
Radiation Exposure Reduction by Digital Variance Angiography in Lower Limb Angiography: A Randomized Controlled Trial
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
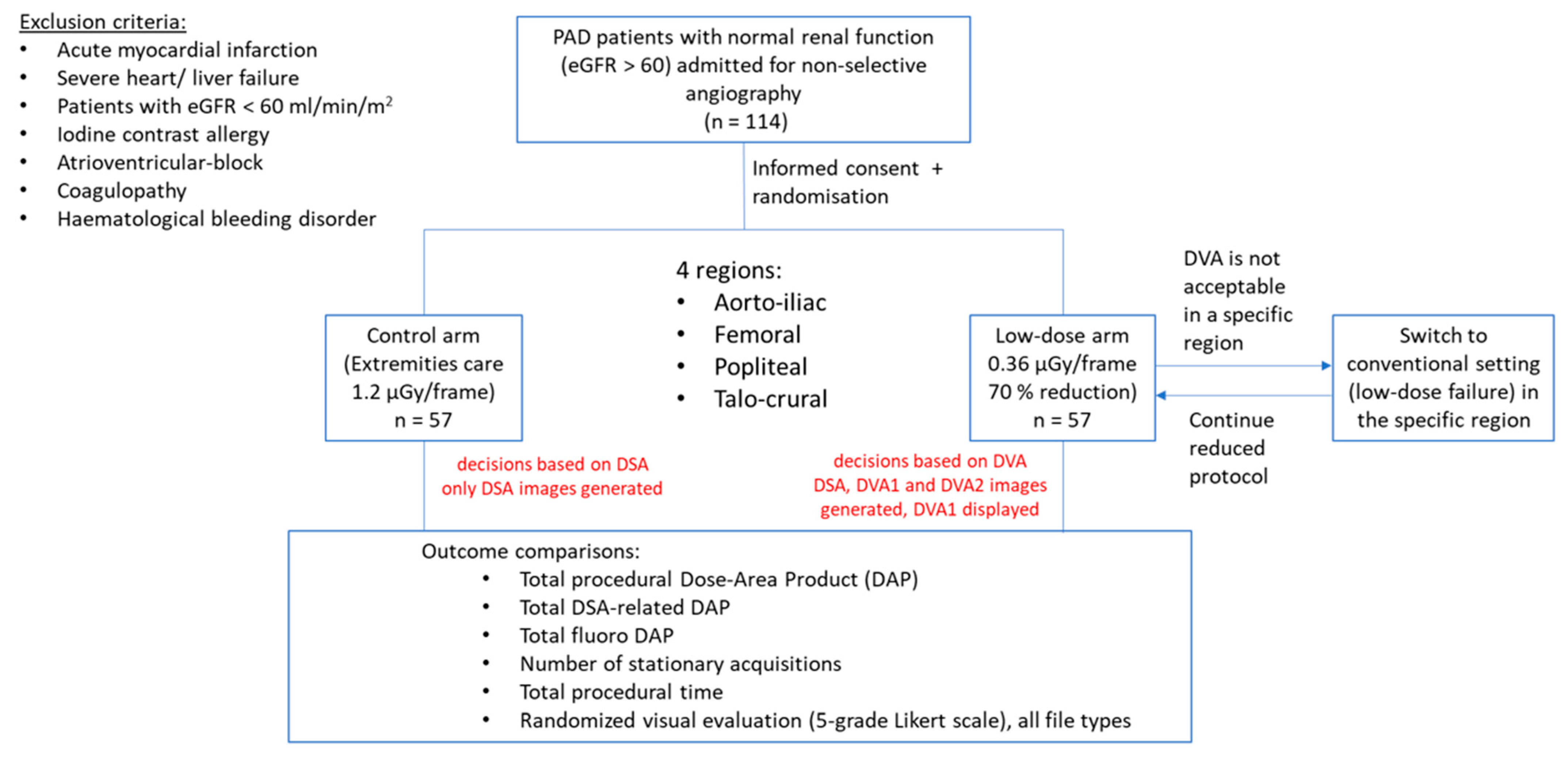
2.1. Patient Selection
2.2. Study Design
2.3. Image Acquisition
2.4. Image Processing
2.5. Visual Evaluation
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Procedural Details
3.2. Radiation Dose
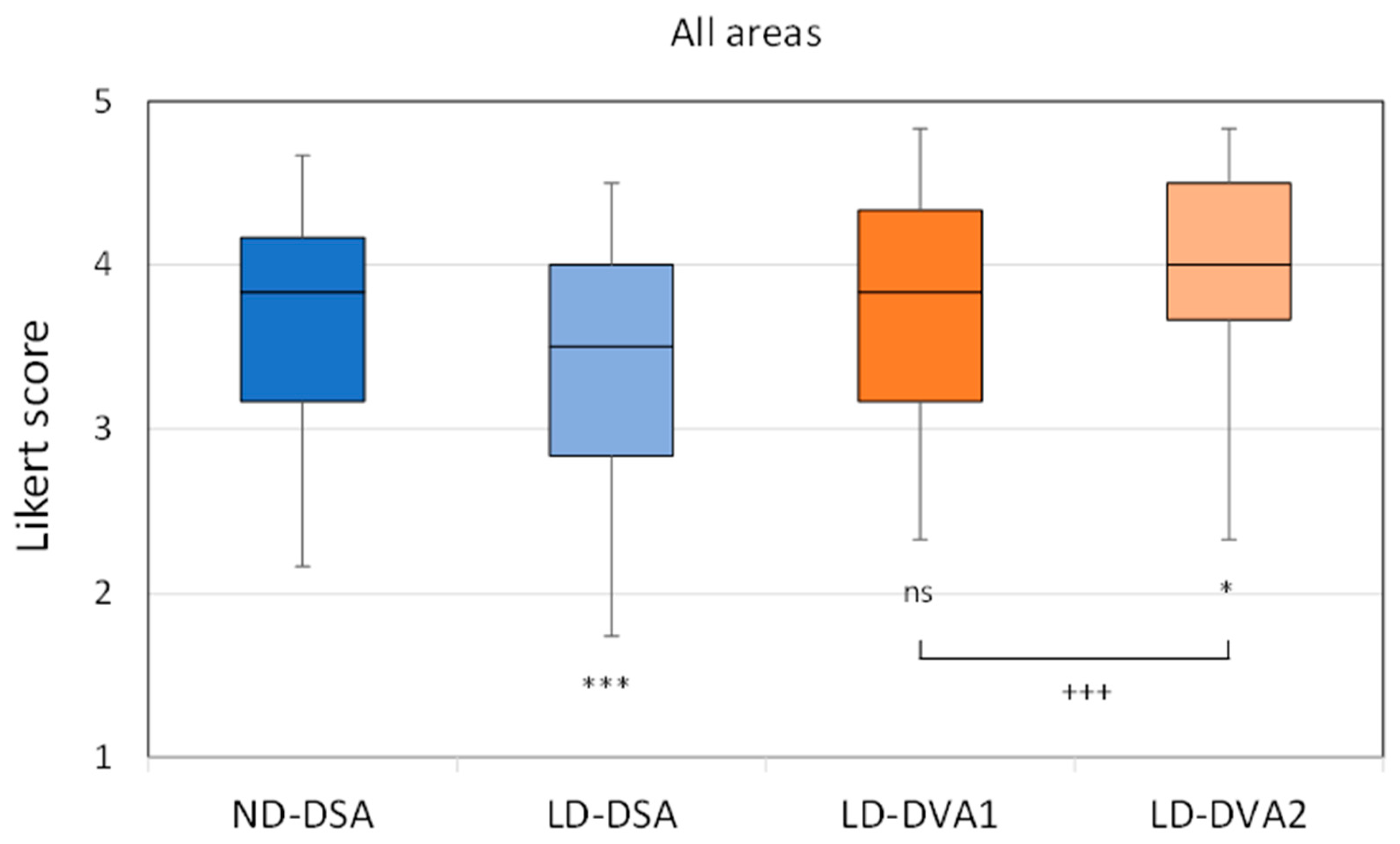
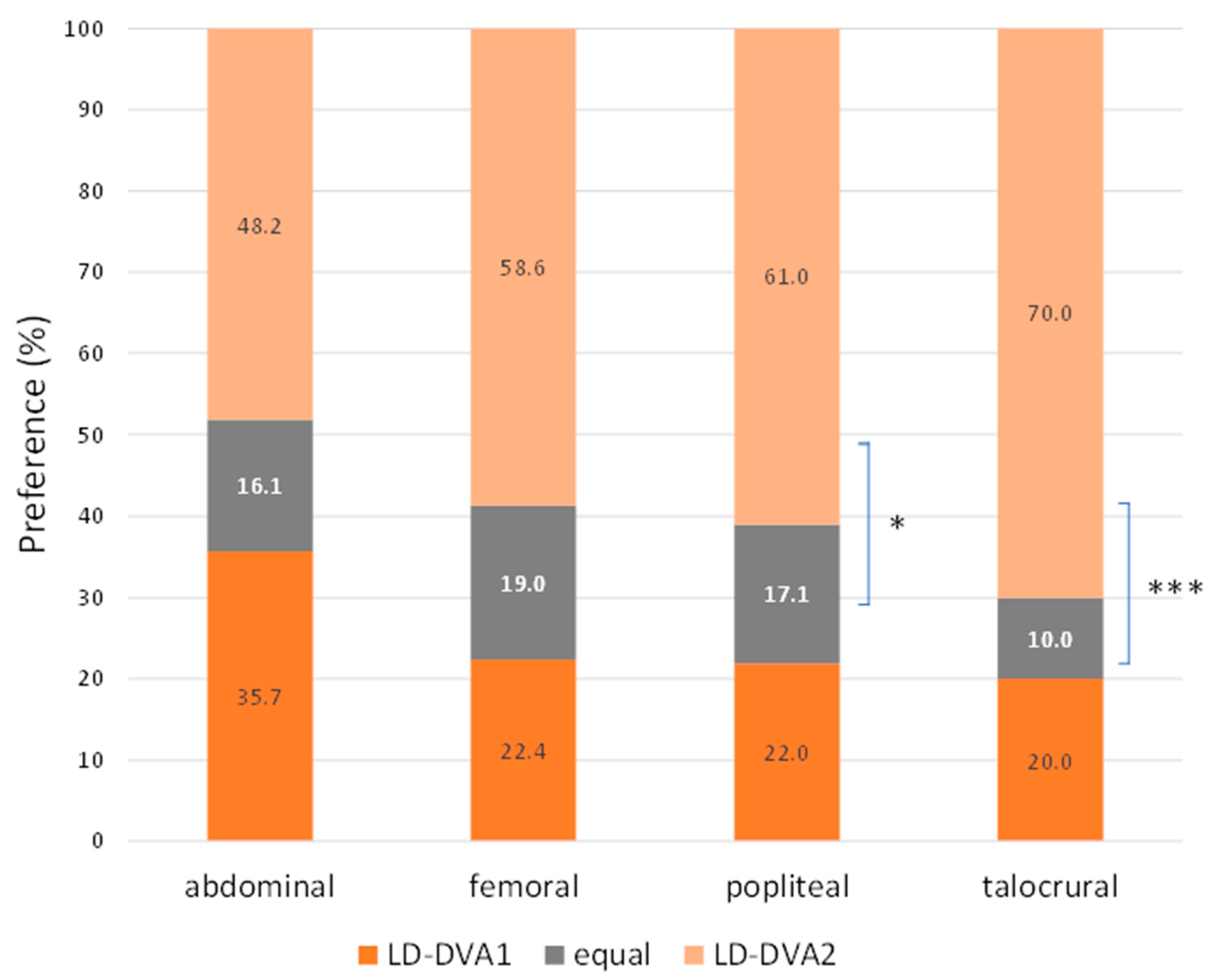
3.3. Visual Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spiliopoulos, S.; Festas, G.; Paraskevopoulos, I.; Mariappan, M.; Brountzos, E. Overcoming ischemia in the diabetic foot: Minimally invasive treatment options. World J. Diabetes 2021, 12, 2011–2026. [Google Scholar] [CrossRef] [PubMed]
- Vogl, T.J.; Alizadeh, L.S.; Maeder, R.; Naguib, N.N.; Herrmann, E.; Bickford, M.W.; Burck, I.; Albrecht, M.H. Advanced Robotic Angiography Systems for Image Guidance During Conventional Transarterial Chemoembolization: Impact on Radiation Dose and Image Quality. Investig. Radiol. 2019, 54, 153–159. [Google Scholar] [CrossRef] [PubMed]
- White, C.J.; Brott, T.G.; Gray, W.A.; Heck, D.; Jovin, T.; Lyden, S.P.; Metzger, D.C.; Rosenfield, K.; Roubin, G.; Sachar, R.; et al. Carotid Artery Stenting: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 80, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-J.; Hong, J.M.; Kim, J.S.; Lee, J.S. Endovascular Treatment for Posterior Circulation Stroke: Ways to Maximize Therapeutic Efficacy. J. Stroke 2022, 24, 207–223. [Google Scholar] [CrossRef]
