Long-Chain Polyunsaturated Fatty Acids Are Associated with Blood Pressure and Hypertension over 10-Years in Black South African Adults Undergoing Nutritional Transition

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Selection of Study Sample
2.2. Clinical and Biological Measurements
2.3. Statistical Analyses
2.4. Sensitivity Analyses
3. Results
3.1. Baseline Characteristics of the 300 Rural and Urban Black South Africans
3.2. Ten-Year Changes in Blood Pressure and Status of Hypertension
3.3. Ten-Year Changes in Long-Chain Plasma Phospholipid Fatty Acids
3.4. Relationship Between Dietary Intake of N-3 Fatty Acids and Long-Chain Fatty Acids in Plasma Phospholipids
3.5. Ten-Year Associations between Long-Chain Plasma Phospholipid Fatty Acids with Blood Pressure and Hypertension in Black South African Adults
3.5.1. Associations between N-3 Long-Chain Fatty Acids and Blood Pressure
3.5.2. Associations between N-6 Long-Chain Fatty Acids and Blood Pressure
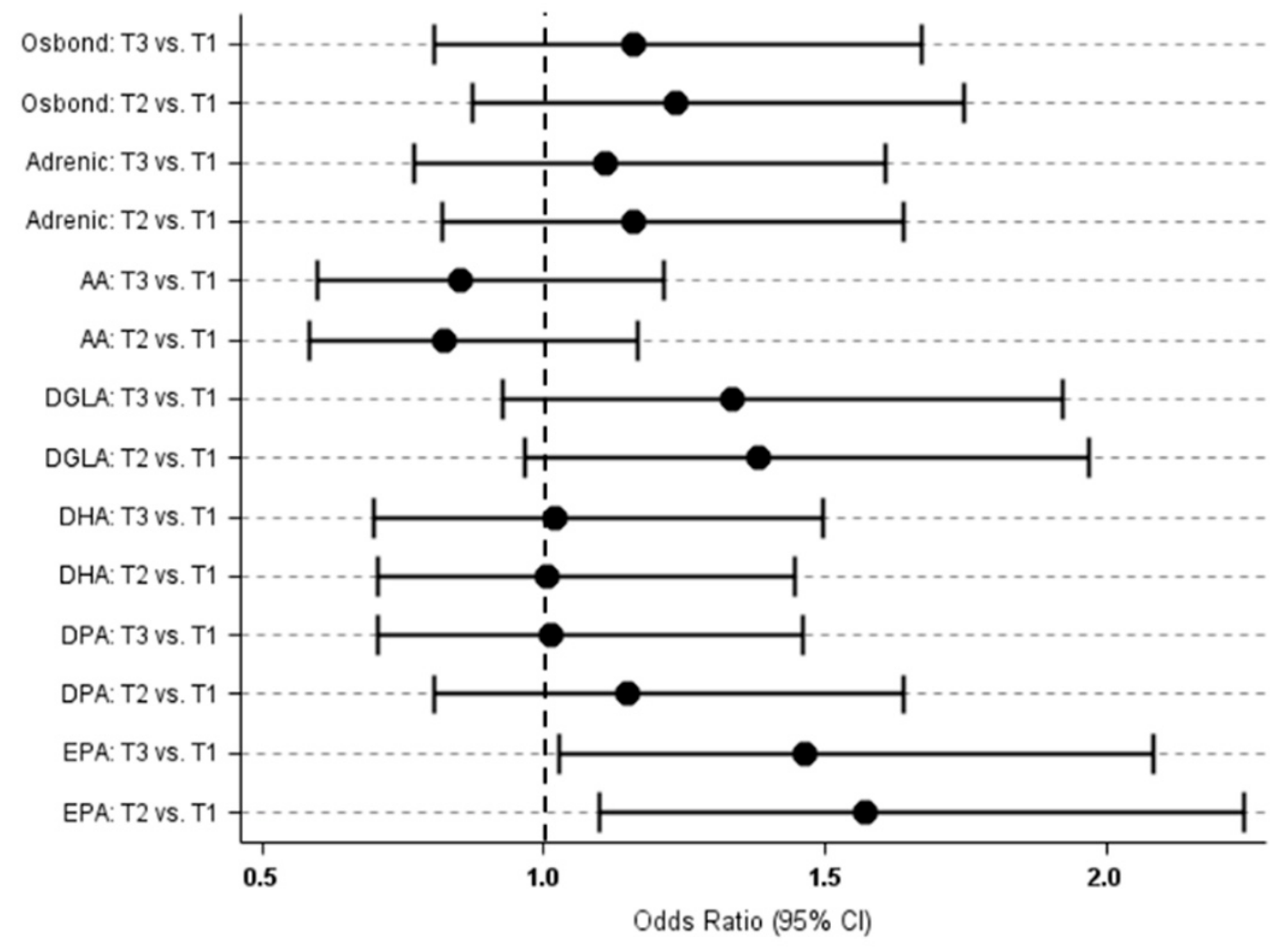
3.5.3. Associations between Long-Chain Plasma Fatty Acids and Status of Hypertension
3.5.4. Sensitivity Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Popkin, B.M. Nutrition in transition: The changing global nutrition challenge. Asia Pac. J. Clin. Nutr. 2001, 10, S13–S18. [Google Scholar] [CrossRef] [Green Version]
- Alsheikh-Ali, A.A.; Omar, M.I.; Raal, F.J.; Rashed, W.; Hamoui, O.; Kane, A.; Alami, M.; Abreu, P.; Mashhoud, W.M. Cardiovascular risk factor burden in Africa and the Middle East: The Africa Middle East Cardiovascular Epidemiological (ACE) study. PLoS ONE 2014, 9, e102830. [Google Scholar] [CrossRef]
- Danaei, G.; Finucane, M.M.; Lin, J.K.; Singh, G.M.; Paciorek, C.J.; Cowan, M.J.; Farzadfar, F.; Stevens, G.A.; Lim, S.S.; Riley, L.M.; et al. Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Blood Pressure). National, regional, and global trends in systolic blood pressure since 1980: Systematic analysis of health examination surveys and epidemiological studies with 786 country-years and 5.4 million participants. Lancet 2011, 377, 568–577. [Google Scholar]
- Schutte, A.E.; Schutte, R.; Huisman, H.W.; van Rooyen, J.M.; Fourie, C.M.; Malan, N.T.; Malan, L.; Mels, C.M.; Smith, W.; Moss, S.J.; et al. Are behavioural risk factors to be blamed for the conversion from optimal blood pressure to hypertensive status in Black South Africans? A 5-year prospective study. Int. J. Epidemiol. 2012, 41, 1114–1123. [Google Scholar] [CrossRef] [Green Version]
- Richter, M.; Baumgartner, J.; Wentzel-Viljoen, E.; Smuts, C.M. Different dietary fatty acids are associated with blood lipids in healthy South African men and women: The PURE study. Int. J. Cardiol. 2014, 172, 368–374. [Google Scholar] [CrossRef]
