Self-Reported Changes in Oral Hygiene Habits among Adolescents Receiving Orthodontic Treatment


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. The Questionnaire
2.3. Statistical Analysis
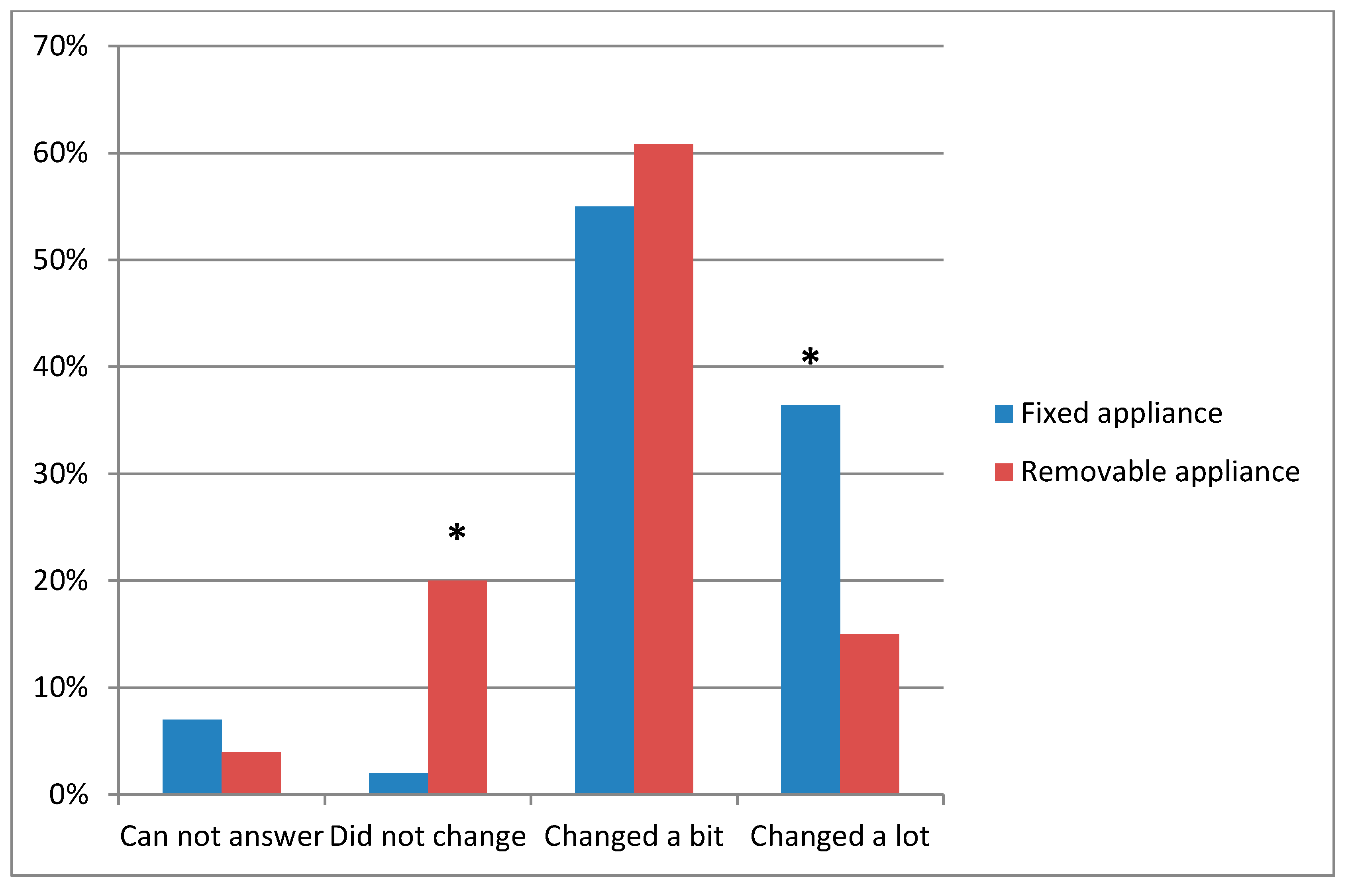
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| LSMU | Lithuanian University of Medical Sciences |
| M | Mean Score |
| SD | Standard Deviation |
| OR | Odds Ratio |
References
- Ashkenazi, M.; Salem, N.F.; Garon, S.; Levin, L. Evaluation of orthodontic and triple-headed toothbrushes when used alone or in conjunction with single-tufted toothbrush in patients with fixed lingual orthodontic appliances. A randomized clinical trial. N. Y. State Dent. J. 2015, 81, 31–37. [Google Scholar] [PubMed]
- De Baets, E.; Lambrechts, H.; Lemiere, J.; Diya, L.; Willems, G. Impact of self-esteem on the relationship between orthodontic treatment need and oral health-related quality of life in 11–16-year-old children. Eur. J. Orthod. 2012, 34, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Nashashibi, S.; Darwish, S.K.; Khalifa El, R. Prevalence of malocclusion and treatment needs in Riadh (Saudi Arabia). Odontostomatol. Trop. 1983, 4, 209–214. [Google Scholar]
- Tayer, B.H.; Burek, M.J. A survey of adults’ attitudes toward orthodontic therapy. Am. J. Orthod. 1981, 79, 305–315. [Google Scholar] [CrossRef]
- Imani, M.M.; Jalali, A.; Dinmohammadi, M.; Nouri, P. The Effect of Orthodontic Intervention on Mental Health and Body Image. Open Access Maced. J. Med. Sci. 2018, 17, 1132–1137. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, M.B. Selling orthodontic need: Innocent business decision or guilty pleasure? J. Med. Ethics 2010, 36, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Meeran, N.A. Iatrogenic possibilities of orthodontic treatment and modalities of prevention. J. Orthod. Sci. 2013, 2, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, P.; Dasar, P.; Nagarajappa, S.; Mishra, P.; Kumar, S.; Balsaraf, S.; Lalani, A.; Chauhan, A. Impact of dental neglect scale on oral health status among different professionals in Indore aity—A cross—Sectional study. J. Clin. Diagn. Res. 2015, 9, 67–70. [Google Scholar] [CrossRef]
- Lara-Carrillo, E.; Montiel-Bastida, N.M.; Sánchez-Pérez, L.; Alanís-Tavira, J. Effect of orthodontic treatment on saliva, plaque and the levels of Streptococcus mutans and Lactobacillus. Med. Oral Patol. Oral Cir. Bucal. 2010, 15, 924–929. [Google Scholar] [CrossRef]
- Oberoi, S.S.; Mohanty, V.; Mahajan, A.; Oberoi, A. Evaluating awareness regarding oral hygiene practices and exploring gender differences among patients attending for oral prophylaxis. J. Indian Soc. Periodontol. 2014, 18, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Arici, S.; Alkan, A.; Arici, N. Comparison of different toothbrushing protocols in poor-toothbrushing orthodontic patients. Eur. J. Orthod. 2007, 29, 488–492. [Google Scholar] [CrossRef]