- Goldsweig, A.M.; Kennedy, K.F.; Abbott, J.D.; Jones, W.S.; Velagapudi, P.; Rutar, F.J.; Curtis, J.C.; Tsai, T.T.; Aronow, H.D. Patient Radiation Dosage During Lower Extremity Endovascular Intervention. JACC Cardiovasc. Interv. 2019, 12, 473–480. [Google Scholar] [CrossRef]
- Roguin, A.; Goldstein, J.; Bar, O.; Goldstein, J.A. Brain and neck tumors among physicians performing interventional procedures. Am. J. Cardiol. 2013, 111, 1368–1372. [Google Scholar] [CrossRef] [PubMed]
- Bernier, M.-O.; Journy, N.; Villoing, D.; Doody, M.M.; Alexander, B.H.; Linet, M.S.; Kitahara, C.M. Cataract Risk in a Cohort of U.S. Radiologic Technologists Performing Nuclear Medicine Procedures. Radiology 2018, 286, 592–601. [Google Scholar] [CrossRef]
- Paulo, G.; Bartal, G.; Vano, E. Radiation Dose of Patients in Fluoroscopically Guided Interventions: An Update. Cardiovasc. Interv. Radiol. 2021, 44, 842–848. [Google Scholar] [CrossRef]
- Bartal, G.; Vano, E.; Paulo, G. Get Protected! Recommendations for Staff in IR. Cardiovasc. Interv. Radiol. 2021, 44, 871–876. [Google Scholar] [CrossRef]
- Santos, J.S.; Uusi-Simola, J.; Kaasalainen, T.; Aho, P.; Venermo, M. Radiation Doses to Staff in a Hybrid Operating Room: An Anthropomorphic Phantom Study with Active Electronic Dosimeters. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 654–660. [Google Scholar] [CrossRef]
- Szigeti, K.; Mathe, D.; Osvath, S. Motion based X-ray imaging modality. IEEE Trans. Med. Imaging 2014, 33, 2031–2038. [Google Scholar] [CrossRef] [PubMed]
