Preoperative Assessment and Management of Cardiovascular Risk in Patients Undergoing Non-Cardiac Surgery: Implementing a Systematic Stepwise Approach during the COVID-19 Pandemic Era

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
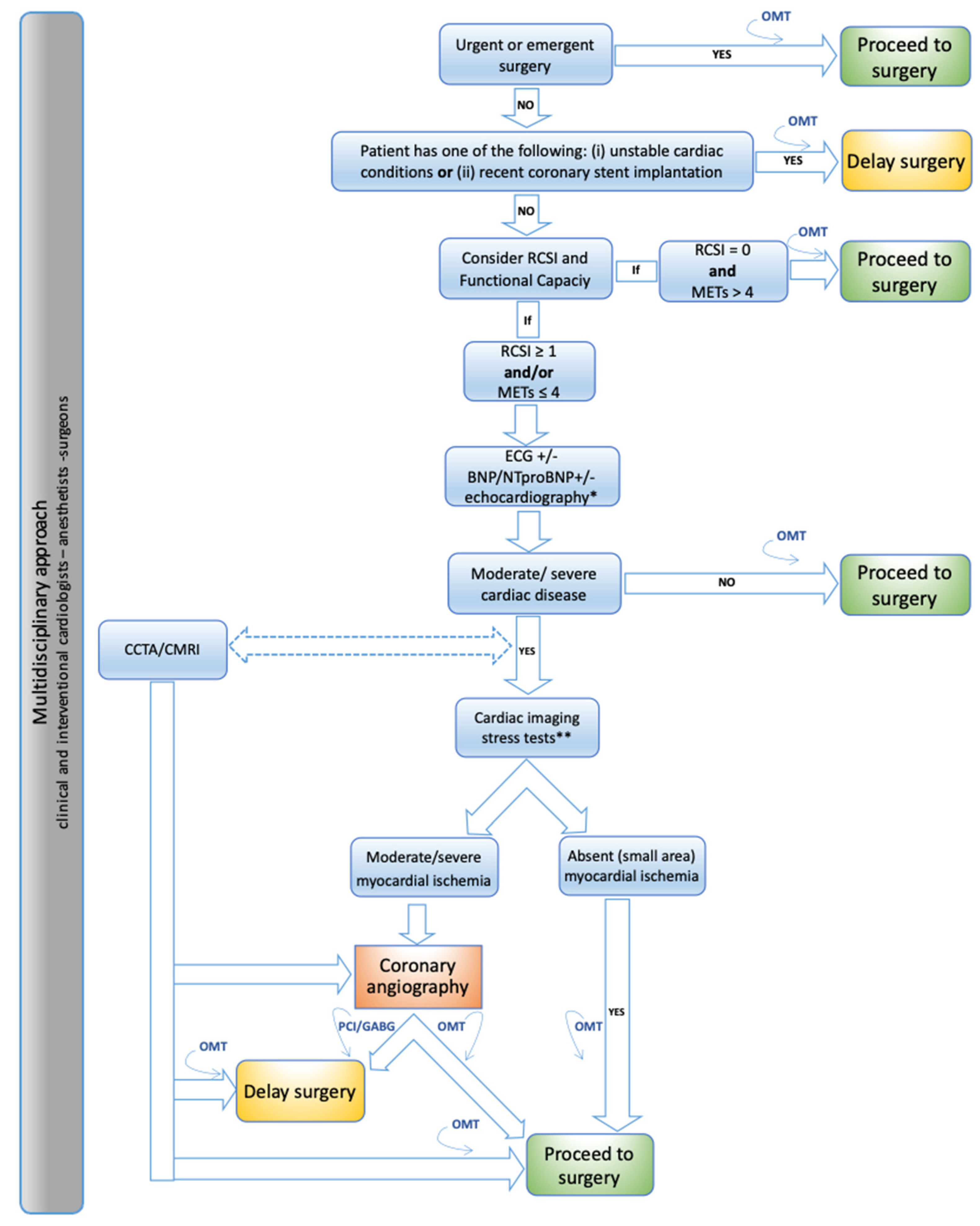
2. Step 1: Consider the Timing of Surgery
3. Step 2: Identify Unstable Cardiac Conditions and Recent Coronary Revascularization
3.1. Unstable Cardiac Conditions
3.2. Recent Coronary Stent Implantation
4. Step 3: Assess the Functional Capacity and the Cardiovascular Perioperative Risk
4.1. Functional Capacity
4.2. Cardiovascular Perioperative Risk Scores
4.3. Combining Functional Capacity and Cardiovascular Perioperative Risk Score
5. Step 4: Measuring Blood Biomarkers Levels and Performing Electrocardiogram/Cardiac Imaging Tests
5.1. Biomarkers: BNP/NT-ProBNP and Troponin
5.2. ECG
5.3. Resting Transthoracic Color-Doppler Echocardiography
5.4. Non-Invasive Imaging Stress Testing for Ischemic Heart Disease
5.5. Coronary Angiography
5.6. Coronary Computed Tomographic Angiography
5.7. Cardiac Magnetic Resonance Imaging
6. Perioperative Management of Cardiovascular Medications
6.1. Beta-Blockers
6.2. Statins
6.3. ACEI-ARBs and Other Drugs
7. Perioperative Management of Antithrombotic Therapy
7.1. Antiplatelet Therapy
Aspirin
7.2. Dual Antiplatelet Therapy
7.3. Intravenous Reversible Antiplatelet Agents
7.4. Anticoagulant Therapy
7.4.1. Vitamin K Antagonists
7.4.2. Non-Vitamin K Antagonist Oral Anticoagulants
7.4.3. Unfractionated Heparin and Low-Molecular-Weight Heparin
8. Post-Operative Major Adverse Cardiovascular Events Prevention
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AF | atrial fibrillation |
| ARBs | angiotensin receptor blockers |
| ASA | aspirin |
| BMS | bare metal stent |
| BNP | brain natriuretic peptide |
| CA | coronary angiography |
| CABG | coronary artery bypass grafting |
| CAD | coronary artery disease |
| CCTA | coronary computed tomographic angiography |
| CMRI | cardiac magnetic resonance imaging |
| COVID-19 | 2019 Coronavirus disease |
| ClCr | creatinine clearance |
| CT | computed tomography |
| DAPT | dual antiplatelet therapy |
| DES | drug eluting stent |
| ECG | electrocardiogram |
| FoCUS | focused cardiac ultrasound study |
| GFR | glomerular filtration rate |
| GPIIb-IIIa | glycoprotein IIb/IIIa inhibitors |
| HF | heart failure |
| INR | international normalized ratio |
| LMWH | low molecular weight heparin |
| MACEs | major adverse cardiac events |
| METs | metabolic equivalents |
| MI | myocardial infarction |
| NOACs | non-vitamin K antagonist oral anticoagulants |
| NSQIP | National Surgical Quality Improvement Program |
| NT-proBNP | N-terminal-pro hormone BNP |
| PCI | percutaneous coronary intervention |
| RCRI | Revised Cardiac Risk Index |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus-2 |
| SPECT | single-photon emission computed tomography |
| TTE | transthoracic color-Doppler echocardiography |
| TURP | transurethral resection of the prostate |
| UFH | unfractionated heparin |
| VKAs | vitamin K antagonists |
References
