
Novel Technique to Reconstruct Peri-Implant Keratinised Mucosa Width Using Xenogeneic Dermal Matrix. Clinical Case Series

1
Department of Periodontology, Semmelweis University, 1088 Budapest, Hungary
2
Evident Pro Private Practice, 1118 Budapest, Hungary
*
Author to whom correspondence should be addressed.
Dent. J. 2024, 12(3), 43; https://doi.org/10.3390/dj12030043
Submission received: 4 December 2023
/
Revised: 29 January 2024
/
Accepted: 5 February 2024
/
Published: 20 February 2024
(This article belongs to the Special Issue Management of Peri-Implantitis II)
Abstract
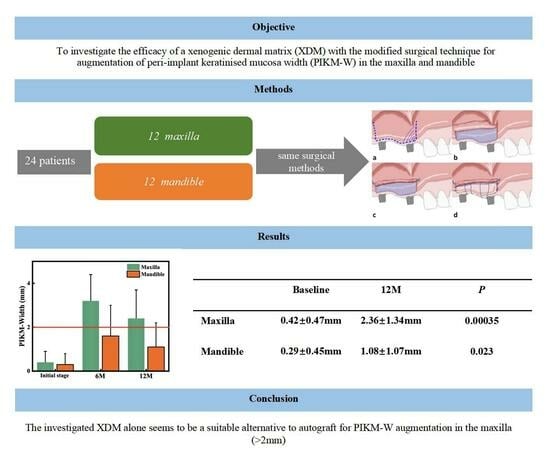
:Reconstruction of sufficient buccal peri-implant keratinised mucosa width (PIKM-W) is reported to reduce the symptoms of peri-implantitis. In order to reduce the drawbacks of autogenous graft harvesting, we investigated a novel porcine dermal matrix (XDM, mucoderm®) using a modified surgical technique for augmentation of PIKM-W. Twenty-four patients were recruited with insufficient (<2 mm) PIKM-W. After split thickness flap preparation, the XDM was trimmed, rehydrated and tightly attached to the recipient periosteal bed using modified internal/external horizontal periosteal mattress sutures via secondary wound healing. Change of the PIKM-W and dimension of the graft remodelling were evaluated at 6 and 12 months postoperatively. The mean PIKM-W changed from 0.42 ± 0.47 to 3.17 ± 1.21 mm at 6 M and to 2.36 ± 1.34 mm at 12 M in the maxilla and from 0.29 ± 0.45 mm to 1.58 ± 1.44 mm at 6 M and to 1.08 ± 1.07 mm at 12 M in the mandible. Graft dimensions decreased by 67.7 ± 11.8% and 81.6 ± 16.6% at 6 M, and continued to 75.9 ± 13.9% and 87.4 ± 12.3% at 12 M, in the maxilla and mandible, respectively. Clinical parameters showed statistically significant intra- and intergroup differences between the baseline and 6 and 12 months (p < 0.05). The present technique using the XDM was safe and successfully reconstructed PIKM-W in both arches. The XDM alone seems to be a suitable alternative to autograft for PIKM-W augmentation in the maxilla.
1. Introduction and Background
The increased use of dental implants in replacing missing teeth is today associated with several challenges. The most common concerns are peri-implant mucositis (prevalence between 19 and 65%) and peri-implantitis (frequency in the range of 1–47%) [1,2,3,4,5]. The aetiology behind peri-implantitis seems to be multifactorial. The most common causative factors are considered to be poor plaque control, history of periodontitis, smoking, diabetes, lack of maintenance visits, lack of sufficient bone volume, iatrogenic factors (e.g., improper patient/implant selection, suboptimal surgical procedure, malpositioning, overheating, over-torque, overloading, excess luting cement), and, last but not least, lack of sufficient vestibulum depth and width of the attached keratinised mucosa [5,6,7]. Wennström (1994) showed that there were no significant differences in the maintenance of peri-implant health in sites with and without an adequate width of keratinised mucosa [8]. However, later, Romanos and co-workers indicated that the presence of an adequate width of PIKM might result in less plaque accumulation, less recession, improved soft and hard tissue stability and a lower incidence of peri-implant mucositis [9]. Roccuzzo et al. demonstrated that when the buccal peri-implant keratinised mucosa width (PIKM-W) was less than 2 mm, the implants were more prone to plaque accumulation as well as gingival recession, even in patients exercising sufficient oral hygiene and undergoing professional periodontal therapy [10]. Furthermore, in the absence of PIKM, increased plaque score, recession and bone loss could be detected [11,12]. In a recent study conducted by Gharpure et al., it was shown that implants with PIKM-W measuring less than 2 mm exhibited a significantly greater prevalence of peri-implantitis (prevalence ratio [PR] = 1.87), peri-implant mucositis (PR = 1.53) and pain or discomfort experienced while tooth brushing (PR = 2.37) compared to implants with appropriate PIKM-W [11]. Previous studies have shown that a decrease in PIKM-W is linked to a development in the formation of biofilm, inflammation of the soft tissue, heightened patient discomfort, recession of the mucosal tissue, loss of marginal bone and a higher occurrence of peri-implantitis [13]. Moreover, it was determined that there exists a favourable correlation between a PIKM-W greater than 2 mm and the general condition of the peri-implant complex [14].
