
β1 Adrenergic Receptor Autoantibodies and IgG Subclasses: Current Status and Unsolved Issues

 , , ,
, , ,
Abstract
:1. Introduction
2. The Basic Aspects of β1AR-AAb
3. β1AR-AAbs in Human DCM
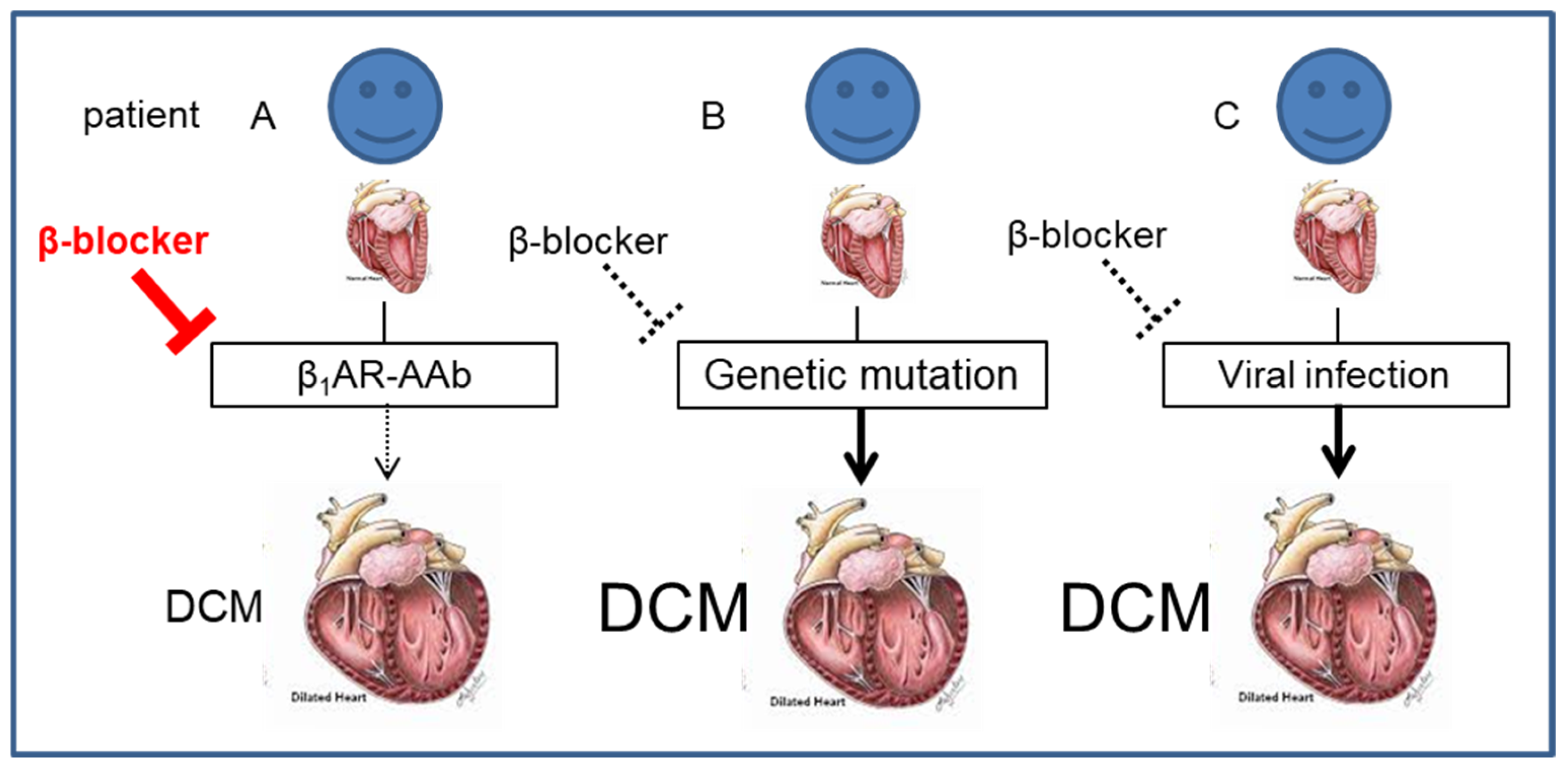
4. The Association of β-Blocker Therapy with β1AR-AAbs Mediating Pathophysiology
5. The Findings from Immunoadsorption Therapy: Proof of Concept
6. Controversy in β1AR-AAbs
7. IgG Subclasses of β1AR-AAbs
8. β1AR-AAbs in the Other Cardiac Diseases
9. Future Perspective
10. Translational Outlook
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maron, B.J.; Towbin, J.A.; Thiene, G.; Antzelevitch, C.; Corrado, D.; Arnett, D.; Moss, A.J.; Seidman, C.E.; Young, J.B. Contemporary definitions and classification of the cardiomyopathies: An American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 2006, 113, 1807–1816. [Google Scholar] [CrossRef]
- Mestroni, L.; Krajinovic, M.; Severini, G.M.; Pinamonti, B.; Di Lenarda, A.; Giacca, M.; Falaschi, A.; Camerini, F. Familial dilated cardiomyopathy. Br. Heart J. 1994, 72, S35–S41. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.; Grazzini, M.; Mann, J.M.; Keeling, P.J.; Bottazzo, G.F.; McKenna, W.J.; Schiaffino, S. Identification of alpha- and beta-cardiac myosin heavy chain isoforms as major autoantigens in dilated cardiomyopathy. Circulation 1992, 85, 1734–1742. [Google Scholar] [CrossRef]
- Schultheiss, H.P.; Schulze, K.; Schauer, R.; Witzenbichler, B.; Strauer, B.E. Antibody-mediated imbalance of myocardial energy metabolism. A causal factor of cardiac failure? Circ. Res. 1995, 76, 64–72. [Google Scholar] [CrossRef]
- Limas, C.J.; Goldenberg, I.F.; Limas, C. Autoantibodies against beta-adrenoceptors in human idiopathic dilated cardiomyopathy. Circ. Res. 1989, 64, 97–103. [Google Scholar] [CrossRef]
- Caforio, A.L.; Goldman, J.H.; Baig, M.K.; Haven, A.J.; Dalla Libera, L.; Keeling, P.J.; McKenna, W.J. Cardiac autoantibodies in dilated cardiomyopathy become undetectable with disease progression. Heart 1997, 77, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.H.; Keeling, P.J.; Warraich, R.S.; Baig, M.K.; Redwood, S.R.; Dalla Libera, L.; Sanderson, J.E.; Caforio, A.L.; McKenna, W.J. Autoimmunity to alpha myosin in a subset of patients with idiopathic dilated cardiomyopathy. Br. Heart J. 1995, 74, 598–603. [Google Scholar] [CrossRef]
- Iwata, M.; Yoshikawa, T.; Baba, A.; Anzai, T.; Nakamura, I.; Wainai, Y.; Takahashi, T.; Ogawa, S. Autoimmunity against the second extracellular loop of beta(1)-adrenergic receptors induces beta-adrenergic receptor desensitization and myocardial hypertrophy in vivo. Circ. Res. 2001, 88, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, Y.; Marullo, S.; Hoyer, S.; Waagstein, F.; Andersson, B.; Vahlne, A.; Guillet, J.G.; Strosberg, A.D.; Hjalmarson, A.; Hoebeke, J. Mapping of a functional autoimmune epitope on the beta 1-adrenergic receptor in patients with idiopathic dilated cardiomyopathy. J. Clin. Investig. 1990, 86, 1658–1663. [Google Scholar] [CrossRef]
- Magnusson, Y.; Wallukat, G.; Waagstein, F.; Hjalmarson, A.; Hoebeke, J. Autoimmunity in idiopathic dilated cardiomyopathy. Characterization of antibodies against the beta 1-adrenoceptor with positive chronotropic effect. Circulation 1994, 89, 2760–2767. [Google Scholar] [CrossRef]
- Magnusson, Y.; Hjalmarson, A.; Hoebeke, J. Beta 1-adrenoceptor autoimmunity in cardiomyopathy. Int. J. Cardiol. 1996, 54, 137–141. [Google Scholar] [CrossRef]
- Jahns, R.; Boivin, V.; Siegmund, C.; Inselmann, G.; Lohse, M.J.; Boege, F. Autoantibodies activating human beta1-adrenergic receptors are associated with reduced cardiac function in chronic heart failure. Circulation 1999, 99, 649–654. [Google Scholar] [CrossRef]
- Sterin-Borda, L.; Gorelik, G.; Borda, E.S. Chagasic IgG binding with cardiac muscarinic cholinergic receptors modifies cholinergic-mediated cellular transmembrane signals. Clin. Immunol. Immunopathol. 1991, 61, 387–397. [Google Scholar] [CrossRef]
- Fu, L.X.; Magnusson, Y.; Bergh, C.H.; Liljeqvist, J.A.; Waagstein, F.; Hjalmarson, A.; Hoebeke, J. Localization of a functional autoimmune epitope on the muscarinic acetylcholine receptor-2 in patients with idiopathic dilated cardiomyopathy. J. Clin. Investig. 1993, 91, 1964–1968. [Google Scholar] [CrossRef] [PubMed]
