
Gait Analysis to Monitor Fracture Healing of the Lower Leg


1
Werner Siemens-Endowed Chair for Innovative Implant Development (Fracture Healing), Clinics and Institutes of Surgery, Saarland University, 66421 Homburg, Germany
2
Department of Trauma, Hand and Reconstructive Surgery, Clinics and Institutes of Surgery, Saarland University, 66421 Homburg, Germany
*
Author to whom correspondence should be addressed.
Bioengineering 2023, 10(2), 255; https://doi.org/10.3390/bioengineering10020255
Submission received: 17 January 2023
/
Revised: 7 February 2023
/
Accepted: 13 February 2023
/
Published: 15 February 2023
(This article belongs to the Special Issue Advanced Engineering Technology in Orthopaedic Research)
Abstract
:Fracture healing is typically monitored by infrequent radiographs. Radiographs come at the cost of radiation exposure and reflect fracture healing with a time lag due to delayed fracture mineralization following increases in stiffness. Since union problems frequently occur after fractures, better and timelier methods to monitor the healing process are required. In this review, we provide an overview of the changes in gait parameters following lower leg fractures to investigate whether gait analysis can be used to monitor fracture healing. Studies assessing gait after lower leg fractures that were treated either surgically or conservatively were included. Spatiotemporal gait parameters, kinematics, kinetics, and pedography showed improvements in the gait pattern throughout the healing process of lower leg fractures. Especially gait speed and asymmetry measures have a high potential to monitor fracture healing. Pedographic measurements showed differences in gait between patients with and without union. No literature was available for other gait measures, but it is expected that further parameters reflect progress in bone healing. In conclusion, gait analysis seems to be a valuable tool for monitoring the healing process and predicting the occurrence of non-union of lower leg fractures.
Keywords:
implant; non-union; malunion; motion capture; movement analysis; rehabilitation; tibial fracture; trauma; wearables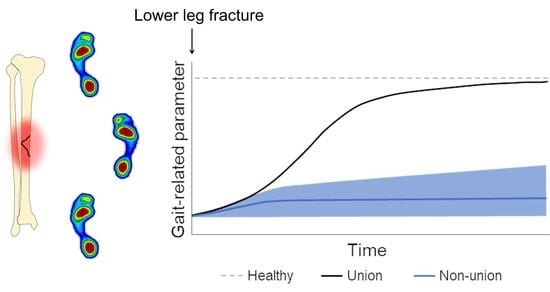
1. Introduction
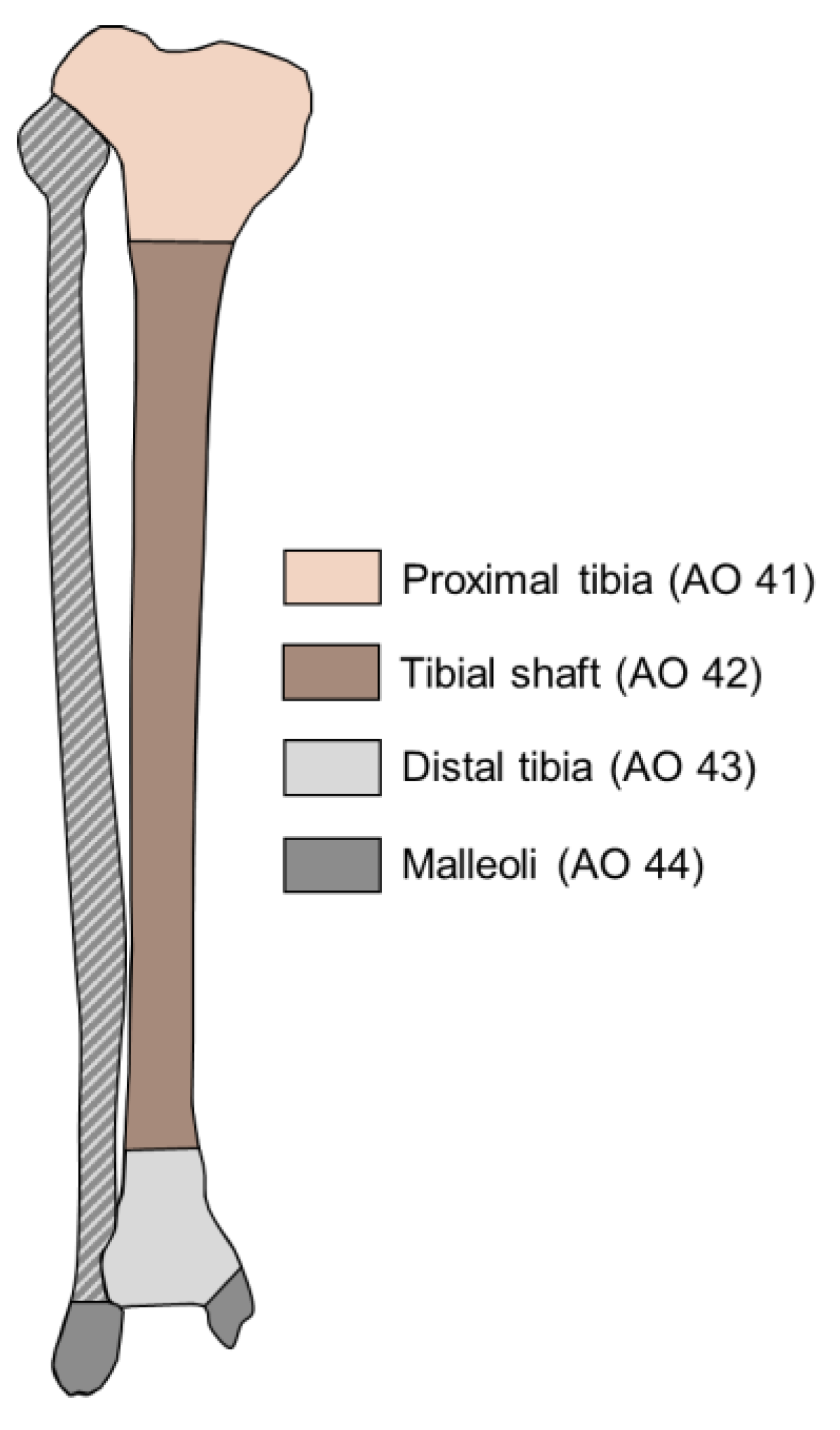
Lower leg fractures include fractures of the tibia or fibula or of both bones combined. The incidence of tibial fractures in Sweden was 52 per 100,000 per year, with proximal tibial fractures (Figure 1) being the most common tibial fractures, followed by tibial shaft and distal tibial fractures, respectively 26.9, 15.7, and 9.1 per 100,000 per year [1]. The incidence of malleolar fractures in Sweden was 152 per 100,000 per year [2]. In some cases, non-displaced fractures are treated conservatively by immobilization using a cast or brace [3]. However, the majority of fractures require surgical treatment, either via external fixation, intramedullary nailing, or via open reduction and internal fixation by screws and/or plates. The mode of surgical fixation depends on the fracture location, fracture type, and soft tissue status (Figure 1). In some cases, e.g., after intramedullary nailing in a tibial shaft fracture, full weight bearing is possible immediately after surgery. In most cases, patients are only allowed partial weight bearing for six weeks or longer, although the benefits of partial weight bearing are currently being re-evaluated [4,5].
Delayed union and non-union are frequent complications in the treatment of long bone fractures and are associated with morbidity, repeated hospitalization, disability, significant functional limitations, and high costs [6,7,8,9]. Definitions of when to classify a non-healing fracture as non-union vary, but a healing period of at least six months after the fracture and more than three months without biological progression seem to be the recent consensus [10,11,12]. Non-union occurs in about 5% to 14% of tibial fractures [13,14] and is classified as either hypertrophic (abundant callus formation) or atrophic (no callus formation) [15]. Known contributing factors are multiple and open fractures, as well as smoking, alcoholism, diabetes, high body mass index, and male sex [13]. Biomechanical and biological factors both play crucial roles in fracture healing and include the fracture gap size, implant stiffness, and the extent of soft tissue damage [16]. Delays in bone healing may currently either be addressed by non-invasive interventions such as pulsed ultrasound, shockwaves and electromagnetic fields, or by revision surgery [11,17].
In clinical practice, the progress of fracture healing is typically monitored by infrequent radiographs that come at the cost of radiation exposure and reflect fracture healing with a time lag, as fracture mineralization occurs later than the increases in stiffness [18]. The inability to monitor the current healing progress in a timelier manner often results in treatment delays. In experimental studies, changes in stiffness or displacement were monitored continuously at the fracture site through sensors attached to the implants. This approach is, however, not yet established for daily clinical routine today and requires special and more expensive implants [19,20]. In addition, it would be desirable to predict fracture healing problems as early as possible to intervene sooner. It thus seems beneficial if further non-invasive diagnostic options could be made available to monitor the progress of fracture healing. Advanced gait analysis is a candidate that might enable for such predictions, potentially by combining several relevant gait parameters and by using regression models or machine learning.
During routine clinical visits, the gait pattern and ability to walk are usually visually inspected by the healthcare professional. Objective gait measures validated to predict the occurrence of non-union have, however, not yet been identified. It is highly desirable to explore such parameters and the possibility to monitor fracture healing via objective gait analysis, i.e., by optical motion capture, wearable sensors, or ground reaction force measurements.
In this narrative review, we provided an overview of what is known about characteristic gait changes throughout the fracture healing process and which gait parameters might be candidates to predict malunion or non-union of the lower leg early on. We included studies with both, surgical and non-surgical treatment. We also present suggestions for which gait aspects should be explored in future studies as potential parameters to predict fracture healing problems.
2. Materials and Methods
Pubmed was searched for studies that analyzed gait-related measures after lower leg fractures. A combination of search terms was used to find relevant studies for this review. The search terms at least included a part about gait (“gait” OR “walking”), fractures (“fracture”), and the lower leg (“lower leg” OR “tibia” OR “fibula” OR “ankle”). Additional search terms indicating a specific measurement method or gait-related parameters were occasionally added.
Studies with conservative or surgical treatment were included. Studies about stress fractures were excluded. Studies in languages other than English, German, or Dutch were also excluded. The references of the studies that were included were manually checked for other studies on this topic. In total, thirty studies were found that measured gait-related parameters at least once after a lower leg fracture (Table 1).
3. Changes in Gait throughout the Healing Process after Lower Leg Fractures
3.1. Spatiotemporal Gait Parameters
Spatiotemporal gait parameters are frequently measured to determine gait deviations. There are several systems available that can be used to extract spatiotemporal gait parameters, such as 3D optical motion capture systems [35,43], electronic walkways (pressure-sensitive mats) [8,44], and inertial measurement units (IMUs) [27]. The spatiotemporal gait parameters can be divided in different gait domains, i.e., pace, rhythm, variability, and asymmetry [49,50]. Spatiotemporal gait parameters that have already been assessed in the context of lower leg fractures are described below per gait domain. In all the described studies, the patients walked at their self-selected speed on an over-ground walkway.
