

Sepsis Management in the Cardiac Intensive Care Unit

Abstract
:1. Introduction
2. Epidemiology and Definitions
3. Pathophysiology of Cardiogenic and Septic Shock
4. Hemodynamic Assessment and Diagnosis of Comorbid Sepsis and Cardiogenic Shock
5. Management Guidelines
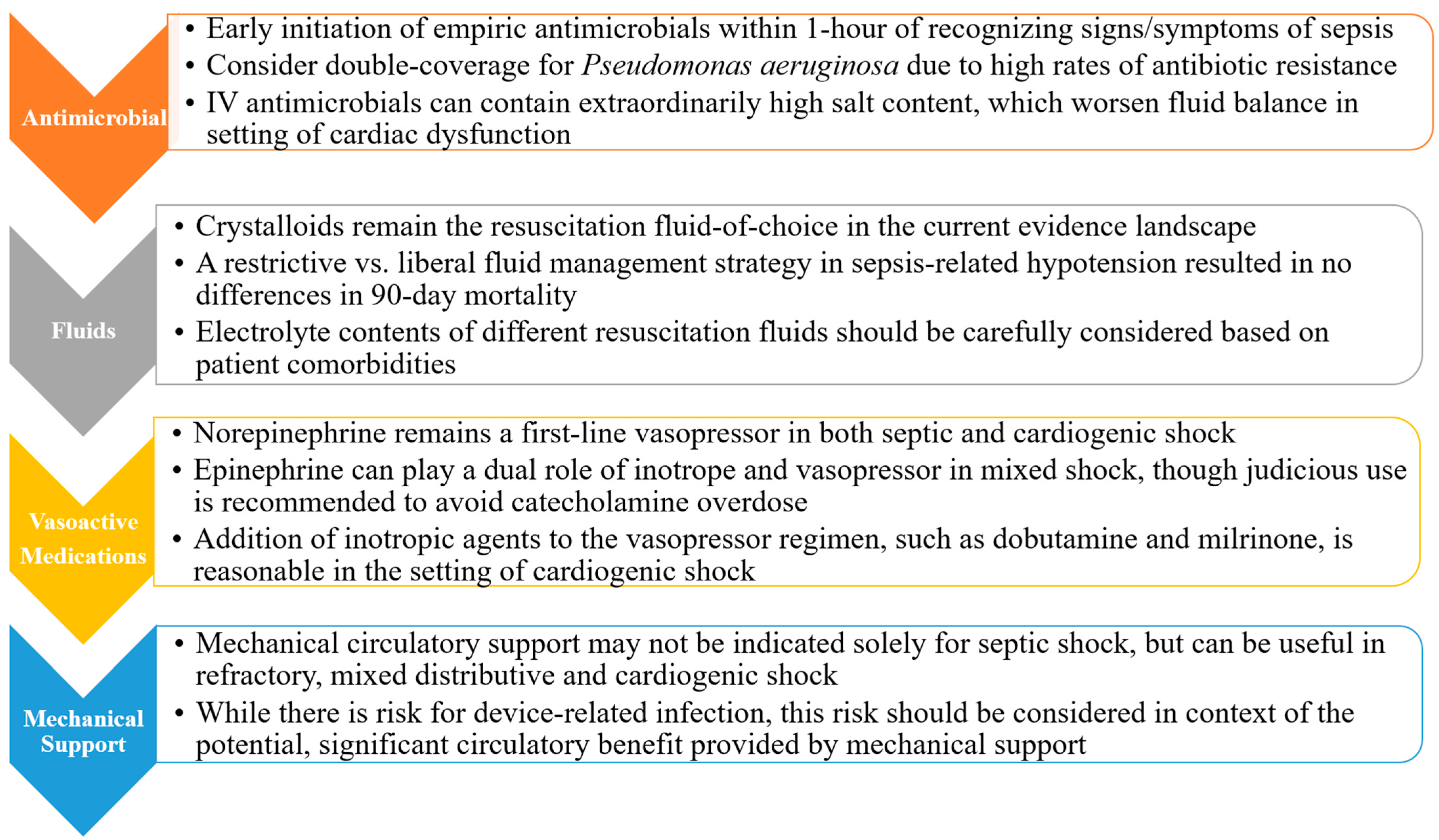
5.1. Antimicrobials
5.2. Fluid Resuscitation
5.3. Vasopressors
5.4. Positive-Pressure Ventilation
5.5. Mechanical Circulatory Support
6. Conclusions and Future Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feldman, E.W.; Dugan, E.; Stephens, R.S.; Schulman, S.; Zakaria, S.; Metkus, T. Presentation and Outcomes of Sepsis in the Cardiac Intensive Care Unit. Am. Heart J. Plus Cardiol. Res. Pract. 2021, 7, 100040. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Govindan, S.; Prescott, H.C. Quick Sequential Organ Failure Assessment: Illness Severity Indicator, Clinical Decision Support Tool, or Both? Crit. Care Med. 2017, 45, 1947–1949. [Google Scholar] [CrossRef]
- Thompson, K.; Venkatesh, B.; Finfer, S. Sepsis and Septic Shock: Current Approaches to Management. Intern. Med. J. 2019, 49, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Jentzer, J.C.; Bhat, A.G.; Patlolla, S.H.; Sinha, S.S.; Miller, P.E.; Lawler, P.R.; van Diepen, S.; Khanna, A.K.; Zhao, D.X.; Vallabhajosyula, S. Concomitant Sepsis Diagnoses in Acute Myocardial Infarction-Cardiogenic Shock: 15-Year National Temporal Trends, Management, and Outcomes. Crit. Care Explor. 2022, 4, e0637. [Google Scholar] [CrossRef] [PubMed]
- Vahdatpour, C.; Collins, D.; Goldberg, S. Cardiogenic Shock. J. Am. Heart Assoc. 2019, 8, e011991. [Google Scholar] [CrossRef]
- Kobbari, G.; Yandrapalli, S.; Anugu, V.R.; Pasam, R.T.; Atti, V.; Kanaparthy, N.; Nabors, C.; Aronow, W. Incidence and Outcomes of Cardiogenic Shock in Patients with Sepsis Complicated by Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73 (Suppl. S1), 288. [Google Scholar] [CrossRef]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Sanborn, T.A.; White, H.D.; Talley, J.D.; Buller, C.E.; Jacobs, A.K.; Slater, J.N.; Col, J.; et al. Early Revascularization in Acute Myocardial Infarction Complicated by Cardiogenic Shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N. Engl. J. Med. 1999, 341, 625–634. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC)Developed with the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Chioncel, O.; Parissis, J.; Mebazaa, A.; Thiele, H.; Desch, S.; Bauersachs, J.; Harjola, V.-P.; Antohi, E.-L.; Arrigo, M.; Ben Gal, T.; et al. Epidemiology, Pathophysiology and Contemporary Management of Cardiogenic Shock—A Position Statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1315–1341. [Google Scholar] [CrossRef]
- Tehrani, B.N.; Truesdell, A.G.; Psotka, M.A.; Rosner, C.; Singh, R.; Sinha, S.S.; Damluji, A.A.; Batchelor, W.B. A Standardized and Comprehensive Approach to the Management of Cardiogenic Shock. JACC Heart Fail. 2020, 8, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Just, H. Peripheral Adaptations in Congestive Heart Failure: A Review. Am. J. Med. 1991, 90, 23S–26S. [Google Scholar] [CrossRef]