- Bagge, C.N.; Strandhave, C.; Skov, C.M.; Svensson, M.; Schmidt, E.B.; Christensen, J.H. Marine n-3 polyunsaturated fatty acids affect the blood pressure control in patients with newly diagnosed hypertension–a 1-year follow-up study. Nutr. Res. 2017, 38, 71–78. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Wu, J.H. Omega-3 fatty acids and cardiovascular disease: Effects on risk factors, molecular pathways, and clinical events. J. Am. Coll. Cardiol. 2011, 58, 2047–2067. [Google Scholar] [CrossRef]
- Archer, E.; Blair, S.N. Implausible data, false memories, and the status quo in dietary assessment. Adv. Nutr. 2015, 6, 229–230. [Google Scholar] [CrossRef]
- Ma, J.; Folsom, A.R.; Shahar, E.; Eckfeldt, J.H. Plasma fatty acid composition as an indicator of habitual dietary fat intake in middle-aged adults. The Atherosclerosis Risk in Communities (ARIC) Study Investigators. Am. J. Clin. Nutr. 1995, 62, 564–571. [Google Scholar] [CrossRef]
- Jackson, K.H.; Harris, W.S. Blood Fatty Acid Profiles: New Biomarkers for Cardiometabolic Disease Risk. Curr. Atheroscler. Rep. 2018, 20, 22. [Google Scholar] [CrossRef]
- Liu, Q.; Matthan, N.R.; Manson, J.E.; Howard, B.V.; Tinker, L.F.; Neuhouser, M.L.; Van Horn, L.V.; Rossouw, J.E.; Allison, M.A.; Martin, L.W.; et al. Plasma Phospholipid Fatty Acids and Coronary Heart Disease Risk: A Matched Case-Control Study within the Women’s Health Initiative Observational Study. Nutrients 2019, 11, 1672. [Google Scholar] [CrossRef]
- Yang, B.; Ding, F.; Yan, J.; Ye, X.W.; Xu, X.L.; Wang, F.L.; Yu, W. Exploratory serum fatty acid patterns associated with blood pressure in community-dwelling middle-aged and elderly Chinese. Lipids Health Dis. 2016, 15, 58. [Google Scholar] [CrossRef]
- Simon, J.A.; Fong, J.; Bernert, J.T., Jr. Serum fatty acids and blood pressure. Hypertension 1996, 27, 303–307. [Google Scholar] [CrossRef]
- Grimsgaard, S.; Bonaa, K.H.; Jacobsen, B.K.; Bjerve, K.S. Plasma saturated and linoleic fatty acids are independently associated with blood pressure. Hypertension 1999, 34, 478–483. [Google Scholar] [CrossRef]
- Virtanen, J.K.; Nyantika, A.N.; Kauhanen, J.; Voutilainen, S.; Tuomainen, T.P. Serum long-chain n-3 polyunsaturated fatty acids, methylmercury and blood pressure in an older population. Hypertens. Res. 2012, 35, 1000–1004. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.C.; Conklin, S.M.; Manuck, S.B.; Yao, J.K.; Muldoon, M.F. Long-chain omega-3 fatty acids and blood pressure. Am. J. Hypertens. 2011, 24, 1121–1126. [Google Scholar] [CrossRef]
- Yang, B.; Ding, F.; Wang, F.L.; Yan, J.; Ye, X.W.; Yu, W.; Li, D. Association of serum fatty acid and estimated desaturase activity with hypertension in middle-aged and elderly Chinese population. Sci. Rep. 2016, 6, 23446. [Google Scholar] [CrossRef]
- Ojwang, A.A.; Kruger, H.S.; Zec, M.; Ricci, C.; Pieters, M.; Kruger, I.M.; Wentzel-Viljoen, E.; Smuts, C.M. Plasma phospholipid fatty acid patterns are associated with adiposity and the metabolic syndrome in black South Africans: A cross-sectional study. Cardiovasc. J. Afr. 2019, 30, 1–11. [Google Scholar]
