Rethinking the Role of the Renin-Angiotensin System in the Pandemic Era of SARS-CoV-2


1
Department of Medicine and Surgery, University of Insubria, 21100 Varese, Italy
2
Department of Medicine and Cardiopulmonary Rehabilitation, Istituti Clinici Scientifici Maugeri IRCCS, 21049 Tradate, Italy
3
Fondazione Umbra Cuore e Ipertensione-ONLUS, and Division of Cardiology, Hospital S. Maria della Misericordia, 06100 Perugia, Italy
*
Author to whom correspondence should be addressed.
J. Cardiovasc. Dev. Dis. 2023, 10(1), 14; https://doi.org/10.3390/jcdd10010014
Submission received: 9 December 2022
/
Revised: 26 December 2022
/
Accepted: 29 December 2022
/
Published: 1 January 2023
{kind=link}
After assessing the levels of spread and severity of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, academic literature focused on the pathophysiology of coronavirus disease 2019 (COVID-19) [1,2,3]. The Journal of Cardiovascular Development and Disease has actively contributed to the growth of our knowledge in this field, with articles spanning a range of topics from mechanisms and risk stratification to therapeutic interventions [4,5,6,7].
It is well documented that SARS-CoV-2 infection may trigger a cascade of systemic events affecting various organs and tissues [8,9]. Emerging data support that the leading actor in the pathogenesis of the complications of COVID-19 is a dysregulation of the renin–angiotensin system (RAS) [10,11,12]. Related evidence from experimental and clinical studies have been accrued [12] and the imbalance between angiotensin II (Ang II) and Angiotensin1–7 (Ang1–7) caused by the interaction between SARS-CoV-2 (as mediated by the binding of the Spike protein of the virus) and the angiotensin converting enzyme 2 (ACE2) receptors exerts a pivotal role on the clinical picture and outcome of COVID-19 [10,11,12,13]. More specifically, SARS-CoV-2 entry into human cells is mediated by the efficient binding of the Spike protein to ACE2 [14,15]. The ACE2 is a trans-membrane type I glycoprotein (expressed in almost all human tissues [16]) which uses a single extracellular catalytic domain to cleave an amino acid from Ang II to form Ang1–7 [17]. The viral entry process consists of three main steps [14,18]. In the first step, the N-terminal portion of the viral protein unit S1 binds to a pocket of the ACE2 receptor [14]. In