
Sudden Cardiac Death in Athletes: Facts and Fallacies
by
 , , ,
, , ,
Jennie Han
1,† ,
,
Andrea Lalario
2,† ,
,
Enzo Merro
2,
Gianfranco Sinagra
2,
Sanjay Sharma
3,
Michael Papadakis
3 and
Gherardo Finocchiaro
3,* 1
Department of Cardiology, Royal Brompton Hospital, London SW3 6NP, UK
2
Department of Cardiology, Azienda Sanitaria Universitaria Integrata Giuliano Isontina (ASUGI), University of Trieste, 34123 Trieste, Italy
3
Cardiovascular Sciences Research Centre, St. George’s, University of London, London SW17 0RE, UK
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
J. Cardiovasc. Dev. Dis. 2023, 10(2), 68; https://doi.org/10.3390/jcdd10020068
Submission received: 28 November 2022
/
Revised: 23 January 2023
/
Accepted: 29 January 2023
/
Published: 5 February 2023
(This article belongs to the Special Issue Cardiovascular Disease in Athletes)
Abstract
:The benefits of exercise for cardiovascular and general health are many. However, sudden cardiac death (SCD) may occur in apparently healthy athletes who perform at the highest levels. A diverse spectrum of diseases is implicated in SCD in athletes, and while atherosclerotic coronary artery disease predominates in individuals of >35 years of age, primary cardiomyopathies and ion channelopathies are prevalent in young individuals. Prevention of SCD in athletes relies on the implementation of health policies aimed at the early identification of arrhythmogenic diseases (such as cardiac screening) and successful resuscitation (such as widespread utilization of automatic external defibrillators and training members of the public on cardiopulmonary resuscitation). This review will focus on the epidemiology and aetiologies of SCD in athletes, and examine fallacies in the approach to this controversial field. Furthermore, potential strategies to prevent these tragic events will be discussed, analysing current practice, gaps in knowledge and future directions.
1. Introduction
The beneficial effects of regular physical activity on general health are well established. Several studies have demonstrated a lower all-cause mortality and incidence of cardiovascular diseases, cancer and metabolic conditions in individuals who engage in regular exercise [1,2,3,4,5,6,7,8,9,10]. Despite these premises, sudden cardiac death (SCD) may occur in apparently healthy individuals, including athletes. Sudden cardiac death is defined as an unexpected death from cardiac causes that occurs within one hour (or within 24 h in unwitnessed cases) from the onset of an acute change in cardiovascular status in the absence of external causal factors [11]. In Western countries, SCD is estimated to account for up to 13–20% of all deaths [11,12].
The epidemiology and aetiology of SCD in athletes is a controversial area. In this review, we will discuss the epidemiological burden of SCD in athletes and the most common underlying aetiologies. We will examine landmark studies and historical fallacies as well as review policies aimed at preventing these tragic events.
2. Methods
The authors approached this topic with the following research questions: (1) What are the incidences, determinants and causes of sudden cardiac death or aborted sudden death in athletes? (2) What are the controversial issues on this topic? (3) What are the issues in differential diagnosis between “athlete’s heart and cardiac conditions that predispose to sudden cardiac death and what are the possible means to prevent sudden death in athletes? Therefore, a systematic search through the web-based engine PubMed was conducted to identify all studies meeting the eligibility criteria. Most relevant studies answering the main research questions were selected. Finally, results are presented systematically, taking in account the complexity of the topic.
3. Incidence of Sudden Cardiac Death in Athletes
Several studies have reported on the epidemiology of SCD in athletes, describing an extremely variable incidence (Table 1) [13,14,15]. Differences among studies are probably due to many factors and most importantly the methodologies used. A unifying definition of “athlete” does not exist, and this inevitably results in a selection bias and heterogeneous approach. The methods of recording SCD events are many (some studies rely on media reports or insurance claims, others on national or regional registries) and differ among studies, as do the approaches to the post-mortem investigations aimed at clarifying the cause of death. Furthermore, some studies include only SCDs, while others also include sudden cardiac arrests (SCAs) in the calculation of events. Finally, public health measures, such as pre-participation cardiac screening and the public availability of automatic external defibrillators (AEDs), are different among countries, and these factors may lead to variability in the assessed incidence of events [16].
3.1. Relationship with Age
The incidence of sports-related SCD increases with age in both non-competitive and competitive sports. The last decades have witnessed an increasing number of “older” (age > 35 years) athletes participating in organized competitive sport events. In the United States, in 2013, 54% of the 19,025,000 participants in competitive running races were ≥35 years of age [26]. As reported by Risgaard et al. [27], the estimated incidence of SCD was 0.47–1.21 per 100,000 person years in young (age ≤ 35 years) competitive athletes compared to 6.64 per 100,000 person years in older (age > 35 years) athletes [27,28]. The incidence of SCD in Minnesota high school athletes (age 12 to 19 years) over 19 academic years was lower: 0.24 per 100,000 athlete years [24]. Harmon et al. [20] described an annual incidence of SCD of 1:43,770 in athletes who were a part of the United States National Collegiate Athletic Association (NCAA) (age 17–23 years). Marijon et al. [29] reported on patients from 35 to 65 years of age who had experienced SCA during sport activities. The mean age was 51.1 ± 8.8 years and sports-related sudden cardiac arrests (SrSCA) occurred in a small proportion of SCA cases (5%), more frequently in middle-age individuals and those with at least one cardiovascular risk factor and a known heart disease.
3.2. Relationship with Sex
Several studies consistently showed that SCD is more common in male compared with female athletes (Table 1). A study by Corrado et al. [18] on more than 110,000 athletes reported an incidence rate of SCD of 2.6/100,000 person years in male athletes compared to 1.1/100,000 person years in female athletes. On the other side of the Atlantic, Maron et al. [21] showed that out of 1049 SCDs in young competitive athletes (median age 19 ± 6 years) in the United States, only 11% occurred in females. This trend also persists despite the increase in female participation in different sports, among ethnicities and at any age [18,21].
A large regional registry in the United Kingdom found that among 748 cases of SCD in individuals who engaged in sport activities (>3 h of organized physical training per week), only 98 (13%) were women [30]. The same study demonstrated a significant lower incidence of death during intense exertion in female athletes compared to male athletes (58% versus 83%; p < 0.001) [30].
The hypotheses explaining the higher incidence of SCD in male athletes include the effect of sex on physiological cardiac adaptation to exercise and chamber remodelling; the higher male prevalence of myocardial fibrosis, which may constitute a substrate for life-threatening arrhythmias [30,31,32]; hormonal factors (where oestrogens may be protective in females); the higher male prevalence of atherosclerotic coronary artery disease; and psychological factors, particularly considering the tendency of males to reach levels of exhaustion and engage in addictive behaviours more frequently [31,33,34].
3.3. Relationship with Ethnicity
Recent studies have shown an association between ethnicity and SCD (Table 1). The NCAA database reported an overall SCD rate among athletes of 1:43,770 student athletes per year [24]. The incidence rose to 1:17,696 athletes per year among black college athletes and to 1:5284 athletes per year in the college basketball Division I African American players subgroup [24]. It was estimated that young African American athletes had a threefold increase in the rate of SCD compared to white athletes, with an incidence rate of 5.6/100,000 per year. These epidemiological trends are consistent with other studies on young athletes in the United States [22,35,36].
A recent prospective study conducted through the National Center for Catastrophic Sports Injury Research in the United States reported on 331 confirmed cases of SCA and SCD (158 survivors, 173 fatalities) and showed that the annual incidence rate among African American male NCAA Division I basketball players was 1:2087 athlete years, the highest compared to other ethnic groups [23].
3.4. Relationship with Type and Intensity of Sport
The type and the level of effort may impact the risk of developing life-threating arrhythmias if an underlying cardiac condition is present. It appears that strenuous exercise performed by competitive athletes, as opposed to recreational exercise, has the potential to lead to a higher risk of SCD (Table 1) [17,21,25]. Sollazzo et al. [12] showed a rate of 1:100,000 SCDs among competitive athletes versus 0.32:100,000 in those practicing leisure activities or recreational sports. Toresdahl et al. [25] reported a relative risk of 3.6 of sudden cardiac arrest in high school campus student athletes compared to their sedentary counterparts. In contrast, a study from Maron et al. [37] reported a threefold higher incidence of SCD among young individuals who did not engage in intense exercise compared to competitive athletes. Sudden cardiac deaths were 8-fold more common in non-athletes [37].
In the United States, the highest incidence of SCD has been reported in basketball players [18,19,21]. In contrast, in Europe, football leads to most sports-related SCD events. According to a study from Malhotra et al. [38], the incidence of SCD was 6.8 per 100,000 athlete years among young football players who were screened with an ECG and health questionnaire at the age of 16. An Italian study reported that 45% of all SCD events in athletes occurred whilst playing football, with a similar percentage (39%) reported in Israel [39,40]. This may be reflective of the greater popularity of both amateur and professional soccer in Europe compared to the United States, which may have influenced the size of the sporting population.
