Effect of Food and Vitamin D Supplements on the Serum 25(OH)D3 Concentration in Children during Winter Months

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Study Population
2.3. Measurements
2.4. Statistical Analysis
2.5. Ethical Committee
3. Results and Discussion
3.1. Descriptives

{kind=link}
| Characteristic | Patients ( n = 174) |
|---|---|
| Age, median (IQR) (years) | 8.5 (5.0–13.1) |
| Gender, number (%) | |
| Female | 89 (51.1%) |
| Male | 85 (48.9%) |
| Serum 25(OH)D concentration, mean ± SD (nmol/L) | 52.0 ± 18.4 |
| Vitamine D obtained with the total amount of food per day, mean ± SD (μg) | 1.3 ± 1.9 |
| Vitamin D obtained with milk per day, mean ± SD (μg) | 0.5 ± 1.8 |
| Vitamin D obtained with butter per day, mean ± SD (μg) | 0.7 ± 0.5 |
| Vitamin D obtained with fish, mean ± SD (μg) | 0.1 ± 0.2 |
| Vitamin D obtained with vitamin D supplements, mean ± SD (μg) | 3.4 ± 4.8 |
| Groups | Butter (μg) | Milk (μg) | Fish (μg) | Supplementation (μg) | Total (μg) |
|---|---|---|---|---|---|
| Toddlers (1–4 years old) | 0.7 ± 0.3 | 3.2 ± 3.7 | 0.0 ± 0.1 | 5.8 ± 4.8 | 9.7 |
| School-aged (4–12 years old) | 0.8 ± 0.5 | 0.3 ± 1.5 | 0.1 ± 0.2 | 3.8 ± 4.6 | 5.0 |
| Adolescents (>12 years old) | 0.6 ± 0.6 | 0.0 ± 0.2 | 0.2 ± 0.3 | 1.8 ± 4.8 | 2.6 |
3.2. Correlations
| Variables | Linear regression B * (95% CI **); ß, coefficient |
|---|---|
| Gender | −1.7 (−7.2–3.8), p = 0.535; ß = −0.047 |
| Total amount of vitamin D obtained from food | 2.1 (0.7–3.5), p = 0.004 ***; ß = 0.218 |