- Wallukat, G.; Fu, H.M.; Matsui, S.; Hjalmarson, A.; Fu, M.L. Autoantibodies against M2 muscarinic receptors in patients with cardiomyopathy display non-desensitized agonist-like effects. Life Sci. 1999, 64, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Baba, A.; Yoshikawa, T.; Fukuda, Y.; Sugiyama, T.; Shimada, M.; Akaishi, M.; Tsuchimoto, K.; Ogawa, S.; Fu, M. Autoantibodies against M2-muscarinic acetylcholine receptors: New upstream targets in atrial fibrillation in patients with dilated cardiomyopathy. Eur. Heart J. 2004, 25, 1108–1115. [Google Scholar] [CrossRef]
- Del Corsso, C.; de Carvalho, A.C.; Martino, H.F.; Varanda, W.A. Sera from patients with idiopathic dilated cardiomyopathy decrease ICa in cardiomyocytes isolated from rabbits. Am. J. Physiol. Heart Circ. Physiol. 2004, 287, H1928–H1936. [Google Scholar] [CrossRef] [PubMed]
- Shmilovich, H.; Danon, A.; Binah, O.; Roth, A.; Chen, G.; Wexler, D.; Keren, G.; George, J. Autoantibodies to cardiac troponin I in patients with idiopathic dilated and ischemic cardiomyopathy. Int. J. Cardiol. 2007, 117, 198–203. [Google Scholar] [CrossRef]
- Doesch, A.O.; Mueller, S.; Nelles, M.; Konstandin, M.; Celik, S.; Frankenstein, L.; Goeser, S.; Kaya, Z.; Koch, A.; Zugck, C.; et al. Impact of troponin I-autoantibodies in chronic dilated and ischemic cardiomyopathy. Basic Res. Cardiol. 2011, 106, 25–35. [Google Scholar] [CrossRef]
- Halley, C.M.; Lappe, J.M.; Cotleur, A.C.; Shrestha, K.; Borowski, A.G.; Pelfrey, C.; Ransohoff, R.; Tang, W.H. Antiinflammatory autoimmune cellular responses to cardiac troponin I in idiopathic dilated cardiomyopathy. J. Card. Fail. 2011, 17, 359–365. [Google Scholar] [CrossRef]
- Miettinen, K.H.; Eriksson, S.; Magga, J.; Tuomainen, P.; Kuusisto, J.; Vanninen, E.J.; Turpeinen, A.; Punnonen, K.R.; Pettersson, K.; Peuhkurinen, K.J. Clinical significance of troponin I efflux and troponin autoantibodies in patients with dilated cardiomyopathy. J. Card. Fail. 2008, 14, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Nagatomo, Y.; Tang, W.H. Autoantibodies and cardiovascular dysfunction: Cause or consequence? Curr. Heart Fail. Rep. 2014, 11, 500–508. [Google Scholar] [CrossRef]
- Ferrari, I.; Levin, M.J.; Wallukat, G.; Elies, R.; Lebesgue, D.; Chiale, P.; Elizari, M.; Rosenbaum, M.; Hoebeke, J. Molecular mimicry between the immunodominant ribosomal protein P0 of Trypanosoma cruzi and a functional epitope on the human beta 1-adrenergic receptor. J. Exp. Med. 1995, 182, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Smulski, C.; Labovsky, V.; Levy, G.; Hontebeyrie, M.; Hoebeke, J.; Levin, M.J. Structural basis of the cross-reaction between an antibody to the Trypanosoma cruzi ribosomal P2beta protein and the human beta1 adrenergic receptor. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2006, 20, 1396–1406. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Y.; Chen, M.; Zhao, W.; Wang, X.; Wang, H.; Zhang, Z.; Zhang, J.; Xu, L.; Chen, J.; et al. The correlation between peripartum cardiomyopathy and autoantibodies against cardiovascular receptors. PLoS ONE 2014, 9, e86770. [Google Scholar] [CrossRef]
- Stork, S.; Boivin, V.; Horf, R.; Hein, L.; Lohse, M.J.; Angermann, C.E.; Jahns, R. Stimulating autoantibodies directed against the cardiac beta1-adrenergic receptor predict increased mortality in idiopathic cardiomyopathy. Am. Heart J. 2006, 152, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Nagatomo, Y.; Li, D.; Kirsop, J.; Borowski, A.; Thakur, A.; Tang, W.H. Autoantibodies Specifically Against β1 Adrenergic Receptors and Adverse Clinical Outcome in Patients With Chronic Systolic Heart Failure in the β-Blocker Era: The Importance of Immunoglobulin G3 Subclass. J. Card. Fail. 2016, 22, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Chen, Y.; Wan, Z.; Zhou, D.; Ma, A. The prognostic value of autoantibodies against β1-adrenoceptor and cardiac troponin-I for clinical outcomes in STEMI. J. Cardiovasc. Med. 2017, 18, 34–41. [Google Scholar] [CrossRef]
- Brisinda, D.; Sorbo, A.R.; Venuti, A.; Ruggieri, M.P.; Manna, R.; Fenici, P.; Wallukat, G.; Hoebeke, J.; Frustaci, A.; Fenici, R. Anti-β-adrenoceptors autoimmunity causing ‘idiopathic’ arrhythmias and cardiomyopathy. Circ. J. Off. J. Jpn. Circ. Soc. 2012, 76, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Fedorowski, A.; Li, H.; Yu, X.; Koelsch, K.A.; Harris, V.M.; Liles, C.; Murphy, T.A.; Quadri, S.M.S.; Scofield, R.H.; Sutton, R.; et al. Antiadrenergic autoimmunity in postural tachycardia syndrome. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2017, 19, 1211–1219. [Google Scholar] [CrossRef]
