
Exercise-Induced Blood Pressure Dynamics: Insights from the General Population and the Athletic Cohort

 , ,
, , {kind=link}
{kind=link}
Abstract
1. Introduction
2. Blood Pressure Responses to Exercise
2.1. Historical Perspective on Exercise Blood Pressure Guidelines
2.2. Physiological Dynamics of Blood Pressure during Exercise
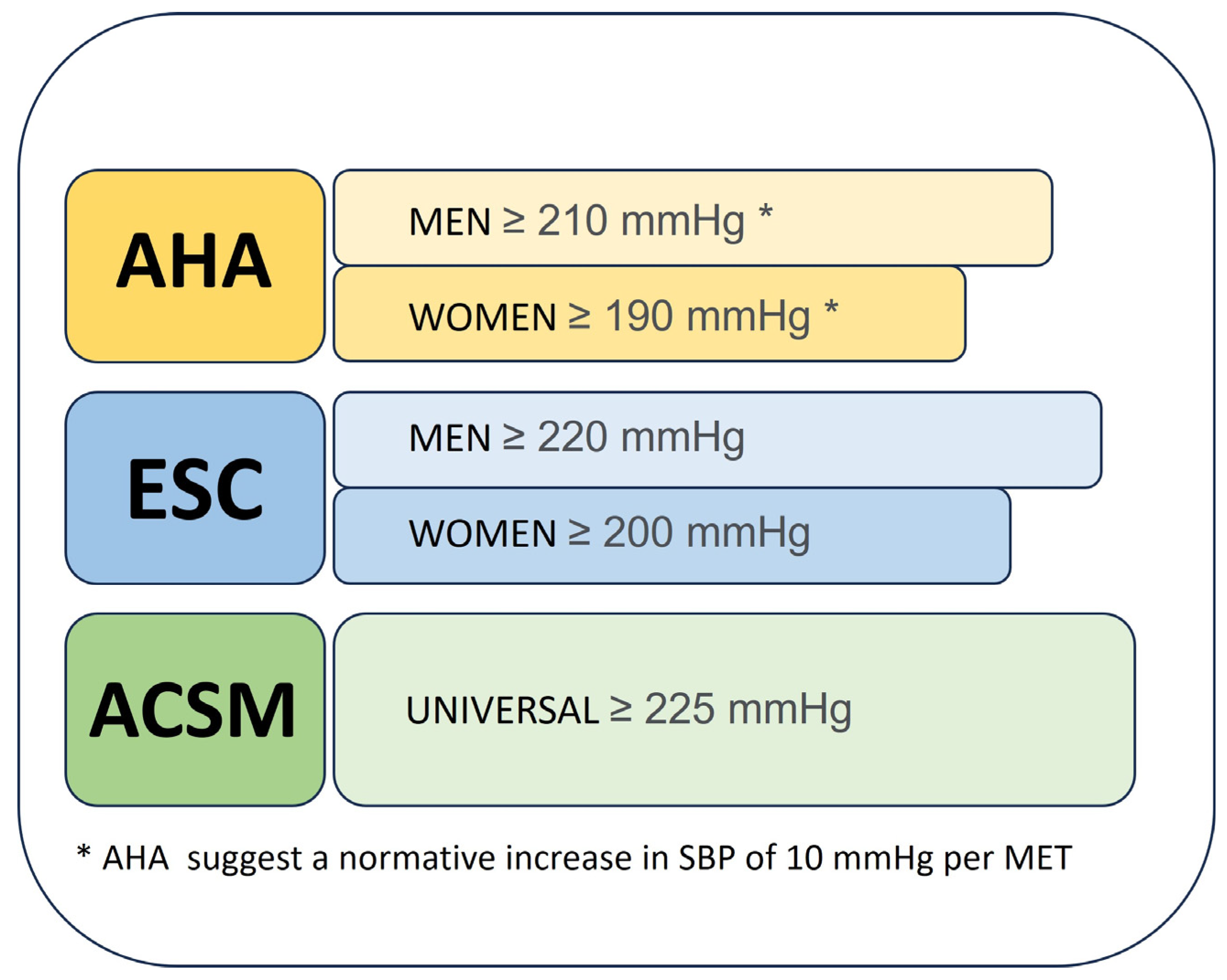
2.3. Different Guidelines for Defining an Exaggerated BP Response
- American Heart Association: The AHA defines a systolic blood pressure of 210 mmHg for men and 190 mmHg for women as potentially worrying during exercise, emphasising an approximate increase in SBP of 10 mmHg per MET [22].
- European Society of Cardiology (ESC): The ESC has slightly higher thresholds, recommending 220 mmHg for men and 200 mmHg for women [23].
- American College of Sports Medicine (ACSM): Taking a different approach, the ACSM proposes a unisex threshold, setting a cut-off of 225 mmHg for both sexes [24].
