
The Ketogenic Effect of SGLT-2 Inhibitors—Beneficial or Harmful?

 ,
,  , , , and
, , , and
Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Generic Name (Brand Name) | Dose (mg) Based on eGFR | Indications | Beneficial Effects | Adverse Effects |
|---|---|---|---|---|
| Canagliflozin (Invokana) [22] | eGFR > 60: 100 mg once daily and if tolerated, may increase to 300 mg once daily for additional glycemic control eGFR 30–60: 100 mg once daily eGFR < 30: initiation is not recommended, although patients with albuminuria (>300 mg/day) may continue 100 mg once daily to reduce the risk of ESRD, CV death, and hospitalization for HF On dialysis: contraindicated | Adjunct to diet and exercise Glycemic control in T2DM Heart attacks, stroke DKD CKD | ↓Blood sugar levels ↓Body weight ↓BP ↓Risk of CV events in high-risk patients with T2DM ↓Risk of kidney disease progression | ↑Risk of mycotic yeast infections, UTIs ↑Dehydration ↑Hypotension ↑Ketoacidosis ↑Risk of fractures ↑Risk of amputations in patients with PAD ↑AKI |
| Dapagliflozin (Farxiga) [23] | eGFR > 45: (a) initiation with 5 mg once daily if for glycemic control only. If tolerated, may increase to 10 mg once daily for additional glycemic control. (b) if other indications: initiation with 10 mg once daily eGFR 25–45: 10 mg once daily eGFR < 25: initiation is not recommended, but patients may continue 10 mg once daily to reduce the risk of eGFR decline, ESRD, CV death and hospitalization for HF On dialysis: contraindicated | Adjunct to diet and exercise Glycemic control in T2DM Chronic HFrEF ,CKD | ↓Blood sugar levels ↓Body weight ↓BP ↓Risk of CV events in high-risk patients with T2DM ↓Risk of kidney disease progression ↓Risk of HF hospitalizations ↓Reduces MAFLD ↑Improves long-term glycemic control | ↑Risk of mycotic yeast infections, UTIs ↑Dehydration ↑Hypotension ↑Ketoacidosis ↑Risk of fractures ↑Risk of amputations in patients with PAD ↑AKI |
| Empagliflozin (Jardiance) [24] | eGFR ≥ 30: initiation with 10 mg once daily. If tolerated, may increase to 25 mg once daily for additional glycemic control eGFR < 30: patients with T2DM and CV disease: no specific recommendations (lack of substantial evidence) eGFR < 20: patients with HF: no specific recommendations (lack of substantial evidence) On dialysis: contraindicated | Adjunct to diet and exercise Glycemic control in T2DM Chronic HFrEF CKD | ↓Blood sugar levels ↓Body weight ↓BP ↓Risk of HF hospitalizations ↓CV mortality ↓Albuminuria ↑Improves arterial stiffness and endothelial function | ↑Risk of mycotic yeast infections, UTIs ↑Dehydration ↑Hypotension ↑Ketoacidosis ↑Risk of fractures ↑Risk of hyperkalemia ↑AKI |
| Ertugliflozin (Steglatro) [25] | eGFR ≥ 45: (a) initiation with 5 mg once daily. If tolerated, may increase to 15 mg once daily for additional glycemic control eGFR < 45: it is not recommended On dialysis: contraindicated | Adjunct to diet and exercise Glycemic control in T2DM | ↓Blood sugar levels ↓Body weight ↓BP | ↑Risk of mycotic yeast infections, UTIs ↑Dehydration ↑Ketoacidosis |
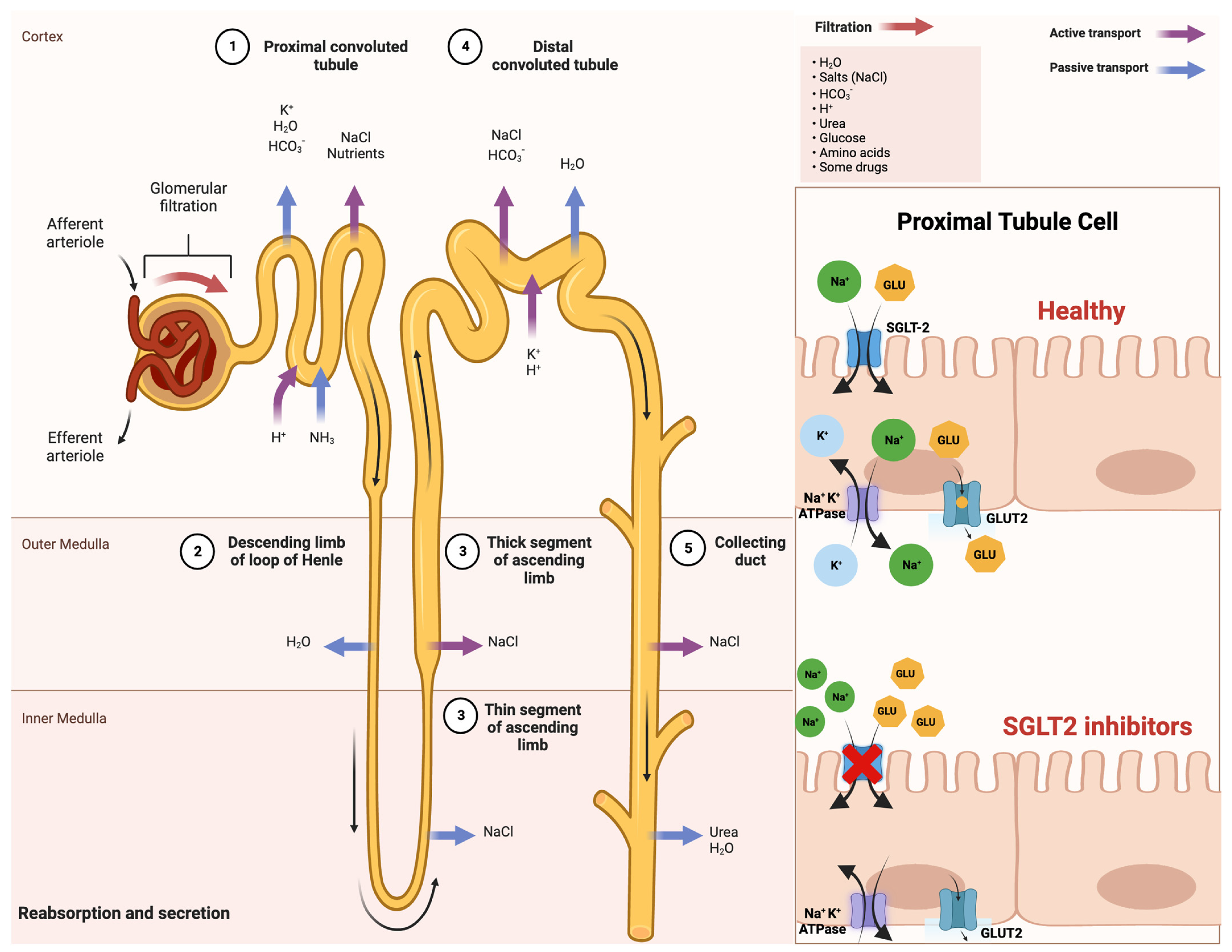
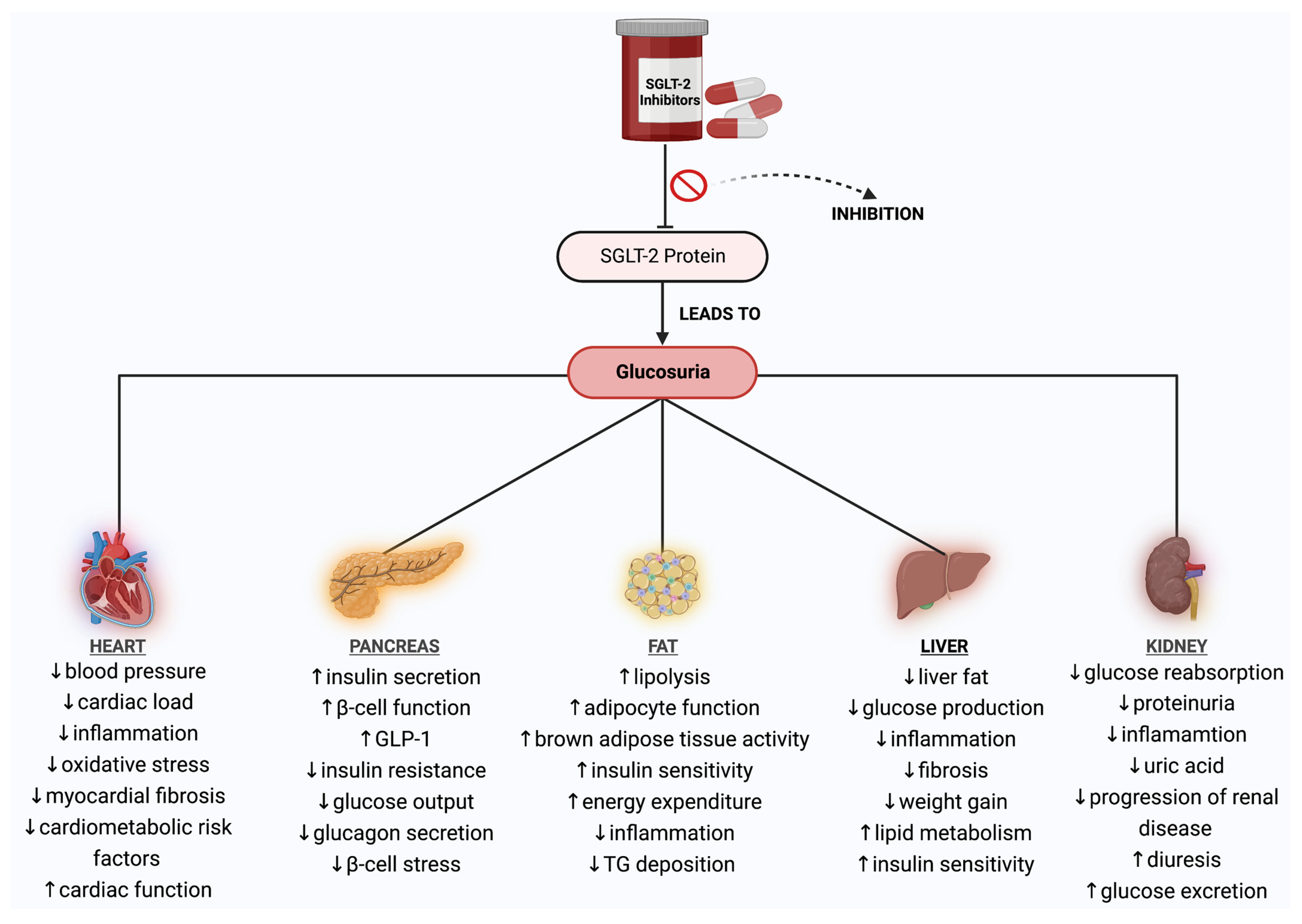
2. Mechanism of Action of SGLT-2 Inhibitors
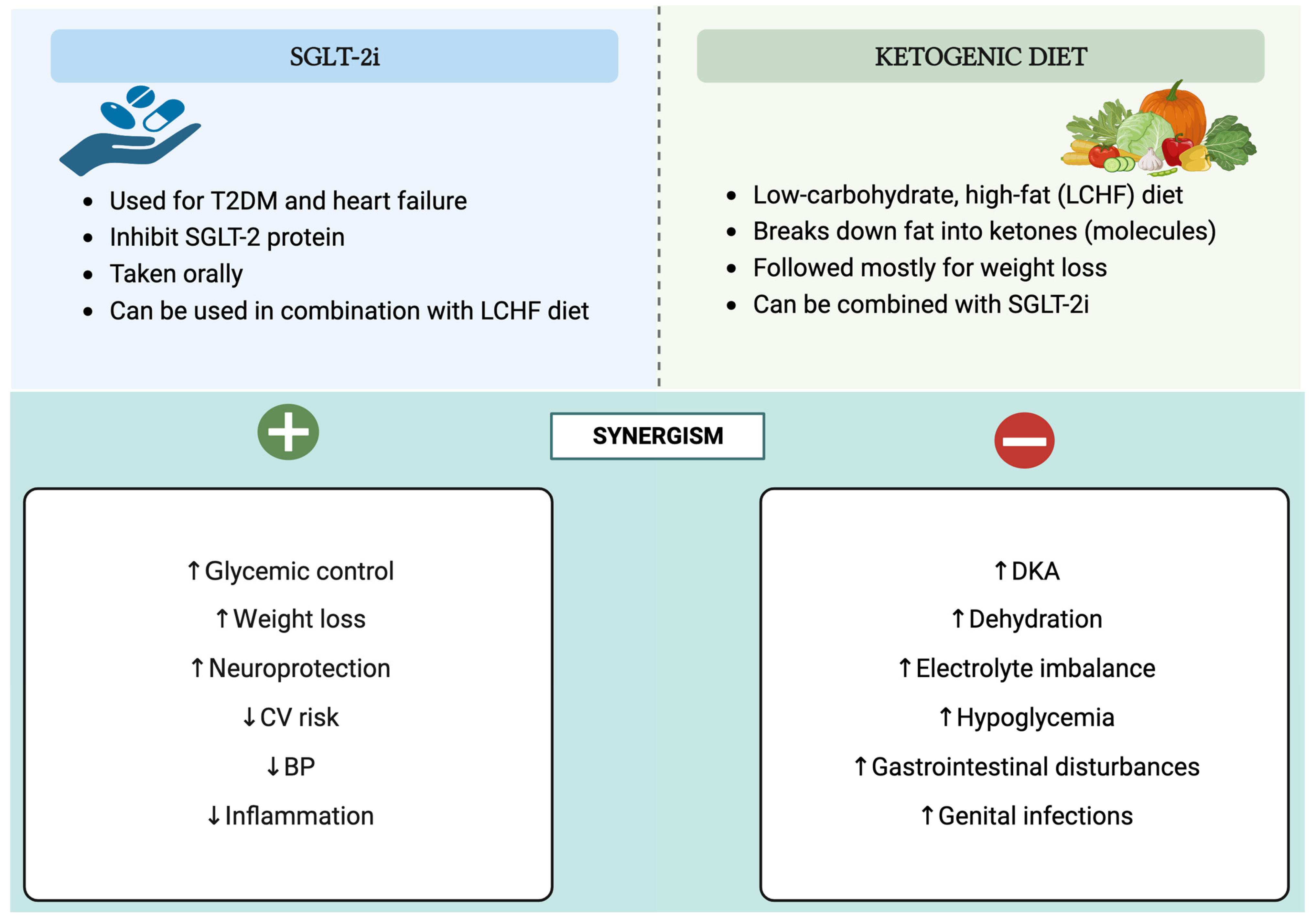
3. Synergism of SGLT-2 Inhibitors and Ketogenic Diet: Benefits and Risks
3.1. Positive Synergistic Effect of SGLT-2 Inhibitors and Ketogenic Diet: Benefits
3.2. Negative Synergistic Effect of SGLT-2 Inhibitors and Ketogenic Diet: Risks
4. Clinical Applications of SGLT-2 Inhibitors as Ketogenic Agents
4.1. Type 2 Diabetes Mellitus
4.2. Obesity
4.3. Heart Failure
4.4. Kidney Disease
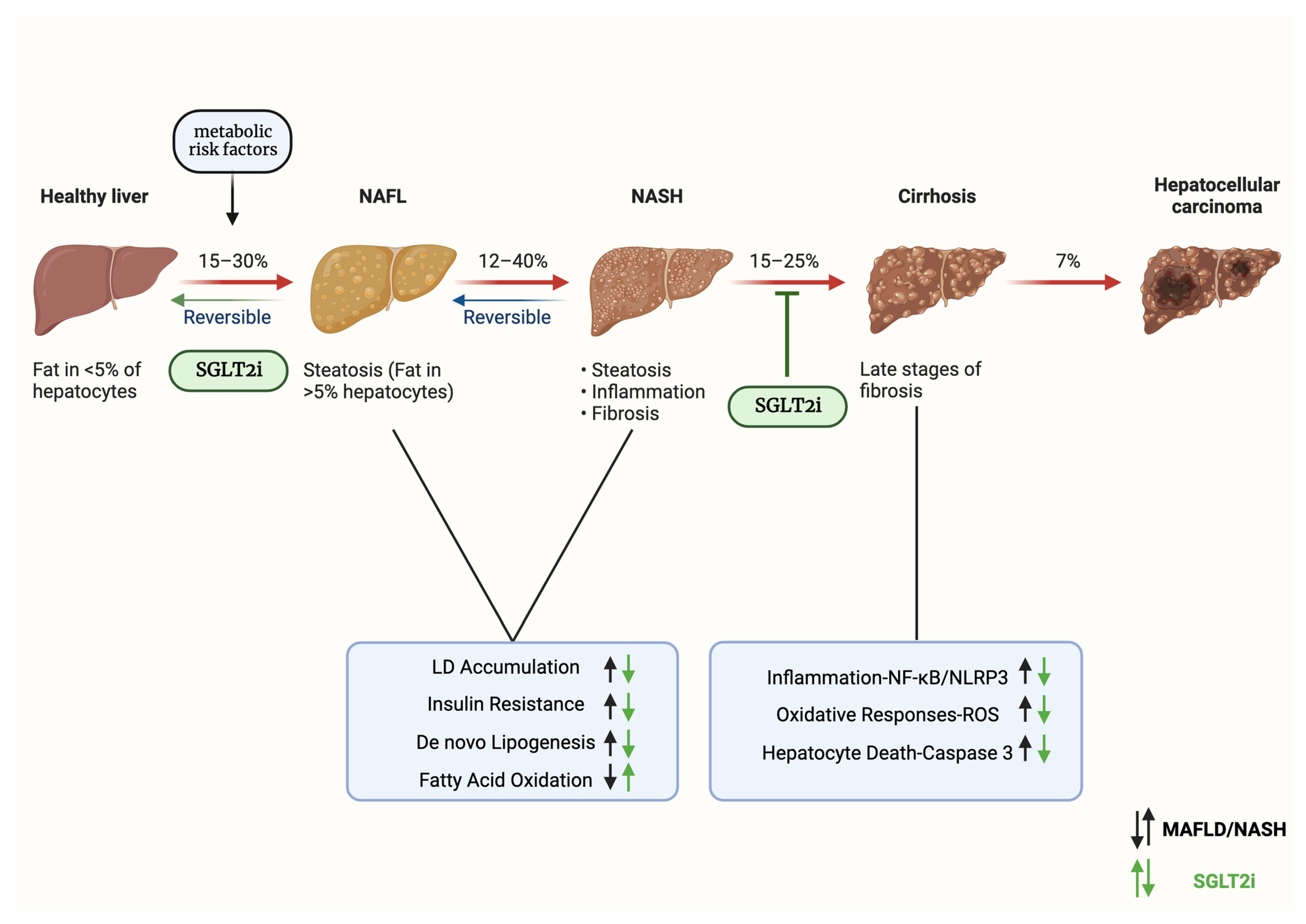
4.5. Metabolic-Associated Fatty Liver Disease (MAFLD)
5. Comparison of SGLT-2 Inhibitors with Other Anti-Diabetic Agents in Terms of Ketogenesis
6. Future Directions Regarding the Ketogenic Effects of SGLT-2 Inhibitors
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Padda, I.S.; Mahtani, A.U.; Parmar, M. Sodium-Glucose Transport Protein 2 (SGLT2) Inhibitors; StatPearls: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors|FDA. Available online: https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/sodium-glucose-cotransporter-2-sglt2-inhibitors (accessed on 11 March 2023).