In order to overcome the above complications, surgical enhancement of PIKM was suggested with autogenous or xenogeneic soft-tissue grafts. Previous papers have provided insufficient reliable evidence to provide recommendations on whether the techniques to broaden the PIKM or attached mucosa are beneficial to patients or not [15]. However, the recent literature has indicated that soft-tissue grafting treatments have been associated with improved peri-implant health outcomes. (i) In the reconstruction of the keratinised mucosa, autogenous grafts have been found to be effective in improving bleeding indices and promoting higher levels of marginal bone. (ii) Autogenous grafts have been shown to be a suitable method for increasing the mucosal thickness, resulting in much-reduced marginal bone loss [1]. Finally, free autogenous gingival grafts are considered the surgical standard to increase PIKM-W effectively. However, xenografts may be successful alternatives, since similar results were reported compared to autografts [13].
Free gingival graft, or, more accurately described, epithelialised connective tissue graft (ECTG), represents the gold standard as it results in minimal postoperative soft-tissue contraction and maximal predictability [16,17,18,19,20,21]. However, harvesting the ECTG may cause significant pain and discomfort at the donor sites (hard palate, maxillary tuberosity). Furthermore, the available amount of tissue is limited, and a colour match at the recipient site might be compromised [17,18,22,23].
To overcome the limitations of ECTG, authors have suggested using a xenogeneic collagen matrix (XCM) to enhance the PIKM-W. The existing literature shows that the XCM results in satisfactory outcomes in increasing the width of keratinised mucosa. However, the XCM undergoes significant contraction (resorption) due to its porous surface, resulting in far lower PIKM-W during secondary wound healing than is the case with ECTG [24,25]. As an alternative, a recently developed xenogeneic dermal matrix (XDM, mucoderm®) of porcine origin can be utilised, as this material undergoes less contraction, presents a quick rehydration time and slow resorption, facilitates angiogenesis and attracts fibroblast and osteoblast [26,27,28]. In order to test the potential effective graft materials for increasing PIKM-W, we conducted a pilot study including ECTG, sub-epithelial connective tissue graft (SCTG), allogenic dermal matrix (ADM), XCM and XDM. Six months postoperatively, the ECTG (3.5 ± 1.5 mm) and XDM (3.0 ± 1.6 mm) had created >2 mm PIKM-W compared to the SCTG (1.0 ± 0.0 mm), ADM (2.1 ± 1.0 mm) and XCM (1.5 ± 2.1 mm), respectively [29].
Therefore, the present prospective case series aimed to evaluate the efficacy of the novel XDM to widen the band of the buccal keratinised mucosa at 6- and 12-month observation periods by comparing the upper and lower jaws. In addition, we aimed to provide a detailed description of the surgical procedures we developed. According to the best of our knowledge, no study has investigated the above parameters.
Null Hypothesis 1:
The use of this XDM with a modified surgical technique does not significantly widen the PIKM in the maxilla and mandible compared to baseline measurements.
Null Hypothesis 2:
There is no significant difference in PIKM-W augmentation using the present technique and material between the maxilla and mandible.
2. Materials and Methods
2.1. Study Design
This prospective case series study examined the clinical outcomes of 24 patients who presented insufficient (<2 mm) width of PIKM in the maxilla and the mandible. Subjects were selected and treated at the Department of Periodontology, Semmelweis University, Budapest, Hungary, between 2018 and 2020. Participants signed a written informed consent statement prior to treatment. The local ethics committee, Semmelweis University Regional and Institutional Committee of Science and Research Ethics, approved the study protocol (approval number: SE RKEB 223/2017). The study was conducted in full accordance with the Declaration of Helsinki, as revised in 2013 [30].
2.2. Eligibility Criteria
The inclusion criteria were the following:
- Men and women older than 18 years of age;
- Good compliance to adhere to follow-up protocol and a willingness to commit to a long-term maintenance program after treatment;
- Good oral hygiene (full mouth plaque score, FMPS < 20%);
- PIKM-W either absent or less than 2 mm, measured with a UNC 15 periodontal probe;
- Planned implant placement in the area of keratinised soft-tissue augmentation.
The major exclusion criteria were the following:
- Contributing medical history in which any elective oral surgical intervention would be contraindicated;
- Smoking;
- Pregnant or lactating women;
- Presence of uncontrolled or untreated periodontal disease (full mouth bleeding score > 20%).
2.3. Presurgical Treatment
The patients underwent professional oral hygiene instruction and full-mouth supragingival scaling, and 2–400 mg ibuprofen was given as NSAID.
2.4. Surgical Treatment
Following local anaesthesia, a horizontal incision was performed at the mucogingival junction (MGJ) using a 15C blade, paying attention not to cut through the periosteum. At the mesial and distal aspects of the initial incision, two vertical releasing incisions were carried out in the mobile mucosa. A split-thickness flap was then gently reflected by the blade or periosteal elevator to prepare a recipient periosteal bed for the graft material based on individual anatomical need. The dimension of the recipient bed was designed to correspond to the planned implant site.