- Becker, N.P.; Müller, J.; Göttel, P.; Wallukat, G.; Schimke, I. Cardiomyopathy—An approach to the autoimmune background. Autoimmun. Rev. 2017, 16, 269–286. [Google Scholar] [CrossRef]
- Schulze, W.; Kunze, R.; Wallukat, G. Pathophysiological role of autoantibodies against G-protein-coupled receptors in the cardiovascular system. Exp. Clin. Cardiol. 2005, 10, 170–172. [Google Scholar] [PubMed]
- Wallukat, G.; Wollenberger, A.; Morwinski, R.; Pitschner, H.F. Anti-beta 1-adrenoceptor autoantibodies with chronotropic activity from the serum of patients with dilated cardiomyopathy: Mapping of epitopes in the first and second extracellular loops. J. Mol. Cell. Cardiol. 1995, 27, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Nikolaev, V.O.; Boivin, V.; Störk, S.; Angermann, C.E.; Ertl, G.; Lohse, M.J.; Jahns, R. A novel fluorescence method for the rapid detection of functional beta1-adrenergic receptor autoantibodies in heart failure. J. Am. Coll. Cardiol. 2007, 50, 423–431. [Google Scholar] [CrossRef]
- Mobini, R.; Magnusson, Y.; Wallukat, G.; Viguier, M.; Hjalmarson, A.; Hoebeke, J. Probing the immunological properties of the extracellular domains of the human beta(1)-adrenoceptor. J. Autoimmun. 1999, 13, 179–186. [Google Scholar] [CrossRef]
- Mobini, R.; Fu, M.; Wallukat, G.; Magnusson, Y.; Hjalmarson, A.; Hoebeke, J. A monoclonal antibody directed against an autoimmune epitope on the human beta1-adrenergic receptor recognized in idiopathic dilated cardiomyopathy. Hybridoma 2000, 19, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Staudt, A.; Mobini, R.; Fu, M.; Grosse, Y.; Stangl, V.; Stangl, K.; Thiele, A.; Baumann, G.; Felix, S.B. beta(1)-Adrenoceptor antibodies induce positive inotropic response in isolated cardiomyocytes. Eur. J. Pharmacol. 2001, 423, 115–119. [Google Scholar] [CrossRef]
- Podlowski, S.; Luther, H.P.; Morwinski, R.; Muller, J.; Wallukat, G. Agonistic anti-beta1-adrenergic receptor autoantibodies from cardiomyopathy patients reduce the beta1-adrenergic receptor expression in neonatal rat cardiomyocytes. Circulation 1998, 98, 2470–2476. [Google Scholar] [CrossRef]
- Jahns, R.; Boivin, V.; Krapf, T.; Wallukat, G.; Boege, F.; Lohse, M.J. Modulation of beta1-adrenoceptor activity by domain-specific antibodies and heart failure-associated autoantibodies. J. Am. Coll. Cardiol. 2000, 36, 1280–1287. [Google Scholar] [CrossRef]
- Staudt, Y.; Mobini, R.; Fu, M.; Felix, S.B.; Kuhn, J.P.; Staudt, A. Beta1-adrenoceptor antibodies induce apoptosis in adult isolated cardiomyocytes. Eur. J. Pharmacol. 2003, 466, 1–6. [Google Scholar] [CrossRef]
- Fukuda, Y.; Miyoshi, S.; Tanimoto, K.; Oota, K.; Fujikura, K.; Iwata, M.; Baba, A.; Hagiwara, Y.; Yoshikawa, T.; Mitamura, H.; et al. Autoimmunity against the second extracellular loop of beta(1)-adrenergic receptors induces early afterdepolarization and decreases in K-channel density in rabbits. J. Am. Coll. Cardiol. 2004, 43, 1090–1100. [Google Scholar] [CrossRef]
- Christ, T.; Wettwer, E.; Dobrev, D.; Adolph, E.; Knaut, M.; Wallukat, G.; Ravens, U. Autoantibodies against the beta1 adrenoceptor from patients with dilated cardiomyopathy prolong action potential duration and enhance contractility in isolated cardiomyocytes. J. Mol. Cell. Cardiol. 2001, 33, 1515–1525. [Google Scholar] [CrossRef] [PubMed]
- Medei, E.H.; Nascimento, J.H.; Pedrosa, R.C.; Barcellos, L.; Masuda, M.O.; Sicouri, S.; Elizari, M.V.; de Carvalho, A.C. Antibodies with beta-adrenergic activity from chronic chagasic patients modulate the QT interval and M cell action potential duration. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2008, 10, 868–876. [Google Scholar] [CrossRef]