- Gyánó, M.; Góg, I.; Óriás, V.I.; Ruzsa, Z.; Nemes, B.; Csobay-Novák, C.; Oláh, Z.; Nagy, Z.; Merkely, B.; Szigeti, K.; et al. Kinetic imaging in lower extremity arteriography: Comparison to digital subtraction angiography. Radiology 2019, 290, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Óriás, V.I.; Gyánó, M.; Góg, I.; Szöllősi, D.; Veres, D.S.; Nagy, Z.; Csobay-Novák, C.; Zoltán, O.; Kiss, J.P.; Osváth, S.; et al. Digital Variance Angiography as a Paradigm Shift in Carbon Dioxide Angiography. Investig. Radiol. 2019, 54, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Bastian, M.B.; König, A.M.; Viniol, S.; Gyánó, M.; Szöllősi, D.; Góg, I.; Kiss, J.P.; Osvath, S.; Szigeti, K.; Mahnken, A.H.; et al. Digital Variance Angiography in Lower-Limb Angiography with Metal Implants. Cardiovasc. Interv. Radiol. 2021, 44, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.P.; Bastian, M.B.; Viniol, S.; König, A.M.; Amin, S.S.; Eldergash, O.; Schnabel, J.; Gyánó, M.; Szöllősi, D.; Góg, I.; et al. Digital variance angiography in selective lower limb interventions. J. Vasc. Interv. Radiol. 2022, 33, 104–112. [Google Scholar] [CrossRef]
- Alizadeh, L.S.; Gyánó, M.; Góg, I.; Szigeti, K.; Osváth, S.; Kiss, J.P.; Yel, I.; Koch, V.; Grünewald, L.D.; Vogl, T.J.; et al. Initial experience using Digital Variance Angiography in context of Prostatic Artery Embolization in comparison with Digital Subtraction Angiography. Acad. Radiol. 2022, 30, 689–697. [Google Scholar] [CrossRef]
- Gyánó, M.; Berczeli, M.; Csobay-Novák, C.; Szöllősi, D.; Óriás, V.I.; Góg, I.; Kiss, J.P.; Veres, D.S.; Szigeti, K.; Osváth, S.; et al. Digital variance angiography allows about 70% decrease of DSA-related radiation exposure in lower limb X-ray angiography. Sci. Rep. 2021, 11, 21790. [Google Scholar] [CrossRef]