the second step, the protein cleavage between the S1 and S2 units is operated by the receptor transmembrane protease serine 2 (TMPRSS2) which facilitates viral entry and downregulates surface ACE2 expression [19]. In the third step, the viral S2 unit undergoes a conformational rearrangement after the cleavage of the viral protein by TMPRSS2, driving the fusion between the viral and cellular membrane and promoting the entry of the virus into cell, release of its content, replication, and infection [20].
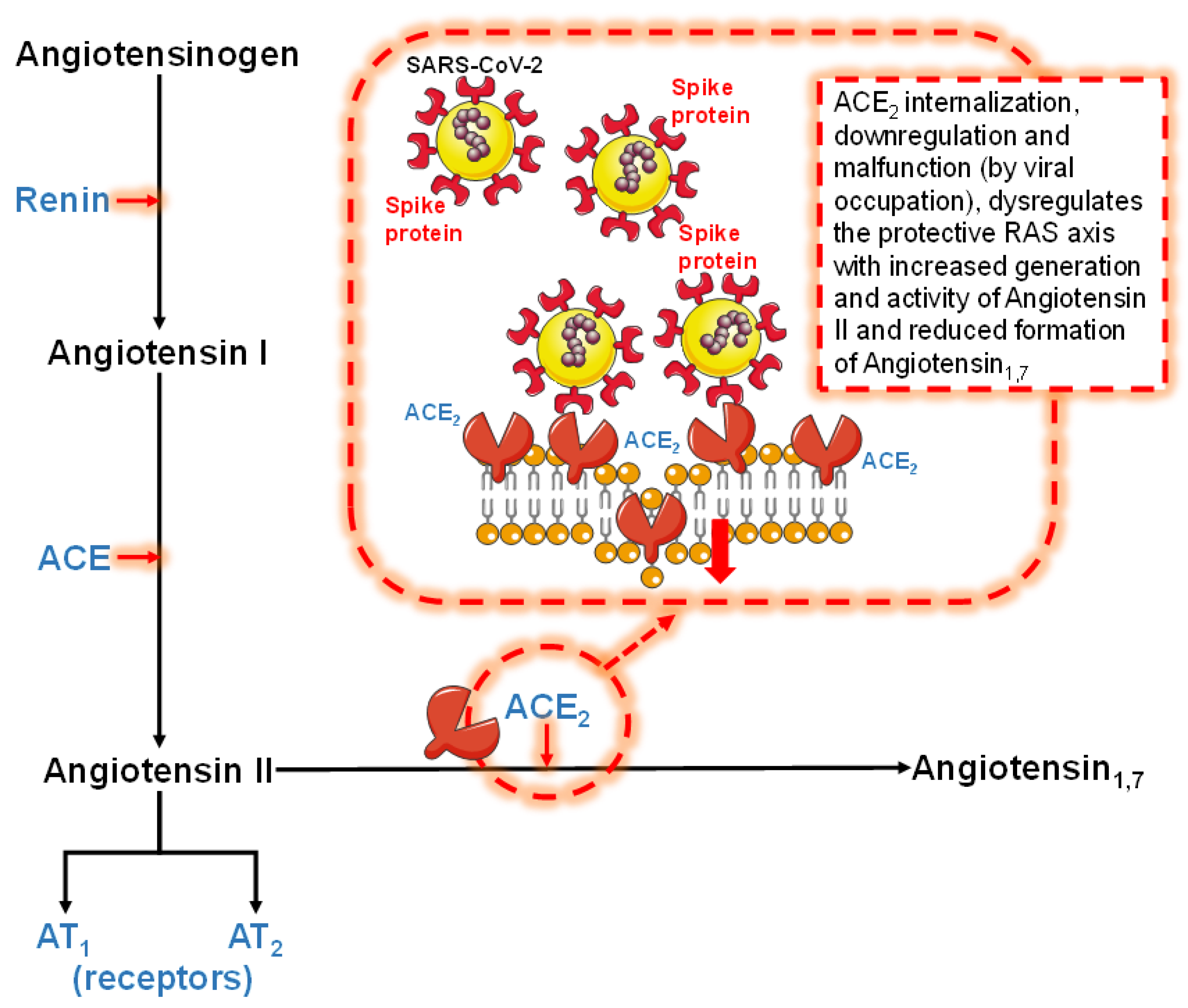
The failure of the counter-regulatory RAS axis, characterized by the decrease in ACE2 expression and generation of the protective Ang1–7, is strictly implicated in the development of severe forms of COVID-19 [10,11,13,14,21,22]. ACE2 internalization, downregulation, and malfunction, predominantly due to viral occupation, dysregulates the protective RAS axis with increased generation and activity of Ang II and reduced formation of Ang1–7 [10,11,13] (Figure 1). This has been corroborated by recent investigations supporting the evidence of the development of an “Ang II storm” [23] or “Ang II intoxication” [24] during the SARS-CoV-2 infection [7,11,12,13,25,26]. Ramos and co-workers provided a new assessment of available data, exploring COVID-19 as a molecular disease that causes negative regulation of ACE2 and RAS with microcirculatory changes responsible for the wide variety of injury mechanisms observed in different organs as a result of the disease [23]. Similarly, Sfera and co-workers proposed a common pathophysiological denominator for COVID-19 [24]. They hypothesized that the outlook of COVID-19 is negatively correlated with the intracellular accumulation of Ang II promoted by the viral blockade of its degrading enzyme receptors [24]. Notably, similar effects of COVID-19 vaccines have been recently postulated [8,27]. Indeed, COVID-19 vaccines increase the endogenous synthesis of SARS-CoV-2 Spike proteins. The free-floating Spike proteins synthetized by cells targeted by vaccines and destroyed by the immune response may massively circulate in the blood and systematically interact with ACE2 receptors, thereby promoting ACE2 internalization and degradation [8,27]. In other words, these reactions might result in pathological features which resemble those of SARS-CoV-2 infection [8,27].
