
An Overview of Sport Participation and Exercise Prescription in Mitral Valve Disease
 , , , and
, , , and
Abstract
:1. Introduction
2. Mitral Stenosis
2.1. Pathophysiology
2.2. Diagnosis and Risk Stratification
2.3. Physical Activity and Exercise Prescription
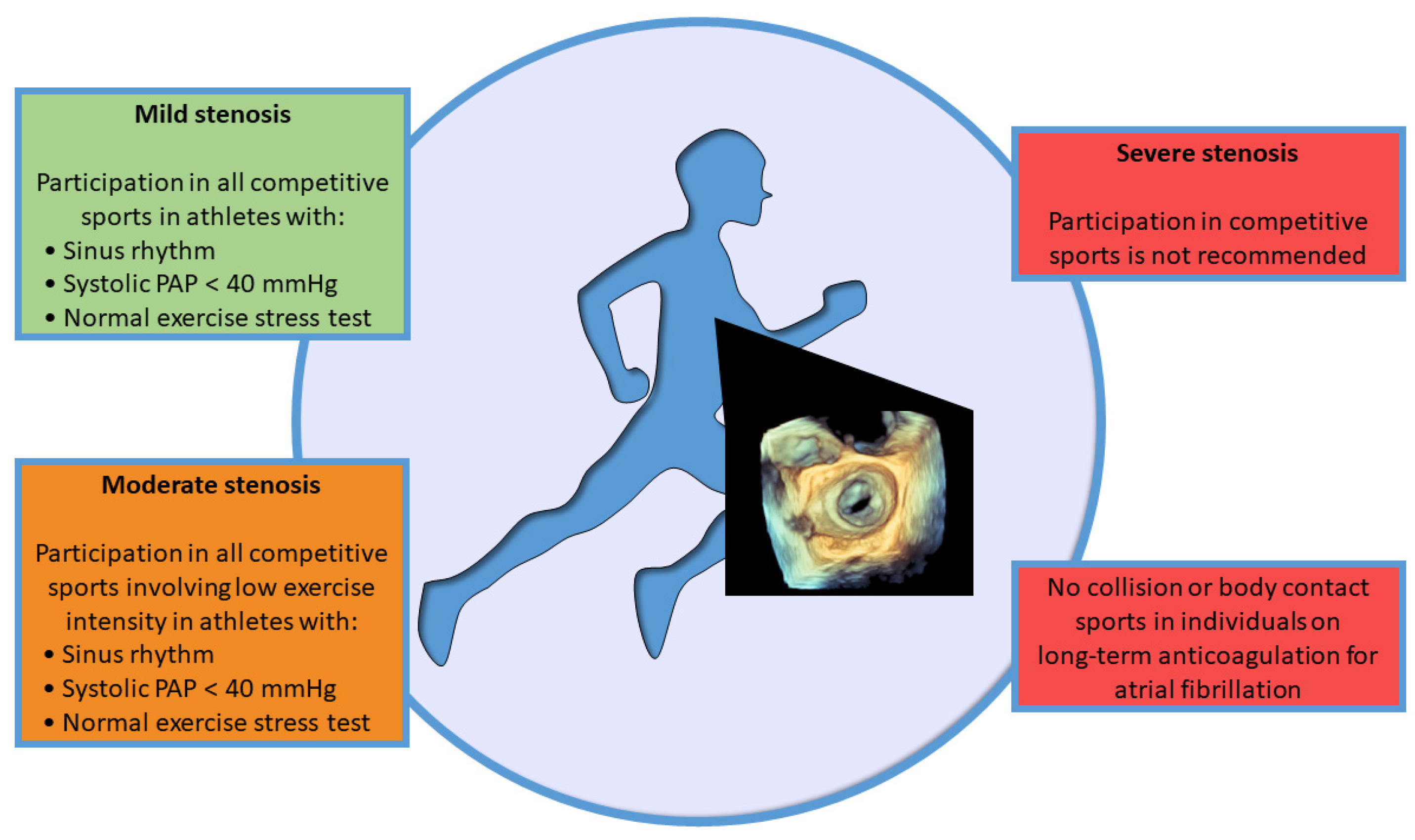
2.4. Competitive Sport Participation
3. Degenerative Mitral Regurgitation
3.1. Pathophysiology
3.2. Diagnosis and Risk Stratification
3.3. Arrhythmogenic Mitral Valve Prolapse and Mitral Annulus Disjunction
3.4. Physical Activity and Exercise Prescription
3.5. Competitive Sport Participation
4. Secondary Mitral Regurgitation
4.1. Pathophysiology
4.2. Diagnosis and Risk Stratification
4.3. Physical Activity and Exercise Prescription
4.3.1. Coronary Artery Disease
4.3.2. Heart Failure
4.4. Competitive Sport Participation
5. Percutaneous and Surgical Mitral Valve Repair and Replacement
5.1. Percutaneous Mitral Valve Interventions
5.2. Surgical Mitral Valve Repair or Replacement
5.3. Physical Activity, Exercise Prescription, and Competitive Sport Participation
6. Discussion and Future Perspectives
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suaya, J.A.; Stason, W.B.; Ades, P.A.; Normand, S.-L.T.; Shepard, D.S. Cardiac rehabilitation and survival in older coronary patients. J. Am. Coll. Cardiol. 2009, 54, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Eijsvogels, T.M.H.; Maessen, M.F.H.; Bakker, E.A.; Meindersma, E.P.; van Gorp, N.; Pijnenburg, N.; Thompson, P.D.; Hopman, M.T.E. Association of Cardiac Rehabilitation with All-Cause Mortality Among Patients with Cardiovascular Disease in the Netherlands. JAMA Netw. Open 2020, 3, e2011686. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; De Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary presentation and management of valvular heart disease: The Eur Observational Research Programme Valvular Heart Disease II Survey. Circulation 2019, 140, 1156–1169. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [Green Version]
- Rees, K.; Taylor, R.R.; Singh, S.; Coats, A.J.; Ebrahim, S. Exercise based rehabilitation for heart failure. Cochrane Database Syst. Rev. 2004, 3, CD003331. [Google Scholar] [CrossRef] [Green Version]
- Saberi, S.; Wheeler, M.; Bragg-Gresham, J.; Hornsby, W.; Agarwal, P.P.; Attili, A.; Concannon, M.; Dries, A.M.; Shmargad, Y.; Salisbury, H.; et al. Effect of moderate-intensity exercise training on peak oxygen consumption in patients with hypertrophic cardiomyopathy: A randomized clinical trial. JAMA 2017, 317, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Pingitore, A.; Autore, C.; Peruzzi, M.; Cavarretta, E. Non-alcoholic fatty liver disease and heart valve disease: A neglected link. Minerva Cardioangiol. 2020, 68, 542–544. [Google Scholar] [CrossRef]
- Robles, A.G.; Palamà, Z.; Nesti, M.; Tunzi, R.M.; Delise, P.; Cavarretta, E.; Penco, M.; Romano, S.; Sciarra, L. Sport Related Sudden Death: The Importance of Primary and Secondary Prevention. J. Clin. Med. 2022, 11, 4683. [Google Scholar] [CrossRef]
- van Buuren, F.; Gati, S.; Sharma, S.; Papadakis, M.; Adami, P.E.; Niebauer, J.; Pelliccia, A.; Rudolph, V.; Börjesson, M.; Carre, F.; et al. Athletes with valvular heart disease and competitive sports: A position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 1569–1578. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.-P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef]
- Giannitsi, S.; Bougiakli, M.; Bechlioulis, A.; Kotsia, A.; Michalis, L.K.; Naka, K.K. 6-minute walking test: A useful tool in the management of heart failure patients. Ther. Adv. Cardiovasc. Dis. 2019, 13, 1753944719870084. [Google Scholar] [CrossRef] [Green Version]