4. Causes of Sudden Cardiac Death
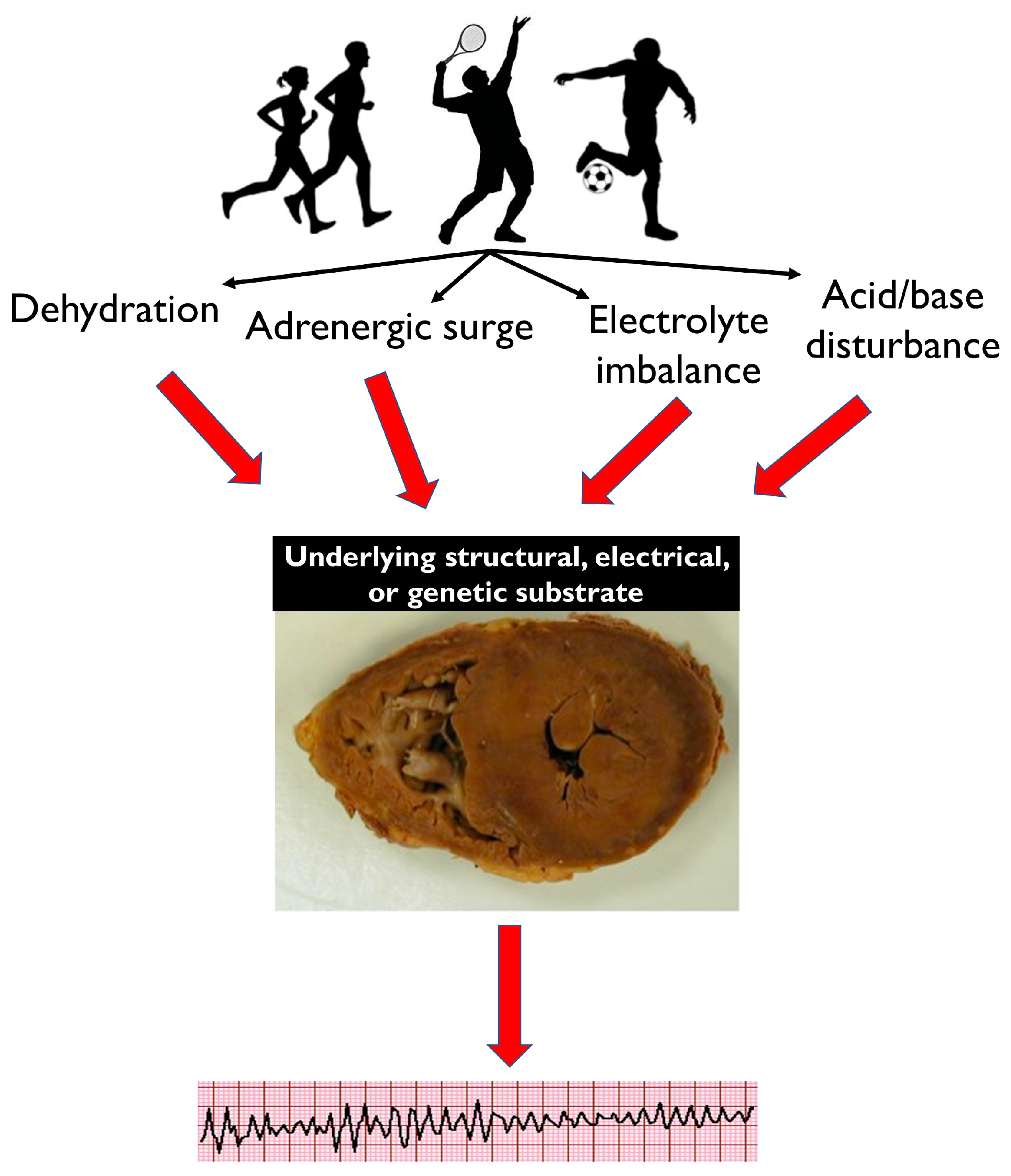
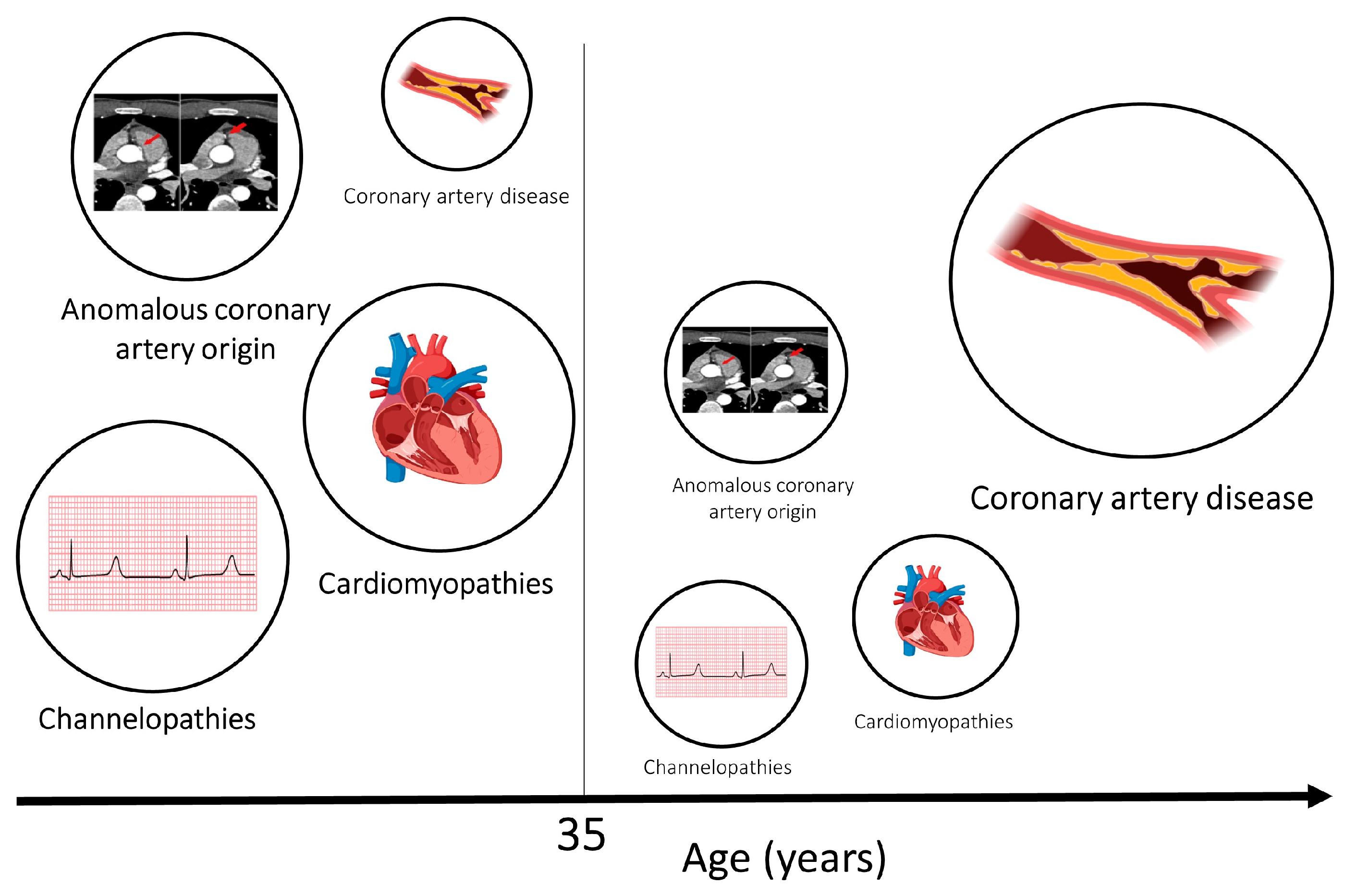
Common physiological effects of intense exercise, such as dehydration, adrenergic surge, electrolyte imbalance and acid/base disturbance, may not be well tolerated by athletes with a pathological electrical or structural substrate, resulting in potentially fatal arrhythmias (Figure 1). A diverse spectrum of diseases is implicated in SCD, with variable prevalence dependent on the demographics of the victims and the circumstances of death. The majority of SCDs are attributable to atherosclerotic coronary artery disease and generally manifest in individuals in the fourth decade onward (Figure 2). The primary cardiomyopathies and ion channelopathies are the predominant causes of SCD in the young (<35 years). The inherited nature of these conditions underscores the need for cardiac evaluation of first-degree relatives of the deceased. Post-mortem examination is an essential first diagnostic step to guiding clinical evaluation of surviving relatives toward inherited structural diseases or primary arrhythmogenic syndromes. Often, the post-mortem assessment is not performed by expert cardiac pathologists through standardized protocols, and this may result in inaccuracy in establishing the cause of death [41,42,43].