The reduced catalytic efficiency of ACE2 resulting from viral occupation and down-regulation of these receptors may be particularly detrimental in patients with baseline deficiency of ACE2 receptor activity [11,12]. Notably, phenotypes of ACE2 deficiency include advanced age, some cardiovascular risk factors, and previous cardiovascular events [9,10,11,12,28,29,30,31,32,33,34,35,36,37]. Aging is associated with declining levels of ACE2 expression in experimental and human models [38,39,40,41]. Chen and co-workers analyzed GTEx and other public data in 30 tissues across thousands of individuals and they found an age-dependent decrease in ACE2 expression in all ethnic groups [40]. Furthermore, human and mouse data analysis revealed that ACE2 expression is reduced in type 2 diabetes [40]. Similar results have been also obtained in other reports showing that diabetes mellitus is associated with a reduction in ACE2 expression and with Ang1–7-generating system downregulation [42,43].
Hypertension is associated with RAS over-activation, increased angiotensin type 1 receptor (AT1R) stimulation by Ang II, and downregulation of ACE2 [44].
ACE2 deficiency is also documented in several experimental models of cardiovascular complications, including congestive heart failure, myocardial ischemia and infarction, and coronary artery disease [45,46,47,48,49]. For example, Kassiri and co-workers reported that loss of ACE2 facilitates adverse post-myocardial ventricular remodeling through potentiation of Ang II effects [48]. In their experimental analyses, myocardial infarction was associated with a persistent increase in ACE2 protein in the infarct zone in wild-type mice, whereas loss of ACE2 enhanced the susceptibility to myocardial infarction, with increased mortality, infarct expansion, and adverse ventricular remodeling characterized by ventricular dilation and systolic dysfunction [48]. In ACE2-deficient hearts, elevated myocardial levels of Ang II and decreased levels of Ang1–7 in the infarct-related zone were associated with increased production of reactive oxygen species [48]. Additionally, ACE2 deficiency leads to increased matrix metalloproteinase (MMP) 2 and MMP9 levels with MMP2 activation in the infarct and peri-infarct regions, as well as increased gelatinase activity leading to a disrupted extracellular matrix structure after myocardial infarction. Moreover, loss of ACE2 was also associated with increased neutrophilic infiltration in the infarct and peri-infarct regions, resulting in upregulation of inflammatory cytokines [48].
However, ACE2 are not the exclusive angiotensinases in humans. Other angiotensinases involved in the processing of Ang II to Ang1–7 may influence the detrimental interactions between Spike proteins of SARS-CoV-2 and ACE2 receptors [50,51,52,53]. As recently suggested, the relative activity of different angiotensinases (including ACE2, prolyl carboxypeptidases, and prolyl oligopeptidases) and their changes in the cardiovascular continuum disease, should be taken into consideration to fully understand the pathogenesis of COVID-19. In other words, different mechanisms of Ang II cleavage and accumulation may be involved in a unique pathophysiological mechanism explaining the risk of the progression to severe forms of COVID-19 [8,12].
In conclusion, understanding the pathophysiology of COVID-19 influences the treatment of these patients. Importantly, some hypotheses have been made on the potential therapeutic approach of restoring the ACE2/Ang1–7 pathway.
Pharmacological modulation of RAS may be useful to enhance the blockade of the transition from infection to severe forms of COVID-19 [25]. In a recent prospective study of hypertensive patients with COVID-19, we documented that exposure to RAS modifiers was associated with a significant reduction in the risk of in-hospital mortality compared to other blood pressure-lowering strategies [7]. Exposure to ACE-inhibitors was not significantly associated with a reduced risk of in-hospital mortality compared with patients who were not treated with RAS modifiers [7]. Conversely, angiotensin receptor blockers users showed a 59% lower risk of death (p = 0.016) even after allowance for several prognostic markers, including age, oxygen saturation, occurrence of severe hypotension during hospitalization, and lymphocyte count [7].