3.1.1. Pace
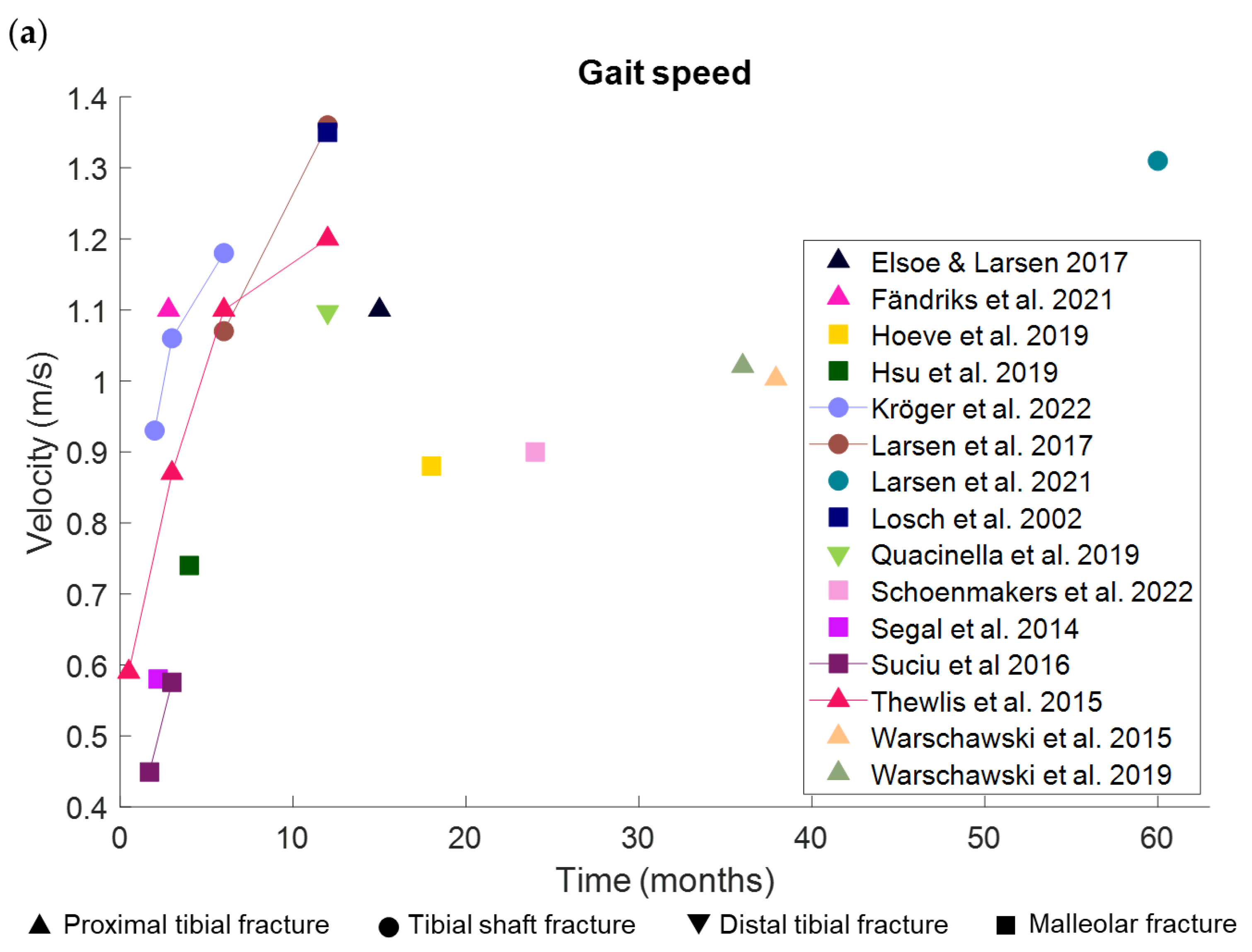
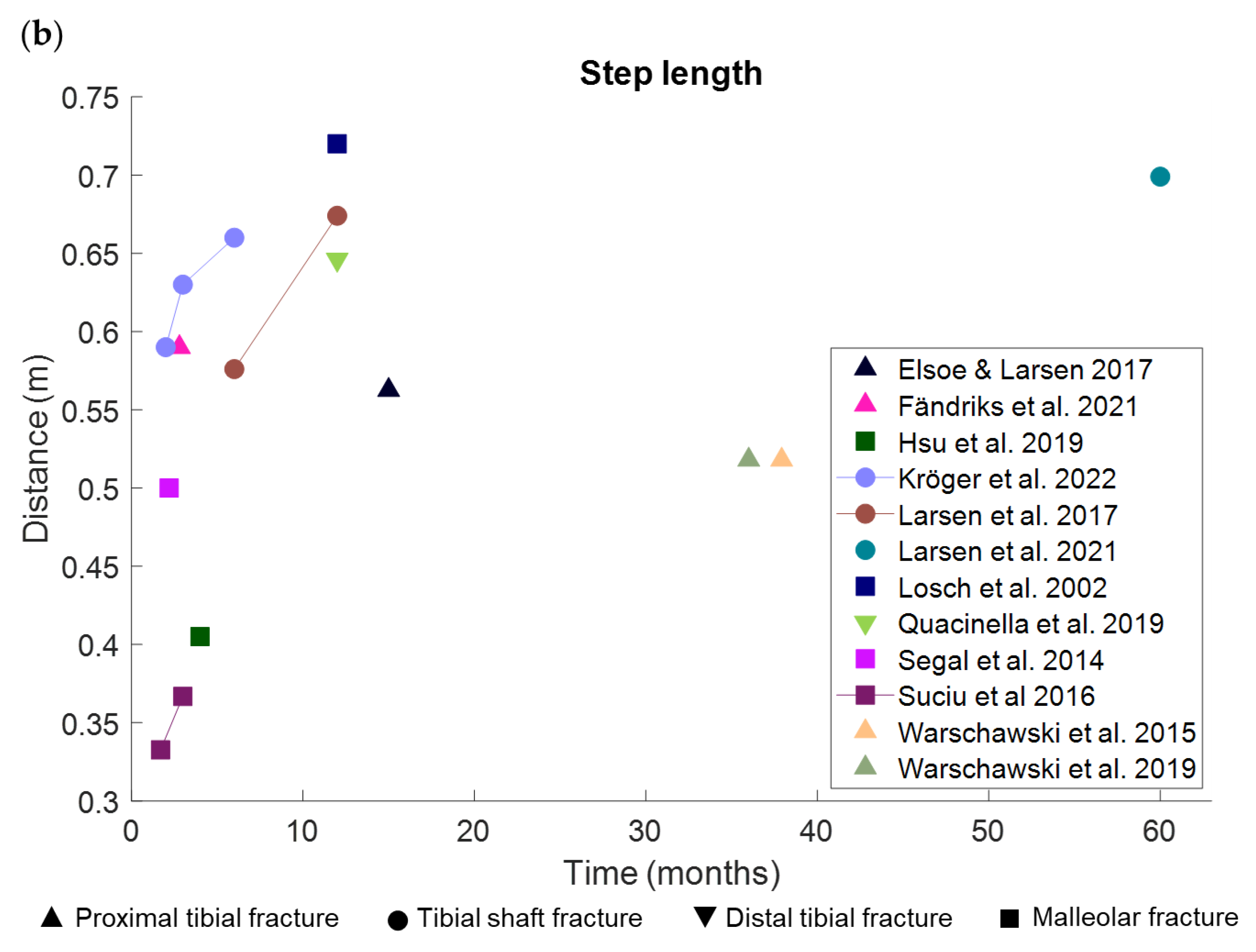
The pace-related gait domain consists of the parameters gait speed and step length. In the context of lower leg fractures, we found four studies that measured gait speed and three of these studies also measured step length throughout the healing process after proximal tibial, tibial shaft and malleolar fractures (Figure 2) [35,37,45,46]. These studies showed significant increases in gait speed and step length of the injured side over time. Twelve months after surgery, one study with tibial plateau fractures and another study with tibial shaft fractures did not find significant differences in gait speed anymore compared to healthy controls [8,37]. Multiple other studies that presented cross-sectional data ranging from about two months to five years after surgery or injury from patients with all types of lower leg fractures showed that gait speed and step length remained significantly shorter in patients compared to controls [7,29,30,31,35,39,42,43,44].
3.1.2. Rhythm
Gait parameters from the rhythm domain that were reported by studies analyzing gait after a lower leg fracture were single-limb support time, cadence, swing time, stance time, and step time. Only the results for the injured side will be described below. Single-limb support time was the most frequently reported rhythm-related parameter. In some studies, it was reported in percentage of the gait cycle [7,44,45], while in others, it was presented in seconds [8,37,38,42]. From 6 to 12 months after surgery, cadence and step time increased in proximal tibial and tibial shaft fractures [25,51]. The single-limb support time increased between 6 and 12 weeks after surgery in patients with malleolar fractures but remained significantly shorter compared to healthy controls [45]. The single-limb support time did not change between 6 and 12 months after surgery for tibial shaft fractures [37]. The few studies that compared rhythm-related parameters with healthy controls showed that the single-limb support time between six weeks and three months after surgery and the cadence at four months and three years after surgery were both lower in patients after proximal tibial and malleolar fractures [7,31,44,45]. The stance time was shorter in the injured leg compared to the non-injured leg, but there was no significant difference between the injured leg and controls six to eight weeks after surgery for proximal tibial fractures [29]. Another study also found no significant differences between the stance time of the injured leg and that of healthy controls about three months after malleolar fractures [45]. Several other studies only reported rhythm-related parameters measured at one time point and did not compare their results with healthy controls, which makes it difficult to draw conclusions from these data with regard to the present questions [8,38,42,48].
3.1.3. Variability
The stance time and swing time variability in patients after proximal tibial and tibial shaft fractures were reported only by one and two studies, respectively. The swing time variability showed 8% asymmetry between the injured and non-injured leg 12 months after frame removal following ring fixation of proximal tibial fractures in 23 patients [8]. The stance time variability was increased in the injured leg following a tibial shaft fracture in 49 patients, and it decreased significantly from 6 to 12 months after surgery [37]. It remained slightly higher in the injured leg compared to the non-injured leg five years after surgery (significance not tested) in another study with 29 patients with tibial shaft fractures [38].
3.1.4. Asymmetry
Four studies reported one or more asymmetry-related parameters after proximal tibial and tibial shaft fractures [8,35,37,38]. Step length asymmetry is the percentage difference in step length between the injured and non-injured sides. Step length asymmetry decreased throughout the first months after surgery for tibial shaft fractures in 23 patients from 18.2% at two months to 5.5% at six months but was still higher six months after the surgery compared to healthy controls [35]. From the 6th to the 12th month after surgery, step length asymmetry, single support time asymmetry, and swing time asymmetry decreased significantly in 49 patients with tibial shaft fractures [37]. One study reported symmetry values based on the trunk acceleration signal characteristics in anterior–posterior and vertical directions in 10 patients with malleolar fractures [31]. Only the symmetry in the vertical acceleration signal was lower compared to healthy controls about four months after injury.