- Kristensen, S.D.; Knuuti, J.; Saraste, A.; Anker, S.D.; Bøtker, H.E.; De Hert, S.; Ford, I.; Juanatey, J.R.G.; Gorenek, B.; Heyndrickx, G.R.; et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management. Eur. Heart J. 2014, 35, 2383–2431. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Berger, J.S. Perioperative Cardiovascular Risk Assessment and Management for Noncardiac Surgery. JAMA 2020, 324, 279. [Google Scholar] [CrossRef] [PubMed]
- Duceppe, E.; Parlow, J.; MacDonald, P.; Lyons, K.; McMullen, M.; Srinathan, S.; Graham, M.; Tandon, V.; Styles, K.; Bessissow, A.; et al. Canadian Cardiovascular Society Guidelines on Perioperative Cardiac Risk Assessment and Management for Patients Who Undergo Noncardiac Surgery. Can. J. Cardiol. 2016, 33, 17–32. [Google Scholar] [CrossRef] [Green Version]
- Fleisher, L.A.; Fleischmann, K.E.; Auerbach, A.; Barnason, S.A.; Beckman, J.; Bozkurt, B.; Davila-Roman, V.G.; Gerhard-Herman, M.D.; Holly, T.A.; Kane, G.C.; et al. 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation 2014, 130, e278–e333. [Google Scholar] [CrossRef]
- Zipes, D.P.; Libby, P.; Bonow, R.O.; Mann, D.L.; Tomaselli, G.F. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, 11th ed.; Elsevier: New York, NY, USA, 2018. [Google Scholar]
- Skulstad, H.; Cosyns, B.; Popescu, B.A.; Galderisi, M.; Di Salvo, G.; Donal, E.; Petersen, S.; Gimelli, A.; Haugaa, K.; Muraru, D.; et al. COVID-19 pandemic and cardiac imaging: EACVI recommendations on precautions, indications, prioritization, and protection for patients and healthcare personnel. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 592–598. [Google Scholar] [CrossRef] [PubMed]
- The European Society for Cardiology. ESC Guidance for the Diagnosis and Management of CV Disease during the COVID-19 Pandemic. 2020. Available online: https://www.escardio.org/Education/COVID-19-and-Cardiology/ESC-COVID-19-Guidance (accessed on 10 June 2020).
- Bossone, E.; Mauro, C.; Maiellaro, A.; Raiola, E.; Cocchia, R.; Ranieri, B.; Sepe, C.; Capone, V.; Chianese, S.; Maramaldi, R.; et al. Cardiac teleconsulting in the time of COVID-19 global pandemic: The “Antonio Cardarelli” Hospital project. Monaldi Arch. Chest Dis. 2021, 91. [Google Scholar] [CrossRef] [PubMed]
- Società Italiana di Ecocardiografia e Cardiovascular Imaging (SIECVI). Documento ad uso Degli Operatori di Ecografia Cardiovascolare per COVID-19. 2020. Available online: https://www.siec.it/download/siecvi-documento-ad-uso-degli-operatori-di-ecografia-cardiovascolare-per-covid-19 (accessed on 10 June 2020).
- Giustino, G.; Chieffo, A.; Palmerini, T.; Valgimigli, M.; Feres, F.; Abizaid, A.; Costa, R.A.; Hong, M.-K.; Kim, B.-K.; Jang, Y.; et al. Efficacy and Safety of Dual Antiplatelet Therapy After Complex PCI. J. Am. Coll. Cardiol. 2016, 68, 1851–1864. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2017, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2020, 42, 1289–1367. [Google Scholar] [CrossRef]