- European Medicines Agency Recommends Authorisation of Novel Treatment for Type-2 Diabetes|European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/european-medicines-agency-recommends-authorisation-novel-treatment-type-2-diabetes (accessed on 27 August 2023).
- Hsia, D.S.; Grove, O.; Cefalu, W.T. An Update on SGLT2 Inhibitors for the Treatment of Diabetes Mellitus. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 73. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Perkins, B.A.; Fitchett, D.H.; Husain, M.; Cherney, D.Z.I. Sodium Glucose Cotransporter 2 Inhibitors in the Treatment of Diabetes Mellitus. Circulation 2016, 7, 10–30. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, S.G.; Kakarla, M.; Gambo, M.A.; Salama, M.Y.; Ismail, N.H.; Tavalla, P.; Uppal, P.; Mohammed, S.A.; Rajashekar, S.; Hamid, P. The Effects of Sodium-Glucose Cotransporter-2 Inhibitors (SLGT-2i) on Cardiovascular and Renal Outcomes in Non-Diabetic Patients: A Systematic Review. Cureus 2022, 14, e25476. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.K.; White, J.R. Overview of Ertugliflozin. Clin. Diabetes 2019, 37, 176. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 17–18. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Braunwald, E. Cardiac and Renal Effects of Sodium-Glucose Co-Transporter 2 Inhibitors in Diabetes: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 1845–1855. [Google Scholar] [CrossRef]
- Kalra, S.; Jain, A.; Ved, J.; Unnikrishnan, A.G. Sodium-Glucose Cotransporter 2 Inhibition and Health Benefits: The Robin Hood Effect. Indian J. Endocrinol. Metab. 2016, 20, 725. [Google Scholar] [CrossRef]
- Tentolouris, A.; Vlachakis, P.; Tzeravini, E.; Eleftheriadou, I.; Tentolouris, N. SGLT2 Inhibitors: A Review of Their Antidiabetic and Cardioprotective Effects. Int. J. Environ. Res. Public Health 2019, 16, 2965. [Google Scholar] [CrossRef] [PubMed]
- Tharmaraja, T.; Ho, J.S.Y.; Sia, C.H.; Lim, N.A.; Chong, Y.F.; Lim, A.Y.L.; Rathakrishnan, R.R.; Yeo, L.L.L.; Sharma, V.K.; Tan, B.Y.Q. Sodium-glucose cotransporter 2 inhibitors and neurological disorders: A scoping review. Ther. Adv. Chronic Dis. 2022, 13, 1–15. [Google Scholar] [CrossRef]
- Lin, K.-J.; Wang, T.-J.; Chen, S.-D.; Lin, K.-L.; Liou, C.-W.; Lan, M.-Y.; Chuang, Y.-C.; Chuang, J.-H.; Wang, P.-W.; Lee, J.-J.; et al. Two Birds One Stone: The Neuroprotective Effect of Antidiabetic Agents on Parkinson Disease—Focus on Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors. Antioxidants 2021, 10, 1935. [Google Scholar] [CrossRef] [PubMed]
- Nakhal, M.M.; Aburuz, S.; Sadek, B.; Akour, A. Repurposing SGLT2 Inhibitors for Neurological Disorders: A Focus on the Autism Spectrum Disorder. Molecules 2022, 27, 7174. [Google Scholar] [CrossRef]
- Lupsa, B.C.; Inzucchi, S.E. Use of SGLT2 Inhibitors in Type 2 Diabetes: Weighing the Risks and Benefits. Diabetologia 2018, 61, 2118–2125. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Fan, F.; Wang, J.Y.; Long, Y.; Gao, C.L.; Stanton, R.C.; Xu, Y. The Efficacy and Safety of SGLT2 Inhibitors for Adjunctive Treatment of Type 1 Diabetes: A Systematic Review and Meta-Analysis. Sci. Rep. 2017, 7, 44128. [Google Scholar] [CrossRef] [PubMed]
- Chábová, V.Č.; Zakiyanov, O. Sodium Glucose Cotransporter-2 Inhibitors: Spotlight on Favorable Effects on Clinical Outcomes beyond Diabetes. Int. J. Mol. Sci. 2022, 23, 2812. [Google Scholar] [CrossRef] [PubMed]
- Kapila, V.; Topf, J. Sodium-Glucose Co-Transporter 2 Inhibitor-Associated Euglycemic Diabetic Ketoacidosis After Bariatric Surgery: A Case and Literature Review. Cureus 2021, 13, e17093. [Google Scholar] [CrossRef]
- Invokana (Canagliflozin); Janssen Pharmaceuticals, Inc.: Titusville, NJ, USA, 2023.
- Farxiga (Dapagliflozin); AstraZeneca Pharmaceutical LP: Wilmington, DE, USA, 2020.
- Jardiance (Empagliflozin); Boehringer Ingelheim Pharmaceuticals, Inc.: Ridgefield, CT, USA, 2022.
- Steglatro (Ertugliflozin); Merck & Co, Inc.: Whitehouse Station, NJ, USA, 2021.
