
Marginal Vertical Fit along the Implant-Abutment Interface: A Microscope Qualitative Analysis


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
- -
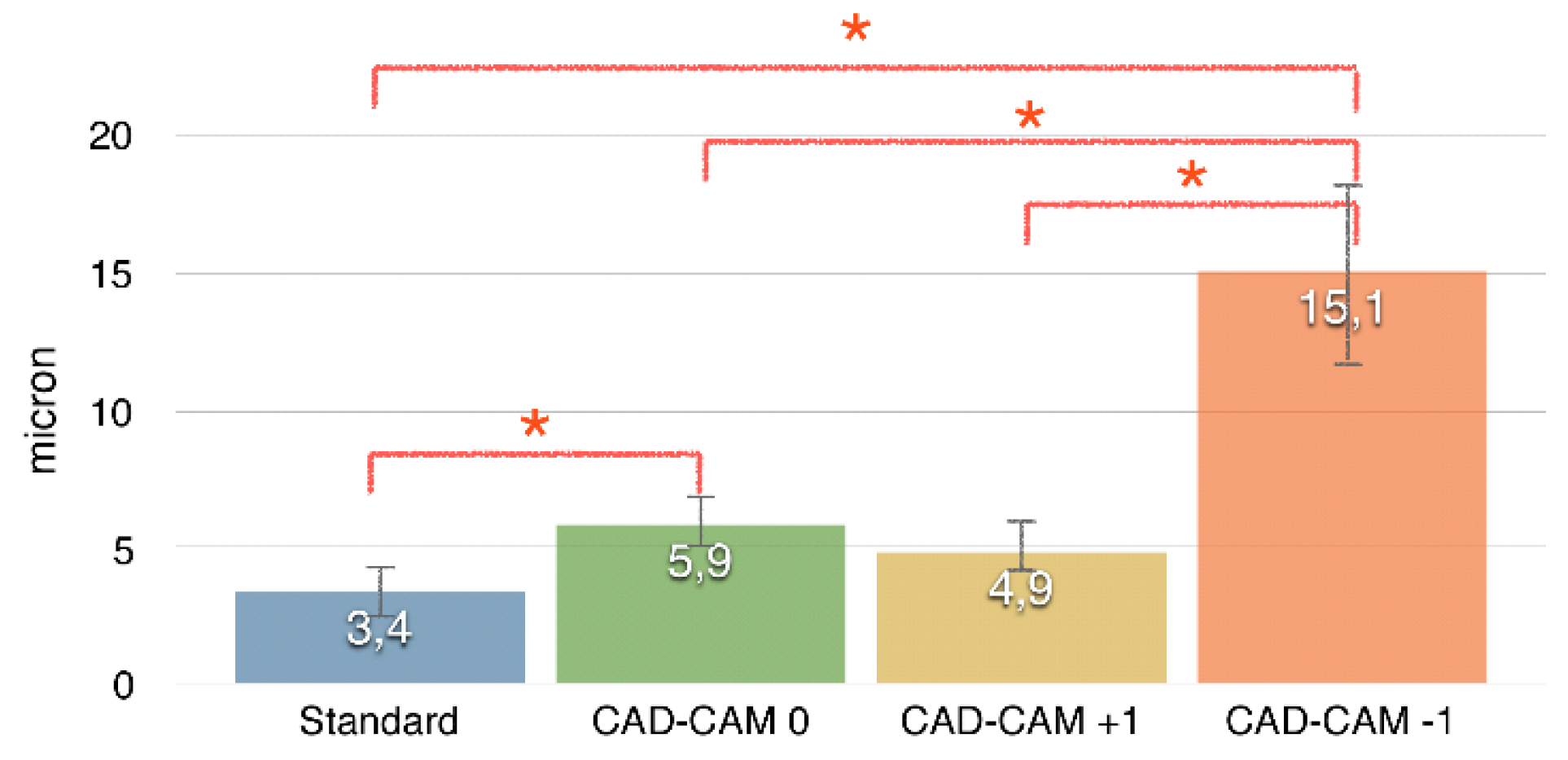
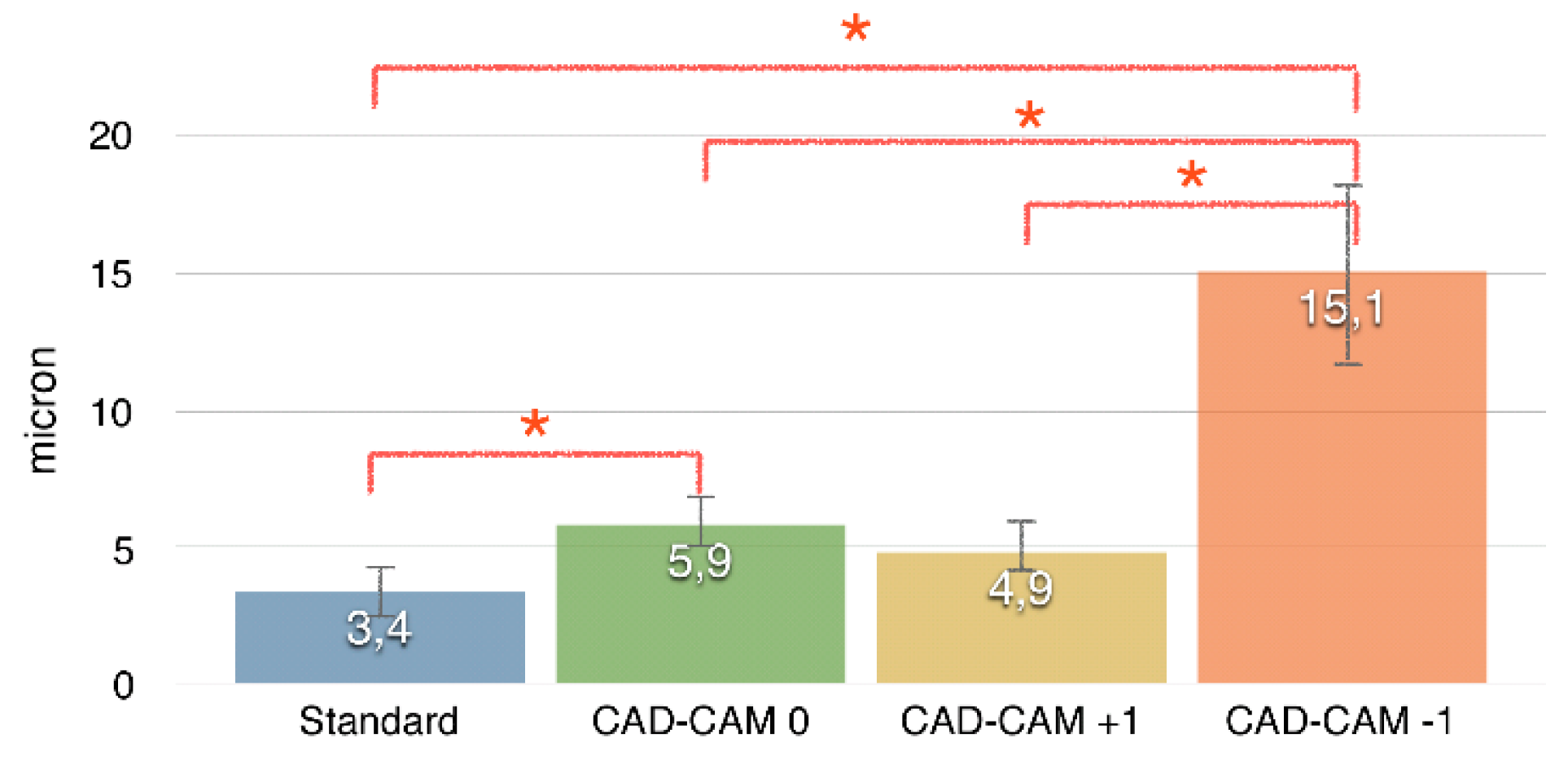
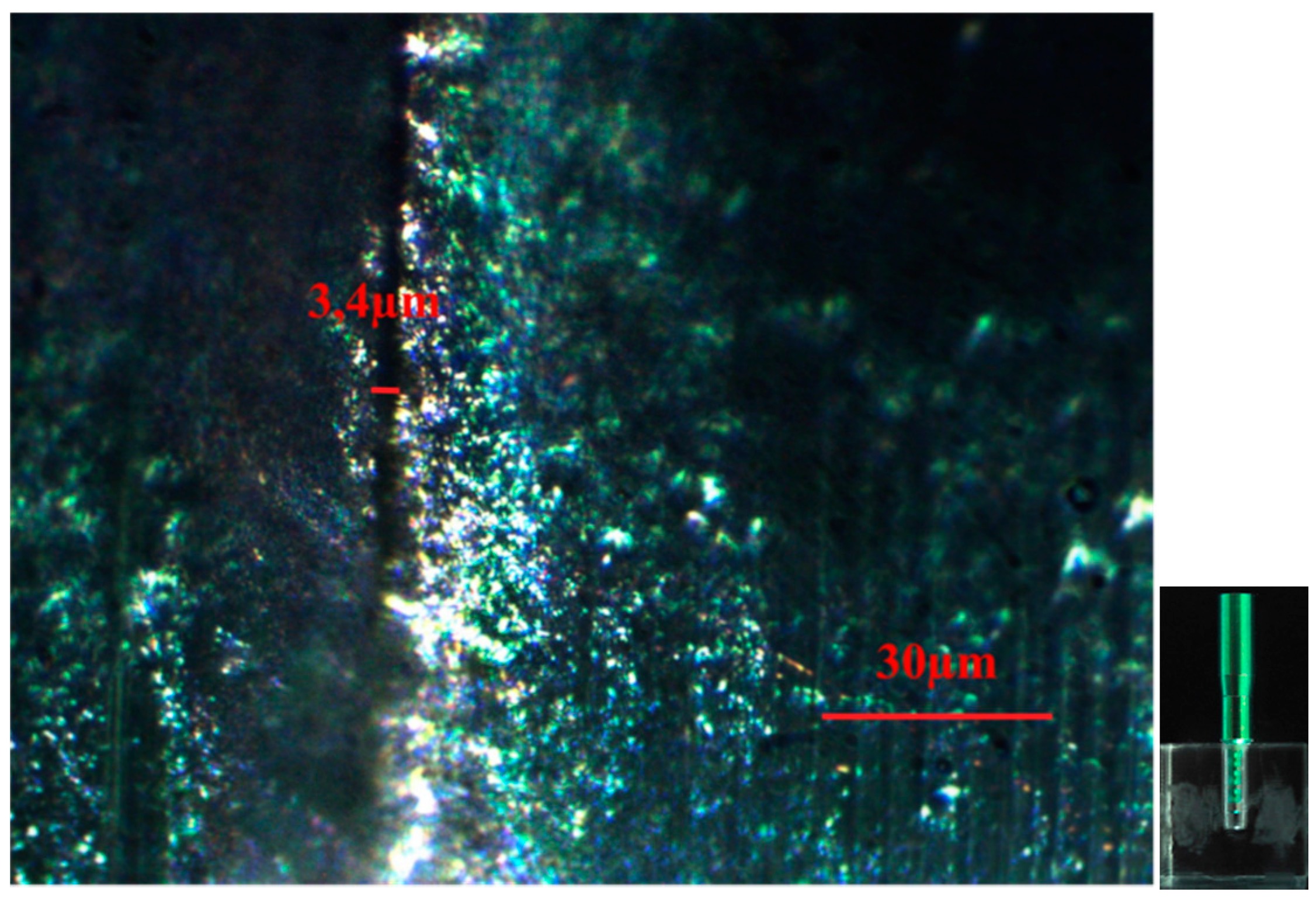
- CAD-CAM 0: tolerance value equal to that declared by manufacturer;
- -
- CAD-CAM +1: augmented tolerance (+10 micron);
- -
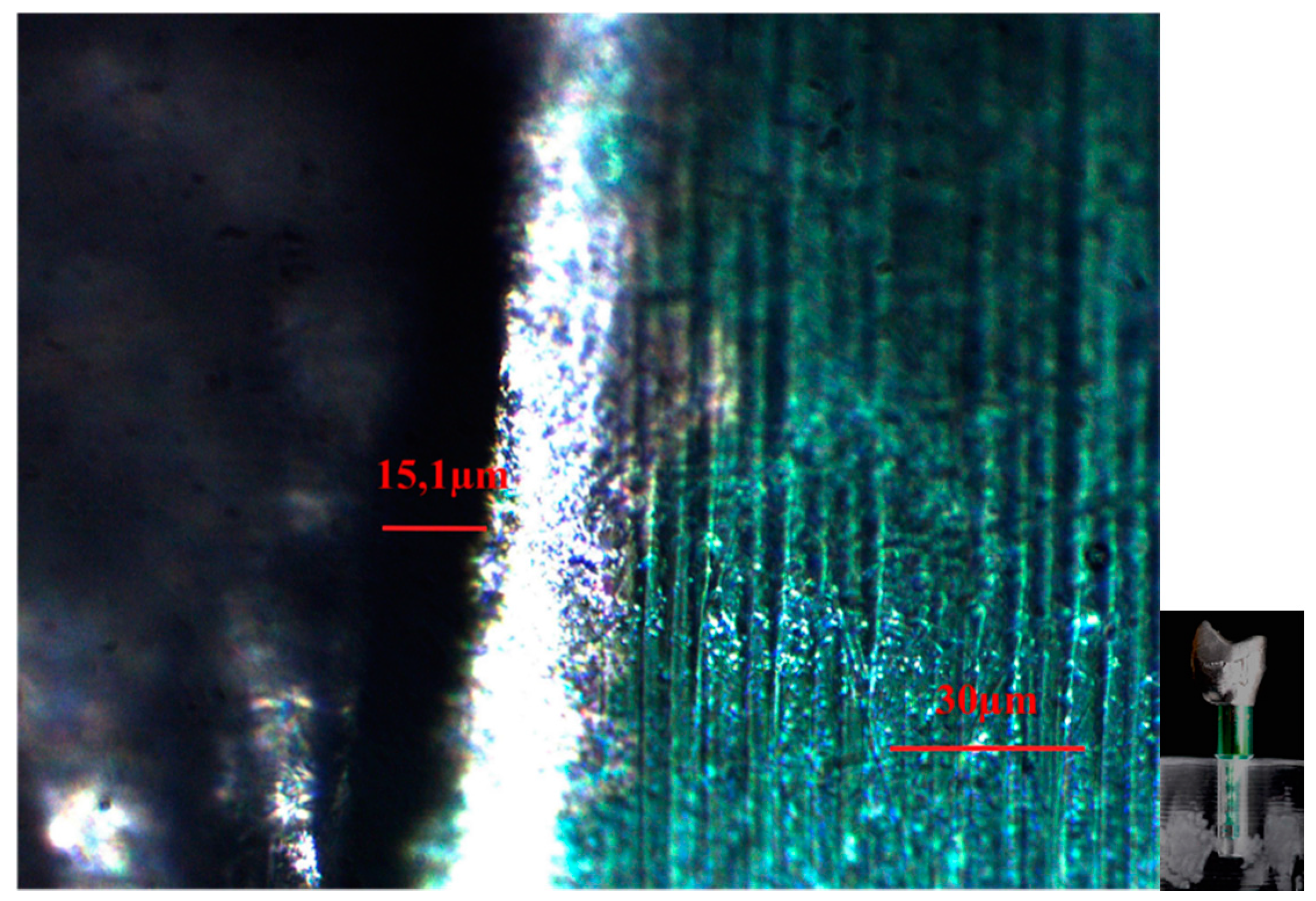
- CAD-CAM −1: reduced tolerance (−10 micron).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Kim, E.S.; Shin, S.Y. Influence of the implant abutment types and the dynamic loading on initial screw loosening. J. Adv. Prosthodont. 2013, 5, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Shafie, H.R. Clinical and Laboratory Manual of Dental Implant Abutments; Wiley-Blackwell: Oxford, UK, 2014. [Google Scholar]