- Rossini, R.; Tarantini, G.; Musumeci, G.; Masiero, G.; Barbato, E.; Calabrò, P.; Capodanno, D.; Leonardi, S.; Lettino, M.; Limbruno, U.; et al. A Multidisciplinary Approach on the Perioperative Antithrombotic Management of Patients with Coronary Stents Undergoing Surgery. JACC: Cardiovasc. Interv. 2018, 11, 417–434. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.H.; Marcantonio, E.R.; Mangione, C.M.; Thomas, E.J.; Polanczyk, C.A.; Cook, E.F.; Sugarbaker, D.J.; Donaldson, M.C.; Poss, R.; Ho, K.K.L.; et al. Derivation and Prospective Validation of a Simple Index for Prediction of Cardiac Risk of Major Noncardiac Surgery. Circulation 1999, 100, 1043–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, P.K.; Gupta, H.; Sundaram, A.; Kaushik, M.; Fang, X.; Miller, W.J.; Esterbrooks, D.J.; Hunter, C.B.; Pipinos, I.I.; Johanning, J.M.; et al. Development and Validation of a Risk Calculator for Prediction of Cardiac Risk After Surgery. Circulation 2011, 124, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, G.F.; Balady, G.J.; Amsterdam, E.A.; Chaitman, B.; Eckel, R.; Fleg, J.; Froelicher, V.F.; Leon, A.S.; Piña, I.L.; Rodney, R.; et al. Exercise Standards for Testing and Training. Circulation 2001, 104, 1694–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise Capacity and Mortality among Men Referred for Exercise Testing. New Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef]
- Hlatky, M.; Boineau, R.E.; Higginbotham, M.B.; Lee, K.L.; Mark, D.; Califf, R.M.; Cobb, F.R.; Pryor, D.B. A brief self-administered questionnaire to determine functional capacity (The Duke Activity Status Index). Am. J. Cardiol. 1989, 64, 651–654. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Agewall, S.; Giannitsis, E.; Jernberg, T.; Katus, H. Troponin elevation in coronary vs. non-coronary disease. Eur. Heart J. 2010, 32, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Feigenbaum, H.; Armstrong, W.F.; Ryan, T. Feigenbaum’s Echocardiography; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2019. [Google Scholar]
- Cardim, N.; Dalen, H.; Voigt, J.-U.; Ionescu, A.; Price, S.; Neskovic, A.N.; Edvardsen, T.; Galderisi, M.; Sicari, R.; Donal, E.; et al. The use of handheld ultrasound devices: A position statement of the European Association of Cardiovascular Imaging (2018 update). Eur. Heart J. Cardiovasc. Imaging 2018, 20, 245–252. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2019, 41, 407–477. [Google Scholar] [CrossRef]
- Zipes, D.P.; Libby, P. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, 2-Volume Set, 11th ed.; Elsevier: Philadelphia, PA, USA, 2019. [Google Scholar]
- Serruys, P.W.; Hara, H.; Garg, S.; Kawashima, H.; Nørgaard, B.L.; Dweck, M.R.; Bax, J.J.; Knuuti, J.; Nieman, K.; Leipsic, J.A.; et al. Coronary Computed Tomographic Angiography for Complete Assessment of Coronary Artery Disease. J. Am. Coll. Cardiol. 2021, 78, 713–736. [Google Scholar] [CrossRef]