- Dhakal, B.P.; Malhotra, R.; Murphy, R.M.; Pappagianopoulos, P.P.; Baggish, A.L.; Weiner, R.B.; Houstis, N.E.; Eisman, A.S.; Hough, S.S.; Lewis, G.D. Mechanisms of Exercise Intolerance in Heart Failure with Preserved Ejection Fraction: The Role of Abnormal Peripheral Oxygen Extraction. Circ. Heart Fail. 2015, 8, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Greer, J. Pathophysiology of Cardiovascular Dysfunction in Sepsis. BJA Educ. 2015, 15, 316–321. [Google Scholar] [CrossRef]
- VINCENT, J.-L.; ZHANG, H.; SZABO, C.; PREISER, J.-C. Effects of Nitric Oxide in Septic Shock. Am. J. Respir. Crit. Care Med. 2000, 161, 1781–1785. [Google Scholar] [CrossRef] [PubMed]
- Kakihana, Y.; Ito, T.; Nakahara, M.; Yamaguchi, K.; Yasuda, T. Sepsis-Induced Myocardial Dysfunction: Pathophysiology and Management. J. Intensive Care 2016, 4, 22. [Google Scholar] [CrossRef]
- Jarczak, D.; Kluge, S.; Nierhaus, A. Sepsis—Pathophysiology and Therapeutic Concepts. Front. Med. 2021, 8, 609. [Google Scholar] [CrossRef]
- Brealey, D.; Brand, M.; Hargreaves, I.; Heales, S.; Land, J.; Smolenski, R.; Davies, N.A.; Cooper, C.E.; Singer, M. Association between Mitochondrial Dysfunction and Severity and Outcome of Septic Shock. Lancet Lond. Engl. 2002, 360, 219–223. [Google Scholar] [CrossRef]
- Niederbichler, A.D.; Hoesel, L.M.; Westfall, M.V.; Gao, H.; Ipaktchi, K.R.; Sun, L.; Zetoune, F.S.; Su, G.L.; Arbabi, S.; Sarma, J.V.; et al. An Essential Role for Complement C5a in the Pathogenesis of Septic Cardiac Dysfunction. J. Exp. Med. 2006, 203, 53–61. [Google Scholar] [CrossRef]
- Sheyin, O.; Davies, O.; Duan, W.; Perez, X. The Prognostic Significance of Troponin Elevation in Patients with Sepsis: A Meta-Analysis. Heart Lung J. Crit. Care 2015, 44, 75–81. [Google Scholar] [CrossRef]
- Frencken, J.F.; Donker, D.W.; Spitoni, C.; Koster-Brouwer, M.E.; Soliman, I.W.; Ong, D.S.Y.; Horn, J.; van der Poll, T.; van Klei, W.A.; Bonten, M.J.M.; et al. Myocardial Injury in Patients with Sepsis and Its Association with Long-Term Outcome. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004040. [Google Scholar] [CrossRef] [PubMed]
- Omar, A.S.; Ur Rahman, M.; Dhatt, G.S.; Salami, G.O.; Abuhasna, S. Dynamics of Brain Natriuretic Peptide in Critically Ill Patients with Severe Sepsis and Septic Shock. Saudi J. Anaesth. 2013, 7, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Jeyaraju, M.; McCurdy, M.T.; Levine, A.R.; Devarajan, P.; Mazzeffi, M.A.; Mullins, K.E.; Reif, M.; Yim, D.N.; Parrino, C.; Lankford, A.S.; et al. Renin Kinetics Are Superior to Lactate Kinetics for Predicting In-Hospital Mortality in Hypotensive Critically Ill Patients. Crit. Care Med. 2022, 50, 50–60. [Google Scholar] [CrossRef]
- Villacorta, H.; Maisel, A.S. Soluble ST2 Testing: A Promising Biomarker in the Management of Heart Failure. Arq. Bras. Cardiol. 2016, 106, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Gomes, D.A.; de Almeida Beltrão, R.L.; de Oliveira Junior, F.M.; da Silva Junior, J.C.; de Arruda, E.P.C.; Lira, E.C.; da Rocha, M.J.A. Vasopressin and Copeptin Release during Sepsis and Septic Shock. Peptides 2021, 136, 170437. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Tang, D.; Chen, J.; Hu, Y.; Cai, X.; Zhang, P. The Clinical Value of GDF15 and Its Prospective Mechanism in Sepsis. Front. Immunol. 2021, 12, 710977. [Google Scholar] [CrossRef]
