, 24, 38–47. [Google Scholar] [CrossRef]
- Huijts, M.; Van Oostenbrugge, R.J.; Duits, A.; Burkard, T.; Muzzarelli, S.; Maeder, M.T.; Schindler, R.; Pfisterer, M.E.; Rocca, H.-P.B.-L. Cognitive impairment in heart failure: Results from the Trial of Intensified versus standard Medical therapy in Elderly patients with Congestive Heart Failure (TIME-CHF) randomized trial. Eur. J. Hear. Fail. 2013, 15, 699–707. [Google Scholar] [CrossRef] [Green Version]
- Stanek, K.M.; Gunstad, J.; Paul, R.H.; Poppas, A.; Jefferson, A.L.; Sweet, L.H.; Hoth, K.F.; Haley, A.P.; Forman, D.E.; Cohen, R.A. Longitudinal cognitive performance in older adults with cardiovascular disease: Evidence for improvement in heart failure. J. Cardiovasc. Nurs. 2009, 24, 192–197. [Google Scholar] [CrossRef] [Green Version]
- Kindermann, I.; Fischer, D.; Karbach, J.; Link, A.; Walenta, K.; Barth, C.; Ukena, C.; Mahfoud, F.; Köllner, V.; Kindermann, M.; et al. Cognitive function in patients with decompensated heart failure: The Cognitive Impairment in Heart Failure (CogImpair-HF) study. Eur. J. Heart Fail. 2012, 14, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.; Fazekas, F.; Offenbacher, H.; Dusleag, J.; Lechner, H. Brain magnetic resonance imaging and neuropsychologic evaluation of patients with idiopathic dilated cardiomyopathy. Stroke 1991, 22, 195–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, M.A.; Ogren, J.A.; Abouzeid, C.M.; Macey, P.; Sairafian, K.G.; Saharan, P.S.; Thompson, P.; Fonarow, G.; Hamilton, M.A.; Harper, R.M.; et al. Regional hippocampal damage in heart failure. Eur. J. Hear. Fail. 2015, 17, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Woo, M.A.; Birrer, B.V.; Macey, P.M.; Fonarow, G.C.; Hamilton, M.A.; Harper, R.M. Mammillary bodies and fornix fibers are injured in heart failure. Neurobiol. Dis. 2009, 33, 236–242. [Google Scholar] [CrossRef] [Green Version]
- Kumar, R.; Nguyen, H.D.; Ogren, J.A.; Macey, P.; Thompson, P.; Fonarow, G.; Hamilton, M.A.; Harper, R.M.; Woo, M.A. Global and regional putamen volume loss in patients with heart failure. Eur. J. Hear. Fail. 2011, 13, 651–655. [Google Scholar] [CrossRef] [Green Version]
- Kumar, R.; Yadav, S.K.; Palomares, J.A.; Park, B.; Joshi, S.H.; Ogren, J.A.; Macey, P.M.; Fonarow, G.C.; Harper, R.M.; Woo, M.A. Reduced Regional Brain Cortical Thickness in Patients with Heart Failure. PLoS ONE 2015, 10, e0126595. [Google Scholar] [CrossRef] [Green Version]
- Almeida, O.P.; Garrido, G.J.; Etherton-Beer, C.; Lautenschlager, N.T.; Arnolda, L.; Flicker, L. Cognitive and brain changes associated with ischaemic heart disease and heart failure. Eur. Hear. J. 2012, 33, 1769–1776. [Google Scholar] [CrossRef] [Green Version]
- Alves, T.C.; Rays, J.; Fráguas, R., Jr.; Wajngarten, M.; Meneghetti, J.C.; Prando, S.; Busatto, G.F. Localized cerebral blood flow reductions in patients with heart failure: A study using 99mTc-HMPAO SPECT. J. Neuroimaging 2005, 15, 150–156. [Google Scholar] [CrossRef]