- Koopman, J.E.; van der Kaaij, N.C.; Buijs, M.J.; Elyassi, Y.; van der Veen, M.H.; Crielaard, W.; Ten Cate, J.M.; Zaura, E. The effect of fixed orthodontic appliances and fluoride mouthwash on the oral microbiome of adolescents—A randomized controlled clinical trial. PLoS ONE 2015, 10, e0137318. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Jongsma, M.A.; Mei, L.; van der Mei, H.C.; Busscher, H.J. Orthodontic treatment with fixed appliances and biofilm formation—A potential public health threat? Clin. Oral Investig. 2014, 18, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Gomes, S.C.; Varela, C.C.; da Veiga, S.L.; Rösing, C.K.; Oppermann, R.V. Periodontal conditions in subjects following orthodontic therapy. A preliminary study. Eur. J. Orthod. 2007, 29, 477–481. [Google Scholar] [CrossRef]
- Ristic, M.; Vlahovic Svabic, M.; Sasic, M.; Zelic, O. Clinical and microbiological effects of fixed orthodontic appliances on periodontal tissues in adolescents. Orthod. Craniofac. Res. 2007, 10, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Karkhanechi, M.; Chow, D.; Sipkin, J.; Sherman, D.; Boylan, R.J.; Norman, R.G.; Craig, R.G.; Cisneros, G.J. Periodontal status of adult patients treated with fixed buccal appliances and removable aligners over one year of active orthodontic therapy. Angle Orthod. 2013, 83, 146–151. [Google Scholar] [CrossRef]
- Wheeler, T.T.; McGorray, S.P.; Dolce, C.; Taylor, M.G.; King, G.J. Effectiveness of early treatment of Class II malocclusion. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Turatti, G.; Womack, R.; Bracco, P. Incisor intrusion with Invisalign treatment of an adult periodontal patient. J. Clin. Orthod. 2006, 40, 171–174. [Google Scholar]
- Saxer, U.P.; Yankell, S.L. Impact of improved toothbrushes on dental diseases. I. Quintessence Int. 1997, 28, 513–525. [Google Scholar]
- Chhibber, A.; Agarwal, S.; Yadav, S.; Kuo, C.L.; Upadhyay, M. Which orthodontic appliance is best for oral hygiene? A randomized clinical trial. Am. J. Orthod Dentofac. Orthop. 2018, 153, 175–183. [Google Scholar] [CrossRef]
- Gao, X.; Lo, E.C.; McGrath, C.; Ho, S.M. Innovative interventions to promote positive dental health behaviors and prevent dental caries in preschool children: Study protocol for a randomized controlled trial. Trials 2013, 14, 118. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Rollnick, S. Ten things that motivational interviewing is not. Behav. Cogn. Psychother. 2009, 37, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Moyers, T.B.; Martin, T.; Manuel, J.K.; Hendrickson, S.M.; Miller, W.R. Assessing competence in the use of motivational interviewing. J. Subst. Abuse Treat. 2005, 28, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Van der Kaaij, N.C.; van der Veen, M.H.; van der Kaaij, M.A.; ten Cate, J.M. A prospective, randomized placebo-controlled clinical trial on the effects of a fluoride rinse on white spot lesion development and bleeding in orthodontic patients. Eur. J. Oral Sci. 2015, 123, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Bos, A.; Kleverlaan, C.J.; Hoogstraten, J.; Prahl-Andersen, B.; Kuitert, R. Comparing subjective and objective measures of headgear compliance. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 801–805. [Google Scholar] [CrossRef]