- Martijn, S.; Cindel, B.; Maarten, F.; Dominique, H.; Deeman, M.; Toshiki, K.; Linqi, X.; Elaine, J.; Lotte, S.; Hanne, K.; et al. Smartphone-based 6-minute walking test while walking in the park: Bringing physical fitness monitoring to the patient’s hands. Eur. J. Prev. Cardiol. 2022, 29, e350–e352. [Google Scholar] [CrossRef]
- D’Ascenzi, F.; Cavigli, L.; Pagliaro, A.; Focardi, M.; Valente, S.; Cameli, M.; Mandoli, G.E.; Mueller, S.; Dendale, P.; Piepoli, M.; et al. Clinician approach to cardiopulmonary exercise testing for exercise prescription in patients at risk of and with cardiovascular disease. Br. J. Sports Med. 2022, 56, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Glaab, T.; Taube, C. Practical guide to cardiopulmonary exercise testing in adults. Respir. Res. 2022, 23, 9. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Evangelista, A.; Griffin, B.P.; Iung, B.; Otto, C.M.; Pellikka, P.A.; Quiñones, M.; et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J. Am. Soc. Echocardiogr. 2009, 22, 1–23. [Google Scholar] [CrossRef]
- Sud, K.; Agarwal, S.; Parashar, A.; Raza, M.Q.; Patel, K.; Min, D.; Rodriguez, L.L.; Krishnaswamy, A.; Mick, S.L.; Gillinov, A.M.; et al. Degenerative Mitral Stenosis: Unmet Need for Percutaneous Interventions. Circulation 2016, 133, 1594–1604. [Google Scholar] [CrossRef] [Green Version]
- Patil, S.; Pingle, S.-R.; Shalaby, K.; Kim, A.S. Mediastinal irradiation and valvular heart disease. Cardio-Oncology 2022, 8, 7. [Google Scholar] [CrossRef] [PubMed]
- Lev, E.I.; Sagie, A.; Vaturi, M.; Sela, N.; Battler, A.; Shapira, Y. Value of exercise echocardiography in rheumatic mitral stenosis with and without significant mitral regurgitation. Am. J. Cardiol. 2004, 93, 1060–1063. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Nunes, M.C.P.; Tan, T.C.; Elmariah, S.; Lago, R.D.; Margey, R.; Cruz-Gonzalez, I.; Zheng, H.; Handschumacher, M.D.; Inglessis, I.; Palacios, I.F.; et al. The Echo Score Revisited: Impact of incorporating commissural morphology and leaflet displacement to the prediction of outcome for patients undergoing percutaneous mitral valvuloplasty. Circulation 2014, 129, 886–895. [Google Scholar] [CrossRef] [Green Version]
- Cavarretta, E.; Pressler, A. Exercise in specific diseases: Valvular heart disease. In Textbook of Sports Cardiology; Pressler, A., Niebauer, J., Eds.; Springer: Cham, Switzerland, 2020; ISBN 978-3-030-35373-5. [Google Scholar] [CrossRef]
- Lancellotti, P.; Pellikka, P.A.; Budts, W.; Chaudhry, F.A.; Donal, E.; Dulgheru, R.; Edvardsen, T.; Garbi, M.; Ha, J.W.; Kane, G.C.; et al. The clinical use of stress echocardiography in non-ischaemic heart disease: Recommendations from the european association of cardiovascular imaging and the american society of echocardiography. J. Am. Soc. Echocardiogr. 2017, 30, 101–138. [Google Scholar] [CrossRef] [Green Version]
- Gohlke-Bärwolf, C. Exercise Training in Valvular Heart Disease. In Cardiovascular Prevention and Rehabilitation; Springer: London, UK, 2007. [Google Scholar]
- Biffi, A.; Delise, P.; Zeppilli, P.; Giada, F.; Pelliccia, A.; Penco, M.; Casasco, M.; Colonna, P.; D’andrea, A.; D’andrea, L.; et al. Italian cardiological guidelines for sports eligibility in athletes with heart disease: Part 1. J. Cardiovasc. Med. 2013, 14, 477–499. [Google Scholar] [CrossRef] [PubMed]
- Delise, P.; Mos, L.; Sciarra, L.; Basso, C.; Biffi, A.; Cecchi, F.; Colivicchi, F.; Corrado, D.; D’andrea, A.; Di Cesare, E.; et al. Italian Cardiological Guidelines (COCIS) for Competitive Sport Eligibility in athletes with heart disease: Update 2020. J. Cardiovasc. Med. 2021, 22, 874–891. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef]
