
A Systematic Investigation of American Vaccination Preference via Historical Data
by
Jason Chen
1,†, 
Angie Chen
1,†,
Youran Shi
1,†,
Kathryn Chen
1,†,
Kevin Han Zhao
1,†,
Morwen Xu
1,
Ricky He
1 and
Zuyi Huang
2,* 1
American Scholars, Philadelphia, PA 19111, USA
2
Department of Chemical and Biological Engineering, Villanova University, Villanova, PA 19085, USA
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Processes 2022, 10(8), 1665; https://doi.org/10.3390/pr10081665
Submission received: 22 July 2022
/
Revised: 16 August 2022
/
Accepted: 19 August 2022
/
Published: 22 August 2022
(This article belongs to the Special Issue Analysis, Control and Modeling of Big Data for COVID-19 and Other Pandemics)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:While COVID-19 vaccines are generally available, not all people receive vaccines. To reach herd immunity, most of a population must be vaccinated. It is, thus, important to identify factors influencing people’s vaccination preferences, as knowledge of these preferences allows for governments and health programs to increase their vaccine coverage more effectively. Fortunately, vaccination data were collected by U.S. Census Bureau in partnership with the CDC via the Household Pulse Survey (HPS) for Americans. This study presents the first analysis of the 24 vaccination datasets collected by the HPS from January 2021 to May 2022 for 250 million respondents of different ages, genders, sexual orientations, races, education statuses, marital statuses, household sizes, household income levels, and resources used for spending needs, and with different reasons for not receiving or planning to receive a vaccine. Statistical analysis techniques, including an analysis of variance (ANOVA), Tukey multiple comparisons test, and hierarchical clustering (HC), were implemented to analyze the HPS vaccination data in the R language. It was found that sexual orientation, gender, age, and education had statistically significant influences on the vaccination rates. In particular, the gay/lesbian group showed a higher vaccination rate than the straight group; the transgender group had a lower vaccination rate than either the female or the male groups; older respondents showed greater preference for vaccination; respondents with higher education levels also preferred vaccination. As for the other factors that were not significant enough to influence vaccinations in the ANOVA, notable trends were found. Asian Americans had higher vaccination rates than other races; respondents from larger household sizes had a lower chance of getting vaccinated; the unmarried group showed the lowed vaccination rate in the marital category; the respondents depending on borrowed money from the Supplemental Nutrition Assistance Program (SNAP) showed a lower vaccination rate than people with regular incomes. Concerns regarding the side-effects and the safety of the vaccines were the two major reasons for vaccination hesitance at the beginning of the pandemic, while having no trust in the vaccines and no trust in the government became more common in the later stage of the pandemic. The findings in this study can be used by governments or organizations to improve their vaccination campaigns or methods of combating future pandemics.
1. Introduction
The 2019 coronavirus epidemic detrimentally affected the lives of billions of people across the globe. Infecting hundreds of millions of people, it destroyed economies and caused society to cease to function [1,2]. As of September 2021, COVID-19 has affected more than 234 million people in 223 countries, areas, or territories, causing over 6 million deaths [3]. For example, the statistics from a study conducted in India revealed the severe consequences of COVID-19 on the country in terms of affecting India’s economy and causing social unrest and increased rates of domestic violence [2]. To combat and slow the spread of the COVID-19 virus, governments have implemented protocols such as physical distancing, mass-facemask usage, and quarantines. However, these non-pharmaceutical interventions proved intrusive to daily life and were unsustainable [4]. As a result, mass vaccination presented itself as the most cost-effective and efficient method for returning to the previous ‘status quo’ [5,6]. However, vaccines were not accepted universally. Studies conducted by Guillon and Kergall found that only 30.5% of respondents would agree to get vaccinated when in France [7]. Similarly, a Chinese survey found that 47.8% of the participants opted to wait until the safety of the vaccine was determined [8]. It is crucial to determine and analyze the factors that discourage parts of the population from becoming vaccinated.
Surveys have been conducted to study the factors influencing people’s preference for vaccination in quite a few countries, including but not limited to European countries, Arabic-speaking countries, and Asian countries (e.g., China, India, Japan, Iran, and Thailand). An overview on those existing survey studies is given below to highlight the factors influencing people’s vaccination preferences in various countries. Since neighboring countries have influenced each other in battling COVID-19, the countries are generally listed below according to their geographic locations. Studies in four European countries (i.e., the UK, Germany, Italy, and Spain) and India found that the vaccine efficacy followed by the vaccine cost were considered the most prominent factors in vaccine hesitancy [3], while studies in France found a direct correlation between knowledge of the vaccine’s safety and vaccination rates [7]. Meanwhile, the studies conducted by Toshkov 2022 [9] using the data from Eurobarometer for 27 European Union countries determined that individuals who trust the Internet and social networks as sources of information on health were less likely to trust the COVID-19 vaccine. This was further confirmed by the arguments against COVID-19 vaccines on Facebook in Poland [10]. In addition, trust in institutions was found to be an important factor behind vaccine acceptance in certain European countries [11,12]. Meanwhile, a study conducted in Poland revealed that fears of adverse side effects and allergic reactions were the most prominent reasons for vaccine hesitancy [13]. Furthermore, studies performed in Italy and Germany found that despite their occupation, healthcare workers were not much more likely to accept the vaccine than ordinary people [14,15]. Studies conducted in the UK posited vaccine safety [16,17] and distrust in the government [18] as the top reasons for vaccine hesitancy. Furthermore, ethnic minority groups in the UK have been found to be less accepting of the vaccine than the white population [19,20]. In addition, surveys performed in the UK have found individuals who are strongly against getting vaccinated to be especially affected by incentives of personal benefit [21], and more than one-third of respondents felt uncertain about the vaccine [22]. The rates of vaccine hesitancy were also found to be different by country in Europe; for example, the rate was 6.8% in Spain versus 61.8% in Bulgaria [23]. Studies performed in Arabic-speaking countries determined that demographics such as sex, age, and the highest level of education had a significant influence on vaccine acceptance [24], with respondents who were male or achieved higher education being more likely to accept the vaccine [25,26]. Meanwhile, the most prominent factors behind vaccine hesitation in the Arabic population were determined to be a fear of adverse side effects and distrust of healthcare policies and centers [27,28]. Furthermore, studies found that Arabs who resided outside of their birth countries were more likely to get vaccinated [29] and a connection was identified between vaccine hesitancy and unemployment [30]. Another study suggests that the large majority of the Saudi population are knowledgeable and have positive attitudes about the vaccine [31]. Studies conducted in China determined that individuals were more likely to accept the vaccine if they believed in its efficacy [1] and if it had a long and effective lifespan [5]. Conversely, factors such as the vaccine price and convenience encouraged vaccine hesitancy among respondents [8]. Meanwhile, concerns of potential side effects were determined to be the top reasons for vaccine hesitancy in both children ages 15–17 [32] and medical students in China [33]. Another study performed in China found that women and those who practiced preventative measures such as masking and social distancing were more likely to accept the vaccine [34]. Individuals who were accepting of recommendations from family and friends had higher vaccination rates [35], and 69% of respondents reported having trust in the vaccine [36]. Studies conducted in India identified fear of side effects and peer vaccination rates as important influencers in vaccine acceptance [2]. Other factors such as the perception of the vaccine being necessary, trusting the government, and indifference towards the vaccine costs were all correlated with vaccine acceptance [37]. Another study conducted in India found that although 33.1% of respondents were hesitant to get the vaccine, only 50% were confident in the vaccine’s efficacy [38]. Meanwhile, medical students in India who were hesitant about the vaccine were more likely to absorb medical information from social media rather than from teachers at medical school [39]. Studies conducted in Japan concluded that respondents who were older, married, or achieved higher education were more likely to get vaccinated [40], and that the vaccine’s efficacy and side effects had the most significant impacts on vaccine preference [41]. A study performed in Iran found that respondents who were older, female, or working in healthcare were less likely to accept the vaccine [42], while a study in Pakistan identified income, education level, and contact with COVID-19 as significant influences on vaccine preference [43]. A study conducted in Thailand found political affiliation to be a significant factor on not only vaccine acceptance, but also vaccine type [44]. Studies from both Europe and Asia [44,45] concluded that the idea of vaccination was not only swayed by pre-existing attitudes, but also by ethnic background, country of origin of the vaccine, duration of immunity, and political affiliation. In particular, studies conducted in the politically divided nations of Thailand and Hungary showed that support for the governing political party was directly correlated to the acceptance of the government-approved vaccine [44]. Vaccine acceptance in Thailand was also based upon ethnic biases, as Western-made vaccines were overwhelmingly more preferred over vaccines produced in China. Likewise, Hungarians were more inclined to accept an Eastern vaccine from Eastern countries (e.g., Russia or China) than other Central Europeans, a circumstance linked to the growing rift between Western Europe and Hungary [45]. On the contrary, the Chinese public was found to be more accepting and less afraid of a domestic vaccine [1]. Furthermore, studies conducted in the United States revealed that African Americans were the most skeptical of coronavirus vaccination. This distrust, caused by concerns of underlying racism in the healthcare system and medical injustices such as the Tuskegee Syphilis Study, was a focal point of the American vaccination campaign [46,47]. Similar studies performed in China showed that vaccine hesitancy was linked to a low perceived benefit, low risk of the virus, concern about fake or faulty vaccines, as well as income affecting the willingness to pay, all owing to the tight lockdown and quarantine procedures enforced by the Chinese government [48,49]. Parallels can be drawn to another study for household income, as an Indian survey found that low-income respondents were nearly 1.5 times as likely to receive a vaccine when compared to high-income participants.