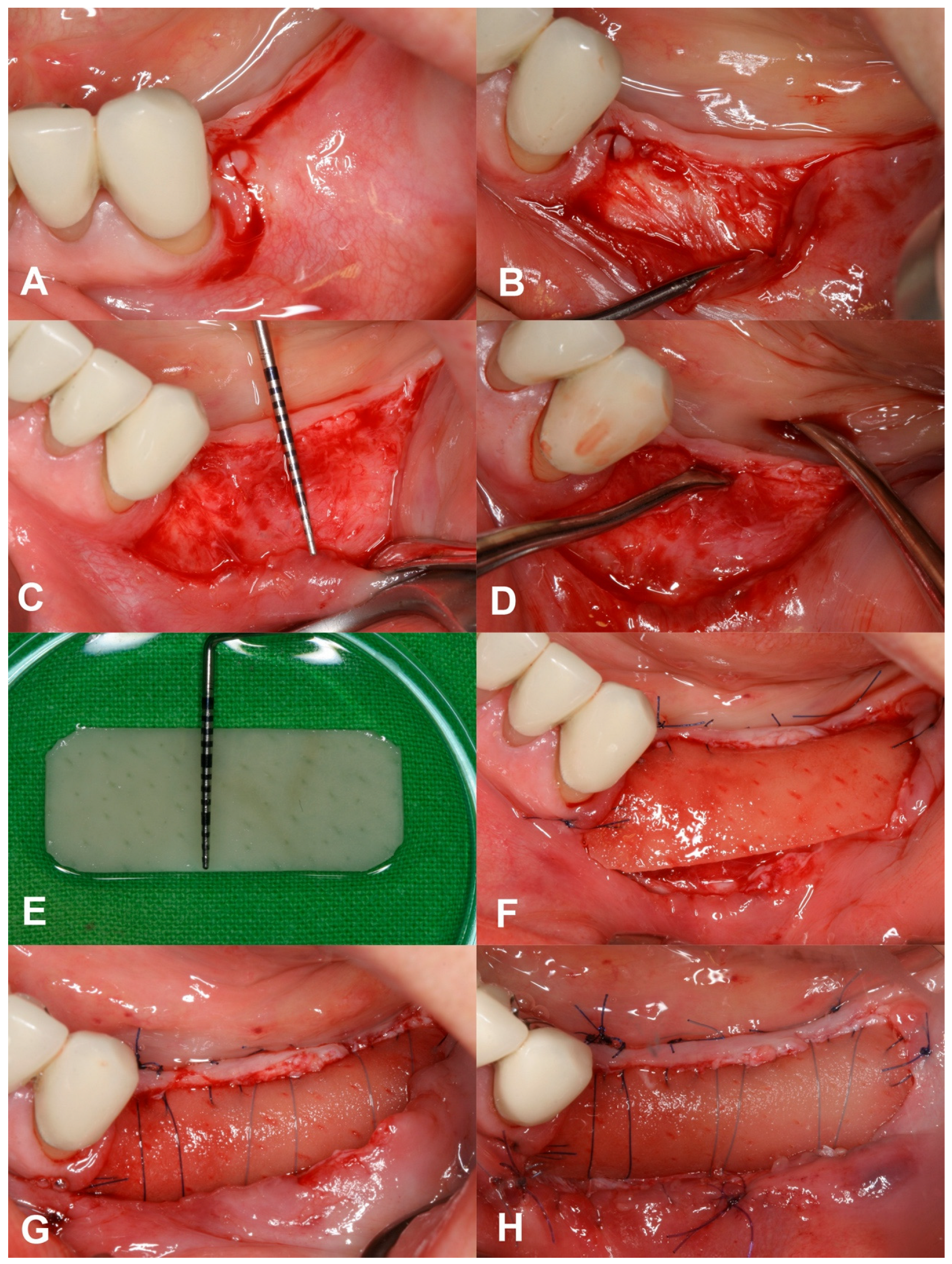
The XDM (mucoderm®, Botiss, Zossen, Germany) was trimmed according to the size of the prepared recipient bed (mean width: 9.75 ± 0.62 mm and 8.58 ± 1.16 mm in the maxilla and mandible, respectively) and fully rehydrated with a sterile saline solution. At the coronal part of the recipient bed, the rim of the keratinised mucosa was slightly elevated in order to insert the coronal edge of the XDM underneath. The mesio, mid, and distal coronal parts of the graft were then fixed to/under the attached mucosa via internal (mucosa)/external (graft) horizontal mattress suturing using 5-0 non-resorbable monofilament sutures (Dafilon®, B. Braun, Rubí, Spain). After that, deep periosteal internal horizontal mattress sutures were placed above the graft material to compress the XDM to the periosteal bed, making tight contact and avoiding blood clot formation between the recipient site and the XDM. The rim of the mucosal flap was sutured to the apical portion of the same flap via a simple continuous suturing technique using a 6-0 monofilament absorbable suture (Monolac, Chirmax, Prague, Czech Republic), thereby deepening the oral vestibulum as well (Figure 1). The sutures were removed after 14 days. Surgeries were carried out by a periodontal specialist (A.H.).
2.5. Postsurgical Instructions and Infection Control
The patients were instructed to avoid mechanical cleaning in the surgical area for two weeks. Instead, chemical plaque control was prescribed with 0.12% chlorhexidine + 0.05% Cetylpyridinium chloride mouth rinse (Paroex, GUM Sunstar, Etoy, Switzerland). The patients were prescribed 250 mg of amoxicillin + clavulanic acid 125 mg (Augmentin 375, GlaxoSmithKline, Brentford, UK) thrice daily for one week. Per individual need, postoperative pain was controlled with diclofenac 50 mg (Cataflam 50, Novartis, Basel, Switzerland).
The patients were recalled 1 and 2 weeks and 6 and 12 months after surgery for suture removal, plaque control and healing evaluation. Implants were inserted between the 6- and 12-month visits according to individual needs.