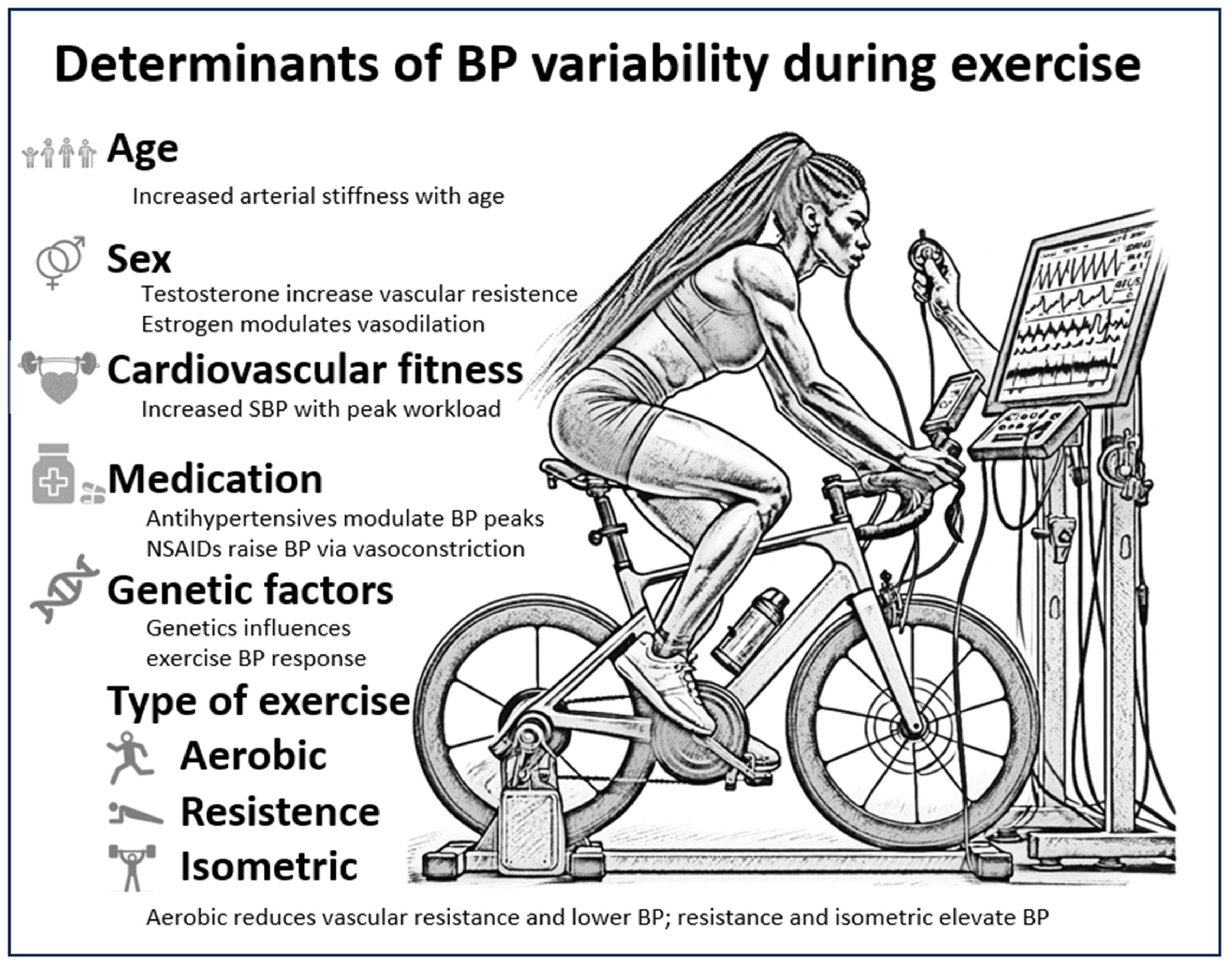
2.4. Determinants of BP Variability during Exercise
- Age and gender: Both age and sex have been found to be important determinants of BP dynamics during exercise. Tuka et al. [30] found that older individuals have an increased SBP response compared to their younger counterparts. This age-related increase in BP is a multifaceted phenomenon influenced by several factors. It is partly a consequence of reduced arterial wall elasticity, which may lead to increased resistance in the peripheral vasculature [31]. In addition, Trinity et al. [9] have shown that age-related changes in vascular function, such as increased arterial stiffness, contribute to the enhanced blood pressure responses observed during exercise. BP patterns in women, which are often different from those in men, may be due to hormonal variations and different vascular characteristics. For example, Smith et al. [32] noted that oestrogen is known to exert vasodilatory effects that may modulate BP responses in premenopausal women. Experimental research has further elucidated the complex interplay of various cardiovascular parameters during exercise in both sexes. These parameters include heart rate, stroke volume and vascular resistance [5,6]. In addition, Smith et al. [32] and Trinity et al. [9] have shown that the exercise pressure reflex, the body’s own mechanism for regulating blood pressure during physical activity, works differently in men and women.