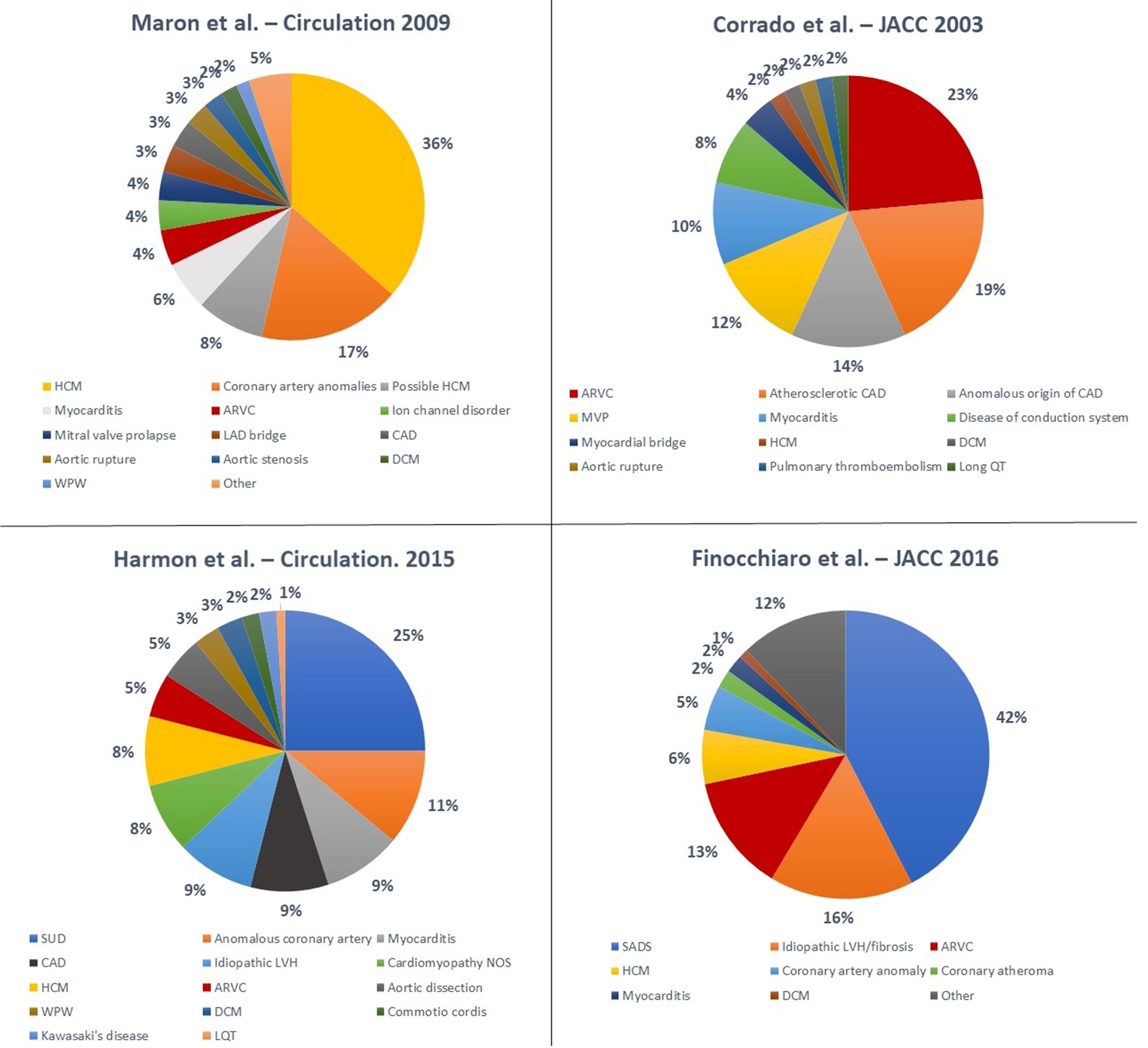
Numerous studies have been conducted to elucidate the underlying aetiologies of SCD in athletes (Figure 3) [18,21,41,44,45]. The variability in terms of results is significant. Hypertrophic cardiomyopathy (HCM) is traditionally considered the most common cause of SCD in young athletes in the United States; Maron et al. [21] reported on the National Registry of SCD in Athletes (based in the United States) and showed that HCM accounted for 36% of all SCD events in young athletes. These data are based on a large cohort but are limited by the fact that an autopsy was not performed in all athletes and was carried out by an expert cardiac pathologist only in the minority of cases.
Recent studies have reported different results (Table 2). A study by Corrado et al. [18] showed that in the Veneto region in Italy, arrhythmogenic right ventricular cardiomyopathy (ARVC) was the most common cause of SCD in young athletes (23% of cases), while HCM accounted for only 2% of deaths. Mandatory pre-participation screening (using the ECG) in Italy may explain the reported low incidence of HCM. In fact, ECG abnormalities are common in HCM, and the disqualification of affected athletes may have prevented SCDs [46].
Eckart et al. [44] examined 902 cases of SCD in active military personnel from the Department of Defense in the United States. These individuals were in active service, and therefore were required to maintain a certain level of fitness. In young individuals (<35 years), the heart appeared structurally normal at the post-mortem examination in 41% of cases. Hypertrophic cardiomyopathy accounted for only 13% of cases. In older individuals the most common cause of death was atherosclerotic disease (73%). This study was retrospective, and most of autopsies were conducted by a local medical examiner with no regular involvement of a specialist cardiac pathologist. Harmon et al. [45] reported that a structurally normal heart at the post-mortem examination was the most common finding (25%) in 64 cases of college athletes who died suddenly. Coronary artery anomalies were the second most frequent cause (11%), and HCM accounted for 8% of the cases.
Finocchiaro et al. [41] described a cohort of 357 athletes who died suddenly in the United Kingdom where the post-mortem examination was performed by an expert cardiac pathologist. The most common finding at the post-mortem examination was a normal heart (42% of cases), followed by myocardial disease including idiopathic left ventricular hypertrophy (LVH) and idiopathic fibrosis (16%), ARVC (13%), and HCM (6%). Coronary artery anomalies were found in 5% of cases.
The interpretation of the post-mortem results is a complex task and uncertainty may exist about the exact significance of certain pathological findings and their causal relationship with SCD. The clinical significance of a structurally normal heart with normal toxicology (defined as sudden arrhythmic death syndrome (SADS)) in the context of SCD is not fully understood. In SADS cases, death is most likely caused by primary arrhythmia syndromes, such as long QT syndrome, Brugada syndrome or catecholaminergic polymorphic tachycardia. Genetic testing of the deceased proband (molecular autopsy) and family screening of family members may help in providing a unifying diagnosis. Recent studies showed that up to 50% of families of SADS victims are affected by an inherited cardiac condition (usually a channelopathy) that can be linked with the SCD in the proband [47,48,49]. In some cases of SADS or unexplained cardiac arrest, pathogenic variants in cardiomyopathy-related genes are found, which raises the possibility of an arrhythmic phenotype preceding a fully expressed structural phenotype [50].
Idiopathic fibrosis and idiopathic LVH are common autopsy findings in young athletes who have died suddenly. The clinical significance of these entities is unclear as they may be incidental and innocent bystanders or may constitute substrates for potentially fatal arrhythmias. Finocchiaro et al. [51] investigated whether idiopathic LVH and familial HCM are part of the same disease. These authors comprehensively assessed first-degree family members of 46 decedents with idiopathic LVH and found that none fulfilled diagnostic criteria for HCM, suggesting that idiopathic LVH is a distinct disease entity.
Although genetic and inherited cardiac conditions are the predominant causes of SCD in young individuals, the contribution of non-genetic and “acquired” factors may be relevant. Specifically, drugs, alcohol and smoking may act as second hits in predisposed individuals, resulting in maladaptation and potentially fatal arrhythmias. The use of performance-enhancing drugs has progressively increased recently. These drugs are constantly under review by the World Anti-Doping Agency (WADA) [52]. Side effects are many and depend on the type of substance, the amount and the duration of use, leading in some cases to tragic consequences, including SCD [53].
Circumstances of Death
Sudden cardiac death in athletes often occurs during exercise, but it can also occur at rest and sometimes during sleep. A recent study on athletes in the United Kingdom showed that 61% of athletes died suddenly during exertion, including a small proportion of individuals (4%) who died during altercation. Of the individuals who died at rest, one-third died while sleeping [41]. Certain cardiac conditions, such as arrhythmogenic cardiomyopathy (AC) and coronary artery anomalies, often lead to SCD during exertion [41]. Intense exercise has been shown to be particularly deleterious in AC, where the higher risk of fatal arrhythmias is often accompanied by a worsening of the phenotype [54,55]. Coronary artery anomalies comprise many anatomical subtypes. A retrospective analysis of 30 cases with an anomalous origin of the coronary artery revealed that anomalous left coronary artery arising from the right sinus of Valsalva was mostly associated with SCD during exercise (73% of SCDs occurred during exercise, compared to 18% in the anomalous right coronary artery arising from the left sinus of Valsalva) [56]. In contrast, in cases of SADS, SCD occurs more often at rest or during sleep [57].
5. Prevention of SCD in Athletes
Sudden cardiac death in athletes may be prevented through the implementation of policies aimed at identifying cardiac conditions that may pose a risk in asymptomatic individuals (screening) and policies that increase the likelihood of successful resuscitation of cardiac arrests.
5.1. Pre-Participation Cardiac Screening
Both the American Heart Association/American College of Cardiology (AHA/ACC) and the European Society of Cardiology (ESC) recommend pre-participation cardiac screening with the aim of identifying cardiac conditions that pose a risk of SCD [58,59,60,61,62]. There is no global consensus on whether or how cardiac screening should be performed, with high variability among countries, sports governing bodies and level of competition. Both American and European guidelines suggest that medical history and physical examination should be part of the cardiac screening assessment [57,58,59,60,61]. However, while the 12-lead ECG is the key investigation proposed by the ESC, this test is not recommended by the AHA, which instead focuses on personal and family history and physical examination [58,59,60]. Corrado et al. [16] showed that the implementation of a mandatory pre-participation cardiac screening program with the use of the ECG led to a significant decrease in the incidence of SCD in athletes. In the Veneto region of Italy, the annual incidence of SCD in athletes decreased by 89% after cardiac screening become compulsory in 1982. In contrast, Maron et al. [63] analysed 13 cases of SCD that occurred in high school student athletes in Minnesota over a 26-year period and reported that only 4 (31%) individuals had cardiovascular conditions that could have been reliably detected through cardiac screening with history, examination and ECG. Furthermore, Steinvil et al. [64] showed that the effect of implementing mandatory pre-participation cardiac screening with ECG and exercise testing in Israel in 1997 did not lead to a significant change in documented events of SCD in competitive athletes. This study relied on the systematic search of two main newspapers in Israel, which constitutes a significant limitation as data were not collected through a prospective database, resulting in a possible underestimation of the events.