2.6. Outcome Variables
The primary outcome of the study was to evaluate the overall change in the buccal PIKM-W between baseline and the 6- and 12-month follow-up. PIKM-W was measured as the distance in mm between the mid-crestal line of the edentulous ridge or the mid-buccal margin of the implant and the MGJ using a UNC 15 periodontal probe, rounded to the nearest mm, at baseline and at 6 and 12 months postoperatively. In addition, we compared the possible outcome differences between the maxilla and the mandible. The secondary outcome was to evaluate the dimension of remodelling (shrinkage, contraction) of the XDM using the following formula: (1 − ((PIKM-W at 6 M in mm − PIKM-W baseline in mm)/trimmed XDM width in mm)) × 100 = …%. Measurements were performed by a single calibrated examiner periodontist (X.L.).
2.7. Statistical Analysis
We performed a patient-based analysis. In the case of multiple sites per patient, one mean value was calculated and utilised in the research. Descriptive statistics were calculated (mean, range and standard deviation) for each study variable. The statistical significance between each group was calculated using Student’s t-test (p-value < 0.05). The mean values of the PIKM-W were calculated at each examination time point to facilitate intragroup comparison using a paired t-test. An intergroup analysis was conducted using an unpaired t-test to compare the upper and lower jaw. The statistical analysis was performed in SPSS Statistics V26 (IBM, Armonk, NY, USA).
3. Results
3.1. Patient Demographics
A total of 24 patients (8 men and 16 women with a mean age of 56.88 ± 12.29 years; range: 33–75 years) were enrolled, with equal distribution in the maxilla and the mandible (Table 1).
3.2. Primary Outcome: Changes in PIKM-W
Intragroup measurements of the change in the PIKM-W were performed separately in both the maxilla and the mandible (Table 2 and Table 3). The mean PIKM-W changed from 0.42 ± 0.47 mm to 3.17 ± 1.21 mm (2.75 ± 0.53 mm difference, p < 0.001) at the 6-month follow-up and to 2.36 ± 1.34 mm (1.94 ± 0.62 mm difference, p < 0.001) at the 12-month follow-up in the 12 maxillary sites (Figure 2).
3.3. Secondary Outcome: Dimension of Graft Remodelling
The decrease in the width of the graft at the 6-month evaluation equalled 67.7 ± 11.8% in the maxilla and 81.6 ± 16.6% in the mandible, and this continued to 75.9 ± 13.9% and 87.4 ± 12.3% at 12 months in the maxilla and mandible, respectively. A statistically significant intergroup difference was detected between the maxilla and mandible at 6 as well as 12 months (p < 0.05).
4. Discussion
The present study demonstrated a safe and uneventful postoperative period of the investigated technique and material for increasing PIKM-W. In addition, despite the marked graft remodelling, a statistically significant and clinically sufficient (>2 mm) amount of new keratinised mucosa was achieved in the maxilla. Although the widening of the PIKM was also significant in the mandibular sites, the desired minimum width was reached with varying success.
In order to reconstruct the desirable minimum amount of 2 mm of PIKM-W, ECTG (FGG) is widely regarded as the most effective method due to its ability to minimise soft-tissue contraction after surgery and provide the highest level of predictability [13,16,17,18,19,21]. A study by Schmitt et al. reported that ECTG-augmented PIKM-W remained 8.4 mm after a 5-year follow-up [31]. The systematic review by Thoma et al. reported that an apically positioned flap (APF) combined with ECTG resulted in an excellent improvement in peri-implant health [1]. A similar conclusion was drawn by Vignoletti et al., who found that the mean PIKM-W increased by 4.5 mm using the augmentation procedure of APF plus autograft [32]. Nevertheless, harvesting the ECTG has the potential to induce substantial pain and excessive bleeding, and it compromised healing at the donor sites. In addition, it is essential to note that there is a restricted supply of tissue, and achieving a precise colour match at the recipient location is suboptimal, as indicated by previous studies [17,18,22,23].
In order to address the constraints of ECTG, researchers have proposed using a xenogeneic collagen matrix (XCM) to enhance the potential growth in peri-implant keratinised mucosa width (PIKM-W). Sanz et al. reported a mean increase of 2.5 mm in the keratinised mucosa width using XCM (Mucograft®, Geistlich Pharma AG, Wolhusen, Switzerland) [24,26,27]. Their study documented a shrinkage rate of 67% [24]. Another study, by Lorenzo et al., reported that PIKM-W augmentation procedures using XCM (Mucograft®) and connective tissue graft achieved a mean value of 2.75 mm and 2.8 mm, respectively [25]. However, both investigations were discontinued at 6 months. The literature indicates that XCM has yielded favourable outcomes in augmenting the width of keratinised mucosa. Nevertheless, XCM is subjected to swift resorption/remodelling due to its porous surface and loose structure. This leads to a significantly lower amount of keratinised tissue during open healing than is the case with ECTG [31].
A novel xenogeneic dermal matrix of porcine origin composed of I/III type collagen (XDM, mucoderm®) has been recently introduced as a potential substitution for autograft in periodontology and implant dentistry.
According to a study by Pabst et al., this material showed excellent tissue integration and rapid revascularisation [33]. Park et al. explored the cell proliferation characteristics of mucoderm®. Host cell migration and penetration in this matrix were complemented by its interconnected structure, which allowed microvessel formation and neo-angiogenesis [34]. Some studies have investigated the immune response of this XDM and revealed that its natural 3D matrix scaffold structure prolongs the degradation period and improves its mechanical properties, which is an additional advantage when slow resorption and keratinisation are targets during “open”, secondary wound healing [32,35].