- Bonow, R.O.; Nishimura, R.A.; Thompson, P.D.; Udelson, J.E. Eligibility and Disqualification Recommendations for Competitive Athletes with Cardiovascular Abnormalities: Task Force 5: Valvular Heart Disease: A Scientific Statement From the American Heart Association and American College of Cardiology. J. Am. Coll. Cardiol. 2015, 66, 2385–2392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yared, K.; Lam, K.M.-T.; Hung, J. The use of exercise echocardiography in the evaluation of mitral regurgitation. Curr. Cardiol. Rev. 2009, 5, 312–322. [Google Scholar] [CrossRef]
- Kusunose, K.; Popović, Z.B.; Motoki, H.; Marwick, T.H. Prognostic significance of exercise-induced right ventricular dysfunction in asymptomatic degenerative mitral regurgitation. Circ. Cardiovasc. Imaging 2013, 6, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Lancellotti, P.; Pibarot, P.; Chambers, J.; La Canna, G.; Pepi, M.; Dulgheru, R.; Dweck, M.; Delgado, V.; Garbi, M.; Vannan, A.M.; et al. Multi-modality imaging assessment of native valvular regurgitation: An EACVI and ESC council of valvular heart disease position paper. Eur. Heart J.-Cardiovasc. Imaging 2022, 23, e171–e232. [Google Scholar] [CrossRef]
- Devereux, R.B.; Jones, E.C.; Roman, M.J.; Howard, B.V.; Fabsitz, R.R.; Liu, J.E.; Palmieri, V.; Welty, T.K.; Lee, E.T. Prevalence and correlates of mitral valve prolapse in a population-based sample of American Indians: The strong heart study. Am. J. Med. 2001, 111, 679–685. [Google Scholar] [CrossRef]
- Nalliah, C.J.; Mahajan, R.; Elliott, A.D.; Haqqani, H.; Lau, D.H.; Vohra, J.K.; Morton, J.B.; Semsarian, C.; Marwick, T.; Kalman, J.M.; et al. Mitral valve prolapse and sudden cardiac death: A systematic review and meta-analysis. Heart 2019, 105, 144–151. [Google Scholar] [CrossRef]
- Finocchiaro, G.; Papadakis, M.; Robertus, J.-L.; Dhutia, H.; Steriotis, A.K.; Tome, M.; Mellor, G.; Merghani, A.; Malhotra, A.; Behr, E.; et al. Etiology of Sudden Death in Sports: Insights from a United Kingdom regional registry. J. Am. Coll. Cardiol. 2016, 67, 2108–2115. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, K.; Uy-Evanado, A.; Teodorescu, C.; Reinier, K.; Nichols, G.A.; Gunson, K.; Jui, J.; Chugh, S.S. Mitral valve prolapse and sudden cardiac arrest in the community. Heart Rhythm. 2016, 13, 498–503. [Google Scholar] [CrossRef] [Green Version]
- Basso, C.; Marra, M.P.; Rizzo, S.; De Lazzari, M.; Giorgi, B.; Cipriani, A.; Frigo, A.C.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Arrhythmic Mitral Valve Prolapse and Sudden Cardiac Death. Circulation 2015, 132, 556–566. [Google Scholar] [CrossRef] [Green Version]
- van Wijngaarden, A.L.; Kruithof, B.P.T.; Vinella, T.; Barge-Schaapveld, D.Q.C.M.; Marsan, N.A. Characterization of Degenerative Mitral Valve Disease: Differences between Fibroelastic Deficiency and Barlow’s Disease. J. Cardiovasc. Dev. Dis. 2021, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Cavarretta, E.; Peruzzi, M.; Versaci, F.; Frati, G.; Sciarra, L. How to manage an athlete with mitral valve prolapse. Eur. J. Prev. Cardiol. 2021, 28, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Faletra, F.F.; Leo, L.A.; Paiocchi, V.L.; Schlossbauer, S.A.; Pavon, A.G.; Ho, S.Y.; Maisano, F. Morphology of Mitral Annular Disjunction in Mitral Valve Prolapse. J. Am. Soc. Echocardiogr. 2022, 35, 176–186. [Google Scholar] [CrossRef]
- Bennett, S.; Thamman, R.; Griffiths, T.; Oxley, C.; Khan, J.N.; Phan, T.; Patwala, A.; Heatlie, G.; Kwok, C.S. Mitral annular disjunction: A systematic review of the literature. Echocardiography 2019, 36, 1549–1558. [Google Scholar] [CrossRef]
- Marra, M.P.; Basso, C.; De Lazzari, M.; Rizzo, S.; Cipriani, A.; Giorgi, B.; Lacognata, C.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Morphofunctional Abnormalities of Mitral Annulus and Arrhythmic Mitral Valve Prolapse. Circ. Cardiovasc. Imaging 2016, 9, e005030. [Google Scholar] [CrossRef] [Green Version]