Moreover, the delivery of functional soluble ACE2 forms may trap the virus and stimulate the RAS protective pathway [13]. Finally, ACE2 inhibitors may block or attenuate the binding of SARS-CoV-2 Spike protein to the pocket of the ACE2 [13]. This pharmacological approach could reduce viral internalization into ACE2-expressing cells [13]. However, pharmacological inhibition of ACE2 may exert enzymatic activities with or without inactivation of ACE2. The real challenge in the field of ACE inhibition is to modulate SARS-CoV-2 binding to ACE2 without blocking the protective conversion of Ang II into Ang1–7 [13].
Author Contributions
Conceptualization, methodology, resources, data curation, writing—original draft preparation, writing—review and editing, visualization, and supervision, F.A., M.Z. and P.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zappa, M.; Verdecchia, P.; Angeli, F. Knowing the new Omicron BA.2.75 variant (‘Centaurus’): A simulation study. Eur. J. Intern. Med. 2022, 105, 107–108. [Google Scholar] [CrossRef]
- Zappa, M.; Verdecchia, P.; Angeli, F. The new phase of pandemic: Are BA.2.75 and BQ.1 competitive variants? An in silico evaluation. Eur. J. Intern. Med. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Zappa, M.; Verdecchia, P.; Spanevello, A.; Angeli, F. Structural evolution of severe acute respiratory syndrome coronavirus 2: Implications for adhesivity to angiotensin-converting enzyme 2 receptors and vaccines. Eur. J. Intern. Med. 2022, 104, 33–36. [Google Scholar] [CrossRef]
- Zajac, P.; Kazirod-Wolski, K.; Oles, I.; Sielski, J.; Siudak, Z. Role of Fibrinolysis in the Management of Patients with COVID-19 and Thromboembolic Complications: A Review. J. Cardiovasc. Dev. Dis. 2022, 9, 356. [Google Scholar] [CrossRef] [PubMed]
- Akkaif, M.A.; Bitar, A.N.; Al-Kaif, L.; Daud, N.A.A.; Sha’aban, A.; Noor, D.A.M.; Abd Aziz, F.; Cesaro, A.; Sk Abdul Kader, M.A.; Abdul Wahab, M.J.; et al. The Management of Myocardial Injury Related to SARS-CoV-2 Pneumonia. J. Cardiovasc. Dev. Dis. 2022, 9, 307. [Google Scholar] [CrossRef] [PubMed]
- Cimmino, G.; Conte, S.; Morello, M.; Pellegrino, G.; Marra, L.; Morello, A.; Nicoletti, G.; De Rosa, G.; Golino, P.; Cirillo, P. Vitamin D Inhibits IL-6 Pro-Atherothrombotic Effects in Human Endothelial Cells: A Potential Mechanism for Protection against COVID-19 Infection? J. Cardiovasc. Dev. Dis. 2022, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Verdecchia, P.; Balestrino, A.; Bruschi, C.; Ceriana, P.; Chiovato, L.; Dalla Vecchia, L.A.; Fanfulla, F.; La Rovere, M.T.; Perego, F.; et al. Renin Angiotensin System Blockers and Risk of Mortality in Hypertensive Patients Hospitalized for COVID-19: An Italian Registry. J. Cardiovasc. Dev. Dis. 2022, 9, 15. [Google Scholar] [CrossRef]
- Angeli, F.; Reboldi, G.; Trapasso, M.; Zappa, M.; Spanevello, A.; Verdecchia, P. COVID-19, vaccines and deficiency of ACE(2) and other angiotensinases. Closing the loop on the “Spike effect”. Eur. J. Intern. Med. 2022, 103, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Spanevello, A.; De Ponti, R.; Visca, D.; Marazzato, J.; Palmiotto, G.; Feci, D.; Reboldi, G.; Fabbri, L.M.; Verdecchia, P. Electrocardiographic features of patients with COVID-19 pneumonia. Eur. J. Intern. Med. 2020, 78, 101–106. [Google Scholar] [CrossRef]
- Verdecchia, P.; Cavallini, C.; Spanevello, A.; Angeli, F. COVID-19: ACE2centric Infective Disease? Hypertension 2020, 76, 294–299. [Google Scholar] [CrossRef]
