
Pulmonary Vasodilator Therapy in Severe Pulmonary Hypertension Due to Chronic Obstructive Pulmonary Disease (Severe PH-COPD): A Systematic Review and Meta-Analysis
 , ,
, , 

Abstract
:1. Background
2. Study Designs and Methods
2.1. Protocol and Registration
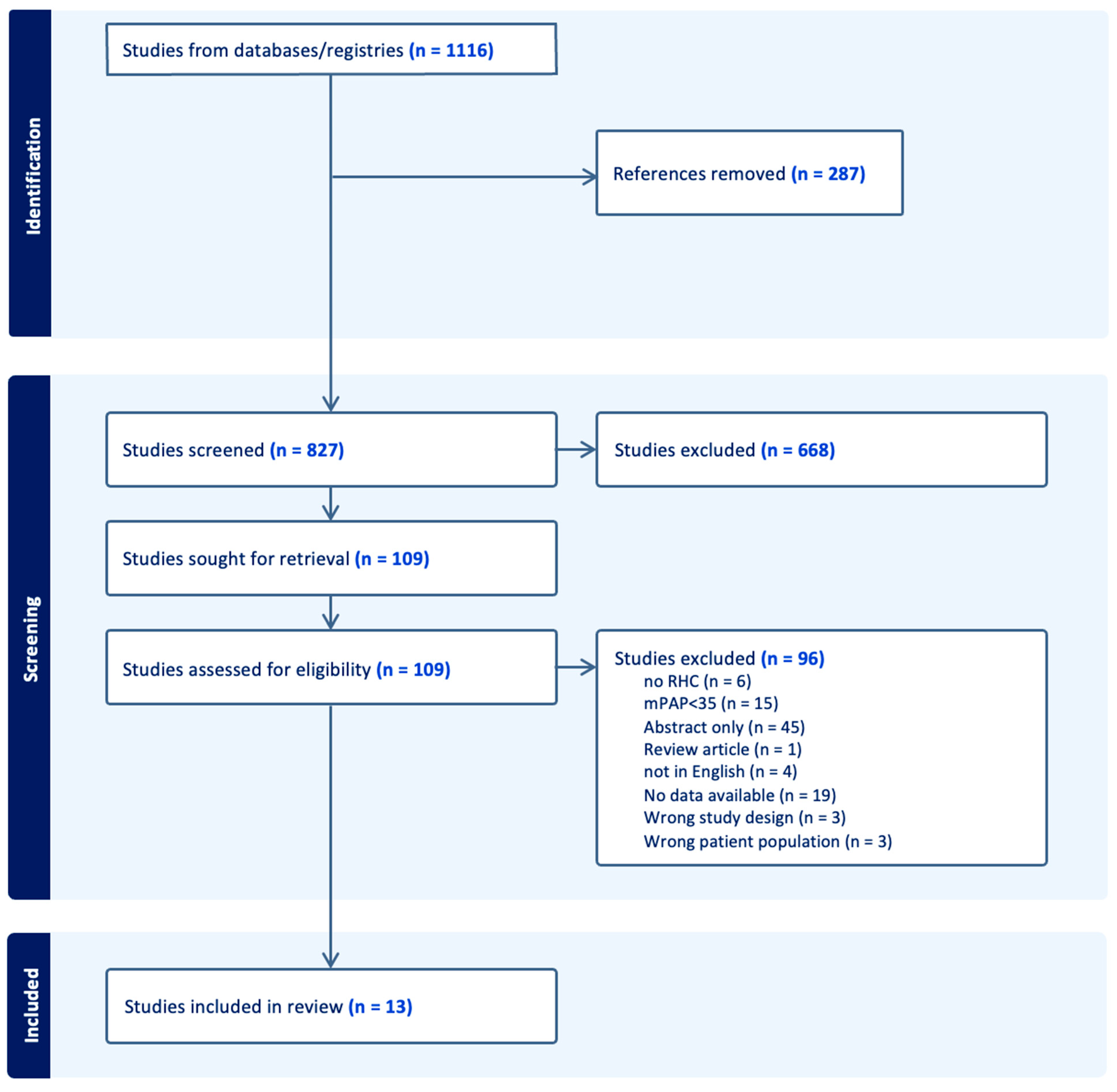
2.2. Search Strategy
2.3. Data Extraction
2.4. Statistical Analysis
2.5. Quality of the Included Studies
3. Results
3.1. Study Characteristics
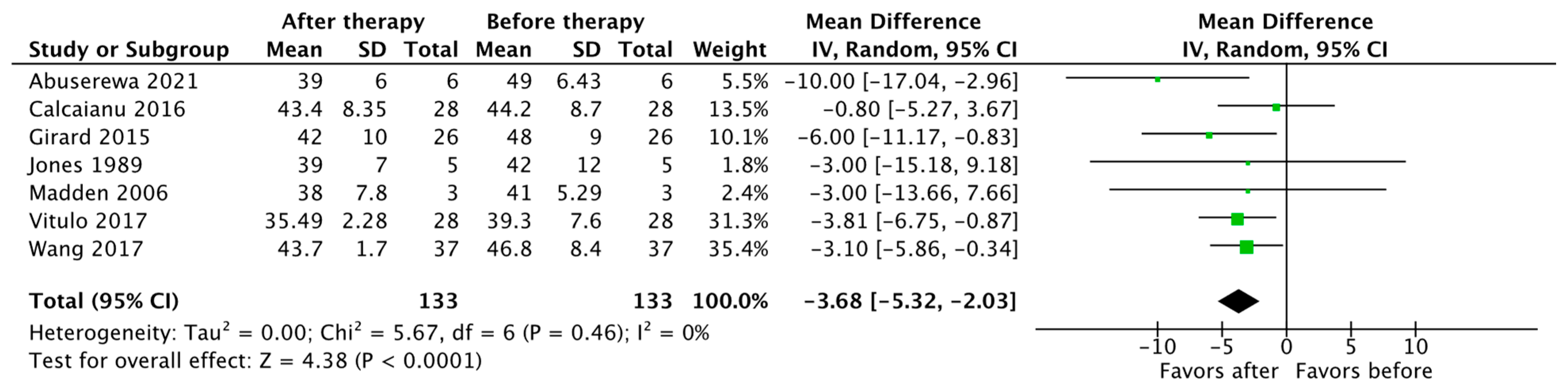
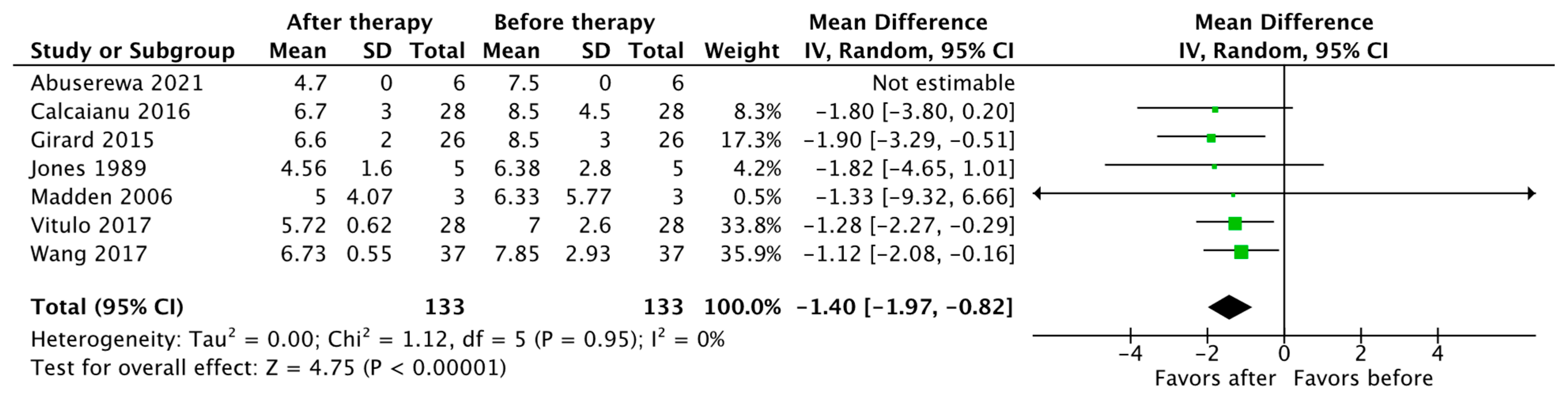
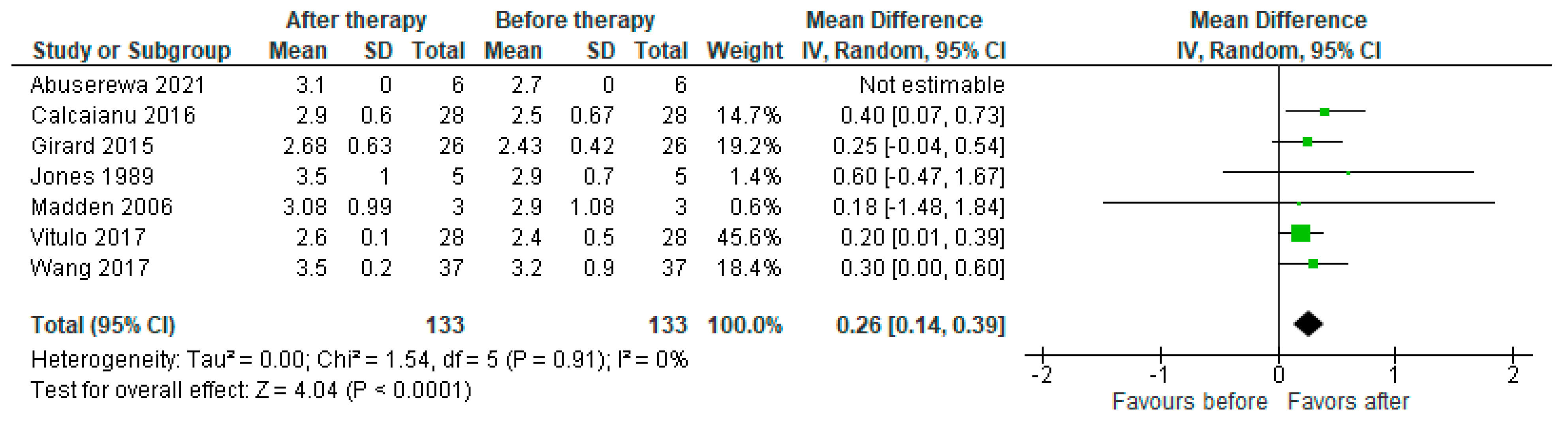
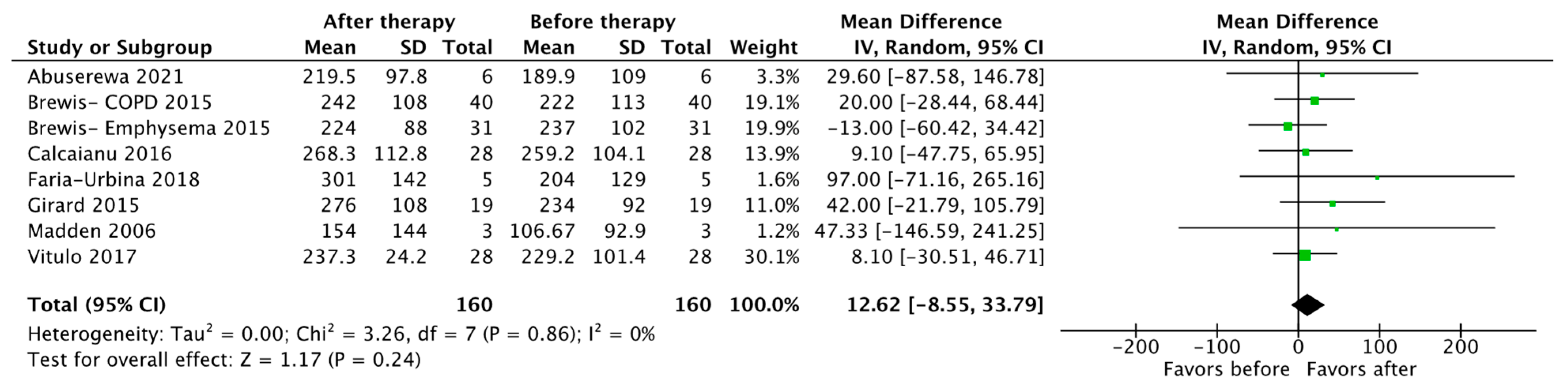
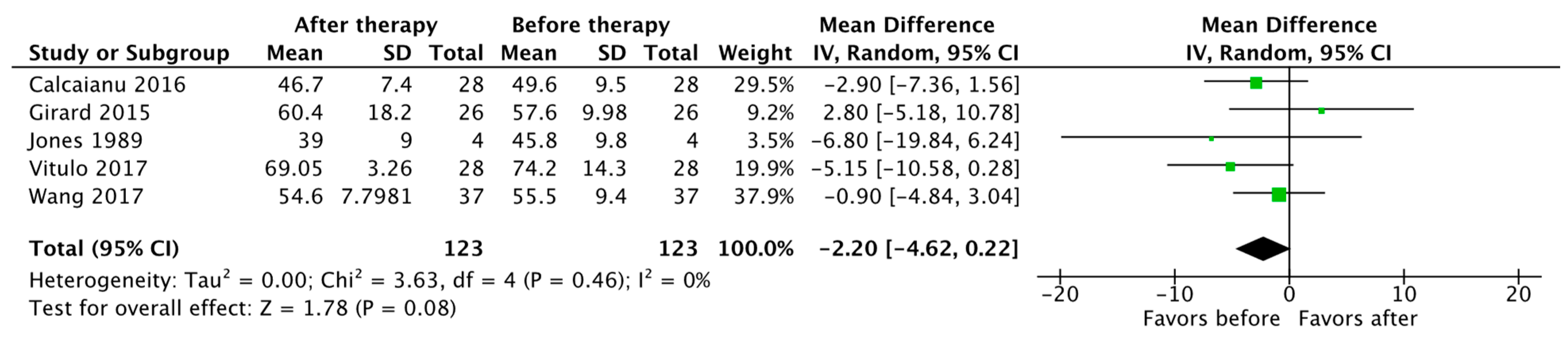
3.2. Hemodynamics
3.3. Exercise Capacity and Functional Status
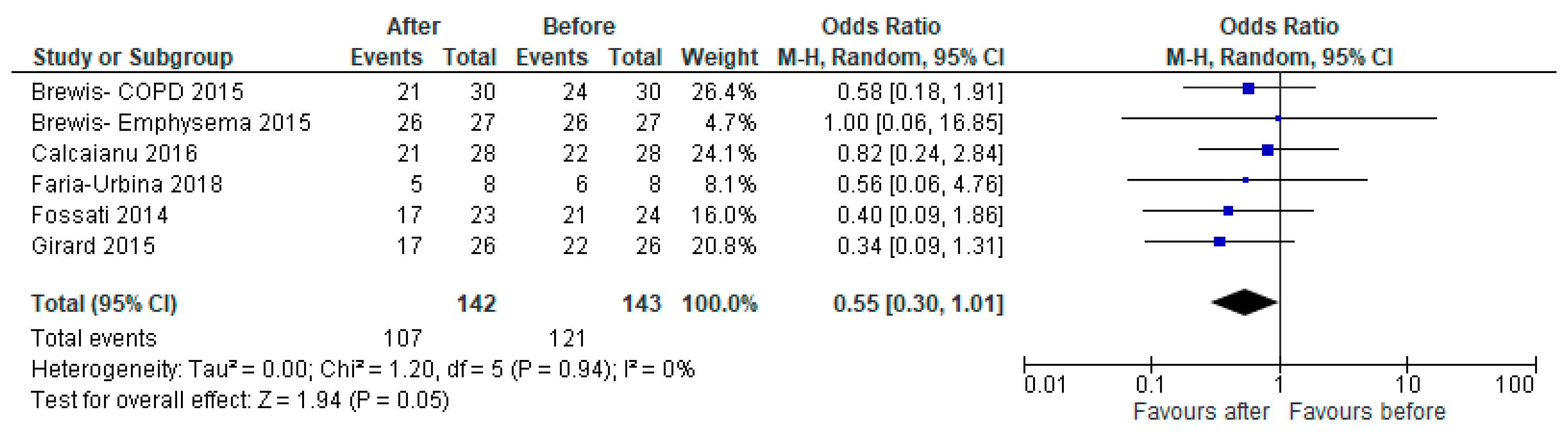
3.4. Survival and Secondary Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Vender, R.L. Chronic hypoxic pulmonary hypertension. Cell biology to pathophysiology. Chest 1994, 106, 236–243. [Google Scholar] [CrossRef] [PubMed]
- McQuillan, L.P.; Leung, G.K.; Marsden, P.A.; Kostyk, S.K.; Kourembanas, S. Hypoxia inhibits expression of eNOS via transcriptional and posttranscriptional mechanisms. Am. J. Physiol. 1994, 267 Pt 2, H1921–H1927. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, N.; McLoughlin, P. The structural basis of pulmonary hypertension in chronic lung disease: Remodelling, rarefaction or angiogenesis? J. Anat. 2002, 201, 335–348. [Google Scholar] [CrossRef]
- Campo, A.; Mathai, S.C.; Le Pavec, J.; Zaiman, A.L.; Hummers, L.K.; Boyce, D.; Housten, T.; Lechtzin, N.; Chami, H.; Girgis, R.E.; et al. Outcomes of hospitalisation for right heart failure in pulmonary arterial hypertension. Eur. Respir. J. 2011, 38, 359–367. [Google Scholar] [CrossRef]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef]
- Zeder, K.; Avian, A.; Bachmaier, G.; Douschan, P.; Foris, V.; Sassmann, T.; Troester, N.; Brcic, L.; Fuchsjaeger, M.; Marsh, L.M.; et al. Elevated pulmonary vascular resistance predicts mortality in COPD patients. Eur. Respir. J. 2021, 58, 2100944. [Google Scholar] [CrossRef]
- Olsson, K.M.; Hoeper, M.M.; Pausch, C.; Grünig, E.; Huscher, D.; Pittrow, D.; Rosenkranz, S.; Gall, H. Pulmonary vascular resistance predicts mortality in patients with pulmonary hypertension associated with interstitial lung disease: Results from the COMPERA registry. Eur. Respir. J. 2021, 58, 2101483. [Google Scholar] [CrossRef]
- Chaouat, A.; Bugnet, A.S.; Kadaoui, N.; Schott, R.; Enache, I.; Ducoloné, A.; Ehrhart, M.; Kessler, R.; Weitzenblum, E. Severe pulmonary hypertension and chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2005, 172, 189–194. [Google Scholar] [CrossRef]