- Lombardi, M.; Plein, S. The EACVI Textbook of Cardiovascular Magnetic Resonance; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- Hundley, W.G.; Bluemke, D.A.; Finn, J.P.; Flamm, S.D.; Fogel, M.A.; Friedrich, M.G.; Ho, V.B.; Jerosch-Herold, M.; Kramer, C.M.; Manning, W.J.; et al. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: A report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J. Am. Coll. Cardiol. 2010, 55, 2614–2662. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease. Circulation 2016, 134, e123–e155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. EP Eur. 2021. [Google Scholar] [CrossRef]
- London, M.J.; Hur, K.; Schwartz, G.G.; Henderson, W.G. Association of Perioperative β-Blockade with Mortality and Cardiovascular Morbidity Following Major Noncardiac Surgery. JAMA 2013, 309, 1704–1713. [Google Scholar] [CrossRef] [Green Version]
- Flu, W.-J.; Van Kuijk, J.-P.; Chonchol, M.; Winkel, T.A.; Verhagen, H.J.; Bax, J.J.; Poldermans, D. Timing of Pre-Operative Beta-Blocker Treatment in Vascular Surgery Patients: Influence on Post-Operative Outcome. J. Am. Coll. Cardiol. 2010, 56, 1922–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijeysundera, D.; Duncan, D.; Nkonde-Price, C.; Virani, S.; Washam, J.B.; Fleischmann, K.E.; Fleisher, L.A. Perioperative Beta Blockade in Noncardiac Surgery: A Systematic Review for the 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. J. Am. Coll. Cardiol. 2014, 64, 2406–2425. [Google Scholar] [CrossRef] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2019, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Gremmel, T.; Yanachkov, I.; Yanachkova, M.I.; Wright, G.E.; Wider, J.; Undyala, V.V.; Michelson, A.D.; FrelingerIII, A.L.; Przyklenk, K. Synergistic Inhibition of Both P2Y 1 and P2Y 12 Adenosine Diphosphate Receptors as Novel Approach to Rapidly Attenuate Platelet-Mediated Thrombosis. Arter. Thromb. Vasc. Biol. 2016, 36, 501–509. [Google Scholar] [CrossRef] [Green Version]
- Eisen, A.; Bhatt, D.L. Defining the optimal duration of DAPT after PCI with DES. Nat. Rev. Cardiol. 2015, 12, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Rossini, R.; Musumeci, G.; Visconti, L.O.; Bramucci, E.; Castiglioni, B.; De Servi, S.; Lettieri, C.; Lettino, M.; Piccaluga, E.; Savonitto, S.; et al. Perioperative management of antiplatelet therapy in patients with coronary stents undergoing cardiac and non-cardiac surgery: A consensus document from Italian cardiological, surgical and anaesthesiological societies. EuroIntervention 2014, 10, 38–46. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Schneider, D.J.; Bhatt, D.L.; French, W.J.; Price, M.J.; Saucedo, J.F.; Shaburishvili, T.; Huber, K.; Prats, J.; Liu, T.; et al. Pharmacodynamic effects of cangrelor and clopidogrel: The platelet function substudy from the cangrelor versus standard therapy to achieve optimal management of platelet inhibition (CHAMPION) trials. J. Thromb. Thrombolysis 2012, 34, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Mekaj, A.; Mekaj, Y.; Duci, S.; Miftari, E. New oral anticoagulants: Their advantages and disadvantages compared with vitamin K antagonists in the prevention and treatment of patients with thromboembolic events. Ther. Clin. Risk Manag. 2015, ume 11, 967–977. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| General Recommendations |