- Ferrannini, E. Sodium-Glucose Co-Transporters and Their Inhibition: Clinical Physiology. Cell Metab. 2017, 26, 27–38. [Google Scholar] [CrossRef]
- Wright, E.M.; Loo, D.D.F.L.; Hirayama, B.A. Biology of Human Sodium Glucose Transporters. Physiol. Rev. 2011, 91, 733–794. [Google Scholar] [CrossRef]
- Gallo, L.A.; Wright, E.M.; Vallon, V. Probing SGLT2 as a Therapeutic Target for Diabetes: Basic Physiology and Consequences. Diabetes Vasc. Dis. Res. 2015, 12, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Nespoux, J.; Vallon, V. Renal Effects of SGLT2 Inhibitors: An Update. Curr. Opin. Nephrol. Hypertens. 2020, 29, 190. [Google Scholar] [CrossRef] [PubMed]
- Pittampalli, S.; Upadyayula, S.; Mekala, M.H.; Lippmann, S. Risks vs. Benefits for SGLT2 Inhibitor Medications. Fed. Pract. 2018, 35, 45. [Google Scholar] [PubMed]
- Sarafidis, P.; Ferro, C.J.; Morales, E.; Ortiz, A.; Malyszko, J.; Hojs, R.; Khazim, K.; Ekart, R.; Valdivielso, J.; Fouque, D.; et al. SGLT-2 Inhibitors and GLP-1 Receptor Agonists for Nephroprotection and Cardioprotection in Patients with Diabetes Mellitus and Chronic Kidney Disease. A Consensus Statement by the EURECA-m and the DIABESITY Working Groups of the ERA-EDTA. Nephrol. Dial. Transplant. 2019, 34, 208–230. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.-Y.; Liu, L.-Y.; Jia, Y.; Li, Y.; Cai, J.-N.; Shu, Y.; Tan, J.-Y.; Chen, P.-Y.; Li, H.-W.; Cai, H.-H.; et al. Correlation between Gut Microbiota and Glucagon-like Peptide-1 in Patients with Gestational Diabetes Mellitus. World J. Diabetes 2022, 13, 861. [Google Scholar] [CrossRef]
- Das, U.S.; Paul, A.; Banerjee, S. SGLT2 Inhibitors in Heart Failure with Reduced Ejection Fraction. Egypt. Heart J. 2021, 73, 93. [Google Scholar] [CrossRef]
- Neuen, B.L.; Young, T.; Heerspink, H.J.L.; Neal, B.; Perkovic, V.; Billot, L.; Mahaffey, K.W.; Charytan, D.M.; Wheeler, D.C.; Arnott, C.; et al. SGLT2 Inhibitors for the Prevention of Kidney Failure in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Lancet Diabetes Endocrinol. 2019, 7, 845–854. [Google Scholar] [CrossRef]
- Abdelgadir, E.; Rashid, F.; Bashier, A.; Ali, R. SGLT-2 Inhibitors and Cardiovascular Protection: Lessons and Gaps in Understanding the Current Outcome Trials and Possible Benefits of Combining SGLT-2 Inhibitors With GLP-1 Agonists. J. Clin. Med. Res. 2018, 10, 615. [Google Scholar] [CrossRef]
- Bonora, B.M.; Avogaro, A.; Fadini, G.P. Extraglycemic Effects of SGLT2 Inhibitors: A Review of the Evidence. Diabetes Metab. Syndr. Obes. 2020, 13, 161. [Google Scholar] [CrossRef]
- Gao, J.; Xue, G.; Zhan, G.; Wang, X.; Li, J.; Yang, X.; Xia, Y. Benefits of SGLT2 Inhibitors in Arrhythmias. Front. Cardiovasc. Med. 2022, 9, 3066. [Google Scholar] [CrossRef]
- Kolijn, D.; Pabel, S.; Tian, Y.; Lódi, M.; Herwig, M.; Carrizzo, A.; Zhazykbayeva, S.; Kovács, Á.; Fülöp, G.; Falcão-Pires, I.; et al. Empagliflozin Improves Endothelial and Cardiomyocyte Function in Human Heart Failure with Preserved Ejection Fraction via Reduced Pro-Inflammatory-Oxidative Pathways and Protein Kinase Gα Oxidation. Cardiovasc. Res. 2021, 117, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Bellanti, F.; Buglio, A.L.; Serviddio, G.; Vendemiale, G.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Aich, P.; Singh, S.P. Impact of Sodium Glucose Cotransporter-2 Inhibitors on Liver Steatosis/Fibrosis/Inflammation and Redox Balance in Non-Alcoholic Fatty Liver Disease. World J. Gastroenterol. 2022, 28, 3243. [Google Scholar] [CrossRef] [PubMed]
- Androutsakos, T.; Nasiri-Ansari, N.; Bakasis, A.D.; Kyrou, I.; Efstathopoulos, E.; Randeva, H.S.; Kassi, E. SGLT-2 Inhibitors in NAFLD: Expanding Their Role beyond Diabetes and Cardioprotection. Int. J. Mol. Sci. 2022, 23, 3107. [Google Scholar] [CrossRef]
- Yanai, H.; Hakoshima, M.; Katsuyama, H.; Email, J. The Possible Mechanisms for Improvement of Liver Function Due to Sodium-Glucose Cotransporter-2 Inhibitors. J. Clin. Med. Res. 2019, 11, 769–772. [Google Scholar] [CrossRef] [PubMed]
- Maejima, Y. SGLT2 Inhibitors Play a Salutary Role in Heart Failure via Modulation of the Mitochondrial Function. Front. Cardiovasc. Med. 2020, 6, 186. [Google Scholar] [CrossRef]
- Gharaibeh, N.E.; Rahhal, M.N.; Rahimi, L.; Ismail-Beigi, F. SGLT-2 Inhibitors as Promising Therapeutics for Non-Alcoholic Fatty Liver Disease: Pathophysiology, Clinical Outcomes, and Future Directions. Diabetes Metab. Syndr. Obes. 2019, 12, 1001. [Google Scholar] [CrossRef]
- Merovci, A.; Abdul-Ghani, M.; Mari, A.; Solis-Herrera, C.; Xiong, J.; Daniele, G.; Tripathy, D.; DeFronzo, R.A. Effect of Dapagliflozin with and without Acipimox on Insulin Sensitivity and Insulin Secretion in T2DM Males. J. Clin. Endocrinol. Metab. 2016, 101, 1249–1256. [Google Scholar] [CrossRef]
- Merovci, A.; Mari, A.; Solis, C.; DeFronzo, R.A.; Daniele, G.; Chavez-Velazquez, A.; Tripathy, D.; McCarthy, S.U.; Abdul-Ghani, M.; Xiong, J. Dapagliflozin Lowers Plasma Glucose Concentration and Improves β-Cell Function. J. Clin. Endocrinol. Metab. 2015, 100, 1927. [Google Scholar] [CrossRef]
- Al Jobori, H.; Daniele, G.; Adams, J.; Cersosimo, E.; Solis-Herrera, C.; Triplitt, C.; Defronzo, R.A.; Abdul-Ghani, M. Empagliflozin Treatment Is Associated with Improved β-Cell Function in Type 2 Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2018, 103, 1402. [Google Scholar] [CrossRef]
- Liu, X.; Chen, Y.; Liu, T.; Cai, L.; Yang, X.; Mou, C. The Effects of Sodium-Glucose Cotransporter 2 Inhibitors on Adipose Tissue in Patients with Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials. Front. Endocrinol. 2023, 14, 114. [Google Scholar] [CrossRef]
- Lauritsen, K.M.; Voigt, J.H.; Pedersen, S.B.; Hansen, T.K.; Møller, N.; Jessen, N.; Gormsen, L.C.; Søndergaard, E. Effects of SGLT2 Inhibition on Lipid Transport in Adipose Tissue in Type 2 Diabetes. Endocr. Connect. 2022, 11, e210558. [Google Scholar] [CrossRef]
- Pratama, K.G.; Tandarto, K.; Hengky, A. Weight loss effect of sodium-glucose cotransporter-2 (sglt2) inhibitors in patients with obesity without diabetes: A systematic review. Acta Endocrinol. 2022, 18, 216. [Google Scholar] [CrossRef]
- Kurinami, N.; Sugiyama, S.; Nishimura, H.; Morita, A.; Yoshida, A.; Hieshima, K.; Miyamoto, F.; Kajiwara, K.; Jinnouchi, K.; Jinnouchi, T.; et al. Clinical Factors Associated with Initial Decrease in Body-Fat Percentage Induced by Add-on Sodium-Glucose Co-Transporter 2 Inhibitors in Patient with Type 2 Diabetes Mellitus. Clin. Drug Investig. 2018, 38, 19. [Google Scholar] [CrossRef] [PubMed]
- Global Epidemic of Type 2 Diabetes: Implications for Developing Countries–PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/13677423/ (accessed on 23 March 2023).
- Unnikrishnan, R.; Pradeepa, R.; Joshi, S.R.; Mohan, V. Type 2 Diabetes: Demystifying the Global Epidemic. Diabetes 2017, 66, 1432–1442. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Colditz, G.; Liu, S.; Solomon, C.G.; Willett, W.C. Diet, Lifestyle, and the Risk of Type 2 Diabetes Mellitus in Women. N. Engl. J. Med. 2001, 345, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, A.; Perry, L.; Gholizadeh, L.; Al-Ganmi, A. Incidence and Prevalence Rates of Diabetes Mellitus in Saudi Arabia: An Overview. J. Epidemiol. Glob. Health 2017, 7, 211. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Kaabi, J. Al Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107. [Google Scholar] [CrossRef]
- Lone, S.; Lone, K.; Khan, S.; Pampori, R.A. Assessment of Metabolic Syndrome in Kashmiri Population with Type 2 Diabetes Employing the Standard Criteria’s given by WHO, NCEPATP III and IDF. J. Epidemiol. Glob. Health 2017, 7, 235. [Google Scholar] [CrossRef]
- Mahanta, T.G.; Joshi, R.; Mahanta, B.N.; Xavier, D. Prevalence of Modifiable Cardiovascular Risk Factors among Tea Garden and General Population in Dibrugarh, Assam, India. J. Epidemiol. Glob. Health 2013, 3, 147–156. [Google Scholar] [CrossRef]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and Regional Diabetes Prevalence Estimates for 2019 and Projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th Edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef]
- Dashti, H.M.; Mathew, T.C.; Khadada, M.; Al-Mousawi, M.; Talib, H.; Asfar, S.K.; Behbahani, A.I.; Al-Zaid, N.S. Beneficial Effects of Ketogenic Diet in Obese Diabetic Subjects. Mol. Cell Biochem. 2007, 302, 249–256. [Google Scholar] [CrossRef] [PubMed]
- US FDA Approves FARXIGATM Tablets for the Treatment of Adult Patients–AstraZeneca. Available online: https://www.astrazeneca.com/media-centre/press-releases/2014/us-fda-approved-farxiga-treatment-type-2-diabetes-patients-13012014.html# (accessed on 29 March 2023).
- Ferrannini, E.; Solini, A. SGLT2 Inhibition in Diabetes Mellitus: Rationale and Clinical Prospects. Nat. Rev. Endocrinol. 2012, 8, 495–502. [Google Scholar] [CrossRef]
- Srinivas, N.; Sarnaik, M.K.; Modi, S.; Pisipati, Y.; Vaidya, S.; Gaggatur, N.S.; Sange, A.H.; Sange, I. Sodium-Glucose Cotransporter 2 (SGLT-2) Inhibitors: Delving into the Potential Benefits of Cardiorenal Protection Beyond the Treatment of Type-2 Diabetes Mellitus. Cureus 2021, 13, e16868. [Google Scholar] [CrossRef] [PubMed]
- Freeman, J.M.; Kossoff, E.H.; Hartman, A.L. The Ketogenic Diet: One Decade Later. Pediatrics 2007, 119, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Yancy, W.S.; Foy, M.; Chalecki, A.M.; Vernon, M.C.; Westman, E.C. A Low-Carbohydrate, Ketogenic Diet to Treat Type 2 Diabetes. Nutr. Metab. 2005, 2, 34. [Google Scholar] [CrossRef]
- Diet Review: Ketogenic Diet for Weight Loss|The Nutrition Source|Harvard, T.H. Chan School of Public Health. Available online: https://www.hsph.harvard.edu/nutritionsource/healthy-weight/diet-reviews/ketogenic-diet/ (accessed on 29 March 2023).