- Medication and medical conditions: Medication, particularly antihypertensive drugs such as beta-blockers, can significantly modulate BP dynamics during exercise, as observed by Chick, T.W. et al. [16]. It is important to note that according to Chant, B. et al. [34], despite control of baseline blood pressure, antihypertensive medication does not protect against exaggerated increases in blood pressure during peak exercise testing.
- Genetic factors: Genetics, an often-overlooked determinant, may influence exercise-induced BP responses. Certain genetic markers or hereditary predispositions may increase or decrease blood pressure variability during exercise. Studies by Rankinen, T. et al. [35], Rankinen, T. et al. [36] and Montasser, M.E. et al. [37] have all addressed this area. Although not the focus of this review, recent research suggests a genetic basis for BP variability during exercise.
- Type of exercise: The type of exercise undoubtedly plays a crucial role in determining cardiovascular responses, particularly in terms of blood pressure dynamics.
- 1.
- Aerobic exercise (e.g., running, cycling):
- 2.
- Resistance training (e.g., weightlifting):
- 3.
- Isometric exercises (e.g., handgrip, plank):
2.5. The Importance of Submaximal versus Peak Blood Pressure
2.6. Prognostic Significance of BP Responses
2.7. Blood Pressure Dynamics in Athletes: A Special Consideration
- Athletes should be vigilant against unwarranted gains in adiposity, given its established association with hypertension [61].
- Furthermore, the increased SBP observed in endurance athletes is often associated with superior peak oxygen consumption (VO2max), increased work capacity and, occasionally, increased myocardial mass. The lack of evidence of adverse outcomes suggests that the elevated SBP in such athletes may be a manifestation of physiological adaptations to rigorous training rather than a pathological deviation [68,69].
- Bjarnason-Wehrens et al. [70] highlighted the nuances of exercise-induced arterial hypertension (EAH) in athletes. Their work highlighted the importance of considering various factors such as exercise intensity, duration and modality when assessing BP responses in athletes. They suggested that EAH may not always be a maladaptive response but rather an adaptive mechanism to meet the increased metabolic demands of strenuous physical activity.
- Furthermore, Hedman et al. [71] emphasised the role of the workload-indexed BP response in predicting mortality, highlighting the multifaceted nature of exercise-induced BP dynamics in athletes.
- Recent research in the field of cardiorespiratory fitness and its correlation with blood pressure dynamics introduces new parameters that may better differentiate between adaptive and maladaptive cardiovascular responses in athletes. For example, the study by Ligetvari et al. [72] sheds light on the complex interplay between apelin levels—a cardiokine/myokine—and peak exercise performance. The observed correlation between changes in plasma apelin-13 levels and key performance indicators such as maximal metabolic equivalent, relative maximal O2 consumption and peak aerobic performance suggests that, beyond traditional SBP measurements, a more comprehensive assessment including SBP/VO2 and SBP/W slopes, as well as aerobic performance and stroke work, may provide a more refined understanding of an athlete’s cardiovascular efficiency and adaptability. Such metrics could be invaluable in distinguishing the elevated SBP response during exercise as an adaptive mechanism associated with improved physical performance rather than a premature sign of cardiovascular stress or pathology. This nuanced perspective highlights the potential of integrating multifactorial assessments to cultivate a more accurate and athlete-centred model of cardiovascular health in sports medicine.