- Teo, K.; Chow, C.K.; Vaz, M.; Rangarajan, S.; Yusuf, S. PURE Investigators-Writing Group. The Prospective Urban Rural Epidemiology (PURE) study: Examining the impact of societal influences on chronic noncommunicable diseases in low-, middle-, and high-income countries. Am. Heart J. 2009, 158, 1–7. [Google Scholar] [CrossRef]
- Baumgartner, J.; Smuts, C.M.; Malan, L.; Kvalsvig, J.; van Stuijvenberg, M.E.; Hurrell, R.F.; Zimmermann, M.B. Effects of iron and n-3 fatty acid supplementation, alone and in combination, on cognition in school children: A randomized, double-blind, placebo-controlled intervention in South Africa. Am. J. Clin. Nutr. 2012, 96, 1327–1338. [Google Scholar] [CrossRef]
- Folch, J.; Lees, M.; Sloane Stanley, G.H. A simple method for the isolation and purification of total lipides from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar]
- Kruger, H.S.; Venter, C.S.; Vorster, H.H.; Margetts, B.M. Physical inactivity is the major determinant of obesity in black women in the North West Province, South Africa: The THUSA study. Transition and Health During Urbanisation of South Africa. Nutrition 2002, 18, 422–427. [Google Scholar] [CrossRef]
- Wentzel-Viljoen, E.; Laubscher, R.; Kruger, A. Using different approaches to assess the reproducibility of a culturally sensitive quantified food frequency questionnaire. S. Afr. J. Clin. Nutr. 2011, 24, 143–148. [Google Scholar] [CrossRef]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean diet; a literature review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Tucker, L.A. Fiber Intake and Insulin Resistance in 6374 Adults: The Role of Abdominal Obesity. Nutrients 2018, 10, 237. [Google Scholar] [CrossRef]
- Toyama, K.; Nishioka, T.; Isshiki, A.; Ando, T.; Inoue, Y.; Kirimura, M.; Kamiyama, T.; Sasaki, O.; Ito, H.; Maruyama, Y.; et al. Eicosapentaenoic acid combined with optimal statin therapy improves endothelial dysfunction in patients with coronary artery disease. Cardiovasc. Drugs Ther. 2014, 28, 53–59. [Google Scholar] [CrossRef]
- Sasaki, J.; Miwa, T.; Odawara, M. Administration of highly purified eicosapentaenoic acid to statin-treated diabetic patients further improves vascular function. Endocr. J. 2012, 59, 297–304. [Google Scholar] [CrossRef] [Green Version]
- Bäck, M.; Hansson, G.K. Omega-3 fatty acids, cardiovascular risk, and the resolution of inflammation. FASEB J. 2019, 33, 1536–1539. [Google Scholar] [CrossRef]
- Zeng, F.F.; Sun, L.L.; Liu, Y.H.; Xu, Y.; Guan, K.; Ling, W.H.; Chen, Y.M. Higher Erythrocyte n–3 PUFAs Are Associated with Decreased Blood Pressure in Middle-Aged and Elderly Chinese Adults–3. J. Nutr. 2014, 144, 1240–1246. [Google Scholar] [CrossRef]
- Puzyrenko, A.M.; Chekman, I.S.; Briuzhina, T.S.; Horchakova, N.O. Influence of antihypertensive and metabolic drugs on fatty acids content of lipids in cardiomyocytes of rats with spontaneous hypertension. Ukr. Kyi Biokhimichnyi Zhurnal (1999) 2013, 85, 67–74. [Google Scholar] [CrossRef]
