
A Comprehensive Review of Management Strategies for Bicuspid Aortic Valve (BAV): Exploring Epidemiology, Aetiology, Aortopathy, and Interventions in Light of Recent Guidelines
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Epidemiology of Bicuspid Aortic Valve
4. Aetiology of Bicuspid Aortic Valve
4.1. Bicuspid Aortic Valve and Genetic Background
- Function and Dysfunction of Cardiogenesis-Polarization Genes: Notably, genes integral to cardiogenesis, such as GATA and NKX2-5, play a pivotal role. These genes are central to the establishment and proper functioning of the heart.
- Dysregulation of Genes Associated with Neural Crest Cell Migration: Genes like ROBO4, implicated in the regulation of neural crest cell migration, also feature in the genetic context of BAV. Dysfunction here might contribute to anomalies in cardiac development.
- Defects and Disorders in Genes Governing Valve Microenvironment Maintenance: The integrity of the valve microenvironment relies on genes like TGFB2 and TBX. Irregularities in these genes can potentially lead to disruptions in the microenvironment, affecting valve development.
- Gene Aberrations in Structural Aspects of Connective Tissues: Structural issues concerning connective tissues are influenced by gene disorders, including FBN1 deficiency. These genetic irregularities can give rise to problems in the structural integrity of tissues that constitute the cardiovascular system.
4.2. Genetical Background of Bicuspid Aortic Valve and Aorta
4.3. Hemodynamic Features of Bicuspid Aortic Valve
5. Aortic Pathologies and Bicuspid Aortic Valve
5.1. Calcific Aortic Valve Disease
5.2. Aortic Regurgitation
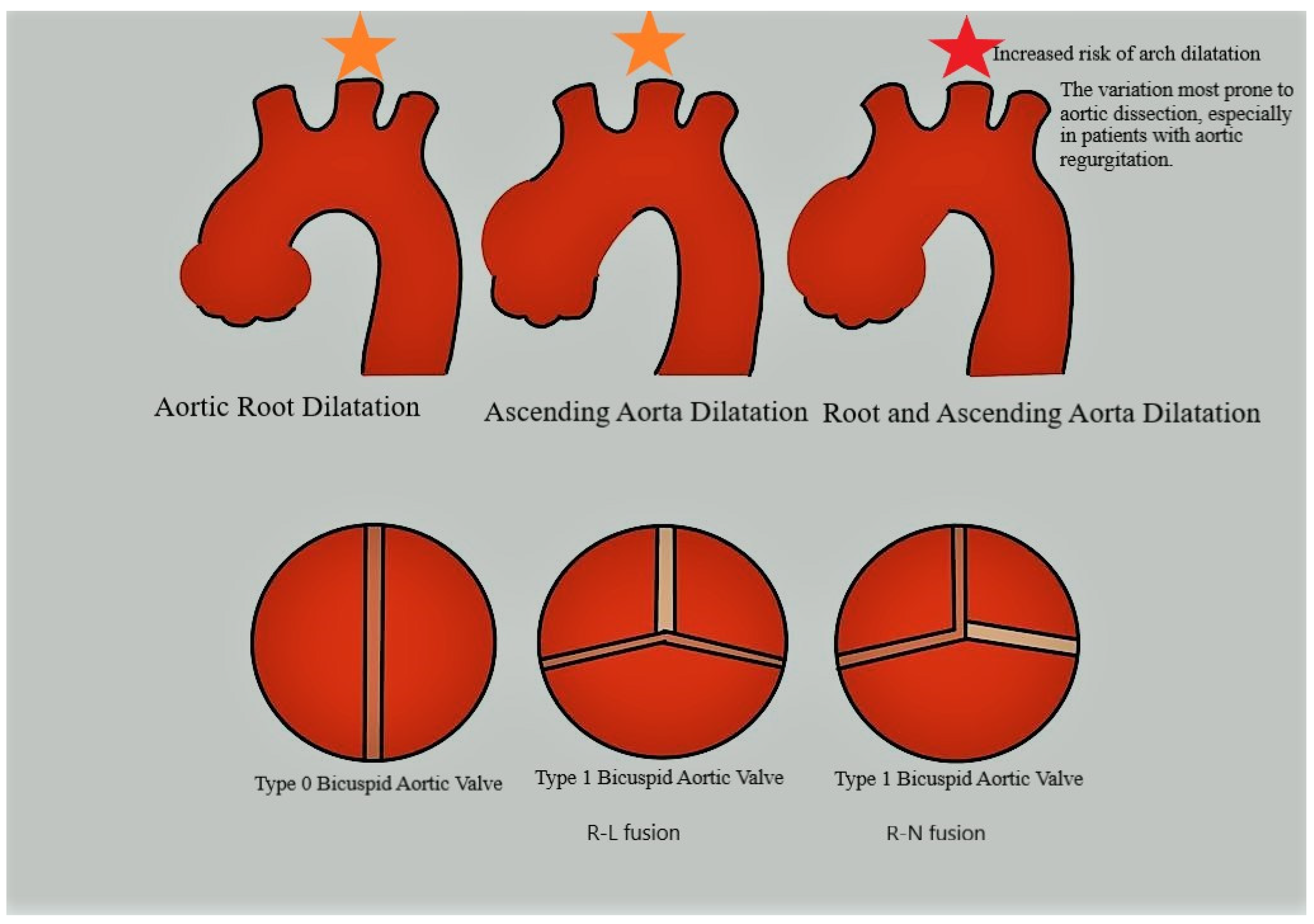
5.3. Aortic Dilation
5.4. Aortic Dissection
6. Bicuspid Aortic Valve Clinical Management in Current Aortic Guidelines
6.1. Familial Screening Recommendations
6.2. Surgical Management of Bicuspid Aortic Valve
6.3. Transcatheter and Rapid Deployment Valves for Bicuspid Aortic Valve
6.4. Management of Bicuspid Aortic Valve-Related Aorthopathy
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Detaint, D.; Michelena, H.I.; Nkomo, V.T.; Vahanian, A.; Jondeau, G.; Sarano, M.E. Aortic dilatation patterns and rates in adults with bicuspid aortic valves: A comparative study with Marfan syndrome and degenerative aortopathy. Heart 2014, 100, 126–134. [Google Scholar] [CrossRef]
- Aluru, J.S.; Barsouk, A.; Saginala, K.; Rawla, P.; Barsouk, A. Valvular Heart Disease Epidemiology. Med. Sci. 2022, 10, 32. [Google Scholar] [CrossRef]
- Bolar, N.; Verstraeten, A.; Van Laer, L.; Loeys, B. Molecular insights into bicuspid aortic valve development and the associated aortopathy. AIMS Mol. Sci. 2017, 4, 478–508. [Google Scholar] [CrossRef]
- Kodolitsch, Y.V.; Kaemmerer, H. Bicuspid aortic valve. In Aortopathy; Springer: Tokyo, Japan, 2017; pp. 229–256. [Google Scholar]
- Michelena, H.I.; Prakash, S.K.; Della Corte, A.; Bissell, M.M.; Anavekar, N.; Mathieu, P.; Bosse, Y.; Limongelli, G.; Bossone, E.; Benson, D.W.; et al. Bicuspid aortic valve: Identifying knowledge gaps and rising to the challenge from the International Bicuspid Aortic Valve Consortium (BAVCon). Circulation 2014, 129, 2691–2704. [Google Scholar] [CrossRef]