- Rivers, E.; Nguyen, B.; Havstad, S.; Ressler, J.; Muzzin, A.; Knoblich, B.; Peterson, E.; Tomlanovich, M. Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. N. Engl. J. Med. 2001, 345, 1368–1377. [Google Scholar] [CrossRef]
- Baloch, K.; Rehman Memon, A.; Ikhlaq, U.; Umair, M.; Ansari, M.I.; Abubaker, J.; Salahuddin, N. Assessing the Utility of End-Tidal Carbon Dioxide as a Marker for Fluid Responsiveness in Cardiogenic Shock. Cureus 2021, 13, e13164. [Google Scholar] [CrossRef]
- Salerno, A.; Kuhn, D.; El Sibai, R.; Levine, A.R.; McCurdy, M.T. Real-Time Remote Tele-Mentored Echocardiography: A Systematic Review. Med. Kaunas Lith. 2020, 56, 668. [Google Scholar] [CrossRef]
- Safadi, S.; Murthi, S.; Kashani, K.B. Use of Ultrasound to Assess Hemodynamics in Acutely Ill Patients. Kidney360 2021, 2, 1349–1359. [Google Scholar] [CrossRef]
- Beaubien-Souligny, W.; Rola, P.; Haycock, K.; Bouchard, J.; Lamarche, Y.; Spiegel, R.; Denault, A.Y. Quantifying Systemic Congestion with Point-Of-Care Ultrasound: Development of the Venous Excess Ultrasound Grading System. Ultrasound J. 2020, 12, 16. [Google Scholar] [CrossRef] [PubMed]
- Barjaktarevic, I.; Kenny, J.-É.S.; Berlin, D.; Cannesson, M. The Evolution of Ultrasound in Critical Care: From Procedural Guidance to Hemodynamic Monitor. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2021, 40, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Teboul, J.-L. Passive Leg Raising: Five Rules, Not a Drop of Fluid! Crit. Care 2015, 19, 18. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E. Noninvasive Cardiac Output Monitors: A State-of the-Art Review. J. Cardiothorac. Vasc. Anesth. 2013, 27, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Argueta, E.; Berdine, G.; Pena, C.; Nugent, K.M. FloTrac® Monitoring System: What Are Its Uses in Critically Ill Medical Patients? Am. J. Med. Sci. 2015, 349, 352–356. [Google Scholar] [CrossRef]
- Ranka, S.; Mastoris, I.; Kapur, N.K.; Tedford, R.J.; Rali, A.; Acharya, P.; Weidling, R.; Goyal, A.; Sauer, A.J.; Gupta, B.; et al. Right Heart Catheterization in Cardiogenic Shock Is Associated with Improved Outcomes: Insights From the Nationwide Readmissions Database. J. Am. Heart Assoc. 2021, 10, e019843. [Google Scholar] [CrossRef]
- Shah, M.R.; Hasselblad, V.; Stevenson, L.W.; Binanay, C.; O’Connor, C.M.; Sopko, G.; Califf, R.M. Impact of the Pulmonary Artery Catheter in Critically Ill Patients: Meta-Analysis of Randomized Clinical Trials. JAMA 2005, 294, 1664–1670. [Google Scholar] [CrossRef]
- Bertaina, M.; Galluzzo, A.; Morici, N.; Sacco, A.; Oliva, F.; Valente, S.; D’Ascenzo, F.; Frea, S.; Sbarra, P.; Petitti, E.; et al. Pulmonary Artery Catheter Monitoring in Patients with Cardiogenic Shock: Time for a Reappraisal? Card. Fail. Rev. 2022, 8, e15. [Google Scholar] [CrossRef]
- Saxena, A.; Garan, A.R.; Kapur, N.K.; O’Neill, W.W.; Lindenfeld, J.; Pinney, S.P.; Uriel, N.; Burkhoff, D.; Kern, M. Value of Hemodynamic Monitoring in Patients with Cardiogenic Shock Undergoing Mechanical Circulatory Support. Circulation 2020, 141, 1184–1197. [Google Scholar] [CrossRef]
- Martínez, M.L.; Plata-Menchaca, E.P.; Ruiz-Rodríguez, J.C.; Ferrer, R. An Approach to Antibiotic Treatment in Patients with Sepsis. J. Thorac. Dis. 2020, 12, 1007–1021. [Google Scholar] [CrossRef]