2.8. Looking Ahead: Navigating the Future Landscape of Exercise Blood Pressure Dynamics
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J. Exercise Standards for Testing and Training: A Scientific Statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef] [PubMed]
- Currie, K.D.; Floras, J.S.; La Gerche, A.; Goodman, J.M. Exercise Blood Pressure Guidelines: Time to Re-Evaluate What Is Normal and Exaggerated? Sports Med. 2018, 48, 1763–1771. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.M.; Naughton, J.P.; Haskell, W.L. Physical Activity and the Prevention of Coronary Heart Disease. Ann. Clin. Res. 1971, 3, 404–432. [Google Scholar] [CrossRef] [PubMed]
- Naughton, J.P.; Haider, R. Methods of Exercise Testing. In Exercise Testing and Exercise Training in Coronary Heart Disease; Academic Press: New York, NY, USA, 1973; pp. 79–95. [Google Scholar]
- Ekblom, B.; Astrand, P.O.; Saltin, B.; Stenberg, J.; Wallström, B. Effect of Training on Circulatory Response to Exercise. J. Appl. Physiol. 1968, 24, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Pollock, M.L.; Foster, C.; Schmidt, D.; Hellman, C.; Linnerud, A.C.; Ward, A. Comparative Analysis of Physiologic Responses to Three Different Maximal Graded Exercise Test Protocols in Healthy Women. Am. Heart J. 1982, 103, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Spina, R.J.; Martin, W.H.; Kohrt, W.M.; Schechtman, K.B.; Holloszy, J.O.; Ehsani, A.A. Effects of Aging, Sex, and Physical Training on Cardiovascular Responses to Exercise. Circulation 1992, 86, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Hedman, K.; Lindow, T.; Elmberg, V.; Brudin, L.; Ekström, M. Age- and Gender-Specific Upper Limits and Reference Equations for Workload-Indexed Systolic Blood Pressure Response during Bicycle Ergometry. Eur. J. Prev. Cardiol. 2021, 28, 1360–1369. [Google Scholar] [CrossRef]
- Trinity, J.D.; Layec, G.; Hart, C.R.; Richardson, R.S. Sex-Specific Impact of Aging on the Blood Pressure Response to Exercise. Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H95–H104. [Google Scholar] [CrossRef]
- Schultz, M.G.; Otahal, P.; Cleland, V.J.; Blizzard, L.; Marwick, T.H.; Sharman, J.E. Exercise-Induced Hypertension, Cardiovascular Events, and Mortality in Patients Undergoing Exercise Stress Testing: A Systematic Review and Meta-Analysis. Am. J. Hypertens. 2013, 26, 357–366. [Google Scholar] [CrossRef]
- Mohammed, L.M.; Dhavale, M.; Abdelaal, M.K.; Alam, A.B.M.N.; Blazin, T.; Prajapati, D.; Mostafa, J.A. Exercise-Induced Hypertension in Healthy Individuals and Athletes: Is It an Alarming Sign? Cureus 2020, 12, e11988. [Google Scholar] [CrossRef]
- Rowell, L.B. Human Cardiovascular Control; Oxford University Press: Oxford, UK, 1993; ISBN 978-0-19-507362-1. [Google Scholar]
- Nystoriak, M.A.; Bhatnagar, A. Cardiovascular Effects and Benefits of Exercise. Front. Cardiovasc. Med. 2018, 5, 135. [Google Scholar] [CrossRef] [PubMed]
- Everson, S.A.; Kaplan, G.A.; Goldberg, D.E.; Salonen, J.T. Anticipatory Blood Pressure Response to Exercise Predicts Future High Blood Pressure in Middle-Aged Men. Hypertension 1996, 27, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Carpio-Rivera, E.; Moncada-Jiménez, J.; Salazar-Rojas, W.; Solera-Herrera, A. Acute Effects of Exercise on Blood Pressure: A Meta-Analytic Investigation. Arq. Bras. Cardiol. 2016, 106, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.A.; Tran, Z.V. Aerobic Exercise and Resting Blood Pressure: A Meta-Analytic Review of Randomized, Controlled Trials. Prev. Cardiol. 2001, 4, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Charkoudian, N.; Rabbitts, J.A. Sympathetic Neural Mechanisms in Human Cardiovascular Health and Disease. Mayo Clin. Proc. 2009, 84, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Charkoudian, N.; Wallin, B.G. The Sympathetic Nervous System and Blood Pressure in Humans: Individualized Patterns of Regulation and Their Implications. Hypertension 2010, 56, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Jia, G.; Aroor, A.R.; Hill, M.A.; Sowers, J.R. Role of Renin-Angiotensin-Aldosterone System Activation in Promoting Cardiovascular Fibrosis and Stiffness. Hypertension 2018, 72, 537–548. [Google Scholar] [CrossRef]
