Effect of Fixed Orthodontic Treatment on Salivary Nickel and Chromium Levels: A Systematic Review and Meta-Analysis of Observational Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction from Studies
2.4. Quality Evaluation
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Included Studies
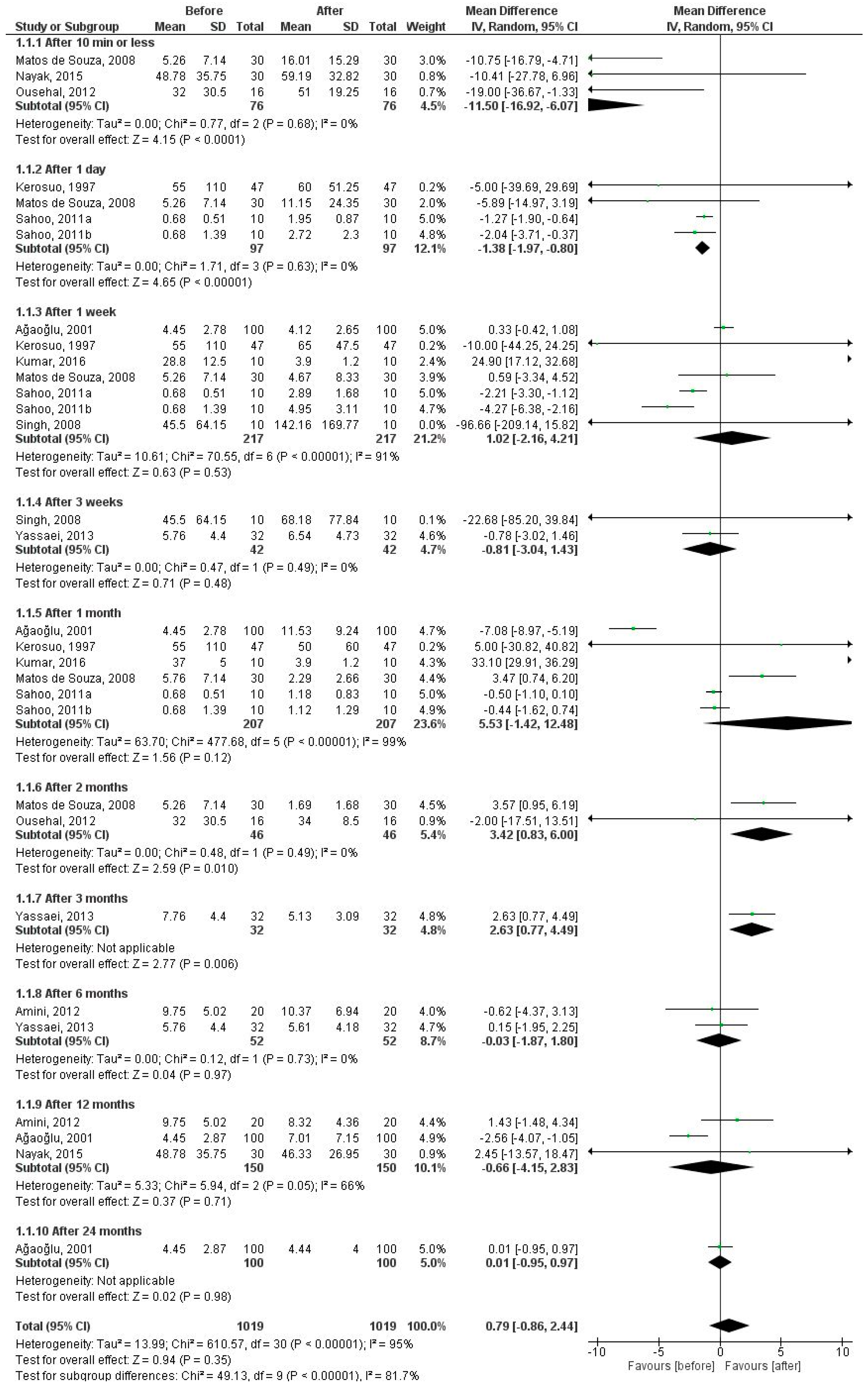
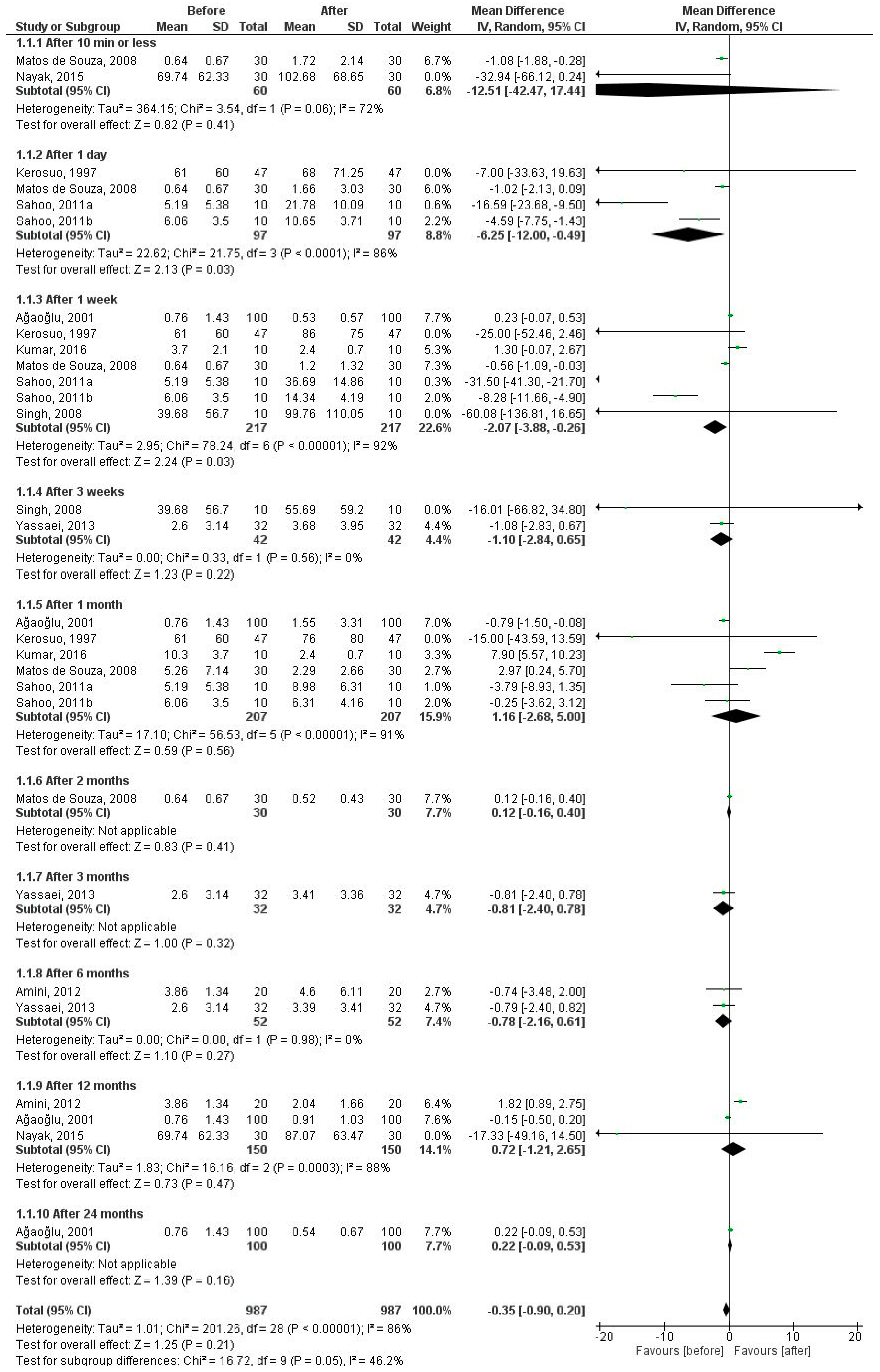
3.2. Salivary Nickel and Chromium Levels (before versus after Fixed Orthodontic Treatment)
3.2.1. Nickel Levels in 10 Time Periods
3.2.2. Chromium Levels in 10 Time Periods
3.2.3. Nickel Levels in Five Time Periods
3.3. Salivary Nickel and Chromium Levels (Case-Control Studies)
3.3.1. Nickel Levels
3.3.2. Chromium Levels
3.3.3. Quality Evaluation
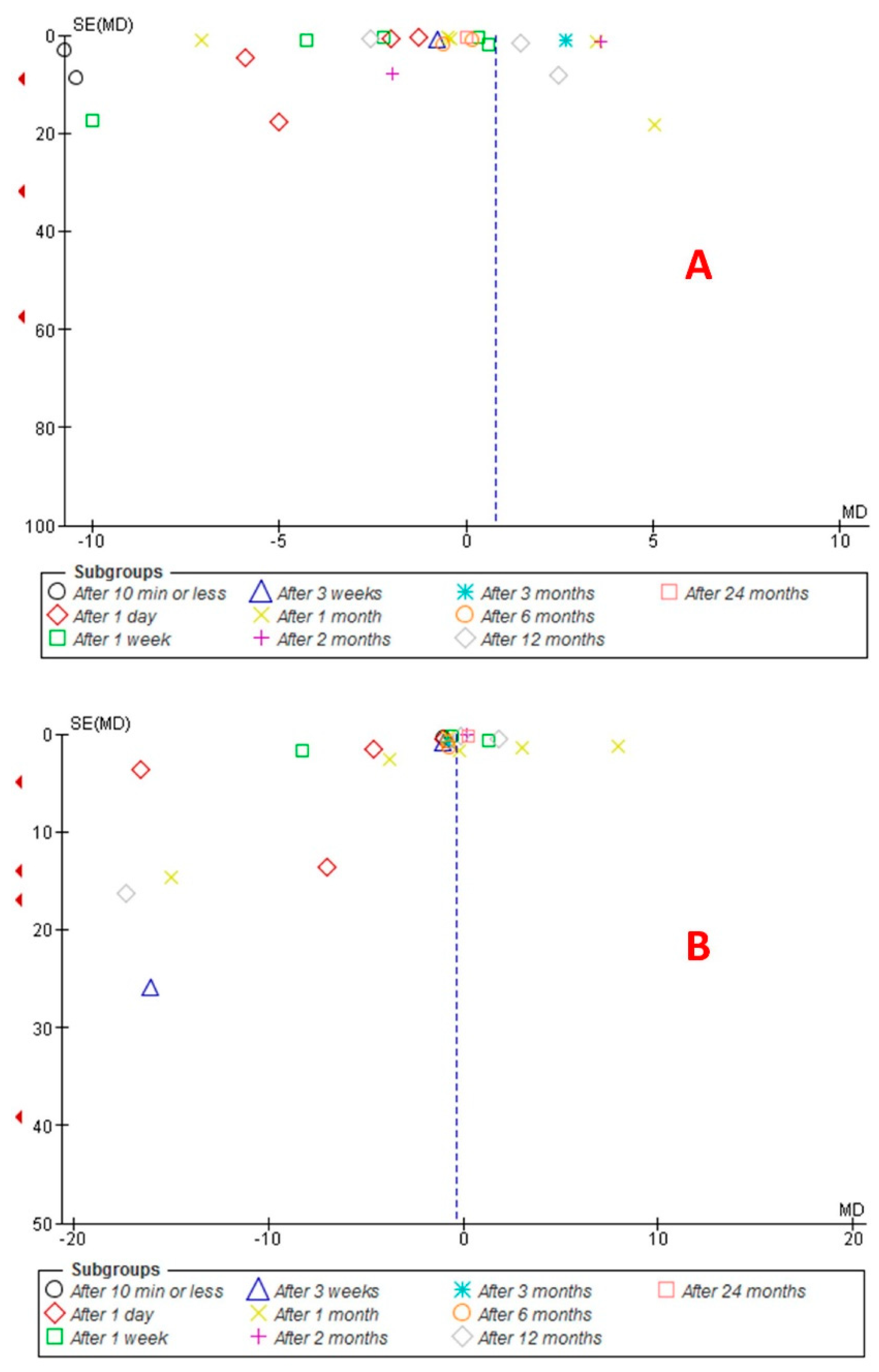
3.4. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gölz, L.; Knickenberg, A.C.; Keilig, L.; Reimann, S.; Papageorgiou, S.N.; Jäger, A.; Bourauel, C. Nickel ion concentrations in the saliva of patients treated with self-ligating fixed appliances: A prospective cohort study. J. Orofac. Orthop. 