While the aforementioned surveys or studies reveal certain factors for vaccination preference, few studies have been conducted with the consideration of these factors for Americans’ preferences in vaccination. An analysis of the elements relating to vaccine reluctance is essential when combating COVID-19 or any future epidemic. The World Health Organization identified vaccine hesitancy as one of the top dangers to world health in 2019 [50], and the coronavirus epidemic proved that vaccine hesitancy was not linked to a single set of factors, but to a multitude of elements depending on, but not limited to, ethnicity, education, marital status, household size, and sexual orientation. Fortunately, the U.S. Census Bureau in partnership with the CDC conducted the Household Pulse Survey (HPS) [51,52] in which questions on various factors concerning vaccination reluctance in the U.S. were designed for twenty-four 20-min online surveys from January 2021 to May 2022. The Household Pulse Survey is the first nationally representative survey providing timely information about the most comprehensive factors that reflect the social and economic implications of COVID-19. The sample pool consisted of around 250 million people selected via the Master Address File (MAF), which is a system in which the survey could be distributed to the most representative households in the country. Since the survey was designed to collect and distribute the data efficiently, the data were collected in phases in which new demographics could be surveyed. Certain studies have been performed with the HSP data due to the high reliability and abundance of information. For example, a study conducted by Cai et al. [51] utilized the HSP data to evaluate trends in anxiety and depression systems during the coronavirus pandemic. Another study made use of the HSP data to analyze the racial and ethnic disparities in household food insecurity during the pandemic [52]. Differing from these existing studies, in this study we utilized the HSP data to examine potential reasons for vaccine hesitancy. In addition, more factors, including but not limited to race, age, education status, marital status, household incomes, household sizes, income resources, and sex orientation, were included in the 24 datasets in this study. As no comprehensive study has been performed with these datasets on a multitude of factors suspected to impact rates of vaccine acceptance in the U.S., this work presents the first comprehensive study on the HSP vaccination preference data.
Since the HPS database contains 24 datasets that include many factors for vaccination preference, an analysis of variance (ANOVA), a statistical analysis technique commonly used to determine if there is statistical difference in the means of three or more independent groups [53,54,55,56], was used to determine if people show statistical differences in their vaccination preference because of age, gender, sexual orientation, races, education status, marital status, household size, household income level, resources used for spending needs, and reasons for not receiving or planning to receive a vaccine. A Tukey multiple comparisons test, which is similar to the t-test but with multiple pairwise comparisons [57], was further used to identify the groups with statistical differences in their vaccination preference for each of the aforementioned ten categories of factors. The hierarchical clustering method [58,59] was also used to illustrate the differences in the different groups’ preferences for vaccination. Moreover, the most dominant reasons for vaccine rejection were analyzed from the datasets. RStudio, a free open-source software used for data science, was used to compile and analyze the 24 datasets chosen for this study. The results from this research could provide valuable information regarding vaccine hesitancy to governments or organizations battling future pandemics.
2. Materials and Methods
2.1. The Household Pulse Survey Dataset on COVID-19 Vaccination
The datasets utilized within this study were derived from the Household Pulse Survey conducted by the U.S. Census Bureau in partnership with the CDC. For this study, only data from adults over the age of 18 were used because vaccination data for younger ages did not become available until the vaccine was approved for minors later in the vaccination rollout process. The Household Pulse Survey started on 23 April 2020 and continued through numerous phases, including phase 1 (23 April 2020 to 21 July 2020), phase 2 (19 August 2020 to 26 October 2020), phase 3 (28 October 2020 to 29 March 2021), phase 3.1 (14 April to 5 July 2021), phase 3.2 (21 July 2021 to 11 October 2021), phase 3.3 (1 December 2021, to 7 February 2022), and phase 3.4 (2 March to 9 May 2022). While the Household Pulse Survey began in April 2020, the first set of vaccination data became available on 6 January 2021, in phase 3. Since the main focus of the study was on the vaccination data, 6 January 2021 was called period 1 for the vaccination survey. Furthermore, phases 3.3 and later maintained the two-week collection periods but shifted to a two-weeks on, two-weeks off approach. Despite this, continuous period indexes were used for these collection “weeks” to maintain continuity. There were 24 datasets in total used in this study for vaccination preference. Because some options and categories were added in later weeks of the survey, the categories with all data for all periods were prioritized, with gender and sexual orientation being two exceptions with only 12 datasets.
The specific datasets utilized in this study include the numbers of vaccination cases for people from different groups of ages, genders, sexual orientations, races, education statuses, marital statuses, household sizes, household income levels, resources used for vaccination, and reasons for not receiving or planning to receive a vaccine. The data provided in the Household Pulse Survey only contain general statistical information for these ten categories. For example, each of the 24 datasets is listed in a table to show the total number of survey participants, the number of vaccinated participants, and the number of participants not vaccinated for each group in each category (e.g., ages 18–24 (Age18), ages 25–39 (Age25), ages 40–54 (Age40), ages 55–64 (Age55), and ages 65 and over (Age65)). The information for the ten categories (e.g., ages, genders, and races) is not integrated for any individual participants so that no personal information is provided. This limits the possibility to study the interactions of these ten categories in terms of participants’ vaccination preferences.
2.2. Statistical Analysis of the Dataset to Identify Factors for Vaccination Preference in the U.S.
The data for the age category are used as an example in Figure 1 to illustrate the statistical analysis procedure implemented in this study. The data from the Household Pulse Survey first were downloaded onto a Microsoft Excel spreadsheet and sorted into sampling periods, with each period composed of data on the vaccination preferences of various groups of sociodemographic information. In order to prepare the data for analysis, it was necessary to extract the data. To do so, the data were organized into a matrix where each row represented each option in the survey (e.g., different age groups in Figure 1A), and each column was grouped into trios: the first column represented the total number of respondents in that category, the second column represented participants who had been vaccinated, and the third column represented participants who had not or would not get vaccinated. Due to the varying numbers of total responses for each category in each sampling period, the data were translated into percentage profiles by normalizing the participants with and without vaccination by the total number of participants in each period. Only the results for the vaccination percentage data were shown in this work, as similar conclusions were obtained from the analysis of the data for the non-vaccination percentage.
After the data were extracted and integrated into a matrix for each of the ten selected categories (e.g., ages and races), they were imported into Rstudio (a user interface of the R language) for a subsequent analysis. In particular, R programs were written to create graphs to illustrate similarities and differences for each option in each of the ten categories over the 24 time periods. The data matrix for each category was then analyzed via an analysis of variance (ANOVA) test. The purpose of an ANOVA test was to analyze the data matrix to conclude if the groups of participants in each category show statistically significant differences in vaccination preference. Since each data matrix had more than two groups (which is the constraint of the t-test), the ANOVA was more suited to analyze the statistical differences. The ANOVA test produces a p-value that indicates whether or not the options showed significant statistical differences. If the p-value is less than 0.05, it supports an alternate hypothesis, meaning there is a statistical difference in vaccination preference in the groups of survey participants in the studied category. However, if the p-value is higher than 0.05, there is evidence to support the null hypothesis, meaning that there is no statistical difference in vaccination preference in the studied category. An ANOVA was conducted for each of the following nine categories: ages, genders, sexual orientations, races, education statuses, marital statuses, household sizes, household income levels, and resources used for vaccination. The last category, i.e., reasons for not receiving or planning to receive a vaccine, was not analyzed with an ANOVA, as the options in it may not have been independent of each other (e.g., concern for vaccine safety versus concern for vaccine side-effects).