If initial tests are suspicious for cardiac disease, further investigations, such as echocardiogram, cardiovascular magnetic resonance, cardio-pulmonary exercise testing and family testing, are recommended. In the presence of a suspicious phenotype, genetic testing may be helpful for diagnosis and risk stratification [58]. Although specific genetic testing can be helpful, in the absence of a suspicious phenotype or a positive proband, genetic screening is not routinely carried out [65]. This is because it has a low yield and variants of unknown significance, which may not be clinically significant, may be found [65].
While pre-participation screening may be ethically justified to prevent SCD in athletes, there are a number of complex ethical issues relating to disqualification decisions [66]. Athletes, especially those competing at very high levels, may perceive disqualification based on the results generated by screening as discrimination on the basis of a medical condition. Moreover, disqualification can cause significant psychological stress in athletes, which may affect their well-being in the long term.
A shared decision-making process regarding sport participation is always advisable, taking into account the lack of robust evidence on the risk of exercise in individuals with cardiac disease. There are certain conditions and situations wherein exercise appears to be deleterious and carries significant risk. These include AC prior cardiac arrest or unexplained syncope, symptomatic/obstructive HCM, DCM with significant impairment of systolic function and/or high-risk genotypes (lamin A/C—filamin C) [58].
The use of mass cardiac screening in athletes remains controversial. The most cited issues are those relating to the economic sustainability of a nationwide screening program, the uncertain benefits in terms of SCD reduction, the potential for false positives and consequential unnecessary disqualifications and the fact that screening does not prevent all cardiac deaths among young athletes [38,61].
5.2. Differential Diagnosis between “Athlete’s Heart” and Pathological Cardiac Conditions
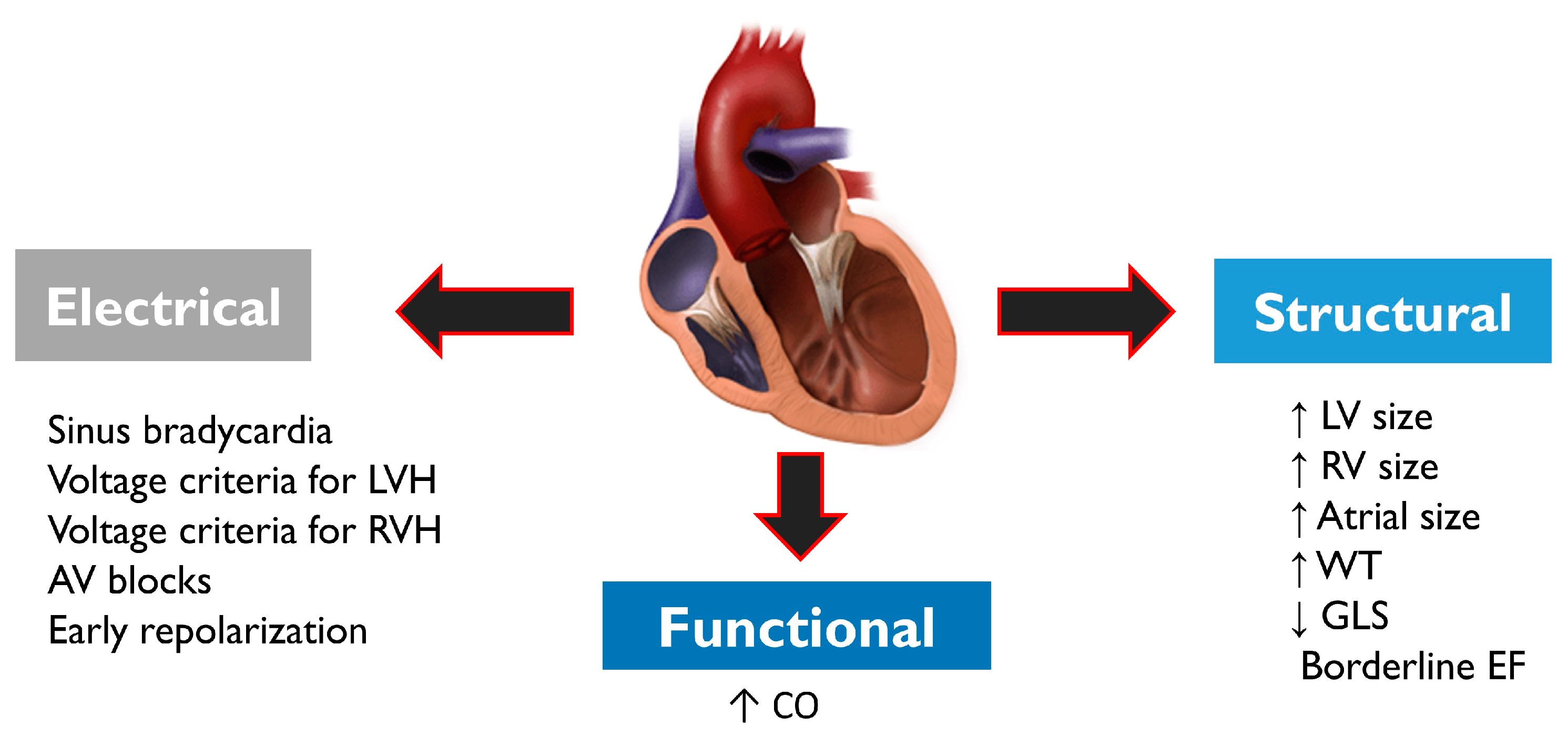
Pre-participation cardiac screening in athletes may lead to further investigations aimed at ruling out cardiac disease. Diagnosis is often complex as athletes usually exhibit a series of electrical, structural and functional physiological changes (Figure 4), which may overlap with cardiac pathology. Structural changes on echocardiogram include an increased cardiac chamber size and myocardial wall thickness. Electrical changes on ECG include sinus bradycardia or arrhythmia, first-degree or Mobitz type 1 atrioventricular block, voltage criteria for ventricular hypertrophy, incomplete right bundle branch block, T-wave inversion and J-point elevation with ascending ST segments [67]. Functional changes include increased diastolic filling and stroke volume. Demographic factors such as sex and ethnicity may influence cardiac adaptation to exercise in athletes; concentric remodelling and hypertrophy of the left ventricle are more prevalent in males, while females more frequently exhibit eccentric LV hypertrophy [32].
5.3. Role of cardiopulmonary resuscitation (CPR) and AEDs
A cornerstone in the prevention of SCD in athletes is the immediate availability of quality CPR performed by bystanders and AEDs. A study based on a dedicated Luxembourg nationwide database showed that the ratio of survival among patients receiving bystander CPR during a cardiac arrest was about 50% [17]. In contrast, all cases of cardiac arrests not having CPR were fatal. The greatest determinant of survival after SCA is the time from collapse to defibrillation, with survival rates declining from 7% to 10% per minute for every minute lost [19].
AEDs should be promptly available so that a first shock can be applied within 3 minutes of the collapse [68]. The role of education in the general population is fundamental, as well as the deployment of external defibrillators in public areas and training and sports grounds to exponentially increase the chance of better outcomes [20]. A recent investigation by Karam et al. [69] described a substantial stability of incidence of sport-related SCA between 2005 and 2018; in the first 2-year period of the study, the estimated incidence was 7.00 per million inhabitants/years compared to 6.24 per million inhabitants/years in the last 2 years. The increased education of the general population in terms of bystander cardiopulmonary resuscitation (CPR) and use of public automated external defibrillators (AEDs) led to a significant improvement in survival to hospital discharge rates (23.8% in the first period compared to 66.7% in the last) [69].
6. Conclusions
Sudden cardiac death is a tragic event that may affect apparently healthy individuals, including athletes. Underlying cardiac conditions may pose a risk of SCD, and the combination of an abnormal electrical or structural substrate with the physiological changes and demands associated with intense exercise may result in fatal arrhythmias. The incidence of SCD is higher in males and in older athletes. While primary cardiomyopathies and channelopathies are the main causes of SCD in young athletes, atherosclerotic coronary artery disease is the prevalent cause of fatal events in veteran athletes. The underlying aetiologies of SCD vary among cohorts, emphasizing the complexity of autopsy interpretation in this context. A structurally normal heart is increasingly found at post-mortem examination in young athletes who die suddenly, suggesting that primary arrhythmia syndromes may often play a role.
Pre-participation cardiac screening is a possible means to identify cardiac conditions that may cause SCD in athletes. While European guidelines recommend the use of a 12-lead ECG, American guidelines focus on personal and family history and physical examination. Cardiac screening in athletes remains controversial, with critics raising concerns regarding the economic sustainability, the cost-effectiveness and the ethical issues related to disqualification. Although early identification of silent cardiac diseases may help in preventing these tragedies, the implementation of policies aimed at the widespread use of AEDs and early CPR remain crucial.