In a recent retrospective investigation, Zafiropoulos et al. utilised XDM to increase the PIKM-W, and a 5.4 mm mean growth was reported after the 6-month follow-up [28]. Two-thirds of the sites were located in the maxilla. Nevertheless, the same amount of shrinkage was reported in both arches at all site locations (3.9 ± 1.2 mm vs. 3.9 ± 1.1 mm and 3.9 ± 1.3 mm vs. 3.9 ± 1.1 mm in the maxilla vs. mandible and anterior vs. posterior sites, respectively).
Our data revealed a smaller decrease in graft width in the maxilla (67.7 ± 11.8%) in contrast to the mandible (81.6 ± 16.6%) and also revealed statistically significant differences between the two jaws in PIKM-W change and in the magnitude of graft remodelling at 6- (p = 0.008; p = 0.03) and 12-month (p = 0.02; p = 0.04) intervals. The reason for these results may originate in the anatomic differences, since the mandibular sites present with a shallower vestibule and more coronal adhesion of the more voluminous buccal muscles. Therefore, instead of graft contraction or shrinkage, this may be more likely defined as the coronal migration of the MGJ as a result of undesired but natural soft-tissue remodelling. Nandkeoliar et al. demonstrated that this interarch divergence is around 2 mm in the age group of our subjects (11.28 ± 2.31 in the maxilla and 9.42 ± 2.87 in the mandible) [36]. Based on these differences, the maxillary and mandibular regions should be investigated separately. The cumulative PIKM-W outcomes of both arches in our investigation would have led to different results and conclusions than the separate ones. This should be considered in further study designs; otherwise, it may lead to deceptive outcomes that could potentially impact clinical decision making.
The other strength of the present trial is the 1-year length of the investigation period. Our results indicate that the newly formed PIKM remodelling continues from 6 to 12 months, reaching statistical significance (p = 0.009 maxilla; p = 0.03 mandible). Therefore, a minimum investigation period of 12 months should be considered when seeking long-term tissue stability.
According to the authors’ knowledge, this prospective case series investigation is the only study to test this novel XDM in peri-implant soft-tissue augmentation in the maxilla and mandible, with 12 months of follow-up. When comparing the results of this study to other investigations, it needs to be highlighted that not only the material but also the surgical technique could play a crucial role. Based on our previous pilot aiming at fast revascularisation and prevention of graft detachment, it is essential to attain tight contact between the XDM and the periosteal bed. A commonly used surgical technique anchors the graft to the adjacent flaps with single interrupted sutures. Due to a lack of immobility and insufficient connection between the graft and the periosteum, this technique may create blood clot formation in between and, thereby, cause graft disintegration. This, and the insufficient apical locking of the mobile mucosa, may lead to considerable remodelling of the graft and coronal remigration of the mobile non-keratinised mucosa.
The newly formed tissue should not only be keratinised but also attached to the mucosa. To reach this goal, we applied modified internal/external horizontal deep periosteal mattress sutures to stabilise the graft to the periosteum and fixed epithelium only and avoided apical/lateral sutures to the mobile mucosa. Furthermore, the coronal edges of the graft were inserted under the keratinised epithelium. In order to keep the split-thickness mucosal flap edge as apical as possible, the coronal rim of the flap was folded to the most apical part of the same flap in such a way that its non-keratinised epithelium adhered to the periosteum and fixed with simple continuous sutures. We aimed to disclose a step-by-step description of our surgical procedure in this manuscript.
The slightly different measurement landmark at 12 M could be considered a limitation of the study. The reason for this was the “put patients’ benefit first” research initiative, as we believed it would not have been ethically correct to expect patients to wait a whole year to receive their fixtures, when the sites were ready to be implanted. In addition, implants were placed following midcrestal incision; thereby, the PIKM dimensions were not altered but only buccally shifted.
While the study achieved statistical significance in several outcomes, the clinical significance of these findings, particularly in terms of long-term implant survival and patient-centred outcomes, remains to be established. Future studies should focus not only on the statistical analysis of clinical parameters but also on the impact of these changes on implant success rate, patients’ quality of life, oral function, brushing discomfort, aesthetic outcomes, etc.
Due to the continued remodelling after 6 months, 12-month investigations are warranted. In order to draw broader conclusions and provide more predictable solutions in the lower jaw, randomised controlled clinical trials with large sample sizes and with an ECTG control group as gold standard are needed in this field.
5. Conclusions
- The investigated surgical technique using XDM was safe and significantly widened the PIKM in both jaws.
- The new PIKM formation surpassed the clinically desired 2 mm width in the maxilla. The mandibular sites presented with more variable success.
- The remodelling of the newly formed PIKM continued after 6 months.
- The investigated XDM alone could be considered as a suitable alternative to autograft to reconstruct an adequate amount of keratinised mucosa width in the maxilla.
With respect to the nature of a case series, the conclusions of the present study have to be interpreted carefully.