While an ANOVA will indicate whether there is a significant difference in vaccination preference in the studied category, it will not show which groups of participants have significantly different vaccination preferences. A Tukey multiple comparison test was, thus, conducted to further validate the category with no significant differences (all p-values in the paired groups with p-values higher than 0.05 in the Tukey multiple comparisons test) or identify the pairs of groups with significant differences in vaccination preference (the pairs with p-values less than 0.05). Compared with a t-test, a Tukey multiple comparisons test can analyze all groups of participants in the category (not being limited to two groups at one time like the t-test) and correct the family-wise error rate. Finally, hierarchical clustering was performed to present the similarities of different groups in their vaccination preference in a dendrogram (no matter whether a significant difference in vaccination preference was detected or not for the category). Each cluster is distant from one another and allows for a tree-like visual, representing which sets of data share similarities and which are widely different from one another. In particular, the groups at similar heights in the dendrogram (e.g., Age18 group and Age25 group in Figure 1D) show similar preferences in vaccination, while the groups more distant from each other (e.g., the Age65 group and Age18 group in Figure 1D) show less similarity in their vaccination preference.
3. Results
This study analyzed various categories of factors that could have affected the respondents’ attitudes toward COVID-19 vaccines: age, education level, race, household size, gender, sexual orientation, marital status, sources, household income, and reasons for non-vaccination. The data were used to draw graphs that were then analyzed via an ANOVA to determine whether a specific category or factor had a statistically significant influence on the vaccine preference. The Tukey multiple comparisons test was then used to examine the statistical significance of the differences in vaccine preference between different groups of that factor. Hierarchical clustering diagrams were finally utilized to illustrate the similarity of different groups for the selected factors in terms of their vaccination preference.
3.1. The Preferences of People from Different Ages for Vaccination
Figure 2A illustrates the vaccination percentages of people in different age groups. It is interesting to see that people from older age groups generally show higher preference for vaccination. In particular, the Age65 group had the highest vaccination rate. This may be due to participants in this age group being prioritized during the time of limited vaccine production. An ANOVA was conducted to study whether any age group showed a significant difference in their preference for vaccination. The p-value returned from the ANOVA was 0.021. Since the p-value was less than 0.05, the people with different ages did show a significant difference in vaccination preference. Meanwhile, the Tukey multiple comparisons test demonstrated that people from the Age65 group had a stronger preference for vaccination than people from the Age18 group (p-value 0.025) and people from the Age25 group (p-value 0.055, close to 0.05). To further validate this result, hierarchical clustering was implemented to show the similarities of vaccine preferences between the different age groups (Figure 2B). The figure reveals that people from the Age65 group had the least similarity to people from the Age18 and Age25 groups and that the older age groups were generally separated from younger ones.
3.2. The Preferences of People with Different Education Levels towards Vaccination
In Figure 3A, each line represents a different level of academic achievement, ranging from individuals who have not graduated from high school to those who hold a bachelor’s degree or higher, with data collected at the end of each interval. The visual analysis of the graph revealed that the growth of each group follows a general exponential growth model until approximately the 7th sampling period, where the vaccine percentage values begin to level out. The ANOVA provided a p-value of 0.046. As this value is less than the alpha level of 0.05, there was evidence to reject the null hypothesis (i.e., the mean difference of each group was statistically similar to one another). This hypothesis was further reinforced by the results of a Tukey multiple comparisons test: the mean difference between the groups ‘bachelor or higher’ and ‘less than high school’ yielded a p-value of 0.038, proving that the difference in means was statistically significant due to being less than the alpha level. Furthermore, the group ‘bachelor or higher’ was shown to be the least similar to the cluster of groups ‘less than high school’ and ‘high school or GED’ when an analysis of a cluster dendrogram obtained through hierarchical clustering was performed (Figure 3B).
3.3. The Preferences of People of Different Races for Vaccination
Through the ANOVA that was conducted to determine whether race played a significant role in vaccination preference, a p-value of 0.19 was found. Since this value was not less than or equal to 0.05, it can be concluded that race was not an important factor in the differences in vaccination preference. This hypothesis was further supported by the Tukey multiple comparisons test, which tested whether any particular racial group had a stronger preference towards getting vaccinated. All p-values obtained from the test suggested that none of the racial groups had a stronger preference over the others. The two comparisons with the closest value to 0.05 were the Asian group compared to the others group (with two or more races) with a p-value of 0.15, and the Asian group compared to the Black group with a p-value of 0.29. Although there was no statistical evidence that any of the groups favored vaccination more than the others, Figure 4A shows that the Asian group generally surpassed every other racial group in their vaccination percentages. This showed that while a difference did exist, the difference was not significant enough for the ANOVA test and the Tukey multiple comparisons test to conclude a statistically significant difference between racial groups in terms of getting vaccinated. The hierarchical clustering result in Figure 4B supports the data found in the Tukey multiple comparisons test by showing how the Asian group was the most different from the others and Black groups. Figure 4B also shows that the White and Latino racial groups were most similar to each other in their vaccination preferences, while the Black and others racial groups were most similar to each other in their vaccination preferences.
3.4. The Preferences of People with different Household Sizes forf Vaccination
As can be determined by a brief firsthand examination of Figure 5A, the rates of vaccination among every household size increase at an exponential rate until the 7th sampling period. With the exception of household sizes 5, 6, and 7+, which continue to fluctuate more significantly, the percentages of vaccine acceptance largely flatline from the 7th time period onwards. Then, in order to determine whether the household size played an important role in the respondents’ decisions to get vaccinated, an ANOVA was conducted, which returned a p-value of 0.13. Because this value is larger than 0.05, it can be concluded that the null hypothesis is true, or that differences in the respondents’ household sizes did not have a significant corresponding effect on their vaccine preferences. This result was further corroborated by a Tukey multiple comparisons test, which only returned p-values of no less than 0.12 (households with 2 people versus households with 7+ people). Since no value was less than 0.05, there was no extraordinary difference between the vaccine acceptance rates of respondents from any two differing household sizes. Figure 5B further validates this result, showing the similarities of each household size by vaccine acceptance. Notably, the household size with 7+ people appeared as an outlier both in the hierarchical clustering and the previous Tukey multiple comparisons test, but not to a significant enough degree to consider the alternative hypothesis, or that differences in respondents’ household sizes did have a significant corresponding effect on their vaccine preference.
3.5. The Preferences of People with Different Marital Statuses for Vaccination
It can be observed from Figure 6A that each of the groups increased exponentially (until around the 7th sampling period) in a specific order. Throughout the graph, the order remained the same with much overlap: the status “widowed” continuously had the highest percentage, with the “married” status being second, “divorced/separated” being third, and “never married” remaining last. Before the 7th sampling period, the “divorced/separated” status and “married” status were more clumped together. From period 7 onwards, each groups’ data points remained mostly stagnant, as the only change that occurred was that the points of the groups gradually moved closer. Since the ANOVA returned a p-value of 0.26, which was greater 0.05, the null hypothesis was accepted, meaning the groups with different marital statuses did not show a significant difference in their preference for vaccination. A Tukey multiple comparison test also returned p-values that were all above 0.05, further indicating no significant difference between the groups with different marital statuses. Although the difference between different marital groups was not significant, Figure 6B does show that the participants from the “widowed” group and the “married” group were less similar to those from the “married” group and the “divorced/separated” group.
3.6. The Preferences of People with Different Income Sources for Vaccination
Figure 7A illustrates that all resources increased exponentially until the 6th and 7th time periods. After the 7th period, the ‘RegIncome’, ‘credit or loans’, and ‘savings’ groups maintained a relatively consistent pattern, while the others showed significant fluctuations. Of all the datasets, the resources from the regular income remained the greatest until period 14, where ‘credit or loans’ surpassed this group. The resources from ‘SNAP’, however, consistently had the lowest percentage. Moreover, the p-value from the ANOVA was 0.27 (p > 0.05), which indicated that the eight groups with different income resources did not have significant statistical differences in vaccination preference. This result was reflected in the Tukey multiple comparisons test, where the returned p-values were all above 0.05. Furthermore, the hierarchical clustering in Figure 7B demonstrated similarities between participants with a ‘regular income’ and ‘credit or loans’, between ‘savings’ and ‘stimulus’, and between ‘borrowing’ and ‘SNAP’. The less similar groups, such as ‘regular income’ versus ‘SNAP’, are located in separate branches in Figure 7B.
3.7. The Vaccination Preferences of People with Different Household Incomes
An ANOVA was conducted to study whether those with different household incomes showed significant differences in their preference for vaccination (Figure 8A). The p-value returned from the ANOVA was 0.22. Since the p-value was more than 0.05, the households with different incomes did not show significant differences in vaccination preference. Although the data collectively did not show conclusive evidence proving a substantial variation in vaccination results, a Tukey multiple comparisons test was performed, which showed that people from the “>$250,000” group had a slightly stronger preference for vaccination than people from the “<$25,000” group (p-value 0.23). Although the p-value was not less than 0.05, it was the lowest p-value calculated from the Tukey multiple comparisons test. The results between the highest salary and lowest salary showed the most sizable difference. To further validate the results, hierarchical clustering was implemented to show the similarities of different household income groups in their preferences for vaccination (Figure 8B). This showed that people from the “>$200,000”, “$199,999”, and “$149,999” groups showed the least similarity to people from the “<$25,000” group.