- Goessler, K.; Polito, M.; Cornelissen, V.A. Effect of Exercise Training on the Renin–Angiotensin–Aldosterone System in Healthy Individuals: A Systematic Review and Meta-Analysis. Hypertens. Res. 2016, 39, 119–126. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Franklin, B.A.; Fagard, R.; Farquhar, W.B.; Kelley, G.A.; Ray, C.A.; American College of Sports Medicine American College of Sports Medicine Position Stand. Exercise and Hypertension. Med. Sci. Sports Exerc. 2004, 36, 533–553. [Google Scholar] [CrossRef]
- Gibbons, R.J.; Balady, G.J.; Bricker, J.T.; Chaitman, B.R.; Fletcher, G.F.; Froelicher, V.F.; Mark, D.B.; McCallister, B.D.; Mooss, A.N.; O’Reilly, M.G.; et al. ACC/AHA 2002 Guideline Update for Exercise Testing: Summary Article. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). J. Am. Coll. Cardiol. 2002, 40, 1531–1540. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Hunter, S.K.; Angadi, S.; Bhargava, A.; Harper, J.; Hirschberg, A.L.; Levine, B.D.; Moreau, K.L.; Nokoff, N.J.; Stachenfeld, N.S.; Bermon, S. The Biological Basis of Sex Differences in Athletic Performance: Consensus Statement for the American College of Sports Medicine. Med. Sci. Sports Exerc. 2023, 55, 2328–2360. [Google Scholar] [CrossRef]
- Sabbahi, A.; Arena, R.; Kaminsky, L.A.; Myers, J.; Phillips, S.A. Peak Blood Pressure Responses During Maximum Cardiopulmonary Exercise Testing. Hypertension 2018, 71, 229–236. [Google Scholar] [CrossRef]
- Keller, K.; Hartung, K.; del Castillo Carillo, L.; Treiber, J.; Stock, F.; Schröder, C.; Hugenschmidt, F.; Friedmann-Bette, B. Exercise Hypertension in Athletes. J. Clin. Med. 2022, 11, 4870. [Google Scholar] [CrossRef] [PubMed]
- Schultz, M.G.; Sharman, J.E. Exercise Hypertension. Pulse 2014, 1, 161–176. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.; Min, S.; Villa, C.; Weintraub, R.G.; Nakano, S.; Godown, J.; Tatangelo, M.; Armstrong, K.; Richmond, M.; Kaufman, B.; et al. The Prevalence and Association of Exercise Test Abnormalities With Sudden Cardiac Death and Transplant-Free Survival in Childhood Hypertrophic Cardiomyopathy. Circulation 2023, 147, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Benbassat, J.; Froom, P. Blood Pressure Response to Exercise as a Predictor of Hypertension. Arch. Intern. Med. 1986, 146, 2053–2055. [Google Scholar] [CrossRef] [PubMed]
- Tuka, V.; Rosa, J.; Dědinová, M.; Matoulek, M. The Determinants of Blood Pressure Response to Exercise. Cor. Vasa 2015, 57, e163–e167. [Google Scholar] [CrossRef]
- Joyner, M.J.; Casey, D.P. Regulation of Increased Blood Flow (Hyperemia) to Muscles during Exercise: A Hierarchy of Competing Physiological Needs. Physiol. Rev. 2015, 95, 549–601. [Google Scholar] [CrossRef]
- Smith, J.R.; Koepp, K.E.; Berg, J.D.; Akinsanya, J.G.; Olson, T.P. Influence of Sex, Menstrual Cycle, and Menopause Status on the Exercise Pressor Reflex. Med. Sci. Sports Exerc. 2019, 51, 874–881. [Google Scholar] [CrossRef]
- Miyai, N.; Arita, M.; Miyashita, K.; Morioka, I.; Shiraishi, T.; Nishio, I. Blood Pressure Response to Heart Rate During Exercise Test and Risk of Future Hypertension. Hypertension 2002, 39, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Chant, B.; Bakali, M.; Hinton, T.; Burchell, A.E.; Nightingale, A.K.; Paton, J.F.R.; Hart, E.C. Antihypertensive Treatment Fails to Control Blood Pressure During Exercise. Hypertension 2018, 72, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Rankinen, T.; An, P.; Rice, T.; Sun, G.; Chagnon, Y.C.; Gagnon, J.; Leon, A.S.; Skinner, J.S.; Wilmore, J.H.; Rao, D.C.; et al. Genomic Scan for Exercise Blood Pressure in the Health, Risk Factors, Exercise Training and Genetics (HERITAGE) Family Study. Hypertension 2001, 38, 30–37. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rankinen, T.; Bouchard, C. Genetics and Blood Pressure Response to Exercise, and Its Interactions with Adiposity. Prev. Cardiol. 2002, 5, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Montasser, M.E.; Gu, D.; Chen, J.; Shimmin, L.C.; Gu, C.; Kelly, T.N.; Jaquish, C.E.; Rice, T.; Rao, D.C.; Cao, J.; et al. Interactions of Genetic Variants with Physical Activity Are Associated with Blood Pressure in Chinese: The GenSalt Study. Am. J. Hypertens. 2011, 24, 1035–1040. [Google Scholar] [CrossRef]