- Matsui, S.; Fu, M.L.; Hayase, M.; Katsuda, S.; Yamaguchi, N.; Teraoka, K.; Kurihara, T.; Takekoshi, N. Active immunization of combined beta1-adrenoceptor and M2-muscarinic receptor peptides induces cardiac hypertrophy in rabbits. J. Card. Fail. 1999, 5, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Zuo, L.; Bao, H.; Tian, J.; Wang, X.; Zhang, S.; He, Z.; Yan, L.; Zhao, R.; Ma, X.L.; Liu, H. Long-term active immunization with a synthetic peptide corresponding to the second extracellular loop of β1-adrenoceptor induces both morphological and functional cardiomyopathic changes in rats. Int. J. Cardiol. 2011, 149, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Jane-wit, D.; Altuntas, C.Z.; Johnson, J.M.; Yong, S.; Wickley, P.J.; Clark, P.; Wang, Q.; Popović, Z.B.; Penn, M.S.; Damron, D.S.; et al. Beta 1-adrenergic receptor autoantibodies mediate dilated cardiomyopathy by agonistically inducing cardiomyocyte apoptosis. Circulation 2007, 116, 399–410. [Google Scholar] [CrossRef]
- Abdelkrim, M.A.; Noireaud, J.; Chatagnon, G.; Gogny, M.; Desfontis, J.C.; Mallem, M.Y. Antibodies against the second extracellular loop of beta1-adrenergic receptor induce aortic endothelial dysfunction in Wistar rat. Ann. Cardiol. D’angeiol. 2012, 61, 167–172. [Google Scholar] [CrossRef]
- Torre-Amione, G.; Orrego, C.M.; Khalil, N.; Kottner-Assad, C.; Leveque, C.; Celis, R.; Youker, K.A.; Estep, J.D. Therapeutic plasma exchange a potential strategy for patients with advanced heart failure. J. Clin. Apher. 2010, 25, 323–330. [Google Scholar] [CrossRef]
- Dandel, M.; Weng, Y.; Siniawski, H.; Potapov, E.; Drews, T.; Lehmkuhl, H.B.; Knosalla, C.; Hetzer, R. Prediction of cardiac stability after weaning from left ventricular assist devices in patients with idiopathic dilated cardiomyopathy. Circulation 2008, 118, S94–S105. [Google Scholar] [CrossRef]
- Iwata, M.; Yoshikawa, T.; Baba, A.; Anzai, T.; Mitamura, H.; Ogawa, S. Autoantibodies against the second extracellular loop of beta1-adrenergic receptors predict ventricular tachycardia and sudden death in patients with idiopathic dilated cardiomyopathy. J. Am. Coll. Cardiol. 2001, 37, 418–424. [Google Scholar] [CrossRef]
- Zhang, L.; Hu, D.; Li, J.; Wu, Y.; Liu, X.; Yang, X. Autoantibodies against the myocardial beta1-adrenergic and M2-muscarinic receptors in patients with congestive heart failure. Chin. Med. J. 2002, 115, 1127–1131. [Google Scholar]
- Miao, G.B.; Liu, J.C.; Liu, M.B.; Wu, J.L.; Zhang, G.; Chang, J.; Zhang, L. Autoantibody against beta1-adrenergic receptor and left ventricular remodeling changes in response to metoprolol treatment. Eur. J. Clin. Investig. 2006, 36, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Nagatomo, Y.; Yoshikawa, T.; Kohno, T.; Yoshizawa, A.; Baba, A.; Anzai, T.; Meguro, T.; Satoh, T.; Ogawa, S. A pilot study on the role of autoantibody targeting the beta1-adrenergic receptor in the response to beta-blocker therapy for congestive heart failure. J. Card. Fail. 2009, 15, 224–232. [Google Scholar] [CrossRef]
- Nagatomo, Y.; Yoshikawa, T.; Okamoto, H.; Kitabatake, A.; Hori, M. Presence of autoantibody directed against β1-adrenergic receptors is associated with amelioration of cardiac function in response to carvedilol: Japanese Chronic Heart Failure (J-CHF) Study. J. Card. Fail. 2015, 21, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Pei, J.; Li, N.; Chen, J.; Li, X.; Zhang, Y.; Wang, Z.; Zhang, P.; Cao, K.; Pu, J. The predictive values of beta1-adrenergic and M2 muscarinic receptor autoantibodies for sudden cardiac death in patients with chronic heart failure. Eur. J. Heart Fail. 2012, 14, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Markousis-Mavrogenis, G.; Minich, W.B.; Al-Mubarak, A.A.; Anker, S.D.; Cleland, J.G.F.; Dickstein, K.; Lang, C.C.; Ng, L.L.; Samani, N.J.; Zannad, F.; et al. Clinical and prognostic associations of autoantibodies recognizing adrenergic/muscarinic receptors in patients with heart failure. Cardiovasc. Res. 2023, 119, 1690–1705. [Google Scholar] [CrossRef]
- Nagatomo, Y.; McNamara, D.M.; Alexis, J.D.; Cooper, L.T.; Dec, G.W.; Pauly, D.F.; Sheppard, R.; Starling, R.C.; Tang, W.H. Myocardial Recovery in Patients With Systolic Heart Failure and Autoantibodies Against β(1)-Adrenergic Receptors. J. Am. Coll. Cardiol. 2017, 69, 968–977. [Google Scholar] [CrossRef]
- The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): A randomised trial. Lancet 1999, 353, 9–13. [CrossRef]
- Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999, 353, 2001–2007. [CrossRef]