- Itagaki, S.; Chikwe, J.P.; Chiang, Y.P.; Egorova, N.N.; Adams, D.H. Long-Term Risk for Aortic Complications After Aortic Valve Replacement in Patients With Bicuspid Aortic Valve Versus Marfan Syndrome. J. Am. Coll. Cardiol. 2015, 65, 2363–2369. [Google Scholar] [CrossRef]
- Junco-Vicente, A.; Del Río-García, Á.; Martín, M.; Rodríguez, I. Update in Biomolecular and Genetic Bases of Bicuspid Aortopathy. Int. J. Mol. Sci. 2021, 22, 5694. [Google Scholar] [CrossRef] [PubMed]
- Girdauskas, E.; Disha, K.; Borger, M.A.; Kuntze, T. Risk of proximal aortic dissection in patients with bicuspid aortic valve: How to address this controversy? Interact. Cardiovasc. Thorac. Surg. 2014, 18, 355–359. [Google Scholar] [CrossRef]
- Kallenbach, K.; Sundt, T.M.; Marwick, T.H. Aortic surgery for ascending aortic aneurysms under 5.0 cm in diameter in the presence of bicuspid aortic valve. JACC Cardiovasc. Imaging 2013, 6, 1321–1326. [Google Scholar] [CrossRef] [PubMed]
- Martín, M.; Lorca, R.; Rozado, J.; Alvarez-Cabo, R.; Calvo, J.; Pascual, I.; Cigarran, H.; Rodriguez, I.; Morís, C. Bicuspid aortic valve syndrome: A multidisciplinary approach for a complex entity. J. Thorac. Dis. 2017, 9 (Suppl. S6), S454. [Google Scholar] [CrossRef] [PubMed]
- Sillesen, A.S.; Vøgg, O.; Pihl, C.; Raja, A.A.; Sundberg, K.; Vedel, C.; Zingenberg, H.; Jørgensen, F.S.; Veljstrup, N.; Iversen, K.; et al. Prevalence of bicuspid aortic valve and associated aortopathy in newborns in Copenhagen, Denmark. JAMA 2021, 325, 561–567. [Google Scholar] [CrossRef] [PubMed]
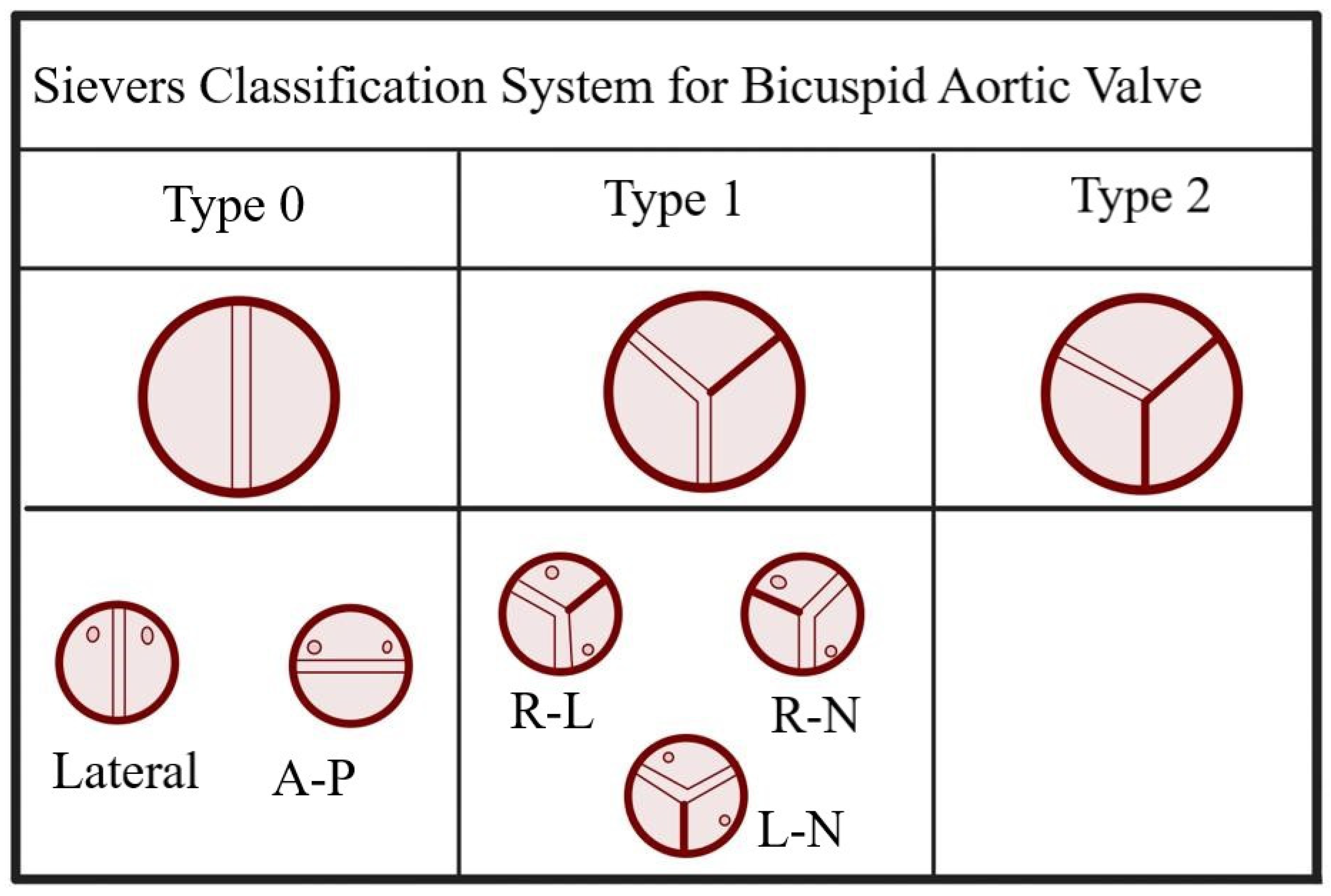
- Sievers, H.H.; Schmidtke, C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J. Thorac. Cardiovasc. Surg. 2007, 133, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Xie, M.; Lv, Q.; Li, Y.; Fang, L.; Zhang, L.; Deng, W.; Wang, J. Bicuspid aortic valve: An update in morphology, genetics, biomarker, complications, imaging diagnosis and treatment. Front. Physiol. 2019, 9, 1921. [Google Scholar] [CrossRef] [PubMed]
- Laforest, B.; Nemer, M. Genetic insights into bicuspid aortic valve formation. Cardiol. Res. Pract. 2012, 2012, 180297. [Google Scholar] [CrossRef]
- Bernard, C.; Morgant, M.C.; Guillier, D.; Cheynel, N.; Bouchot, O. Point on the Aortic Bicuspid Valve. Life 2022, 12, 518. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Jaimes, K.; Prakash, S.K. Genetics in bicuspid aortic valve disease: Where are we? Prog. Cardiovasc. Dis. 2020, 63, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Boureau, A.S.; Karakachoff, M.; Le Scouarnec, S.; Capoulade, R.; Cueff, C.; de Decker, L.; Senage, T.; Verhoye, J.-P.; Baufreton, C.; Roussel, J.-C.; et al. Heritability of aortic valve stenosis and bicuspid enrichment in families with aortic valve stenosis. Int. J. Cardiol. 2022, 359, 91–98. [Google Scholar] [CrossRef]
- Tessler, I.; Leshno, M.; Shmueli, A.; Shpitzen, S.; Durst, R.; Gilon, D. Cost-effectiveness analysis of screening for first-degree relatives of patients with bicuspid aortic valve. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 447–457. [Google Scholar] [CrossRef]
- Escárcega, R.O.; Michelena, H.I.; Bove, A.A. Bicuspid aortic valve: A neglected feature of Shone’s complex? Pediatr. Cardiol. 2014, 35, 186–187. [Google Scholar] [CrossRef]
- Borger, M.A.; Fedak, P.W.; Stephens, E.H.; Gleason, T.G.; Girdauskas, E.; Ikonomidis, J.S.; Khoynezhad, A.; Siu, S.C.; Verma, S.; Hope, M.D.; et al. The American Association for Thoracic Surgery consensus guidelines on bicuspid aortic valve–related aortopathy: Full online-only version. J. Thorac. Cardiovasc. Surg. 2018, 156, e41–e74. [Google Scholar] [CrossRef] [PubMed]