- Fieger, E.I.; Fadel, K.M.; Modarres, A.H.; Edmond, P.; Wickham, I.; Wolver, S.E. Successful Reimplementation of a Very Low Carbohydrate Ketogenic Diet after sglt2 Inhibitor Associated Euglycemic Diabetic Ketoacidosis. AACE Clin. Case Rep. 2020, 6, e330. [Google Scholar] [CrossRef]
- Vallon, V.; Thomson, S.C. Targeting Renal Glucose Reabsorption to Treat Hyperglycaemia: The Pleiotropic Effects of SGLT2 Inhibition. Diabetologia 2017, 60, 215–225. [Google Scholar] [CrossRef]
- Pereira, M.J.; Eriksson, J.W. Emerging Role of SGLT-2 Inhibitors for the Treatment of Obesity. Drugs 2019, 79, 219. [Google Scholar] [CrossRef]
- Bashier, A.; Khalifa, A.A.; Rashid, F.; Abdelgadir, E.I.; Al Qaysi, A.A.; Ali, R.; Eltinay, A.; Nafach, J.; Alsayyah, F.; Alawadi, F. Efficacy and Safety of SGLT2 Inhibitors in Reducing Glycated Hemoglobin and Weight in Emirati Patients With Type 2 Diabetes. J. Clin. Med. Res. 2017, 9, 499. [Google Scholar] [CrossRef]
- Dowis, K.; Banga, S. The Potential Health Benefits of the Ketogenic Diet: A Narrative Review. Nutrients 2021, 13, 1654. [Google Scholar] [CrossRef]
- Haimoto, H.; Sasakabe, T.; Wakai, K.; Umegaki, H. Effects of a Low-Carbohydrate Diet on Glycemic Control in Outpatients with Severe Type 2 Diabetes. Nutr. Metab. 2009, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Markovikj, G.; Knights, V.; Kljusurić, J.G. Ketogenic Diet Applied in Weight Reduction of Overweight and Obese Individuals with Progress Prediction by Use of the Modified Wishnofsky Equation. Nutrients 2023, 15, 927. [Google Scholar] [CrossRef]
- Bueno, N.B.; De Melo, I.S.V.; De Oliveira, S.L.; Da Rocha Ataide, T. Very-Low-Carbohydrate Ketogenic Diet v. Low-Fat Diet for Long-Term Weight Loss: A Meta-Analysis of Randomised Controlled Trials. Br. J. Nutr. 2013, 110, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Yancy, W.S.; Olsen, M.K.; Dudley, T.; Westman, E.C. Acid-Base Analysis of Individuals Following Two Weight Loss Diets. Eur. J. Clin. Nutr. 2007, 61, 1416–1422. [Google Scholar] [CrossRef] [PubMed]
- Guirguis, H.; Beroukhim Afrahimi, S.; Pham, C. The Use of SGLT-2 Inhibitors Coupled with a Strict Low-Carbohydrate Diet: A Set-Up for Inducing Severe Diabetic Ketoacidosis. Clin. Med. Insights Case Rep. 2022, 15, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Li, S.; Kang, B.; Zhou, J. The Current Role of Sodium-Glucose Cotransporter 2 Inhibitors in Type 2 Diabetes Mellitus Management. Cardiovasc. Diabetol. 2022, 21, 83. [Google Scholar] [CrossRef] [PubMed]
- Alarim, R.A.; Alasmre, F.A.; Alotaibi, H.A.; Alshehri, M.A.; Hussain, S.A. Effects of the Ketogenic Diet on Glycemic Control in Diabetic Patients: Meta-Analysis of Clinical Trials. Cureus 2020, 12, e10796. [Google Scholar] [CrossRef]
- Dashti, H.M.; Mathew, T.C.; Hussein, T.; Asfar, S.K.; Behbahani, A.; Khoursheed, M.A.; Al-Sayer, H.M.; Bo-Abbas, Y.Y.; Al-Zaid, N.S. Long-Term Effects of a Ketogenic Diet in Obese Patients. Exp. Clin. Cardiol. 2004, 9, 200. [Google Scholar]
- Di Raimondo, D.; Buscemi, S.; Musiari, G.; Rizzo, G.; Pirera, E.; Corleo, D.; Pinto, A.; Tuttolomondo, A. Ketogenic Diet, Physical Activity, and Hypertension—A Narrative Review. Nutrients 2021, 13, 2567. [Google Scholar] [CrossRef]
- Baker, W.L.; Smyth, L.R.; Riche, D.M.; Bourret, E.M.; Chamberlin, K.W.; White, W.B. Effects of Sodium-Glucose Co-Transporter 2 Inhibitors on Blood Pressure: A Systematic Review and Meta-Analysis. J. Am. Soc. Hypertens. 2014, 8, 262–275.e9. [Google Scholar] [CrossRef]
- Tang, J.; Ye, L.; Yan, Q.; Zhang, X.; Wang, L. Effects of Sodium-Glucose Cotransporter 2 Inhibitors on Water and Sodium Metabolism. Front. Pharmacol. 2022, 13, 330. [Google Scholar] [CrossRef] [PubMed]
- García-Ropero, Á.; Santos-Gallego, C.G.; Badimon, J.J. The Anti-Inflammatory Effects of SGLT Inhibitors. Aging 2019, 11, 5866. [Google Scholar] [CrossRef] [PubMed]
- Pinto, A.; Bonucci, A.; Maggi, E.; Corsi, M.; Businaro, R. Anti-Oxidant and Anti-Inflammatory Activity of Ketogenic Diet: New Perspectives for Neuroprotection in Alzheimer’s Disease. Antioxidants 2018, 7, 63. [Google Scholar] [CrossRef] [PubMed]
- Gough, S.M.; Casella, A.; Ortega, K.J.; Hackam, A.S. Neuroprotection by the Ketogenic Diet: Evidence and Controversies. Front. Nutr. 2021, 8, 782657. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Sung, S.F. From Kidney Protection to Stroke Prevention: The Potential Role of Sodium Glucose Cotransporter-2 Inhibitors. Int. J. Mol. Sci. 2023, 24, 351. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.A.; Hartman, A.L. Ketone Bodies in Epilepsy. J. Neurochem. 2012, 121, 28. [Google Scholar] [CrossRef]
- Pawlos, A.; Broncel, M.; Woźniak, E.; Gorzelak-Pabiś, P. Neuroprotective Effect of SGLT2 Inhibitors. Molecules 2021, 26, 7213. [Google Scholar] [CrossRef]
- Hierro-Bujalance, C.; Infante-Garcia, C.; Del Marco, A.; Herrera, M.; Carranza-Naval, M.J.; Suarez, J.; Alves-Martinez, P.; Lubian-Lopez, S.; Garcia-Alloza, M. Empagliflozin Reduces Vascular Damage and Cognitive Impairment in a Mixed Murine Model of Alzheimer’s Disease and Type 2 Diabetes. Alzheimers Res. Ther. 2020, 12, 40. [Google Scholar] [CrossRef]
- Tsai, W.H.; Chuang, S.M.; Liu, S.C.; Lee, C.C.; Chien, M.N.; Leung, C.H.; Liu, S.J.; Shih, H.M. Effects of SGLT2 Inhibitors on Stroke and Its Subtypes in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 15364. [Google Scholar] [CrossRef]
- Zhou, Z.; Jardine, M.J.; Li, Q.; Neuen, B.L.; Cannon, C.P.; De Zeeuw, D.; Edwards, R.; Levin, A.; Mahaffey, K.W.; Perkovic, V.; et al. Effect of SGLT2 Inhibitors on Stroke and Atrial Fibrillation in Diabetic Kidney Disease: Results From the CREDENCE Trial and Meta-Analysis. Stroke 2021, 52, 1545–1556. [Google Scholar] [CrossRef]
- Batch, J.T.; Lamsal, S.P.; Adkins, M.; Sultan, S.; Ramirez, M.N. Advantages and Disadvantages of the Ketogenic Diet: A Review Article. Cureus 2020, 12, e9639. [Google Scholar] [CrossRef] [PubMed]
- Ting, R.; Dugré, N.; Allan, G.M.; Lindblad, A.J. Ketogenic Diet for Weight Loss. Can. Fam. Physician 2018, 64, 906. [Google Scholar] [CrossRef]
- Masood, W.; Annamaraju, P.; Uppaluri, K.R. Ketogenic Diet; StatPearls: St. Petersburg, FL, USA, 2022. [Google Scholar]
- D’Andrea Meira, I.; Romão, T.T.; Do Prado, H.J.P.; Krüger, L.T.; Pires, M.E.P.; Da Conceição, P.O. Ketogenic Diet and Epilepsy: What We Know So Far. Front. Neurosci. 2019, 13, 5. [Google Scholar] [CrossRef]
- Paoli, A. Ketogenic Diet for Obesity: Friend or Foe? Int. J. Environ. Res. Public Health 2014, 11, 2092. [Google Scholar] [CrossRef] [PubMed]
- Mistry, S.; Eschler, D.C. Euglycemic Diabetic Ketoacidosis Caused by SGLT2 Inhibitors and a Ketogenic Diet: A Case Series and Review of Literature. AACE Clin. Case Rep. 2021, 7, 17–19. [Google Scholar] [CrossRef]
- Plewa, M.C.; Bryant, M.; King-Thiele, R. Euglycemic Diabetic Ketoacidosis; StatPearls: St. Petersburg, FL, USA, 2023. [Google Scholar]
- Meyer, E.J.; Gabb, G.; Jesudason, D. SGLT2 Inhibitor–Associated Euglycemic Diabetic Ketoacidosis: A South Australian Clinical Case Series and Australian Spontaneous Adverse Event Notifications. Diabetes Care 2018, 41, e47–e49. [Google Scholar] [CrossRef]
- Hamblin, P.S.; Wong, R.; Ekinci, E.I.; Fourlanos, S.; Shah, S.; Jones, A.R.; Hare, M.J.L.; Calder, G.L.; Epa, D.S.; George, E.M.; et al. SGLT2 Inhibitors Increase the Risk of Diabetic Ketoacidosis Developing in the Community and During Hospital Admission. J. Clin. Endocrinol. Metab. 2019, 104, 3077–3087. [Google Scholar] [CrossRef] [PubMed]
- White-Cotsmire, A.J.; Healy, A.M. Ketogenic Diet as a Trigger for Diabetic Ketoacidosis in a Misdiagnosis of Diabetes: A Case Report. Clin. Diabetes 2020, 38, 318. [Google Scholar] [CrossRef] [PubMed]
- Hester, J.C.; Zimmerman, S.; Nimmo, T.A.; Cunningham, W.; Liu, J.; Sukpraprut-Braaten, S.; Pasquel, F.J. Euglycemic Diabetic Ketoacidosis Secondary to SGLT2-Inhibitor Use in Combination with a Ketogenic Diet. J. Endocr. Soc. 2021, 5, A380–A381. [Google Scholar] [CrossRef]
- Shaheen, N.A.; Alqahtani, A.A.; Assiri, H.; Alkhodair, R.; Hussein, M.A. Public Knowledge of Dehydration and Fluid Intake Practices: Variation by Participants’ Characteristics. BMC Public Health 2018, 18, 1346. [Google Scholar] [CrossRef]
- Taylor, K.; Jones, E.B. Adult Dehydration; StatPearls: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Horii, T.; Oikawa, Y.; Kunisada, N.; Shimada, A.; Atsuda, K. Real-World Risk of Hypoglycemia-Related Hospitalization in Japanese Patients with Type 2 Diabetes Using SGLT2 Inhibitors: A Nationwide Cohort Study. BMJ Open Diabetes Res. Care 2020, 8, e001856. [Google Scholar] [CrossRef] [PubMed]
- Bolla, A.M.; Caretto, A.; Laurenzi, A.; Scavini, M.; Piemonti, L. Low-Carb and Ketogenic Diets in Type 1 and Type 2 Diabetes. Nutrients 2019, 11, 962. [Google Scholar] [CrossRef] [PubMed]
- Chao, E.C. SGLT-2 Inhibitors: A New Mechanism for Glycemic Control. Clin. Diabetes 2014, 32, 4. [Google Scholar] [CrossRef] [PubMed]
- Duchowny, M.S. Food for Thought: The Ketogenic Diet and Adverse Effects in Children. Epilepsy Curr. 2005, 5, 152. [Google Scholar] [CrossRef]
- Yang, H.; Choi, E.; Park, E.; Na, E.; Chung, S.Y.; Kim, B.; Han, S.Y. Risk of Genital and Urinary Tract Infections Associated with SGLT-2 Inhibitors as an Add-on Therapy to Metformin in Patients with Type 2 Diabetes Mellitus: A Retrospective Cohort Study in Korea. Pharmacol. Res. Perspect. 2022, 10, e00910. [Google Scholar] [CrossRef]
- Ruskin, D.N.; Sturdevant, I.C.; Wyss, L.S.; Masino, S.A. Ketogenic Diet Effects on Inflammatory Allodynia and Ongoing Pain in Rodents. Sci. Rep. 2021, 11, 725. [Google Scholar] [CrossRef]
- Crosby, L.; Davis, B.; Joshi, S.; Jardine, M.; Paul, J.; Neola, M.; Barnard, N.D. Ketogenic Diets and Chronic Disease: Weighing the Benefits Against the Risks. Front. Nutr. 2021, 8, 403. [Google Scholar] [CrossRef]
- ‘Keto-Like’ Diet May Be Linked to Higher Risk of Heart Disease, Cardiac Events–American College of Cardiology. Available online: https://www.acc.org/About-ACC/Press-Releases/2023/03/05/15/07/Keto-Like-Diet-May-Be-Linked-to-Higher-Risk (accessed on 1 April 2023).