- Cuttica, M.J.; Kalhan, R.; Shlobin, O.A.; Ahmad, S.; Gladwin, M.; Machado, R.F.; Barnett, S.D.; Nathan, S.D. Categorization and impact of pulmonary hypertension in patients with advanced COPD. Respir. Med. 2010, 104, 1877–1882. [Google Scholar] [CrossRef]
- Andersen, K.H.; Iversen, M.; Kjaergaard, J.; Mortensen, J.; Nielsen-Kudsk, J.E.; Bendstrup, E.; Videbaek, R.; Carlsen, J. Prevalence, predictors, and survival in pulmonary hypertension related to end-stage chronic obstructive pulmonary disease. J. Heart Lung Transpl. 2012, 31, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Piccari, L.; Wort, S.J.; Meloni, F.; Rizzo, M.; Price, L.C.; Martino, L.; Salvaterra, E.; Scelsi, L.; López Meseguer, M.; Blanco, I.; et al. The Effect of Borderline Pulmonary Hypertension on Survival in Chronic Lung Disease. Respiration 2022, 101, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Myronenko, O.; Foris, V.; Crnkovic, S.; Olschewski, A.; Rocha, S.; Nicolls, M.R.; Olschewski, H. Endotyping COPD: Hypoxia-inducible factor-2 as a molecular "switch" between the vascular and airway phenotypes? Eur. Respir. Rev. 2023, 32, 220173. [Google Scholar] [CrossRef] [PubMed]
- Waxman, A.; Restrepo-Jaramillo, R.; Thenappan, T.; Ravichandran, A.; Engel, P.; Bajwa, A.; Allen, R.; Feldman, J.; Argula, R.; Smith, P.; et al. Inhaled Treprostinil in Pulmonary Hypertension Due to Interstitial Lung Disease. N. Engl. J. Med. 2021, 384, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Ghofrani, H.A.; D’Armini, A.M.; Grimminger, F.; Hoeper, M.M.; Jansa, P.; Kim, N.H.; Mayer, E.; Simonneau, G.; Wilkins, M.R.; Fritsch, A.; et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension. N. Engl. J. Med. 2013, 369, 319–329. [Google Scholar] [CrossRef]
- Stolz, D.; Rasch, H.; Linka, A.; Di Valentino, M.; Meyer, A.; Brutsche, M.; Tamm, M. A randomised, controlled trial of bosentan in severe COPD. Eur. Respir. J. 2008, 32, 619–628. [Google Scholar] [CrossRef]
- Blanco, I.; Santos, S.; Gea, J.; Güell, R.; Torres, F.; Gimeno-Santos, E.; Rodriguez, D.A.; Vilaró, J.; Gómez, B.; Roca, J.; et al. Sildenafil to improve respiratory rehabilitation outcomes in COPD: A controlled trial. Eur. Respir. J. 2013, 42, 982–992. [Google Scholar] [CrossRef]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- Vitulo, P.; Stanziola, A.; Confalonieri, M.; Libertucci, D.; Oggionni, T.; Rottoli, P.; Paciocco, G.; Tuzzolino, F.; Martino, L.; Beretta, M.; et al. Sildenafil in severe pulmonary hypertension associated with chronic obstructive pulmonary disease: A randomized controlled multicenter clinical trial. J. Heart Lung Transpl. 2017, 36, 166–174. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2002. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 November 2023).