- Donadille, B.; Rousseau, A.; Zenaty, D.; Cabrol, S.; Courtillot, C.; Samara-Boustani, D.; Salenave, S.; Monnier-Cholley, L.; Meuleman, C.; Jondeau, G.; et al. Cardiovascular findings and management in Turner syndrome: Insights from a French cohort. Eur. J. Endocrinol. 2012, 167, 517–522. [Google Scholar] [CrossRef]
- Digilio, M.C.; Gnazzo, M.; Lepri, F.; Dentici, M.L.; Pisaneschi, E.; Baban, A.; Passarelli, C.; Capolino, R.; Angioni, A.; Novelli, A.; et al. Congenital heart defects in molecularly proven Kabuki syndrome patients. Am. J. Med. Genet. Part A 2017, 173, 2912–2922. [Google Scholar] [CrossRef] [PubMed]
- Zapata, H.H.; Sletten, L.J.; Pierpont, M.E.M. Congenital Cardiac Malformations in Adams-Oliver Syndrome. Clin. Genet. 2008, 47, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Hinton, R.B.; Martin, L.J.; Tabangin, M.E.; Mazwi, M.L.; Cripe, L.H.; Benson, D.W. Hypoplastic left heart syndrome is heritable. J. Am. Coll. Cardiol. 2007, 50, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Egbe, A.C.; Crestanello, J.; Miranda, W.R.; Connolly, H.M. Thoracic aortic dissection in tetralogy of Fallot: A review of the National Inpatient Sample Database. J. Am. Heart Assoc. 2019, 8, e011943. [Google Scholar] [CrossRef]
- Patel, N.D.; Crawford, T.; Magruder, J.T.; Alejo, D.E.; Hibino, N.; Black, J.; Dietz, H.C.; Vricella, L.A.; Cameron, D.E. Cardiovascular operations for Loeys-Dietz syndrome: Intermediate-term results. J. Thorac. Cardiovasc. Surg. 2017, 153, 406–412. [Google Scholar] [CrossRef]
- Giusti, B.; Sticchi, E.; De Cario, R.; Magi, A.; Nistri, S.; Pepe, G. Genetic bases of bicuspid aortic valve: The contribution of traditional and high-throughput sequencing approaches on research and diagnosis. Front. Physiol. 2017, 8, 612. [Google Scholar] [CrossRef]
- John, A.S.; McDonald-McGinn, D.M.; Zackai, E.H.; Goldmuntz, E. Aortic root dilation in patients with 22q11.2 deletion syndrome. Am. J. Med. Genet. A 2009, 149A, 939–942. [Google Scholar] [CrossRef]
- Russell, M.W.; Chung, W.K.; Kaltman, J.R.; Miller, T.A. Advances in the understanding of the genetic determinants of congenital heart disease and their impact on clinical outcomes. J. Am. Heart Assoc. 2018, 7, e006906. [Google Scholar] [CrossRef]
- Williams, K.; Carson, J.; Lo, C. Genetics of Congenital Heart Disease. Biomolecules 2019, 9, 879. [Google Scholar] [CrossRef]
- Choudhury, T.Z.; Garg, V. Molecular Genetic Mechanisms of Congenital Heart Disease. Curr. Opin. Genet. Dev. 2022, 75, 101949. [Google Scholar] [CrossRef]
- Gould, R.A.; Aziz, H.; Woods, C.E.; Seman-Senderos, M.A.; Sparks, E.; Preuss, C.; Wünnemann, F.; Bedja, D.; Moats, C.R.; McClymont, S.A.; et al. ROBO4 variants predispose individuals to bicuspid aortic valve and thoracic aortic aneurysm. Nat. Genet. 2019, 51, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Bonachea, E.M.; Chang, S.W.; Zender, G.; LaHaye, S.; Fitzgerald-Butt, S.; McBride, K.L.; Garg, V. Rare GATA5 sequence variants identified in individuals with bicuspid aortic valve. Pediatr. Res. 2014, 76, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Padang, R.; Bagnall, R.D.; Richmond, D.R.; Bannon, P.G.; Semsarian, C. Rare non-synonymous variations in the transcriptional activation domains of GATA5 in bicuspid aortic valve disease. J. Mol. Cell. Cardiol. 2012, 53, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.M.; Tao, J.W.; Qiu, X.B.; Wang, J.; Yuan, F.; Xu, L.; Liu, H.; Li, R.G.; Xu, Y.J.; Wang, Q.; et al. GATA5 loss-of-function mutations associated with congenital bicuspid aortic valve. Int. J. Mol. Med. 2014, 33, 1219–1226. [Google Scholar] [CrossRef]