Author Contributions
A.H. performed the clinical treatments and the study design. X.L. searched and analysed the literature, blueprinted the study, performed the statistical analysis and wrote the results and tables. A.H., X.L., D.P. and P.W. contributed to writing and editing the article’s final version. All authors worked on the concept and protocol of this study and in the final review and writing of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
The study did not receive any sponsorship or funding. The graft material was provided by the manufacturer.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Semmelweis University Regional and Institutional Committee of Science and Research Ethics (approval number: SE RKEB 223/2017, approval date: 13 November 2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Thoma, D.S.; Naenni, N.; Figuero, E.; Hämmerle, C.H.F.; Schwarz, F.; Jung, R.E.; Sanz-Sánchez, I. Effects of Soft Tissue Augmentation Procedures on Peri-Implant Health or Disease: A Systematic Review and Meta-Analysis. Clin. Oral Implants Res. 2018, 29 (Suppl. S15), 32–49. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Pjetursson, B.E.; Glauser, R.; Zembic, A.; Zwahlen, M.; Lang, N.P. A Systematic Review of the 5-Year Survival and Complication Rates of Implant-Supported Single Crowns. Clin. Oral Implants Res. 2008, 19, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Effectiveness of Implant Therapy Analyzed in a Swedish Population: Prevalence of Peri-Implantitis. J. Dent. Res. 2016, 95, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Wilson, V. An Insight into Peri-Implantitis: A Systematic Literature Review. Prim. Dent. J. 2013, 2, 69–73. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-Implantitis. J. Clin. Periodontol. 2018, 45, S246–S266. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Almutairi, Z.; Amir-Rad, F.; Koleilat, M.; Tawse-Smith, A.; Ma, S.; Lin, L.; Alsabeeha, N.H.M. A Retrospective Analysis of Biological Complications of Dental Implants. Int. J. Dent. 2022, 2022, 1545748. [Google Scholar] [CrossRef] [PubMed]
- Hämmerle, C.H.F.; Tarnow, D. The Etiology of Hard- and Soft-Tissue Deficiencies at Dental Implants: A Narrative Review. J. Periodontol. 2018, 89 (Suppl. S1), S291–S303. [Google Scholar] [CrossRef]
- Wennström, J.L.; Bengazi, F.; Lekholm, U. The Influence of the Masticatory Mucosa on the Peri-Implant Soft Tissue Condition. Clin. Oral Implants Res. 1994, 5, 1–8. [Google Scholar] [CrossRef]
- Bouri, A.; Bissada, N.; Al-Zahrani, M.S.; Faddoul, F.; Nouneh, I. Width of Keratinized Gingiva and the Health Status of the Supporting Tissues around Dental Implants. Int. J. Oral Maxillofac. Implants 2008, 23, 323–326. [Google Scholar]
- Roccuzzo, M.; Grasso, G.; Dalmasso, P. Keratinized Mucosa around Implants in Partially Edentulous Posterior Mandible: 10-Year Results of a Prospective Comparative Study. Clin. Oral Implants Res. 2016, 27, 491–496. [Google Scholar] [CrossRef]
- Gharpure, A.S.; Latimer, J.M.; Aljofi, F.E.; Kahng, J.H.; Daubert, D.M. Role of Thin Gingival Phenotype and Inadequate Keratinized Mucosa Width (<2 mm) as Risk Indicators for Peri-Implantitis and Peri-Implant Mucositis. J. Periodontol. 2021, 92, 1687–1696. [Google Scholar] [PubMed]
- Kim, B.-S.; Kim, Y.-K.; Yun, P.-Y.; Yi, Y.-J.; Lee, H.-J.; Kim, S.-G.; Son, J.-S. Evaluation of Peri-Implant Tissue Response According to the Presence of Keratinized Mucosa. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, e24–e28. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Schwarz, F.; Herrera, D.; McClain, P.; Figuero, E.; Molina, A.; Monje, A.; Montero, E.; Pascual, A.; Ramanauskaite, A.; et al. Importance of Keratinized Mucosa around Dental Implants: Consensus Report of Group 1 of the DGI/SEPA/Osteology Workshop. Clin. Oral Implants Res. 2022, 33 (Suppl. S23), 47–55. [Google Scholar] [CrossRef]
- Longoni, S.; Tinto, M.; Pacifico, C.; Sartori, M.; Andreano, A. Effect of Peri-Implant Keratinized Tissue Width on Tissue Health and Stability: Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implants 2019, 34, 1307–1317. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Maghaireh, H.; Grusovin, M.G.; Ziounas, I.; Worthington, H.V. Soft Tissue Management for Dental Implants: What Are the Most Effective Techniques? A Cochrane Systematic Review. Eur. J. Oral Implantol. 2012, 5, 221–238. [Google Scholar]
- Wu, Q.; Qu, Y.; Gong, P.; Wang, T.; Gong, T.; Man, Y. Evaluation of the Efficacy of Keratinized Mucosa Augmentation Techniques around Dental Implants: A Systematic Review. J. Prosthet. Dent. 2015, 113, 383–390. [Google Scholar] [CrossRef]
- Seibert, J.S. Reconstruction of Deformed, Partially Edentulous Ridges, Using Full Thickness Onlay Grafts. Part I. Technique and Wound Healing. Compend. Contin. Educ. Dent. 1983, 4, 437–453. [Google Scholar] [PubMed]