- Strich, J.R.; Heil, E.L.; Masur, H. Considerations for Empiric Antimicrobial Therapy in Sepsis and Septic Shock in an Era of Antimicrobial Resistance. J. Infect. Dis. 2020, 222 (Suppl. S2), S119–S131. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- DiPiro, J.T. Pathophysiology and Treatment of Gram-Negative Sepsis. Am. J. Hosp. Pharm. 1990, 47 (Suppl. S3), S6–S10. [Google Scholar] [CrossRef] [PubMed]
- Gentile, L.F.; Moldawer, L.L. DAMPs, PAMPs, and the Origins of SIRS in Bacterial Sepsis. Shock 2013, 39, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults with Hospital-Acquired and Ventilator-Associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Zakhour, J.; Sharara, S.L.; Hindy, J.-R.; Haddad, S.F.; Kanj, S.S. Antimicrobial Treatment of Pseudomonas Aeruginosa Severe Sepsis. Antibiotics 2022, 11, 1432. [Google Scholar] [CrossRef]
- Amaral, A.C.K.B.; Fowler, R.A.; Pinto, R.; Rubenfeld, G.D.; Ellis, P.; Bookatz, B.; Marshall, J.C.; Martinka, G.; Keenan, S.; Laporta, D.; et al. Patient and Organizational Factors Associated with Delays in Antimicrobial Therapy for Septic Shock. Crit. Care Med. 2016, 44, 2145–2153. [Google Scholar] [CrossRef]
- Deshpande, A.; Haessler, S.; Brizendine, K.; Lindenauer, P.; Lagu, T.; Yu, P.-C.; Bakaki, P.; Pekow, P.; Rothberg, M. Empiric Double Coverage for Healthcare-Associated Pneumonia: Is It Still Necessary? Open Forum Infect. Dis. 2016, 3 (Suppl. S1), 1252. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Maimone, S.; Mazzeo, A.T.; Squadrito, G.; Raimondo, G. Sodium Load and Intravenous Antimicrobials in Patients with Cirrhosis. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2019, 51, 1490–1492. [Google Scholar] [CrossRef]
- Wang, N.; Nguyen, P.K.; Pham, C.U.; Smith, E.A.; Kim, B.; Goetz, M.B.; Graber, C.J. Sodium Content of Intravenous Antibiotic Preparations. Open Forum Infect. Dis. 2019, 6, ofz508. [Google Scholar] [CrossRef] [PubMed]
- Semler, M.W.; Rice, T.W. Sepsis Resuscitation: Fluid Choice and Dose. Clin. Chest Med. 2016, 37, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Finfer, S.; Liu, B.; Taylor, C.; Bellomo, R.; Billot, L.; Cook, D.; Du, B.; McArthur, C.; Myburgh, J. Resuscitation Fluid Use in Critically Ill Adults: An International Cross-Sectional Study in 391 Intensive Care Units. Crit. Care Lond. Engl. 2010, 14, R185. [Google Scholar] [CrossRef] [PubMed]
- Sivapalan, P.; Ellekjaer, K.L.; Jessen, M.K.; Meyhoff, T.S.; Cronhjort, M.; Hjortrup, P.B.; Wetterslev, J.; Granholm, A.; Møller, M.H.; Perner, A. Lower vs Higher Fluid Volumes in Adult Patients with Sepsis: An Updated Systematic Review with Meta-Analysis and Trial Sequential Analysis. Chest 2023, 164, 892–912. [Google Scholar] [CrossRef]
- Moschopoulos, C.D.; Dimopoulou, D.; Dimopoulou, A.; Dimopoulou, K.; Protopapas, K.; Zavras, N.; Tsiodras, S.; Kotanidou, A.; Fragkou, P.C. New Insights into the Fluid Management in Patients with Septic Shock. Medicina 2023, 59, 1047. [Google Scholar] [CrossRef]
- Caironi, P.; Tognoni, G.; Masson, S.; Fumagalli, R.; Pesenti, A.; Romero, M.; Fanizza, C.; Caspani, L.; Faenza, S.; Grasselli, G.; et al. Albumin Replacement in Patients with Severe Sepsis or Septic Shock. N. Engl. J. Med. 2014, 370, 1412–1421. [Google Scholar] [CrossRef]