- Varzideh, F.; Kansakar, U.; Santulli, G. SGLT2 Inhibitors in Cardiovascular Medicine. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, e67–e68. [Google Scholar] [CrossRef]
- Saisho, Y. SGLT2 Inhibitors: The Star in the Treatment of Type 2 Diabetes? Diseases 2020, 8, 14. [Google Scholar] [CrossRef]
- Goddard, C.; Allenspach, K.; Deflandre, A.; Zemirline, C.; Guillot, E.; Mochel, J.P. SGLT2 Inhibitors and Potential Applications in Treating Metabolic Syndrome. Preprints 2022, 2022040202. [Google Scholar] [CrossRef]
- Devenny, J.J.; Godonis, H.E.; Harvey, S.J.; Rooney, S.; Cullen, M.J.; Pelleymounter, M.A. Weight Loss Induced by Chronic Dapagliflozin Treatment Is Attenuated by Compensatory Hyperphagia in Diet-Induced Obese (DIO) Rats. Obesity 2012, 20, 1645–1652. [Google Scholar] [CrossRef] [PubMed]
- Yokono, M.; Takasu, T.; Hayashizaki, Y.; Mitsuoka, K.; Kihara, R.; Muramatsu, Y.; Miyoshi, S.; Tahara, A.; Kurosaki, E.; Li, Q.; et al. SGLT2 Selective Inhibitor Ipragliflozin Reduces Body Fat Mass by Increasing Fatty Acid Oxidation in High-Fat Diet-Induced Obese Rats. Eur. J. Pharmacol. 2014, 727, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Takeda, M.; Kito, A.; Fukazawa, M.; Yata, T.; Yamamoto, M.; Nagata, T.; Fukuzawa, T.; Yamane, M.; Honda, K.; et al. Tofogliflozin, a Sodium/Glucose Cotransporter 2 Inhibitor, Attenuates Body Weight Gain and Fat Accumulation in Diabetic and Obese Animal Models. Nutr. Diabetes 2014, 4, e125. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E.; Baldi, S.; Frascerra, S.; Astiarraga, B.; Heise, T.; Bizzotto, R.; Mari, A.; Pieber, T.R.; Muscelli, E. Shift to Fatty Substrate Utilization in Response to Sodium-Glucose Cotransporter 2 Inhibition in Subjects Without Diabetes and Patients with Type 2 Diabetes. Diabetes 2016, 65, 1190–1196. [Google Scholar] [CrossRef]
- Nishimura, R.; Tanaka, Y.; Koiwai, K.; Inoue, K.; Hach, T.; Salsali, A.; Lund, S.S.; Broedl, U.C. Effect of Empagliflozin Monotherapy on Postprandial Glucose and 24-Hour Glucose Variability in Japanese Patients with Type 2 Diabetes Mellitus: A Randomized, Double-Blind, Placebo-Controlled, 4-Week Study. Cardiovasc. Diabetol. 2015, 14, 11. [Google Scholar] [CrossRef]
- Nishimura, R.; Osonoi, T.; Kanada, S.; Jinnouchi, H.; Sugio, K.; Omiya, H.; Ubukata, M.; Sakai, S.; Samukawa, Y. Effects of Luseogliflozin, a Sodium-Glucose Co-Transporter 2 Inhibitor, on 24-h Glucose Variability Assessed by Continuous Glucose Monitoring in Japanese Patients with Type 2 Diabetes Mellitus: A Randomized, Double-Blind, Placebo-Controlled, Crossover Study. Diabetes Obes. Metab. 2015, 17, 800–804. [Google Scholar] [CrossRef]
- Inagaki, N.; Kondo, K.; Yoshinari, T.; Takahashi, N.; Susuta, Y.; Kuki, H. Efficacy and Safety of Canagliflozin Monotherapy in Japanese Patients with Type 2 Diabetes Inadequately Controlled with Diet and Exercise: A 24-Week, Randomized, Double-Blind, Placebo-Controlled, Phase III Study. Expert. Opin. Pharmacother. 2014, 15, 1501–1515. [Google Scholar] [CrossRef]
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41, 2669–2701. [Google Scholar] [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycaemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2022, 65, 1925–1966. [Google Scholar] [CrossRef]
- Marx, N.; Federici, M.; Schütt, K.; Müller-Wieland, D.; Ajjan, R.A.; Antunes, M.J.; Christodorescu, R.M.; Crawford, C.; Di Angelantonio, E.; Eliasson, B.; et al. 2023 ESC Guidelines for the Management of Cardiovascular Disease in Patients with DiabetesDeveloped by the Task Force on the Management of Cardiovascular Disease in Patients with Diabetes of the European Society of Cardiology (ESC). Eur. Heart J. 2023, 44, 4043–4140. [Google Scholar] [CrossRef]
- SCORE2-Diabetes Working Group; the ESC Cardiovascular Risk Collaboration; Pennells, L.; Kaptoge, S.; Østergaard, H.B.; Read, S.H.; Carinci, F.; Franch-Nadal, J.; Petitjean, C.; Taylor, O.; et al. SCORE2-Diabetes: 10-Year Cardiovascular Risk Estimation in Type 2 Diabetes in Europe. Eur. Heart J. 2023, 44, 2544–2556. [Google Scholar] [CrossRef]
- Obesity and Overweight. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 5 April 2023).
- Zaccardi, F.; Webb, D.R.; Htike, Z.Z.; Youssef, D.; Khunti, K.; Davies, M.J. Efficacy and Safety of Sodium-Glucose Co-Transporter-2 Inhibitors in Type 2 Diabetes Mellitus: Systematic Review and Network Meta-Analysis. Diabetes Obes. Metab. 2016, 18, 783–794. [Google Scholar] [CrossRef]
- Liu, X.Y.; Zhang, N.; Chen, R.; Zhao, J.G.; Yu, P. Efficacy and Safety of Sodium-Glucose Cotransporter 2 Inhibitors in Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials for 1 to 2 years. J. Diabetes Complicat. 2015, 29, 1295–1303. [Google Scholar] [CrossRef]
- Maruthur, N.M.; Tseng, E.; Hutfless, S.; Wilson, L.M.; Suarez-Cuervo, C.; Berger, Z.; Chu, Y.; Iyoha, E.; Segal, J.B.; Bolen, S. Diabetes Medications as Monotherapy or Metformin-Based Combination Therapy for Type 2 Diabetes: A Systematic Review and Meta-Analysis. Ann. Intern. Med. 2016, 164, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Mearns, E.S.; Sobieraj, D.M.; White, C.M.; Saulsberry, W.J.; Kohn, C.G.; Doleh, Y.; Zaccaro, E.; Coleman, C.I. Comparative Efficacy and Safety of Antidiabetic Drug Regimens Added to Metformin Monotherapy in Patients with Type 2 Diabetes: A Network Meta-Analysis. PLoS ONE 2015, 10, e0125879. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Yang, W.; Gao, X.; Chen, Y.; Zhou, L.; Zhang, S.; Han, X.; Ji, L. The Association Between the Dosage of SGLT2 Inhibitor and Weight Reduction in Type 2 Diabetes Patients: A Meta-Analysis. Obesity 2018, 26, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.J.; Gross, J.L.; Hennicken, D.; Iqbal, N.; Mansfield, T.A.; List, J.F. Dapagliflozin Add-on to Metformin in Type 2 Diabetes Inadequately Controlled with Metformin: A Randomized, Double-Blind, Placebo-Controlled 102-Week Trial. BMC Med. 2013, 11, 43. [Google Scholar] [CrossRef]
- Bolinder, J.; Ljunggren, O.; Johansson, L.; Wilding, J.; Langkilde, A.M.; Sjöström, C.D.; Sugg, J.; Parikh, S. Dapagliflozin Maintains Glycaemic Control While Reducing Weight and Body Fat Mass over 2 Years in Patients with Type 2 Diabetes Mellitus Inadequately Controlled on Metformin. Diabetes Obes. Metab. 2014, 16, 159–169. [Google Scholar] [CrossRef]
- Del Prato, S.; Nauck, M.; Durán-Garcia, S.; Maffei, L.; Rohwedder, K.; Theuerkauf, A.; Parikh, S. Long-Term Glycaemic Response and Tolerability of Dapagliflozin versus a Sulphonylurea as Add-on Therapy to Metformin in Patients with Type 2 Diabetes: 4-Year Data. Diabetes Obes. Metab. 2015, 17, 581–590. [Google Scholar] [CrossRef]
- Bays, H.E.; Weinstein, R.; Law, G.; Canovatchel, W. Canagliflozin: Effects in Overweight and Obese Subjects without Diabetes Mellitus. Obesity 2014, 22, 1042–1049. [Google Scholar] [CrossRef]
- Busch, R.S.; Kane, M.P. Combination SGLT2 Inhibitor and GLP-1 Receptor Agonist Therapy: A Complementary Approach to the Treatment of Type 2 Diabetes. Postgrad. Med. 2017, 129, 686–697. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Nagata, N.; Nagashimada, M.; Zhuge, F.; Ni, Y.; Chen, G.; Mayoux, E.; Kaneko, S.; Ota, T. SGLT2 Inhibition by Empagliflozin Promotes Fat Utilization and Browning and Attenuates Inflammation and Insulin Resistance by Polarizing M2 Macrophages in Diet-Induced Obese Mice. EBioMedicine 2017, 20, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Sugizaki, T.; Zhu, S.; Guo, G.; Matsumoto, A.; Zhao, J.; Endo, M.; Horiguchi, H.; Morinaga, J.; Tian, Z.; Kadomatsu, T.; et al. Treatment of Diabetic Mice with the SGLT2 Inhibitor TA-1887 Antagonizes Diabetic Cachexia and Decreases Mortality. NPJ Aging Mech. Dis. 2017, 3, 12. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, A.S.; Obin, M.S. Obesity and the Role of Adipose Tissue in Inflammation and Metabolism. Am. J. Clin. Nutr. 2006, 83, 461S–465S. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 2020, 141, E139–E596. [Google Scholar] [CrossRef]
- Groenewegen, A.; Rutten, F.H.; Mosterd, A.; Hoes, A.W. Epidemiology of Heart Failure. Eur. J. Heart Fail. 2020, 22, 1342–1356. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC)Developed with the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Baumbach, A.; Böhm, M.; Burri, H.; Čelutkiene, J.; Chioncel, O.; Cleland, J.G.F.; Coats, A.J.S.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart FailureDeveloped by the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC) With the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, E254–E743. [Google Scholar] [CrossRef]
- Visco, V.; Esposito, C.; Manzo, M.; Fiorentino, A.; Galasso, G.; Vecchione, C.; Ciccarelli, M. A Multistep Approach to Deal with Advanced Heart Failure: A Case Report on the Positive Effect of Cardiac Contractility Modulation Therapy on Pulmonary Pressure Measured by CardioMEMS. Front. Cardiovasc.Med. 2022, 9, 874433. [Google Scholar] [CrossRef]
- Tsao, C.W.; Lyass, A.; Enserro, D.; Larson, M.G.; Ho, J.E.; Kizer, J.R.; Gottdiener, J.S.; Psaty, B.M.; Vasan, R.S. Temporal Trends in the Incidence of and Mortality Associated with Heart Failure with Preserved and Reduced Ejection Fraction. JACC Heart Fail. 2018, 6, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Straw, S.; McGinlay, M.; Witte, K.K. Four Pillars of Heart Failure: Contemporary Pharmacological Therapy for Heart Failure with Reduced Ejection Fraction. Open Heart 2021, 8, e001585. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Dual Angiotensin Receptor and Neprilysin Inhibition as an Alternative to Angiotensin-Converting Enzyme Inhibition in Patients with Chronic Systolic Heart Failure: Rationale for and Design of the Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure Trial (PARADIGM-HF). Eur. J. Heart Fail. 2013, 15, 1062–1073. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, J.R.; Diaz, R.; Felker, G.M.; McMurray, J.J.V.; Metra, M.; Solomon, S.D.; Adams, K.F.; Anand, I.; Arias-Mendoza, A.; Biering-Sørensen, T.; et al. Cardiac Myosin Activation with Omecamtiv Mecarbil in Systolic Heart Failure. N. Engl. J. Med. 2021, 384, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, P.W.; Pieske, B.; Anstrom, K.J.; Ezekowitz, J.; Hernandez, A.F.; Butler, J.; Lam, C.S.; Ponikowski, P.; Voors, A.A.; Jia, G.; et al. Vericiguat in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2020, 382, 1883–1893. [Google Scholar] [CrossRef]
- Maddox, T.M.; Januzzi, J.L.; Allen, L.A.; Breathett, K.; Butler, J.; Davis, L.L.; Fonarow, G.C.; Ibrahim, N.E.; Lindenfeld, J.A.; Masoudi, F.A.; et al. 2021 Update to the 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure with Reduced Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2021, 77, 772–810. [Google Scholar] [CrossRef]
- Ferrannini, E.; Mark, M.; Mayoux, E. CV Protection in the EMPA-REG OUTCOME Trial: A “Thrifty Substrate” Hypothesis. Diabetes Care 2016, 39, 1108–1114. [Google Scholar] [CrossRef]
- Honka, H.; Solis-Herrera, C.; Triplitt, C.; Norton, L.; Butler, J.; DeFronzo, R.A. Therapeutic Manipulation of Myocardial Metabolism: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 77, 2022–2039. [Google Scholar] [CrossRef]