2016, 77, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Nayak, R.S.; Khanna, B.; Pasha, A.; Vinay, K.; Narayan, A.; Chaitra, K. Evaluation of Nickel and Chromium Ion Release During Fixed Orthodontic Treatment Using Inductively Coupled Plasma-Mass Spectrometer: An In Vivo Study. J. Int. Oral Health 2015, 7, 14–20. [Google Scholar] [PubMed]
- Andreasen, G.F.; Hilleman, T.B. An evaluation of 55 cobalt substituted Nitinol wire for use in orthodontics. J. Am. Dent. Assoc. 1971, 82, 1373–1375. [Google Scholar] [CrossRef] [PubMed]
- Petoumenou, E.; Arndt, M.; Keilig, L.; Reimann, S.; Hoederath, H.; Eliades, T.; Jäger, A.; Bourauel, C. Nickel concentration in the saliva of patients with nickel-titanium orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Kerosuo, H.; Moe, G.; Hensten-Pettersen, A. Salivary nickel and chromium in subjects with different types of fixed orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 1997, 111, 595–598. [Google Scholar] [CrossRef]
- Ousehal, L.; Lazrak, L. Change in nickel levels in the saliva of patients with fixed orthodontic appliances. Int. Orthod. 2012, 10, 190197. [Google Scholar] [CrossRef] [PubMed]