3.8. The Preferences of People with Different Genders for Vaccination
Unlike the factors listed in previous subsections, there were only 12 samples of vaccination data available on gender and sexual orientation, as these categories were added onto the survey questionnaire in the middle stage of the Household Pulse Survey. The options that were used in this category included cisgender male, cisgender female, and transgender. The ANOVA returned a p-value of 0.002, which was smaller than 0.05. It can, thus, be concluded that gender had a significant impact on vaccination preference. With evidence from Figure 9A, it can be observed that the vaccination rates of transgender people were relatively lower than the rates of male and female people for the first ten sampling periods, before climbing up and reaching rates higher than those of male and female people during sampling periods ten to twelve. Nevertheless, the vaccination rates for males and females stayed comparatively constant throughout the whole period of data collection.
The Tukey multiple comparisons analysis indicated that the transgender group held a p-value of less than 0.05, as compared with either the male or female groups, with p-values of 0.010 and 0.002, respectively. This also indicates that the transgender group showed significant differences from the other two groups in their vaccination preference. By analyzing the hierarchical clustering diagram, it can be seen that the “transgender” group had less similarities with both the male and female groups in terms of vaccination preference.
3.9. The Preferences of People with Different Sexual Orientations for Vaccination
Similar to the factor ‘gender’, the data for ‘sexual orientation’ were only sampled in the last 12 periods. This category included three options: “gay/lesbian”, “straight”, and “bisexual”. The p-value returned from the ANOVA was less than 0.001. Since this value was lower than 0.05, the sexual orientation had a significant impact on the participants’ vaccination attitudes. As seen in Figure 10A, the vaccination rates of the straight group always fluctuated below those of the bisexual and gay/lesbian groups. The gay/lesbian group surpassed all other groups when it came to vaccination rates. The Tukey multiple comparisons test further strengthened this conclusion by showing that the gay/lesbian groups had a similarity p-value of less than 0.05 with either the straight group or the bisexual group. This trend was also reflected in the hierarchical clustering diagram (Figure 10B), in which the gay/lesbian group had less similarity with the straight and bisexual groups.
3.10. Reason for Not Receiving or Planning to Receive Vaccines
The following nine reasons were surveyed in all 24 datasets: (1) concerned about possible side effects; (2) do not know if a vaccine will protect me; (3) do not believe I need a vaccine; (4) doctor has not recommended it; (5) plan to wait and see if it is safe; (6) concerned about the cost; (7) do not trust COVID-19 vaccines; (8) do not trust the government; (9) do not think COVID-19 is a big threat. The numbers of people not receiving or planning to receive vaccines due to each of these reasons are shown in Figure 11. It can be seen that concerns regarding the side effects (reason 1, the blue curve) and vaccine safety (reason 5, the cyan curve) were the two dominant reasons for people not taking vaccines at the beginning of the pandemic. It can be recognized that the number of people not taking vaccines due to these two reasons generally decreased over time. “COVID-19 is not a big threat” seemed to show a slight gradual increase throughout the time periods. “Do not trust COVID-19 vaccines” and “do not trust the government” generally had the highest numbers of non-vaccination cases besides the two dominant factors. “Doctor has not recommended it” and “concerned about the cost”, on the other hand, were the reasons that had generally the lowest numbers of non-vaccination cases.
4. Discussion
4.1. Factors with Significant Impacts on Respondents’ Vaccination Preferences
This study presents the first analysis of vaccination data from the Household Pulse Survey data to deeply investigate and identify various sociodemographic factors that strongly influence vaccine preference in the U.S.. The findings of this study suggest that an individual’s age plays an important role in his or her decision to get vaccinated (p-value 0.021). In particular, the respondents who were at least 65 years old showed a significantly greater preference for vaccination than those who were 18–24 years old or 25–39 years old. These findings are consistent with previous studies that claimed that COVID-19 is particularly threatening to the elderly, where elderly individuals were allotted priority access to vaccines [60]. Hence, as reflected in the data, those who are at least 65 years old are more likely to receive the vaccine. However, disparities in vaccination rates do not exist solely between these polar age groups. With the exception of ages 18–24 and 25–39, which frequently fluctuated and overtook each other over the course of the survey, older age groups generally showed higher vaccinations rate than younger ones (Figure 2). Thus, the data suggest a directly proportional relationship between age and vaccination rates.
Through the same data analysis methods, this study identified education level as a prominent factor in vaccine preference (p-value 0.0464), with a statistically significant difference in vaccination rates between respondents with a bachelor’s degree or higher and those with less than a high school education. These results suggest that individuals who have reached higher levels of education are more likely to accept the vaccine than those at lower levels, which builds upon the existing evidence of this hypothesis from past studies [25,61,62]. Coupled with data that identified the fear of potential side effects as a top reason for vaccine hesitancy (Figure 11), these results may support the belief that those with greater education are generally knowledgeable about the vaccine’s side effects and more willing to get vaccinated [63].
Individual gender was also determined to have a significant impact on vaccine preference (p-value 0.002). In particular, the difference in vaccination rates of individuals who identified as transgender compared to those who identified as cisgender males or females was statistically significant. These data indicate that transgender individuals are more likely to reject the vaccine than cisgender males or females. Another notable observation that can be made from the data is that males and females shared very similar percentages of vaccination throughout all 12 sampling periods of data collection (Figure 9). This result was different from the findings of previous studies, which had shown women to be less likely to accept the vaccine than men [7,40,50,64]. The difference may have been due to the different countries involved (European region for [7,50], Japan for [40], and Hong Kong for [64]) compared to this study (i.e., the U.S.).
Another factor that demonstrated an important influence on the individual vaccine preference was sexual orientation (p-value less than 0.001). The data show that individuals who identified as gay or lesbian were consistently more likely to accept the vaccine than those who identified as straight or bisexual (Figure 10). Unlike other common factors such as age and education that have been included in existing surveys or studies, few general statements or assumptions have been made towards groups belonging to different sexual or gender identities. While this study reflects the impact of sexual or gender identities on vaccination preferences, further research is needed to sufficiently explain these findings.
While the aforementioned factors (i.e., age, education status, gender, and sexual orientation) were found significant by the ANOVA regarding vaccination preference, certain patterns were found in the vaccination profiles for other factors. Although these patterns were not significant enough in the ANOVA, they are of value for further investigations. These patterns include: (1) Asian Americans showing stronger preferences for vaccination than other races (Figure 4); (2) lower vaccination rates were generally found in larger households (Figure 5); (3) the respondents who had never been married returned relatively lower vaccination rates than respondents with other marital statues (Figure 6); (4) the respondents whose incomes were borrowed or depended on the Supplemental Nutrition Assistance Program (SNAP) showed relatively lower vaccination rates than respondents living on other income sources (Figure 7); (5) respondents with higher household income levels generally had higher vaccination rates (Figure 8).
4.2. Major Reasons for Respondents’ Vaccination Hesitancy
Among the various reasons individuals reported for vaccine hesitancy, the concerns regarding the potential side effects and vaccine safety were most prominent at the initial phases of data collection (Figure 11). This finding could be attributed to the lack of information on the COVID-19 vaccine available to the general public when distribution first began. Although fears of adverse side effects have remained the top reason for vaccine hesitancy, this explanation is further corroborated by the sharp decline in the two aforementioned reasons as more information on the vaccine circulated over time (Figure 11). Another significant trend observed in the figure was the steady increase in individuals who refused the vaccine because they did not consider the outbreak of COVID-19 as a serious pandemic. This finding suggests that over time, individuals began to see the pandemic as less dangerous, which may have been a result of gradual reductions in COVID-19 cases and deaths as vaccination rates increased in the U.S. This public attitude reached state authorities, as evidenced by attempts to soften preventive measures such as quarantining and masking [47]. However, these scenarios were often followed by new outbreaks of the pandemic which caused increases in new COVID-19 cases [65]. Thus, care should be taken in the future to contain any similar pandemic more strictly before starting to lift preventive measures.
Meanwhile, concerns about the price of the COVID-19 vaccine decreased steadily over time, eventually becoming the least influential reason for vaccine hesitancy (Figure 11). This finding may have been the result of the gradual introduction of programs that offer cost-free vaccines to the public. The number of individuals rejecting the vaccine due to their distrust of the government fluctuated frequently (Figure 11). This pattern may reflect the wavering public responses to the U.S. government’s methods of containing the COVID-19 pandemic. Additionally, as the vaccine’s efficacy was proven as time went on, the number of individuals who were doubtful of whether the vaccine would protect them generally decreased (Figure 11).