- MacDougall, J.D.; Tuxen, D.; Sale, D.G.; Moroz, J.R.; Sutton, J.R. Arterial Blood Pressure Response to Heavy Resistance Exercise. J. Appl. Physiol. 1985, 58, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Millar, P.J.; Levy, A.S.; McGowan, C.L.; McCartney, N.; MacDonald, M.J. Isometric Handgrip Training Lowers Blood Pressure and Increases Heart Rate Complexity in Medicated Hypertensive Patients. Scand. J. Med. Sci. Sports 2013, 23, 620–626. [Google Scholar] [CrossRef]
- Canivel, R.G.; Wyatt, F.B.; Baker, J.S. Cardiovascular Responses to Isometric Hand Grip vs. Relaxed Hand Grip in Sustained Cycling Efforts. J. Strength. Cond. Res. 2012, 26, 3101–3105. [Google Scholar] [CrossRef]
- Edwards, J.J.; Deenmamode, A.H.P.; Griffiths, M.; Arnold, O.; Cooper, N.J.; Wiles, J.D.; O’Driscoll, J.M. Exercise Training and Resting Blood Pressure: A Large-Scale Pairwise and Network Meta-Analysis of Randomised Controlled Trials. Br. J. Sports Med. 2023, 57, 1317–1326. [Google Scholar] [CrossRef]
- Schultz, M.G.; Otahal, P.; Picone, D.S.; Sharman, J.E. Clinical Relevance of Exaggerated Exercise Blood Pressure. J. Am. Coll. Cardiol. 2015, 66, 1843–1845. [Google Scholar] [CrossRef]
- Schultz, M.G.; Currie, K.D.; Hedman, K.; Climie, R.E.; Maiorana, A.; Coombes, J.S.; Sharman, J.E. The Identification and Management of High Blood Pressure Using Exercise Blood Pressure: Current Evidence and Practical Guidance. Int. J. Environ. Res. Public Health 2022, 19, 2819. [Google Scholar] [CrossRef] [PubMed]
- Dutra-Marques, A.C.; Rodrigues, S.; Cepeda, F.X.; Toschi-Dias, E.; Rondon, E.; Carvalho, J.C.; Alves, M.J.N.N.; Braga, A.M.F.W.; Rondon, M.U.P.B.; Trombetta, I.C. Exaggerated Exercise Blood Pressure as a Marker of Baroreflex Dysfunction in Normotensive Metabolic Syndrome Patients. Front. Neurosci. 2021, 15, 680195. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.E.; LaGerche, A. Exercise Blood Pressure: Clinical Relevance and Correct Measurement. J. Hum. Hypertens. 2015, 29, 351–358. [Google Scholar] [CrossRef]
- Wielemborek-Musial, K.; Szmigielska, K.; Leszczynska, J.; Jegier, A. Blood Pressure Response to Submaximal Exercise Test in Adults. Biomed. Res. Int. 2016, 2016, 5607507. [Google Scholar] [CrossRef] [PubMed]
- Sarma, S.; Howden, E.; Carrick-Ranson, G.; Lawley, J.; Hearon, C.; Samels, M.; Everding, B.; Livingston, S.; Adams-Huet, B.; Palmer, M.D.; et al. Elevated Exercise Blood Pressure in Middle-Aged Women Is Associated with Altered Left Ventricular and Vascular Stiffness. J. Appl. Physiol. 2020, 128, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A.; Nishimura, R.A.; Sorajja, P.; Lam, C.S.P.; Redfield, M.M. Exercise Hemodynamics Enhance Diagnosis of Early Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2010, 3, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Mariampillai, J.E.; Liestøl, K.; Kjeldsen, S.E.; Prestgaard, E.E.; Engeseth, K.; Bodegard, J.; Berge, E.; Gjesdal, K.; Erikssen, J.; Grundvold, I.; et al. Exercise Systolic Blood Pressure at Moderate Workload Is Linearly Associated With Coronary Disease Risk in Healthy Men. Hypertension 2020, 75, 44–50. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- Matthews, C.E.; Pate, R.R.; Jackson, K.L.; Ward, D.S.; Macera, C.A.; Kohl, H.W.; Blair, S.N. Exaggerated Blood Pressure Response to Dynamic Exercise and Risk of Future Hypertension. J. Clin. Epidemiol. 1998, 51, 29–35. [Google Scholar] [CrossRef]
- Keller, K.; Stelzer, K.; Ostad, M.A.; Post, F. Impact of Exaggerated Blood Pressure Response in Normotensive Individuals on Future Hypertension and Prognosis: Systematic Review According to PRISMA Guideline. Adv. Med. Sci. 2017, 62, 317–329. [Google Scholar] [CrossRef]