- Packer, M.; Fowler, M.B.; Roecker, E.B.; Coats, A.J.; Katus, H.A.; Krum, H.; Mohacsi, P.; Rouleau, J.L.; Tendera, M.; Staiger, C.; et al. Effect of carvedilol on the morbidity of patients with severe chronic heart failure: Results of the carvedilol prospective randomized cumulative survival (COPERNICUS) study. Circulation 2002, 106, 2194–2199. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Yan, L.; Wang, J.; Zhan, W.; Song, K.; Han, X.; Li, X.; Cao, J.; Liu, H. β1-Adrenoceptor autoantibodies from DCM patients enhance the proliferation of T lymphocytes through the β1-AR/cAMP/PKA and p38 MAPK pathways. PLoS ONE 2012, 7, e52911. [Google Scholar] [CrossRef] [PubMed]
- Dörffel, W.V.; Felix, S.B.; Wallukat, G.; Brehme, S.; Bestvater, K.; Hofmann, T.; Kleber, F.X.; Baumann, G.; Reinke, P. Short-term hemodynamic effects of immunoadsorption in dilated cardiomyopathy. Circulation 1997, 95, 1994–1997. [Google Scholar] [CrossRef]
- Felix, S.B.; Staudt, A.; Dörffel, W.V.; Stangl, V.; Merkel, K.; Pohl, M.; Döcke, W.D.; Morgera, S.; Neumayer, H.H.; Wernecke, K.D.; et al. Hemodynamic effects of immunoadsorption and subsequent immunoglobulin substitution in dilated cardiomyopathy: Three-month results from a randomized study. J. Am. Coll. Cardiol. 2000, 35, 1590–1598. [Google Scholar] [CrossRef]
- Müller, J.; Wallukat, G.; Dandel, M.; Bieda, H.; Brandes, K.; Spiegelsberger, S.; Nissen, E.; Kunze, R.; Hetzer, R. Immunoglobulin adsorption in patients with idiopathic dilated cardiomyopathy. Circulation 2000, 101, 385–391. [Google Scholar] [CrossRef]
- Knebel, F.; Böhm, M.; Staudt, A.; Borges, A.C.; Tepper, M.; Jochmann, N.; Wernicke, K.D.; Felix, S.; Baumann, G. Reduction of morbidity by immunoadsorption therapy in patients with dilated cardiomyopathy. Int. J. Cardiol. 2004, 97, 517–520. [Google Scholar] [CrossRef]
- Dörffel, W.V.; Wallukat, G.; Dörffel, Y.; Felix, S.B.; Baumann, G. Immunoadsorption in idiopathic dilated cardiomyopathy, a 3-year follow-up. Int. J. Cardiol. 2004, 97, 529–534. [Google Scholar] [CrossRef]
- Camino, M.; Morales, M.D. Beta(1)-adrenergic receptor antibodies in children with dilated cardiomyopathy. Front. Biosci. 2019, 11, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Dandel, M.; Wallukat, G.; Englert, A.; Lehmkuhl, H.B.; Knosalla, C.; Hetzer, R. Long-term benefits of immunoadsorption in β(1)-adrenoceptor autoantibody-positive transplant candidates with dilated cardiomyopathy. Eur. J. Heart Fail. 2012, 14, 1374–1388. [Google Scholar] [CrossRef]
- Wallukat, G.; Müller, J.; Hetzer, R. Specific removal of beta1-adrenergic autoantibodies from patients with idiopathic dilated cardiomyopathy. New Engl. J. Med. 2002, 347, 1806. [Google Scholar] [CrossRef] [PubMed]
- Schimke, I.; Muller, J.; Dandel, M.; Gremmels, H.D.; Bayer, W.; Wallukat, B.; Wallukat, G.; Hetzer, R. Reduced oxidative stress in parallel to improved cardiac performance one year after selective removal of anti-beta 1-adrenoreceptor autoantibodies in patients with idiopathic dilated cardiomyopathy: Data of a preliminary study. J. Clin. Apher. 2005, 20, 137–142. [Google Scholar] [CrossRef]
- Stavrakis, S.; Kem, D.C.; Patterson, E.; Lozano, P.; Huang, S.; Szabo, B.; Cunningham, M.W.; Lazzara, R.; Yu, X. Opposing cardiac effects of autoantibody activation of β-adrenergic and M2 muscarinic receptors in cardiac-related diseases. Int. J. Cardiol. 2011, 148, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Nagatomo, Y.; Baba, A.; Ito, H.; Naito, K.; Yoshizawa, A.; Kurita, Y.; Nakamura, I.; Monkawa, T.; Matsubara, T.; Wakabayashi, Y.; et al. Specific immunoadsorption therapy using a tryptophan column in patients with refractory heart failure due to dilated cardiomyopathy. J. Clin. Apher. 2011, 26, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; Baba, A.; Akaishi, M.; Wakabayashi, Y.; Monkawa, T.; Kitakaze, M.; Izumi, T.; Tomoike, H. Immunoadsorption therapy for dilated cardiomyopathy using tryptophan column-A prospective, multicenter, randomized, within-patient and parallel-group comparative study to evaluate efficacy and safety. J. Clin. Apher. 2016, 31, 535–544. [Google Scholar] [CrossRef]
- Cooper, L.T.; Belohlavek, M.; Korinek, J.; Yoshifuku, S.; Sengupta, P.P.; Burgstaler, E.A.; Winters, J.L. A pilot study to assess the use of protein a immunoadsorption for chronic dilated cardiomyopathy. J. Clin. Apher. 2007, 22, 210–214. [Google Scholar] [CrossRef]