- Camargo, P.M.; Melnick, P.R.; Kenney, E.B. The Use of Free Gingival Grafts for Aesthetic Purposes. Periodontology 2000 2001, 27, 72–96. [Google Scholar] [CrossRef]
- Dorfman, H.S.; Kennedy, J.E.; Bird, W.C. Longitudinal Evaluation of Free Autogenous Gingival Grafts. A Four Year Report. J. Periodontol. 1982, 53, 349–352. [Google Scholar] [CrossRef]
- Keceli, H.G.; Sengun, D.; Berberoğlu, A.; Karabulut, E. Use of Platelet Gel with Connective Tissue Grafts for Root Coverage: A Randomized-Controlled Trial. J. Clin. Periodontol. 2008, 35, 255–262. [Google Scholar] [CrossRef]
- Cairo, F.; Pagliaro, U.; Nieri, M. Treatment of Gingival Recession with Coronally Advanced Flap Procedures: A Systematic Review. J. Clin. Periodontol. 2008, 35, 136–162. [Google Scholar] [CrossRef]
- Ioannou, A.L.; Kotsakis, G.A.; McHale, M.G.; Lareau, D.E.; Hinrichs, J.E.; Romanos, G.E. Soft Tissue Surgical Procedures for Optimizing Anterior Implant Esthetics. Int. J. Dent. 2015, 2015, 740764. [Google Scholar] [CrossRef] [PubMed]
- Levine, R.A.; Huynh-Ba, G.; Cochran, D.L. Soft Tissue Augmentation Procedures for Mucogingival Defects in Esthetic Sites. Int. J. Oral Maxillofac. Implants 2014, 29, 155–185. [Google Scholar] [CrossRef]
- Sanz, M.; Lorenzo, R.; Aranda, J.J.; Martin, C.; Orsini, M. Clinical Evaluation of a New Collagen Matrix (Mucograft Prototype) to Enhance the Width of Keratinized Tissue in Patients with Fixed Prosthetic Restorations: A Randomized Prospective Clinical Trial. J. Clin. Periodontol. 2009, 36, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, R.; García, V.; Orsini, M.; Martin, C.; Sanz, M. Clinical Efficacy of a Xenogeneic Collagen Matrix in Augmenting Keratinized Mucosa around Implants: A Randomized Controlled Prospective Clinical Trial. Clin. Oral Implants Res. 2012, 23, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Puisys, A.; Zukauskas, S.; Kubilius, R.; Barbeck, M.; Razukevičius, D.; Linkevičiene, L.; Linkevičius, T. Clinical and Histologic Evaluations of Porcine-Derived Collagen Matrix Membrane Used for Vertical Soft Tissue Augmentation: A Case Series. Int. J. Periodontics Restor. Dent. 2019, 39, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Papi, P.; Pompa, G. The Use of a Novel Porcine Derived Acellular Dermal Matrix (Mucoderm) in Peri-Implant Soft Tissue Augmentation: Preliminary Results of a Prospective Pilot Cohort Study. Biomed. Res. Int. 2018, 2018, 6406051. [Google Scholar] [CrossRef]
- Zafiropoulos, G.-G.; Al-Asfour, A.A.; Abuzayeda, M.; Kačarević, Z.P.; Murray, C.A.; Trajkovski, B. Peri-Implant Mucosa Augmentation with an Acellular Collagen Matrix. Membranes 2021, 11, 698. [Google Scholar] [CrossRef]
- Horvath, A.; Molnar, B.; Gera, I.; Windisch, P. Comparison of Different Approaches Aimed at Increasing Peri-Implant Keratinised Mucosa. In Proceedings of the ITI World Symposium 2014, Geneva, Switzerland, 24–26 April 2014. [Google Scholar]
- Emanuel, E.J. Reconsidering the Declaration of Helsinki. Lancet 2013, 381, 1532–1533. [Google Scholar] [CrossRef]
- Schmitt, C.M.; Moest, T.; Lutz, R.; Wehrhan, F.; Neukam, F.W.; Schlegel, K.A. Long-Term Outcomes after Vestibuloplasty with a Porcine Collagen Matrix (Mucograft ®) versus the Free Gingival Graft: A Comparative Prospective Clinical Trial. Clin. Oral Implants Res. 2016, 27, e125–e133. [Google Scholar] [CrossRef]
- Vignoletti, F.; Nunez, J.; Sanz, M. Soft Tissue Wound Healing at Teeth, Dental Implants and the Edentulous Ridge When Using Barrier Membranes, Growth and Differentiation Factors and Soft Tissue Substitutes. J. Clin. Periodontol. 2014, 41 (Suppl. S15), S23–S35. [Google Scholar] [CrossRef] [PubMed]
- Rothamel, D.; Benner, M.; Fienitz, T.; Happe, A.; Kreppel, M.; Nickenig, H.-J.; Zöller, J.E. Biodegradation Pattern and Tissue Integration of Native and Cross-Linked Porcine Collagen Soft Tissue Augmentation Matrices—An Experimental Study in the Rat. Head. Face Med. 2014, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Pabst, A.M.; Ackermann, M.; Moergel, M.; Jung, J.; Kasaj, A. Biofunctionalization of Porcine-Derived Collagen Matrix Using Enamel Matrix Derivative and Platelet-Rich Fibrin: Influence on Mature Endothelial Cell Characteristics In Vitro. Clin. Oral Investig. 2018, 22, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Pabst, A.; Lehmann, K.-M.; Walter, C.; Krueger, M.; Stratul, S.-I.; Kasaj, A. Influence of Porcine-Derived Collagen Matrix on Endothelial Progenitor Cells: An in Vitro Study. Odontol. Soc. Nippon Dent. Univ. 2014, 104, 19–26. [Google Scholar] [CrossRef]
- Nandkeoliar, T.; Kumar, A.; Chungkham, S.; Singh, S.S. Estimation of Vestibular Depth: An Observational Cross-Sectional Study. J. Indian Soc. Periodontol. 2023, 27, 320–327. [Google Scholar] [CrossRef]
Figure 1.