- Jae, S.Y.; Kurl, S.; Kunutsor, S.K.; Franklin, B.A.; Laukkanen, J.A. Relation of Maximal Systolic Blood Pressure during Exercise Testing to the Risk of Sudden Cardiac Death in Men with and without Cardiovascular Disease. Eur. J. Prev. Cardiol. 2020, 27, 2220–2222. [Google Scholar] [CrossRef] [PubMed]
- Tahir, E.; Starekova, J.; Muellerleile, K.; von Stritzky, A.; Münch, J.; Avanesov, M.; Weinrich, J.M.; Stehning, C.; Bohnen, S.; Radunski, U.K.; et al. Myocardial Fibrosis in Competitive Triathletes Detected by Contrast-Enhanced CMR Correlates With Exercise-Induced Hypertension and Competition History. JACC Cardiovasc. Imaging 2018, 11, 1260–1270. [Google Scholar] [CrossRef] [PubMed]
- Aker, A.; Saliba, W.; Hislop, E.; Zafrir, B. Blood Pressure Measurements during Treadmill Exercise Testing and the Risk for the Future Development of Atrial Fibrillation. Hypertens. Res. 2022, 45, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Schultz, M.G.; La Gerche, A.; Sharman, J.E. Blood Pressure Response to Exercise and Cardiovascular Disease. Curr. Hypertens. Rep. 2017, 19, 89. [Google Scholar] [CrossRef] [PubMed]
- Caselli, S.; Serdoz, A.; Mango, F.; Lemme, E.; Vaquer Seguì, A.; Milan, A.; Attenhofer Jost, C.; Schmied, C.; Spataro, A.; Pelliccia, A. High Blood Pressure Response to Exercise Predicts Future Development of Hypertension in Young Athletes. Eur. Heart J. 2019, 40, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Caselli, S.; Vaquer Segui, A.; Quattrini, F.; Di Gacinto, B.; Milan, A.; Assorgi, R.; Verdile, L.; Spataro, A.; Pelliccia, A. Upper Normal Values of Blood Pressure Response to Exercise in Olympic Athletes. Am. Heart J. 2016, 177, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Richard, N.A.; Hodges, L.; Koehle, M.S. Elevated Peak Systolic Blood Pressure in Endurance-Trained Athletes: Physiology or Pathology? Scand. J. Med. Sci. Sports 2021, 31, 956–966. [Google Scholar] [CrossRef]
- Pressler, A.; Jähnig, A.; Halle, M.; Haller, B. Blood Pressure Response to Maximal Dynamic Exercise Testing in an Athletic Population. J. Hypertens. 2018, 36, 1803–1809. [Google Scholar] [CrossRef]
- Kim, J.H.; Hollowed, C.; Liu, C.; Al-Badri, A.; Alkhoder, A.; Dommisse, M.; Gowani, Z.; Miller, A.; Nguyen, P.; Prabakaran, G.; et al. Weight Gain, Hypertension, and the Emergence of a Maladaptive Cardiovascular Phenotype Among US Football Players. JAMA Cardiol. 2019, 4, 1221–1229. [Google Scholar] [CrossRef]
- Jiravska Godula, B.; Jiravsky, O.; Pesova, P.; Jelinek, L.; Sovova, M.; Moravcova, K.; Ozana, J.; Hudec, M.; Miklik, R.; Hecko, J.; et al. Preparticipation Screening of Athletes: The Prevalence of Positive Family History. J. Cardiovasc. Dev. Dis. 2023, 10, 183. [Google Scholar] [CrossRef]
- Schweiger, V.; Niederseer, D.; Schmied, C.; Attenhofer-Jost, C.; Caselli, S. Athletes and Hypertension. Curr. Cardiol. Rep. 2021, 23, 176. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.-Y.; Park, J.-I.; Park, S.K.; Barrett-Connor, E. Utility of Graded Exercise Tolerance Tests for Prediction of Cardiovascular Mortality in Old Age: The Rancho Bernardo Study. Int. J. Cardiol. 2015, 181, 323–327. [Google Scholar] [CrossRef] [PubMed][Green Version]
- O’Connor, F.G.; Deuster, P.A.; Davis, J.; Pappas, C.G.; Knapik, J.J. Functional Movement Screening: Predicting Injuries in Officer Candidates. Med. Sci. Sports Exerc. 2011, 43, 2224–2230. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Chun, H.; Kim, C.-H. Exaggerated Response of Systolic Blood Pressure to Cycle Ergometer. Ann. Rehabil. Med. 2013, 37, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Brubaker, P.H. Exercise Testing. In Encyclopedia of Exercise Medicine in Health and Disease; Mooren, F.C., Ed.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 318–323. ISBN 978-3-540-29807-6. [Google Scholar]
- Carlén, A.; Eklund, G.; Andersson, A.; Carlhäll, C.-J.; Ekström, M.; Hedman, K. Systolic Blood Pressure Response to Exercise in Endurance Athletes in Relation to Oxygen Uptake, Work Rate and Normative Values. J. Cardiovasc. Dev. Dis. 2022, 9, 227. [Google Scholar] [CrossRef] [PubMed]