| • At the time of hospital admission, patients should undergo clinical and laboratory assessment for COVID-19 infection + SARS-CoV-2 nucleic acid amplification testing (for example, RT-PCR) or antigen testing. |
| • Use “personal protective equipment” (protective masks/clothing, gloves, googles, surgical cap, etc.). |
| • Observe social distancing rules and routinely clean medical equipment. |
| • Implement teleconsulting/telemedicine whenever possible and limit number of caregivers. |
| • Patients should undergo SARS-CoV-2 polymerase chain reaction 48–72 h before invasive/high-risk contamination procedures (i.e., coronary angiography, TEE, physical stress tests, etc.). |
| • Perform periodic COVID-19 screening of patients and caregivers (SARS-CoV-2 nucleic acid amplification testing (for example, RT-PCR) or antigen testing. |
| • Check COVID-19 vaccination status for patients and caregivers. |
| Cardiac Imaging |
| • Cardiac imaging should be performed if appropriate and only if it is likely to substantially change patient management. |
| • A focused cardiac ultrasound study (FoCUS) is recommended to reduce the duration of exposure. Handheld ultrasound devices should be implemented. |
| • The risk of contamination of equipment and personnel is very high during TEE; if necessary, consider as alternatives CCTA or cardiac CMRI. |
| • CCTA may be implemented to exclude or confirm coronary heart disease. |
| • Avoid cardiac stress tests; if necessary, favor pharmacologic (or CCTA) to physical stress. |
| • If an urgent coronary angiography is needed (i.e., ACS), a dedicated COVID-19 Cath-Lab should be used. |
| • CMRI may be implemented in the suspicion of takotsubo syndrome or myocarditis. |
| Activities | Wheight (METs) |
|---|---|
| • Can you take care of yourself (eating, dressing, bathing or using the toilet)? | 2.75 |
| • Can you walk indoors, such as around your house? | 1.75 |
| • Can you walk a block or two on level ground? | 2.75 |
| • Can you climb a flight of stairs or walk up a hill? | 5.50 |
| • Can you run a short distance? | 8.00 |
| • Can you undertake light work around the house, such as dusting or washing dishes? | 2.70 |
| • Can you perform moderate work around the house, such as vacuuming, sweeping floors or carrying in groceries? | 3.50 |
| • Can you perform heavy work around the house, such as scrubbing floors or lifting and moving heavy furniture? | 8.00 |
| • Can you perform yard work, such as raking leaves, weeding or pushing a power mower? | 4.50 |
| • Can you have sexual relations? | 5.25 |
| • Can you participate in moderate recreational activities, such as golf, bowling, dancing, doubles tennis or throwing a baseball or football? | 6.00 |
| • Can you participate in strenuous sports, such as swimming, singles tennis, football, basketball or skiing? | 7.50 |
| Ref/Web-Sites/Apps | Link |
|---|---|
| 2014 ‘ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management’. | https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/ESC-ESA-Guidelines-on-non-cardiac-surgery-cardiovascular-assessment-and-managem |
| ‘ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery’. | https://www.ahajournals.org/doi/pdf/10.1161/CIR.0000000000000106 |