Author Contributions
Conceptualization, G.F.; writing—original draft preparation, J.H., A.L. and E.M.; writing—review and editing, G.F., J.H., A.L. and E.M.; supervision, G.F., G.S., S.S. and M.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mandsager, K.; Harb, S.; Cremer, P.; Phelan, D.; Nissen, S.E.; Jaber, W. Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Netw. Open. 2018, 1, e183605. [Google Scholar] [CrossRef]
- Shiroma, E.J.; Lee, I.-M. Physical activity and cardiovascular health: Lessons learned from epidemiological studies across age, gender, and race/ethnicity. Circulation 2010, 122, 743–752. [Google Scholar] [CrossRef]
- Radford, N.B.; DeFina, L.F.; Leonard, D.; Barlow, C.E.; Willis, B.L.; Gibbons, L.W.; Gilchrist, S.C.; Khera, A.; Levine, B.D. Cardiorespiratory Fitness, Coronary Artery Calcium, and Cardiovascular Disease Events in a Cohort of Generally Healthy Middle-Age Men: Results From the Cooper Center Longitudinal Study. Circulation 2018, 137, 1888–1895. [Google Scholar] [CrossRef]
- Shah, R.V.; Murthy, V.L.; Colangelo, L.A.; Reis, J.; Venkatesh, B.A.; Sharma, R.; Abbasi, S.A.; Goff, D.C.J.; Carr, J.J.; Rana, J.S.; et al. Association of Fitness in Young Adulthood With Survival and Cardiovascular Risk: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. JAMA Intern Med. 2016, 176, 87–95. [Google Scholar] [CrossRef]
- Hussain, N.; Gersh, B.J.; Gonzalez Carta, K.; Sydo, N.; Lopez-Jimenez, F.; Kopecky, S.L.; Thomas, R.J.; Asirvatham, S.J.; Allison, T.G. Impact of Cardiorespiratory Fitness on Frequency of Atrial Fibrillation, Stroke, and All-Cause Mortality. Am. J. Cardiol. 2018, 121, 41–49. [Google Scholar] [CrossRef]
- Juraschek, S.P.; Blaha, M.J.; Whelton, S.P.; Blumenthal, R.; Jones, S.R.; Keteyian, S.J.; Schairer, J.; Brawner, C.A.; Al-Mallah, M.H. Physical fitness and hypertension in a population at risk for cardiovascular disease: The Henry Ford ExerciIse Testing (FIT) Project. J. Am. Heart Assoc. 2014, 3, e001268. [Google Scholar] [CrossRef]
- Juraschek, S.P.; Blaha, M.J.; Blumenthal, R.S.; Brawner, C.; Qureshi, W.; Keteyian, S.J.; Schairer, J.; Ehrman, J.K.; Al-Mallah, M.H. Cardiorespiratory fitness and incident diabetes: The FIT (Henry Ford ExercIse Testing) Project. Diabetes Care 2015, 38, 1075–1081. [Google Scholar] [CrossRef]
- Vainshelboim, B.; Muller, J.; Lima, R.M.; Nead, K.T.; Chester, C.; Chan, K.; Kokkinos, P.; Myers, J. Cardiorespiratory fitness and cancer incidence in men. Ann. Epidemiol. 2017, 27, 442–447. [Google Scholar] [CrossRef]
- Powell, K.E.; King, A.C.; Buchner, D.M.; Campbell, W.W.; DiPietro, L.; Erickson, K.I.; Hillman, C.H.; Jakicic, J.M.; Janz, K.F.; Katzmarzyk, P.T.; et al. The Scientific Foundation for the Physical Activity Guidelines for Americans, 2nd Edition. J. Phys. Act. Health 2018, 16, 1–11. [Google Scholar] [CrossRef]
- Kyu, H.H.; Bachman, V.F.; Alexander, L.T.; Mumford, J.E.; Afshin, A.; Estep, K.; Veerman, J.L.; Delwiche, K.; Iannarone, M.L.; Moyer, M.L.; et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: Systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ 2016, 354, i3857. [Google Scholar] [CrossRef] [Green Version]
- Deo, R.; Albert, C.M. Epidemiology and genetics of sudden cardiac death. Circulation 2012, 125, 620–637. [Google Scholar] [CrossRef]
- Sollazzo, F.; Palmieri, V.; Gervasi, S.F.; Cuccaro, F.; Modica, G.; Narducci, M.L.; Pelargonio, G.; Zeppilli, P.; Bianco, M. Sudden Cardiac Death in Athletes in Italy during 2019: Internet-based epidemiological research. Medicina 2021, 57, 61. [Google Scholar] [CrossRef] [PubMed]
- Link, M.S.; Mark Estes, N.A., 3rd. Sudden cardiac death in the athlete: Bridging the gaps between evidence, policy, and practice. Circulation 2012, 125, 2511–2516. [Google Scholar] [CrossRef] [PubMed]
- Landry, C.H.; Allan, K.S.; Connelly, K.A.; Cunningham, K.; Morrison, L.J.; Dorian, P. Sudden Cardiac Arrest during Participation in Competitive Sports. N. Engl. J. Med. 2017, 377, 1943–1953. [Google Scholar] [CrossRef] [PubMed]
- Harmon, K.G.; Asif, I.M.; Maleszewski, J.J.; Owens, D.S.; Prutkin, J.M.; Salerno, J.C.; Zigman, M.L.; Ellenbogen, R.; Rao, A.L.; Ackerman, M.J.; et al. Incidence and Etiology of Sudden Cardiac Arrest and Death in High School Athletes in the United States. Mayo Clin. Proc. 2016, 91, 1493–1502. [Google Scholar] [CrossRef]
- Corrado, D.; Basso, C.; Pavei, A.; Michieli, P.; Schiavon, M.; Thiene, G. Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. JAMA 2006, 296, 1593–1601. [Google Scholar] [CrossRef]
- Besenius, E.; Cabri, J.; Delagardelle, C.; Stammet, P.; Urhausen, A. Five Years-Results of a Nationwide Database on Sudden Cardiac Events in Sports Practice in Luxembourg. Dtsch Z. Sportmed. 2022, 73, 24–29. [Google Scholar] [CrossRef]
- Corrado, D.; Basso, C.; Rizzoli, G.; Schiavon, M.; Thiene, G. Does sports activity enhance the risk of sudden death in adolescents and young adults? J. Am. Coll. Cardiol. 2003, 42, 1959–1963. [Google Scholar] [CrossRef]
- Drezner, J.A.; Rao, A.L.; Heistand, J.; Bloomingdale, M.K.; Harmon, K.G. Effectiveness of emergency response planning for sudden cardiac arrest in United States high schools with automated external defibrillators. Circulation 2009, 120, 518–525. [Google Scholar] [CrossRef]
- Harmon, K.G.; Asif, I.M.; Klossner, D.; Drezner, J.A. Incidence of sudden cardiac death in National Collegiate Athletic Association Athletes. Circulation 2011, 123, 1594–1600. [Google Scholar] [CrossRef] [Green Version]
- Maron, B.J.; Doerer, J.J.; Haas, T.S.; Tierney, D.M.; Mueller, F.O. Sudden deaths in young competitive athletes: Analysis of 1866 deaths in the United States, 1980-2006. Circulation 2009, 119, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Haas, T.S.; Murphy, C.J.; Ahluwalia, A.; Rutten-Ramos, S. Incidence and causes of sudden death in U.S. college athletes. J. Am. Coll. Cardiol. 2014, 63, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Peterson, D.F.; Kucera, K.; Thomas, L.C.; Maleszewski, J.; Siebert, D.; Lopez-Anderson, M.; Zigman, M.; Schattenkerk, J.; Harmon, K.G.; Drezner, J.A. Aetiology and incidence of sudden cardiac arrest and death in young competitive athletes in the USA: A 4-year prospective study. Br. J. Sports Med. 2021, 55, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.O.; Stovitz, S.D. Incidence of sudden cardiac death in Minnesota high school athletes 1993–2012 screened with standardized pre-participation evaluation. J. Am. Coll. Cardiol. 2013, 62, 1298–1301. [Google Scholar] [CrossRef]
- Toresdahl, B.G.; Rao, A.L.; Harmon, K.G.; Drezner, J.A. Incidence of sudden cardiac arrest in high school student athletes on school campus. Heart Rhythm 2014, 11, 1190–1194. [Google Scholar] [CrossRef]
- State of the Sport—Part III: U.S. Race Trends. Running USA. Available online: http://www.runningusa.org/2014-state-of-the-sport-part-III-us-race-trends (accessed on 9 July 2014).