- Mobini, R.; Staudt, A.; Felix, S.B.; Baumann, G.; Wallukat, G.; Deinum, J.; Svensson, H.; Hjalmarson, A.; Fu, M. Hemodynamic improvement and removal of autoantibodies against beta1-adrenergic receptor by immunoadsorption therapy in dilated cardiomyopathy. J. Autoimmun. 2003, 20, 345–350. [Google Scholar] [CrossRef]
- Staudt, A.; Bohm, M.; Knebel, F.; Grosse, Y.; Bischoff, C.; Hummel, A.; Dahm, J.B.; Borges, A.; Jochmann, N.; Wernecke, K.D.; et al. Potential role of autoantibodies belonging to the immunoglobulin G-3 subclass in cardiac dysfunction among patients with dilated cardiomyopathy. Circulation 2002, 106, 2448–2453. [Google Scholar] [CrossRef] [PubMed]
- Staudt, A.; Dörr, M.; Staudt, Y.; Böhm, M.; Probst, M.; Empen, K.; Plötz, S.; Maschke, H.E.; Hummel, A.; Baumann, G.; et al. Role of immunoglobulin G3 subclass in dilated cardiomyopathy: Results from protein A immunoadsorption. Am. Heart J. 2005, 150, 729–736. [Google Scholar] [CrossRef]
- Baba, A.; Akaishi, M.; Shimada, M.; Monkawa, T.; Wakabayashi, Y.; Takahashi, M.; Nagatomo, Y.; Yoshikawa, T. Complete elimination of cardiodepressant IgG3 autoantibodies by immunoadsorption in patients with severe heart failure. Circ. J. Off. J. Jpn. Circ. Soc. 2010, 74, 1372–1378. [Google Scholar] [CrossRef]
- Jahns, R.; Boivin, V.; Siegmund, C.; Boege, F.; Lohse, M.J.; Inselmann, G. Activating beta-1-adrenoceptor antibodies are not associated with cardiomyopathies secondary to valvular or hypertensive heart disease. J. Am. Coll. Cardiol. 1999, 34, 1545–1551. [Google Scholar] [CrossRef]
- Bornholz, B.; Weidtkamp-Peters, S.; Schmitmeier, S.; Seidel, C.A.; Herda, L.R.; Felix, S.B.; Lemoine, H.; Hescheler, J.; Nguemo, F.; Schafer, C.; et al. Impact of human autoantibodies on beta1-adrenergic receptor conformation, activity, and internalization. Cardiovasc. Res. 2013, 97, 472–480. [Google Scholar] [CrossRef]
- Xu, B.Y.; Pirskanen, R.; Lefvert, A.K. Antibodies against beta1 and beta2 adrenergic receptors in myasthenia gravis. J. Neuroimmunol. 1998, 91, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Fujii, H.; Sato, W.; Kimura, Y.; Matsuda, H.; Ota, M.; Maikusa, N.; Suzuki, F.; Amano, K.; Shin, I.; Yamamura, T.; et al. Altered Structural Brain Networks Related to Adrenergic/Muscarinic Receptor Autoantibodies in Chronic Fatigue Syndrome. J. Neuroimaging Off. J. Am. Soc. Neuroimaging 2020, 30, 822–827. [Google Scholar] [CrossRef]
- Segovia, M.; Ganzinelli, S.; Reina, S.; Borda, E.; Sterin-Borda, L. Role of anti-β1 adrenergic antibodies from patients with periodontitis in cardiac dysfunction. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2012, 41, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Reina, S.; Ganzinelli, S.; Sterin-Borda, L.; Borda, E. Pro-apoptotic effect of anti-β1-adrenergic receptor antibodies in periodontitis patients. Int. Immunopharmacol. 2012, 14, 710–721. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, M.; Swanson, M.C.; Gleich, G.J.; Kita, H. Allergen-specific IgG1 and IgG3 through Fc gamma RII induce eosinophil degranulation. J. Clin. Investig. 1995, 95, 2813–2821. [Google Scholar] [CrossRef]
- Mijares, A.; Lebesgue, D.; Wallukat, G.; Hoebeke, J. From agonist to antagonist: Fab fragments of an agonist-like monoclonal anti-beta(2)-adrenoceptor antibody behave as antagonists. Mol. Pharmacol. 2000, 58, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Staudt, A.; Eichler, P.; Trimpert, C.; Felix, S.B.; Greinacher, A. Fc(gamma) receptors IIa on cardiomyocytes and their potential functional relevance in dilated cardiomyopathy. J. Am. Coll. Cardiol. 2007, 49, 1684–1692. [Google Scholar] [CrossRef]
- Staudt, A.; Herda, L.R.; Trimpert, C.; Lubenow, L.; Landsberger, M.; Dörr, M.; Hummel, A.; Eckerle, L.G.; Beug, D.; Müller, C.; et al. Fcgamma-receptor IIa polymorphism and the role of immunoadsorption in cardiac dysfunction in patients with dilated cardiomyopathy. Clin. Pharmacol. Ther. 2010, 87, 452–458. [Google Scholar] [CrossRef]
- Ernst, D.; Westerbergh, J.; Sogkas, G.; Jablonka, A.; Ahrenstorf, G.; Schmidt, R.E.; Heidecke, H.; Wallentin, L.; Riemekasten, G.; Witte, T. Lowered anti-beta1 adrenergic receptor antibody concentrations may have prognostic significance in acute coronary syndrome. Sci. Rep. 2019, 9, 14552. [Google Scholar] [CrossRef]