3.1.5. Spatiotemporal Gait Parameters Are Associated with Gait Speed
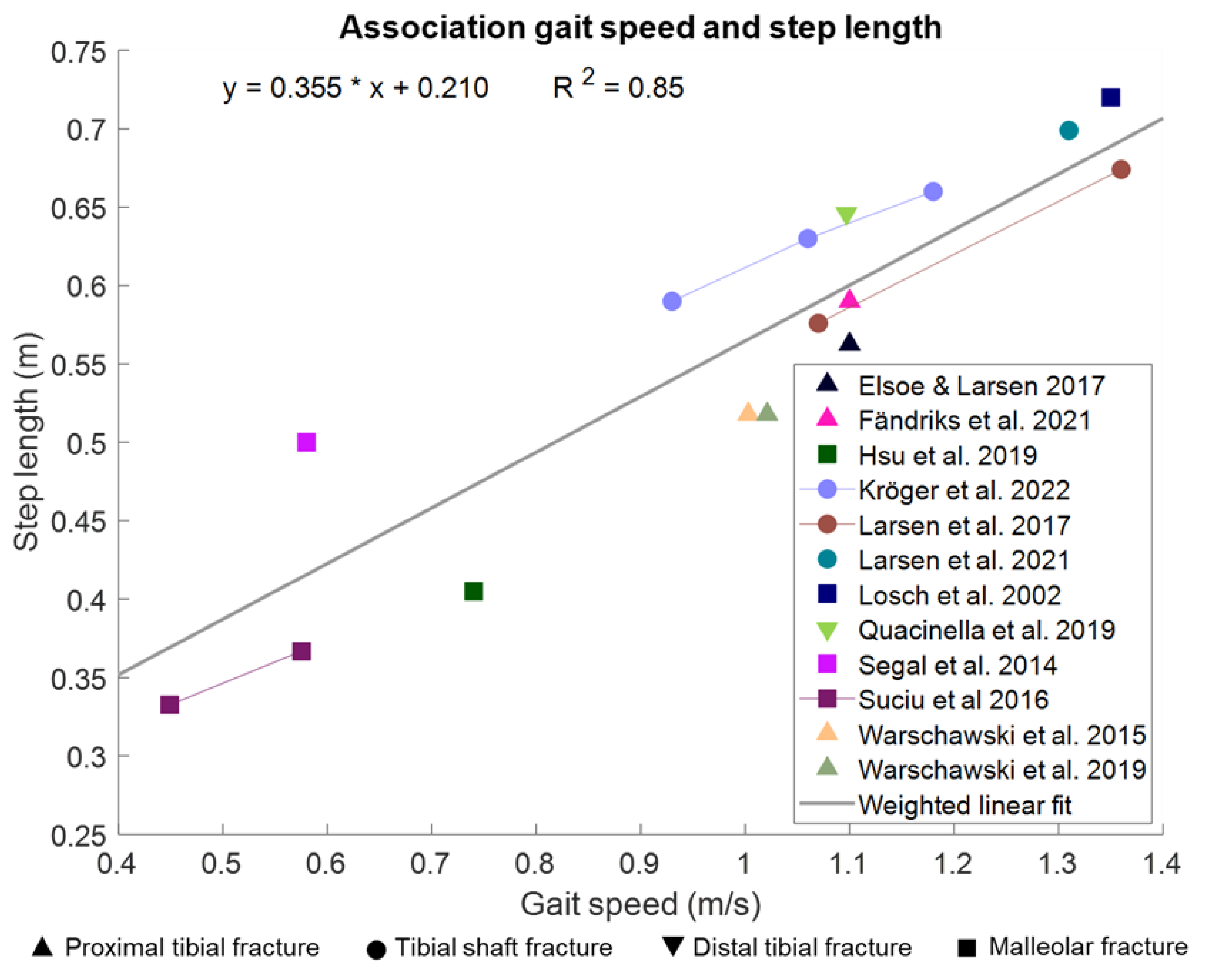
It is known that gait speed is associated with gait-related parameters in healthy adults [52,53]. Gait-related parameters improve with an increase in gait speed. We have pooled the data from the studies that measured gait speed and step length of the injured side that was described in the preceding paragraphs. We used the average values of these lower leg fracture studies and weighted them by the number of patients in the study. A weighted correlation showed a significant linear association between gait speed and step length (R2 = 0.85, p = 0.001, Figure 3), as expected based on the literature [54,55]. For the rhythm-related and variability-related gait parameters, there are currently not enough lower leg fracture studies available that could be used to pool the data to analyze a potential correlation. However, from existing literature on healthy adults, we know that the rhythm-related parameters change with gait speed. With higher speed, the cadence increased, and the temporal parameters decreased [52,53]. The spatiotemporal variability-related parameters slightly decrease with increasing walking speed [56] and increase with a decrease in walking speed [57]. The asymmetry-related gait parameters do not seem to be influenced by gait speed [58].
3.2. Kinematics
Kinematics are regularly assessed to obtain joint angles during a specific phase of the gait cycle or to obtain the range of motion (ROM). To measure kinematics, several technical solutions are available. To date, the gold standard is 3D optical motion capture systems that assess the exact position of markers located on the body and their position changes during movement in the 3D space [23,35,47]. There are also systems available that can be more easily used outside of the lab, such as IMUs, [27] and markerless motion capture based on video data [59]. IMUs are wearable sensors that are usually fixed to one or multiple body segments and measure acceleration and angular velocity. By placing IMUs on consecutive body segments, the joint angle between these two segments can be calculated. Markerless motion capture systems often use multiple synchronized cameras to detect the pose of one or multiple individuals based on machine learning models [59].
We found two studies that analyzed joint kinematics during walking more than once during the healing process after tibial fractures [23,35]. In one study with proximal tibial fractures, 18 patients were measured six times in the two years after the fracture [23]. This study showed that the hip functions had already returned to a normal pattern after six weeks, whereas for the knee and ankle, it took 26 weeks to function close to a normal pattern. Even after two years, the maximum knee flexion and the plantarflexion were still smaller in the injured leg compared to healthy controls. In the other study, 23 patients with tibial shaft fractures were measured three times within six months after the fracture [35]. This study showed that the knee flexion of the injured leg during the swing phase already returned close to normal in the first three months. Between three and six months post-surgery, the ankle plantarflexion during pre-swing and hip extension during stance improved but remained smaller compared to controls. Knee flexion during loading response and ankle dorsiflexion during the stance phase did not significantly increase throughout the 6 months and remained significantly smaller compared to controls.
Several studies that measured the kinematics after lower leg fractures showed that not all joint kinematics returned to similar values as controls [27,29,30,39,43,47]. This could partly be due to the lower walking speed of patients compared to controls, as gait speed is known to influence joint kinematics [52,53]. However, two studies compared the kinematics of patients at normal speed with controls walking at slow walking speeds, measuring at rather similar gait speeds, and still found significant differences between the groups [30,43]. Moreover, the location of the fracture might influence which joint kinematics return (faster) to control-like values and which remain altered. In patients with a proximal tibial fracture, the maximum knee flexion angle during the swing phase remained lower compared to controls after two years [23], whereas in patients with a tibial shaft fracture, the knee flexion during the swing phase returned close to normal in the first three months after surgery [35].
3.3. Kinetics
The forces and moments acting on the body during walking are often measured with force plates and optical motion capture systems. Changes in ground reaction forces, joint moments, and the generated power during walking throughout the rehabilitation process after lower leg fractures are described below.
3.3.1. Ground Reaction Forces
The vertical ground reaction force (vGRF), measured by force plates or pressure sensors during walking, is characterized by a double-peak pattern (two maxima with a minimum in between). The first peak occurs during loading and the second peak during push-off [32,34,35]. The height of the peaks is normally presented as a percentage of body weight. The two peaks did not significantly increase between the second and third month after surgery, but they did significantly increase from the second and third month to the sixth month after surgery in patients with tibial shaft fractures [35]. The two maxima were, however, still significantly lower compared to healthy controls six months after surgery. This could, at least partially, be because of the lower gait speed of the patients since vGRF is smaller in lower gait speeds [52]. Three to six months after the removal of a circular Ilizarov frame, a type of external fixator that can be used to treat fractures, there were no differences in peak forces anymore between the injured and non-injured leg in patients with proximal tibial fractures [32]. Another study used the vGRF to determine the changes in weight bearing of patients with tibial fractures over time and found a moderate correlation between weight bearing with fracture stiffness [34].
3.3.2. Joint Moments
Joint moments are calculated based on the kinematic data and the GRF data during walking. Two studies that measured joint moments while walking multiple times after the surgery in patients with tibial fractures showed significant increases in hip, knee, and ankle moments during the stance and loading response phases within the first six months after surgery [35,46]. Between 6 and 12 months after surgery, the knee joint reaction forces did not significantly increase further [46]. Six months after the surgery, joint moments were still significantly lower in patients compared to controls [35]. Another study that measured 12 months after surgery in patients with malleolar fractures showed significantly lower plantar flexion moments in patients compared to controls but did not find differences in dorsal flexion moments between the groups [39].
3.3.3. Generated Power
Two studies looked at how much power was generated in the knee and ankle joints during walking [29,35]. The generated power is calculated as a product of the moment and angular velocity of the joint. The generated power increased significantly between two and six months after surgery in patients with proximal tibial fractures but remained significantly lower compared to controls at six months [35]. About three months after a proximal tibial fracture, the generated power was lower in the injured leg compared to the non-injured leg and compared to controls [29].
3.4. Pedography
Pedography captures the plantar pressure of the foot with a pressure plate or with pressure-measuring insoles. Studies have shown that at least one year after a lower leg fracture, the plantar pressure has moved more laterally compared to the non-injured side [21,22,28,33,40]. Especially under the fourth metatarsal, the pressure increased compared to the non-injured side in distal tibial fractures, and there was less loading in the heel and first metatarsal region [28,33]. Similar results were found for the force-time integral, which was higher in the fourth and fifth metatarsal regions and lower in the heel and first metatarsal regions [28,33]. The pedographic results seem to correlate with clinical scores in distal tibial fractures, such as the American Orthopeadic Foot and Ankle Society score, visual analog scale, Phillips scores, Ovadia-Beals score, Teeny-Wiss score and Takura score [21,33].
Two studies used pressure insoles to measure patients during daily living [24,36]. In one study where the insole was worn in a walking boot, a posterior shift of the center of pressure was found in seven patients in the weeks following surgery for tibial shaft or malleolar fractures [36]. The other study that analyzed 10 patients after malleolar fracture identified significant correlations between weight bearing during daily living and the visual analog pain scale, the Olerud–Molander score, and the American Orthopeadic Foot and Ankle Society score [24].
3.5. Muscle Activity and Mass
Electrical activity in the muscle can be measured with electromyography. Little is known about muscle activity after lower leg fractures. A cross-sectional study showed that muscle activity patterns did not significantly differ between the injured and non-injured leg in 17 patients that were measured once between 9 months and 14 years after free-flap reconstructions because of open tibial fractures [40]. They found, however, high variability in muscle activity patterns between patients.
Muscle cross-sectional area, as well as muscle volume of the lower leg, decreased during the immobilization phase with a cast after ankle fractures, measured in 18 patients with longitudinal magnetic resonance imaging [41]. The cross-sectional area of the tibialis anterior, gastrocnemius medialis, and gastrocnemius lateralis muscles stopped decreasing after about 30 days in a cast, whereas the soleus muscle was still decreasing at the last measurement point at 43 days in a cast. The total muscle volume in the injured leg was reduced by 16% due to immobilization and in the non-injured leg by 7%. Another study showed that after the removal of the cast following a malleolar fracture, the muscle strength was significantly lower in the injured leg compared to the non-injured leg [26]. Following a rehabilitation program, there were no significant differences anymore between the injured and non-injured leg at three and six months after cast removal.