- FDA Center for Devices and Radiological Health. Guidance for the submission of 510(k)s for solid state X-ray imaging devices. 2016, Docket number: FDA-1997-N-0389. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/guidance-submission-510ks-solid-state-x-ray-imaging-devices (accessed on 26 April 2023).
- Liu, B.; Hirsch, J.A.; Li, X.; Sheridan, R.M.; Rehani, M.; Zheng, H.; Rabinov, J.D. Radiation Dose Monitoring for Fluoroscopically Guided Interventional Procedures: Effect on Patient Radiation Exposure. Radiology 2019, 290, 744–749. [Google Scholar] [CrossRef]
- Meisinger, Q.C.; Stahl, C.M.; Andre, M.P.; Kinney, T.B.; Newton, I.G. Radiation Protection for the Fluoroscopy Operator and Staff. Am. J. Roentgenol. 2016, 207, 745–754. [Google Scholar] [CrossRef]
- Miller, D.L.; Balter, S.; Schueler, B.A.; Wagner, L.K.; Strauss, K.J.; Vano, E. Clinical radiation management for fluoroscopically guided interventional procedures. Radiology 2010, 257, 321–332. [Google Scholar] [CrossRef]
- Ingwersen, M.; Drabik, A.; Kulka, U.; Oestreicher, U.; Fricke, S.; Krankenberg, H.; Schwencke, C.; Mathey, D. Physicians’ radiation exposure in the catheterization lab: Does the type of procedure matter? JACC Cardiovasc. Interv. 2013, 6, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Óriás, V.I.; Szöllősi, D.; Gyánó, M.; Veres, D.S.; Nardai, S.; Csobay-Novák, C.; Nemes, B.; Kiss, J.P.; Szigeti, K.; Osváth, S.; et al. Initial evidence of a 50% reduction of contrast media using digital variance angiography in endovascular carotid interventions. Eur. J. Radiol. Open 2020, 7, 100288. [Google Scholar] [CrossRef] [PubMed]