- Hahn, R.G.; Lyons, G. The Half-Life of Infusion Fluids: An Educational Review. Eur. J. Anaesthesiol. 2016, 33, 475–482. [Google Scholar] [CrossRef]
- The SAFE Study Investigators. A Comparison of Albumin and Saline for Fluid Resuscitation in the Intensive Care Unit. N. Engl. J. Med. 2004, 350, 2247–2256. [Google Scholar] [CrossRef]
- Annane, D.; Siami, S.; Jaber, S.; Martin, C.; Elatrous, S.; Declère, A.D.; Preiser, J.C.; Outin, H.; Troché, G.; Charpentier, C.; et al. Effects of Fluid Resuscitation with Colloids vs Crystalloids on Mortality in Critically Ill Patients Presenting with Hypovolemic Shock: The CRISTAL Randomized Trial. JAMA 2013, 310, 1809–1817. [Google Scholar] [CrossRef]
- Hanley, C.; Callum, J.; Karkouti, K.; Bartoszko, J. Albumin in Adult Cardiac Surgery: A Narrative Review. Can. J. Anesth. Can. Anesth. 2021, 68, 1197–1213. [Google Scholar] [CrossRef]
- Geng, L.; Tian, X.; Gao, Z.; Mao, A.; Feng, L.; He, C. Different Concentrations of Albumin Versus Crystalloid in Patients with Sepsis and Septic Shock: A Meta-Analysis of Randomized Clinical Trials. J. Intensive Care Med. 2023, 38, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Bauer, M.; Nierhaus, A.; Kluge, S.; Schumacher, U.; Putensen, C.; Fichtner, F.; Petros, S.; Scheer, C.; Jaschinski, U.; et al. Randomized Controlled Multicentre Study of Albumin Replacement Therapy in Septic Shock (ARISS): Protocol for a Randomized Controlled Trial. Trials 2020, 21, 1002. [Google Scholar] [CrossRef] [PubMed]
- Semler, M.W.; Kellum, J.A. Balanced Crystalloid Solutions. Am. J. Respir. Crit. Care Med. 2019, 199, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Semler, M.W.; Self, W.H.; Wanderer, J.P.; Ehrenfeld, J.M.; Wang, L.; Byrne, D.W.; Stollings, J.L.; Kumar, A.B.; Hughes, C.G.; Hernandez, A.; et al. Balanced Crystalloids versus Saline in Critically Ill Adults. N. Engl. J. Med. 2018, 378, 829–839. [Google Scholar] [CrossRef]
- Self, W.H.; Semler, M.W.; Wanderer, J.P.; Wang, L.; Byrne, D.W.; Collins, S.P.; Slovis, C.M.; Lindsell, C.J.; Ehrenfeld, J.M.; Siew, E.D.; et al. Balanced Crystalloids versus Saline in Noncritically Ill Adults. N. Engl. J. Med. 2018, 378, 819–828. [Google Scholar] [CrossRef]
- Zampieri, F.G.; Machado, F.R.; Biondi, R.S.; Freitas, F.G.R.; Veiga, V.C.; Figueiredo, R.C.; Lovato, W.J.; Amêndola, C.P.; Serpa-Neto, A.; Paranhos, J.L.R.; et al. Effect of Intravenous Fluid Treatment with a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial. JAMA 2021, 326, 818–829. [Google Scholar] [CrossRef]
- Finfer, S.; Micallef, S.; Hammond, N.; Navarra, L.; Bellomo, R.; Billot, L.; Delaney, A.; Gallagher, M.; Gattas, D.; Li, Q.; et al. Balanced Multielectrolyte Solution versus Saline in Critically Ill Adults. N. Engl. J. Med. 2022, 386, 815–826. [Google Scholar] [CrossRef]
- Vallon, V. Tubuloglomerular Feedback and the Control of Glomerular Filtration Rate. Physiology 2003, 18, 169–174. [Google Scholar] [CrossRef]
- Toporek, A.H.; Semler, M.W.; Self, W.H.; Bernard, G.R.; Wang, L.; Siew, E.D.; Stollings, J.L.; Wanderer, J.P.; Rice, T.W.; Casey, J.D. Balanced Crystalloids versus Saline in Critically Ill Adults with Hyperkalemia or Acute Kidney Injury: Secondary Analysis of a Clinical Trial. Am. J. Respir. Crit. Care Med. 2021, 203, 1322–1325. [Google Scholar] [CrossRef]