4. Predicting Non-Union Based on Gait
About 5% to 14% of patients experience delayed union or non-union following lower leg fracture [13,14]. Multiple studies with large sample sizes will be needed to be able to determine which gait factors can predict union problems. So far, only a few studies have reported gait parameters in patients with union problems after fractures of the lower leg. Patients with delayed union were only able to bear 40% of their weight at 20 weeks post-surgery, measured with pedography, whereas patients with union were able to bear their full weight at that time [34]. Another study that measured pedography data with insoles in seven patients with tibial shaft or malleolar fractures for several weeks showed that one patient with non-union shifted the center of pressure (COP) anteriorly and that it remained near the forefoot over time, whereas the patients with union moved their COP posteriorly toward the heel [36]. Another study reported about patients with unsuccessful results (not solely non-union) and showed decreased loading of the lateral forefoot, whereas patients with successful results showed an increased loading of the lateral forefoot compared to the non-injured side [22]. From the described studies in this review, only studies with pedography assessed differences in gait-related parameters in non-union patients. The results from these studies are promising; however, a larger sample size is required to really draw conclusions from the data. Moreover, other gait measures than pedography should be explored regarding their potential to predict non-union early. We expect that also, in the spatiotemporal, kinematic, and kinetic gait measures, there will be parameters that have the potential to predict non-union. A combination of multiple gait-related parameters that change with fracture healing will provide a more accurate prediction of the healing process.
5. Discussion
In this review, we provided an overview of how gait changes throughout the healing process of lower leg fractures in patients with union. We also explored whether gait can be used to predict union problems in a timelier manner.
Improvements were found in all gait-related parameters that were measured longitudinally after a lower leg fracture with normal healing. Spatial parameters, joint kinematics, kinetics, and weight bearing increased, and temporal parameters decreased in the months following a lower leg fracture. However, not all parameters returned to normal values within several months after the injury. Gait speed is an important parameter to monitor since it increases throughout the healing process, and many gait-related parameters improve with increasing gait speed. Only very few studies described gait-related parameters in patients with non-union fractures, but pedography showed clear differences between patients with union and patients with non-union.
Gait analysis to monitor fracture healing could reduce the number of radiographs that are currently made. Radiographs will still be required to diagnose the fracture, check the position of the implant, analyze fracture reduction, and make sure via a final radiograph that the fracture has healed properly. The number of radiographs during the healing phase can be reduced when gait analysis is used to monitor fracture healing, and the gait pattern improves as expected. The final radiographs to make sure the fracture healed properly could, for example, be made when the gait asymmetry has returned to normal values. This has the potential to reduce the number of clinical visits after a fracture.
There was a large variance between the studies in terms of the types of fractures, type of implants, partial weight bearing or immobilization, the time after injury that gait analysis was performed, the equipment used for the gait analysis, and the parameters extracted. Nonetheless, multiple types of gait-related parameters improved during the first year(s) after a lower leg fracture. Therefore, gait analysis might be a suitable tool to monitor the healing process.
Different types of lower leg fractures were included in this review. Based on the limited available data, it is difficult to say whether the gait pattern improves in a similar fashion or if there are differences among fracture types. Several studies compared different ankle fracture types with each other and found significant differences in gait parameters [27,30]. The spatiotemporal gait parameters were significantly better in patients with a unimalleolar fracture compared to bimalleolar and trimalleolar fractures [27]. Ankle fracture severity correlated with the ROM of the ankle during walking [30]. However, these studies have not analyzed how the gait pattern changes throughout the healing process by, i.e., comparing the longitudinal gait parameters in different fracture types.
Besides the type of fracture, also the type of implant can have an effect on the gait parameters, especially when comparing a nail versus a plate. Patients with a plate often need to adhere to restricted weight-bearing instructions throughout the first few weeks after the surgery. This will affect the gait pattern differently compared to patients with a nail, who are often allowed to fully weight-bear shortly after the surgery.
To be able to interpret gait changes, it is necessary to know the gait alterations typical for specific patient cohorts. It is known that several factors, such as age, body weight, and pain, influence the gait pattern. With increasing age, gait becomes more cautious, and reductions of the preferred gait speed, cadence, and step length can be observed, while gait variability and asymmetry measures remain stable over time [60,61]. In people with obesity, the spatiotemporal gait parameters, joint kinematics, and pedography show significant differences compared with normal-weight-matched control groups [62,63]. Pain is also known to influence gait. Plantar heel pain causes reductions and changes in the GRF-based gait parameters [64]. Chronic joint pain is associated with poor gait performance, quantified by several spatiotemporal gait parameters [65]. Therefore, these kinds of factors should be taken into account when interpreting the gait data.
In the studies analyzed in this review, the average of all study age averages pooled is 44 years. However, most studies also provided the range of the age of the patients. The average number of years between the youngest and oldest participants is 48 years. This indicates that in most studies, the age range was rather large, which could have potentially led to differences within studies and also between studies.
Another important factor that should be taken into account in gait analysis is gait speed. Several gait-related parameters are known to change with gait speed [52,53]. It is currently unknown whether the improvements in gait after a lower leg fracture are solely due to an increase in gait speed or whether the gait pattern also improves besides the improvements due to an increase in gait speed. Since gait speed has a large effect on several gait-related parameters, it appears to be one of the most important parameters to track during the healing process.
Several gait-related parameters were still significantly different from controls months to multiple years after the injury. The current literature and data do not explain why these parameters do not return to control-like values, but possible reasons include persisting pain, damage and scarring of the soft tissues due to the injury and surgery, losses of sensation and proprioception, alterations of neuromuscular interaction, as well as losses in muscle strength and mass. Patients lose muscle strength and mass due to the immobilization and restrictions in weight bearing during the first weeks after the fracture [41]. Moreover, patients are, in general, likely to be less active because they are limited in the activities that they can perform. After immobilization or restricted weight bearing, the muscle mass and strength will increase again. Three months after the removal of the cast, there was no longer a difference in muscle strength between the injured and non-injured leg [40]. Similar results were found after 90 days of bed rest; the calf muscle cross-sectional area returned to baseline values after about 100 days [66]. However, in many patients with fractures, muscle strength never returns to pre-injury values [67].
Multiple studies showed that several patients were not pain-free one or multiple years after a lower leg fracture [28,38,39]. An association between the pain level in the foot and the gait performance measured with the Edinburgh visual gait score was shown based on normal video recordings in patients with malunited tibia fractures treated with external fixation [68]. It is also known that in other medical conditions with pain, such as plantar heel pain and chronic joint pain, the gait pattern is different from healthy controls [64,65]. Therefore, pain after the injury certainly contributes to gait changes.
Several other factors that are known to influence the gait pattern, in general, are age, body weight, physical function, and cognition [60,63,69,70]. Most of these factors will not change substantially during the healing process of a fracture and thus only have a small influence on the changes in the gait pattern. However, these demographics-induced differences in gait patterns between patients make it hard to compare fracture healing between patients. We, therefore, recommend looking at changes in the gait pattern within patients throughout the healing process. Moreover, especially in people at high age, with low physical function and comorbidities, these factors may influence the healing process and might need to be taken into account when monitoring the course of fracture healing based on the gait pattern. In this population, a period of inactivity can further reduce their function, and a large part of these patients might not return to pre-injury levels of mobility anymore, as was seen after hip fractures [71]. A high body weight will not only affect the gait pattern but might also have an effect on fracture healing. The healing process after a fracture took longer in obese mice compared to non-obese mice [72].
5.1. Predicting Non-Union Based on Gait
Several studies showed that gait analysis has the potential to detect healing problems based on gait-related parameters. The plantar pressure distribution and weight bearing were different in patients with healing problems [22,24,34,36]. Differences were found between healing and non-healing patients in pressure distribution already about 2 months after surgery for tibia shaft or malleolar fractures [36]. This is sooner than radiographs allow to determine healing problems. This shows that gait-related parameters have the potential to detect union problems early on. There are still many gait parameters that have not yet been analyzed in relation to bone healing problems. Longitudinal studies with a large sample size that include multiple patients with healing problems are required to analyze the relation between gait-related parameters and the occurrence of healing problems.