- Gyánó, M.; Csobay-Novák, C.; Berczeli, M.; Góg, I.; Kiss, J.P.; Szigeti, K.; Osváth, S.; Nemes, B. Initial Operating Room Experience with Digital Variance Angiography in Carbon Dioxide-Assisted Lower Limb Interventions: A Pilot Study. Cardiovasc. Interv. Radiol. 2020, 43, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Björck, M.; Earnshaw, J.J.; Acosta, S.; Gonçalves, F.B.; Cochennec, F.; Debus, E.; Hinchliffe, R.; Jongkind, V.; Koelemay, M.J.; Menyhei, G.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2020 Clinical Practice Guidelines on the Management of Acute Limb Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 173–218. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.-B.; Suresh, K.R.; Murad, M.H.; et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur. J. Vasc. Endovasc. Surg. 2019, 58, S1–S109. [Google Scholar] [CrossRef]
- Lucatelli, P.; Rocco, B.; Ciaglia, S.; Teodoli, L.; Argirò, R.; Guiu, B.; Saba, L.; Vallati, G.; Spiliopoulos, S.; Patrone, L.; et al. Possible use of digital variance angiography in liver transarterial chemoembolization: A retrospective observational study. Cardiovasc. Interv. Radiol. 2023. Online ahead of print. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total, Median (IQR) or n(%) | ND | LD | p (ND vs. LD) | |
|---|---|---|---|---|
| Male | 83 (72.8) | 38 (66.6) | 45 (88.9) | 0.14 |
| Age (years) | 66 (9) | 68 (9) | 65 (11) | 0.42 |
| BMI (kg/m2) | 26.1 (7.2) | 25 (8) | 26.6 (6.5) | 0.35 |
| GFR (mL/min/1.73 m2) | 87 (16) | 87 (13) | 85 (19) | 0.28 |
| Smoking | 43 (38) | 22 (39) | 21 (37) | 0.91 |
| Hypertension | 82 (72) | 41 (72) | 41 (72) | 1.00 |