- Nielsen, R.; Møller, N.; Gormsen, L.C.; Tolbod, L.P.; Hansson, N.H.; Sorensen, J.; Harms, H.J.; Frøkiær, J.; Eiskjaer, H.; Jespersen, N.R.; et al. Cardiovascular Effects of Treatment with the Ketone Body 3-Hydroxybutyrate in Chronic Heart Failure Patients. Circulation 2019, 139, 2129–2141. [Google Scholar] [CrossRef]
- Santos-Gallego, C.G.; Requena-Ibanez, J.A.; San Antonio, R.; Ishikawa, K.; Watanabe, S.; Picatoste, B.; Flores, E.; Garcia-Ropero, A.; Sanz, J.; Hajjar, R.J.; et al. Empagliflozin Ameliorates Adverse Left Ventricular Remodeling in Nondiabetic Heart Failure by Enhancing Myocardial Energetics. J. Am. Coll. Cardiol. 2019, 73, 1931–1944. [Google Scholar] [CrossRef]
- Yurista, S.R.; Silljé, H.H.W.; Oberdorf-Maass, S.U.; Schouten, E.M.; Pavez Giani, M.G.; Hillebrands, J.L.; van Goor, H.; van Veldhuisen, D.J.; de Boer, R.A.; Westenbrink, B.D. Sodium-Glucose Co-Transporter 2 Inhibition with Empagliflozin Improves Cardiac Function in Non-Diabetic Rats with Left Ventricular Dysfunction after Myocardial Infarction. Eur. J. Heart Fail. 2019, 21, 862–873. [Google Scholar] [CrossRef] [PubMed]
- Yurista, S.R.; Matsuura, T.R.; Silljé, H.H.W.; Nijholt, K.T.; McDaid, K.S.; Shewale, S.V.; Leone, T.C.; Newman, J.C.; Verdin, E.; Van Veldhuisen, D.J.; et al. Ketone Ester Treatment Improves Cardiac Function and Reduces Pathologic Remodeling in Preclinical Models of Heart Failure. Circ. Heart Fail. 2021, 14, E007684. [Google Scholar] [CrossRef] [PubMed]
- Lopaschuk, G.D.; Verma, S. Mechanisms of Cardiovascular Benefits of Sodium Glucose Co-Transporter 2 (SGLT2) Inhibitors: A State-of-the-Art Review. JACC Basic. Transl. Sci. 2020, 5, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Polidori, D.; Iijima, H.; Goda, M.; Maruyama, N.; Inagaki, N.; Crawford, P.A. Intra- and Inter-Subject Variability for Increases in Serum Ketone Bodies in Patients with Type 2 Diabetes Treated with the Sodium Glucose Co-Transporter 2 Inhibitor Canagliflozin. Diabetes Obes. Metab. 2018, 20, 1321–1326. [Google Scholar] [CrossRef]
- Yabe, D.; Iwasaki, M.; Kuwata, H.; Haraguchi, T.; Hamamoto, Y.; Kurose, T.; Sumita, K.; Yamazato, H.; Kanada, S.; Seino, Y. Sodium-Glucose Co-Transporter-2 Inhibitor Use and Dietary Carbohydrate Intake in Japanese Individuals with Type 2 Diabetes: A Randomized, Open-Label, 3-Arm Parallel Comparative, Exploratory Study. Diabetes Obes. Metab. 2017, 19, 739–743. [Google Scholar] [CrossRef]
- Verma, S.; Rawat, S.; Ho, K.L.; Wagg, C.S.; Zhang, L.; Teoh, H.; Dyck, J.E.; Uddin, G.M.; Oudit, G.Y.; Mayoux, E.; et al. Empagliflozin Increases Cardiac Energy Production in Diabetes: Novel Translational Insights into the Heart Failure Benefits of SGLT2 Inhibitors. JACC Basic. Transl. Sci. 2018, 3, 575–587. [Google Scholar] [CrossRef]
- Ekanayake, P.; Hupfeld, C.; Mudaliar, S. Sodium-Glucose Cotransporter Type 2 (SGLT-2) Inhibitors and Ketogenesis: The Good and the Bad. Curr. Diab Rep. 2020, 20, 74. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Perry, R.J.; Shulman, G.I. Sodium-Glucose Cotransporter-2 Inhibitors: Understanding the Mechanisms for Therapeutic Promise and Persisting Risks. J. Biol. Chem. 2020, 295, 14379–14390. [Google Scholar] [CrossRef]
- Saucedo-Orozco, H.; Voorrips, S.N.; de Boer, R.A.; Westenbrink, B.D.; Yurista, S.R. SGLT2 Inhibitors and Ketone Metabolism in Heart Failure. J. Lipid Atheroscler. 2022, 11, 1–19. [Google Scholar] [CrossRef]
- Manolis, A.S.; Manolis, T.A.; Manolis, A.A. Ketone Bodies and Cardiovascular Disease: An Alternate Fuel Source to the Rescue. Int. J. Mol.Sci. 2023, 24, 3534. [Google Scholar] [CrossRef] [PubMed]
- Palmiero, G.; Cesaro, A.; Vetrano, E.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Moscarella, E.; Gragnano, F.; Salvatore, T.; Rinaldi, L.; et al. Impact of SGLT2 Inhibitors on Heart Failure: From Pathophysiology to Clinical Effects. Int. J. Mol. Sci. 2021, 22, 5863. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Garg, A.; Yan, A.T.; Gupta, A.K.; Al-Omran, M.; Sabongui, A.; Teoh, H.; Mazer, C.D.; Connelly, K.A. Effect of Empagliflozin on Left Ventricular Mass and Diastolic Function in Individuals with Diabetes: An Important Clue to the EMPA-REG OUTCOME Trial? Diabetes Care 2016, 39, e212–e213. [Google Scholar] [CrossRef] [PubMed]
- Cohen, N.D.; Gutman, S.J.; Briganti, E.M.; Taylor, A.J. Effects of Empagliflozin Treatment on Cardiac Function and Structure in Patients with Type 2 Diabetes: A Cardiac Magnetic Resonance Study. Intern. Med. J. 2019, 49, 1006–1010. [Google Scholar] [CrossRef] [PubMed]
- Lan, N.S.R.; Fegan, P.G.; Yeap, B.B.; Dwivedi, G. The Effects of Sodium-Glucose Cotransporter 2 Inhibitors on Left Ventricular Function: Current Evidence and Future Directions. ESC Heart Fail. 2019, 6, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Di Franco, A.; Cantini, G.; Tani, A.; Coppini, R.; Zecchi-Orlandini, S.; Raimondi, L.; Luconi, M.; Mannucci, E. Sodium-Dependent Glucose Transporters (SGLT) in Human Ischemic Heart: A New Potential Pharmacological Target. Int. J. Cardiol. 2017, 243, 86–90. [Google Scholar] [CrossRef]
- Cowie, M.R.; Fisher, M. SGLT2 Inhibitors: Mechanisms of Cardiovascular Benefit beyond Glycaemic Control. Nat. Rev. Cardiol. 2020, 17, 761–772. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Wiviott, S.D.; Raz, I.; Im, K.; Goodrich, E.L.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Furtado, R.H.M.; et al. SGLT2 Inhibitors for Primary and Secondary Prevention of Cardiovascular and Renal Outcomes in Type 2 Diabetes: A Systematic Review and Meta-Analysis of Cardiovascular Outcome Trials. Lancet 2019, 393, 31–39. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on Diabetes, Pre-Diabetes, and Cardiovascular Diseases Developed in Collaboration with the EASDThe Task Force for Diabetes, Pre-Diabetes, and Cardiovascular Diseases of the European Society of Cardiology (ESC) and the European Association for the Study of Diabetes (EASD). Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef]
- Sattar, N.; McLaren, J.; Kristensen, S.L.; Preiss, D.; McMurray, J.J. SGLT2 Inhibition and Cardiovascular Events: Why Did EMPA-REG Outcomes Surprise and What Were the Likely Mechanisms? Diabetologia 2016, 59, 1333–1339. [Google Scholar] [CrossRef]
- Xie, M.; Hill, J.A. HDAC-Dependent Ventricular Remodeling. Trends Cardiovasc. Med. 2013, 23, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.; Tannous, P.; Lu, G.; Berenji, K.; Rothermel, B.A.; Olson, E.N.; Hill, J.A. Suppression of Class I and II Histone Deacetylases Blunts Pressure-Overload Cardiac Hypertrophy. Circulation 2006, 113, 2579–2588. [Google Scholar] [CrossRef] [PubMed]
- Shimazu, T.; Hirschey, M.D.; Newman, J.; He, W.; Shirakawa, K.; Le Moan, N.; Grueter, C.A.; Lim, H.; Saunders, L.R.; Stevens, R.D.; et al. Suppression of Oxidative Stress by β-Hydroxybutyrate, an Endogenous Histone Deacetylase Inhibitor. Science 2013, 339, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Uchihashi, M.; Hoshino, A.; Okawa, Y.; Ariyoshi, M.; Kaimoto, S.; Tateishi, S.; Ono, K.; Yamanaka, R.; Hato, D.; Fushimura, Y.; et al. Cardiac-Specific Bdh1 Overexpression Ameliorates Oxidative Stress and Cardiac Remodeling in Pressure Overload-Induced Heart Failure. Circ. Heart Fail. 2017, 10, e004417. [Google Scholar] [CrossRef] [PubMed]
- Schugar, R.C.; Moll, A.R.; André d’Avignon, D.; Weinheimer, C.J.; Kovacs, A.; Crawford, P.A. Cardiomyocyte-Specific Deficiency of Ketone Body Metabolism Promotes Accelerated Pathological Remodeling. Mol. Metab. 2014, 3, 754–769. [Google Scholar] [CrossRef]
- Nassif, M.E.; Windsor, S.; Tang, F.; Khariton, Y.; Husain, M.; Inzucchi, S.; McGuire, D.; Pitt, B.; Scirica, B.; Austin, B.; et al. Dapagliflozin Effects on Biomarkers, Symptoms, and Functional Status in Patients with Heart Failure with Reduced Ejection Fraction. Circulation 2019, 140, 042929. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Zinman, B.; Wanner, C.; Ferrari, R.; Fitchett, D.; Hantel, S.; Espadero, R.M.; Woerle, H.J.; Broedl, U.C.; Johansen, O.E. SGLT-2 Inhibitors and Cardiovascular Risk: Proposed Pathways and Review of Ongoing Outcome Trials. Diabetes Vasc. Dis. Res. 2015, 12, 90–100. [Google Scholar] [CrossRef]
- Cannon, C.P.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; et al. Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes. N. Engl. J. Med. 2020, 383, 1425–1435. [Google Scholar] [CrossRef]
- Kim, S.R.; Lee, S.G.; Kim, S.H.; Kim, J.H.; Choi, E.; Cho, W.; Rim, J.H.; Hwang, I.; Lee, C.J.; Lee, M.; et al. SGLT2 Inhibition Modulates NLRP3 Inflammasome Activity via Ketones and Insulin in Diabetes with Cardiovascular Disease. Nat. Commun. 2020, 11, 2127. [Google Scholar] [CrossRef]
- Packer, M. Role of Ketogenic Starvation Sensors in Mediating the Renal Protective Effects of SGLT2 Inhibitors in Type 2 Diabetes. J. Diabetes Complicat. 2020, 34, 107647. [Google Scholar] [CrossRef]
- Nirengi, S.; Peres Valgas da Silva, C.; Stanford, K.I. Disruption of Energy Utilization in Diabetic Cardiomyopathy; a Mini Review. Curr. Opin. Pharmacol. 2020, 54, 82–90. [Google Scholar] [CrossRef]
- Bragagni, A.; Piani, F.; Borghi, C. Surprises in Cardiology: Efficacy of Gliflozines in Heart Failure Even in the Absence of Diabetes. Eur. Heart J. Suppl. 2021, 23, E40. [Google Scholar] [CrossRef]
- Prosperi, S.; D’Amato, A.; Severino, P.; Myftari, V.; Monosilio, S.; Marchiori, L.; Zagordi, L.M.; Filomena, D.; Di Pietro, G.; Birtolo, L.I.; et al. Sizing SGLT2 Inhibitors Up: From a Molecular to a Morpho-Functional Point of View. Int. J. Mol. Sci. 2023, 24, 13848. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; et al. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N. Engl. J. Med. 2021, 384, 117–128. [Google Scholar] [CrossRef]
- Abraham, W.T.; Lindenfeld, J.A.; Ponikowski, P.; Agostoni, P.; Butler, J.; Desai, A.S.; Filippatos, G.; Gniot, J.; Fu, M.; Gullestad, L.; et al. Effect of Empagliflozin on Exercise Ability and Symptoms in Heart Failure Patients with Reduced and Preserved Ejection Fraction, with and without Type 2 Diabetes. Eur. Heart J. 2021, 42, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.-F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- Pollock, C.; Stefánsson, B.; Reyner, D.; Rossing, P.; Sjöström, C.D.; Wheeler, D.C.; Langkilde, A.M.; Heerspink, H.J.L. Albuminuria-Lowering Effect of Dapagliflozin Alone and in Combination with Saxagliptin and Effect of Dapagliflozin and Saxagliptin on Glycaemic Control in Patients with Type 2 Diabetes and Chronic Kidney Disease (DELIGHT): A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet Diabetes Endocrinol. 2019, 7, 429–441. [Google Scholar] [CrossRef]
- Fioretto, P.; Del Prato, S.; Buse, J.B.; Goldenberg, R.; Giorgino, F.; Reyner, D.; Langkilde, A.M.; Sjöström, C.D.; Sartipy, P. Efficacy and Safety of Dapagliflozin in Patients with Type 2 Diabetes and Moderate Renal Impairment (Chronic Kidney Disease Stage 3A): The DERIVE Study. Diabetes Obes. Metab. 2018, 20, 2532–2540. [Google Scholar] [CrossRef]
- Cherney, D.Z.I.; Dekkers, C.C.J.; Barbour, S.J.; Cattran, D.; Abdul Gafor, A.H.; Greasley, P.J.; Laverman, G.D.; Lim, S.K.; Di Tanna, G.L.; Reich, H.N.; et al. Effects of the SGLT2 Inhibitor Dapagliflozin on Proteinuria in Non-Diabetic Patients with Chronic Kidney Disease (DIAMOND): A Randomised, Double-Blind, Crossover Trial. Lancet Diabetes Endocrinol. 2020, 8, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Committee, A.D.A.P.P. 11. Chronic Kidney Disease and Risk Management: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45, S175–S184. [Google Scholar] [CrossRef]