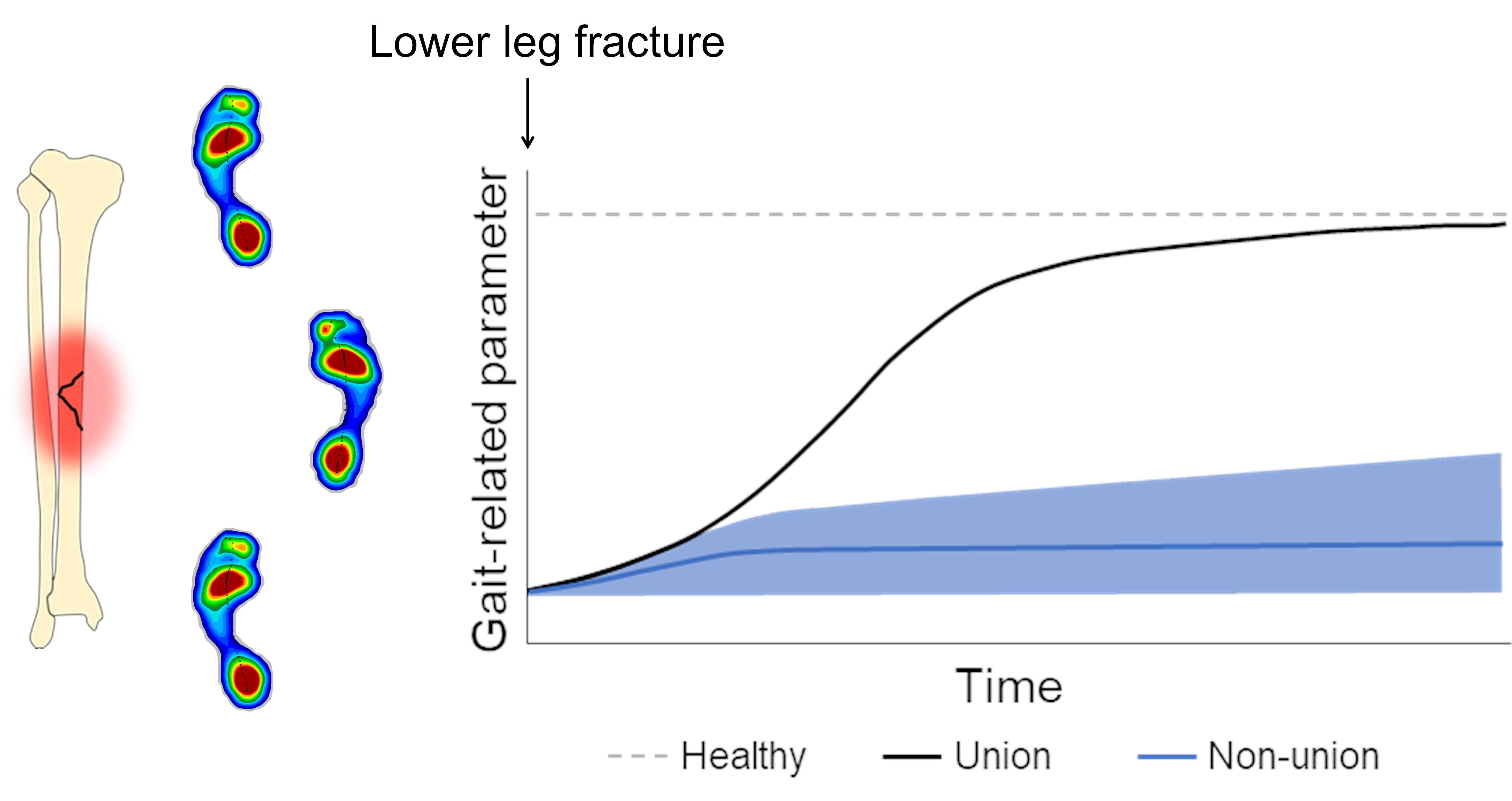
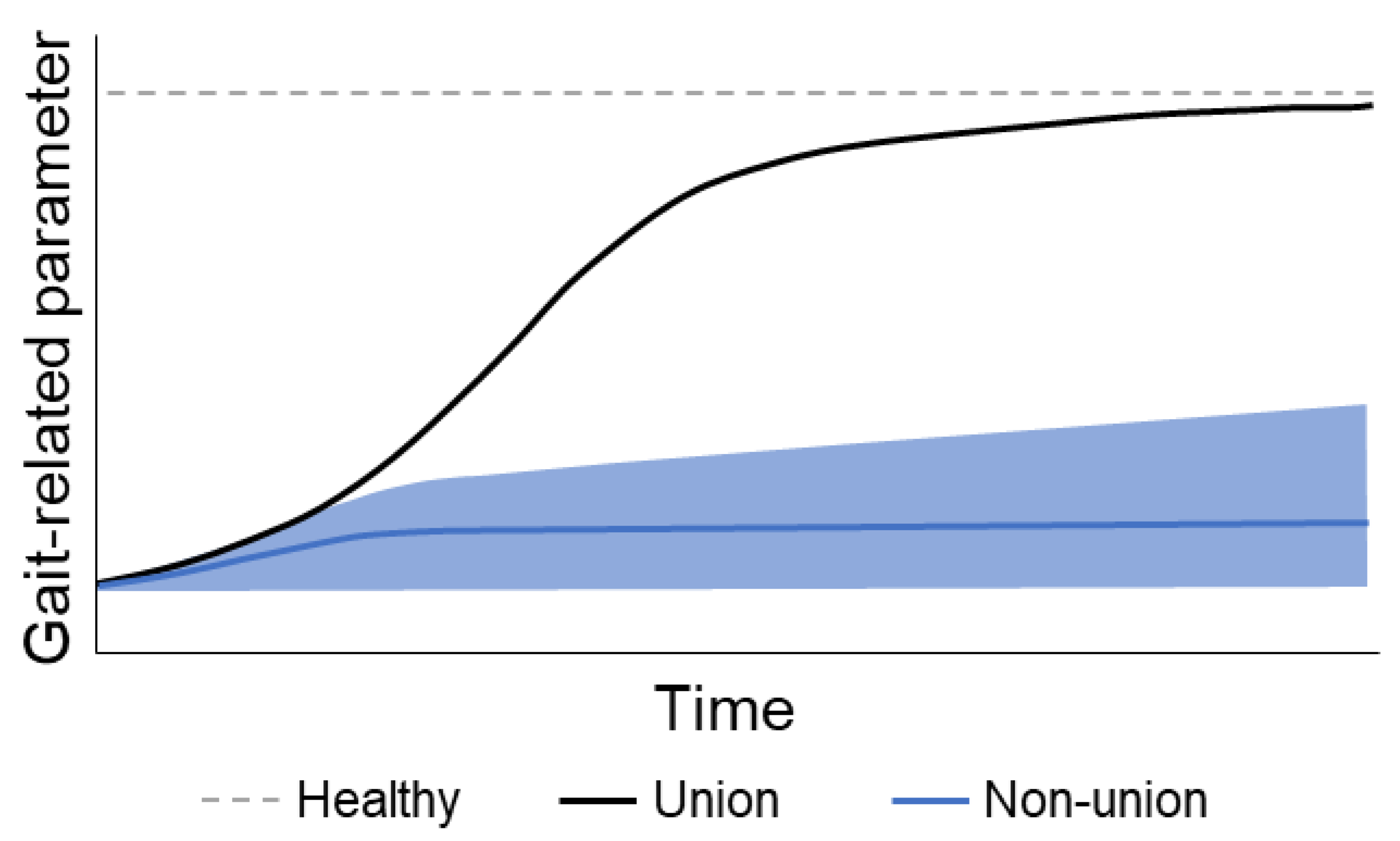
We expect that in patients without healing problems, gait-related parameters will improve over time and that there will be only minor improvements seen in patients with healing problems. This hypothetical relationship between time and healing in patients with and without healing problems is depicted in Figure 4. This relationship can be influenced by, e.g., type and severity of the fracture, soft tissue damage, and type of implant. Moreover, factors such as age, body weight, cognition, comorbidities, and fear of falling might determine which values the gait-related parameters will return to in patients without healing problems.
5.2. Suggestions for Future Research Analyzing Gait after Lower Leg Fractures
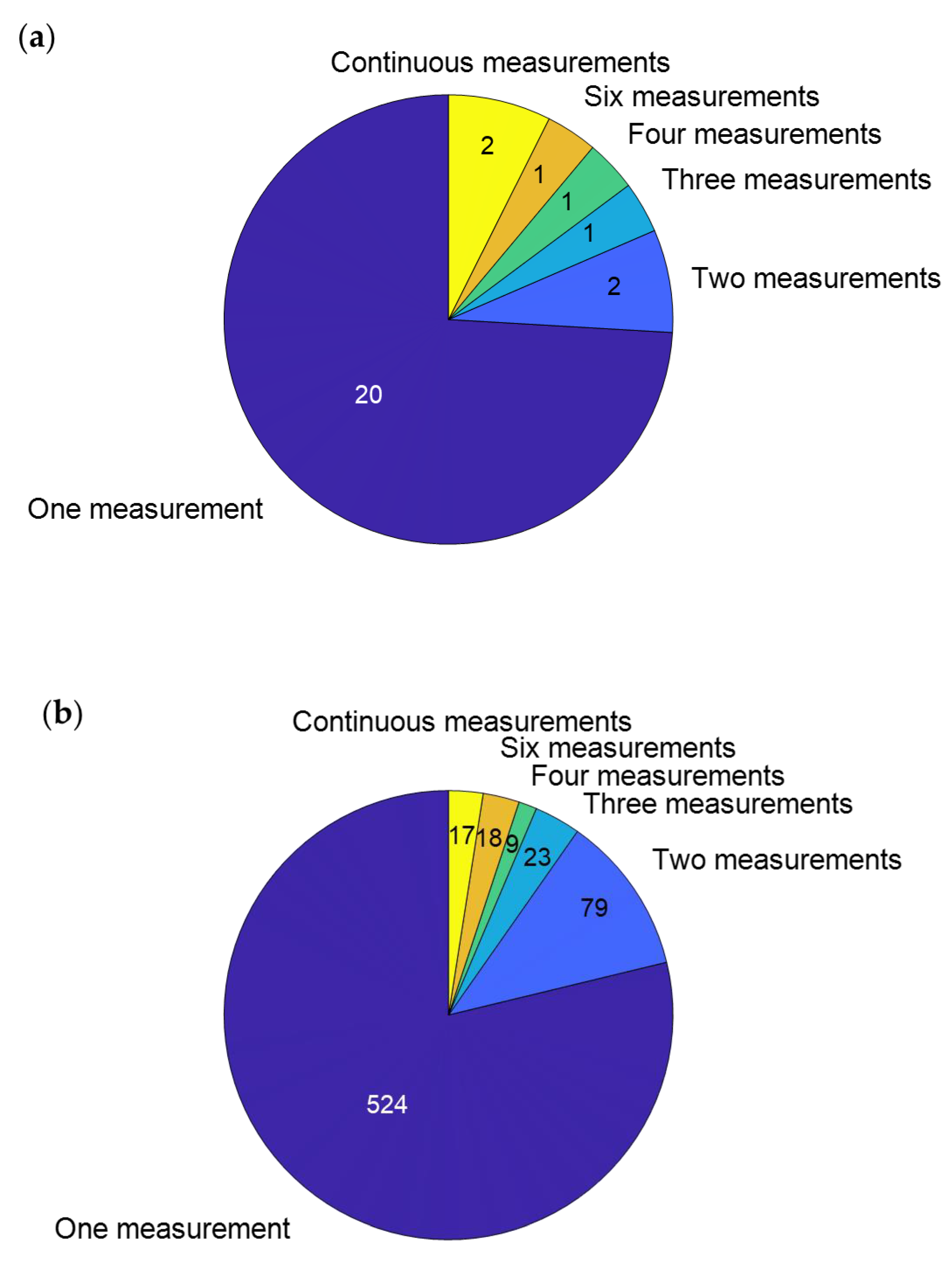
Gait analysis has the potential to monitor the fracture healing process. However, more data about changes in gait-related parameters throughout the healing process are required to determine how the gait changes in patients with union and non-union. Most of the described studies only measured the gait pattern once (Figure 5); however, to monitor the healing process, multiple measurements are required. We suggest analyzing the gait pattern multiple times within the first year. However, to analyze when and if the gait pattern fully returns to normal values, measurements might even need to take place beyond one year after the injury.
After a lower limb fracture, a large part of the patients is asked to perform partial weight bearing for a certain period of time. The time and duration of no or partial weight bearing differed quite a bit between the studies that reported this information. It is known that it is difficult to adhere to partial weight-bearing instructions [5,73]. Nonetheless, to be able to look into the effects of partial weight-bearing strategies or immobilization after a lower leg fracture, it would be helpful if future studies could report this information.
Several studies compared the gait-related parameters of the injured leg with the non-injured leg [32,33,37,38]. However, it could be that the gait pattern of the non-injured leg has also changed because of changes in walking speed or compensation and adaptation due to the injury in the other leg. Therefore, we recommend comparing the results to a control group with comparable characteristics (e.g., age, body weight) since they are known to influence the gait pattern [60,63,69,70]. In case the patients and the matched control group are not measured at the same gait speed, if possible, a correction for gait speed should be performed for the parameters that change with gait speed for a fair comparison between the groups. Gait speed should also be taken into account when comparing longitudinal measurements within patients.
Asymmetry parameters might be a suitable measure to quantify fracture healing. The asymmetry is high shortly after the fracture and decreases throughout the healing process. An advantage of asymmetry measures is that they are not influenced by gait speed and age [58,74]. Therefore, we recommend measuring the asymmetry of gait-related parameters throughout the healing process.
A very promising approach is to analyze signal characteristics of the gait data, such as via accelerometers. An accelerometer on the trunk was used to look at movement intensity by calculating the root mean square of the acceleration and studying symmetry and regularity based on the calculation of autocorrelation [31]. There are more signal characteristics, such as entropy, smoothness, Lyapunov exponent, and harmonic ratio, that could be explored to monitor changes in the gait pattern during fracture healing.