| ‘CCS Guidelines on Perioperative Cardiac Risk Assessment and Management for Patients Who Undergo Noncardiac Surgery’. | https://www.onlinecjc.ca/article/S0828-282X(16)30980-1/pdf |
| 2021 ‘EHRA Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation’. | https://www.escardio.org/Guidelines/Recommended-Reading/Heart-Rhythm/Novel-Oral-Anticoagulants-for-Atrial-Fibrillation |
| ‘ESC Guidance for the Diagnosis and Management of CV Disease during the COVID-19 Pandemic’. | https://www.escardio.org/static-file/Escardio/Education-General/Topic%20pages/Covid-19/ESC%20Guidance%20Document/ESC-Guidance-COVID-19-Pandemic.pdf |
| ‘COVID-19 pandemic and cardiac imaging: EACVI recommendations on precautions, indications, prioritization, and pro-tection for patients and healthcare personnel’. | https://academic.oup.com/ehjcimaging/article/21/6/592/5815408 |
| Stent and Surgery App | https://play.google.com/store/apps/details?id=com.araneum.stentsurgery&hl=it&gl=US |
| MDCalc Medical Calculator App | https://play.google.com/store/apps/details?id=com.mdaware.mdcalc&hl=it&gl=US • ASA Physical Status/ASA Classification. • Creatinine clearance (Cockcroft-Gault Equation). • CHA2DS2-VASc Score. • Child–Pugh Score. • QT corrected interval (QTc). • HAS-BLED Score. • Revised Cardiac Risk Index. |
| VKAs | ➢ Elective surgery |
| • Minor bleeding risk surgery: no change in oral anticoagulation therapy is needed but keep INR levels in the lower therapeutic range. | |
| • Low/high bleeding risk surgery: take the last dose 3–5 days before surgery; when INR is ≤1.5, surgery can be performed safely. | |
| ➢ VKAs should be resumed on day 1 or 2 after surgery depending on the patient’s hemostatic status, but no less than 12 h after the procedure. ➢ If high risk of thromboembolism 1, bridging therapy with UFH or LMWH 2 needs to be implemented. ➢ In case of urgent/emergent surgery, immediately discontinue. If needed, reversal with vitamin K or fresh-frozen plasma/PCCs. | |
| NOACs | ➢ Elective surgery |
| Take the last dose before surgery according to CrCl: | |
| • Minor bleeding risk surgery: ≥12 h or 24 h 1 • Low bleeding risk surgery: - apixaban/edoxaban/rivaroxaban ≥24 h 2 - dabigatran ≥ 24–48 h 3 | |
| • High bleeding risk surgery: - apixaban/edoxaban/rivaroxaban ≥48 h 4 - dabigatran ≥48–96 h 5 | |
| ➢ No bridging with heparin required. ➢ In case of urgent/emergent surgery immediately discontinue. If needed, reversal with idaracizumab (dabigatran) or PCCs or aPCCs. |
| Features | UFH | LMWH |
|---|---|---|
| Mean molecular weight | 15,000 Da | 5000 Da |
| Target | Xa and IIa | Xa and IIa (greater Xa inhibition than IIa) |
| Bioavailability (%) | 30 | 90 |
| Half-life | 1 h | 4 h |
| Renal Excretion | No | Yes |
| Antidote (Protamine sulfate) | Complete reversal | Partial reversal (~50%) |
| Heparin-induced thrombocytopenia (HIT) | <5% | <1% |
| Method of administration | Intravenous infusion or less frequently subcutaneously. | Subcutaneously (less frequently can be administered intravenously if a rapid anticoagulant response is needed). |