- Zheng, Z.J.; Folsom, A.R.; Ma, J.; Arnett, D.K.; McGovern, P.G.; Eckfeldt, J.H. ARIC Study Investigators. Plasma fatty acid composition and 6-year incidence of hypertension in middle-aged adults: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Epidemiol. 1999, 150, 492–500. [Google Scholar] [CrossRef]
- Sergeant, S.; Hugenschmidt, C.E.; Rudock, M.E.; Ziegler, J.T.; Ivester, P.; Ainsworth, H.C.; Vaidya, D.; Case, L.D.; Langefeld, C.D.; Freedman, B.I.; et al. Differences in arachidonic acid levels and fatty acid desaturase (FADS) gene variants in African Americans and European Americans with diabetes or the metabolic syndrome. Br. J. Nutr. 2012, 107, 547–555. [Google Scholar] [CrossRef]
- Conquer, J.A.; Martin, J.B.; Tummon, I.; Watson, L.; Tekpetey, F. Fatty acid analysis of blood serum, seminal plasma, and spermatozoa of normozoospermic vs. asthenozoospermic Men. Lipids 1999, 34, 793–799. [Google Scholar] [CrossRef]
- Laidlaw, M.; Holub, B.J. Effects of supplementation with fish oil-derived n-3 fatty acids and gamma-linolenic acid on circulating plasma lipids and fatty acid profiles in women. Am. J. Clin. Nutr. 2003, 77, 37–42. [Google Scholar] [CrossRef]
- Young, G.S.; Maharaj, N.J.; Conquer, J.A. Blood phospholipid fatty acid analysis of adults with and without attention deficit/hyperactivity disorder. Lipids 2004, 39, 117–123. [Google Scholar] [CrossRef]
- Brenna, J.T.; Salem, N., Jr.; Sinclair, A., Jr.; Cunnane, S.C. Alpha-linolenic acid supplementation and conversion to n-3 long-chain polyunsaturated fatty acids in humans. Prostaglandins Leukot. Essent. Fat. Acids 2009, 80, 85–91. [Google Scholar] [CrossRef]
- Elmadfa, I.; Kornsteiner, M. Fats and fatty acid requirements for adults. Ann. Nutr. Metab. 2009, 55, 56. [Google Scholar] [CrossRef]
- Vessby, B.; Ahrén, B.; Warensjö, E.; Lindgärde, F. Plasma lipid fatty acid composition, desaturase activities and insulin sensitivity in Amerindian women. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 176–181. [Google Scholar] [CrossRef]
- King, I.B.; Lemaitre, R.N.; Kestin, M. Effect of a low-fat diet on fatty acid composition in red cells, plasma phospholipids, and cholesterol esters: Investigation of a biomarker of total fat intake. Am. J. Clin. Nutr. 2006, 83, 227–236. [Google Scholar] [CrossRef]
- Tanaka, T.; Shen, J.; Abecasis, G.R.; Kisialiou, A.; Ordovas, J.M.; Guralnik, J.M.; Singleton, A.; Bandinelli, S.; Cherubini, A.; Arnett, D.; et al. Genome-wide association study of plasma polyunsaturated fatty acids in the InCHIANTI Study. PLoS Genet. 2009, 5, e1000338. [Google Scholar] [CrossRef]
- Wang, L.; Folsom, A.R.; Eckfeldt, J.H. Plasma fatty acid composition and incidence of coronary heart disease in middle aged adults: The Atherosclerosis Risk in Communities (ARIC) Study. Nutr. Metab. Cardiovasc. Dis. 2003, 13, 256–266. [Google Scholar] [CrossRef]