- Tervonen, M.; Pirttiniemi, P.; Lahti, S. Development of a measure for orthodontists to evaluate patient compliance. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Kardelis, K. Mokslinių Tyrimų Metodologija ir Metodai, 6th ed.; Mokslo ir enciklopedijų leidybos centras: Vilnius, Lithuania, 2017; pp. 147–172. [Google Scholar]
- Sidlauskas, A.; Lopatiene, K. The prevalence of malocclusion among 7–15-year-old Lithuanian schoolchildren. Medicina 2009, 45, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Kavaliauskienė, A.; Šidlauskas, A.; Zaborskis, A. Relationship between orthodontic treatment need and oral health-related quality of life among 11–18-year-old adolescents in Lithuania. Int. J. Environ. Res. Public Health 2018, 17, 1012. [Google Scholar] [CrossRef]
- Baubiniene, D.; Sidlauskas, A.; Miseviciene, I. The need for orthodontic treatment among 10–11- and 14–15-year-old Lithuanian schoolchildren. Medicina 2009, 45, 814–821. [Google Scholar] [CrossRef]
- Kavaliauskienė, A.; Sidlauskas, A.; Zaborskis, A. Demographic and social inequalities in need for orthodontic treatment among schoolchildren in Lithuania. Medicina 2010, 46, 767–773. [Google Scholar] [CrossRef]
- Mei, L.; Chieng, J.; Wong, C.; Benic, G.; Farella, M. Factors affecting dental biofilm in patients wearing fixed orthodontic appliances. Prog. Orthod. 2017, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Eid, H.A.; Assiri, H.A.; Kandyala, R.; Togoo, R.A.; Turakhia, V.S. Gingival enlargement in different age groups during fixed Orthodontic treatment. J. Int. Oral Health 2014, 6, 1–4. [Google Scholar] [PubMed]
- Pandey, V.; Chandra, S.; Dilip Kumar, H.P.; Gupta, A.; Bhandari, P.P.; Rathod, P. Impact of dental neglect score on oral health among patients receiving fixed orthodontic treatment. A cross-sectional study. J. Int. Soc. Prev. Community Dent. 2016, 6, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Baheti, M.J.; Toshniwal, N.G. Survey on oral hygiene protocols among orthodontic correction-seeking individuals. J. Educ. Ethics Dent. 2015, 5, 8–13. [Google Scholar] [CrossRef]
- Krupińska-Nanys, M.; Zarzecka, J. An assessment of oral hygiene in 7–14 year-old children undergoing orthodontic treatment. J. Int. Oral Health. 2015, 7, 6–11. [Google Scholar]
- Sharma, R.; Trehan, M.; Sharma, S.; Jharwal, V.; Rathore, N. Comparison of effectiveness of manual orthodontic, powered and sonic toothbrushes on oral hygiene of fixed orthodontic patients. Int. J. Clin. Pediatr. Dent. 2015, 8, 181189. [Google Scholar] [CrossRef]
- Mazzoleni, S.; Bonaldo, G.; Pontarolo, E.; Zuccon, A.; De Francesco, M.; Stellini, E. Experimental assessment of oral hygiene achieved by children wearing rapid palatal expanders, comparing manual and electric toothbrushes. Int. J. Dent. Hyg. 2014, 12, 187–192. [Google Scholar] [CrossRef]