- Abuserewa, S.T.; Selim, A.; Youssef, A.; Zolty, R. Role of Selexipag in Chronic Obstructive Pulmonary Disease (COPD) Patients With Out-of-Proportion Pulmonary Hypertension. Cureus 2021, 13, e16520. [Google Scholar] [CrossRef] [PubMed]
- Brewis, M.J.; Church, A.C.; Johnson, M.K.; Peacock, A.J. Severe pulmonary hypertension in lung disease: Phenotypes and response to treatment. Eur. Respir. J. 2015, 46, 1378–1389. [Google Scholar] [CrossRef] [PubMed]
- Calcaianu, G.; Canuet, M.; Schuller, A.; Enache, I.; Chaouat, A.; Kessler, R. Pulmonary Arterial Hypertension-Specific Drug Therapy in COPD Patients with Severe Pulmonary Hypertension and Mild-to-Moderate Airflow Limitation. Respiration 2016, 91, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Faria-Urbina, M.; Oliveira, R.K.F.; Agarwal, M.; Waxman, A.B. Inhaled Treprostinil in Pulmonary Hypertension Associated with Lung Disease. Lung 2018, 196, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Fossati, L.; Müller-Mottet, S.; Hasler, E.; Speich, R.; Bloch, K.E.; Huber, L.C.; Ulrich Somaini, S. Long-term effect of vasodilator therapy in pulmonary hypertension due to COPD: A retrospective analysis. Lung 2014, 192, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Girard, A.; Jouneau, S.; Chabanne, C.; Khouatra, C.; Lannes, M.; Traclet, J.; Turquier, S.; Delaval, P.; Cordier, J.F.; Cottin, V. Severe pulmonary hypertension associated with COPD: Hemodynamic improvement with specific therapy. Respiration 2015, 90, 220–228. [Google Scholar] [CrossRef]
- Hurdman, J.; Condliffe, R.; Elliot, C.A.; Swift, A.; Rajaram, S.; Davies, C.; Hill, C.; Hamilton, N.; Armstrong, I.J.; Billings, C.; et al. Pulmonary hypertension in COPD: Results from the ASPIRE registry. Eur. Respir. J. 2013, 41, 1292–1301. [Google Scholar] [CrossRef]
- Jones, K.; Higenbottam, T.; Wallwork, J. Pulmonary vasodilation with prostacyclin in primary and secondary pulmonary hypertension. Chest 1989, 96, 784–789. [Google Scholar] [CrossRef]
- Lange, T.J.; Baron, M.; Seiler, I.; Arzt, M.; Pfeifer, M. Outcome of Patients with Severe PH due to Lung Disease with and without Targeted Therapy. Cardiovasc. Ther. 2014, 32, 202–208. [Google Scholar] [CrossRef]
- Madden, B.P.; Allenby, M.; Loke, T.K.; Sheth, A. A potential role for sildenafil in the management of pulmonary hypertension in patients with parenchymal lung disease. Vasc. Pharmacol. 2006, 44, 372–376. [Google Scholar] [CrossRef]