Most studies performed the data collection in the clinic and measured either only once or at multiple time points. With all the wearable devices on the market, it would also be possible to measure gait-related parameters continuously in the normal environment of the patient’s everyday life. Continuous data may provide additional and relevant information about fracture healing. We only found two studies that monitored gait continuously for several weeks after a lower leg fracture. These studies used pressure-sensitive insoles that were already described in the Section 3.4. To our knowledge, there have been no studies using other wearable devices for continuous monitoring of gait parameters after lower leg fractures. Tools that might be particularly suitable are accelerometers and/or gyroscope-based devices. These have already been used frequently in other patient groups for continuous measurements [75]. These devices can also be used to obtain simple quantitative gait or physical activity measures, such as the number of steps. Daily step count or physical activity is known to increase after lower leg fractures [76] and could potentially also be used to monitor fracture healing.
To implement gait analysis in routine clinical care, it needs to be clarified which gait parameters can differentiate between normal healing and delayed or non-union. Not all of the available equipment used for gait analysis is suitable for a quick assessment in clinical practice. Wearable sensors, such as pressure-sensing insoles and IMUs, are devices that can be used relatively fast and easily to quantify the gait pattern. Additionally, an appropriate software package that can instantly analyze the data and report on the gait quality and the healing process needs to be developed.
A limitation of this review is that there were few studies found that presented longitudinal patient data. The studies with a single measurement often measured at different time points after the injury. By combining those studies, it was still possible to see improvements in the gait pattern; however, more longitudinal studies would have been desirable.
6. Conclusions
Gait analysis can be used to determine changes in the gait pattern after lower leg fractures. In patients with union, the spatiotemporal parameters, joint kinematics, kinetics, and pedographic measures improved in the months following the fracture. Three studies with pedograpic measures were able to show differences in the changes in gait patterns during the healing process in patients with and without union. These differences in patients with healing problems were detected earlier than would have been possible with radiographs. Therefore, gait analysis can be used to monitor the healing process and to predict the occurrence of non-union of the lower leg. However, several steps still need to be taken before gait analysis can be implemented in routine clinical care to monitor fracture healing of the lower leg.
Author Contributions
Conceptualization, E.W. and B.G.; methodology, E.W.; software, E.W.; validation, E.W.; formal analysis, E.W.; investigation, E.W.; resources, E.W.; data curation, E.W.; writing—original draft preparation, E.W.; writing—review and editing, B.G., M.O., and T.P.; visualization, E.W.; supervision, B.G.; project administration, B.G.; funding acquisition, T.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Werner Siemens Foundation (project Smart Implants 2.0). We acknowledge support by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) and Saarland University within the ‚Open Access Publication Funding‘ program.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data can be extracted from the cited papers.
Conflicts of Interest
T.P. is president elect and board member of the AO Foundation, Switzerland, and extended board member of the German Society of Orthopedic Trauma Surgery (DGU), the German Society of Orthopedic Surgery and Traumatology (DGOU), and the German Society of Surgery (DGCH). T.P. is also the speaker of the medical advisory board of the German Ministry of Defense. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. The other authors declare no conflict of interest.
References
- Wennergren, D.; Bergdahl, C.; Ekelund, J.; Juto, H.; Sundfeldt, M.; Möller, M. Epidemiology and Incidence of Tibia Fractures in the Swedish Fracture Register. Injury 2018, 49, 2068–2074. [Google Scholar] [CrossRef] [Green Version]
- Rydberg, E.M.; Wennergren, D.; Stigevall, C.; Ekelund, J.; Möller, M. Epidemiology of More than 50,000 Ankle Fractures in the Swedish Fracture Register during a Period of 10 Years. J. Orthop. Surg. Res. 2023, 18, 79. [Google Scholar] [CrossRef]
- Sarmiento, A.; Latta, L. The Evolution of Functional Bracing of Fractures. J. Bone Jt. Surg. 2006, 88, 141–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eickhoff, A.M.; Cintean, R.; Fiedler, C.; Gebhard, F.; Schütze, K.; Richter, P. Influence of Weight Bearing on Postoperative Complications after Surgical Treatment of the Lower Extremity. Z. Orthop. Unf. 2022. [Google Scholar] [CrossRef] [PubMed]
- Ganse, B.; Yang, P.F.; Gardlo, J.; Gauger, P.; Kriechbaumer, A.; Pape, H.C.; Koy, T.; Müller, L.P.; Rittweger, J. Partial Weight Bearing of the Tibia. Injury 2016, 47, 1777–1782. [Google Scholar] [CrossRef] [PubMed]
- Hak, D.J.; Fitzpatrick, D.; Bishop, J.A.; Marsh, J.L.; Tilp, S.; Schnettler, R.; Simpson, H.; Alt, V. Delayed Union and Nonunions: Epidemiology, Clinical Issues, and Financial Aspects. Injury 2014, 45, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Warschawski, Y.; Elbaz, A.; Segal, G.; Norman, D.; Haim, A.; Jacov, E.; Grundshtein, A.; Steinberg, E. Gait Characteristics and Quality of Life Perception of Patients Following Tibial Plateau Fracture. Arch. Orthop. Trauma Surg. 2015, 135, 1541–1546. [Google Scholar] [CrossRef]
- Elsoe, R.; Larsen, P. Asymmetry in Gait Pattern Following Bicondylar Tibial Plateau Fractures—A Prospective One-Year Cohort Study. Injury 2017, 48, 1657–1661. [Google Scholar] [CrossRef]
- Tian, R.; Zheng, F.; Zhao, W.; Zhang, Y.; Yuan, J.; Zhang, B.; Li, L. Prevalence and Influencing Factors of Nonunion in Patients with Tibial Fracture: Systematic Review and Meta-Analysis. J. Orthop. Surg. Res. 2020, 15, 377. [Google Scholar] [CrossRef]
- Gómez-Barrena, E.; Padilla-Eguiluz, N.G.; Rosset, P. Frontiers in Non-Union Research. EFORT Open Rev. 2020, 5, 574–583. [Google Scholar] [CrossRef]
- Großner, T.; Schmidmaier, G. Konservative Therapieoptionen der Pseudarth. Unfallchirurg 2020, 123, 705–710. [Google Scholar] [CrossRef]
- Padilla-Eguiluz, N.G.; Gómez-Barrena, E. Epidemiology of Long Bone Non-Unions in Spain. Injury 2021, 52, S3–S7. [Google Scholar] [CrossRef]
- Zura, R.; Xiong, Z.; Einhorn, T.; Watson, J.T.; Ostrum, R.F.; Prayson, M.J.; della Rocca, G.J.; Mehta, S.; McKinley, T.; Wang, Z.; et al. Epidemiology of Fracture Nonunion in 18 Human Bones. JAMA Surg. 2016, 151, e162775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, L.A.; Aitken, S.A.; Simpson, A.H.R.W. The Risk of Non-Union per Fracture: Current Myths and Revised Figures from a Population of over 4 Million Adults. Acta Orthop. 2017, 88, 434–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, A.; Templeman, D.; Weinlein, J.C. Nonunion of the Femur and Tibia: An Update. Orthop. Clin. N. Am. 2016, 47, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Claes, L. Improvement of Clinical Fracture Healing—What Can Be Learned from Mechano-Biological Research? J. Biomech. 2021, 115, 110148. [Google Scholar] [CrossRef]
- Assiotis, A.; Sachinis, N.P.; Chalidis, B.E. Pulsed Electromagnetic Fields for the Treatment of Tibial Delayed Unions and Nonunions. A Prospective Clinical Study and Review of the Literature. J. Orthop. Surg. Res. 2012, 7, 24. [Google Scholar] [CrossRef] [Green Version]
- Blokhuis, J.H.D.; de Bruine, J.A.M.; Bramer den Boer, F.C.; Bakker, P.; Patka, H.J.; Th, M.; Haarman, R.A.; Manoliu, T.F. The Reliability of Plain Radiography in Experimental Fracture Healing. Skelet. Radiol. 2001, 30, 151–156. [Google Scholar] [CrossRef]
- Augat, P.; Faschingbauer, M.; Seide, K.; Tobita, K.; Callary, S.A.; Solomon, L.B.; Holstein, J.H. Biomechanical Methods for the Assessment of Fracture Repair. Injury 2014, 45, S32–S38. [Google Scholar] [CrossRef]
- Ledet, E.H.; Liddle, B.; Kradinova, K.; Harper, S. Smart Implants in Orthopedic Surgery, Improving Patient Outcomes: A Review. Innov. Entrep. Health 2018, 5, 41–51. [Google Scholar] [CrossRef]
- Agar, A.; Sahin, A.; Guclu, S.; Gulabi, D.; Erturk, C. Foot Loading Analysis of Intraarticular Tibia Pilon Fracture. J. Am. Podiatr. Med. Assoc. 2022, 112, 21–107. [Google Scholar] [CrossRef] [PubMed]
- Becker, H.P.; Rosenbaum, D.; Kriese, T.; Gerngroj, H.; Clues, L. Gait Asymmetry Following Successful Surgical Treatment of Ankle Fractures in Young Adults. Clin. Orthopeadics Relat. Res. 1995, 311, 262–269. [Google Scholar]
- Bennett, K.J.; Millar, S.C.; Fraysse, F.; Arnold, J.B.; Atkins, G.J.; Solomon, L.B.; Martelli, S.; Thewlis, D. Postoperative Lower Limb Joint Kinematics Following Tibial Plateau Fracture: A 2-Year Longitudinal Study. Gait Posture 2021, 83, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Braun, B.J.; Bushuven, E.; Hell, R.; Veith, N.T.; Buschbaum, J.; Holstein, J.H.; Pohlemann, T. A Novel Tool for Continuous Fracture Aftercare—Clinical Feasibility and First Results of a New Telemetric Gait Analysis Insole. Injury 2016, 47, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Deleanu, B.; Prejbeanu, R.; Crisan, D.; Predescu, V.; Popa, I.; Poenaru, D.V. Gait Characteristics before Hardware Removal in Patients Operated upon for Tibial Plateau Fractures. Int. Orthop. 2015, 39, 1411–1415. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, M.; Birisik, F.; Ersin, M.; Sahinkaya, T.; Öztürk, I. A Prospective Evaluation of Strength and Endurance of Ankle Dorsiflexors-Plantar Flexors after Conservative Management of Lateral Malleolar Fractures. Turk. J. Phys. Med. Rehabil. 2021, 67, 300–307. [Google Scholar] [CrossRef]
- Elbaz, A.; Mor, A.; Segal, G.; Bar, D.; Monda, M.K.; Kish, B.; Nyska, M.; Palmanovich, E. Lower Extremity Kinematic Profile of Gait of Patients After Ankle Fracture: A Case-Control Study. J. Foot Ankle Surg. 2016, 55, 918–921. [Google Scholar] [CrossRef]
- Falzarano, G.; Pica, G.; Medici, A.; Rollo, G.; Bisaccia, M.; Cioffi, R.; Pavone, M.; Meccariello, L. Foot Loading and Gait Analysis Evaluation of Nonarticular Tibial Pilon Fracture: A Comparison of Three Surgical Techniques. J. Foot Ankle Surg. 2018, 57, 894–898. [Google Scholar] [CrossRef]
- Fändriks, A.; Tranberg, R.; Karlsson, J.; Möller, M.; Zügner, R. Gait Biomechanics in Patients with Intra-Articular Tibial Plateau Fractures—Gait Analysis at Three Months Compared with Age- and Gender-Matched Healthy Subjects. BMC Musculoskelet. Disord. 2021, 22, 702. [Google Scholar] [CrossRef]
- van Hoeve, S.; Houben, M.; Verbruggen, J.P.A.M.; Willems, P.; Meijer, K.; Poeze, M. Gait Analysis Related to Functional Outcome in Patients Operated for Ankle Fractures. J. Orthop. Res. 2019, 37, 1658–1666. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Tsai, Y.S.; Yau, C.S.; Shie, H.H.; Wu, C.M. Differences in Gait and Trunk Movement between Patients after Ankle Fracture and Healthy Subjects. Biomed. Eng. Online 2019, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Iliopoulos, E.; Agarwal, S.; Khaleel, A. Walking Impairments after Severe Tibia Plateau Fractures. A Gait Pattern Analysis. J. Orthop. Sci. 2020, 25, 276–278. [Google Scholar] [CrossRef] [PubMed]