- Erbe, C.; Klukowska, M.; Tsaknaki, I.; Timm, H.; Grender, J.; Wehrbein, H. Efficiacy of 3 toothbrush treatments on plaque removal in orthodontic patients assessed with digital plaque imaging: A randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 760–766. [Google Scholar] [CrossRef]
- Tilliss, T.; Carey, C.M. Insufficient Evidence within a Systematic Review and Meta-Analysis of Powered Toothbrushes over Manual Toothbrushes for Soft Tissue Health during Orthodontic Treatment. J. Evid. Based Dent. Pract. 2018, 18, 176–177. [Google Scholar] [CrossRef]
- Al Makhmari, S.A.; Kaklamanos, E.G.; Athanasiou, A.E. Short-term and long-term effectiveness of powered toothbrushes in promoting periodontal health during orthodontic treatment: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 753–766. [Google Scholar] [CrossRef]
- Enerbäck, H.; Möller, M.; Nylén, C.; Ödman Bresin, C.; Östman Ros, I.; Westerlund, A. Effects of orthodontic treatment and different fluoride regimens on numbers of cariogenic bacteria and caries risk: A randomized controlled trial. Eur. J. Orthod. 2019, 41, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Anuwongnukroh, N.; Dechkunakorn, S.; Kanpiputana, R. Oral Hygiene Behavior during Fixed Orthodonic Treatment. Dentistry 2017, 7, 457. [Google Scholar] [CrossRef]
- Nadar, S.; Dinesh, S.P. A questionnaire study about oral hygiene awareness among orthodontic patients. Int. J. Orthod. Rehabil. 2016, 7, 97–100. [Google Scholar] [CrossRef]
- Scheerman, J.F.M.; van Empelen, P.; van Loveren, C.; Pakpour, A.H.; van Meijel, B.; Gholami, M.; Mierzaie, Z.; van den Braak, M.C.T.; Verrips, G.H.W. An application of the health action process approach model to oral hygiene behaviour and dental plaque in adolescents with fixed orthodontic appliances. Int. J. Paediatr. Dent. 2017, 27, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Zanatta, F.B.; Moreira, C.H.; Rösing, C.K. Association between dental floss use and gingival conditions in orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Abuaffan, A.H.; Elamin, L.T. Oral hygiene performance among a sample of sudanese orthodontic patients. J. Dent. Oral. Hyg. 2015, 1, 1–8. [Google Scholar]
- Lee, J.H.; Abdullah, A.A.A.; Yahya, N.A. Oral Hygiene Practices among Fixed. Orthodontic Patients in a University Dental Setting. Int. J. Oral Dent. Health 2016, 2, 27. [Google Scholar] [CrossRef]
- Sobouti, F.; Rakhshan, V.; Heydari, M.; Keikavusi, S.; Dadgar, S.; Shariati, M. Effects of fixed orthodontic treatment and two new mouth rinses on gingival health: A prospective cohort followed by a single-blind placebo-controlled randomized clinical trial. Int. Orthod. 2018, 16, 12–30. [Google Scholar] [CrossRef]
- Langlie, J.K. Social networks, health beliefs, and preventive health behavior. J. Health Soc. Behav. 1977, 18, 244–260. [Google Scholar] [CrossRef]