- Tanabe, N.; Taniguchi, H.; Tsujino, I.; Sakamaki, F.; Emoto, N.; Kimura, H.; Takamura, K.; Hanaoka, M.; Nishimura, M.; Tatsumi, K. Multi-institutional retrospective cohort study of patients with severe pulmonary hypertension associated with respiratory diseases. Respirology 2015, 20, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Jin, Y.-Z.; Zhao, Q.-H.; Jiang, R.; Wu, W.-H.; Gong, S.-G.; He, J.; Liu, J.-M.; Jing, Z.-C. Hemodynamic and gas exchange effects of inhaled iloprost in patients with COPD and pulmonary hypertension. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 3353–3360. [Google Scholar] [CrossRef]
- Blanco, I.; Gimeno, E.; Munoz, P.A.; Pizarro, S.; Gistau, C.; Rodriguez-Roisin, R.; Roca, J.; Barbera, J.A. Hemodynamic and gas exchange effects of sildenafil in patients with chronic obstructive pulmonary disease and pulmonary hypertension. Am. J. Respir. Crit. Care Med. 2010, 181, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Rao, R.S.; Singh, S.; Sharma, B.B.; Agarwal, V.V.; Singh, V. Sildenafil improves six-minute walk distance in chronic obstructive pulmonary disease: A randomised, double-blind, placebo-controlled trial. Indian. J. Chest Dis. Allied Sci. 2011, 53, 81–85. [Google Scholar] [PubMed]
- Goudie, A.R.; Lipworth, B.J.; Hopkinson, P.J.; Wei, L.; Struthers, A.D. Tadalafil in patients with chronic obstructive pulmonary disease: A randomised, double-blind, parallel-group, placebo-controlled trial. Lancet. Respir. Med. 2014, 2, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Vizza, C.D.; Hoeper, M.M.; Huscher, D.; Pittrow, D.; Benjamin, N.; Olsson, K.M.; Ghofrani, H.A.; Held, M.; Klose, H.; Lange, T.; et al. Pulmonary Hypertension in Patients with COPD: Results From the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA). Chest 2021, 160, 678–689. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, G.; Agusti, A.; Barberà, J.A.; Celli, B.; Criner, G.; Humbert, M.; Sin, D.D.; Voelkel, N.; Olschewski, H. Pulmonary Vascular Involvement in Chronic Obstructive Pulmonary Disease. Is There a Pulmonary Vascular Phenotype? Am. J. Respir. Crit. Care Med. 2018, 198, 1000–1011. [Google Scholar] [CrossRef]
- Nathan, S.D.; Barbera, J.A.; Gaine, S.P.; Harari, S.; Martinez, F.J.; Olschewski, H.; Olsson, K.M.; Peacock, A.J.; Pepke-Zaba, J.; Provencher, S.; et al. Pulmonary hypertension in chronic lung disease and hypoxia. Eur. Respir. J. 2019, 53, 1801914. [Google Scholar] [CrossRef]