Detailed description of the surgical procedure. (A) Split-thickness incision at MGJ. (B) Split-thickness mobilisation using a blade or periosteal elevator. (C) Recipient site with depth of 10 mm. (D) Slight liberation of lingual flap edge to allow the XDM to tuck underneath. (E) Trimming and rehydration of the XDM with sterile saline. (F) Adaptation and positioning of the XDM towards the attached mucosa using modified mattress and single interrupted sutures. (G) Provision of tight contact between periosteum and graft using deep periosteal internal horizontal mattress sutures. (H) Immobilisation of the coronal flange of the buccal mucosal flap to the apical part of the same flap using simple continuous suture.
Figure 1.
Detailed description of the surgical procedure. (A) Split-thickness incision at MGJ. (B) Split-thickness mobilisation using a blade or periosteal elevator. (C) Recipient site with depth of 10 mm. (D) Slight liberation of lingual flap edge to allow the XDM to tuck underneath. (E) Trimming and rehydration of the XDM with sterile saline. (F) Adaptation and positioning of the XDM towards the attached mucosa using modified mattress and single interrupted sutures. (G) Provision of tight contact between periosteum and graft using deep periosteal internal horizontal mattress sutures. (H) Immobilisation of the coronal flange of the buccal mucosal flap to the apical part of the same flap using simple continuous suture.

Figure 2.
Overview of treatment stages in the upper jaw. (A) Lack of sufficient keratinised mucosa preoperatively. (B) Immediate view after surgery. (C) Six-month follow-up. (D) Twelve-month follow-up. (Black two-way arrows indicate the measured buccal width dimensions of the newly formed PIKM).
Figure 2.
Overview of treatment stages in the upper jaw. (A) Lack of sufficient keratinised mucosa preoperatively. (B) Immediate view after surgery. (C) Six-month follow-up. (D) Twelve-month follow-up. (Black two-way arrows indicate the measured buccal width dimensions of the newly formed PIKM).

Figure 3.
Overview of treatment stages in the lower jaw. (A) Lack of sufficient keratinised mucosa preoperatively. (B) Immediate view after surgery. (C) Six-month follow-up. (D) Twelve-month follow-up. (Black two-way arrows indicate the measured buccal width dimensions of the newly formed PIKM).
Figure 3.
Overview of treatment stages in the lower jaw. (A) Lack of sufficient keratinised mucosa preoperatively. (B) Immediate view after surgery. (C) Six-month follow-up. (D) Twelve-month follow-up. (Black two-way arrows indicate the measured buccal width dimensions of the newly formed PIKM).

Figure 4.
PIKM-W changes in the maxilla and mandible. The red line indicates the 2 mm minimum necessary PIKM-W.
Figure 4.
PIKM-W changes in the maxilla and mandible. The red line indicates the 2 mm minimum necessary PIKM-W.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Demographic data and site distribution.
| Maxilla | Mandible | |
|---|---|---|
| Age | 55.92 ± 14.38 | 57.71 ± 11.2 |
| Male | 4 | 0 |
| Female | 8 | 12 |
| Premolar | 3 | 4 |
| Molar | 9 | 8 |
Table 2.
Changes in PIKM-W in the maxilla.
| Time | Mean | SD | p-Value |
|---|---|---|---|
| Initial | 0.42 | 0.47 | 0.00002 |
| 6 months | 3.17 | 1.21 | |
| Difference | 2.36 | 1.34 | |
| Initial | 0.42 | 0.47 | 0.00035 |
| 12 months | 2.36 | 1.34 | |
| Difference | 1.94 | 1.37 | |
| 6 months | 3.17 | 1.21 | 0.009 |
| 12 months | 2.36 | 1.34 | |
| Difference | 0.81 | 0.09 |
Table 3.
Changes in PIKM-W in the mandible.
| Time | Mean | SD | p-Value |
|---|---|---|---|
| Initial | 0.29 | 0.45 | 0.010 |
| 6 months | 1.58 | 1.44 | |
| Difference | 1.29 | 0.70 | |
| Initial | 0.29 | 0.45 | 0.023 |
| 12 months | 1.08 | 1.07 | |
| Difference | 0.79 | 0.44 | |
| 6 months | 1.58 | 1.44 | 0.033 |
| 12 months | 1.08 | 1.07 | |
| Difference | 0.50 | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Horváth, A.; Windisch, P.; Palkovics, D.; Li, X. Novel Technique to Reconstruct Peri-Implant Keratinised Mucosa Width Using Xenogeneic Dermal Matrix. Clinical Case Series. Dent. J. 2024, 12, 43. https://doi.org/10.3390/dj12030043
AMA Style
Horváth A, Windisch P, Palkovics D, Li X. Novel Technique to Reconstruct Peri-Implant Keratinised Mucosa Width Using Xenogeneic Dermal Matrix. Clinical Case Series. Dentistry Journal. 2024; 12(3):43. https://doi.org/10.3390/dj12030043
Chicago/Turabian StyleHorváth, Attila, Péter Windisch, Dániel Palkovics, and Xinda Li. 2024. "Novel Technique to Reconstruct Peri-Implant Keratinised Mucosa Width Using Xenogeneic Dermal Matrix. Clinical Case Series" Dentistry Journal 12, no. 3: 43. https://doi.org/10.3390/dj12030043
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.