- Tomah, S.; Alkhouri, N.; Hamdy, O. Nonalcoholic Fatty Liver Disease and Type 2 Diabetes: Where Do Diabetologists Stand? Clin. Diabetes Endocrinol. 2020, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The Global Epidemiology of NAFLD and NASH in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease-Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Byrne, C.D.; Targher, G. NAFLD: A Multisystem Disease. J. Hepatol. 2015, 62, S47–S64. [Google Scholar] [CrossRef]
- Yabiku, K. Efficacy of Sodium-Glucose Cotransporter 2 Inhibitors in Patients with Concurrent Type 2 Diabetes Mellitus and Non-Alcoholic Steatohepatitis: A Review of the Evidence. Front. Endocrinol. 2021, 12, 768850. [Google Scholar] [CrossRef]
- Mooli, R.G.R.; Ramakrishnan, S.K. Emerging Role of Hepatic Ketogenesis in Fatty Liver Disease. Front. Physiol. 2022, 13, 1300. [Google Scholar] [CrossRef] [PubMed]
- Osataphan, S.; Macchi, C.; Singhal, G.; Chimene-Weiss, J.; Sales, V.; Kozuka, C.; Dreyfuss, J.M.; Pan, H.; Tangcharoenpaisan, Y.; Morningstar, J.; et al. SGLT2 Inhibition Reprograms Systemic Metabolism via FGF21-Dependent and -Independent Mechanisms. JCI Insight 2019, 4, e123130. [Google Scholar] [CrossRef]
- Coelho, F.d.S.; Borges-Canha, M.; von Hafe, M.; Neves, J.S.; Vale, C.; Leite, A.R.; Carvalho, D.; Leite-Moreira, A. Effects of sodium-glucose co-transporter 2 inhibitors on liver parameters and steatosis: A meta-analysis of randomized clinical trials. Diabetes/Metabolism Res. Rev. 2021, 37, e3413. [Google Scholar] [CrossRef]
- Green, C.J.; Pramfalk, C.; Charlton, C.A.; Gunn, P.J.; Cornfield, T.; Pavlides, M.; Karpe, F.; Hodson, L. Hepatic de Novo Lipogenesis Is Suppressed and Fat Oxidation Is Increased by Omega-3 Fatty Acids at the Expense of Glucose Metabolism. BMJ Open Diabetes Res. Care 2020, 8, e000871. [Google Scholar] [CrossRef] [PubMed]
- Wree, A.; McGeough, M.D.; Peña, C.A.; Schlattjan, M.; Li, H.; Inzaugarat, M.E.; Messer, K.; Canbay, A.; Hoffman, H.M.; Feldstein, A.E. NLRP3 Inflammasome Activation Is Required for Fibrosis Development in NAFLD. J. Mol. Med. 2014, 92, 1069–1082. [Google Scholar] [CrossRef] [PubMed]
- Kleinert, M.; Müller, T.D. A New FGF21 Analog for the Treatment of Fatty Liver Disease. Diabetes 2020, 69, 1605–1607. [Google Scholar] [CrossRef] [PubMed]
- Post, A.; Garcia, E.; van den Berg, E.H.; Flores-Guerrero, J.L.; Gruppen, E.G.; Groothof, D.; Westenbrink, B.D.; Connelly, M.A.; Bakker, S.J.L.; Dullaart, R.P.F. Nonalcoholic Fatty Liver Disease, Circulating Ketone Bodies and All-Cause Mortality in a General Population-Based Cohort. Eur. J. Clin. Investig. 2021, 51, e13627. [Google Scholar] [CrossRef] [PubMed]
- Jojima, T.; Tomotsune, T.; Iijima, T.; Akimoto, K.; Suzuki, K.; Aso, Y. Empagliflozin (an SGLT2 Inhibitor), Alone or in Combination with Linagliptin (a DPP-4 Inhibitor), Prevents Steatohepatitis in a Novel Mouse Model of Non-Alcoholic Steatohepatitis and Diabetes. Diabetol. Metab. Syndr. 2016, 8, 45. [Google Scholar] [CrossRef] [PubMed]
- Nakano, S.; Katsuno, K.; Isaji, M.; Nagasawa, T.; Buehrer, B.; Walker, S.; Wilkison, W.O.; Cheatham, B. Remogliflozin Etabonate Improves Fatty Liver Disease in Diet-Induced Obese Male Mice. J. Clin. Exp. Hepatol. 2015, 5, 190. [Google Scholar] [CrossRef]
- Yabiku, K.; Nakamoto, K.; Tsubakimoto, M. Effects of Sodium-Glucose Cotransporter 2 Inhibition on Glucose Metabolism, Liver Function, Ascites, and Hemodynamics in a Mouse Model of Nonalcoholic Steatohepatitis and Type 2 Diabetes. J. Diabetes Res. 2020, 2020, 168290. [Google Scholar] [CrossRef]
- Tanase, D.M.; Gosav, E.M.; Costea, C.F.; Ciocoiu, M.; Lacatusu, C.M.; Maranduca, M.A.; Ouatu, A.; Floria, M. The Intricate Relationship between Type 2 Diabetes Mellitus (T2DM), Insulin Resistance (IR), and Nonalcoholic Fatty Liver Disease (NAFLD). J. Diabetes Res. 2020, 2020, 3920196. [Google Scholar] [CrossRef]
- Takeda, A.; Irahara, A.; Nakano, A.; Takata, E.; Koketsu, Y.; Kimata, K.; Senda, E.; Yamada, H.; Ichikawa, K.; Fujimori, T.; et al. The Improvement of the Hepatic Histological Findings in a Patient with Non-Alcoholic Steatohepatitis with Type 2 Diabetes after the Administration of the Sodium-Glucose Cotransporter 2 Inhibitor Ipragliflozin. Intern. Med. 2017, 56, 2739. [Google Scholar] [CrossRef]
- Raj, H.; Durgia, H.; Palui, R.; Kamalanathan, S.; Selvarajan, S.; Kar, S.S.; Sahoo, J. SGLT-2 Inhibitors in Non-Alcoholic Fatty Liver Disease Patients with Type 2 Diabetes Mellitus: A Systematic Review. World J. Diabetes 2019, 10, 114. [Google Scholar] [CrossRef]
- Ito, D.; Shimizu, S.; Inoue, K.; Saito, D.; Yanagisawa, M.; Inukai, K.; Akiyama, Y.; Morimoto, Y.; Noda, M.; Shimada, A. Comparison of Ipragliflozin and Pioglitazone Effects on Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes: A Randomized, 24-Week, Open-Label, Active-Controlled Trial. Diabetes Care 2017, 40, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.W.; Lundkvist, P.; Jansson, P.A.; Johansson, L.; Kvarnström, M.; Moris, L.; Miliotis, T.; Forsberg, G.B.; Risérus, U.; Lind, L.; et al. Effects of Dapagliflozin and N-3 Carboxylic Acids on Non-Alcoholic Fatty Liver Disease in People with Type 2 Diabetes: A Double-Blind Randomised Placebo-Controlled Study. Diabetologia 2018, 61, 1923. [Google Scholar] [CrossRef] [PubMed]
- Zughaib, M.T.; Patel, K.; Leka, M.; Affas, S. Self-Induced Euglycemic Diabetic Ketoacidosis: When to Stop the Drip. Cureus 2022, 14, e21768. [Google Scholar] [CrossRef]
- Bonora, B.M.; Avogaro, A.; Fadini, G.P. Sodium-Glucose Co-Transporter-2 Inhibitors and Diabetic Ketoacidosis: An Updated Review of the Literature. Diabetes Obes. Metab. 2018, 20, 25–33. [Google Scholar] [CrossRef]
- Mahfooz, R.S.; Khan, M.K.; Al Hennawi, H.; Khedr, A. SGLT-2 Inhibitor-Associated Euglycemic Diabetic Ketoacidosis: A Case Report and a Literature Review. Cureus 2022, 14, e26267. [Google Scholar] [CrossRef] [PubMed]
- Farxiga (Dapagliflozin): Side Effects, Dosage, Uses, and More. Available online: https://www.medicalnewstoday.com/articles/326257#What-is-Farxiga? (accessed on 23 May 2023).
- Liu, C.; Wu, D.; Zheng, X.; Li, P.; Li, L. Efficacy and Safety of Metformin for Patients with Type 1 Diabetes Mellitus: A Meta-Analysis. Diabetes Technol. Ther. 2015, 17, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Voss, E.A.; Weaver, J.; Hester, L.; Yuan, Z.; DeFalco, F.; Schuemie, M.J.; Ryan, P.B.; Sun, D.; Freedman, A.; et al. Diabetic Ketoacidosis in Patients with Type 2 Diabetes Treated with Sodium Glucose Co-Transporter 2 Inhibitors versus Other Antihyperglycemic Agents: An Observational Study of Four US Administrative Claims Databases. Pharmacoepidemiol. Drug Saf. 2019, 28, 1620–1628. [Google Scholar] [CrossRef]
- Davidson, J.A.; Kuritzky, L. Sodium Glucose Co-Transporter 2 Inhibitors and Their Mechanism for Improving Glycemia in Patients with Type 2 Diabetes. Postgrad. Med. 2014, 126, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Desai, M.; Ryan, P.B.; DeFalco, F.J.; Schuemie, M.J.; Stang, P.E.; Berlin, J.A.; Yuan, Z. Incidence of Diabetic Ketoacidosis among Patients with Type 2 Diabetes Mellitus Treated with SGLT2 Inhibitors and Other Antihyperglycemic Agents. Diabetes Res. Clin. Pract. 2017, 128, 83–90. [Google Scholar] [CrossRef]
- Kim, Y.G.; Jeon, J.Y.; Han, S.J.; Kim, D.J.; Lee, K.W.; Kim, H.J. Sodium-Glucose Co-Transporter-2 Inhibitors and the Risk of Ketoacidosis in Patients with Type 2 Diabetes Mellitus: A Nationwide Population-Based Cohort Study. Diabetes Obes. Metab. 2018, 20, 1852–1858. [Google Scholar] [CrossRef]
- D’Andrea, E.; Wexler, D.J.; Kim, S.C.; Paik, J.M.; Alt, E.; Patorno, E. Comparing Effectiveness and Safety of SGLT2 Inhibitors vs DPP-4 Inhibitors in Patients with Type 2 Diabetes and Varying Baseline HbA1c Levels. JAMA Intern. Med. 2023, 183, 242–254. [Google Scholar] [CrossRef] [PubMed]
- The EMPA-KIDNEY Collaborative Group. Empagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2023, 388, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Zelniker, T.A.; Braunwald, E. Mechanisms of Cardiorenal Effects of Sodium-Glucose Cotransporter 2 Inhibitors: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Inzucchi, S.E.; Iliev, H.; Pfarr, E.; Zinman, B. Empagliflozin and Assessment of Lower-Limb Amputations in the EMPA-REG OUTCOME Trial. Diabetes Care 2018, 41, e4–e5. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Jiang, Z.; Wei, Y. Efficacy and Safety of the SGLT2 Inhibitor Dapagliflozin in Type 1 Diabetes: A Meta-Analysis of Randomized Controlled Trials. Exp. Ther. Med. 2021, 21, 382. [Google Scholar] [CrossRef] [PubMed]
- Laursen, H.V.B.; Røikjer, J.B.; Dal, J.; Jensen, M.H. Sodium Glucose Cotransporter-2 Inhibitor Treatment and the Risk of Diabetic Ketoacidosis in Denmark: A Retrospective Cohort Study of Five Years of Use. Curr. Drug Saf. 2021, 16, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Janssens, B.; Caerels, S.; Mathieu, C. SGLT Inhibitors in Type 1 Diabetes: Weighing Efficacy and Side Effects. Ther. Adv. Endocrinol. Metab. 2020, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Burke, K.R.; Schumacher, C.A.; Harpe, S.E. SGLT2 Inhibitors: A Systematic Review of Diabetic Ketoacidosis and Related Risk Factors in the Primary Literature. Pharmacotherapy 2017, 37, 187–194. [Google Scholar] [CrossRef]
- Kaneto, H.; Obata, A.; Kimura, T.; Shimoda, M.; Kinoshita, T.; Matsuoka, T.A.; Kaku, K. Unexpected Pleiotropic Effects of SGLT2 Inhibitors: Pearls and Pitfalls of This Novel Antidiabetic Class. Int. J. Mol. Sci. 2021, 22, 3062. [Google Scholar] [CrossRef]
- Lytvyn, Y.; Bjornstad, P.; Udell, J.A.; Lovshin, J.A.; Cherney, D.Z.I. Sodium Glucose Cotransporter-2 Inhibition in Heart Failure. Circulation 2017, 136, 1643–1658. [Google Scholar] [CrossRef]
- Dekkers, C.C.J.; Sjöström, C.D.; Greasley, P.J.; Cain, V.; Boulton, D.W.; Heerspink, H.J.L. Effects of the Sodium-glucose Co-transporter-2 Inhibitor Dapagliflozin on Estimated Plasma Volume in Patients with Type 2 Diabetes. Diabetes Obes. Metab. 2019, 21, 2667. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, D.; Longo, M.; Scappaticcio, L.; Bellastella, G.; Maiorino, M.I.; Esposito, K. SGLT-2 Inhibitors and Cardiorenal Outcomes in Patients with or without Type 2 Diabetes: A Meta-Analysis of 11 CVOTs. Cardiovasc. Diabetol. 2021, 20, 236. [Google Scholar] [CrossRef] [PubMed]
- Yau, K.; Dharia, A.; Alrowiyti, I.; Cherney, D.Z.I. Prescribing SGLT2 Inhibitors in Patients With CKD: Expanding Indications and Practical Considerations. Kidney Int. Rep. 2022, 7, 1463. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Vellipuram, A.R.; Bandaru, S.S.; Raj, J.P. Euglycemic Diabetic Ketoacidosis: A Diagnostic and Therapeutic Dilemma. Endocrinol. Diabetes Metab. Case Rep. 2017, 2017, 17-0081. [Google Scholar] [CrossRef]
- Earle, M.; Ault, B.; Bonney, C. Euglycemic Diabetic Ketoacidosis in Concurrent Very Low-Carbohydrate Diet and Sodium-Glucose Transporter-2 Inhibitor Use: A Case Report. Clin. Pract. Cases Emerg. Med. 2020, 4, 185. [Google Scholar] [CrossRef]