- Blanco, I.; Tura-Ceide, O.; Peinado, V.I.; Barbera, J.A. Updated Perspectives on Pulmonary Hypertension in COPD. Int. J. Chron. Obs. Pulmon Dis. 2020, 15, 1315–1324. [Google Scholar] [CrossRef]
- Carlsen, J.; Hasseriis Andersen, K.; Boesgaard, S.; Iversen, M.; Steinbruchel, D.; Bogelund Andersen, C. Pulmonary arterial lesions in explanted lungs after transplantation correlate with severity of pulmonary hypertension in chronic obstructive pulmonary disease. J. Heart Lung Transpl. 2013, 32, 347–354. [Google Scholar] [CrossRef]
- El-Mahdy, M.A.; Abdelghany, T.M.; Hemann, C.; Ewees, M.G.; Mahgoup, E.M.; Eid, M.S.; Shalaan, M.T.; Alzarie, Y.A.; Zweier, J.L. Chronic cigarette smoke exposure triggers a vicious cycle of leukocyte and endothelial-mediated oxidant stress that results in vascular dysfunction. Am. J. Physiol. Heart Circ. Physiol. 2020, 319, H51–H65. [Google Scholar] [CrossRef] [PubMed]
- Pistenmaa, C.L.; Nardelli, P.; Ash, S.Y.; Come, C.E.; Diaz, A.A.; Rahaghi, F.N.; Barr, R.G.; Young, K.A.; Kinney, G.L.; Simmons, J.P.; et al. Pulmonary Arterial Pruning and Longitudinal Change in Percent Emphysema and Lung Function: The Genetic Epidemiology of COPD Study. Chest 2021, 160, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Pullamsetti, S.S.; Mamazhakypov, A.; Weissmann, N.; Seeger, W.; Savai, R. Hypoxia-inducible factor signaling in pulmonary hypertension. J. Clin. Investig. 2020, 130, 5638–5651. [Google Scholar] [CrossRef] [PubMed]
- Shimoda, L.A.; Semenza, G.L. HIF and the lung: Role of hypoxia-inducible factors in pulmonary development and disease. Am. J. Respir. Crit. Care Med. 2011, 183, 152–156. [Google Scholar] [CrossRef]
- Dai, Z.; Zhu, M.M.; Peng, Y.; Machireddy, N.; Evans, C.E.; Machado, R.; Zhang, X.; Zhao, Y.Y. Therapeutic Targeting of Vascular Remodeling and Right Heart Failure in Pulmonary Arterial Hypertension with a HIF-2α Inhibitor. Am. J. Respir. Crit. Care Med. 2018, 198, 1423–1434. [Google Scholar] [CrossRef]
- Hu, C.J.; Poth, J.M.; Zhang, H.; Flockton, A.; Laux, A.; Kumar, S.; McKeon, B.; Mouradian, G.; Li, M.; Riddle, S.; et al. Suppression of HIF2 signalling attenuates the initiation of hypoxia-induced pulmonary hypertension. Eur. Respir. J. 2019, 54, 1900378. [Google Scholar] [CrossRef]
- Pasupneti, S.; Tian, W.; Tu, A.B.; Dahms, P.; Granucci, E.; Gandjeva, A.; Xiang, M.; Butcher, E.C.; Semenza, G.L.; Tuder, R.M.; et al. Endothelial HIF-2α as a Key Endogenous Mediator Preventing Emphysema. Am. J. Respir. Crit. Care Med. 2020, 202, 983–995. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NOS Criteria | Studies (Year) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abuserewa, 2021 [22] | Brewis, 2015 [23] | Calcaianu, 2016 [24] | Faria-Urbina, 2018 [25] | Fossati, 2014 [26] | Girard, 2015 [27] | Hurdman, 2013 [28] | Jones, 1989 [29] | Lange, 2014 [30] | Madden, 2006 [31] | Tanabe, 2015 [32] | Wang, 2017 [33] | |