- Jansen, H.; Fenwick, A.; Doht, S.; Frey, S.; Meffert, R. Clinical Outcome and Changes in Gait Pattern after Pilon Fractures. Int. Orthop. 2013, 37, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joslin, C.C.; Eastaugh-Waring, S.J.; Hardy, J.R.W.; Cunningham, J.L. Weight Bearing after Tibial Fracture as a Guide to Healing. Clin. Biomech. 2008, 23, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Kröger, I.; Müßig, J.; Brand, A.; Pätzold, R.; Wackerle, H.; Klöpfer-Krämer, I.; Augat, P. Recovery of Gait and Function during the First Six Months after Tibial Shaft Fractures. Gait Posture 2022, 91, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Lajevardi-Khosh, A.; Bamberg, S.; Rothberg, D.; Kubiak, E.; Petelenz, T.; Hitchcock, R. Center of Pressure in a Walking Boot Shifts Posteriorly in Patients Following Lower Leg Fracture. Gait Posture 2019, 70, 218–221. [Google Scholar] [CrossRef]
- Larsen, P.; Laessoe, U.; Rasmussen, S.; Graven-Nielsen, T.; Berre Eriksen, C.; Elsoe, R. Asymmetry in Gait Pattern Following Tibial Shaft Fractures—A Prospective One-Year Follow-up Study of 49 Patients. Gait Posture 2017, 51, 47–51. [Google Scholar] [CrossRef] [Green Version]
- Larsen, P.; Eriksen, C.B.; Stokholm, R.; Elsoe, R. Results Following Prolonged Recovery Show Satisfactory Functional and Patient-Reported Outcome after Intramedullary Nailing of a Tibial Shaft Fracture: A Prospective 5-Year Follow-up Cohort Study. Arch. Orthop. Trauma Surg. 2021, 141, 1303–1310. [Google Scholar] [CrossRef]
- Losch, A.; Meybohm, P.; Schmalz, T.; Fuchs, M.; Vamvukakis, F.; Dresing, K.; Blumentritt, S.; Stürmer, K.M. Funktionelle Ergebnisse Bei Freizeitsportlern in Der Dynamischen Ganganalyse 1 Jahr Nach Operativ Versorgten Sprunggelenkfrakturen. Sportverletz. Sportschaden 2002, 16, 101–107. [Google Scholar] [CrossRef]
- Perttunen, J.R.; Nieminen, H.; Tukiainen, E.; Kuokkanen, H.; Asko-Seljavaara, S.; Komi, P.V. Asymmetry of Gait after Free Flap Reconstruction of Severe Tibial Fractures with Extensive Soft-Tissue Damage. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2000, 34, 237–243. [Google Scholar] [CrossRef]
- Psatha, M.; Wu, Z.; Gammie, F.M.; Ratkevicius, A.; Wackerhage, H.; Lee, J.H.; Redpath, T.W.; Gilbert, F.J.; Ashcroft, G.P.; Meakin, J.R.; et al. A Longitudinal MRI Study of Muscle Atrophy during Lower Leg Immobilization Following Ankle Fracture. J. Magn. Reson. Imaging 2012, 35, 686–695. [Google Scholar] [CrossRef]
- Quacinella, M.; Bernstein, E.; Mazzone, B.; Wyatt, M.; Kuhn, K.M. Do Spatiotemporal Gait Parameters Improve after Pilon Fracture in Patients Who Use the Intrepid Dynamic Exoskeletal Orthosis? Clin. Orthop. Relat. Res. 2019, 477, 838–847. [Google Scholar] [CrossRef] [Green Version]
- Schoenmakers, S.; Houben, M.; van Hoeve, S.; Willems, P.; Meijer, K.; Poeze, M. The Influence of Size and Comminution of the Posterior Malleolus Fragment on Gait in Trimalleolar Ankle Fractures. Clin. Biomech. 2022, 91, 105550. [Google Scholar] [CrossRef]
- Segal, G.; Elbaz, A.; Parsi, A.; Heller, Z.; Palmanovich, E.; Nyska, M.; Feldbrin, Z.; Kish, B. Clinical Outcomes Following Ankle Fracture: A Cross-Sectional Observational Study. J. Foot Ankle Res. 2014, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Suciu, O.; Onofrei, R.R.; Totorean, A.D.; Suciu, S.C.; Amaricai, E.C. Gait Analysis and Functional Outcomes after Twelve-Week Rehabilitation in Patients with Surgically Treated Ankle Fractures. Gait Posture 2016, 49, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Thewlis, D.; Callary, S.A.; Fraysse, F.; Solomon, L.B. Peak Loading during Walking Is Not Associated with Fracture Migration Following Tibial Plateau Fracture: A Preliminary Case Series. J. Orthop. Res. 2015, 33, 1398–1406. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Thur, C.K.; Gutierrez-Farewik, E.M.; Wretenberg, P.; Broström, E. One Year Follow-up after Operative Ankle Fractures: A Prospective Gait Analysis Study with a Multi-Segment Foot Model. Gait Posture 2010, 31, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Warschawski, Y.; Drexler, M.; Batko, B.; Elias, S.; Goldstein, Y.; Frenkel Rutenberg, T.; Schermann, H.; Steinberg, E.L. Correlation between Preoperative Imaging Parameters and Postoperative Basic Kinematics-Based Functional Outcome in Patients with Tibial Plateau Fractures. Clin. Biomech. 2019, 65, 87–91. [Google Scholar] [CrossRef]
- Thingstad, P.; Taraldsen, K.; Saltvedt, I.; Sletvold, O.; Vereijken, B.; Lamb, S.E.; Helbostad, J.L. The Long-Term Effect of Comprehensive Geriatric Care on Gait after Hip Fracture: The Trondheim Hip Fracture Trial—a Randomised Controlled Trial. Osteoporosis International 2016, 27, 933–942. [Google Scholar] [CrossRef]
- Lord, S.; Galna, B.; Verghese, J.; Coleman, S.; Burn, D.; Rochester, L. Independent Domains of Gait in Older Adults and Associated Motor and Nonmotor Attributes: Validation of a Factor Analysis Approach. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 820–827. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, J.J.; Godinho, C.; Santos, A.T.; Domingos, J.; Abreu, D.; Lobo, R.; Gonçalves, N.; Barra, M.; Larsen, F.; Fagerbakke, Ø.; et al. Quantitative Home-Based Assessment of Parkinson’s Symptoms: The SENSE-PARK Feasibility and Usability Study. BMC Neurol. 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- Fukuchi, C.A.; Fukuchi, R.K.; Duarte, M. Effects of Walking Speed on Gait Biomechanics in Healthy Participants: A Systematic Review and Meta-Analysis. Syst. Rev. 2019, 8, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bejek, Z.; Paróczai, R.; Illyés, Á.; Kiss, R.M. The Influence of Walking Speed on Gait Parameters in Healthy People and in Patients with Osteoarthritis. Knee Surg. Sport. Traumatol. Arthrosc. 2006, 14, 612–622. [Google Scholar] [CrossRef]
- Lewek, M.D. The Influence of Body Weight Support on Ankle Mechanics during Treadmill Walking. J. Biomech. 2011, 44, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Kirtley, C.; Whittle, M.W.; Jefferson, R.J. Influence of Walking Speed on Gait Parameters. J. Biomed. Eng. 1985, 7, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Jordan, K.; Challis, J.H.; Newell, K.M. Walking Speed Influences on Gait Cycle Variability. Gait Posture 2007, 26, 128–134. [Google Scholar] [CrossRef] [PubMed]
- James, E.G.; Conatser, P.; Karabulut, M.; Leveille, S.G.; Hausdorff, J.M.; Travison, T.; Bean, J.F. Walking Speed Affects Gait Coordination and Variability Among Older Adults With and Without Mobility Limitations. Arch. Phys. Med. Rehabil. 2020, 101, 1377–1382. [Google Scholar] [CrossRef] [PubMed]
- Plotnik, M.; Bartsch, R.P.; Zeev, A.; Giladi, N.; Hausdorff, J.M. Effects of Walking Speed on Asymmetry and Bilateral Coordination of Gait. Gait Posture 2013, 38, 864–869. [Google Scholar] [CrossRef] [Green Version]
- Kanko, R.M.; Laende, E.; Selbie, W.S.; Deluzio, K.J. Inter-Session Repeatability of Markerless Motion Capture Gait Kinematics. J. Biomech. 2021, 121, 110422. [Google Scholar] [CrossRef]
- Herssens, N.; Verbecque, E.; Hallemans, A.; Vereeck, L.; van Rompaey, V.; Saeys, W. Do Spatiotemporal Parameters and Gait Variability Differ across the Lifespan of Healthy Adults? A Systematic Review. Gait Posture 2018, 64, 181–190. [Google Scholar] [CrossRef]
- Zadik, S.; Benady, A.; Gutwillig, S.; Florentine, M.M.; Solymani, R.E.; Plotnik, M. Age Related Changes in Gait Variability, Asymmetry, and Bilateral Coordination—When Does Deterioration Starts? Gait Posture 2022, 96, 87–92. [Google Scholar] [CrossRef]
- Pau, M.; Capodaglio, P.; Leban, B.; Porta, M.; Galli, M.; Cimolin, V. Kinematics Adaptation and Inter-Limb Symmetry during Gait in Obese Adults. Sensors 2021, 21, 5980. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Lim, J.; Lee, S. Body Fat-Related Differences in Gait Parameters and Physical Fitness Level in Weight-Matched Male Adults. Clin. Biomech. 2021, 81, 105243. [Google Scholar] [CrossRef]
- Phillips, A.; McClinton, S. Gait Deviations Associated with Plantar Heel Pain: A Systematic Review. Clin. Biomech. 2017, 42, 55–64. [Google Scholar] [CrossRef]
- Ogawa, E.F.; Shi, L.; Bean, J.F.; Hausdorff, J.M.; Dong, Z.; Manor, B.; McLean, R.R.; Leveille, S.G. Chronic Pain Characteristics and Gait in Older Adults: The MOBILIZE Boston Study II. Arch. Phys. Med. Rehabil. 2020, 101, 418–425. [Google Scholar] [CrossRef]
- Rittweger, J.; Felsenberg, D. Recovery of Muscle Atrophy and Bone Loss from 90 Days Bed Rest: Results from a One-Year Follow-Up. Bone 2009, 44, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Szulc, P. Impact of Bone Fracture on Muscle Strength and Physical Performance—Narrative Review. Curr. Osteoporos. Rep. 2020, 18, 633–645. [Google Scholar] [CrossRef]
- Manjra, M.A.; Naude, J.; Birkholtz, F.; Glatt, V.; Tetsworth, K.; Hohmann, E. The Relationship between Gait and Functional Outcomes in Patients Treated with Circular External Fixation for Malunited Tibial Fractures. Gait Posture 2019, 68, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Maktouf, W.; Durand, S.; Boyas, S.; Pouliquen, C.; Beaune, B. Interactions among Obesity and Age-Related Effects on the Gait Pattern and Muscle Activity across the Ankle Joint. Exp. Gerontol. 2020, 140, 111054. [Google Scholar] [CrossRef]
- Cohen, J.A.; Verghese, J.; Zwerling, J.L. Cognition and Gait in Older People. Maturitas 2016, 93, 73–77. [Google Scholar] [CrossRef]
- Vergara, I.; Vrotsou, K.; Orive, M.; Gonzalez, N.; Garcia, S.; Quintana, J.M. Factors Related to Functional Prognosis in Elderly Patients after Accidental Hip Fractures: A Prospective Cohort Study. BMC Geriatr. 2014, 14, 124. [Google Scholar] [CrossRef]
- Gao, F.; Lv, T.R.; Zhou, J.C.; Qin, X.D. Effects of Obesity on the Healing of Bone Fracture in Mice. J. Orthop. Surg. Res. 2018, 13, 145. [Google Scholar] [CrossRef] [Green Version]
- Braun, B.J.; Veith, N.T.; Rollmann, M.; Orth, M.; Fritz, T.; Herath, S.C.; Holstein, J.H.; Pohlemann, T. Weight-Bearing Recommendations after Operative Fracture Treatment—Fact or Fiction? Gait Results with and Feasibility of a Dynamic, Continuous Pedobarography Insole. Int. Orthop. 2017, 41, 1507–1512. [Google Scholar] [CrossRef] [PubMed]
- Patterson, K.K.; Nadkarni, N.K.; Black, S.E.; McIlroy, W.E. Gait Symmetry and Velocity Differ in Their Relationship to Age. Gait Posture 2012, 35, 590–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasanth, H.; Caban, M.; Keller, U.; Courtine, G.; Ijspeert, A.; Vallery, H.; von Zitzewitz, J. Wearable Sensor-Based Real-Time Gait Detection: A Systematic Review. Sensors 2021, 21, 2727. [Google Scholar] [CrossRef] [PubMed]
- Ceroni, D.; Martin, X.; Lamah, L.; Delhumeau, C.; Farpour-Lambert, N.; de Coulon, G.; Ferrière, V.D. Recovery of Physical Activity Levels in Adolescents after Lower Limb Fractures: A Longitudinal, Accelerometry-Based Activity Monitor Study. BMC Musculoskelet. Disord. 2012, 13, 131. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Fracture locations of the lower leg. The fibula can be involved in both distal tibial fractures as well as malleolar fractures. The distal tibia may also be involved in malleolar fractures. The AO classification numbers associated with the fracture locations are provided between brackets.