- Demiselle, J.; Fage, N.; Radermacher, P.; Asfar, P. Vasopressin and Its Analogues in Shock States: A Review. Ann. Intensive Care 2020, 10, 9. [Google Scholar] [CrossRef]
- Tarvasmäki, T.; Lassus, J.; Varpula, M.; Sionis, A.; Sund, R.; Køber, L.; Spinar, J.; Parissis, J.; Banaszewski, M.; Silva Cardoso, J.; et al. Current Real-Life Use of Vasopressors and Inotropes in Cardiogenic Shock—Adrenaline Use Is Associated with Excess Organ Injury and Mortality. Crit. Care Lond. Engl. 2016, 20, 208. [Google Scholar] [CrossRef]
- De Backer, D.; Biston, P.; Devriendt, J.; Madl, C.; Chochrad, D.; Aldecoa, C.; Brasseur, A.; Defrance, P.; Gottignies, P.; Vincent, J.-L. Comparison of Dopamine and Norepinephrine in the Treatment of Shock. N. Engl. J. Med. 2010, 362, 779–789. [Google Scholar] [CrossRef]
- Conti, N.; Gatti, M.; Raschi, E.; Diemberger, I.; Potena, L. Evidence and Current Use of Levosimendan in the Treatment of Heart Failure: Filling the Gap. Drug Des. Devel. Ther. 2021, 15, 3391–3409. [Google Scholar] [CrossRef]
- Gordon, A.C.; Perkins, G.D.; Singer, M.; McAuley, D.F.; Orme, R.M.L.; Santhakumaran, S.; Mason, A.J.; Cross, M.; Al-Beidh, F.; Best-Lane, J.; et al. Levosimendan for the Prevention of Acute Organ Dysfunction in Sepsis. N. Engl. J. Med. 2016, 375, 1638–1648. [Google Scholar] [CrossRef]
- McCurdy, M.T.; Busse, L.W. Rethinking Vasopressor Education: The Need to Avoid Teaching the Bare Minimum. ATS Sch. 2023, 4, 389–390. [Google Scholar] [CrossRef]
- Khanna, A.; English, S.W.; Wang, X.S.; Ham, K.; Tumlin, J.; Szerlip, H.; Busse, L.W.; Altaweel, L.; Albertson, T.E.; Mackey, C.; et al. Angiotensin II for the Treatment of Vasodilatory Shock. N. Engl. J. Med. 2017, 377, 419–430. [Google Scholar] [CrossRef]
- Busse, L.W.; McCurdy, M.T.; Ali, O.; Hall, A.; Chen, H.; Ostermann, M. The Effect of Angiotensin II on Blood Pressure in Patients with Circulatory Shock: A Structured Review of the Literature. Crit. Care Lond. Engl. 2017, 21, 324. [Google Scholar] [CrossRef]
- Mercat, A.; Richard, J.-C.M.; Vielle, B.; Jaber, S.; Osman, D.; Diehl, J.-L.; Lefrant, J.-Y.; Prat, G.; Richecoeur, J.; Nieszkowska, A.; et al. Positive End-Expiratory Pressure Setting in Adults with Acute Lung Injury and Acute Respiratory Distress Syndrome: A Randomized Controlled Trial. JAMA 2008, 299, 646–655. [Google Scholar] [CrossRef]
- Alviar, C.L.; Miller, P.E.; McAreavey, D.; Katz, J.N.; Lee, B.; Moriyama, B.; Soble, J.; van Diepen, S.; Solomon, M.A.; Morrow, D.A. Positive Pressure Ventilation in the Cardiac Intensive Care Unit. J. Am. Coll. Cardiol. 2018, 72, 1532–1553. [Google Scholar] [CrossRef]
- Corp, A.; Thomas, C.; Adlam, M. The Cardiovascular Effects of Positive Pressure Ventilation. BJA Educ. 2021, 21, 202–209. [Google Scholar] [CrossRef]
- Disselkamp, M.; Adkins, D.; Pandey, S.; Coz Yataco, A.O. Physiologic Approach to Mechanical Ventilation in Right Ventricular Failure. Ann. Am. Thorac. Soc. 2018, 15, 383–389. [Google Scholar] [CrossRef]
- Atti, V.; Narayanan, M.A.; Patel, B.; Balla, S.; Siddique, A.; Lundgren, S.; Velagapudi, P. A Comprehensive Review of Mechanical Circulatory Support Devices. Heart Int. 2022, 16, 37–48. [Google Scholar] [CrossRef]