| Representativeness of the exposed cohort | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ||
| Selection of the nonexposed cohort | NA | NA | NA | NA | NA | NA | NA | NA | ★ | NA | NA | NA |
| Ascertainment of exposure | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Demonstration that outcome of interest was not present at the start of the study | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Comparability of cohort on the basis of the design or analysis | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| Assessment of outcome | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Follow-up duration >3 months | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ||
| Adequacy of follow-up of cohorts | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ |
| Total (maximum of nine stars) | 5 | 6 | 5 | 6 | 6 | 6 | 6 | 5 | 7 | 6 | 6 | 5 |
| Study ID | Title | Country | Study Design | Population Description | Treated/Total (n/n) | PH Specific Therapy Used (n) | Outcomes Assessed |
|---|---|---|---|---|---|---|---|
| Abuserewa 2021 [22] | Role of Selexipag in Chronic Obstructive Pulmonary Disease (COPD) Patients With Out-of-Proportion Pulmonary Hypertension | United States | Cohort study | PH-COPD patients treated with selexipag for “out-of-proportion” PH (FEV1 > 50%) | 6 | Selexipag | Hemodynamics, 6MWD, Borg scale |
| Brewis 2015 [23] | Severe pulmonary hypertension in lung disease: phenotypes and response to treatment | UK | Cohort study | Severe PH-COPD who received a minimum of 3 months of PH-targeted therapy. | 71 | ERA (16), prostanoid (4), combination (1) | NYHA, 6MWD, NT-proBNP, survival |
| Calcaianu 2016 [24] | Pulmonary Arterial Hypertension-Specific Drug Therapy in COPD Patients with Severe Pulmonary Hypertension and Mild-to-Moderate Airflow Limitation | France | Cohort study | Severe PH-COPD who were treated with PH-specific therapy. | 28 | ERA (23), PDE5 (1), Combination (2), other (2) | Hemodynamics, survival, NYHA class, BNP |
| Faria-Urbina 2018 [25] | Inhaled Treprostinil in Pulmonary Hypertension Associated with Lung Disease | United States | Cohort study | Severe PH patients evaluated at tertiary PH center; 22/72 patients had Group 3 PH. | 8 | Treprostinil | WHO-FC, echocardiography, 6MWD, SpO2 |