- Kapos, T.; Evans, C. CAD/CAM technology for implant abutments, crowns, and superstructures. Int. J. Oral Maxillofac. Implants 2014, 29, 117–136. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.K.; Rungcharassaeng, K.; Bohsali, K.; Goodacre, C.J.; Lang, B.R. Clinical methods for evaluating implant framework fit. J. Prosthet. Dent. 1999, 81, 7–13. [Google Scholar] [CrossRef]
- Jemt, T.; Rubenstein, J.E.; Carlsson, L.; Lang, B.R. Measuring fit at the implant prosthodontic interface. J. Prosthet. Dent. 1996, 75, 314–325. [Google Scholar] [CrossRef]
- Wee, A.G.; Aquilino, S.A.; Schneider, R.L. Strategies to achieve fit in implant prosthodontics: A review of the literature. Int. J. Prosthodont. 1999, 12, 167–178. [Google Scholar] [PubMed]
- Sailer, I.; Philipp, A.; Zembic, A.; Pjetursson, B.E.; Hämmerle, C.H.; Zwahlen, M. A systematic review of the performance of ceramic and metal implant abutments supporting fixed implant reconstructions. Clin. Oral Implants Res. 2009, 20, 4–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodacre, C.J.; Kan, J.Y.; Rungcharassaeng, K. Clinical complication of osseointegrated implants. J. Prosthet. Dent. 1999, 81, 537–552. [Google Scholar] [CrossRef]
- Winkler, S.; Ring, K.; Ring, J.D.; Boberick, K.G. Implant screw mechanics and the settling effect: An overview. J. Oral Implantol. 2003, 29, 242–245. [Google Scholar] [CrossRef]
- Kim, S.K.; Koal, J.Y.; Heo, S.J.; Taylor, T.D.; Ryoo, S.; Lee, S.Y. Screw loosening with interchangeable abutments in internally connected implants after cyclic loading. Int. J. Oral Maxillofac. Implants 2012, 27, 42–47. [Google Scholar] [PubMed]
- Park, K.K.; Choi, J.U.; Jeon, Y.C.; Choi, K.S.; Jeong, C.M. Effects of retaining prothetic screw coating on implant preload. J. Prosthodont. 2010, 19, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Jorge, J.R.P.; Bravo, V.A.R.; Delben, J.A.; Assuncao, W.G. The role of Implant/Abutment system on