- Xu, Y.J.; Di, R.M.; Qiao, Q.; Li, X.M.; Huang, R.T.; Xue, S.; Liu, X.Y.; Wang, J.; Yang, Y.Q. GATA6 loss-of-function mutation contributes to congenital bicuspid aortic valve. Gene 2018, 663, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Li, R.G.; Xu, Y.J.; Wang, J.; Liu, X.Y.; Yuan, F.; Huang, R.T.; Xue, S.; Li, L.; Liu, H.; Li, Y.J.; et al. Gata4 loss-of-function mutation and the congenitally bicuspid aortic valve. Am J Cardiol. 2018, 121, 469–474. [Google Scholar] [CrossRef]
- Tessler, I.; Albuisson, J.; Goudot, G.; Carmi, S.; Shpitzen, S.; Messas, E.; Gilon, D.; Durst, R. Bicuspid aortic valve: Genetic and clinical insights. Aorta 2021, 9, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Parker, L.E.; Landstrom, A.P. Genetic Etiology of Left-Sided Obstructive Heart Lesions: A Story in Development. J. Am. Heart Assoc. 2021, 10, e019006. [Google Scholar] [CrossRef]
- Jin, J.Y.; Wu, L.P.; Dong, Y.; Pi, H.C.; Wu, H.F.; Xiang, R. Identification of a novel GATA binding protein 5 variant (c. 830C > T/p. P277L) damaging the nuclear translocation and causing tetralogy of Fallot. QJM Int. J. Med. 2022, 115, 256–258. [Google Scholar] [CrossRef]
- Jaouadi, H.; Gérard, H.; Théron, A.; Collod-Béroud, G.; Collart, F.; Avierinos, J.F.; Zaffran, S. Identification of non-synonymous variations in ROBO1 and GATA5 genes in a family with bicuspid aortic valve disease. J. Hum. Genet. 2022, 67, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Debiec, R.M.; Hamby, S.E.; Jones, P.D.; Safwan, K.; Sosin, M.; Hetherington, S.L.; Sprigings, D.; Sharman, D.; Lee, K.; Salahshouri, P.; et al. Contribution of NOTCH1 genetic variants to bicuspid aortic valve and other congenital lesions. Heart 2022, 108, 1114–1120. [Google Scholar] [CrossRef]
- Abhinav, P.; Zhang, G.F.; Zhao, C.M.; Xu, Y.J.; Wang, J.; Yang, Y.Q. A novel KLF13 mutation underlying congenital patent ductus arteriosus and ventricular septal defect, as well as bicuspid aortic valve. Exp. Ther. Med. 2022, 23, 1–9. [Google Scholar] [CrossRef]
- Theis, J.L.; Niaz, T.; Sundsbak, R.S.; Fogarty, Z.C.; Bamlet, W.R.; Hagler, D.J.; Olson, T.M. CELSR1 risk alleles in familial bicuspid aortic valve and hypoplastic left heart syndrome. Circ. Genom. Precis. Med. 2022, 15, e0035. [Google Scholar] [CrossRef] [PubMed]
- Bonachea, E.M.; Zender, G.; White, P.; Corsmeier, D.; Newsom, D.; Fitzgerald-Butt, S.; Garg, V.; McBride, K.L. Use of a Target-ed, Combinatorial next-Generation Sequencing Approach for the Study of Bicuspid Aortic Valve. BMC Med. Genom. 2014, 7. [Google Scholar] [CrossRef]
- Rashad, S.; Han, X.; Saqr, K.; Tupin, S.; Ohta, M.; Niizuma, K.; Tominaga, T. Epigenetic response of endothelial cells to different wall shear stress magnitudes: A report of new mechano-miRNAs. J. Cell. Physiol. 2020, 235, 7827–7839. [Google Scholar] [CrossRef]
- Cao, K.; Sucosky, P. Predictions of Wall-shear Stress on the Bicuspid Aortic Valves Using Three-dimensional Fluid-structure Interaction Models. Circulation 2014, 130 (Suppl. S2). [Google Scholar]