- Chiale, P.A.; Garro, H.A.; Schmidberg, J.; Sánchez, R.A.; Acunzo, R.S.; Lago, M.; Levy, G.; Levin, M. Inappropriate sinus tachycardia may be related to an immunologic disorder involving cardiac beta andrenergic receptors. Heart Rhythm. 2006, 3, 1182–1186. [Google Scholar] [CrossRef]
- Hu, B.; Sun, Y.; Li, S.; Sun, J.; Liu, T.; Wu, Z.; Feng, L.I. Association of β1-Adrenergic, M2-Muscarinic Receptor Autoantibody with Occurrence and Development of Nonvalvular Atrial Fibrillation. Pacing Clin. Electrophysiol. 2016, 39, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Yalcin, M.U.; Gurses, K.M.; Kocyigit, D.; Kesikli, S.A.; Ates, A.H.; Evranos, B.; Yorgun, H.; Sahiner, M.L.; Kaya, E.B.; Oto, M.A.; et al. Elevated M2-muscarinic and β1-adrenergic receptor autoantibody levels are associated with paroxysmal atrial fibrillation. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2015, 104, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Stavrakis, S.; Yu, X.; Patterson, E.; Huang, S.; Hamlett, S.R.; Chalmers, L.; Pappy, R.; Cunningham, M.W.; Morshed, S.A.; Davies, T.F.; et al. Activating autoantibodies to the beta-1 adrenergic and m2 muscarinic receptors facilitate atrial fibrillation in patients with Graves’ hyperthyroidism. J. Am. Coll. Cardiol. 2009, 54, 1309–1316. [Google Scholar] [CrossRef]
- Galloway, A.; Li, H.; Vanderlinde-Wood, M.; Khan, M.; Benbrook, A.; Liles, C.; Zillner, C.; Rao, V.; Cunningham, M.W.; Yu, X.; et al. Activating autoantibodies to the β1/2-adrenergic and M2 muscarinic receptors associate with atrial tachyarrhythmias in patients with hyperthyroidism. Endocrine 2015, 49, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Song, J.; Li, K.; Li, Y.; Shang, L.; Zhou, Q.; Lu, Y.; Zong, Y.; He, X.; Kari, M.; et al. Increased β1-adrenergic receptor antibody confers a vulnerable substrate for atrial fibrillation via mediating Ca2+ mishandling and atrial fibrosis in active immunization rabbit models. Clin. Sci. 2023, 137, 195–217. [Google Scholar] [CrossRef]
- Li, H.; Murphy, T.; Zhang, L.; Huang, B.; Veitla, V.; Scherlag, B.J.; Kem, D.C.; Yu, X. β1-Adrenergic and M2 Muscarinic Autoantibodies and Thyroid Hormone Facilitate Induction of Atrial Fibrillation in Male Rabbits. Endocrinology 2016, 157, 16–22. [Google Scholar] [CrossRef]
- Li, H.; Zhang, G.; Zhou, L.; Nuss, Z.; Beel, M.; Hines, B.; Murphy, T.; Liles, J.; Zhang, L.; Kem, D.C.; et al. Adrenergic Autoantibody-Induced Postural Tachycardia Syndrome in Rabbits. J. Am. Heart Assoc. 2019, 8, e013006. [Google Scholar] [CrossRef] [PubMed]
- Gunning, W.T., 3rd; Kvale, H.; Kramer, P.M.; Karabin, B.L.; Grubb, B.P. Postural Orthostatic Tachycardia Syndrome Is Associated With Elevated G-Protein Coupled Receptor Autoantibodies. J. Am. Heart Assoc. 2019, 8, e013602. [Google Scholar] [CrossRef]
- Ke, F.; Kuang, W.; Hu, X.; Li, C.; Ma, W.; Shi, D.; Li, X.; Wu, Z.; Zhou, Y.; Liao, Y.; et al. A novel vaccine targeting β1-adrenergic receptor. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2023, 46, 1582–1595. [Google Scholar] [CrossRef] [PubMed]
- Wallukat, G.; Haberland, A.; Berg, S.; Schulz, A.; Freyse, E.J.; Dahmen, C.; Kage, A.; Dandel, M.; Vetter, R.; Salzsieder, E.; et al. The first aptamer-apheresis column specifically for clearing blood of beta1-receptor autoantibodies. Circ. J. Off. J. Jpn. Circ. Soc. 2012, 76, 2449–2455. [Google Scholar] [CrossRef]
- Düngen, H.D.; Dordevic, A.; Felix, S.B.; Pieske, B.; Voors, A.A.; McMurray, J.J.V.; Butler, J. β(1)-Adrenoreceptor Autoantibodies in Heart Failure: Physiology and Therapeutic Implications. Circulation. Heart Fail. 2020, 13, e006155. [Google Scholar] [CrossRef]
- Konishi, M.; Ishida, J.; Springer, J.; von Haehling, S.; Akashi, Y.J.; Shimokawa, H.; Anker, S.D. Heart failure epidemiology and novel treatments in Japan: Facts and numbers. ESC Heart Fail. 2016, 3, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Plosker, G.L.; Figgitt, D.P. Rituximab: A review of its use in non-Hodgkin’s lymphoma and chronic lymphocytic leukaemia. Drugs 2003, 63, 803–843. [Google Scholar] [CrossRef] [PubMed]
- Tschöpe, C.; Van Linthout, S.; Spillmann, F.; Posch, M.G.; Reinke, P.; Volk, H.D.; Elsanhoury, A.; Kühl, U. Targeting CD20+ B-lymphocytes in inflammatory dilated cardiomyopathy with rituximab improves clinical course: A case series. Eur. Heart J. Case Rep. 2019, 3, ytz131. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | No. of Patients | % β-B | Outcome in β1AR-AAb Positive Group (vs. Negative Unless Otherwise Specified) | The Other Findings | |