- Risgaard, B.; Gregers Winkel, B.; Jabbari, R.; Glinge, C.; Ingemann-Hansen, O.; Large Thomsen, J.; Lolk Ottesen, G.; Haunsø, S.; Gaarsdal Holst, A.; Tfelt-Hansen, J. Sports-related sudden cardiac death in a competitive and a noncompetitive athlete population aged 12 to 49 years: Data from an unselected nationwide study in Denmark. Heart Rhythm 2014, 11, 1673–1681. [Google Scholar] [CrossRef]
- Gaarsdal Holst, A.; Gregers Winkel, B.; Theilade, J.; Bayer Kristensen, I.; Large Thomsen, J.; Lolk Ottesen, G.; Hastrup Svendsen, J.; Haunsø, S.; Prescott, E.; Tfelt-Hansen, J. Incidence and etiology of sports-related sudden cardiac death in Denmark—Implications for preparticipation screening. Heart Rhythm 2010, 7, 1365–1371. [Google Scholar] [CrossRef]
- Marijon, E.; Uy-Evanado, A.; Reinier, K.; Teodorescu, C.; Narayanan, K.; Jouven, X.; Gunson, K.; Jui, J.; Chug, S.S. Sudden cardiac arrest during sports activity in middle age. Circulation 2015, 131, 1384–1391. [Google Scholar] [CrossRef]
- Finocchiaro, G.; Westaby, J.; Bhatia, R.; Malhotra, A.; Behr, E.R.; Papadakis, M.; Sharma, S.; Sheppard, M.N. Sudden Death in Female Athletes: Insights From a Large Regional Registry in the United Kingdom. Circulation 2021, 144, 1827–1829. [Google Scholar] [CrossRef]
- Haukilahti, M.A.E.; Holmström, L.; Vähätalo, J.; Kenttä; Tikkanen, J.; Pakanen, L.; Kortelainen Marja-Leena Perkiömäki, J.; Huikuri, H.; Myerburg, R.J.; Juhani Junttila, M. Sudden Cardiac Death in Women: Causes of Death, Autopsy Findings, and Electrocardiographic Risk Markers. Circulation 2019, 139, 1012–1021. [Google Scholar] [CrossRef]
- Finocchiaro, G.; Dhutia, H.; D’Silva, A.; Malhotra, A.; Steriotis, A.; Millar, L.; Prakash, K.; Narain, R.; Papadakis, M.; Sharma, R.; et al. Effect of Sex and Sporting Discipline on LV Adaptation to Exercise. JACC Cardiovasc. Imaging 2017, 10, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Drici, M.D.; Burklow, T.R.; Haridasse, V.; Glazer, R.I.; Woosley, R.L. Sex hormones prolong the QT interval and downregulate Potassium Channel expression in the rabbit heart. Circulation 1996, 94, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Cavasin, M.A.; Sankey, S.S.; Yu, A.-L.; Menon, S.; Yang, X.-P. Estrogen and testosterone have opposing effects on chronic cardiac remodeling and function in mice with myocardial infarction. Am. J. Physiol. Circ. Physiol. 2003, 284, H1560–H1569. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Doerer, J.J.; Haas, T.S.; Tierney, D.M.; Mueller, F.O. Profile and frequency of sudden death in 1463 young competitive athletes: From a 25 year U.S. National registry: 1980–2005. Circulation 2006, 114, II_830. [Google Scholar]
- Maron, B.J.; Shirani, J.; Poliac, L.C.; Mathenge, R.; Roberts, W.C.; Mueller, F.O. Sudden death in young competitive athletes. Clinical, demographic, and pathological profiles. JAMA 1996, 276, 199–204. [Google Scholar] [CrossRef]
- Maron, B.J.; Haas, T.S.; Duncanson, E.R.; Garberich, R.F.; Baker, A.M.; Mackey-Bojack, S. Comparison of the Frequency of Sudden Cardiovascular Deaths in Young Competitive Athletes Versus Nonathletes: Should We Really Screen Only Athletes? Am. J. Cardiol. 2016, 117, 1339–1341. [Google Scholar] [CrossRef]
- Malhotra, A.; Dhutia, H.; Finocchiaro, G.; Gati, S.; Beasley, I.; Clift, P.; Cowie, C.; Kenny, A.; Mayet, J.; Oxborough, D.; et al. Outcomes of Cardiac Screening in Adolescent Soccer Players. N. Engl. J. Med. 2018, 379, 524–534. [Google Scholar] [CrossRef]
- Corrado, D.; Basso, C.; Schiavon, M.; Thiene, G. Screening for hypertrophic cardiomyopathy in young athletes. N. Engl. J. Med. 1998, 339, 364–369. [Google Scholar] [CrossRef]
- Yanai, O.; Phillips, E.D.; Hiss, J. Sudden cardiac death during sport and recreational activities in Israel. J. Clin. Forensic. Med. 2000, 7, 88–91. [Google Scholar] [CrossRef]
- Finocchiaro, G.; Papadakis, M.; Robertus, J.L.; Dhutia, H.; Steriotis, A.K.; Tome, M.; Mellor, G.; Merghani, A.; Malhotra, A.; Behr, E.; et al. Etiology of Sudden Death in Sports: Insights From a United Kingdom Regional Registry. J. Am. Coll. Cardiol. 2016, 67, 2108–2115. [Google Scholar] [CrossRef]
- Basso, C.; Aguilera, B.; Banner, J.; Cohle, S.; d’Amati, G.; de Gouveia, R.H.; di Gioia, C.; Fabre, A.; Gallagher, P.J.; Leone, O.; et al. Association for European Cardiovascular Pathology. Guidelines for autopsy investigation of sudden cardiac death: 2017 update from the Association for European Cardiovascular Pathology. Virchows. Arch. 2017, 471, 691–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiene, G.; Veinot, J.P.; Angelini, A.; Baandrup, U.T.; Basso, C.; Bruneval, P.; Buja, L.M.; Butany, J.; d’Amati, G.; de Gouveia, R.H.; et al. Association for European Cardiovascular Pathology and Society for Cardiovascular Pathology Task Force on Training in Cardiovascular Pathology. AECVP and SCVP 2009 recommendations for training in cardiovascular pathology. Cardiovasc. Pathol. 2010, 19, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Eckart, R.E.; Shry, E.A.; Burke, A.P.; McNear, J.A.; Appel, D.A.; Castillo-Rojas, L.M.; Avedissian, L.; Pearse, L.A.; Potter, R.N.; Tremaine, L.; et al. Sudden death in young adults: An autopsy-based series of a population undergoing active surveillance. J. Am. Coll. Cardiol. 2011, 58, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Harmon, K.G.; Drezner, J.A.; Maleszewski, J.J.; Lopez-Anderson, M.; Owens, D.; Prutkin, J.M.; Asif, I.M.; Klossner, D.; Ackerman, M.J. Pathogeneses of sudden cardiac death in national collegiate athletic association athletes. Circ. Arrhythm. Electrophysiol. 2014, 7, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, G.; Sheikh, N.; Biagini, E.; Papadakis, M.; Maurizi, N.; Sinagra, G.; Pelliccia, A.; Rapezzi, C.; Sharma, S.; Olivotto, I. The electrocardiogram in the diagnosis and management of patients with hypertrophic cardiomyopathy. Heart Rhythm 2020, 17, 142–151. [Google Scholar] [CrossRef]
- Behr, E.R.; Dalageorgou, C.; Christiansen, M.; Syrris, P.; Hughes, S.; Tome Esteban, M.T.; Rowland, E.; Jeffery, S.; McKenna, W.J. Sudden arrhythmic death syndrome: Familial evaluation identifies inheritable heart disease in the majority of families. Eur. Heart J. 2008, 29, 1670–1680. [Google Scholar] [CrossRef]
- Papadakis, M.; Papatheodorou, E.; Mellor, G.; Raju, H.; Bastiaenen, R.; Wijeyeratne, Y.; Wasim, S.; Ensam, B.; Finocchiaro, G.; Gray, B.; et al. The Diagnostic Yield of Brugada Syndrome After Sudden Death With Normal Autopsy. J. Am. Coll. Cardiol. 2018, 71, 1204–1214. [Google Scholar] [CrossRef]
- Lahrouchi, N.; Raju, H.; Lodder, E.M.; Papatheodorou, E.; Ware, J.S.; Papadakis, M.; Tadros, R.; Cole, D.; Skinner, J.R.; Crawford, J.; et al. Utility of Post-Mortem Genetic Testing in Cases of Sudden Arrhythmic Death Syndrome. J. Am. Coll. Cardiol. 2017, 69, 2134–2145. [Google Scholar] [CrossRef]
- Gerull, B.; Brodehl, A. Insights Into Genetics and Pathophysiology of Arrhythmogenic Cardiomyopathy. Curr. Heart Fail. Rep. 2021, 18, 378–390. [Google Scholar] [CrossRef]
- Finocchiaro, G.; Dhutia, H.; Gray, B.; Ensam, B.; Papatheodorou, S.; Miles, C.; Malhotra, A.; Fanton, Z.; Bulleros, P.; Homfray, T.; et al. Diagnostic yield of hypertrophic cardiomyopathy in first-degree relatives of decedents with idiopathic left ventricular hypertrophy. Europace 2020, 22, 632–642. [Google Scholar] [CrossRef]
- Watson, C.J.; Stone, G.L.; Overbeek, D.L.; Chiba, T.; Burns, M.M. Performance-enhancing drugs and the Olympics. J. Intern Med. 2022, 291, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Adami, P.E.; Koutlianos, N.; Baggish, A.; Bermon, S.; Cavarretta, E.; Deligiannis, A.; Furlanello, F.; Kouidi, E.; Marques-Vidal, P.; Niebauer, J.; et al. Cardiovascular effects of doping substances, commonly prescribed medications and ergogenic aids in relation to sports: A position statement of the sport cardiology and exercise nucleus of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2022, 29, 559–575. [Google Scholar] [CrossRef] [PubMed]
- James, C.A.; Bhonsale, A.; Tichnell, C.; Murray, B.; Russell, S.D.; Tandri, H.; Tedford, R.J.; Judge, D.P.; Calkins, H. Exercise increases age-related penetrance and arrhythmic risk in arrhythmogenic right ventricular dysplasia/cardiomyopathy-associated desmosomal mutation carriers. J. Am. Coll. Cardiol. 2013, 62, 1290–1297. [Google Scholar] [CrossRef]