- Thiele, H.; Ohman, E.M.; Desch, S.; Eitel, I.; de Waha, S. Management of Cardiogenic Shock. Eur. Heart J. 2015, 36, 1223–1230. [Google Scholar] [CrossRef]
- Alkhunaizi, F.A.; Burkhoff, D.; Brener, M.I. Right-Sided Mechanical Circulatory Support—A Hemodynamic Perspective. Curr. Heart Fail. Rep. 2022, 19, 334–345. [Google Scholar] [CrossRef]
- Vis, A.; Arfaee, M.; Khambati, H.; Slaughter, M.S.; Gummert, J.F.; Overvelde, J.T.B.; Kluin, J. The Ongoing Quest for the First Total Artificial Heart as Destination Therapy. Nat. Rev. Cardiol. 2022, 19, 813–828. [Google Scholar] [CrossRef]
- Marasco, S.F.; Lukas, G.; McDonald, M.; McMillan, J.; Ihle, B. Review of ECMO (Extra Corporeal Membrane Oxygenation) Support in Critically Ill Adult Patients. Heart Lung Circ. 2008, 17 (Suppl. S4), S41–S47. [Google Scholar] [CrossRef]
- Shin, T.G.; Choi, J.-H.; Jo, I.J.; Sim, M.S.; Song, H.G.; Jeong, Y.K.; Song, Y.-B.; Hahn, J.-Y.; Choi, S.H.; Gwon, H.-C. Extracorporeal Cardiopulmonary Resuscitation in Patients with Inhospital Cardiac Arrest: A Comparison with Conventional Cardiopulmonary Resuscitation. Crit. Care Med. 2011, 39, 1–7. [Google Scholar] [CrossRef]
- Chen, Y.-S.; Lin, J.-W.; Yu, H.-Y.; Ko, W.-J.; Jerng, J.-S.; Chang, W.-T.; Chen, W.-J.; Huang, S.-C.; Chi, N.-H.; Wang, C.-H. Cardiopulmonary Resuscitation with Assisted Extracorporeal Life-Support versus Conventional Cardiopulmonary Resuscitation in Adults with in-Hospital Cardiac Arrest: An Observational Study and Propensity Analysis. Lancet 2008, 372, 554–561. [Google Scholar] [CrossRef]
- Ostadal, P.; Rokyta, R.; Karasek, J.; Kruger, A.; Vondrakova, D.; Janotka, M.; Naar, J.; Smalcova, J.; Hubatova, M.; Hromadka, M.; et al. Extracorporeal Membrane Oxygenation in the Therapy of Cardiogenic Shock: Results of the ECMO-CS Randomized Clinical Trial. Circulation 2023, 147, 454–464. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Akin, I.; Behnes, M.; Rassaf, T.; Mahabadi, A.A.; Lehmann, R.; Eitel, I.; Graf, T.; Seidler, T.; et al. Extracorporeal Life Support in Infarct-Related Cardiogenic Shock. N. Engl. J. Med. 2023, 389, 1286–1297. [Google Scholar] [CrossRef]
- Ling, R.R.; Ramanathan, K.; Poon, W.H.; Tan, C.S.; Brechot, N.; Brodie, D.; Combes, A.; MacLaren, G. Venoarterial Extracorporeal Membrane Oxygenation as Mechanical Circulatory Support in Adult Septic Shock: A Systematic Review and Meta-Analysis with Individual Participant Data Meta-Regression Analysis. Crit. Care 2021, 25, 246. [Google Scholar] [CrossRef]
- Geller, B.J.; Sinha, S.S.; Kapur, N.K.; Bakitas, M.; Balsam, L.B.; Chikwe, J.; Klein, D.G.; Kochar, A.; Masri, S.C.; Sims, D.B.; et al. Escalating and De-Escalating Temporary Mechanical Circulatory Support in Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation 2022, 146, e50–e68. [Google Scholar] [CrossRef]
- Sato, R.; Hasegawa, D.; Guo, S.C.; Nishida, K.; Dugar, S. Temporary Mechanical Circulatory Support in Sepsis-Associated Cardiogenic Shock with and Without Acute Myocardial Infarction. J. Cardiothorac. Vasc. Anesth. 2023, 9, 26. [Google Scholar] [CrossRef]