| Fossati 2014 [26] | Long-term effect of vasodilator therapy in pulmonary hypertension due to COPD: a retrospective analysis | Switzerland | Cohort study | Retrospective review of patients seen at pulmonary hypertension clinic who had PH-COPD and received PH target therapy for at least 3 months. | 27 | Prostanoid (15), ERA (15), PDE5I (25) | Survival, NYHA, 6MWD, SpO2 |
| Girard 2015 [27] | Severe pulmonary hypertension associated with COPD: hemodynamic improvement with specific therapy | France | Cohort study | Retrospective review of patients seen at pulmonary hypertension referral center who had PH-COPD. | 26 | ERA (11), PDE5I (11), Mix (3) | 6MWD, NYHA, echocardiography, NT proBNP, SpO2 |
| Hurdman 2013 [28] | Pulmonary hypertension in COPD: Results from the ASPIRE registry | UK | Cohort study | Consecutive patients seen at pulmonary hypertension referral center and diagnosed with PH-COPD were included, subdivided by severity of PH. | 43/59 | PDE-5I (31), ERA (10), Prostanoid (2) | Hemodynamics, survival, 6MWD, WHO-FC |
| Jones 1989 [29] | Pulmonary vasodilation with prostacyclin in primary and secondary pulmonary hypertension | UK | Nonrandomized experimental study | Twenty-three patients with PH underwent vasodilation testing with prostacyclin. Five patients had PH-COPD. | 5 | Prostacyclin IV | Hemodynamics |
| Lange 2014 [30] | Outcome of Patients with Severe PH due to Lung Disease with and without Targeted Therapy | Germany | Cohort study | Consecutive patients with a new diagnosis of Group 3 PH (retrospectively from a database and prospectively from a single center); 29/72 patients had PH-COPD, and 12 patients had severe PH-COPD. | 12 | Various, not reported | Hemodynamics, survival, 6MWD |
| Madden, 2006 [31] | A potential role for sildenafil in the management of pulmonary hypertension in patients with parenchymal lung disease | UK | Cohort study | Consecutive patients seen for Group 3 pulmonary hypertension at the referral center and treated with sildenafil; 4/7 patients had PH-COPD. | 3 | Sildenafil | Hemodynamics, 6MWD |
| Tanabe, 2015 [32] | Multi-institutional retrospective cohort study of patients with severe pulmonary hypertension associated with respiratory diseases | Japan | Cohort study | Patients with Group 3 severe PH; 18/70 patients had PH-COPD. | 14/18 | Beraprost (7), ERA (9), PDE5I (15) | Hemodynamics, survival |
| Vitulo, 2017 [19] | Sildenafil in severe pulmonary hypertension associated with chronic obstructive pulmonary disease: A randomized controlled multicenter clinical trial | Italy | Randomized controlled trial | Patients with COPD were screened for PH. Patients in whom PH was significantly out of proportion relative to COPD severity were included in the trial. | 28 | Sildenafil | Hemodynamics, BODE, 6MWD, QOL. PaO2 |