- Petrungaro, M.; Fusco, L.; Cavarretta, E.; Scarà, A.; Borrelli, A.; Romano, S.; Petroni, R.; D’ascenzi, F.; Sciarra, L. Long-Term Sports Practice and Atrial Fibrillation: An Updated Review of a Complex Relationship. J. Cardiovasc. Dev. Dis. 2023, 10, 218. [Google Scholar] [CrossRef]
- Gornick, C.C.; Tobler, H.G.; Pritzker, M.C.; Tuna, I.C.; Almquist, A.; Benditt, D.G. Electrophysiologic effects of papillary muscle traction in the intact heart. Circulation 1986, 73, 1013–1021. [Google Scholar] [CrossRef] [Green Version]
- Basso, C.; Marra, M.P. Mitral Annulus Disjunction: Emerging Role of Myocardial Mechanical Stretch in Arrhythmo-genesis. J. Am. Coll. Cardiol. 2018, 72, 1610–1612. [Google Scholar] [CrossRef] [PubMed]
- Sniezek-Maciejewska, M.; Dubiel, J.P.; Piwowarska, W.; Mroczek-Czernecka, D.; Mazurek, S.; Jaśkiewicz, J.; Kitliński, M. Ventricular arrhythmias and the autonomic tone in patients with mitral valve prolapse. Clin. Cardiol. 1992, 15, 720–724. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, A.K.; Bogun, F.; Liang, J.J. Arrhythmic Mitral Valve Prolapse and Mitral Annular Disjunction: Clinical Features, Pathophysiology, Risk Stratification, and Management. J. Cardiovasc. Dev. Dis. 2022, 9, 61. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.A.; Dukkipati, S.R.; Turagam, M.; Liao, S.L.; Adams, D.H.; Reddy, V.Y. Arrhythmic Mitral Valve Prolapse: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2018, 72 Pt A, 2904–2914. [Google Scholar] [CrossRef]
- Sciarra, L.; Cavarretta, E.; Siciliani, S.; Sette, A.; Scarà, A.; Grieco, D.; de Ruvo, E.; Palamà, Z.; Nesti, M.; Romano, S.; et al. Managing athletes with palpitations of unknown origin with an external loop recorder: A cohort study. J. Sports Med. Phys. Fit. 2022, 62, 554–559. [Google Scholar] [CrossRef]
- Russo, A.D.; Compagnucci, P.; Zorzi, A.; Cavarretta, E.; Castelletti, S.; Contursi, M.; D’Aleo, A.; D’Ascenzi, F.; Mos, L.; Palmieri, V.; et al. Electroanatomic mapping in athletes: Why and when. An expert opinion paper from the Italian Society of Sports Cardiology. Int. J. Cardiol. 2023, 383, 166–174. [Google Scholar] [CrossRef]
- Hiemstra, Y.L.; van Wijngaarden, A.L.; Bos, M.W.; Schalij, M.J.; Klautz, R.J.; Bax, J.J.; Delgado, V.; Barge-Schaapveld, D.Q.; Marsan, N.A. Familial occurrence of mitral regurgitation in patients with mitral valve prolapse undergoing mitral valve surgery. Eur. J. Prev. Cardiol. 2020, 27, 272–280. [Google Scholar] [CrossRef] [Green Version]
- Guicciardi, N.A.; De Bonis, M.; Di Resta, C.; Ascione, G.; Alfieri, O.; Maisano, F.; Vergara, P. Genetic background of mitral valve prolapse. Rev. Cardiovasc. Med. 2022, 23, 96. [Google Scholar] [CrossRef]
- Castelletti, S.; Zorzi, A.; Ballardini, E.; Basso, C.; Biffi, A.; Brancati, F.; Cavarretta, E.; Crotti, L.; Contursi, M.; D’Aleo, A.; et al. Molecular genetic testing in athletes: Why and when a position statement from the Italian Society of Sports Cardiology. Int. J. Cardiol. 2022, 364, 169–177. [Google Scholar] [CrossRef]
- McCann, M.; Stamp, N.; Ngui, A.; Litton, E. Cardiac Prehabilitation. J. Cardiothorac. Vasc. Anesth. 2019, 33, 2255–2265. [Google Scholar] [CrossRef]
- Scordo, K.A. Effects of aerobic exercise training on symptomatic women with mitral valve prolapse. Am. J. Cardiol. 1991, 67, 863–868. [Google Scholar] [CrossRef] [PubMed]
- Gati, S.; Malhotra, A.; Sharma, S. Exercise recommendations in patients with valvular heart disease. Heart 2019, 105, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Deferm, S.; Bertrand, P.B.; Verbrugge, F.H.; Verhaert, D.; Rega, F.; Thomas, J.D.; Vandervoort, P.M. Atrial Functional Mitral Regurgitation: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 2465–2476. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Fontaine, A.A.; Schwammenthal, E.; Yoganathan, A.P.; Levine, R.A. Integrated Mechanism for Functional Mitral Regurgitation: Leaflet restriction versus coapting force: In vitro studies. Circulation 1997, 96, 1826–1834. [Google Scholar] [CrossRef]