- Salonen, J.T.; Salonen, R.; Penttila, I.; Herranen, J.; Jauhiainen, M.; Kantola, M.; Lappetelainen, R.; Maenpaa, P.H.; Alfthan, G.; Puska, P. Serum fatty acids, apolipoproteins, selenium and vitamin antioxidants and the risk of death from coronary artery disease. Am. J. Cardiol. 1985, 56, 226–231. [Google Scholar] [CrossRef]
- Yary, T.; Voutilainen, S.; Tuomainen, T.P.; Ruusunen, A.; Nurmi, T.; Virtanen, J.K. Serum n-6 polyunsaturated fatty acids, delta5- and delta6-destaurase activities, and risk of incident type 2 diabetes in men: The Kuopio Ischaemic Heart Disease Risk Factor Study. Am. J. Clin. Nutr. 2016, 103, 1337–1343. [Google Scholar] [CrossRef]
- Sonnweber, T.; Pizzini, A.; Nairz, M.; Weiss, G.; Tancevski, I. Arachidonic Acid Metabolites in Cardiovascular and Metabolic Diseases. Int. J. Mol. Sci. 2018, 19, 3285. [Google Scholar] [CrossRef]
- Caligiuri, S.P.; Aukema, H.M.; Ravandi, A.; Guzman, R.; Dibrov, E.; Pierce, G.N. Flaxseed consumption reduces blood pressure in patients with hypertension by altering circulating oxylipins via an α-linolenic acid–induced inhibition of soluble epoxide hydrolase. Hypertension 2014, 64, 53–59. [Google Scholar] [CrossRef]
- Das, U.N. Nutritional factors in the pathobiology of human essential hypertension. Nutrition 2001, 17, 337–346. [Google Scholar] [CrossRef]
- Nyantika, A.N.; Tuomainen, T.P.; Kauhanen, J.; Voutilainen, S.; Virtanen, J.K. Serum long-chain omega-3 polyunsaturated fatty acids and future blood pressure in an ageing population. J. Nutr. Health Aging 2015, 19, 498–503. [Google Scholar] [CrossRef]
- US Department of Health and Human Services and US Department of Agriculture. 2015–2020 Dietary Guidelines for Americans (DGA), 8th. ed.December 2015. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 29 March 2019).
- Sacks, F.M.; Lichtenstein, A.H.; Wu, J.H.Y.; Appel, L.J.; Creager, M.A.; Kris-Etherton, P.M.; Miller, M.; Rimm, E.B.; Rudel, L.L.; Robinson, J.G.; et al. American Heart Association. Dietary fats and cardiovascular disease: A Presidential Advisory from the American Heart Association. Circulation 2017, 136, e1–e23. [Google Scholar] [CrossRef]
- Nettleton, J.A.; von Schacky, C.; Brouwer, I.A.; Koletzko, B. International Society for the Study of Fatty Acids and Lipids 2016 debate: For science based dietary guidelines on fats, meta-analysis and systematic reviews are decisive. Ann. Nutr. Metab. 2017, 71, 26–30. [Google Scholar] [CrossRef]
- Al-Khudairy, L.; Hartley, L.; Clar, C.; Flowers, N.; Hooper, L.; Rees, K. Omega-6 fatty acids for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2015, 16, CD011094. [Google Scholar] [CrossRef]
- Vafeiadou, K.; Weech, M.; Altowaijri, H.; Todd, S.; Yaqoob, P.; Jackson, K.G.; Lovegrove, J.A. Replacement of saturated with unsaturated fats had no impact on vascular function but beneficial effects on lipid biomarkers, E-selectin, and blood pressure: Results from the randomized, controlled Dietary Intervention and VAScular function (DIVAS) study. Am. J. Clin. Nutr. 2015, 102, 40–48. [Google Scholar] [CrossRef]