- Khraisat, H.M.; Al-Shdeifat, N.A.; Al-Alawneh, A.M.; Al-Zyood, A.I.; Al-Maani, M.O. Oral hygiene practices among fixed orthodontic patients in Az-Zarqua, Jordan. Pak. Oral Dent. J. 2016, 36, 404–407. [Google Scholar]
- Cozzani, M.; Ragazzini, G.; Delucchi, A.; Mutinelli, S.; Barreca, C.; Rinchuse, D.J.; Servetto, R.; Piras, V. Oral hygiene compliance in orthodontic patients: A randomized controlled study on the effects of a post-treatment communication. Prog. Orthod. 2016, 17, 41. [Google Scholar] [CrossRef] [PubMed]
- Al Shammary, N.; Asimakopoulou, K.; McDonald, F.; Newton, J.T.; Scambler, S. How is adult patient adherence recorded in orthodontists’ clinical notes? A mixed—Method case-note study. Patient Prefer. Adherence 2017, 11, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Kudirkaite, I.; Lopatiene, K.; Zubiene, J.; Saldunaite, K. Age and gender influence on oral hygiene among adolescents with fixed orthodontic appliances. Stomatologija 2016, 18, 61–65. [Google Scholar] [PubMed]


{kind=link}
| Control Group N (%) | Patients Receiving Orthodontic Treatment N (%) | Total N (%) | |
|---|---|---|---|
| Gender (Missing N = 1) | |||
| Girls | 65 (53.7) | 99 (58.6) | 164 (56.6) |
| Boys | 56 (46.3) | 70 (41.4) | 126 (43.4) |
| Total N (%) | 121 (100) | 169 (100) | 290 (100) |
| Age (Years) | |||
| 10–12 | 65 (53.7) | 80 (47.1) | 145 (49.8) |
| 13–17 | 56 (46.3) | 90 (52.9) | 146 (50.2) |
| Total N (%) | 121 (100) | 170 (100) | 291 (100) |
| Place of Residence (Missing N = 4) | |||
| Urban | 88 (73.9) | 125 (74.4) | 213 (74.2) |
| Rural | 31 (26.1) | 43 (25.6) | 74 (25.8) |
| Total N (%) | 119 (100) | 168 (100) | 287 (100) |
| Control Group N (%) | Patients Receiving Orthodontic Treatment N (%) | Total N (%) | p-Value | ||
|---|---|---|---|---|---|
| Fixed Appliance | Removable Appliance | ||||
| Frequency of Tooth Brushing (missing N = 4) | |||||
| Irregularly | 16 (13.2) | 1 (2.3) | 11 (9.0) | 28 (9.8) | 0.171 |
| Once a day | 36 (29.8) | 10 (22.7) | 36 (29.5) | 82 (28.6) | |
| ≥2 times a day | 69 (57.0) | 33 (75.0) | 75 (61.5) | 177 (61.6) | |
| Total N (%) | 121 (100) | 44 (100) | 122 (100) | 287 (100) | |
| Duration of Tooth Brushing (missing N = 5) | |||||
| ≤1 min | 18 (15.0) | 8 (18.2) | 29 (23.8) | 55 (19.2) | 0.220 |
| ≥2 min | 102 (85.0) | 36 (81.8) | 93 (76.2) | 231 (80.8) | |
| Total N (%) | 120 (100) | 44 (100) | 122 (100) | 286 (100) | |
| Type of Toothbrush (missing N = 4) | |||||
| Manual | 115 (95.0) | 42 (95.5) | 117 (95.9) | 274 (95.5) | 0.899 |
| Powered | 6 (5.0) | 2 (4.5) | 5 (4.1) | 13 (4.5) | |
| Total N (%) | 121 (100) | 44 (100) | 122 (100) | 287 (100) | |
| Type of Toothpaste (missing N = 4) | |||||
| With fluoride | 44 (36.1) | 20 (45.5) | 43 (35.3) | 107 (37.2) | 0.926 |
| Fluoride-free | 16 (13.1) | 6 (13.6) | 21 (17.2) | 43 (14.9) | |
| Do not know | 62 (50.8) | 18 (40.9) | 58 (47.5) | 138 (47.9) | |
| Total N (%) | 122 (100) | 44 (100) | 122 (100) | 288 (100) | |
| Mouth Rinsing After Meals (missing N = 11) | |||||
| Yes | 62 (54.4) | 35 (79.5) | 77 (63.1) | 174 (62.1) | 0.013 |