| Diabetes mellitus | 51 (45) | 25 (44) | 26 (46) | 0.84 |
| COPD | 16 (14) | 9 (16) | 7 (12) | 0.58 |
| Ischemic heart disease | 38 (33) | 16 (28) | 22 (39) | 0.21 |
| Cerebrovascular disease | 10 (9) | 6 (11) | 4 (7) | 0.50 |
| Fontaine-stage | ||||
| IIB | 58 (51) | 28 (49) | 30 (53) | 0.43 |
| III | 3 (3) | 2 (4) | 1 (2) | 0.50 |
| IV | 53 (47) | 27 (47) | 26 (46) | 0.50 |
| ND | LD | LD/ND (%) | p | ||
|---|---|---|---|---|---|
| Number of DSA acquisitions | 6 (2) | 6 (2) | 100 | 0.41 | |
| Total DAP (µGy*m2) | Median | 1044.8 (1417.3) | 642.3 (614.9) | 62 | <0.0001 |
| Mean | 1544.2 ± 1172.2 | 841.0 ± 633.9 | 54 | ||
| DSA-DAP (µGy*m2) | Median | 724.2 (1002.6) | 279.3 (268.1) | 39 | <0.0001 |
| Mean | 1012.3 ± 790.1 | 372.5 ± 333.1 | 37 | ||
| Fluoro-DAP (µGy*m2) | Median | 349.9 (414.9) | 340.3 (349.7) | 97 | 0.85 |
| Mean | 532.0 ± 556.6 | 468.4 ± 381.9 | 88 | ||
| Contrast use (mL) | 79 (26) | 87 (26) | 110 | 0.13 | |
| Procedural time (min) | 9.5 (6.0) | 10.0 (5.5) | 105 | 0.93 | |
| ND-DSA | LD-DSA | LD-DVA1 | LD-DVA2 | p (DVA1 vs. DVA2) | ||
|---|---|---|---|---|---|---|
| All | Median(SQR) | 3.83 (1.00) | 3.50 (1.17) | 3.83 (1.17) | 4.00 (0.83) | <0.001 |
| p (vs ND-DSA) | <0.001 | >0.999 | 0.028 | |||
| Mean ± SEM | 3.68 ± 0.05 | 3.35 ± 0.05 | 3.69 ± 0.05 | 3.89 ± 0.04 | ||
| Aortoiliac | Median(SQR) | 4.33 (0.66) | 4.00 (0.50) | 4.33 (0.54) | 4.33 (0.50) | 0.55 |
| p (vs ND-DSA) | 0.118 | >0.999 | >0.999 | |||
| Mean ± SEM | 4.20 ± 0.07 | 3.94 ± 0.06 | 4.21 ± 0206 | 4.24 ± 0.06 | ||
| Femoral | Median(SQR) | 4.16 (0.5) | 3.83 (0.66) | 4.17 (0.79) | 4.33 (0.50) | <0.001 |
| p (vs ND-DSA) | <0.001 | >0.9999 | 0.2024 | |||