|---|---|---|---|---|---|---|
| IgG3 | Non-IgG3 | |||||
| Iwata et al. [50] | Obs | 104 | 27% | VT↑ at baseline, cardiac death↑, sudden cardiac death↑ during 31 M | ||
| Miao et al. [52] | Obs | 96 | 100% | Better uptitration of metoprolol LVEF↑, LVEDD↓, LVESD↓ after 1 year | β1AR-AAb frequency↘ after 1 year | |
| Nagatomo et al. [53] | Int | 82 | 100% | LVEF↑, LVEDD↓, LVESD↓ after 16 weeks | ||
| Nagatomo et al. (J-CHF study) [54] | Int | 117 | 100% | LVEF↑, LVEDV↓, LVESV↓ after 14 M | β1AR-AAb titer correlated with ΔLVEF, ΔLVEDV, ΔLVESV | |
| Stork et al. [26] | Obs | DCM: 65 ICM: 40 | DCM: 26% ICM: 13% | All-cause death↑, cardiovascular death↑ in DCM but not in ICM | ||
| Pei et al. [55] | Obs | DCM: 704 ICM: 1054 | DCM: 77% ICM: 70% | All-cause death↑, sudden cardiac death↑ both in DCM and ICM | ||
| Mavrogenis et al. [56] | Obs | 2256 | 83.4% | HF rehospitalization↑ | ||
| Nagatomo et al. (NORDIC-ARCTIC study) [27] | Obs | 116 | 97% | Better event free survival from the primary endpoint 1 compared to non-IgG3 | Worse event free survival from the primary endpoint 1 compared to IgG3 | |
| Nagatomo et al. (IMAC-2 study) [57] | Obs | 373 | 94% | LVEF↑ compared to negative and non-IgG3 Better evet free survival from the primary endpoint 1 compared to negative in NYHA III-IV subgroup | LVEF↓, LVEDD↑, LVESD↑ compared to negative and IgG3 Worse evet free survival from the primary endpoint 1 compared to IgG3 in NYHA III-IV subgroup | IgG3-β1AR-AAb titer correlated with LVEF at 6 M IgG3-β1AR-AAb independently associated with LVEF at 6 M and ΔLVEF |
| Study | Study Design | IA Column | No. of Patients | Duration of Follow Up | Findings |
|---|---|---|---|---|---|
| Muller J et al. [66] | RCT | Anti-human IgG | 34 (control 17) | 12M | β1AR-AAb reduction, LVEF↑, NYHA↓ after IA |
| Felix SB et al. [65] | RCT | Anti-human IgG | 18 (control 9) | 3M | β1AR-AAb reduction, LVEF↑, CI↑, SVi↑, SVR↓, NYHA↓ |
| Wallukat G et al. [71] | No control | Peptide column specific for β1AR-AAbs | 8 | 12M | LVEF↑, LVEDd↓ |
| Cooper LT et al. [76] | No control | Protein A | 4 | 6M | LHFQ↓, SF36↑ |
| Mobini R et al. [77] | No control β1AR-AAb (+) vs. (-) groups | Anti-human IgG | 22 | 3M | LVEF↑, SVi↑, CI↑ both in β1AR-AAb (+) and (-) groups |
| Staudt A et al. [78] | Anti-human IgG vs. protein A column | Anti-human IgG (high affinity to IgG3) vs. Protein A (low affinity) | 18 | 3M | LVEF↑, CI↑, SVi↑ and SVR↓ in anti-human IgG group |
| Staudt A et al. [79] | Protein A vs. protein A + improved IgG3 removal | Protein A | 18 | 3M | LVEF↑, CI↑, SVi↑ and NYHA↓ in improved IgG3 elimination group |
| Nagatomo Y et al. [74] | No control | Tryptophan (IgG3 specific) | 16 | 3M | β1AR-AAb, IgG3 reduction, LVEF↑, BNP↓, distance of 6MWT↑ |
| Baba A et al. [80] | No control | Tryptophan (IgG3 specific) | 16 | 3M | Pre IA titer of IgG3 AAbs correlated with the change of LVEF |
| Yoshikawa T et al. [75] | 2 course IA vs. delayed 1 course IA | Tryptophan (IgG3 specific) | 33 | 12M | LVEF↑, BNP↓, peak VO2↑ distance of 6MWT↑ after IA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawai, A.; Nagatomo, Y.; Yukino-Iwashita, M.; Nakazawa, R.; Taruoka, A.; Yumita, Y.; Takefuji, A.; Yasuda, R.; Toya, T.; Ikegami, Y.; et al. β1 Adrenergic Receptor Autoantibodies and IgG Subclasses: Current Status and Unsolved Issues. J. Cardiovasc. Dev. Dis. 2023, 10, 390. https://doi.org/10.3390/jcdd10090390
Kawai A, Nagatomo Y, Yukino-Iwashita M, Nakazawa R, Taruoka A, Yumita Y, Takefuji A, Yasuda R, Toya T, Ikegami Y, et al. β1 Adrenergic Receptor Autoantibodies and IgG Subclasses: Current Status and Unsolved Issues. Journal of Cardiovascular Development and Disease. 2023; 10(9):390. https://doi.org/10.3390/jcdd10090390
Chicago/Turabian StyleKawai, Akane, Yuji Nagatomo, Midori Yukino-Iwashita, Ryota Nakazawa, Akira Taruoka, Yusuke Yumita, Asako Takefuji, Risako Yasuda, Takumi Toya, Yukinori Ikegami, and et al. 2023. "β1 Adrenergic Receptor Autoantibodies and IgG Subclasses: Current Status and Unsolved Issues" Journal of Cardiovascular Development and Disease 10, no. 9: 390. https://doi.org/10.3390/jcdd10090390