- Burtscher, J.; Strasser, B.; Burtscher, M.; Millet, G.P. The Impact of Training on the Loss of Cardiorespiratory Fitness in Aging Masters Endurance Athletes. Int. J. Environ. Res. Public. Health 2022, 19, 11050. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason-Wehrens, B.; Predel, H.-G. Rays of Light into the “black-Box” of Exercise Hypertension. Eur. J. Prev. Cardiol. 2022, 28, e7–e9. [Google Scholar] [CrossRef] [PubMed]
- Hedman, K.; Cauwenberghs, N.; Christle, J.W.; Kuznetsova, T.; Haddad, F.; Myers, J. Workload-Indexed Blood Pressure Response Is Superior to Peak Systolic Blood Pressure in Predicting All-Cause Mortality. Eur. J. Prev. Cardiol. 2020, 27, 978–987. [Google Scholar] [CrossRef]
- Ligetvári, R.; Szokodi, I.; Far, G.; Csöndör, É.; Móra, Á.; Komka, Z.; Tóth, M.; Oláh, A.; Ács, P. Apelin as a Potential Regulator of Peak Athletic Performance. Int. J. Mol. Sci. 2023, 24, 8195. [Google Scholar] [CrossRef]
- Aengevaeren, V.L.; Hopman, M.T.E.; Thompson, P.D.; Bakker, E.A.; George, K.P.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Exercise-Induced Cardiac Troponin I Increase and Incident Mortality and Cardiovascular Events. Circulation 2019, 140, 804–814. [Google Scholar] [CrossRef]
- Omland, T.; Aakre, K.M. Cardiac Troponin Increase After Endurance Exercise. Circulation 2019, 140, 815–818. [Google Scholar] [CrossRef] [PubMed]
- Airaksinen, K.E.J. Cardiac Troponin Release After Endurance Exercise: Still Much to Learn. J. Am. Heart Assoc. 2020, 9, e015912. [Google Scholar] [CrossRef] [PubMed]
- Aengevaeren, V.L.; Baggish, A.L.; Chung, E.H.; George, K.; Kleiven, Ø.; Mingels, A.M.A.; Ørn, S.; Shave, R.E.; Thompson, P.D.; Eijsvogels, T.M.H. Exercise-Induced Cardiac Troponin Elevations: From Underlying Mechanisms to Clinical Relevance. Circulation 2021, 144, 1955–1972. [Google Scholar] [CrossRef] [PubMed]
- Janssen, S.L.; Berge, K.; Luiken, T.; Aengevaeren, V.L.; Eijsvogels, T.M. Cardiac Troponin Release in Athletes: What Do We Know and Where Should We Go? Curr. Opin. Physiol. 2023, 31, 100629. [Google Scholar] [CrossRef]
- Legaz-Arrese, A.; López-Laval, I.; George, K.; Puente-Lanzarote, J.J.; Mayolas-Pi, C.; Serrano-Ostáriz, E.; Revilla-Martí, P.; Moliner-Urdiales, D.; Reverter-Masià, J. Impact of an Endurance Training Program on Exercise-Induced Cardiac Biomarker Release. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H913–H920. [Google Scholar] [CrossRef]
- Skadberg, Ø.; Kleiven, Ø.; Ørn, S.; Bjørkavoll-Bergseth, M.F.; Melberg, T.H.; Omland, T.; Aakre, K.M. The Cardiac Troponin Response Following Physical Exercise in Relation to Biomarker Criteria for Acute Myocardial Infarction; the North Sea Race Endurance Exercise Study (NEEDED) 2013. Clin. Chim. Acta 2018, 479, 155–159. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pesova, P.; Jiravska Godula, B.; Jiravsky, O.; Jelinek, L.; Sovova, M.; Moravcova, K.; Ozana, J.; Gajdusek, L.; Miklik, R.; Sknouril, L.; et al. Exercise-Induced Blood Pressure Dynamics: Insights from the General Population and the Athletic Cohort. J. Cardiovasc. Dev. Dis. 2023, 10, 480. https://doi.org/10.3390/jcdd10120480
Pesova P, Jiravska Godula B, Jiravsky O, Jelinek L, Sovova M, Moravcova K, Ozana J, Gajdusek L, Miklik R, Sknouril L, et al. Exercise-Induced Blood Pressure Dynamics: Insights from the General Population and the Athletic Cohort. Journal of Cardiovascular Development and Disease. 2023; 10(12):480. https://doi.org/10.3390/jcdd10120480
Chicago/Turabian StylePesova, Petra, Bogna Jiravska Godula, Otakar Jiravsky, Libor Jelinek, Marketa Sovova, Katarina Moravcova, Jaromir Ozana, Libor Gajdusek, Roman Miklik, Libor Sknouril, and et al. 2023. "Exercise-Induced Blood Pressure Dynamics: Insights from the General Population and the Athletic Cohort" Journal of Cardiovascular Development and Disease 10, no. 12: 480. https://doi.org/10.3390/jcdd10120480
APA StylePesova, P., Jiravska Godula, B., Jiravsky, O., Jelinek, L., Sovova, M., Moravcova, K., Ozana, J., Gajdusek, L., Miklik, R., Sknouril, L., Neuwirth, R., & Sovova, E. (2023). Exercise-Induced Blood Pressure Dynamics: Insights from the General Population and the Athletic Cohort. Journal of Cardiovascular Development and Disease, 10(12), 480. https://doi.org/10.3390/jcdd10120480