4.3. Limitation of This Study
This study was based on the vaccination data provided in the Household Pulse Survey on 250 million people from January 2021 to May 2022 January in the U.S.. Therefore, the conclusions on the factors showing significant impacts on people’s vaccination preferences are limited to the 250 million survey respondents. Although this HPS dataset represents the most comprehensive data available on vaccination preferences in the U.S., it only shows the numbers of people taking vaccines from the different groups within each category (e.g., different age groups for the age category). The data between different categories of factors were not linked to individual respondents. Therefore, no integrated information was provided across the categories of factors for individual survey participants. This limited the investigation of the interactions between those factors. Person-based surveys are recommended for future studies to address this issue. Moreover, questions on the types of vaccines should be included in future surveys to obtain a more comprehensive view of people’s vaccination preferences.
5. Conclusions
This study analyzed the factors and reasons that altered people’s vaccination hesitancy. The results were divided into categories, and each category was divided into multiple subgroups (e.g., ‘Asian’ and ‘Latino’ for the category ‘race’). The results demonstrated that sexual orientation, gender, education, and age had the most significant influences on vaccination attitudes. For the category ‘sexual orientation’, it can be concluded that gays and lesbians favored vaccination more than straight and bisexual individuals. For the category ‘gender’, it was shown that the subgroup ‘transgender’ was more reluctant towards vaccination than the subgroups ‘female’ and ‘male’. The results for the education category demonstrated that the subgroups with higher education levels showed higher preference for vaccination. In the data for the vaccination preferences of different age groups, individuals with older ages showed higher vaccination rates. The conclusions for the above factors are of statistical significance in the ANOVA test (i.e., p-value less then 0.05). For the following categories in which the null hypothesis was not rejected and was statistically not significant, notable trends in patterns in the line graphs and clustering dendrograms were still present. For the category ‘race’, the subgroup ‘Asian’ had higher vaccination rates than all other subgroups. In the category ‘household sizes’, the subgroup ‘7 or more people’ fell below all of the other groups in terms of its vaccination rate. The category ‘income source’ showed a similar pattern, whereby the subgroups ‘borrow’ and ‘SNAP’ were lower than the other groups. For the category ‘marital status’, the clustering dendrograms that were generated showed that the subgroups ‘never married’ and the subgroups ‘divorced’ and ‘married’ were the most different. The cluster dendrogram for the category ‘household income’ was also notable because the rich and poor groups were on opposite ends of the chart. The concerns regarding the side-effects and safety of the vaccines were the two major reasons for vaccination hesitancy at the beginning of the pandemic, and “do not trust COVID-19 vaccines” and “do not trust the government” played an important role later.
This study was the first one to be conducted on the vaccination data collected by the Household Pulse Survey in the U.S.. The data did not include all possible factors at the beginning of the survey; namely, the factors of gender and sexual orientation were not able to be recorded until later in the data collection cycle. Nonetheless, the study found the most crucial factors impacting vaccination levels, which may provide a baseline for governments to combat future pandemics. Although the data in this study were only taken from the U.S., the findings of this study may be referenced by other nations in the future.
Author Contributions
Conceptualization, Z.H.; methodology, J.C., A.C., Y.S., K.C., K.H.Z., M.X., R.H., Z.H.; formal analysis, J.C., A.C., Y.S., K.C., K.H.Z., M.X., R.H., Z.H.; data curation, J.C., A.C., Y.S., K.C., K.H.Z., M.X., R.H., Z.H.; writing—original draft preparation, J.C., A.C., Y.S., K.C., K.H.Z., M.X., R.H.; writing—review and editing, Z.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Bansal, P.; Raj, A.; Shukla, D.M.; Sunder, N. COVID-19 vaccine preferences in India. Vaccine 2022, 40, 2242–2246. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; He, Z.; Liu, T.; Huang, J.; Zhang, C.J.P.; Akinwunmi, B.; Ming, W.-K. Acceptance of and Preference for COVID-19 Vaccination in India, the United Kingdom, Germany, Italy, and Spain: An International Cross-Sectional Study, Germany, Italy, and Spain. Vaccines 2022, 10, 832. [Google Scholar] [CrossRef] [PubMed]
- Leng, A.; Maitland, E.; Wang, S.; Nicholas, S.; Liu, R.; Wang, J. Individual preferences for COVID-19 vaccination in China. Vaccine 2020, 39, 247–254. [Google Scholar] [CrossRef]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.; Feng, D.; Feng, Z.; Yeoh, E.; Wong, S.Y. Public preference for COVID-19 vaccines in China: A discrete choice experiment. Health Expect. 2020, 23, 1543–1578. [Google Scholar] [CrossRef]
- Huynh, H.P.; Senger, A.R. A little shot of humility: Intellectual humility predicts vaccination attitudes and intention to vaccinate against COVID-19. J. Appl. Soc. Psychol. 2021, 51, 449–460. [Google Scholar] [CrossRef]
- Guillon, M.; Kergall, P. Factors associated with COVID-19 vaccination intentions and attitudes in France. Public Health 2021, 198, 200–207. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Toshkov, D. What Accounts for the Variation in COVID-19 Vaccine Hesitancy in Eastern, Southern and Western Europe? Center for Open Science: Charlottesville, VA, USA, 2022. [Google Scholar] [CrossRef]
- Steinert, J.I.; Sternberg, H.; Prince, H.; Fasolo, B.; Galizzi, M.M.; Büthe, T.; Veltri, G.A. COVID-19 vaccine hesitancy in eight European countries: Prevalence, determinants, and heterogeneity. Sci. Adv. 2022, 8, abm9825. [Google Scholar] [CrossRef]
- Paul, K.T.; Zimmermann, B.M.; Corsico, P.; Fiske, A.; Geiger, S.; Johnson, S.; Kuiper, J.M.; Lievevrouw, E.; Marelli, L.; Prainsack, B.; et al. Anticipating hopes, fears and expectations towards COVID-19 vaccines: A qualitative interview study in seven European countries. SSM Qual. Res. Health 2022, 2, 100035. [Google Scholar] [CrossRef]
- Velikonja, N.K.; Dobrowolska, B.; Stanisavljević, S.; Erjavec, K.; Velikonja, V.G.; Verdenik, I. Attitudes of Nursing Students towards Vaccination and Other Preventive Measures for Limitation of COVID-19 Pandemic: Cross-Sectional Study in Three European Countries. Healthcare 2021, 9, 781. [Google Scholar] [CrossRef]
- Warren, G.W.; Lofstedt, R. COVID-19 vaccine rollout risk communication strategies in Europe: A rapid response. J. Risk Res. 2021, 24, 369–379. [Google Scholar] [CrossRef]
- Wawrzuta, D.; Jaworski, M.; Gotlib, J.; Panczyk, M. What Arguments against COVID-19 Vaccines Run on Facebook in Poland: Content Analysis of Comments. Vaccines 2021, 9, 481. [Google Scholar] [CrossRef]