- Saikrishnan, N.; Yap, C.H.; Milligan, N.C.; Vasilyev, N.V.; Yoganathan, A.P. In vitro characterization of bicuspid aortic valve hemodynamics using particle image velocimetry. Ann. Biomed. Eng. 2012, 40, 1760–1775. [Google Scholar] [CrossRef]
- Charitos, E.I.; Stierle, U.; Petersen, M.; Mohamed, S.A.; Hanke, T.; Schmidtke, C.; Klotz, S.; Sievers, H.H. The fate of the bicuspid valve aortopathy after aortic valve replacement. Eur. J. Cardio-Thorac. Surg. 2014, 45, e128–e135. [Google Scholar] [CrossRef]
- Longi, F.; Orelaru, F.; Clemence, J., Jr.; Naeem, A.; Wu, X.; Yang, B. Outcomes of bicuspid aortic valve thoracic aorta (4.0–4.5 cm) after aortic valve replacement. Ann. Thorac. Surg. 2022, 113, 1521–1528. [Google Scholar] [CrossRef] [PubMed]
- Yip, C.Y.Y.; Simmons, C.A. The aortic valve microenvironment and its role in calcific aortic valve disease. Cardiovasc. Pathol. 2011, 20, 177–182. [Google Scholar] [CrossRef]
- Lee, J.S.; Morrisett, J.D.; Tung, C.H. Detection of hydroxyapatite in calcified cardiovascular tissues. Atherosclerosis 2012, 224, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Lewin, M.B.; Otto, C.M. The bicuspid aortic valve: Adverse outcomes from infancy to old age. Circulation 2005, 111, 832–834. [Google Scholar] [CrossRef] [PubMed]
- Evangelista, A.; Gallego, P.; Calvo-Iglesias, F.; Bermejo, J.; Robledo-Carmona, J.; Sánchez, V.; Saura, D.; Arnold, R.; Carro, A.; Maldonado, G.; et al. Anatomical and clinical predictors of valve dysfunction and aortic dilation in bicuspid aortic valve disease. Heart 2018, 104, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Flint, N.; Wunderlich, N.C.; Shmueli, H.; Ben-Zekry, S.; Siegel, R.J.; Beigel, R. Aortic regurgitation. Curr. Cardiol. Rep. 2019, 21, 65. [Google Scholar] [CrossRef]
- Masri, A.; Svensson, L.G.; Griffin, B.P.; Desai, M.Y. Contemporary natural history of bicuspid aortic valve disease: A systematic review. Heart 2017, 103, 1323–1330. [Google Scholar] [CrossRef]
- Zhu, Y.; Imbrie-Moore, A.M.; Paulsen, M.J.; Priromprintr, B.; Wang, H.; Lucian, H.J.; Farry, J.M.; Woo, Y.J. Novel bicuspid aortic valve model with aortic regurgitation for hemodynamic status analysis using an ex vivo simulator. J. Thorac. Cardiovasc. Surg. 2020. [Google Scholar] [CrossRef]
- Milleron, O.; Masi, P.; Eliahou, L.; Paul, J.F.; Arnoult, F.; Ouali, N.O.; Lansac, E.; Raffoul, R.; Pellenc, Q.; Ou, P.; et al. Aortic Root Anatomy Is Related to the Bicuspid Aortic Valve Phenotype. J. Am. Soc. Echocardiogr. 2022, 35, 278–286. [Google Scholar] [CrossRef]
- Yassine, N.M.; Shahram, J.T.; Body, S.C. Pathogenic mechanisms of bicuspid aortic valve aortopathy. Front. Physiol. 2017, 8, 687. [Google Scholar] [CrossRef] [PubMed]
- Atkins, S.K.; Sucosky, P. Etiology of bicuspid aortic valve disease: Focus on hemodynamics. World J. Cardiol. 2014, 6, 1227. [Google Scholar] [CrossRef]
- Davies, R.R.; Kaple, R.K.; Mandapati, D.; Gallo, A.; Botta, D.M., Jr.; Elefteriades, J.A.; Coady, M.A. Natural history of ascending aortic aneurysms in the setting of an unreplaced bicuspid aortic valve. Ann. Thorac. Surg. 2007, 83, 1338–1344. [Google Scholar] [CrossRef]