| No | 52 (45.6) | 9 (20.5) | 45 (36.9) | 106 (37.9) | |
| Total N (%) | 114 (100) | 44 (100) | 122 (100) | 280 (100) | |
| Gender * N (%) | Area ** N (%) | Orthodontic Treatment *** N (%) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Boys | Girls | Rural | Urban | Yes | No | ||
| Usage of Auxiliary Interproximal Measures | |||||||
| Yes | 53 (42.7) | 89 (54.6) | 32 (44.4) | 108 (50.9) | 93 (56.0) | 49 (40.8) | p = 0.133 * p = 0.017 ** p = 0.015 *** |
| No | 71 (57.3) | 74 (45.4) | 40 (55.6) | 104 (49.1) | 73 (44.0) | 71 (59.2) | |
| Total N (%) | 124 (100) | 163 (100) | 72 (100) | 212 (100) | 166 (100) | 120 (100) | |
| Tongue Cleaning | |||||||
| Yes | 42 (33.3) | 81 (49.4) | 29 (39.2) | 91 (42.7) | 81 (47.6) | 42 (34.7) | p = 0.006 * p = 0.595 ** p = 0.028 *** |
| No | 84 (66.7) | 83 (50.6) | 45 (60.8) | 122 (57.3) | 89 (52.4) | 79 (65.3) | |
| Total N (%) | 126 (100) | 164 (100) | 74 (100) | 213 (100) | 170 (100) | 121 (100) | |
| Dental Appointments | |||||||
| Irregular | 15 (12.3) | 35 (22.3) | 15 (21.7) | 33 (15.9) | 27 (16.3) | 23 (20.2) | p = 0.05 * p = 0.035 ** p = 0.420 *** |
| Twice a year | 41 (33.6) | 38 (24.2) | 26 (37.7) | 53 (25.6) | 44 (26.5) | 35 (30.7) | |
| Once a year | 66 (54.1) | 84 (53.5) | 28 (40.6) | 121 (58.5) | 95 (57.2) | 56 (49.1) | |
| Total N (%) | 122 (100) | 157 (100) | 69 (100) | 207 (100) | 166 (100) | 114 (100) | |
| Professional Oral Hygiene | |||||||
| Yes | 44 (37.3) | 62 (41.9) | 24 (36.9) | 82 (41.4) | 72 (45.3) | 34 (31.5) | p = 0.446 * p = 0.522 ** p = 0.024 *** |
| No | 74 (62.7) | 86 (58.1) | 41 (63.1) | 116 (58.6) | 87 (54.7) | 74 (68.5) | |
| Total N (%) | 118 (100) | 148 (100) | 65 (100) | 198 (100) | 159 (100) | 108 (100) | |
| OR | 95% CI | p-Value | |
|---|---|---|---|
| Tongue Brushing | |||
| Yes | 1.712 | 1.059–2.767 | 0.028 |
| No | 1 | - | - |
| Auxiliary Measures | |||
| Yes | 1.797 | 1.118–2.887 | 0.015 |
| No | 1 | - | - |
| Mouth Rinsing After Meals | |||
| Yes | 1.707 | 1.048–2.781 | 0.032 |
| No | 1 | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrauskiene, S.; Wanczewska, N.; Slabsinskiene, E.; Zemgulyte, G. Self-Reported Changes in Oral Hygiene Habits among Adolescents Receiving Orthodontic Treatment. Dent. J. 2019, 7, 96. https://doi.org/10.3390/dj7040096
Petrauskiene S, Wanczewska N, Slabsinskiene E, Zemgulyte G. Self-Reported Changes in Oral Hygiene Habits among Adolescents Receiving Orthodontic Treatment. Dentistry Journal. 2019; 7(4):96. https://doi.org/10.3390/dj7040096
Chicago/Turabian StylePetrauskiene, Sandra, Natalia Wanczewska, Egle Slabsinskiene, and Gintare Zemgulyte. 2019. "Self-Reported Changes in Oral Hygiene Habits among Adolescents Receiving Orthodontic Treatment" Dentistry Journal 7, no. 4: 96. https://doi.org/10.3390/dj7040096
APA StylePetrauskiene, S., Wanczewska, N., Slabsinskiene, E., & Zemgulyte, G. (2019). Self-Reported Changes in Oral Hygiene Habits among Adolescents Receiving Orthodontic Treatment. Dentistry Journal, 7(4), 96. https://doi.org/10.3390/dj7040096