torque maintenance of retention screw and vertical misfit of implant-supported crowns before and after mechanical cycling. Int. J. Oral Maxillofac. Implants 2013, 28, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Rimondini, L.; Cerroni, L.; Carrassi, A.; Torricelli, P. Bacterial colonization of zirconia ceramic surfaces: An in vitro and an in vivo study. Int. J. Oral Maxillofac. Implants 2002, 17, 793–798. [Google Scholar] [PubMed]
- Koutouzis, T.; Mesia, R.; Calderon, N.; Wong, F.; Wallet, S. The effect of dinamic loading on bacterial colonization of the dental implant fixture-abutment interface: An in vitro study. J. Oral Implantol. 2014, 40, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Binon, P.P.; McHugh, M.J. The effect of elimanating implant/abutment rotational misfit on screw joint stability. Int. J. Prosthodont. 1996, 9, 511–519. [Google Scholar] [PubMed]
- Hill, E.E.; Phillips, S.M.; Breeding, L.C. Implant abutment screw torque generated by general dentists using a hand driver in limited access space simulating the mouth. J. Oral Implantol. 2007, 33, 277–279. [Google Scholar] [CrossRef]

© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mobilio, N.; Fasiol, A.; Franceschetti, G.; Catapano, S. Marginal Vertical Fit along the Implant-Abutment Interface: A Microscope Qualitative Analysis. Dent. J. 2016, 4, 31. https://doi.org/10.3390/dj4030031
Mobilio N, Fasiol A, Franceschetti G, Catapano S. Marginal Vertical Fit along the Implant-Abutment Interface: A Microscope Qualitative Analysis. Dentistry Journal. 2016; 4(3):31. https://doi.org/10.3390/dj4030031
Chicago/Turabian StyleMobilio, Nicola, Alberto Fasiol, Giulio Franceschetti, and Santo Catapano. 2016. "Marginal Vertical Fit along the Implant-Abutment Interface: A Microscope Qualitative Analysis" Dentistry Journal 4, no. 3: 31. https://doi.org/10.3390/dj4030031