- Verdecchia, P.; Cavallini, C.; Spanevello, A.; Angeli, F. The pivotal link between ACE2 deficiency and SARS-CoV-2 infection. Eur. J. Intern. Med. 2020, 76, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Zappa, M.; Reboldi, G.; Trapasso, M.; Cavallini, C.; Spanevello, A.; Verdecchia, P. The pivotal link between ACE2 deficiency and SARS-CoV-2 infection: One year later. Eur. J. Intern. Med. 2021, 93, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Reboldi, G.; Verdecchia, P. SARS-CoV-2 infection and ACE2 inhibition. J. Hypertens. 2021, 39, 1555–1558. [Google Scholar] [CrossRef]
- Verdecchia, P.; Reboldi, G.; Cavallini, C.; Mazzotta, G.; Angeli, F. ACE-inhibitors, angiotensin receptor blockers and severe acute respiratory syndrome caused by coronavirus. G Ital. Cardiol. 2020, 21, 321–327. [Google Scholar] [CrossRef]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–590. [Google Scholar] [CrossRef] [Green Version]
- Kuba, K.; Imai, Y.; Penninger, J.M. Multiple functions of angiotensin-converting enzyme 2 and its relevance in cardiovascular diseases. Circ. J. 2013, 77, 301–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vickers, C.; Hales, P.; Kaushik, V.; Dick, L.; Gavin, J.; Tang, J.; Godbout, K.; Parsons, T.; Baronas, E.; Hsieh, F.; et al. Hydrolysis of biological peptides by human angiotensin-converting enzyme-related carboxypeptidase. J. Biol. Chem. 2002, 277, 14838–14843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glowacka, I.; Bertram, S.; Muller, M.A.; Allen, P.; Soilleux, E.; Pfefferle, S.; Steffen, I.; Tsegaye, T.S.; He, Y.; Gnirss, K.; et al. Evidence that TMPRSS2 activates the severe acute respiratory syndrome coronavirus spike protein for membrane fusion and reduces viral control by the humoral immune response. J. Virol. 2011, 85, 4122–4134. [Google Scholar] [CrossRef] [Green Version]
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Verdecchia, P.; Angeli, F.; Reboldi, G. Angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers and coronavirus. J. Hypertens. 2020, 38, 1190–1191. [Google Scholar] [CrossRef]
- Angeli, F.; Zappa, M.; Oliva, F.M.; Spanevello, A.; Verdecchia, P. Blood pressure increase during hospitalization for COVID-19. Eur. J. Intern. Med. 2022, 104, 110–112. [Google Scholar] [CrossRef]
- Ramos, S.G.; Rattis, B.; Ottaviani, G.; Celes, M.R.N.; Dias, E.P. ACE2 Down-Regulation May Act as a Transient Molecular Disease Causing RAAS Dysregulation and Tissue Damage in the Microcirculatory Environment Among COVID-19 Patients. Am. J. Pathol. 2021, 191, 1154–1164. [Google Scholar] [CrossRef]
- Sfera, A.; Osorio, C.; Jafri, N.; Diaz, E.L.; Campo Maldonado, J.E. Intoxication With Endogenous Angiotensin II: A COVID-19 Hypothesis. Front. Immunol. 2020, 11, 1472. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Verdecchia, P.; Reboldi, G. Pharmacotherapy for hypertensive urgency and emergency in COVID-19 patients. Expert Opin. Pharm. 2022, 23, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Verdecchia, P.; Reboldi, G. RAAS Inhibitors and Risk of Covid-19. N. Engl. J. Med. 2020, 383, 1990–1991. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Spanevello, A.; Reboldi, G.; Visca, D.; Verdecchia, P. SARS-CoV-2 vaccines: Lights and shadows. Eur. J. Intern. Med. 2021, 88, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Kopel, J.; Perisetti, A.; Roghani, A.; Aziz, M.; Gajendran, M.; Goyal, H. Racial and Gender-Based Differences in COVID-19. Front. Public Health 2020, 8, 418. [Google Scholar] [CrossRef]