- Wilson-Smith, A.R.; Eranki, A.; Muston, B.; Kamalanathan, H.; Yung, A.; Williams, M.L.; Sahai, P.; Zi, C.; Michelena, H. Incidence of bicuspid valve related aortic dissection: A systematic review and meta-analysis. Ann. Cardiothorac. Surg. 2022, 11, 36368. [Google Scholar] [CrossRef] [PubMed]
- Michelena, H.I.; Khanna, A.D.; Mahoney, D.; Margaryan, E.; Topilsky, Y.; Suri, R.M.; Eidem, B.; Edwards, W.D.; Sundt, T.M.; Enriquez-Sarano, M. Incidence of aortic complications in patients with bicuspid aortic valves. JAMA 2011, 306, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Wojnarski, C.M.; Svensson, L.G.; Roselli, E.E.; Idrees, J.J.; Lowry, A.M.; Ehrlinger, J.; Pettersson, G.B.; Gillinov, A.M.; Johnston, D.R.; Soltesz, E.G.; et al. Aortic dissection in patients with bicuspid aortic valve–associated aneurysms. Ann. Thorac. Surg. 2015, 100, 1666–1674. [Google Scholar] [CrossRef]
- Eleid, M.F.; Forde, I.; Edwards, W.D.; Maleszewski, J.J.; Suri, R.M.; Schaff, H.V.; Enriquez-Sarano, M.; Michelena, H.I. Type A aortic dissection in patients with bicuspid aortic valves: Clinical and pathological comparison with tricuspid aortic valves. Heart 2013, 99, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.D.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [PubMed]
- Isselbacher, E.M.; Preventza, O.; Hamilton Black, J.; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; Chen, E.P.; et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guide-lines. Circulation 2022, 146. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease. J. Am. Coll. Cardiol. 2021, 77, e25–e197. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef]
- Kang, D.-H.; Park, S.-J.; Lee, S.-A.; Lee, S.; Kim, D.-H.; Kim, H.-K.; Yun, S.-C.; Hong, G.-R.; Song, J.-M.; Chung, C.-H.; et al. Early surgery or conservative care for asymptomatic aortic stenosis. N. Engl. J. Med. 2020, 382, 111–119. [Google Scholar] [CrossRef]
- Wang, Y.; Jiang, W.; Liu, J.; Li, G.; Liu, Y.; Hu, X.; Dong, N. Early surgery versus conventional treatment for asymptomatic severe aortic regurgitation with normal ejection fraction and left ventricular dilatation. Eur. J. Cardio-Thorac. Surg. 2017, 52, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.H.M.; Chan, J.S.K.; Sanli, D.; Rahimli, R.; Harky, A. Aortic valve repair or replacement in patients with aortic regurgitation: A systematic review and meta-analysis. J. Card. Surg. 2019, 34, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Salcher, M.; Naci, H.; Pender, S.; Kuehne, T. Bicuspid aortic valve disease: Systematic review and meta-analysis of surgical aortic valve repair. Open Heart 2016, 3, e000502. [Google Scholar] [CrossRef] [PubMed]
- Vincent, F.; Ternacle, J.; Denimal, T.; Shen, M.; Redfors, B.; Delhaye, C.; Simonato, M.; Debry, N.; Verdier, B.; Shahim, B.; et al. Transcatheter Aortic Valve Replacement in Bicuspid Aortic Valve Stenosis. Circulation 2021, 143, 1043–1061. [Google Scholar] [CrossRef]
- Saad, M.; Seoudy, H.; Frank, D. Challenging Anatomies for TAVR—Bicuspid and Beyond. Front. Cardiovasc. Med. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.H.L.; Amat-Santos, I.J.; De Backer, O.; Avvedimento, M.; Redondo, A.; Barbanti, M.; Costa, G.; Tchetche, D.; Eltchanioff, H.; Kim, W.-K.; et al. Rationale, Definitions, Techniques, and Outcomes of Commissural Alignment in TAVR. JACC Cardiovasc. Interv. 2022, 15, 1497–1518. [Google Scholar] [CrossRef] [PubMed]