- Rzymski, P.; Zeyland, J.; Poniedziałek, B.; Małecka, I.; Wysocki, J. The Perception and Attitudes toward COVID-19 Vaccines: A Cross-Sectional Study in Poland. Vaccines 2021, 9, 382. [Google Scholar] [CrossRef]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef]
- Kozak, A.; Nienhaus, A. COVID-19 Vaccination: Status and Willingness to Be Vaccinated among Employees in Health and Welfare Care in Germany. Int. J. Environ. Res. Public Health 2021, 18, 6688. [Google Scholar] [CrossRef]
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5c validated tool: An online survey in 13 Arab countries. PLoS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef]
- Magadmi, R.M.; Kamel, F.O. Beliefs and barriers associated with COVID-19 vaccination among the general population in Saudi Arabia. BMC Public Health 2021, 21, 1438. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- A Qunaibi, E.; Helmy, M.; Basheti, I.; Sultan, I. A high rate of COVID-19 vaccine hesitancy in a large-scale survey on Arabs. eLife 2021, 10, 68038. [Google Scholar] [CrossRef]
- Alzubaidi, H.; Samorinha, C.; Saddik, B.; Saidawi, W.; Abduelkarem, A.R.; Abu-Gharbieh, E.; Sherman, S.M. A mixed-methods study to assess COVID-19 vaccination acceptability among university students in the United Arab Emirates. Hum. Vaccines Immunother. 2021, 17, 4074–4082. [Google Scholar] [CrossRef]
- Kaadan, M.I.; Abdulkarim, J.; Chaar, M.; Zayegh, O.; Keblawi, M.A. Determinants of COVID-19 vaccine acceptance in the Arab world: A cross-sectional study. Glob. Health Res. Policy 2021, 6, 23. [Google Scholar] [CrossRef]
- Albahri, A.H.; Alnaqbi, S.A.; Alshaali, A.O.; Shahdoor, S.M. COVID-19 Vaccine Acceptance in a Sample from the United Arab Emirates General Adult Population: A Cross-Sectional Survey, 2020. Front. Public Health 2021, 9, 614499. [Google Scholar] [CrossRef]
- Ghazy, R.M.; ElHafeez, S.A.; Shaaban, R.; Elbarazi, I.; Abdou, M.S.; Ramadan, A.; Kheirallah, K.A. Determining the Cutoff Points of the 5C Scale for Assessment of COVID-19 Vaccines Psychological Antecedents among the Arab Population: A Multinational Study. J. Prim. Care Commun. Health 2021, 12, 34018891. [Google Scholar] [CrossRef]
- Al-Zalfawi, S.M.; Rabbani, S.I.; Asdaq, S.M.B.; Alamri, A.S.; Alsanie, W.F.; Alhomrani, M.; Mohzari, Y.; Alrashed, A.A.; AlRifdah, A.H.; Almagrabe, T. Public Knowledge, Attitude, and Perception towards COVID-19 Vaccination in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 10081. [Google Scholar] [CrossRef]
- Roberts, C.H.; Brindle, H.; Rogers, N.T.; Eggo, R.M.; Enria, L.; Lees, S. Vaccine Confidence and Hesitancy at the Start of COVID-19 Vaccine Deployment in the UK: An Embedded Mixed-Methods Study. Front. Public Health 2021, 9, 745630. [Google Scholar] [CrossRef]
- Allington, D.; McAndrew, S.; Moxham-Hall, V.; Duffy, B. Coronavirus conspiracy suspicions, general vaccine attitudes, trust and coronavirus information source as predictors of vaccine hesitancy among UK residents during the COVID-19 pandemic. Psychol. Med. 2021, 1–12. [Google Scholar] [CrossRef]
- Bacon, A.M.; Taylor, S. Vaccination Hesitancy and Conspiracy Beliefs in the UK during the SARS-CoV-2 (COVID-19) Pandemic. Int. J. Behav. Med. 2021, 29, 448–455. [Google Scholar] [CrossRef]
- Woolf, K.; McManus, I.C.; A Martin, C.; Nellums, L.B.; Guyatt, A.L.; Melbourne, C.; Bryant, L.; Gogoi, M.; Wobi, F.; Al-Oraibi, A.; et al. Ethnic differences in SARS-CoV-2 vaccine hesitancy in United Kingdom healthcare workers: Results from the UK-REACH prospective nationwide cohort study. Lancet Reg. Health Eur. 2021, 9, 100180. [Google Scholar] [CrossRef]
- Cook, E.J.; Elliott, E.; Gaitan, A.; Nduka, I.; Cartwright, S.; Egbutah, C.; Randhawa, G.; Waqar, M.; Ali, N. Vaccination against COVID-19: Factors That Influence Vaccine Hesitancy among an Ethnically Diverse Community in the UK. Vaccines 2022, 10, 106. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Yu, L.-M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Shanyinde, M.; Harris, V.; Waite, F.; Rosebrock, L.; et al. Effects of different types of written vaccination information on COVID-19 vaccine hesitancy in the UK (OCEANS-III): A single-blind, parallel-group, randomised controlled trial. Lancet Public Health 2021, 6, e416–e427. [Google Scholar] [CrossRef]
- Sonawane, K.; Troisi, C.L.; Deshmukh, A.A. COVID-19 vaccination in the UK: Addressing vaccine hesitancy. Lancet Reg. Health Eur. 2021, 1, 100016. [Google Scholar] [CrossRef]
- Lu, X.; Wang, J.; Hu, L.; Li, B.; Lu, Y. Association between Adult Vaccine Hesitancy and Parental Acceptance of Childhood COVID-19 Vaccines: A Web-Based Survey in a Northwestern Region in China. Vaccines 2021, 9, 1088. [Google Scholar] [CrossRef]
- Gao, X.; Li, H.; He, W.; Zeng, W. COVID-19 Vaccine Hesitancy Among Medical Students: The Next COVID-19 Challenge in Wuhan, China. Disaster Med. Public Health Prep. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Li, Q.; Tarimo, C.S.; Wang, M.; Gu, J.; Wei, W.; Ma, M.; Zhao, L.; Mu, Z.; Miao, Y. COVID-19 Vaccine Hesitancy Among Chinese Population: A Large-Scale National Study. Front. Immunol. 2021, 12, 781161. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Li, X.; Gao, J.; Liu, X.; Mao, Y.; Wang, R.; Zheng, P.; Xiao, Q.; Jia, Y.; Fu, H.; et al. Health Belief Model Perspective on the Control of COVID-19 Vaccine Hesitancy and the Promotion of Vaccination in China: Web-Based Cross-sectional Study. J. Med. Internet Res. 2021, 23, e29329. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Han, B.; Zhao, T.; Liu, H.; Liu, B.; Chen, L.; Xie, M.; Liu, J.; Zheng, H.; Zhang, S.; et al. Vaccination willingness, vaccine hesitancy, and estimated coverage at the first round of COVID-19 vaccination in China: A national cross-sectional study. Vaccine 2021, 39, 2833–2842. [Google Scholar] [CrossRef]
- Jacob, J.; Stephen, S.; Issac, A.; Krishnan, N.; Radhakrishnan, R.V.; Dhandapani, M.; Jose, S.; Sm, A.; Nair, A.S. Determinants of Willingness for COVID-19 Vaccine: Implications for Enhancing the Proportion of Vaccination Among Indians. Cureus 2021, 13, 15271. [Google Scholar] [CrossRef]
- Sharun, K.; Rahman, C.K.F.; Haritha, C.V.; Jose, B.; Tiwari, R.; Dhama, K. COVID-19 Vaccine Acceptance: Beliefs and Barriers Associated with Vaccination among the General Population in India. J. Exp. Biol. Agric. Sci. 2020, 8, S210–S218. [Google Scholar] [CrossRef]
- Jain, J.; Saurabh, S.; Kumar, P.; Verma, M.K.; Goel, A.D.; Gupta, M.K.; Bhardwaj, P.; Raghav, P.R. COVID-19 vaccine hesitancy among medical students in India. Epidemiol. Infect. 2021, 149, 34011421. [Google Scholar] [CrossRef]
- Okubo, T.; Inoue, A.; Sekijima, K. Who Got Vaccinated for COVID-19? Evidence from Japan. Vaccines 2021, 9, 1505. [Google Scholar] [CrossRef]
- Kawata, K.; Nakabayashi, M. Determinants of COVID-19 vaccine preference: A survey study in Japan. SSM Popul. Health. 2021, 15, 100902. [Google Scholar] [CrossRef]
- Askarian, M.; Fu, L.; Taghrir, M.H.; Borazjani, R.; Shayan, Z.; Taherifard, E.; Taherifard, E.; Akbarialiabad, H.; Longtin, Y.; Askarian, A.; et al. Factors Affecting COVID-19 Vaccination Intent among Iranians: COVID-19 Vaccination Acceptance. 3 December 2020. Available online: https://ssrn.com/abstract=3741968 (accessed on 30 June 2022).