- Angeli, F.; Marazzato, J.; Verdecchia, P.; Balestrino, A.; Bruschi, C.; Ceriana, P.; Chiovato, L.; Dalla Vecchia, L.A.; De Ponti, R.; Fanfulla, F.; et al. Joint effect of heart failure and coronary artery disease on the risk of death during hospitalization for COVID-19. Eur. J. Intern. Med. 2021, 89, 81–86. [Google Scholar] [CrossRef]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Guo, L.; Shi, Z.; Zhang, Y.; Wang, C.; Do Vale Moreira, N.C.; Zuo, H.; Hussain, A. Comorbid diabetes and the risk of disease severity or death among 8807 COVID-19 patients in China: A meta-analysis. Diabetes Res. Clin. Pract. 2020, 166, 108346. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Masnaghetti, S.; Visca, D.; Rossoni, A.; Taddeo, S.; Biagini, F.; Verdecchia, P. Severity of COVID-19: The importance of being hypertensive. Monaldi Arch. Chest Dis. Arch. Monaldi Per Le Mal. Del Torace 2020, 90. [Google Scholar] [CrossRef]
- Abassi, Z.; Assady, S.; Khoury, E.E.; Heyman, S.N. Letter to the Editor: Angiotensin-converting enzyme 2: An ally or a Trojan horse? Implications to SARS-CoV-2-related cardiovascular complications. Am. J. Physiol. Heart Circ. Physiol. 2020, 318, H1080–H1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheblawi, M.; Wang, K.; Viveiros, A.; Nguyen, Q.; Zhong, J.C.; Turner, A.J.; Raizada, M.K.; Grant, M.B.; Oudit, G.Y. Angiotensin-Converting Enzyme 2: SARS-CoV-2 Receptor and Regulator of the Renin-Angiotensin System: Celebrating the 20th Anniversary of the Discovery of ACE2. Circ. Res. 2020, 126, 1456–1474. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Gheblawi, M.; Oudit, G.Y. Angiotensin Converting Enzyme 2: A Double-Edged Sword. Circulation 2020, 142, 426–428. [Google Scholar] [CrossRef]
- Yoon, H.E.; Kim, E.N.; Kim, M.Y.; Lim, J.H.; Jang, I.A.; Ban, T.H.; Shin, S.J.; Park, C.W.; Chang, Y.S.; Choi, B.S. Age-Associated Changes in the Vascular Renin-Angiotensin System in Mice. Oxid. Med. Cell Longev. 2016, 2016, 6731093. [Google Scholar] [CrossRef] [Green Version]
- Xie, X.; Chen, J.; Wang, X.; Zhang, F.; Liu, Y. Age- and gender-related difference of ACE2 expression in rat lung. Life Sci. 2006, 78, 2166–2171. [Google Scholar] [CrossRef]
- Chen, J.; Jiang, Q.; Xia, X.; Liu, K.; Yu, Z.; Tao, W.; Gong, W.; Han, J.J. Individual variation of the SARS-CoV-2 receptor ACE2 gene expression and regulation. Aging Cell 2020, 19, e13168. [Google Scholar] [CrossRef]
- Angeli, F.; Reboldi, G.; Verdecchia, P. Ageing, ACE2 deficiency and bad outcome in COVID-19. Clin. Chem Lab. Med. 2021, 59, 1607–1609. [Google Scholar] [CrossRef]
- Yamagata, R.; Nemoto, W.; Nakagawasai, O.; Takahashi, K.; Tan-No, K. Downregulation of spinal angiotensin converting enzyme 2 is involved in neuropathic pain associated with type 2 diabetes mellitus in mice. Biochem. Pharmacol. 2020, 174, 113825. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Bhansali, A. COVID-19, diabetes mellitus and ACE2: The conundrum. Diabetes Res. Clin. Pract. 2020, 162, 108132. [Google Scholar] [CrossRef]
- Koka, V.; Huang, X.R.; Chung, A.C.; Wang, W.; Truong, L.D.; Lan, H.Y. Angiotensin II up-regulates angiotensin I-converting enzyme (ACE), but down-regulates ACE2 via the AT1-ERK/p38 MAP kinase pathway. Am. J. Pathol. 2008, 172, 1174–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, V.B.; Zhong, J.C.; Grant, M.B.; Oudit, G.Y. Role of the ACE2/Angiotensin 1-7 Axis of the Renin-Angiotensin System in Heart Failure. Circ. Res. 2016, 118, 1313–1326. [Google Scholar] [CrossRef] [Green Version]
- Crackower, M.A.; Sarao, R.; Oudit, G.Y.; Yagil, C.; Kozieradzki, I.; Scanga, S.E.; Oliveira-dos-Santos, A.J.; da Costa, J.; Zhang, L.; Pei, Y.; et al. Angiotensin-converting enzyme 2 is an essential regulator of heart function. Nature 2002, 417, 822–828. [Google Scholar] [CrossRef]