- Chvojka, J.; Martinkova, V.; Benes, J.; Valesova, L.; Danihel, V.; Nalos, L.; Matejovic, M. Mechanical Circulatory Support in Refractory Vasodilatory Septic Shock: A Randomized Controlled Porcine Study. Shock 2020, 53, 124–131. [Google Scholar] [CrossRef]
- Gilotra, N.A.; Stevens, G.R. Temporary Mechanical Circulatory Support: A Review of the Options, Indications, and Outcomes. Clin. Med. Insights Cardiol. 2014, 8 (Suppl. S1), 75–85. [Google Scholar] [CrossRef]
- Mayr, V.D.; Dünser, M.W.; Greil, V.; Jochberger, S.; Luckner, G.; Ulmer, H.; Friesenecker, B.E.; Takala, J.; Hasibeder, W.R. Causes of Death and Determinants of Outcome in Critically Ill Patients. Crit. Care 2006, 10, R154. [Google Scholar] [CrossRef]
- George, P.; Srivastava, M.C.; Ludmir, J.; Reed, R.M.; Tewelde, S.Z.; Gupta, A.; McCurdy, M.T. Augmenting Function for Infarction from Infection: Impella 2.5 for Ischemic Cardiogenic Shock Complicating Sepsis. Case Rep. Cardiol. 2017, 2017, 8407530. [Google Scholar] [CrossRef]
- Petricevic, M.; Milicic, D.; Boban, M.; Mihaljevic, M.Z.; Baricevic, Z.; Kolic, K.; Dolic, K.; Konosic, L.; Kopjar, T.; Biocina, B. Bleeding and Thrombotic Events in Patients Undergoing Mechanical Circulatory Support: A Review of Literature. Thorac. Cardiovasc. Surg. 2015, 63, 636–646. [Google Scholar] [CrossRef]
- Baumann Kreuziger, L.; Massicotte, M.P. Mechanical Circulatory Support: Balancing Bleeding and Clotting in High-Risk Patients. Hematology 2015, 2015, 61–68. [Google Scholar] [CrossRef]


{kind=link}
| Etiology of Shock | Cardiac Index (CI) | Systemic Vascular Resistance (SVR) | Central Venous O2 Saturation (ScVO2) | Central Venous Pressure (CVP) |
|---|---|---|---|---|
| Cardiogenic | Decreased | Increased | Decreased | Increased |
| Distributive | Increased or normal | Decreased | Increased | Decreased or normal |
| Hypovolemic | Decreased | Increased | Decreased | Decreased |
| Obstructive | Decreased | Increased or normal | Decreased or normal | Increased |
| Mixed Cardiogenic & Distributive | Decreased or variable | Decreased or variable | Variable | Variable |
| Fluid Type | Sodium-Na (mEq/L) | Chloride-Cl (mEq/L) | Potassium-K (mEq/L) | Osmolality (mosm/L) |
|---|---|---|---|---|
| Plasma | 140 | 103 | 4 | 290 |
| Normal Saline (0.9%) | 154 | 154 | 0 | 308 |
| Lactated Ringers | 130 | 109 | 4 | 273 |
| Plasmalyte | 140 | 98 | 5 | 294 |
| Colloids (e.g., 25% albumin) | 145 | Dependent on diluent | Dependent on diluent | ~300 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; McCurdy, M.T.; Ludmir, J. Sepsis Management in the Cardiac Intensive Care Unit. J. Cardiovasc. Dev. Dis. 2023, 10, 429. https://doi.org/10.3390/jcdd10100429
Zhang Y, McCurdy MT, Ludmir J. Sepsis Management in the Cardiac Intensive Care Unit. Journal of Cardiovascular Development and Disease. 2023; 10(10):429. https://doi.org/10.3390/jcdd10100429
Chicago/Turabian StyleZhang, Yichi, Michael T. McCurdy, and Jonathan Ludmir. 2023. "Sepsis Management in the Cardiac Intensive Care Unit" Journal of Cardiovascular Development and Disease 10, no. 10: 429. https://doi.org/10.3390/jcdd10100429
APA StyleZhang, Y., McCurdy, M. T., & Ludmir, J. (2023). Sepsis Management in the Cardiac Intensive Care Unit. Journal of Cardiovascular Development and Disease, 10(10), 429. https://doi.org/10.3390/jcdd10100429