| Milk | 1.9 (0.4–3.4), p = 0.014 ***; ß = 0.186 |
| Butter | 4.2 (−0.9–9.3), p = 0.106; ß = 0.124 |
| Fish | 4.8 (−9.2–18.8), p = 0.497; ß = 0.052 |
| Vitamin D supplements | 0.3 (−0.3–0.9), p = 0.315; ß = 0.077 |
3.3. Linear Regression
| Variables | Linear regression B * (95% CI **); ß, coefficient |
|---|---|
| Yogurt drinks and chocolate milk | −0.6 (−6.7–5.6), p = 0.856; ß = −0.014 |
| Semi-skimmed milk | −3.1 (−9.4–3.1), p = 0.325; ß = −0.075 |
| Whole milk | 7.0 (−2.0–16.0), p = 0.127; ß = 0.116 |
| Residual group | 5.0 (−1.7–11.7), p = 0.143; ß = 0.111 |
3.4. Food or Supplements?
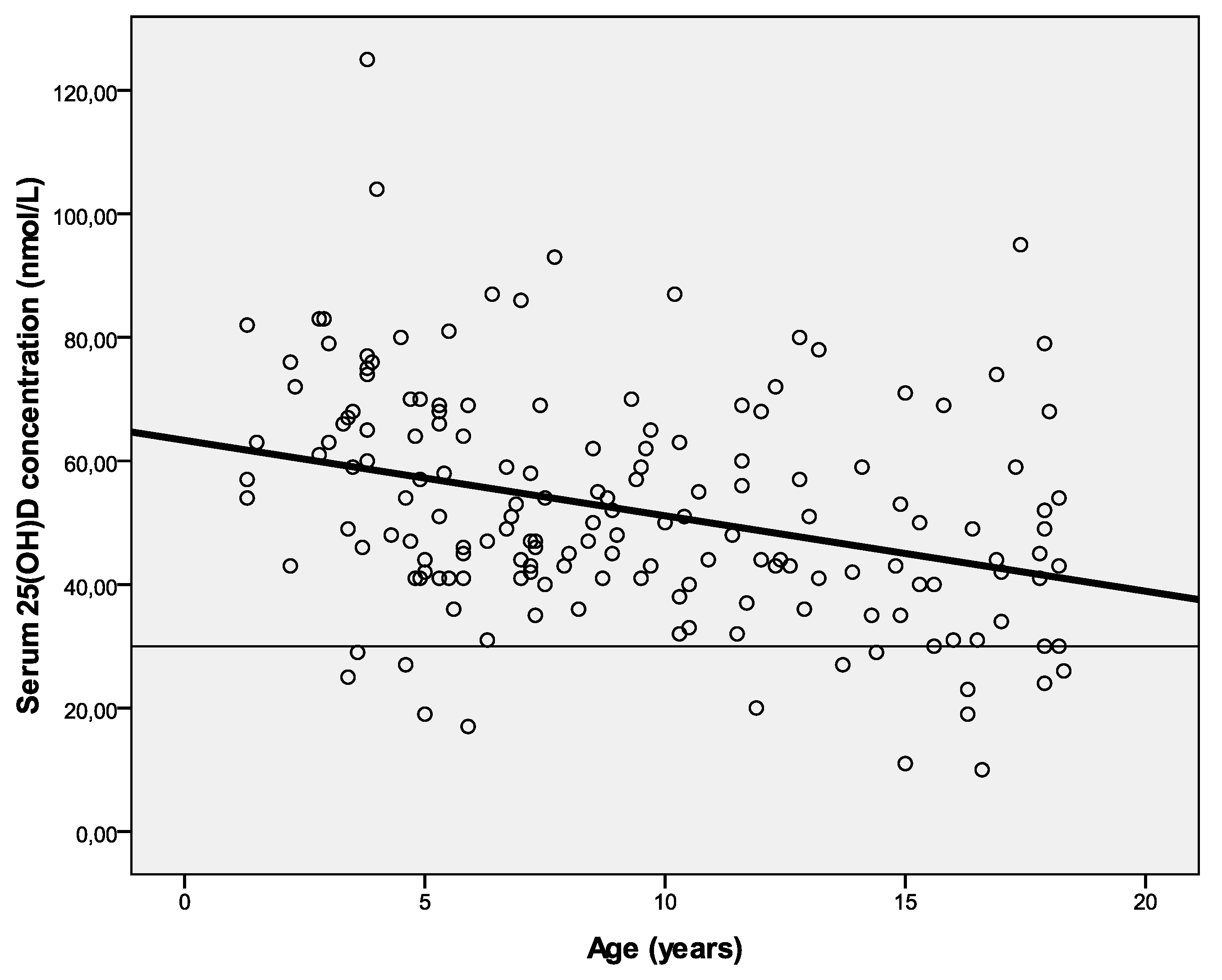
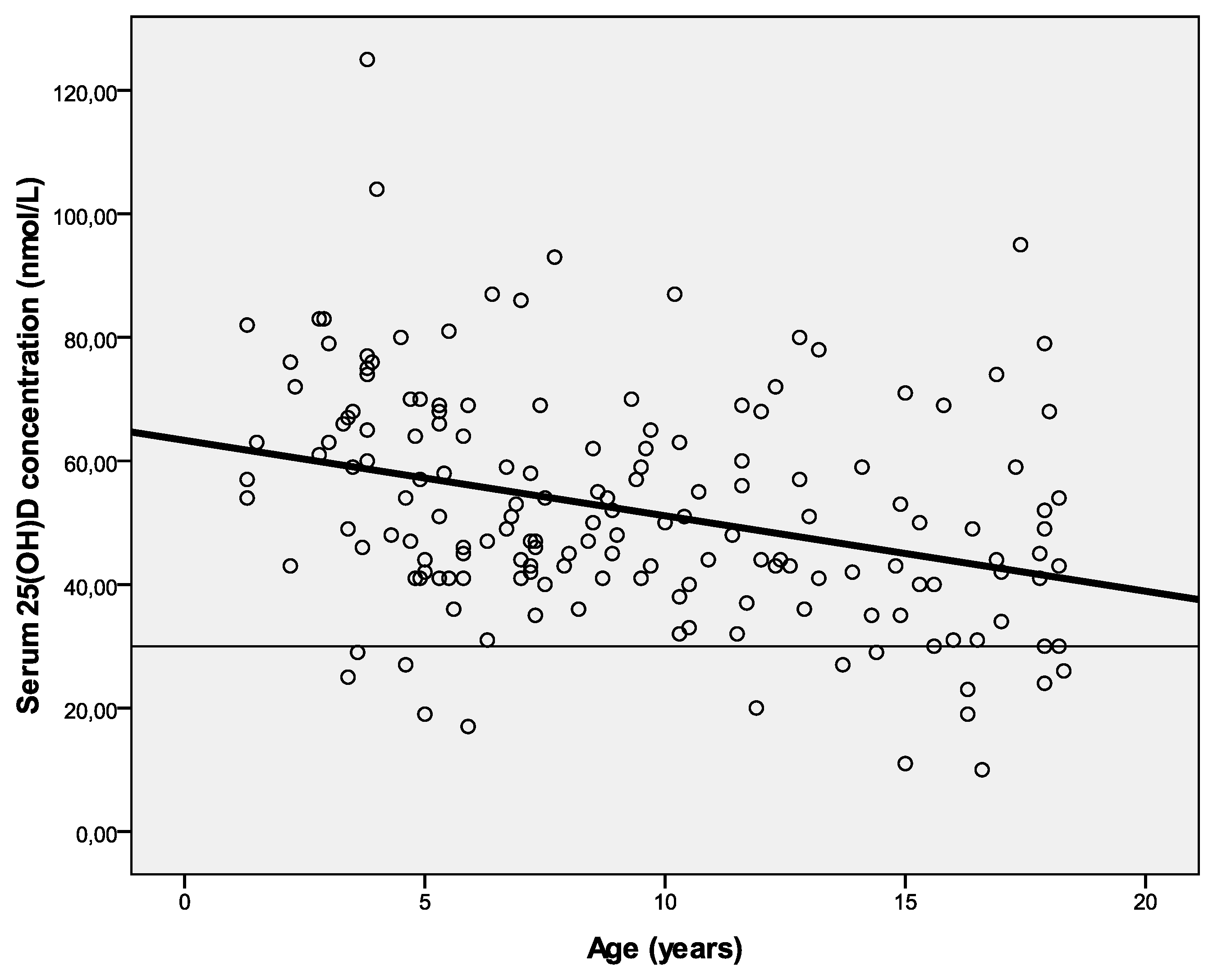
3.5. Intake and Age
3.6. Food Sources
3.7. Limitations
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Holick, M.F. Vitamin D: A D-lightful solution for health. J. Investig. Med. 2011, 59, 872–880. [Google Scholar]
- Webb, A.R. Who, what, where and when-influences on cutaneous vitamin D synthesis. Prog. Biophys. Mol. Biol. 2006, 92, 17–25. [Google Scholar]
- Weggemans, R.M.; Schaafsma, G.; Kromhout, D. Towards an adequate intake of vitamin D. An advisory report of the Health Council of the Netherlands. Eur. J. Clin. Nutr. 2009, 63, 1455–1457. [Google Scholar]
- Webb, A.R.; Kline, L.; Holick, M.F. Influence of season and latitude on the cutaneous synthesis of vitamin D3: Exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in human skin. J. Clin. Endocrinol. Metab. 1988, 67, 373–378. [Google Scholar]
- Hennessy, A.; Walton, J.; Flynn, A. The impact of voluntary food fortification on micronutrient intakes and status in European countries. Proc. Nutr. Soc. 2013, 72, 433–440. [Google Scholar]
- Van Rossum, C.T.M.; Fransen, H.P.; Verkaik-Kloosterman, J.; Buurma-Rethans, E.J.M.; Ocke, M.C. Dutch National Food Consumption Survey 2007–2010: Diet of Children and Adults Aged 7 to 69 Years. Available online: http://www.rivm.nl/bibliotheek/rapporten/350050006.html (accessed on 12 July 2014).