- Tahir, M.J.; Saqlain, M.; Tariq, W.; Waheed, S.; Tan, S.H.S.; Nasir, S.I.; Ullah, I.; Ahmed, A. Population preferences and attitudes towards COVID-19 vaccination: A cross-sectional study from Pakistan. BMC Public Health 2021, 21, 34565351. [Google Scholar] [CrossRef]
- Goodwin, R.; Nguyen Luu, L.A.; Wiwattanapantuwong, J.; Kovács, M.; Suttiwan, P.; Levin, Y. Two-TailTwo-Tailed Dogs, Social Unrest and COVID-19 Vaccination: Politics, Hesitancy and Vaccine Choice in Hungary and Thailanded Dogs, Social Unrest and COVID-19 Vaccination: Politics, Hesitancy and Vaccine Choice in Hungary and Thailand. Vaccines 2022, 10, 789. [Google Scholar] [CrossRef]
- Conklin, M. Racial Preferences in COVID-19 Vaccination: Legal and Practical Implications. SSRN Electron. J. 2021, 5, 141. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A systematic review and meta-analysis of acceptability and its predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef]
- Liu, T.; He, Z.; Huang, J.; Yan, N.; Chen, Q.; Huang, F.; Zhang, Y.; Akinwunmi, O.; Akinwunmi, B.; Zhang, C.; et al. A Comparison of Vaccine Hesitancy of COVID-19 Vaccination in China and the United States. Vaccines 2021, 9, 649. [Google Scholar] [CrossRef]
- Nehal, K.R.; Steendam, L.M.; Ponce, M.C.; van der Hoeven, M.; Smit, G.S.A. Worldwide Vaccination Willingness for COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2021, 9, 1071. [Google Scholar] [CrossRef]
- Cai, C.; Woolhandler, S.; Himmelstein, D.U.; Gaffney, A. Trends in Anxiety and Depression Symptoms During the COVID-19 Pandemic: Results from the US Census Bureau’s Household Pulse Survey. J. Gen. Intern. Med. 2021, 36, 1841–1843. [Google Scholar] [CrossRef]
- Morales, D.X.; Morales, S.A.; Beltran, T.F. Racial/Ethnic Disparities in Household Food Insecurity During the COVID-19 Pandemic: A Nationally Representative Study. J. Racial Ethn. Health Disp. 2020, 8, 1300–1314. [Google Scholar] [CrossRef]
- Marsal, D. Introduction to the Analysis of Variance (ANOVA). Stat. Geosci. 1987, 141–143. [Google Scholar] [CrossRef]
- Rees, D. An Introduction to the Analysis of Variance (ANOVA). In Essential Statistics, 4th ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2001; ISBN 9781315273174. [Google Scholar]
- Singh, G. “Analysis of Variance (ANOVA)|Introduction, Types & Techniques,” Analytics Vidhya. 2018. Available online: https://www.analyticsvidhya.com/blog/2018/01/anova-analysis-of-variance/ (accessed on 30 June 2022).
- Armstrong, R. An introduction to analysis of variance (ANOVA) with special reference to data from clinical experiments in optometry. Ophthalm. Physiol. Opt. 2000, 20, 235–241. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Tukey Multiple Comparison test. J. Clin. Nurs. 1999, 8, 299–304. Available online: http://www.blackwellpublishing.com/specialarticles/jcn_8_304.pdf (accessed on 30 June 2022).
- Jafarzadegan, M.; Safi-Esfahani, F.; Beheshti, Z. Combining hierarchical clustering approaches using the PCA method. Exp. Syst. Appl. 2019, 137, 64. [Google Scholar] [CrossRef]
- Yang, W.; Wang, X.; Lu, J.; Dou, W.; Liu, S. Interactive Steering of Hierarchical Clustering. IEEE Trans. Vis. Comput. Graph. 2020, 27, 3953–3967. [Google Scholar] [CrossRef]
- Al-Amer, R.; Maneze, D.; Everett, B.; Montayre, J.; Villarosa, A.R.; Dwekat, E.; Salamonson, Y. COVID-19 vaccination intention in the first year of the pandemic: A systematic review. J. Clin. Nurs. 2021, 31, 62–86. [Google Scholar] [CrossRef]
- Craig, B.M. United States COVID-19 Vaccination Preferences (CVP): 2020 Hindsight. Patient 2021, 14, 309–318. [Google Scholar] [CrossRef]
- Head, K.J.; Kasting, M.L.; Sturm, L.A.; Hartsock, J.A.; Zimet, G.D. A National Survey Assessing SARS-CoV-2 Vaccination Intentions: Implications for Future Public Health Communication Efforts. Sci. Commun. 2020, 42, 698–723. [Google Scholar] [CrossRef]
- Yigit, M.; Ozkaya-Parlakay, A.; Senel, E. Evaluation of COVID-19 Vaccine Refusal in Parents. Pediatr. Infect. Dis. J. 2021, 40, e134–e136. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.L.-Y.; Cheung, A.W.-L.; Yau, P.S.-Y.; Chung, V.C.-H.; Wong, C.H.-L.; Dong, D.; Wong, S.Y.-S.; Yeoh, E.-K. Influence of Vaccination Characteristics on COVID-19 Vaccine Acceptance Among Working-Age People in Hong Kong, China: A Discrete Choice Experiment. Front. Public Health 2021, 9, 793533. [Google Scholar] [CrossRef] [PubMed]
- Petersen, F.; Errore, A.; Karaca-Mandic, P. Lifting Statewide Mask Mandates and COVID-19 Cases. Med. Care 2022, 60, 538–544. [Google Scholar] [CrossRef]
Figure 1.
An overview of the statistical analysis approach implemented in each sociodemographic category: (A) data extracted and translated into a percentage data matrix for the category (e.g., ages); (B) the ANOVA of the data matrix to indicate whether a significant difference in vaccination preference was detected in different groups in the category; (C) Tukey multiple comparisons of paired groups in the category to identify those pairs of groups showing significant differences in their vaccination preference; (D) hierarchical clustering to illustrate the similarities shown in vaccination preference profiles of different groups in the category.
Figure 1.
An overview of the statistical analysis approach implemented in each sociodemographic category: (A) data extracted and translated into a percentage data matrix for the category (e.g., ages); (B) the ANOVA of the data matrix to indicate whether a significant difference in vaccination preference was detected in different groups in the category; (C) Tukey multiple comparisons of paired groups in the category to identify those pairs of groups showing significant differences in their vaccination preference; (D) hierarchical clustering to illustrate the similarities shown in vaccination preference profiles of different groups in the category.
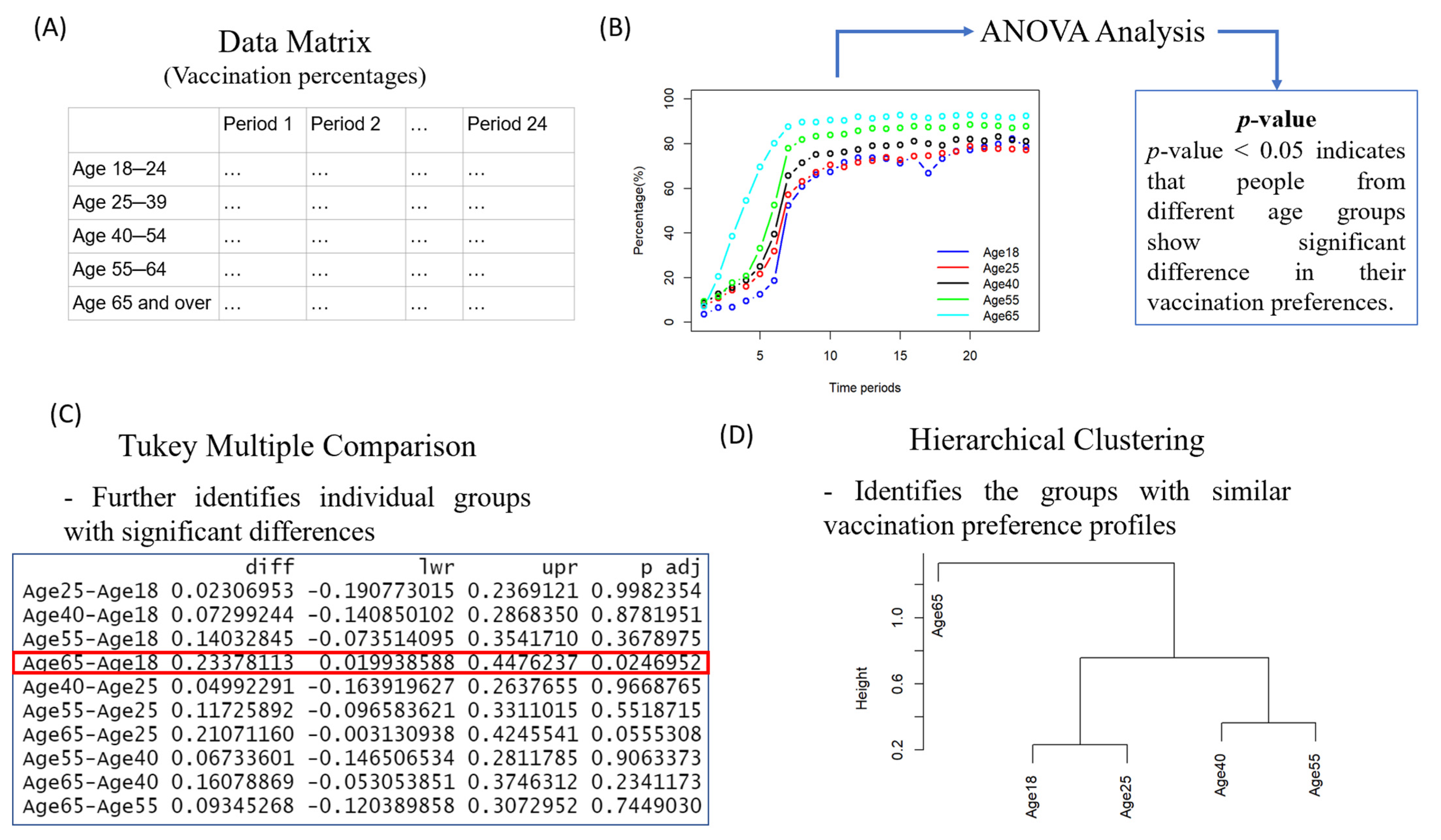
Figure 2.