- Merdler, I.; Case, B.; Bhogal, S.; Reddy, P.K.; Sawant, V.; Zhang, C.; Ali, S.; Ben-Dor, I.; Satler, L.F.; Rogers, T.; et al. Early experience with the Evolut FX self-expanding valve vs. Evolut PRO+ for patients with aortic stenosis undergoing TAVR. Cardiovasc. Revascularization Med. 2023. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Montalto, C.; Sticchi, A.; Crimi, G.; Laricchia, A.; Khokhar, A.A.; Giannini, F.; Reimers, B.; Colombo, A.; Latib, A.; Waksman, R.; et al. Outcomes After Transcatheter Aortic Valve Replacement in Bicuspid Versus Tricuspid Anatomy. JACC Cardiovasc. Interv. 2021, 14, 2144–2155. [Google Scholar] [CrossRef]
- Chen, C.-H.J.; Jiang, H.; Martin, O.; Wilson-Smith, A.R. Procedural and clinical outcomes of transcatheter aortic valve replacement in bicuspid aortic valve patients: A systematic review and meta-analysis. Ann. Cardiothorac. Surg. 2022, 11, 351–362. [Google Scholar] [CrossRef] [PubMed]
- He, J.-J.; Xiong, T.-Y.; Yao, Y.-J.; Peng, Y.; Wei, J.-F.; He, S.; Chen, Y.; Li, Q.; Zhao, Z.-G.; Wei, X.; et al. Sex Difference in Outcomes Following Transcatheter Aortic Valve Replacement in Bicuspid Aortic Stenosis. JACC Cardiovasc. Interv. 2022, 15, 1652–1660. [Google Scholar] [CrossRef] [PubMed]
- Miceli, A.; Berretta, P.; Fiore, A.; Andreas, M.; Solinas, M.; Santarpino, G.; Kappert, U.; Misfield, M.; Savini, C.; Albertini, A. Sutureless and rapid deployment implantation in bicuspid aortic valve: Results from the sutureless and rapid-deployment aortic valve replacement international registry. Ann. Cardiothorac. Surg. 2020, 9, 298–304. [Google Scholar] [CrossRef]
- King, M.; Stambulic, T.; Payne, D.; Fernandez, A.L.; El-Diasty, M. The use of sutureless and rapid-deployment aortic valve prosthesis in patients with bicuspid aortic valve: A focused review. J. Card. Surg. 2022, 37, 3355–3362. [Google Scholar] [CrossRef]
- Ouzounian, M.; LeMaire, S.A. How can genetic diagnosis inform the decision of when to operate? J. Vis. Surg. 2018, 4, 68. [Google Scholar] [CrossRef] [PubMed]
- Syrengela, A.-A.; Shahjahan, S.; Bulut, H.I.; Ttofi, I.; Djordjevic, J.; Krasopoulos, G. How Important are Genetics in the Management of Thoracic Aortic Aneurysms and Acute Aortic Syndromes? What do we Know Today? J. Surg. 2023, 8. epub ahead of print. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Syndrome Name | BAV Prevalence * | Reference |
|---|---|---|
| Shone complex | 88% | [19] |
| Ventricular septal defect (VSD) | 30% | [20] |
| Turner syndrome | 21% | [21] |
| Kabuki syndrome | 21% | [22] |
| Adams–Oliver syndrome | 13.3% | [23] |
| Hypoplastic left heart syndrome | 11% | [24] |
| Tetralogy of Fallot | 6.5% | [25] |
| Loesy–Dietz syndrome | 6% | [26] |
| Marfan syndrome | 4.7% | [27] |
| ACTA2 mutated patients | 3% | [20] |
| Velocardiofacial syndrome | 10% | [28] |
| Gene Name | Variations | Reference |
|---|---|---|
| ROBO4 | exon 13(c.2056+1G>T), R64C, A95T, T232M H411G, R568X, R64C, V247A, Y280S, G534Efs49, N622H, A749L, N510V, Ser327Pro | [32,39,41] |
| GATA | GATA4(rs6601627, S337G) GATA5(L233P, S19Y, Y143H, G166S, Y16D, T252P, Q3R, c.830C>T/p. P277L, p. (Gln3Arg)) GATA6(E38X) | [33,34,35,36,37,38,39,40,41] |
| NOTCH1 | 9q34-35, A1343V, P1390T, H1505del R1108x, T596M, P1797H, R1350L, P1377S,.873C>G/p. Tyr291 | [39,42] |
| FBN1 | - | [39] |
| SMAD6 | C484F, P415L, K242NfsX300, Gly166VfsX23, G26_S27del, Y279X, Y288X, V239M, P257L, G271W, G406C, H408Q, R443H | [39] |