- Maki, K.C.; Eren, F.; Cassens, M.E.; Dicklin, M.R.; Davidson, M.H. ω-6 Polyunsaturated Fatty Acids and Cardiometabolic Health: Current Evidence, Controversies, and Research Gaps. Adv. Nutr. 2018, 9, 688–700. [Google Scholar] [CrossRef]
- Chilton, F.H.; Murphy, R.C.; Wilson, B.A.; Sergeant, S.; Ainsworth, H.; Seeds, M.C.; Mathias, R.A. Diet-gene interactions and PUFA metabolism: A potential contributor to health disparities and human diseases. Nutrients 2014, 6, 1993–2022. [Google Scholar] [CrossRef]
- Smuts, C.M.; Wolmarans, P. The importance of the quality or type of fat in the diet: A food-based dietary guideline for South Africa. S. Afr. J. Clin. Nutr. 2013, 26, S87–S99. [Google Scholar]
- ASCEND Study Collaborative, Group; Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; et al. Effects of n-3 fatty acid supplements in diabetes mellitus. N. Engl. J. Med. 2018, 379, 1540–1550. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Complete Sample (n 300) | Rural Areas (n 140) | Urban Areas (n 160) | p-Value 1 | |
|---|---|---|---|---|
| Gender, men, n (%) | 91 (30.33) | 39 (27.86) | 52 (32.5) | 0.385 |
| Any education, n (%) | 190 (64.63) | 65 (47.10) | 125 (80.13) | <0.001 |
| Current smokers, n (%) | 155 (51.84) | 74 (52.86) | 81 (50.94) | 0.201 |
| Former smokers, n (%) | 135 (45.15) | 59 (42.14) | 76 (47.8) | |
| Clinical parameters | ||||
| Age, years | 53.12 (9.83) | 52.20 (9.16) | 53.93 (10.34) | 0.130 |
| Body mass index, kg m−2 | 23.91 [19.93, 29.61] | 23.39 [19.44, 29.43] | 24.03 [20.43, 29.61] | 0.172 |
| Waist circumference. cm | 80.68 (12.99) | 79.84 (13.43) | 81.42 (12.60) | 0.295 |
| Systolic blood pressure, mmHg | 136.54 (3.29) | 131.56 (22.81) | 140.91 (22.89) | 0.001 |
| Diastolic blood pressure, mmHg | 89.04 (12.69) | 87.10 (13.33) | 90.75 (11.87) | 0.013 |
| Fasting glucose, mmol L−1 | 5.11 (1.53) | 4.87 (1.08) | 5.32 (1.82) | 0.010 |
| Total cholesterol, mmol L−1 | 5.22 (1.30) | 5.12 (1.32) | 5.31 (1.27) | 0.193 |
| HDL-c, mmol L−1 | 1.58 (0.64) | 1.55 (0.65) | 1.62 (0.64) | 0.338 |
| LDL-c, mmol L−1 | 3.01 (1.18) | 3.00 (1.16) | 3.03 (1.19) | 0.820 |
| Tryglicerides, mmol L−1 | 1.15 [0.84, 1.68] | 1.10 [0.84, 1.53] | 1.23 [0.84, 1.75] | 0.142 |
| Weighted physical activity index | 2.76 [2.49, 3.17] | 3.07 [2.61, 3.43] | 2.62 [2.38, 2.89] | <0.0001 |
| GGT, U L−1 | 43.00 [29.00, 85.06] | 37.30 [26.90, 64.35] | 50.29 [34.38, 95.50] | 0.001 |
| hsCRP, mg L−1 | 3.19 [1.04, 7.52] | 3.32 [0.90, 7.36] | 2.90 [1.07, 8.39] | 0.722 |
| Use of hypertension medication, n (%) | 55 (18.3) | 27 (19.3) | 28 (17.5) | 0.691 |
| Hypertensive, n (%) | 176 (58.7) | 68 (48.6) | 108 (67.5) | <0.001 |
| Dietary intake | ||||
| Energy, kJ | 7251.15 [5259.26, 9689.23] | 6103.36 [4681.22, 7928.72] | 8453.99 [5824.48, 11439.46] | <0.0001 |
| Total fat, g | 43.14 [27.73, 63.05] | 30.53 [21.94, 42.22] | 59.04 [40.89, 82.64] | <0.0001 |