- Arab, S.; Nouhzadeh Malekshah, S.; Abouei Mehrizi, E.; Ebrahimi Khanghah, A.; Naseh, R.; Imani, M.M. Effect of Fixed Orthodontic Treatment on Salivary Flow, pH and Microbial Count. J. Dent. (Tehran) 2016, 13, 18–22. [Google Scholar]
- Mikulewicz, M.; Chojnacka, K. Release of metal ions from orthodontic appliances by in vitro studies: A systematic literature review. Biol. Trace Elem. Res. 2011, 139, 241–256. [Google Scholar] [CrossRef] [PubMed]
- Kocadereli, L.; Atac, P.A.; Kale, P.S.; Ozer, D. Salivary nickel and chromium in patients with fixed orthodontic appliances. Angle Orthod. 2000, 70, 431–434. [Google Scholar] [PubMed]
- Sahoo, N.; Kailasam, V.; Padmanabhan, S.; Chitharanjan, A.B. In-vivo evaluation of salivary nickel and chromium levels in conventional and self-ligating brackets. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Matos de Souza, R.; Macedo de Menezes, L. Nickel, chromium and iron levels in the saliva of patients with simulated fixed orthodontic appliances. Angle Orthod. 2008, 78, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Amini, F.; Harandi, S.; Mollaei, M.; Rakhshan, V. Effects of fixed orthodontictreatment using conventional versus metal-injection molding brackets onsalivary nickel and chromium levels: A double-blind randomized clinical trial. Eur. J. Orthod. 2015, 37, 522–5230. [Google Scholar] [CrossRef] [PubMed]
- Ağaoğlu, G.; Arun, T.; Izgi, B.; Yarat, A. Nickel and chromium levels in the saliva and serum of patients with fixed orthodontic appliances. Angle Orthod. 2001, 71, 375–379. [Google Scholar] [PubMed]
- Moffa, J.P. Council on Dental Materials, Instruments, and Equipment. Biological effects of nickel-containing dental alloys. J. Am. Dent. Assoc. 1982, 104, 501–505. [Google Scholar] [PubMed]
- Talic, N.F.; Alnahwi, H.H.; Al-Faraj, A.S. Nickel and chromium levels in the saliva of a Saudi sample treated with fixed orthodontic appliances. Saudi Dent. J. 2013, 25, 129–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eliades, T.; Bourauel, C. Intraoral aging of orthodontic materials: The picture we miss and its clinical relevance. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Robertson, J.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 January 2016).