| TGFBR2 | V387M | [35] |
| KCNJ2 | R67W | [45] |
| NKX2-5 | K192X | [39] |
| NRF2F | C96X | [39] |
| MCTP2 | L847F, T545M | [39] |
| AXIN1/2 | R841Q, A684V | [39] |
| NFATC1 | P77L, V210M | [39] |
| TBX5 | S372L; V263M | [39] |
| KFL13 | Glu144-mutant | [43] |
| CELSR1 | - | [44] |
| Familial Screening | The American Association for Thoracic Surgery Consensus Guidelines on Bicuspid Aortic Valve–Related Aortopathy [20] | 2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases [66] | 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease [67] | 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease [68] | 2021 ESC/EACTS Guideline for the Management of Valvular Heart Disease [69] |
|---|---|---|---|---|---|
| Class I | - | - | - | - | |
| Class IIa/b | Recommended to screen first-degree relatives of patients with BAV using echocardiography. (Class IIa, level of evidence B) | Recommended to screen first-degree relatives of patients with BAV using transthoracic echocardiography (Class IIa, level of evidence C). | Recommended to screen first-degree relatives of patients with BAV using transthoracic echocardiography (Class IIa, level of evidence B) | Recommended to screen first-degree relatives of patients with BAV using transthoracic echocardiography (Class IIb, level of evidence B). | Recommended to screen first-degree relatives of patients with BAV using transthoracic echocardiography. * |
| 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease [68] | 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease [69] | |
|---|---|---|
| Class I |
| * |
| Class IIa/b |
|
|
| Aortic Surgery | The American Association for Thoracic Surgery Consensus Guidelines on Bicuspid Aortic Valve–Related Aortopathy [20] | 2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases [66] | 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease [67] | 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease [68] | 2021 ESC/EACTS Guideline for the Management of Valvular Heart Disease [69] |
|---|---|---|---|---|---|
| Class I |
|
|
|
| |
| Class II A/B |
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bulut, H.I.; Arjomandi Rad, A.; Syrengela, A.-A.; Ttofi, I.; Djordjevic, J.; Kaur, R.; Keiralla, A.; Krasopoulos, G. A Comprehensive Review of Management Strategies for Bicuspid Aortic Valve (BAV): Exploring Epidemiology, Aetiology, Aortopathy, and Interventions in Light of Recent Guidelines. J. Cardiovasc. Dev. Dis. 2023, 10, 398. https://doi.org/10.3390/jcdd10090398
Bulut HI, Arjomandi Rad A, Syrengela A-A, Ttofi I, Djordjevic J, Kaur R, Keiralla A, Krasopoulos G. A Comprehensive Review of Management Strategies for Bicuspid Aortic Valve (BAV): Exploring Epidemiology, Aetiology, Aortopathy, and Interventions in Light of Recent Guidelines. Journal of Cardiovascular Development and Disease. 2023; 10(9):398. https://doi.org/10.3390/jcdd10090398
Chicago/Turabian StyleBulut, Halil Ibrahim, Arian Arjomandi Rad, Angeliki-Aikaterini Syrengela, Iakovos Ttofi, Jasmina Djordjevic, Ramanjit Kaur, Amar Keiralla, and George Krasopoulos. 2023. "A Comprehensive Review of Management Strategies for Bicuspid Aortic Valve (BAV): Exploring Epidemiology, Aetiology, Aortopathy, and Interventions in Light of Recent Guidelines" Journal of Cardiovascular Development and Disease 10, no. 9: 398. https://doi.org/10.3390/jcdd10090398