| Saturated fat, g | 9.97 [5.98, 16.29] | 6.61 [3.88, 9.20] | 15.18 [10.10, 21.39] | <0.0001 |
| Monounsaturated fat, g | 10.92 [6.10, 18.05] | 6.79 [4.20, 10.00] | 16.20 [11.14, 24.69] | <0.0001 |
| Polyunsaturated fat, g | 13.55 [7.85, 20.23] | 9.59 [6.50, 14.26] | 17.10 [11.49, 23.60] | <0.0001 |
| n-3 intake, mg | 314.10 [188.98, 476.17] | 209.19 [137.58, 314.34] | 425.59 [298.12, 608.72] | <0.0001 |
| EPA+DHA intake, mg | 109.91 [49.20, 199.49] | 79.91 [34.66, 137.56] | 130.48 [58.90, 230.20] | <0.0001 |
| Total carbohydrate, g | 279.98 (129.89) | 256.77 (113.15) | 300.29 (140.15) | 0.003 |
| Total fibre, g | 21.35 (10.48) | 18.62 (8.11) | 23.75 (11.68) | <0.0001 |
| Soluble fibre, g | 1.40 [0.84, 2.32] | 0.97 [0.66, 1.43] | 2.12 [1.28, 3.32] | <0.0001 |
| Alcohol, g | 0.00 [0.00, 11.50] | 0.00 [0.00, 5.71] | 0.10 [0.00, 15.33] | 0.010 |
| Study Year | p1 | |||
|---|---|---|---|---|
| 2005 | 2010 | 2015 | ||
| Myristic acid, 14:0 | 0.27 (0.01) | 0.27 (0.01) | 0.33 (0.03) | <0.0001 |
| Palmitic acid, 16:0 | 26.93 (0.31) | 27.17 (0.45) | 24.79 (0.64) | <0.0001 |
| Palmitoleic acid, 16:1 n-7 | 0.86 [0.76, 0.96] | 0.83 [0.70, 0.91] | 0.93 [0.79, 1.04] | 0.086 |
| Stearic acid, 18:0 | 15.26 (0.96) | 14.92 (0.61) | 14.19 (0.07) | <0.0001 |
| Oleic acid, 18:1 n-9 | 8.84 [8.35, 9.27] | 8.48 [7.88, 8.95] | 8.33 [7.73, 8.63] | 0.025 |
| Mead, 20:3 n-9 | 0.25 [0.25, 0.26] | 0.24 [0.22, 0.25] | 0.27 [0.19, 0.28] | 0.216 |
| Linoleic acid, 18:2 n-6 | 16.03 (0.41) | 16.70 (1.01) | 16.07 (0.28) | 0.579 |
| γ-Linolenic, 18:3 n-6 | 0.12 [0.11, 0.12] | 0.12 [0.11, 0.13] | 0.11 [0.10, 0.11] | 0.018 |
| Dihomo-γ-linolenic, 20:3 n-6 | 2.91 (0.09) | 2.89 (0.08) | 3.48 (0.19) | <0.0001 |
| Arachidonic acid, 20:4 n-6 | 13.57 (0.24) | 14.65 (0.31) | 18.13 (0.37) | <0.0001 |
| Adrenic, 22:4 n-6 | 0.60 (0.07) | 0.70 (0.01) | 0.66 (0.02) | <0.0001 |
| Osbond, 22:5 n-6 | 0.57 [0.56, 0.67] | 0.72 [0.70, 0.73] | 1.07 [0.93, 1.09] | <0.0001 |
| α-linolenic acid, 18:3 n-3 | 0.09 [0.09, 0.09] | 0.09 [0.09, 0.11] | 0.07 [0.07, 0.08] | <0.0001 |
| EPA, 20:5 n-3 | 0.78 [0.59, 0.80] | 0.47 [0.45, 0.60] | 0.55 [0.52, 0.59] | <0.0001 |
| Docosapentaenoic, 22:5 n-3 | 1.41 (0.02) | 1.42 (0.19) | 1.53 (0.08) | 0.001 |
| DHA, 22:6 n-3 | 4.56 (0.61) | 3.88 (0.11) | 4.33 (0.14) | 0.009 |
| Systolic Blood Pressure | Diastolic Blood Pressure | |||
|---|---|---|---|---|
| β (95% CI) | p3 | β (95% CI) | p3 | |
| Long-chain n-3 fatty acids | ||||
| EPA, 20:5 n-3 | ||||
| T1 | ref. | ref. | ||
| T21 | 1.89 (−1.40, 5.18) | 0.322 | 1.44 (−0.44, 3.32) | 0.143 |
| T3 | 2.41 (−0.89, 5.70) | 1.80 (−0.09, 3.69) | ||
| T22 | 2.39 (−0.95, 5.72) | 0.191 | 1.37 (−0.56, 3.30) | 0.132 |
| T3 | 2.92 (−0.41, 6.26) | 1.94 (0.01, 3.87) | ||
| Docosapentaenoic, 22:5 n-3 | ||||
| T1 | ref. | ref. | ||
| T2 1 | 0.91 (−2.39, 4.22) | 0.284 | 0.58 (−1.31, 2.48) | 0.056 |
| T3 | −1.75 (−5.26, 1.75) | −1.69 (−3.69, 0.30) | ||
| T2 2 | 0.22 (−3.10, 3.53) | 0.349 | 0.33 (−1.59, 2.24) | 0.068 |