| SGLT-2 Inhibitors | Ketogenic Diets | |
|---|---|---|
| Characteristics | A class of drugs used to treat T2DM by blocking glucose reabsorption in the kidneys, which leads to increased urinary glucose excretion. | A low-carbohydrate, high-fat diet that forces the body to burn fat for energy instead of carbohydrates. This metabolic state is known as ketosis. |
| Advantages of Synergy | Improved glycemic control → both lower blood glucose levels, and their combined effect can lead to better glycemic control. Weight loss → a ketogenic diet can lead to significant weight loss, and SGLT-2 inhibitors have been shown to reduce body weight and body fat. Cardiovascular benefits → SGLT-2 inhibitors reduce the risk of cardiovascular events in people with type 2 diabetes, and a ketogenic diet may also improve cardiovascular health. Blood pressure reduction→ both have been shown to reduce BP. Lowered inflammation → a ketogenic diet may reduce inflammation in the body, and SGLT-2 inhibitors have been shown to have anti-inflammatory effects. Neuroprotective effects → a ketogenic diet has been shown to have neuroprotective effects, and SGLT-2 inhibitors may also have neuroprotective effects. | |
| Disadvantages of Synergy | Diabetic ketoacidosis → both SGLT-2 inhibitors and a ketogenic diet increase the risk of DKA in people with T1DM Dehydration → SGLT-2 inhibitors increase urinary glucose excretion, which can lead to dehydration, whereas a ketogenic diet can also lead to dehydration if not properly balanced with adequate fluid and electrolyte intake. Electrolyte imbalance → SGLT-2 inhibitors increase the urinary excretion of Na+ and K+, which can lead to electrolyte imbalances. A ketogenic diet can also affect electrolyte balance if not properly balanced with an adequate intake of Na+, K+, and Mg2+. Hypoglycemia → a ketogenic diet can lead to hypoglycemia in people with type 2 diabetes who are taking medications that lower blood glucose levels, such as insulin or sulfonylureas. SGLT-2 inhibitors can also increase the risk of hypoglycemia when used in combination with other glucose-lowering medications. Gastrointestinal symptoms → a ketogenic diet can cause gastrointestinal symptoms such as nausea, vomiting, and diarrhea. SGLT-2 inhibitors can cause gastrointestinal symptoms such as nausea and diarrhea. Genital infections → SGLT-2 inhibitors can increase the risk of genital infections such as yeast infections and UTIs. A ketogenic diet may also increase the risk of yeast infections due to the high-fat content. | |
| Clinical Trial | Type of Trial | Study Information | Duration | Outcomes |
|---|---|---|---|---|
| DECLARE-TIMI 58 [163] | Double-blind, placebo-controlled RCT (phase 3) | 17,160 T2DM patients at high risk for CV events (only 7% of patients had an eGFR < 60 mL/min/1.73 m2) Dapagliflozin 10 mg vs. placebo | Up to 6 years | Cardiovascular death, nonfatal MI, nonfatal ischemic stroke; cardiovascular death, hospitalization because of HF Renal composite end point (≥40% decrease in eGFR to <60 and ESRD and renal or cardiovascular death, all-cause mortality) |
| DAPA-HF [9] | Double-blind, placebo-controlled RCT (phase 3) | 4304 diabetic (68%) or non-diabetic patients with class II-IV HF Dapagliflozin 10 mg vs. placebo | 36 months | Time to cardiovascular death or hospitalization for HF or an urgent HF visit Time to ≥50% sustained decline in eGFR or ESRD QoL score by questionnaire Time to death by any cause |
| DEFINE HF [181] | Double-blind, placebo-controlled RCT (phase 4) | 263 diabetic or nondiabetic patients with class II and III HF Dapagliflozin 10 mg vs. placebo | 12 weeks | Change in NTproBNP Change in SBP, weight, HbA1c, BNP, and QoL score by questionnaire |
| EMPA-REG OUTCOME [8] | Double-blind, placebo-controlled RCT (phase 3) | 7020 T2DM patients at high risk for CV events and an eGFR ≥ 30 mL/min/1.73 m2 Empagliflozin 10 mg vs. Empagliflozin 25 mg vs. placebo | Up to 4.6 years | 14% reduction in 3-point MACE (cardiovascular death, nonfatal MI, nonfatal stroke) pooled from 10 mg and 25 mg empagliflozin doses 35% reduction in hospitalization for HF, 39% reduction in the composite renal end point (new macroalbuminuria, doubling of serum creatinine and a GFR ≤ 45, renal replacement therapy, renal death) |
| EMPEROR-Reduced [10] | Double-blind, placebo-controlled RCT (phase 3) | 3730 diabetic or non-diabetic patients with class II, III, or IV HF and an EF ≤ 40% Empagliflozin 10 mg vs. placebo (additionally to recommended treatment) | 38 months | Cardiovascular death or adjudicated hospitalization for HF Change in eGFR Time to sustained reduction in eGFR Time to all-cause mortality Time to DM. |
| EMPEROR-Preserved [11] | Double-blind, placebo-controlled RCT (phase 3) | 5988 diabetic or not diabetic patients with class II-IV HF and EF > 40% Empagliflozin 10 mg vs. placebo (in addition to usual therapy) | 38 months | Cardiovascular death or adjudicated hospitalization for HF Change in eGFR Time to sustained reduction in eGFR Time to all-cause mortality Time to DM. |
| CANVAS [182] | Double-blind, placebo-controlled RCT (phase 3) | 10,142 participants with T2DM and high CV risk Canagliflozin 100 mg (with an increase to 300 mg) vs. placebo | 3.6 years | 14% reduction in 3-point MACE (cardiovascular death, nonfatal MI, nonfatal stroke) 27% reduction in progression of albuminuria, 70% increase in regression of albuminuria, 40% reduction in the composite renal end point (40% reduction in eGFR, renal replacement therapy, renal death) |
| CREDENCE [183] | Double-blind, placebo-controlled RCT (phase 3) | 3627 T2DM patients with stage 2 or 3 CKD and macroalbuminuria and on ACEIs/ARB (>30 y) Canagliflozin 100 mg daily vs placebo | 4 years | ESRD, S-creatinine doubling, renal/cardiovascular death Cardiovascular death, nonfatal MI, nonfatal stroke, hospitalized UAP, hospitalized CHF, composite renal end point (ESRD, doubling of serum creatinine renal death) |
| VERTIS CV [184] | Double-blind, placebo-controlled RCT (phase 3) | 8246 T2DM patients with established CV disease and an eGFR ≥ 30 mL/min/ 1.73 m2 Ertugliflozin 5 or 15 mg vs. placebo | Up to 6 years | Cardiovascular death, nonfatal MI, nonfatal stroke Cardiovascular death, nonfatal MI, nonfatal stroke and hospitalized UAP |
| Drug | Clinical Trial | Type of Trial | Study Information | Outcomes |
| Dapagliflozin | DECLARE-TIMI 58 [163] | Double-blind, placebo-controlled RCT | 7160 T2DM patients at high risk for CV events (only 7% with eGFR < 60 mL/min/1.73 m2) Dapagliflozin 10 mg vs. placebo | Composite of ≥40% reduction in eGFR, new ESRD, or death from renal or CV causes |
| DAPA-CKD [193] | Double-blind, placebo-controlled RCT | 4304 diabetic (68%) or non-diabetic patients suffering from CKD (UACR of 200–5000 mg/g and eGFR of 25–75 mL/min/1.73 m2) Dapagliflozin 10 mg vs. placebo | Composite of ≥50% sustained decline in eGFR or ESRD or CV or renal death Composite of CV death and hospitalization for heart failure Variation in albumin-to-creatinine ratio | |
| DELIGHT [194] | Placebo-controlled RCT | 461 T2DM patients with albuminuria (UACR 30–3500 mg/g) and eGFR of 25–75 mL/min/1.73 m2, treated with ACEIs or ARBs Dapagliflozin 10 mg vs. Dapagliflozin 10 mg Saxagliptin 2.5 mg vs. placebo | ||
| DERIVE [195] | Double-blind, placebo-controlled RCT Randomized-double blind, cross-over trial | 321 T2DM patients with CKD in stage 3A (eGFR of 45–59 mL/min/1.73 m2) Dapagliflozin 10 mg vs. placebo | Change from baseline in urine eGFR | |
| DIAMOND [196] | 53 nondiabetic patients with CKD (24 h urinary protein excretion > 500 mg and ≤3500 mg, eGFR ≥ 25 mL/min/1.73 m2) on stable RAS blockade 27 received Dapagliflozin 10 mg then placebo, 26 received placebo then Dapagliflozin 10 mg | Mean proteinuria Measured GFR | ||
| Empagliflozin | EMPA-REG OUTCOME [8] | Double-blind, placebo-controlled RCT | 7020 T2DM patients with high risk for CV events and eGFR ≥ 30 mL/min/1.73 m2 Empagliflozin 10 mg vs. placebo Empagliflozin 25 mg vs. placebo | Incident or worsening nephropathy Progression to macroalbuminuria Doubling of the serum creatinine level Initiation of renal-replacement therapy Post hoc composite of doubling of serum creatinine, renal replacement therapy, or death for renal causes Incident albuminuria |
| Canagliflozin | CANVAS [182] CREDENCE [190] | Double-blind, placebo-controlled RCT Double-blind, placebo-controlled RCT | 5812 T2DM patients with high risk for CV events and eGFR > 30 mL/min/1.73 m2 Canagliflozin 100 or 300 mg vs. placebo 4401 T2DM patients with albuminuric CKD (eGFR of 30 to < 90 mL/min/1.73 m2) Canagliflozin 100 mg vs. placebo | Lower progression of albuminuria Composite of 40% reduction in eGFR, renal replacement therapy, or death from renal causes Composite of ESRD (dialysis, transplantation, or sustained eGFR < 15 mL/min/1.73 m2), Doubling of serum creatinine or death from renal or CV causes Composite of ESRD, a doubling of the creatinine level, or death from renal causes Composite of cardiovascular death, myocardial infarction, or stroke |
| Ertugliflozin | VERTIS CV [184] | Double-blind, placebo-controlled RCT | 8246 T2DM patients with established CV disease and eGFR ≥ 30 mL/min/1.73 m2 Ertugliflozin 5 or 15 mg vs. placebo | Composite of death from renal causes, renal replacement therapy, or doubling of serum creatinine |
| Anti-Diabetic Agent | Mechanism of Action | Ketogenic Potential |
|---|---|---|
| SGLT-2 Inhibitors | Inhibit glucose reabsorption in the kidney, leading to increased urinary glucose excretion | Promote mild ketogenesis due to increased free fatty acid availability and decreased insulin secretion |
| Metformin | Decreases hepatic glucose production and improves insulin sensitivity | Low potential → Does not promote ketogenesis |
| Sulfonylureas | Stimulate insulin secretion from β cells in the pancreas | Low potential → Does not promote ketogenesis |
| DPP-4 Inhibitors | Inhibit the enzyme DPP-4, which breaks down incretin hormones that stimulate insulin secretion | Low potential → Does not promote ketogenesis |
| GLP-1 Receptor Agonists | Mimic the action of GLP-1, an incretin hormone that stimulates insulin secretion and decreases glucagon secretion | Low potential → Does not promote ketogenesis |
| Insulin | Facilitates glucose uptake by cells and decreases hepatic glucose production | Low potential → Does not promote ketogenesis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koutentakis, M.; Kuciński, J.; Świeczkowski, D.; Surma, S.; Filipiak, K.J.; Gąsecka, A. The Ketogenic Effect of SGLT-2 Inhibitors—Beneficial or Harmful? J. Cardiovasc. Dev. Dis. 2023, 10, 465. https://doi.org/10.3390/jcdd10110465
Koutentakis M, Kuciński J, Świeczkowski D, Surma S, Filipiak KJ, Gąsecka A. The Ketogenic Effect of SGLT-2 Inhibitors—Beneficial or Harmful? Journal of Cardiovascular Development and Disease. 2023; 10(11):465. https://doi.org/10.3390/jcdd10110465
Chicago/Turabian StyleKoutentakis, Michail, Jakub Kuciński, Damian Świeczkowski, Stanisław Surma, Krzysztof J. Filipiak, and Aleksandra Gąsecka. 2023. "The Ketogenic Effect of SGLT-2 Inhibitors—Beneficial or Harmful?" Journal of Cardiovascular Development and Disease 10, no. 11: 465. https://doi.org/10.3390/jcdd10110465