- Watanabe, N.; Ogasawara, Y.; Yamaura, Y.; Wada, N.; Kawamoto, T.; Toyota, E.; Akasaka, T.; Yoshida, K. Mitral annulus flattens in ischemic mitral regurgitation: Geometric differences between inferior and anterior myocardial infarction: A realtime 3-dimensional echocardiographic study. Circulation 2005, 112 (Suppl. 9), I458–I462. [Google Scholar] [CrossRef]
- Agricola, E.; Oppizzi, M.; Galderisi, M.; Pisani, M.; Meris, A.; Pappone, C.; Margonato, A. Role of regional mechanical dyssynchrony as a determinant of functional mitral regurgitation in patients with left ventricular systolic dysfunction. Heart 2006, 92, 1390–1395. [Google Scholar] [CrossRef]
- Lafitte, S.; Bordachar, P.; Lafitte, M.; Garrigue, S.; Reuter, S.; Reant, P.; Serri, K.; Lebouffos, V.; Berrhouet, M.; Jais, P.; et al. Dynamic Ventricular Dyssynchrony: An Exercise-Echocardiography Study. J. Am. Coll. Cardiol. 2006, 47, 2253–2259. [Google Scholar] [CrossRef] [Green Version]
- Lancellotti, P.; Lebrun, F.; Piérard, A.L. Determinants of exercise-induced changes in mitral regurgitation in patients with coronary artery disease and left ventricular dysfunction. J. Am. Coll. Cardiol. 2003, 42, 1921–1928. [Google Scholar] [CrossRef] [Green Version]
- D’Andrea, A.; Caso, P.; Cuomo, S.; Scarafile, R.; Salerno, G.; Limongelli, G.; Di Salvo, G.; Severino, S.; Ascione, L.; Calabrò, P.; et al. Effect of dynamic myocardial dyssynchrony on mitral regurgitation during supine bicycle exercise stress echocardiography in patients with idiopathic dilated cardiomyopathy and ‘narrow’ QRS. Eur. Heart J. 2007, 28, 1004–1011. [Google Scholar] [CrossRef]
- Izumo, M.; Suzuki, K.; Moonen, M.; Kou, S.; Shimozato, T.; Hayashi, A.; Akashi, Y.J.; Osada, N.; Omiya, K.; Miyake, F.; et al. Changes in mitral regurgitation and left ventricular geometry during exercise affect exercise capacity in patients with systolic heart failure. Eur. Heart J.-Cardiovasc. Imaging 2011, 12, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Keren, G.; Katz, S.; Gage, J.; Strom, J.; Sonnenblick, E.H.; LeJemtel, T.H. Effect of isometric exercise on cardiac performance and mitral regurgitation in patients with severe congestive heart failure. Am. Heart J. 1989, 118 Pt 1, 973–979. [Google Scholar] [CrossRef]
- Shen, W.F.; Roubin, G.S.; Hirasawa, K.; Choong, C.Y.-P.; Hutton, B.F.; Harris, P.J.; Fletcher, P.J.; Kelly, D.T. Left ventricular volume and ejection fraction response to exercise in chronic congestive heart failure: Difference between dilated cardiomyopathy and previous myocardial infarction. Am. J. Cardiol. 1985, 55, 1027–1031. [Google Scholar] [CrossRef]
- Mann, D.L.; Scharf, J.; Ahnve, S.; Gilpin, E. Left ventricular volume during supine exercise: Importance of myocardial scar in patients with coronary heart disease. J. Am. Coll. Cardiol. 1987, 9, 26–34. [Google Scholar] [CrossRef]
- Gertz, Z.M.; Raina, A.; Saghy, L.; Zado, E.S.; Callans, D.J.; Marchlinski, F.E.; Keane, M.G.; Silvestry, F.E. Evidence of Atrial Functional Mitral Regurgitation Due to Atrial Fibrillation: Reversal With Arrhythmia Control. J. Am. Coll. Cardiol. 2011, 58, 1474–1481. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Liu, S.; Datta, S.; Rajagopalan, S.; Ryan, T.; Igo, S.R.; Jackson, M.S.; Little, S.H.; De Michelis, N.; Vannan, M.A.; et al. Quantification of Chronic Functional Mitral Regurgitation by Automated 3-Dimensional Peak and Integrated Proximal Isovelocity Surface Area and Stroke Volume Techniques Using Real-Time 3-Dimensional Volume Color Doppler Echocardiography: In vitro and clinical validation. Circ. Cardiovasc. Imaging 2013, 6, 125–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagendorff, A.; Doenst, T.; Falk, V. Echocardiographic assessment of functional mitral regurgitation: Opening Pandora’s box? ESC Heart Fail. 2019, 6, 678–685. [Google Scholar] [CrossRef] [Green Version]