| T3 | −2.11 (−5.63, 1.41) | −1.86 (−3.88, 0.17) | ||
| DHA, 22:6 n-3 | ||||
| T1 | ref. | ref. | ||
| T2 1 | −0.92 (−4.31, 2.47) | 0.386 | −0.76 (−2.70, 1.18) | 0.275 |
| T3 | −2.48 (−6.08, 1.11) | −1.68 (−3.73, 0.38) | ||
| T2 2 | −0.37 (−3.79, 3.06) | 0.427 | −0.51 (−2.49, 1.46) | 0.358 |
| T3 | −2.21 (−5.86, 1.44) | −1.50 (−3.60, 0.60) | ||
| Long-chain n-6 fatty acids | ||||
| Dihomo-γ-linolenic acid, 20:3 n-6 | ||||
| T1 | ref. | ref. | ||
| T2 1 | 1.40 (−1.93, 4.73) | 0.419 | 0.55 (−1.36, 2.46) | 0.396 |
| T3 | −0.77 (−4.17, 2.63) | −0.75 (−2.70, 1.19) | ||
| T2 2 | 0.68 (−2.70, 4.06) | 0.392 | 0.23 (−1.72, 2.19) | 0.305 |
| T3 | −1.59 (−5.07, 1.89) | −1.19 (−3.20, 0.82) | ||
| Arachidonic acid, 20:4 n-6 | ||||
| T1 | ref. | ref. | ||
| T2 1 | −0.06 (−3.29, 3.16) | 0.048 | −0.83 (−2.66, 1.00) | <0.0001 |
| T3 | −3.50 (−6.73, −0.27) | −3.76 (−5.59, −1.93) | ||
| T2 2 | 0.17 (−3.06, 3.39) | 0.024 | −0.62 (−2.47, 1.22) | <0.0001 |
| T3 | −3.81 (−7.07, −0.54) | −3.82 (−5.70, −1.95) | ||
| Adrenic acid, 22:4 n-6 | ||||
| T1 | ref. | ref. | ||
| T2 1 | −1.87 (−5.11, 1.37) | 0.327 | 0.03 (−1.83, 1.88) | 0.999 |
| T3 | 0.45 (−3.02, 3.92) | −0.02 (−2.00, 1.97) | ||
| T2 2 | −2.56 (−5.79, 0.68) | 0.195 | −0.23 (−2.10, 1.65) | 0.943 |
| T3 | 0.00 (−3.52, 3.53) | 0.09 (−1.94, 2.13) | ||
| Osbond acid, 22:5 n-6 | ||||
| T1 | ref. | ref. | ||
| T2 1 | −1.74 (−4.97, 1.48) | 0.449 | −1.22 (−3.05, 0.61) | 0.002 |
| T3 | −2.03 (−5.51, 1.45) | −3.47 (−5.44, −1.49) | ||
| T2 2 | −1.96 (−5.18, 1.26) | 0.197 | −1.22 (−3.07, 0.63) | 0.001 |
| T3 | −3.20 (−6.73, 0.33) | −3.71 (−5.73, −1.70) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zec, M.M.; Schutte, A.E.; Ricci, C.; Baumgartner, J.; Kruger, I.M.; Smuts, C.M. Long-Chain Polyunsaturated Fatty Acids Are Associated with Blood Pressure and Hypertension over 10-Years in Black South African Adults Undergoing Nutritional Transition. Foods 2019, 8, 394. https://doi.org/10.3390/foods8090394
Zec MM, Schutte AE, Ricci C, Baumgartner J, Kruger IM, Smuts CM. Long-Chain Polyunsaturated Fatty Acids Are Associated with Blood Pressure and Hypertension over 10-Years in Black South African Adults Undergoing Nutritional Transition. Foods. 2019; 8(9):394. https://doi.org/10.3390/foods8090394
Chicago/Turabian StyleZec, Manja M., Aletta E. Schutte, Cristian Ricci, Jeannine Baumgartner, Iolanthe M. Kruger, and Cornelius M. Smuts. 2019. "Long-Chain Polyunsaturated Fatty Acids Are Associated with Blood Pressure and Hypertension over 10-Years in Black South African Adults Undergoing Nutritional Transition" Foods 8, no. 9: 394. https://doi.org/10.3390/foods8090394
APA StyleZec, M. M., Schutte, A. E., Ricci, C., Baumgartner, J., Kruger, I. M., & Smuts, C. M. (2019). Long-Chain Polyunsaturated Fatty Acids Are Associated with Blood Pressure and Hypertension over 10-Years in Black South African Adults Undergoing Nutritional Transition. Foods, 8(9), 394. https://doi.org/10.3390/foods8090394