Figure 1.
Fracture locations of the lower leg. The fibula can be involved in both distal tibial fractures as well as malleolar fractures. The distal tibia may also be involved in malleolar fractures. The AO classification numbers associated with the fracture locations are provided between brackets.

Figure 2.
Overview of data from studies with different type of lower leg fractures [7,8,29,30,31,35,37,38,39,42,43,44,45,46,48]. (a) Gait speed after a lower leg fracture. (b). Step length after a lower leg fracture of the injured side. The type of lower leg fracture is indicated by the shape of the marker.
Figure 2.
Overview of data from studies with different type of lower leg fractures [7,8,29,30,31,35,37,38,39,42,43,44,45,46,48]. (a) Gait speed after a lower leg fracture. (b). Step length after a lower leg fracture of the injured side. The type of lower leg fracture is indicated by the shape of the marker.


Figure 3.
Linear relationship between gait speed and step length after a lower leg fracture [7,8,29,31,35,37,38,39,42,44,45,48]. Data pooled from studies with lower leg fractures, the correlation is weighted based on the number of participants per study.

Figure 4.
The expected changes in gait-related parameters after surgery in union and non-union of lower leg fractures. An increase indicates an improvement. The shaded blue indicates the expected range for non-union fractures.
Figure 4.
The expected changes in gait-related parameters after surgery in union and non-union of lower leg fractures. An increase indicates an improvement. The shaded blue indicates the expected range for non-union fractures.

Figure 5.
(a) Pie chart indicating how many studies performed a certain number of measurements. (b) Pie chart indicating how many patients from the studies combined were measured a certain number of times.
Figure 5.
(a) Pie chart indicating how many studies performed a certain number of measurements. (b) Pie chart indicating how many patients from the studies combined were measured a certain number of times.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Studies that measured gait-related parameters after lower leg fractures.
| Authors | Fracture Type(s) Included | n | Age (Years) | Longitudinal Measurements | Time After Fracture/Surgery That Measurement Occurred | Measurement Device(s) | Type of Parameters Calculated |
|---|---|---|---|---|---|---|---|
| Agar et al., 2022 [21] | Intraarticular distal tibial fractures | 62 | 43 | No | 24–58 months | Pressure plate | Pedographic measures |
| Becker et al., 1995 [22] | Malleolar fractures | 40 | 24 | No | 18.5 months | Pressure plate | Pedographic measures |
| Bennet et al., 2021 [23] | Proximal tibial fractures | 18 | 52 | Yes | 2 weeks, 6 weeks, 3 months, 6 months, 1 year, 2 years | Optical motion capture, force plate | Kinematics |
| Braun et al., 2016 [24] | Malleolar fractures | 10 | 53 | Yes | Continuously for 6 weeks | Pressure insoles | Pedographic measures |
| Deleanu et al., 2015 [25] | Proximal tibial fractures | 25 | 39 | No | Before hardware removal | Pressure plate, ultrasound-based motion capture | Spatiotemporal gait parameters |
| Ekinci et al., 2021 [26] | Malleolar fractures | 24 | 41 | Yes | At cast removal, 3 and 6 months after rehabilitation | Isokinetic dynamometer | Muscle strength |
| Elbaz et al., 2016 [27] | Malleolar fractures | 24 | 49 | No | <6 weeks from weight-bearing approval | Inertial measurement units | Kinematics |
| Elsoe et al., 2017 [8] | Proximal tibial fractures | 23 | 54 | No | 12 months after ring fixator removal | Electronic walkway | Spatiotemporal gait parameters |
| Falzarano et al., 2018 [28] | Nonarticular distal tibial fractures | 34 | 32 | No | 12 months | Pressure plate | Kinetics |
| Fändriks et al., 2021 [29] | Proximal tibial fractures | 20 | 44 | No | 85 days | Optical motion capture | Spatiotemporal gait parameters, kinematics |
| Hoeve et al., 2019 [30] | Malleolar fractures | 33 | 57 | No | 18 months | Optical motion capture, force plate | Kinematics |
| Hsu et al., 2019 [31] | Malleolar fractures | 10 | 38 | No | 4 months | accelerometer | Spatiotemporal gait parameters |
| Iliopoulos et al., 2020 [32] | Proximal tibial fractures | 16 | 49 | No | 3–6 months after frame removal | Force plate | Kinetics, spatiotemporal gait parameters |
| Jansen et al., 2013 [33] | Distal tibial fractures | 41 | 48 | No | 50 months | Pressure plate | Pedographic measures |
| Joslin et al., 2008 [34] | Tibial shaft fractures | 12 | 32 | No | 20 weeks | Force plate | Kinetics |
| Kröger et al., 2022 [35] | Tibial shaft fractures | 23 | 39 | Yes | 2, 3, and 6 months | Optical motion capture, force plate | Kinematics, kinetics, spatiotemporal gait parameters |
| Lajevardi-Khosh et al., 2019 [36] | Tibial shaft fractures and malleolar fractures | 7 | Yes | Continuously for 2–12 weeks | Pressure insoles | Pedographic measures | |
| Larsen et al., 2017 [37] | Tibial shaft fractures | 49 | 43 | Yes | 6 months, 12 months | Electronic walkway | Spatiotemporal gait parameters |
| Larsen et al., 2021 [38] | Tibial shaft fractures | 29 | 46 | No | 5 years | Electronic walkway | Spatiotemporal gait parameters |
| Losch et al., 2002 [39] | Malleolar fractures | 20 | 43 | No | 1 year | Optical motion capture, force plate | Kinematics, kinetics, spatiotemporal gait parameters |
| Perttunen et al., 2000 [40] | Tibial fractures | 17 | 51 | No | 9 months–14 years | Pressure insoles, electromyography | Pedographic measures, muscle activity |
| Psatha et al., 2012 [41] | Malleolar fractures | 18 | 43 | Yes | 5, 8, 15, 29 and 43 days | Magnetic resonance imaging | Muscle volume |
| Quacinella et al., 2019 [42] | Distal tibial fractures | 7 | 25 | No | 12 months | Optical motion capture, force plate | Spatiotemporal gait parameters |
| Schoenmakers et al., 2022 [43] | Malleolar fractures | 26 | 58 | No | 24 months | Optical motion capture | Kinematics |
| Segal et al., 2014 [44] | Malleolar fractures | 41 | 48 | No | 67 days | Electronic walkway | Spatiotemporal gait parameters |
| Suciu et al., 2016 [45] | Malleolar fractures | 30 | 53 | Yes | 7 weeks, 12 weeks | Pressure plate | Spatiotemporal gait parameters |
| Thewlis et al., 2015 [46] | Proximal tibial fractures | 9 | 69 | Yes | 2 weeks, 3 months, 6 months, 1 year | Optical motion capture, force plate | Kinetics |
| Wang et al., 2010 [47] | Malleolar fractures | 18 | 39 | No | 1 year | Optical motion capture | Kinematics, spatiotemporal gait parameters |
| Warschawski et al., 2015 [7] | Proximal tibial fractures | 22 | 46 | No | 3 years | Floor-based photocell system | Spatiotemporal gait parameters |
| Warschawski et al., 2019 [48] | Proximal tibial fractures | 21 | 44 | No | 3 years | Floor-based photocell system | Spatiotemporal gait parameters |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Warmerdam, E.; Orth, M.; Pohlemann, T.; Ganse, B. Gait Analysis to Monitor Fracture Healing of the Lower Leg. Bioengineering 2023, 10, 255. https://doi.org/10.3390/bioengineering10020255
AMA Style
Warmerdam E, Orth M, Pohlemann T, Ganse B. Gait Analysis to Monitor Fracture Healing of the Lower Leg. Bioengineering. 2023; 10(2):255. https://doi.org/10.3390/bioengineering10020255
Chicago/Turabian StyleWarmerdam, Elke, Marcel Orth, Tim Pohlemann, and Bergita Ganse. 2023. "Gait Analysis to Monitor Fracture Healing of the Lower Leg" Bioengineering 10, no. 2: 255. https://doi.org/10.3390/bioengineering10020255
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.