- Buck, T.; Plicht, B.; Kahlert, P.; Schenk, I.M.; Hunold, P.; Erbel, R. Effect of Dynamic Flow Rate and Orifice Area on Mitral Regurgitant Stroke Volume Quantification Using the Proximal Isovelocity Surface Area Method. J. Am. Coll. Cardiol. 2008, 52, 767–778. [Google Scholar] [CrossRef] [Green Version]
- Ray, S. The echocardiographic assessment of functional mitral regurgitation. Eur. Heart J.-Cardiovasc. Imaging 2010, 11, i11–i17. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Dini, F.L.; Faggiano, P.; Agricola, E.; Cicoira, M.; Frattini, S.; Simioniuc, A.; Gullace, M.; Ghio, S.; Enriquez-Sarano, M.; et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy. Heart 2011, 97, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.; Moskowitz, A.J.; Gelijns, A.C.; Ailawadi, G.; Parides, M.K.; Perrault, L.P.; Hung, J.W.; Voisine, P.; Dagenais, F.; Gillinov, A.M.; et al. Two-Year Outcomes of Surgical Treatment of Severe Ischemic Mitral Regurgitation. N. Engl. J. Med. 2016, 374, 344–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michler, R.E.; Smith, P.K.; Parides, M.K.; Ailawadi, G.; Thourani, V.; Moskowitz, A.J.; Acker, M.A.; Hung, J.W.; Chang, H.L.; Perrault, L.P.; et al. Two-Year Outcomes of Surgical Treatment of Moderate Ischemic Mitral Regurgitation. N. Engl. J. Med. 2016, 374, 1932–1941. [Google Scholar] [CrossRef] [PubMed]
- Mihos, C.G.; Xydas, S.; Yucel, E.; Capoulade, R.; Williams, R.F.; Mawad, M.; Garcia, G.; Santana, O. Mitral valve repair and subvalvular intervention for secondary mitral regurgitation: A systematic review and meta-analysis of randomized controlled and propensity matched studies. J. Thorac. Dis. 2017, 9 (Suppl. 7), S582–S594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmiero, G.; Melillo, E.; Ferro, A.; Carlomagno, G.; Sordelli, C.; Ascione, R.; Monda, V.; Severino, S.; Ascione, L.; Caso, P. Significant functional mitral regurgitation affects left atrial function in heart failure patients: Haemodynamic correlations and prognostic implications. Eur. Heart J.-Cardiovasc. Imaging 2019, 20, 1012–1019. [Google Scholar] [CrossRef]
- Agricola, E.; Oppizzi, M.; Maisano, F.; De Bonis, M.; Schinkel, A.F.; Torracca, L.; Margonato, A.; Melisurgo, G.; Alfieri, O. Echocardiographic classification of chronic ischemic mitral regurgitation caused by restricted motion according to tethering pattern. Eur. J. Echocardiogr. 2004, 5, 326–334. [Google Scholar] [CrossRef]
- Borjesson, M.; Dellborg, M.; Niebauer, J.; LaGerche, A.; Schmied, C.; Solberg, E.E.; Halle, M.; Adami, P.E.; Biffi, A.; Carré, F.; et al. Brief recommendations for participation in leisure time or competitive sports in athletes–patients with coronary artery disease: Summary of a Position Statement from the Sports Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur. J. Prev. Cardiol. 2020, 27, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Ellingsen, O.; Halle, M.; Conraads, V.; Stoylen, A.; Dalen, H.; Delagardelle, C.; Larsen, A.-I.; Hole, T.; Mezzani, A.; Van Craenenbroeck, E.M.; et al. High-intensity interval training in patients with heart failure with reduced ejection fraction. Circulation 2017, 135, 839–849. [Google Scholar] [CrossRef]
- Omar, W.; Pandey, A.; Haykowsky, M.J.; Berry, J.D.; Lavie, C.J. The Evolving Role of Cardiorespiratory Fitness and Exercise in Prevention and Management of Heart Failure. Curr. Heart Fail. Rep. 2018, 15, 75–80. [Google Scholar] [CrossRef]