| Mean ± SEM | 4.19 ± 0.05 | 3.79 ± 0.07 | 4.18 ± 0.06 | 4.35 ± 0.04 | ||
| Popliteal | Median(SQR) | 3.58 (1) | 3.17 (1.16) | 3.67 (0.87) | 4.00 (0.79) | <0.001 |
| p (vs ND-DSA) | 0.2711 | 0.1191 | <0.001 | |||
| Mean ± SEM | 3.41 ± 0.09 | 3.19 ± 0.09 | 3.67 ± 0.08 | 3.89 ± 0.08 | ||
| Talocrural | Median(SQR) | 3.41 (1.00) | 2.83 (1.00) | 3.17 (1.00) | 3.67 (1.00) | <0.001 |
| p (vs ND-DSA) | <0.001 | 0.8736 | ||||
| Mean ± SEM | 3.22 ± 0.08 | 2.7 ± 0.10 | 3.13 ± 0.08 | 3.44 ± 0.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sótonyi, P.; Berczeli, M.; Gyánó, M.; Legeza, P.; Mihály, Z.; Csobay-Novák, C.; Pataki, Á.; Juhász, V.; Góg, I.; Szigeti, K.; et al. Radiation Exposure Reduction by Digital Variance Angiography in Lower Limb Angiography: A Randomized Controlled Trial. J. Cardiovasc. Dev. Dis. 2023, 10, 198. https://doi.org/10.3390/jcdd10050198
Sótonyi P, Berczeli M, Gyánó M, Legeza P, Mihály Z, Csobay-Novák C, Pataki Á, Juhász V, Góg I, Szigeti K, et al. Radiation Exposure Reduction by Digital Variance Angiography in Lower Limb Angiography: A Randomized Controlled Trial. Journal of Cardiovascular Development and Disease. 2023; 10(5):198. https://doi.org/10.3390/jcdd10050198
Chicago/Turabian StyleSótonyi, Péter, Márton Berczeli, Marcell Gyánó, Péter Legeza, Zsuzsanna Mihály, Csaba Csobay-Novák, Ákos Pataki, Viktória Juhász, István Góg, Krisztián Szigeti, and et al. 2023. "Radiation Exposure Reduction by Digital Variance Angiography in Lower Limb Angiography: A Randomized Controlled Trial" Journal of Cardiovascular Development and Disease 10, no. 5: 198. https://doi.org/10.3390/jcdd10050198