- Egger, M.; Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.P.; Sehgal, V.; Pradhan, K.L.; Chandna, A.; Gupta, R. Estimation of nickel and chromium in saliva of patients with fixed orthodontic appliances. World J. Orthod. 2008, 9, 196–202. [Google Scholar] [PubMed]
- Kumar, R.V.; Rajvikram, N.; Rajakumar, P.; Saravanan, R.; Deepak, V.A.; Vijaykumar, V. An Accurate Methodology to detect Leaching of Nickel and Chromium Ions in the Initial Phase of Orthodontic Treatment: An in vivo Study. J. Contemp. Dent. Pract. 2016, 17, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Amini, F.; Rakhshan, V.; Mesgarzadeh, N. Effects of long-term fixed orthodontic treatment on salivary nickel and chromium levels: A 1-year prospective cohort study. Biol. Trace Elem. Res. 2012, 150, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Yassaei, S.; Dadfarnia, S.; Ahadian, H.; Moradi, F. Nickel and chromium levels in the saliva of patients with fixed orthodontic appliances. Orthodontics (Chic.) 2013, 14, e76–e81. [Google Scholar] [CrossRef] [PubMed]
- Amini, F.; Jafari, A.; Amini, P.; Sepasi, S. Metal ion release from fixed orthodontic appliances—An in vivo study. Eur. J. Orthod. 2012, 34, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Bass, J.K.; Fine, H.; Cisneros, G.J. Nickel hypersensitivity in the orthodontic patient. Am. J. Orthod. Dentofac. Orthop. 1993, 103, 280–285. [Google Scholar] [CrossRef]
- Ferguson, D.B. Current diagnostic uses of saliva. J. Dent. Res. 1987, 66, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Dawes, C. The effects of flow rate and duration of stimulation on the concentration of protein and the main electrolytes in human submandibular saliva. Arch. Oral Biol. 1974, 19, 887–895. [Google Scholar] [CrossRef]
- Bardow, A.; Lynge Petersen, A.M.; Nauntofte, B. Saliva. In Clinical Oral Physiology; Miles, T.S., Nauntofte, B., Svensson, P., Eds.; Quintessenz Verlags-GmbH: Berlin, Germany, 2004; pp. 18, 22–24, 35. [Google Scholar]
- Mikulewicz, M.; Chojnacka, K. Trace metal release from orthodontic appliances by in vivo studies: A systematic literature review. Biol. Trace Elem. Res. 2010, 137, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Fors, R.; Persson, M. Nickel in dental plaque and saliva in patients with and without orthodontic appliances. Eur. J. Orthod. 2006, 28, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Menezes, L.M.; Quintao, C.A.; Bolognese, A.M. Urinary excretion levels of nickel in orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 635–638. [Google Scholar] [CrossRef] [PubMed]
- Eliades, T.; Trapalis, C.; Eliades, G.; Katsavrias, E. Salivary metal levels of orthodontic patients: A novel methodological and analytical approach. Eur. J. Orthod. 2003, 25, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Barrett, R.D.; Bishara, S.E.; Quinn, J.K. Biodegradation of orthodontic appliances. Part I. Biodegradation of nickel and chromium in vitro. Am. J. Orthod. Dentofac. Orthop. 1993, 103, 8–14. [Google Scholar] [CrossRef]
- Tahmasbi, S.; Sheikh, T.; Hemmati, Y.B. Ion Release and Galvanic Corrosion of Different Orthodontic Brackets and Wires in Artificial Saliva. J. Contemp. Dent. Pract. 2017, 18, 222–227. [Google Scholar] [PubMed]