- Cornelis, J.; Beckers, P.; Taeymans, J.; Vrints, C.; Vissers, D. Comparing exercise training modalities in heart failure: A systematic review and meta-analysis. Int. J. Cardiol. 2016, 221, 867–876. [Google Scholar] [CrossRef]
- Smart, N.A.; Giallauria, F.; Dieberg, G. Efficacy of inspiratory muscle training in chronic heart failure patients: A systematic review and meta-analysis. Int. J. Cardiol. 2013, 167, 1502–1507. [Google Scholar] [CrossRef]
- Benito-González, T.; Estévez-Loureiro, R.; Garrote-Coloma, C.; Garriz, I.I.; Gualis, J.; Álvarez-Roy, L.; Rodriguez-Santamarta, M.; De Prado, A.P.; Fernández-Vázquez, F. MitraClip improves cardiopulmonary exercise test in patients with systolic heart failure and functional mitral regurgitation. ESC Heart Fail. 2019, 6, 867–873. [Google Scholar] [CrossRef]
- Vignati, C.; De Martino, F.; Muratori, M.; Salvioni, E.; Tamborini, G.; Bartorelli, A.; Pepi, M.; Alamanni, F.; Farina, S.; Cattadori, G.; et al. Rest and exercise oxygen uptake and cardiac output changes 6 months after successful transcatheter mitral valve repair. ESC Heart Fail. 2021, 8, 4915–4924. [Google Scholar] [CrossRef] [PubMed]
- Pingitore, A.; Polizzi, V.; Cardillo, I.; Lio, A.; Ranocchi, F.; Pergolini, A.; Musumeci, F. 3D mitral annulus echocardiography assessment in patients affected by degenerative mitral regurgitation who underwent mitral valve repair with flexible band. J. Card. Surg. 2022, 37, 4269–4277. [Google Scholar] [CrossRef] [PubMed]
- Vieitez, J.M.; Monteagudo, J.M.; Mahia, P.; Perez, L.; Lopez, T.; Marco, I.; Perone, F.; González, T.; Sitges, M.; Bouzas-Mosquera, A.; et al. New insights of tricuspid regurgitation: A large-scale prospective cohort study. Eur. Heart J.-Cardiovasc. Imaging 2021, 22, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Tamulevičiūtė-Prascienė, E.; Beigienė, A.; Thompson, M.J.; Balnė, K.; Kubilius, R.; Bjarnason-Wehrens, B. The impact of additional resistance and balance training in exercise-based cardiac rehabilitation in older patients after valve surgery or intervention: Randomized control trial. BMC Geriatr. 2021, 21, 23. [Google Scholar] [CrossRef] [PubMed]
- Xue, W.; Xinlan, Z.; Xiaoyan, Z. Effectiveness of early cardiac rehabilitation in patients with heart valve surgery: A randomized, controlled trial. J. Int. Med. Res. 2022, 50, 03000605211044320. [Google Scholar] [CrossRef]
- Goel, K.; Pack, Q.R.; Lahr, B.; Greason, K.L.; Lopez-Jimenez, F.; Squires, R.W.; Zhang, Z.; Thomas, R.J. Cardiac rehabilitation is associated with reduced long-term mortality in patients undergoing combined heart valve and CABG surgery. Eur. J. Prev. Cardiol. 2015, 22, 159–168. [Google Scholar] [CrossRef]
- Rimington, H.; Weinman, J.; Chambers, J.B. Predicting outcome after valve replacement. Heart 2010, 96, 118–123. [Google Scholar] [CrossRef]
- Abraham, L.N.; Sibilitz, K.L.; Berg, S.K.; Tang, L.H.; Risom, S.S.; Lindschou, J.; Taylor, R.S.; Borregaard, B.; Zwisler, A.-D. Exercise-based cardiac rehabilitation for adults after heart valve surgery. Cochrane Database Syst. Rev. 2021, 2021, CD010876. [Google Scholar] [CrossRef]
- Peruzzi, M.; Covi, K.; Saccucci, M.; Pingitore, A.; Saade, W.; Sciarra, L.; Cristalli, M.P.; Miraldi, F.; Frati, G.; Cavarretta, E. Current knowledge on the association between cardiovascular and periodontal disease: An umbrella review. Minerva Cardiol. Angiol. 2023, 71, 208–220. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef]
- Peruzzi, M.; Sanasi, E.; Pingitore, A.; Marullo, A.G.; Carnevale, R.; Sciarretta, S.; Sciarra, L.; Frati, G.; Cavarretta, E. An overview of cycling as active transportation and as benefit for health. Minerva Cardioangiol. 2020, 68, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Androulakis, E.; Perone, F. Multimodality Cardiac Imaging in Young and Veteran Athletes: Updates on Atrial Function Assessment, Arrhythmia Predisposition and Pathology Discrimination. J. Clin. Med. 2023, 12, 797. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Mild | Moderate | Severe | Variation during Stress Echocardiography | |