- Alves, T.C.D.T.F.; Busatto, G.F. Regional cerebral blood flow reductions, heart failure and Alzheimer’s disease. Neurol. Res. 2006, 28, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Woo, M.A.; Macey, P.; Fonarow, G.; Hamilton, M.A.; Harper, R.M. Brain axonal and myelin evaluation in heart failure. J. Neurol. Sci. 2011, 307, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.; Lu, Z.; Wang, L.; Zhao, Y.; Nie, B.; Xu, Q.; Han, X.; Li, T.; Zhao, J.; Cheng, W.; et al. Dynamic Changes in Brain Glucose Metabolism and Neuronal Structure in Rats with Heart Failure. Neuroscience 2019, 424, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Rice, L.; Bisdas, S. The diagnostic value of FDG and amyloid PET in Alzheimer’s disease—A systematic review. Eur. J. Radiol. 2017, 94, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Alongi, P.; Sardina, D.S.; Coppola, R.; Scalisi, S.; Puglisi, V.; Arnone, A.; Di Raimondo, G.; Munerati, E.; Alaimo, V.; Midiri, F.; et al. 18F-Florbetaben PET/CT to Assess Alzheimer’s Disease: A new Analysis Method for Regional Amyloid Quantification. J. Neuroimaging 2019, 29, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Dervenoulas, G.; Politis, M. Magnetic resonance imaging in Alzheimer’s disease and mild cognitive impairment. J. Neurol. 2019, 266, 1293–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollenberg, S.M.; Warner Stevenson, L.; Ahmad, T.; Amin, V.J.; Bozkurt, B.; Butler, J.; Davis, L.L.; Drazner, M.H.; Kirkpatrick, J.N.; Peterson, P.N.; et al. 2019 ACC Expert Consensus Decision Pathway on Risk Assessment, Management, and Clinical Trajectory of Patients Hospitalized With Heart Failure: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2019, 74, 1966–2011. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Progression of brain injury during the natural course of acutely decompensated heart failure.
Figure 1.
Progression of brain injury during the natural course of acutely decompensated heart failure.

Figure 2.
Protection of brain function through the optimal management of acute heart failure clinical profile.
Figure 2.
Protection of brain function through the optimal management of acute heart failure clinical profile.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Features of the most common and brief screening tools for the assessment of cognitive impairment in heart failure.
Table 1.
Features of the most common and brief screening tools for the assessment of cognitive impairment in heart failure.
| Screening Tool | Scoring System | Usual Cut-Off Point | Administration Time (min) | Comments |
|---|---|---|---|---|
| Mini Mental State Examination (MMSE) [35,43,44,45,46,47,48,49] | 0–30 | <24 | 5–10 |
|
| Montreal Cognitive Assessment (MoCA) [50,51,52,53] | 0–30 | <26 | 10 |
|
| Mini-Cog Test [39,40] | Composite score: 5
| ≤2 | 3 |
|
| MoCA 5-min protocol (Mini-MoCA) [41,42] | 12 | ≤9 | 5 |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ventoulis, I.; Arfaras-Melainis, A.; Parissis, J.; Polyzogopoulou, E. Cognitive Impairment in Acute Heart Failure: Narrative Review. J. Cardiovasc. Dev. Dis. 2021, 8, 184. https://doi.org/10.3390/jcdd8120184
AMA Style
Ventoulis I, Arfaras-Melainis A, Parissis J, Polyzogopoulou E. Cognitive Impairment in Acute Heart Failure: Narrative Review. Journal of Cardiovascular Development and Disease. 2021; 8(12):184. https://doi.org/10.3390/jcdd8120184
Chicago/Turabian StyleVentoulis, Ioannis, Angelos Arfaras-Melainis, John Parissis, and Eftihia Polyzogopoulou. 2021. "Cognitive Impairment in Acute Heart Failure: Narrative Review" Journal of Cardiovascular Development and Disease 8, no. 12: 184. https://doi.org/10.3390/jcdd8120184
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.