- Van der Meer, I.M.; Boeke, A.J.; Lips, P.; Grootjans-Geerts, I.; Wuister, J.D.; Devillé, W.L.; Wielders, J.P.; Bouter, L.M.; Middelkoop, B.J. Fatty fish and supplements are the greatest modifiable contributors to the serum 25-hydroxyvitamin D concentration in a multiethnic population. Clin. Endocrinol. (Oxf.) 2008, 68, 466–472. [Google Scholar]
- Gezondheidsraad. Evaluatie van de Voedingsnormen voor Vitamine D. Available online: http://www.gezondheidsraad.nl/sites/default/files/201215evaluatievoedingsnormenvitamineD.pdf (accessed on 6 April 2013).
- Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellof, M.; Fewtrell, M.; Hojsak, I.; Mihastsch, W.; Molgaard, C.; Shamir, R.; et al. Vitamin D in the healthy paediatric population. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 692–701. [Google Scholar]
- Nederlands Voedingsstoffenbestand (NEVO). Available online: http://nevo-online.rivm.nl/ (accessed on 5 April 2013).
- Roth, D.E.; Martz, P.; Yeo, R.; Prosser, C.; Bell, M.; Jones, A.B. Are national vitamin D guidelines sufficient to maintain adequate blood levels in children? Can. J. Public Health 2005, 96, 443–449. [Google Scholar]
- Rajakumar, K.; Holick, M.F.; Jeong, K.; Moore, C.G.; Chen, T.C.; Olabopo, F.; Haralam, M.A.; Nucci, A.; Thomas, S.B.; Greenspan, S.L. Impact of season and diet on vitamin D status of African American and Caucasian children. Clin. Pediatr. (Phila) 2011, 50, 493–502. [Google Scholar]
- Absoud, M.; Cummins, C.; Lim, M.J.; Wassmer, E.; Shaw, N. Prevalence and predictors of vitamin D insufficiency in children: A Great Britain population based study. PLoS One 2011, 6, e22179. [Google Scholar]
- Carpenter, T.O.; Herreros, F.; Zhang, J.H.; Ellis, B.K.; Simpson, C.; Torrealba-Fox, E.; Kim, G.J.; Savoye, M.; Held, N.A.; Cole, D.E. Demographic, dietary, and biochemical determinants of vitamin D status in inner-city children. Am. J. Clin. Nutr. 2012, 95, 137–146. [Google Scholar]
- Heaney, R.P.; Armas, L.A.; French, C. All-source basal vitamin D inputs are greater than previously thought and cutaneous inputs are smaller. J. Nutr. 2013, 143, 571–575. [Google Scholar]
- Schmid, A.; Walther, B. Natural vitamin D content in animal products. Adv. Nutr. 2013, 4, 453–462. [Google Scholar]
- Ovesen, L.; Brot, C.; Jakobsen, J. Food contents and biological activity of 25-hydroxyvitamin D: A vitamin D metabolite to be reckoned with? Ann. Nutr. Metab. 2003, 47, 107–113. [Google Scholar]
- Jakobsen, J. Bioavailability and bioactivity of vitamin D3 active compounds—Which potency should be used for 25-hydroxyvitamin D3? Int. Congr. Ser. 2007, 1297, 133–142. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van der Gaag, E.; Brekhoff, L. Effect of Food and Vitamin D Supplements on the Serum 25(OH)D3 Concentration in Children during Winter Months. Foods 2014, 3, 632-641. https://doi.org/10.3390/foods3040632
Van der Gaag E, Brekhoff L. Effect of Food and Vitamin D Supplements on the Serum 25(OH)D3 Concentration in Children during Winter Months. Foods. 2014; 3(4):632-641. https://doi.org/10.3390/foods3040632
Chicago/Turabian StyleVan der Gaag, Ellen, and Lisanne Brekhoff. 2014. "Effect of Food and Vitamin D Supplements on the Serum 25(OH)D3 Concentration in Children during Winter Months" Foods 3, no. 4: 632-641. https://doi.org/10.3390/foods3040632