|---|---|---|---|---|
| Valve Area (cm2) | >1.5 | 1.0–1.5 | <1.0 | -- |
| Mean transmitral pressure gradient (mmHg) | <5 | 5–10 | >10 | MS is severe if mean gradient increases:
|
| Systolic Pulmonary Artery Pressure (mmHg) | <30 | 30–50 | >50 | A systolic PAP elevation >60 mmHg or a rapid increase in systolic PAP (>90% increase at second step of exercise) are highly predictive of exercise-induced dyspnea |
| Mild | Mild-to-Moderate | Moderate-to-Severe | Severe | Variation during Stress Echocardiography | ||
|---|---|---|---|---|---|---|
| Qualitative Parameters | Primary MR | Secondary MR | ||||
| MV morphology | None-mild leaflets abnormalities/tenting | Moderate leaflets abnormalities/tenting | Moderate leaflets abnormalities/tenting | Flail leaflet, ruptured papillary muscle, severe retraction, large perforation | Normal leaflets with severe tenting and/or poor leaflet coaptation | |
| Color Flow MR jet | Small, central | Intermediate | Intermediate | Large central jet or eccentric jet reaching the posterior wall of the LA | Large central jet or eccentric wall impinging jet of variable size | |
| Flow convergence zoneContinuous wave signalof MR jet | No or small faint/parabolic | Dense, partial or parabolic | Dense, parabolic or triangular |
|
| |
| Semi-quantitative parameters | ||||||
| VC width (mm) | <3 | 3–<5 | 5–<7 | ≥7 | ≥7 | |
| Pulmonary vein flow | Systolic dominance | Normal or systolic blunting | Systolic blunting | Systolic flow reversal | Systolic flow reversal | |
| Mitral inflow | A wave dominant | Variable | Peak E wave >1.2 m/s | Peak E wave >1.2 m/s | Peak E wave >1.2 m/s | |
| TVI mitral/TVI LVOT | <1 | Intermediate | >1.2 | >1.4 | >1.4 | |
| Quantitative parameters | ||||||
| EROA (2D PISA, mm2) | <20 | 20–29 | 30–39 | ≥40 | ≥40 (may be ≥30 if elliptical regurgitant orifice area) | Increase in EROA ≥ 13 mm2 is associated with poor prognosis in secondary MR |
| Regurgitant volume (mL) | <30 | 30–44 | 45–59 | ≥60 | ≥60 (may be ≥45 mL if low flow conditions) | |
| Regurgitant fraction (%) | <30 | 30–39 | 40–49 | ≥50 | ≥50 | |
| Structural Parameters | ||||||
| LA size | Usually Normal | Normal or dilated | Usually dilated | Dilated | Dilated | |
| LV size | Usually Normal | Normal or dilated | Usually dilated | Dilated | Dilated | Absence of contractile reserve is associated with poor prognosis in primary MR |
| PA pressures | Usually Normal | Normal or elevated | Normal or elevated | Usually elevated | Usually elevated | Dynamic PH (sPAP ≥ 60 mmHg) is associated with poor prognosis in primary and secondary MR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perone, F.; Peruzzi, M.; Conte, E.; Sciarra, L.; Frati, G.; Cavarretta, E.; Pingitore, A. An Overview of Sport Participation and Exercise Prescription in Mitral Valve Disease. J. Cardiovasc. Dev. Dis. 2023, 10, 304. https://doi.org/10.3390/jcdd10070304
Perone F, Peruzzi M, Conte E, Sciarra L, Frati G, Cavarretta E, Pingitore A. An Overview of Sport Participation and Exercise Prescription in Mitral Valve Disease. Journal of Cardiovascular Development and Disease. 2023; 10(7):304. https://doi.org/10.3390/jcdd10070304
Chicago/Turabian StylePerone, Francesco, Mariangela Peruzzi, Edoardo Conte, Luigi Sciarra, Giacomo Frati, Elena Cavarretta, and Annachiara Pingitore. 2023. "An Overview of Sport Participation and Exercise Prescription in Mitral Valve Disease" Journal of Cardiovascular Development and Disease 10, no. 7: 304. https://doi.org/10.3390/jcdd10070304