- Sawant, A.C.; Bhonsale, A.; te Riele, A.S.J.M.; Tichnell, C.; Murray, B.; Russell, S.D.; Tandri, H.; Tedford, R.J.; Judge, D.P.; Calkins, H.; et al. Exercise has a disproportionate role in the pathogenesis of arrhythmogenic right ventricular dysplasia/cardiomyopathy in patients without desmosomal mutations. J. Am. Heart Assoc. 2014, 3, e001471. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, G.; Behr, E.R.; Tanzarella, G.; Papadakis, M.; Malhotra, A.; Dhutia, H.; Miles, C.; Diemberger, I.; Sharma, S.; Sheppard, M.N. Anomalous Coronary Artery Origin and Sudden Cardiac Death: Clinical and Pathological Insights From a National Pathology Registry. JACC Clin. Electrophysiol. 2019, 5, 516–522. [Google Scholar] [CrossRef]
- Bagnall, R.D.; Weintraub, R.G.; Ingles, J.; Duflou, J.; Yeates, L.; Lam, L.; Davis, A.M.; Thompson, T.; Connell, V.; Wallace, J.; et al. A Prospective Study of Sudden Cardiac Death among Children and Young Adults. N. Engl. J Med. 2016, 374, 2441–2452. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet Jean-Philippe Corrado, D.; Drezner, J.A.; Halle, M.; Hansen, D.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease: The Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef]
- Corrado, D.; Pelliccia, A.; Bjørnstad, H.H.; Vanhees, L.; Biffi, A.; Borjesson, M.; Panhuyzen-Goedkoop, N.; Deligiannis, A.; Solberg, E.; Dugmore, D.; et al. Cardiovascular pre-participation screening of young competitive athletes for prevention of sudden death: Proposal for a common European protocol. Consensus Statement of the Study Group of Sport Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur. Heart J. 2005, 26, 516–524. [Google Scholar]
- Maron, B.J.; Levine, B.D.; Washington, R.L.; Baggish, A.L.; Kovacs, R.J.; Maron, M.S. Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 2: Preparticipation Screening for Cardiovascular Disease in Competitive Athletes: A Scientific Statement From the American Heart Association and American College of Cardiology. J. Am. Coll. Cardiol. 2015, 66, 2356–2361. [Google Scholar]
- Drezner, J.A.; O’Connor, F.G.; Harmon, K.G.; Fields, K.B.; Asplund, C.A.; Asif, I.M.; Price, D.E.; Dimeff, R.J.; Bernhardt, D.T.; Roberts, W.O. AMSSM Position Statement on Cardiovascular Preparticipation Screening in Athletes: Current evidence, knowledge gaps, recommendations and future directions. Br. J. Sports Med. 2017, 51, 153–167. [Google Scholar] [CrossRef]
- American Academy of Family Physicians; American College of Sports Medicine; American Medical Society for Sports Medicine; American Orthopaedic Society for Sports Medicine; American Osteopathic Academy of Sports Medicine. Preparticipation Physical Evaluation, 4th ed.; American Academy of Pediatrics: Itasca, IL, USA, 2012. [Google Scholar]
- Maron, B.J.; Haas, T.S.; Ahluwalia, A.; Rutten-Ramos, S.C. Incidence of cardiovascular sudden deaths in Minnesota high school athletes. Heart Rhythm 2013, 10, 374–377. [Google Scholar] [CrossRef] [PubMed]
- Steinvil, A.; Chundadze, T.; Zeltser, D.; Rogowski, O.; Halkin, A.; Galily, Y.; Perluk, H.; Viskin, S. Mandatory electrocardiographic screening of athletes to reduce their risk for sudden death: Proven fact or wishful thinking? J. Am. Coll. Cardiol. 2011, 57, 1291–1296. [Google Scholar] [CrossRef]
- Vogiatzi, G.; Lazaros, G.; Oikonomou, E.; Lazarou, E.; Vavuranakis, E.; Tousoulis, D. Role of genetic testing in cardiomyopathies: A primer for cardiologists. World J. Cardiol. 2022, 14, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Magavern, E.F.; Finocchiaro, G.; Sharma, S.; Papadakis, M.; Borry, P. Time out: Ethical reflections on medical disqualification of athletes in the context of mandated pre-participation cardiac screening. Br. J. Sports Med. 2018, 52, 1207–1210. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Merghani, A.; Mont, L. Exercise and the heart: The good, the bad, and the ugly. Eur. Heart J. 2015, 36, 1445–1453. [Google Scholar] [CrossRef] [PubMed]
- Casa, D.J.; Almquist, J.; Anderson, S.A.; Baker, L.; Bergeron, M.F.; Biagioli, B.; Boden, B.; Brenner, J.S.; Carroll, M.; Colgate, B.; et al. The inter-association task force for preventing sudden death in secondary school athletics programs: Best-practices recommendations. J. Athl. Train. 2013, 48, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Karam, N.; Pechmajou, L.; Narayanan, K.; Bougouin, W.; Sharifzadehgan, A.; Anys, S.; Weizman, O.; Perrot, D.; Waldmann, V.; Baganton, F.; et al. Evolutions of Incidence, Management, and Outcomes Over Time in Sports-Related Sudden Cardiac Arrest. J. Am. Coll Cardiol. 2022, 79, 238–246. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Dehydration, adrenergic surge, electrolyte imbalance and acid/base disturbance are common physiological effects of intense exercise. While these are well tolerated by healthy athletes, they may cause potentially fatal arrhythmias in individuals with an underlying electrical, structural or genetic pathological cardiac substrate. This image of a heart at post-mortem is suggestive of HCM, and this is used as an example.
Figure 1.
Dehydration, adrenergic surge, electrolyte imbalance and acid/base disturbance are common physiological effects of intense exercise. While these are well tolerated by healthy athletes, they may cause potentially fatal arrhythmias in individuals with an underlying electrical, structural or genetic pathological cardiac substrate. This image of a heart at post-mortem is suggestive of HCM, and this is used as an example.

Figure 2.
Aetiologies of SCD in athletes and age. Cardiomyopathies, channelopathies and congenital anomalies of the coronary arteries are prevalent causes in younger individuals. Atherosclerotic coronary artery disease is the most common cause of sudden cardiac death and sudden cardiac arrest in older individuals. The size of the circles relate to the relative frequency of SCD caused by the respective pathology. Age 35 has been used as a threshold as this is the most frequently used age in the literature; however, a clear line in terms of age is difficult to draw.
Figure 2.
Aetiologies of SCD in athletes and age. Cardiomyopathies, channelopathies and congenital anomalies of the coronary arteries are prevalent causes in younger individuals. Atherosclerotic coronary artery disease is the most common cause of sudden cardiac death and sudden cardiac arrest in older individuals. The size of the circles relate to the relative frequency of SCD caused by the respective pathology. Age 35 has been used as a threshold as this is the most frequently used age in the literature; however, a clear line in terms of age is difficult to draw.

Figure 3.
Summary of main studies describing the causes of SCD in athletes. Abbreviations: ARVC—arrhythmogenic right ventricular cardiomyopathy; CAD—coronary artery disease; DCM—dilated cardiomyopathy; HCM—hypertrophic cardiomyopathy; LAD—left anterior descending artery; LQT—long QT; LVH—left ventricular hypertrophy; MVP—mitral valve prolapse; NOS—not otherwise specified; SADS—sudden arrhythmic death syndrome; SUD—sudden unexplained death; WPW—Wolff–Parkinson–White [18,21,41,45].
Figure 3.
Summary of main studies describing the causes of SCD in athletes. Abbreviations: ARVC—arrhythmogenic right ventricular cardiomyopathy; CAD—coronary artery disease; DCM—dilated cardiomyopathy; HCM—hypertrophic cardiomyopathy; LAD—left anterior descending artery; LQT—long QT; LVH—left ventricular hypertrophy; MVP—mitral valve prolapse; NOS—not otherwise specified; SADS—sudden arrhythmic death syndrome; SUD—sudden unexplained death; WPW—Wolff–Parkinson–White [18,21,41,45].

Figure 4.
Structural, electrical and functional physiological changes commonly observed in athletes. Physiological changes may overlap with cardiac conditions that may pose a risk of SCD, and therefore differential diagnosis is very important. Abbreviations: AV—atrioventricular; CO—cardiac output; EF—ejection fraction; GLS—global longitudinal strain; LV—left ventricle; LVH—left ventricular hypertrophy; RV—right ventricle; RVH—right ventricular hypertrophy; WT: wall thickness.
Figure 4.