- Danilczyk, U.; Penninger, J.M. Angiotensin-converting enzyme II in the heart and the kidney. Circ. Res. 2006, 98, 463–471. [Google Scholar] [CrossRef]
- Kassiri, Z.; Zhong, J.; Guo, D.; Basu, R.; Wang, X.; Liu, P.P.; Scholey, J.W.; Penninger, J.M.; Oudit, G.Y. Loss of angiotensin-converting enzyme 2 accelerates maladaptive left ventricular remodeling in response to myocardial infarction. Circulation Heart Fail. 2009, 2, 446–455. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, K.; Ohishi, M.; Katsuya, T.; Ito, N.; Ikushima, M.; Kaibe, M.; Tatara, Y.; Shiota, A.; Sugano, S.; Takeda, S.; et al. Deletion of angiotensin-converting enzyme 2 accelerates pressure overload-induced cardiac dysfunction by increasing local angiotensin II. Hypertension 2006, 47, 718–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gass, J.; Khosla, C. Prolyl endopeptidases. Cell Mol. Life Sci. 2007, 64, 345–355. [Google Scholar] [CrossRef]
- Grobe, N.; Weir, N.M.; Leiva, O.; Ong, F.S.; Bernstein, K.E.; Schmaier, A.H.; Morris, M.; Elased, K.M. Identification of prolyl carboxypeptidase as an alternative enzyme for processing of renal angiotensin II using mass spectrometry. Am. J. Physiol. Cell Physiol. 2013, 304, C945–C953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welches, W.R.; Santos, R.A.; Chappell, M.C.; Brosnihan, K.B.; Greene, L.J.; Ferrario, C.M. Evidence that prolyl endopeptidase participates in the processing of brain angiotensin. J. Hypertens. 1991, 9, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Velez, J.C.; Ierardi, J.L.; Bland, A.M.; Morinelli, T.A.; Arthur, J.M.; Raymond, J.R.; Janech, M.G. Enzymatic processing of angiotensin peptides by human glomerular endothelial cells. Am. J. Physiol. Ren. Physiol. 2012, 302, F1583–F1594. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic representation of the renin–angiotensin system (RAS, left side). The effects of viral occupation (right side) on the failure of the counter-regulatory RAS axis are also depicted (see text for details). ACE = angiotensin converting enzyme, ACE2 = angiotensin converting enzyme 2, AT1 = angiotensin II receptor type 1, AT2 = angiotensin II receptor type 2, RAS = renin-angiotensin system, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Figure 1.
Schematic representation of the renin–angiotensin system (RAS, left side). The effects of viral occupation (right side) on the failure of the counter-regulatory RAS axis are also depicted (see text for details). ACE = angiotensin converting enzyme, ACE2 = angiotensin converting enzyme 2, AT1 = angiotensin II receptor type 1, AT2 = angiotensin II receptor type 2, RAS = renin-angiotensin system, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Angeli, F.; Zappa, M.; Verdecchia, P. Rethinking the Role of the Renin-Angiotensin System in the Pandemic Era of SARS-CoV-2. J. Cardiovasc. Dev. Dis. 2023, 10, 14. https://doi.org/10.3390/jcdd10010014
AMA Style
Angeli F, Zappa M, Verdecchia P. Rethinking the Role of the Renin-Angiotensin System in the Pandemic Era of SARS-CoV-2. Journal of Cardiovascular Development and Disease. 2023; 10(1):14. https://doi.org/10.3390/jcdd10010014
Chicago/Turabian StyleAngeli, Fabio, Martina Zappa, and Paolo Verdecchia. 2023. "Rethinking the Role of the Renin-Angiotensin System in the Pandemic Era of SARS-CoV-2" Journal of Cardiovascular Development and Disease 10, no. 1: 14. https://doi.org/10.3390/jcdd10010014
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.