- Tahmasbi, S.; Ghorbani, M.; Masudrad, M. Galvanic Corrosion of and Ion Release from Various Orthodontic Brackets and Wires in a Fluoride-containing Mouthwash. J. Dent. Res. Dent. Clin. Dent. Prospects 2015, 9, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Jithesh, C.; Venkataramana, V.; Penumatsa, N.; Reddy, S.N.; Poornima, K.Y.; Rajasigamani, K. Comparative evaluation of nickel discharge from brackets in artificial saliva at different time intervals. J. Pharm. Bioallied Sci. 2015, 7, S587–S593. [Google Scholar] [PubMed]
- Mikulewicz, M.; Chojnacka, K.; Wołowiec, P. Release of metal ions from fixed orthodontic appliance: An in vitro study in continuous flow system. Angle Orthod. 2014, 84, 140–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sfondrini, M.F.; Cacciafesta, V.; Maffia, E.; Scribante, A.; Alberti, G.; Biesuz, R.; Klersy, C. Nickel release from new conventional stainless steel, recycled, and nickel-free orthodontic brackets: An in vitro study. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Sfondrini, M.F.; Cacciafesta, V.; Maffia, E.; Massironi, S.; Scribante, A.; Alberti, G.; Biesuz, R.; Klersy, C. Chromium release from new stainless steel, recycled and nickel-free orthodontic brackets. Angle Orthod. 2009, 79, 361–367. [Google Scholar] [CrossRef] [PubMed]
- House, K.; Sernetz, F.; Dymock, D.; Sandy, J.R.; Ireland, A.J. Corrosion of orthodontic appliances—Should we care? Am. J. Orthod. Dentofac. Orthop. 2008, 133, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.J.; Shin, J.S.; Cha, J.Y. Metal release from simulated fixed orthodontic appliances. Am. J. Orthod Dentofac. Orthop. 2001, 120, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Lages, R.B.; Bridi, E.C.; Pérez, C.A.; Basting, R.T. Salivary levels of nickel, chromium, iron, and copper in patients treated with metal or esthetic fixed orthodontic appliances: A retrospective cohort study. J. Trace Elem. Med. Biol. 2017, 40, 67–71. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Description |
|---|---|
| Population | Eligible patients for fixed orthodontic treatment |
| Intervention/exposure | Fixed orthodontic treatment |
| Comparison | Before vs after intervention/patients vs controls |
| Outcome | Salivary nickel and/or chromium levels |
| The First Author, Year | Country | Type of Study | Participants (n) | Mean Age/Age Range of Patients, Year | Percentage of Male Patients | Outcome | Follow-Up | Analysis Method | Saliva Sampling |
|---|---|---|---|---|---|---|---|---|---|
| Kerosuo, 1997 [5] | Norway | Cross-sectional | 47 | 12.4/8–30 | 40.4 | Salivary nickel & chromium | 1 day, 1 week, 1 month, | Atomic absorption spectrophotometry | NA/stimulated |
| Ağaoğlu, 2001 [13] | Turkey | Cross-sectional | 100 | 19.5/12–33 | 33 | Salivary nickel & chromium | 1 week, 1 month, 12 months, 24 months | Atomic absorption spectrophotometry | Fasting/unstimulated |
| Matos de Souza, 2008 [11] | Brazil | Cross-sectional | 30 | -/20–26 | 26.7 | Salivary nickel & chromium | 10 min and less, 1 day, 1 week, 1 month, 2 months | Atomic absorption thermal electric spectrophotometry | Fasting/NA |
| Singh, 2008 [22] | India | Cross-sectional | 10 | 17.5/14–24 | 30 | Salivary nickel & chromium | 1 week, 3 weeks, | Atomic absorption thermal electricspectrophotometer | NA/stimulated |
| Petoumenou, 2009 [4] | Greece | Cross-sectional | 18 | 14.9/12–18.1 | 44.5 | Salivary nickel | Up to 8 weeks after the placement of the wires | Atomic absorption spectrometry | Nonfasting/unstimulated |