Structural, electrical and functional physiological changes commonly observed in athletes. Physiological changes may overlap with cardiac conditions that may pose a risk of SCD, and therefore differential diagnosis is very important. Abbreviations: AV—atrioventricular; CO—cardiac output; EF—ejection fraction; GLS—global longitudinal strain; LV—left ventricle; LVH—left ventricular hypertrophy; RV—right ventricle; RVH—right ventricular hypertrophy; WT: wall thickness.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Main studies reporting on Incidence of SCD in athletes.
| Authors—Year—Country Study Design | Case Identification | Denominator | SCD or SCA + SCD | Years Studied (n° of Years) | Population | Incidence | Age Range (Mean Age) | Number of Deaths |
|---|---|---|---|---|---|---|---|---|
| Besenius—2022—Luxembourg Prospective [17] | Declaration by the general population (online questionnaires, public media, informed patients followed by the national cardiology institute and cardiac re-education centres, direct witnesses, and other publicly available information) | Cases of SrSCD on national territory or outside Luxembourg suffered by a Luxembourgish resident or sports license holder | SCD + SCA (+ myocardial infarctions and acute coronary syndromes) | 2015–2019 (5) | Physically active population (competitive and non-competitive) | 2.6 cases/year/100,000 physically active inhabitants | 17–80 (49.7) | 43 (17 fatal) |
| Corrado—2003—Italy Prospective [18] | Mandatory death reporting | Registered Italian athletes | SCD | 1979–1999 (20) | Athletes and young people | 1:47,600 athlete 1:142,900 young people | 12–35 (23) | 55 |
| Drezner—2005—USA Retrospective | Survey answered by 244/326 Div. I NCAA institutions | Number of athletes at surveyed schools | SCD | College athletes | 1:67,000 | 5 | ||
| Drezner—2009—USA Cross-sectional survey [19] | 1710 high schools with AEDs surveyed for SCA or SCD | Number of student athletes reported by schools | SCA + SCD | 2006–2007 (within 6 months of survey) | High school athletes | 1:23,000 SCA + SCD 1:46,000 SCD | 14–17 (16) | 14 |
| Drezner—2014—USA Retrospective | Media reports | NFHS | SCA + SCD | 2003–2013 (10) | High school athletes | 1:153,846 SCD 1:71,428 SCA 1:21,277 male basketball | 14–18 | 6 SCD 7 SCA |
| Harmon—2011—USA Retrospective [20] | Parent Heat Watch database, NCAA Resolutions list, insurance claims | Participation data from NCAA | SCD | 2004–2008 (4) | College athletes | 1:43,770 | 18–26 (20) | 37 |
| Harmon—2014—USA Retrospective | Media reports | NFHS | SCA + SCD | 2007–2013 (5) | High school athletes | 1:63,988 SCA 1:41,662 male 1:33,815 male basketball | 14–18 | 74 SCD 35 SCA |
| Holst—2010—Denmark Retrospective | Review of death certificates, then autopsies if available | Denmark population statistics | SCD | 2000–2006 (7) | Athletes and young people | 1:82,645 SrSCD 1:26,595 general population | 12–35 (26) | 15 SrSCD 470 SCD |
| Maron—1996—USA Retrospective | US Registry for Sudden Death in Athletes | “Unavoidable selection bias and certainly significantly underestimated” | SCD | 1985–1995 (10) | Athletes | 12–40 (17) | 134 | |
| Maron—1998—USA Retrospective | Insurance claims | Minnesota State High School League | SCD | 1985–1997 (12) | High school athlete | 1:217,000 overall 1:129,000 male 0 for female | 16–17 (16.5) | 3 |
| Maron—2003—USA Retrospective | US Registry for Sudden Death in Athletes | Not possible b/c of selection bias | SCD | 1985–2000 (25) | Athletes | 9–40 (17) | 286 | |
| Maron—2009—USA Retrospective [21] | US Registry for Sudden Death in Athletes | Not described (estimated 10.7 million athletes < 39 participating in sports during 2000-2006) | SCA + SCD | 1980–2006 (27) | Athletes | 1:163,934 | 8–39 (18) | 690 |
| Maron—2013—USA Retrospective | US Registry of Sudden Death in Athletes | Minnesota State High School League | SCD | 1986–2011 (26) | High school athletes | 1:150,000 | 12–18 (16) | 13 |
| Maron—2014—USA Retrospective [22] | US Registry for Sudden Death in Athletes and NCAA resolutions list for cardiac cases | Participation data from NCAA | SCD | 2002–2011 (9) | College athletes | 1:62,000 presumed 1:83,000 confirmed | 17–26 (20) | 64 |
| Peterson—2021—USA Prospective [23] | National Center for Catastrophic Sports Injury Research in collaboration with national sports organizations | Participation data from National Federation of State High School Associations and NCAA | SCD + SCA | 2014–2018 (4) | Competitive athletes | High school level: 1:65,872 athlete years NCAA level: 1:50,768 athlete-year | 11–29 (16.7) | 331 SCA + SCD 173 SCD |
| Roberts—2013—USA Retrospective [24] | MSHSL records | Participation data from MSHSL records | SCD | 1993–2012 (19) | High school athletes | 0.24 per 100,000 athlete years | 12–19 (“most aged 15 to 18”) | 4 |
| Steinvil—2011—Israel Retrospective | Retrospective review (2 Israeli newspapers by 2 media researchers) | 45,000 registered competitive athletes in 2009, extrapolating the growth of the Israeli population for those aged 10–40 born after 1985 based on a figure allowed for presumed doubling of the sport-participating population | SCD | 1985–2009 (24) | Athletes | 1st 1:39,370 2nd 1:37,593 | 12–44 (24) | 24 |
| Toresdahl—2014—USA Prospective [25] | 2149 schools with cases of SCA + SCD occurred on school campus | Number of student athletes reported by schools | SCA + SCD | 2009–2011 (2) | High school athletes | 1:87,719 SCA + SCD 1:57,000 male SCA + SCD | 14–18 | 18 SCA + SCD 2 SCD |
| Van Camp—1996—USA Retrospective | National Center for Catastrophic Injury Research and media database | 17 sports, participants in NCAA, NFHS, NAIA, NJCAA, added together, conversion factor (1.9 for high school and 1.2 for college) to account for multisport athletes, used “based on discussions with representatives from the national organisations” | SCD | 1983–1993 (10) | College athletes and high school | 1:300,000 | 17–24 (17) | 100 |
In bold: studies focused on SrSCD or SCA during sports activities. ADHD—attention-deficit hyperactivity disorder; AED—automatic external defibrillators; CV—cardiovascular; DOD—Department of Defense; EMS—emergency medical services; MSHSL—Minnesota High School League; NAIA—National Association of Intercollegiate Athletics; NCAA—US National Collegiate Athletic Association; NFHS—National Federation of State High School Associations; NJCAA—National Junior College Athletic Association; SCA—sudden cardiac arrest; SCD—sudden cardiac death; SrSCD—sports related sudden cardiac death.
Table 2.
Causes of death in athletes.
| Author | Year | Country | Study Design | Case Identification | SCD or SCA + SCD | Years Studied | Population of SCD | Cause of Death | Post-Mortem Assessment |
|---|---|---|---|---|---|---|---|---|---|
| Maron [21] | 2009 | USA | Retrospective cohort | US National Registry of Sudden Death in Athletes | SCA + SCD | 1980–2006 | 690 competitive athletes | HCM (36%), anomalous origin of coronary artery (17%), possible HCM (8%), myocarditis (6%), ARVC (4%), channelopathies (4%) | Autopsy reports by local medical examiners—some primary pathological material selectively analysed |
| Corrado [18] | 2003 | Italy | Prospective cohort | Center for Sports Medicine in Padua | SCD | 1979–1999 | 51 competitive athletes | ARVC (23%), coronary atherosclerosis (19%), anomalous origin of coronary artery (14%), MVP (12%), myocarditis (10%), conduction disease (8%), HCM (2%). | Post-mortem assessment of heart by expert cardiac pathologist |
| Eckart [44] | 2011 | USA | Retrospective cohort | Department of Defense Cardiovascular Death Registry | SCD | 1998–2008 | 902 uniformed personnel from the Department of Defense | <35y—SUD (41.3%), atherosclerotic disease (23.2%), HCM (12.8%), myocarditis (5.7%), DCM (4.7%) ≥35y—atherosclerotic disease (73.2%), SUD (10.6), DCM (3.5%), HCM (3.1%) | Autopsy by medical examiners and Department of Defense, clinical cause of death adjudicated by authors |
| Harmon [45] | 2015 | USA | Retrospective cohort | National Collegiate Athletic Association database (Parent Heart Watch and insurance claims) | SCD | 2003–2013 | 64 NCAA (college) Athletes | SUD (25%), coronary artery abnormalities (11%), myocarditis (9%), coronary artery disease (9%) DCM (8%), HCM (8%), idiopathic LVH/possible HCM (8%), ARVC (5%) | Autopsy reports reviewed by panel of experts including cardiac pathologist |
| Finocchiaro [41] | 2016 | UK | Retrospective cohort | Cardiac Risk in the Young database | SCD | 1994–2014 | 357 individuals engaging in regular sport activity (>3 h training/week) | Normal post-mortem (42%), LVH/fibrosis (16%), ARVC (13%), HCM (6%), coronary artery anomaly (5%) | Post-mortem assessment of heart by expert cardiac pathologist |
ARVC—arrhythmogenic right ventricular cardiomyopathy; DCM—dilated cardiomyopathy; HCM—hypertrophic cardiomyopathy; LVH—left ventricular cardiomyopathy; NCAA—National Collegiate Athletic Association; SCA—sudden cardiac arrest; SCD—sudden cardiac death; SUD—sudden unexplained death.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Han, J.; Lalario, A.; Merro, E.; Sinagra, G.; Sharma, S.; Papadakis, M.; Finocchiaro, G. Sudden Cardiac Death in Athletes: Facts and Fallacies. J. Cardiovasc. Dev. Dis. 2023, 10, 68. https://doi.org/10.3390/jcdd10020068
AMA Style
Han J, Lalario A, Merro E, Sinagra G, Sharma S, Papadakis M, Finocchiaro G. Sudden Cardiac Death in Athletes: Facts and Fallacies. Journal of Cardiovascular Development and Disease. 2023; 10(2):68. https://doi.org/10.3390/jcdd10020068
Chicago/Turabian StyleHan, Jennie, Andrea Lalario, Enzo Merro, Gianfranco Sinagra, Sanjay Sharma, Michael Papadakis, and Gherardo Finocchiaro. 2023. "Sudden Cardiac Death in Athletes: Facts and Fallacies" Journal of Cardiovascular Development and Disease 10, no. 2: 68. https://doi.org/10.3390/jcdd10020068
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.