| Monitoring | aPTT | Not necessary (predictable anticoagulant response). |
| Dosages • Prophylaxis • Therapeutic | - Usually given in fixed doses of 5000 units subcutaneously two or three times daily. * | - 4000 to 5000 units daily or 2500 to 3000 units twice daily subcutaneously. |
| - Initial bolus of 5000 U followed by 30,000 to 35,000 U/24 h followed by intravenous infusion with aPTT monitoring. | - Subcutaneously according to body weight (100 U/kg twice daily). - The dose needs to be reduced in patients with renal impairment (GFR < 30 mL/min/1.73 m2). | |
| Management before non-cardiac surgery | - Discontinue administration ≥4 h before surgery. - Resume full dose ≥12 h after surgery. - In case of urgent/emergent surgery immediately discontinue. If needed, complete reversal with protamine sulphate. | - Discontinue administration ≥12 h before surgery. - Resume full dose ≥12 h after surgery. - In case of urgent/emergent surgery immediately discontinue. If needed, partial reversal (~50%) with protamine sulphate. |
| Limitations | Dose-dependent clearance (binds to endothelial cells); variable anticoagulant response (binds to plasma proteins). | Potential accumulation in patients with renal insufficiency (GFR <30 mL/min/1.73 m2). |
| Side effects | - Short term: • bleeding (most common, increasing with higher heparin doses or concomitant administration of antiplatelet or fibrinolytic agents); • HIT (it occurs 5 to 14 days after the initiation of heparin therapy, but it may be manifested earlier if the patient has received heparin within the past 3 months); • elevated levels of transaminases (rapidly return to normal when the drug is stopped). - Long term: • osteoporosis. | The same as UFH but less frequent. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bossone, E.; Cademartiri, F.; AlSergani, H.; Chianese, S.; Mehta, R.; Capone, V.; Ruotolo, C.; Tarrar, I.H.; Frangiosa, A.; Vriz, O.; et al. Preoperative Assessment and Management of Cardiovascular Risk in Patients Undergoing Non-Cardiac Surgery: Implementing a Systematic Stepwise Approach during the COVID-19 Pandemic Era. J. Cardiovasc. Dev. Dis. 2021, 8, 126. https://doi.org/10.3390/jcdd8100126
Bossone E, Cademartiri F, AlSergani H, Chianese S, Mehta R, Capone V, Ruotolo C, Tarrar IH, Frangiosa A, Vriz O, et al. Preoperative Assessment and Management of Cardiovascular Risk in Patients Undergoing Non-Cardiac Surgery: Implementing a Systematic Stepwise Approach during the COVID-19 Pandemic Era. Journal of Cardiovascular Development and Disease. 2021; 8(10):126. https://doi.org/10.3390/jcdd8100126
Chicago/Turabian StyleBossone, Eduardo, Filippo Cademartiri, Hani AlSergani, Salvatore Chianese, Rahul Mehta, Valentina Capone, Carlo Ruotolo, Imran Hayat Tarrar, Antonio Frangiosa, Olga Vriz, and et al. 2021. "Preoperative Assessment and Management of Cardiovascular Risk in Patients Undergoing Non-Cardiac Surgery: Implementing a Systematic Stepwise Approach during the COVID-19 Pandemic Era" Journal of Cardiovascular Development and Disease 8, no. 10: 126. https://doi.org/10.3390/jcdd8100126