| Sahoo, 2011 [10] | India | Cross-sectional | 20 | 21.5/18–25 | 0 | Salivary nickel & chromium | 1 day, 1 week, 1 month | Atomic absorption spectrometry | NA/unstimulated |
| Amini, 2012 [24] | Iran | Prospective cohort | 20 | 16/14–23 | 40 | Salivary nickel & chromium | 6 months, 12 months | Atomic absorption spectrophotometry | Fasting /unstimulated |
| *Amini, 2012 [26] | Iran | Case-control | 28 vs. 28 | 17.5/16–19 vs. 18.2/14–22 | 42.8 vs. 42.8 | Salivary nickel & chromium | 12–18 months | Atomic absorption spectrophotometry | NA/NA |
| Ousehal, 2012 [6] | Morocco | Cross-sectional | 16 | ~19.1/13–25 | 50 | Salivary nickel | 10 min and less, 2 months | Inductively coupled plasma–mass spectrometry | NA/unstimulated |
| * Talic, 2013 [15] | Saudi Arabia | Case-control (cross-sectional) | 39 vs. 50 | 18.1 vs. 22 | 41 vs. 48 | Salivary nickel & chromium | 1–32 months | Inductively coupled plasma–mass spectrometry | NA/unstimulated |
| Yassaei, 2013 [25] | Iran | Cohort | 32 | ~15.3/11–24 | NA | Salivary nickel & chromium | 3 weeks, 3 months, 6 months | Atomic absorption spectrometry | NA/unstimulated |
| Nayak, 2015 [2] | India | Cross-sectional | 30 | -/10–25 | 50 | Salivary nickel & chromium | 10 min and less, 12 months | Inductively coupled plasma–mass spectrometry | NA/NA |
| Kumar, 2016 [23] | India | Cross-sectional | 10 | NA/14–23 | 50 | Salivary nickel & chromium | 10 days, 1 month | Inductively coupled plasma–optical emission spectrometry | NA/NA |
| Gölz, 2016 [1] | Germany | Prospective cohort | 30 | -/10–13 | NA | Salivary nickel | Up to 8 weeks after the placement of the wires | Inductively coupled plasma–mass spectrometry | Nonfasting/unstimulated |
| First Author, Publication Year | Selection | Comparability | Outcome | Total Score |
|---|---|---|---|---|
| Kerosuo, 1997 [5] | 4 | 1 | 3 | 8 |
| Ağaoğlu, 2001 [13] | 4 | 2 | 3 | 9 |
| Matos de Souza, 2008 [11] | 3 | 1 | 3 | 7 |
| Singh, 2008 [22] | 3 | 1 | 3 | 7 |
| Petoumenou, 2009 [4] | 4 | 2 | 3 | 9 |
| Sahoo, 2011 [10] | 3 | 2 | 3 | 8 |
| Ousehal, 201 [6] | 3 | 2 | 3 | 8 |
| Nayak, 2015 [2] | 3 | 0 | 3 | 6 |
| Kumar, 2016 [23] | 3 | 2 | 3 | 8 |
| Mean score (cross-sectional studies) | 7.78 | |||
| Amini, 2012 [24] | 2 | 2 | 3 | 7 |
| Yassaei, 2013 [25] | 2 | 2 | 3 | 7 |
| Gölz, 2016 [1] | 2 | 2 | 2 | 6 |
| Mean score (cohort studies) | 6.67 | |||
| Amini, 2012 [26] | 4 | 2 | 2 | 8 |
| Talic, 2013 [15] | 3 | 2 | 2 | 7 |
| Mean score (case-control studies) | 7.50 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imani, M.M.; Mozaffari, H.R.; Ramezani, M.; Sadeghi, M. Effect of Fixed Orthodontic Treatment on Salivary Nickel and Chromium Levels: A Systematic Review and Meta-Analysis of Observational Studies. Dent. J. 2019, 7, 21. https://doi.org/10.3390/dj7010021
Imani MM, Mozaffari HR, Ramezani M, Sadeghi M. Effect of Fixed Orthodontic Treatment on Salivary Nickel and Chromium Levels: A Systematic Review and Meta-Analysis of Observational Studies. Dentistry Journal. 2019; 7(1):21. https://doi.org/10.3390/dj7010021
Chicago/Turabian StyleImani, Mohammad Moslem, Hamid Reza Mozaffari, Mazaher Ramezani, and Masoud Sadeghi. 2019. "Effect of Fixed Orthodontic Treatment on Salivary Nickel and Chromium Levels: A Systematic Review and Meta-Analysis of Observational Studies" Dentistry Journal 7, no. 1: 21. https://doi.org/10.3390/dj7010021