| Wang, 2017 [33] | Hemodynamic and gas exchange effects of inhaled iloprost in patients with COPD and pulmonary hypertension | Australia | Nonrandomized experimental study | The efficacy and safety of iloprost inhalation were assessed in patients with COPD and PH; 37/67 patients had severe PH. | 37 | Iloprost | Hemodynamics, gas exchange parameters |
| Number of PH-COPD Patients (Treated Only) | Death + Transplant at End of Follow Up | Transplant-Free Survival at 1 Year | Transplant-Free Survival at 2 Years | Transplant-Free Survival at 3 Years | |
|---|---|---|---|---|---|
| Brewis Emphysema 2015 [23] | 31 | 23 | 74% | NA | 32% |
| Brewis COPD 2015 [23] | 40 | 24 | 82% | NA | 50% |
| Calcaianu 2016 [24] | 28 | 12 | 84% | 63% | 45% |
| Fossati 2014 [26] | 27 | 12 | 92% | 69% | 54% |
| Hurdman 2013 [28] | 43 | Not reported | 72% | 38% | 30% |
| Tanabe 2015 [32] | 14 | Not reported | Not reported | Not reported | 37.5% |
| Total | 183 | NA | 81% | 57% | 41% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elkhapery, A.; Hammami, M.B.; Sulica, R.; Boppana, H.; Abdalla, Z.; Iyer, C.; Taifour, H.; Niu, C.; Deshwal, H. Pulmonary Vasodilator Therapy in Severe Pulmonary Hypertension Due to Chronic Obstructive Pulmonary Disease (Severe PH-COPD): A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2023, 10, 498. https://doi.org/10.3390/jcdd10120498
Elkhapery A, Hammami MB, Sulica R, Boppana H, Abdalla Z, Iyer C, Taifour H, Niu C, Deshwal H. Pulmonary Vasodilator Therapy in Severe Pulmonary Hypertension Due to Chronic Obstructive Pulmonary Disease (Severe PH-COPD): A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2023; 10(12):498. https://doi.org/10.3390/jcdd10120498
Chicago/Turabian StyleElkhapery, Ahmed, M. Bakri Hammami, Roxana Sulica, Hemanth Boppana, Zeinab Abdalla, Charoo Iyer, Hazem Taifour, Chengu Niu, and Himanshu Deshwal. 2023. "Pulmonary Vasodilator Therapy in Severe Pulmonary Hypertension Due to Chronic Obstructive Pulmonary Disease (Severe PH-COPD): A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 10, no. 12: 498. https://doi.org/10.3390/jcdd10120498
APA StyleElkhapery, A., Hammami, M. B., Sulica, R., Boppana, H., Abdalla, Z., Iyer, C., Taifour, H., Niu, C., & Deshwal, H. (2023). Pulmonary Vasodilator Therapy in Severe Pulmonary Hypertension Due to Chronic Obstructive Pulmonary Disease (Severe PH-COPD): A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease, 10(12), 498. https://doi.org/10.3390/jcdd10120498