(A) The historical profiles of vaccination percentages for different age groups; (B) the hierarchical clustering results for different age groups based on their vaccination rates over the sampling periods. One sampling period generally stands for two weeks (started from 6 January 2021). Meaning of legend items: Age18: people at the age of 18 to 24; Age25: people aged 25–39; Age40: people aged 40 to 54; Age55: people aged 55 to 64; Age65: people aged 65 or higher.
Figure 2.
(A) The historical profiles of vaccination percentages for different age groups; (B) the hierarchical clustering results for different age groups based on their vaccination rates over the sampling periods. One sampling period generally stands for two weeks (started from 6 January 2021). Meaning of legend items: Age18: people at the age of 18 to 24; Age25: people aged 25–39; Age40: people aged 40 to 54; Age55: people aged 55 to 64; Age65: people aged 65 or higher.

Figure 3.
(A) The historical profiles of vaccination percentages for groups with different education levels. (B) The hierarchical clustering result for groups with different education levels based on their vaccination rates over sampling periods.
Figure 3.
(A) The historical profiles of vaccination percentages for groups with different education levels. (B) The hierarchical clustering result for groups with different education levels based on their vaccination rates over sampling periods.
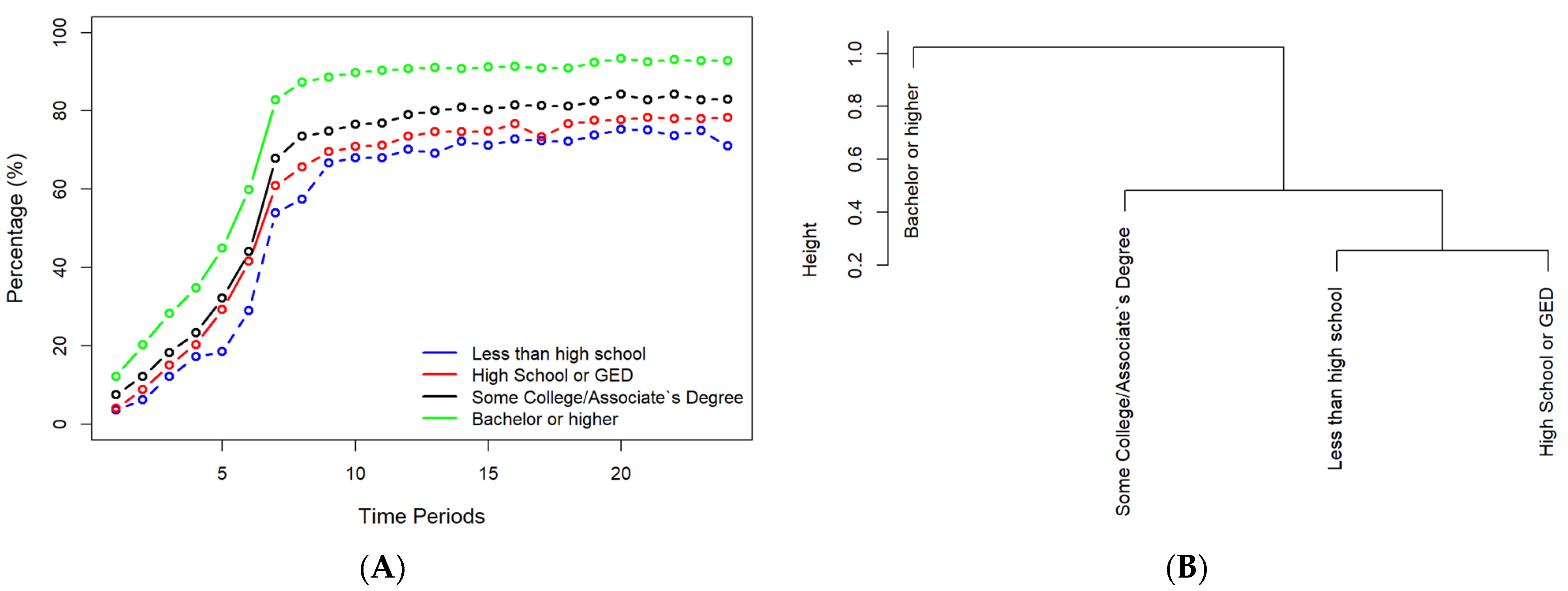
Figure 4.
(A) The historical profiles of vaccination for different racial groups. (B) The hierarchical clustering results for different racial groups based on their vaccination data. Latino: Hispanic or Latino; White: White alone, not Hispanic; Black: Black alone, not Hispanic; Asian: Asian alone, not Hispanic; Others: two or more races + other races, not Hispanic.
Figure 4.
(A) The historical profiles of vaccination for different racial groups. (B) The hierarchical clustering results for different racial groups based on their vaccination data. Latino: Hispanic or Latino; White: White alone, not Hispanic; Black: Black alone, not Hispanic; Asian: Asian alone, not Hispanic; Others: two or more races + other races, not Hispanic.
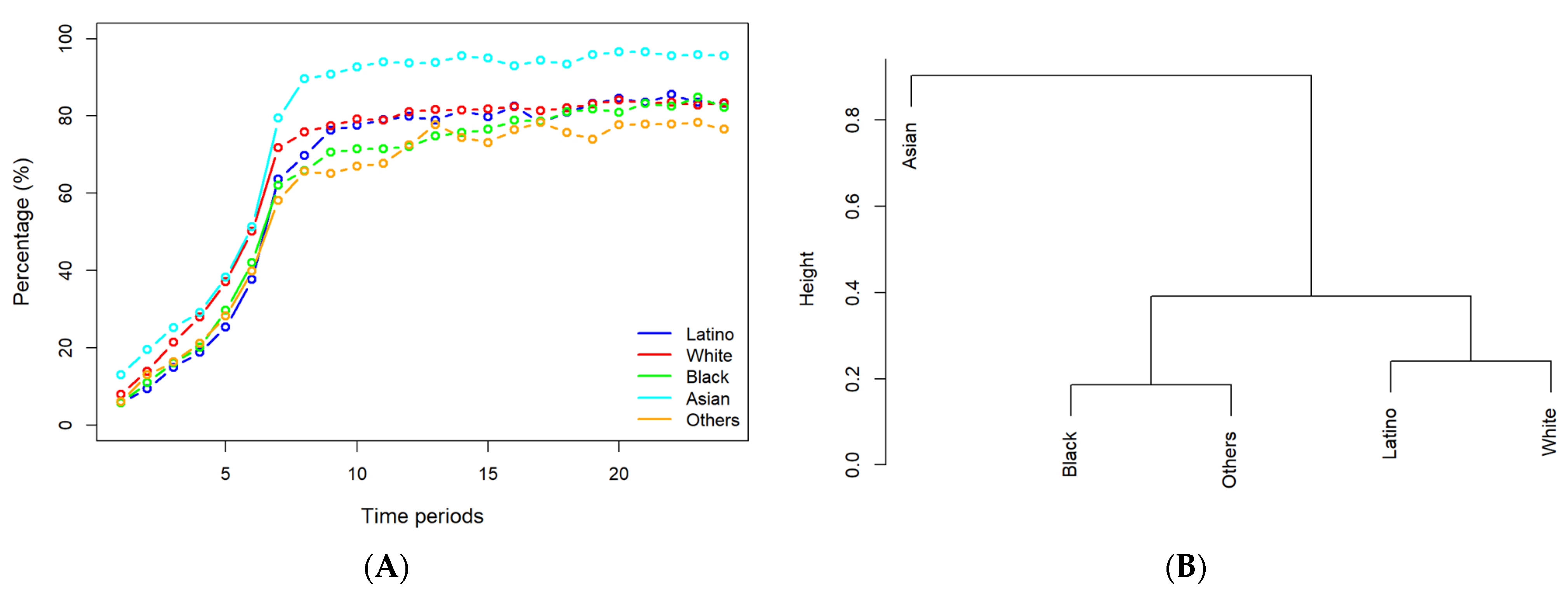
Figure 5.
(A) Historical vaccination profiles by household size, (B) hierarchical clustering of different household sizes by historical vaccination data.
Figure 5.
(A) Historical vaccination profiles by household size, (B) hierarchical clustering of different household sizes by historical vaccination data.
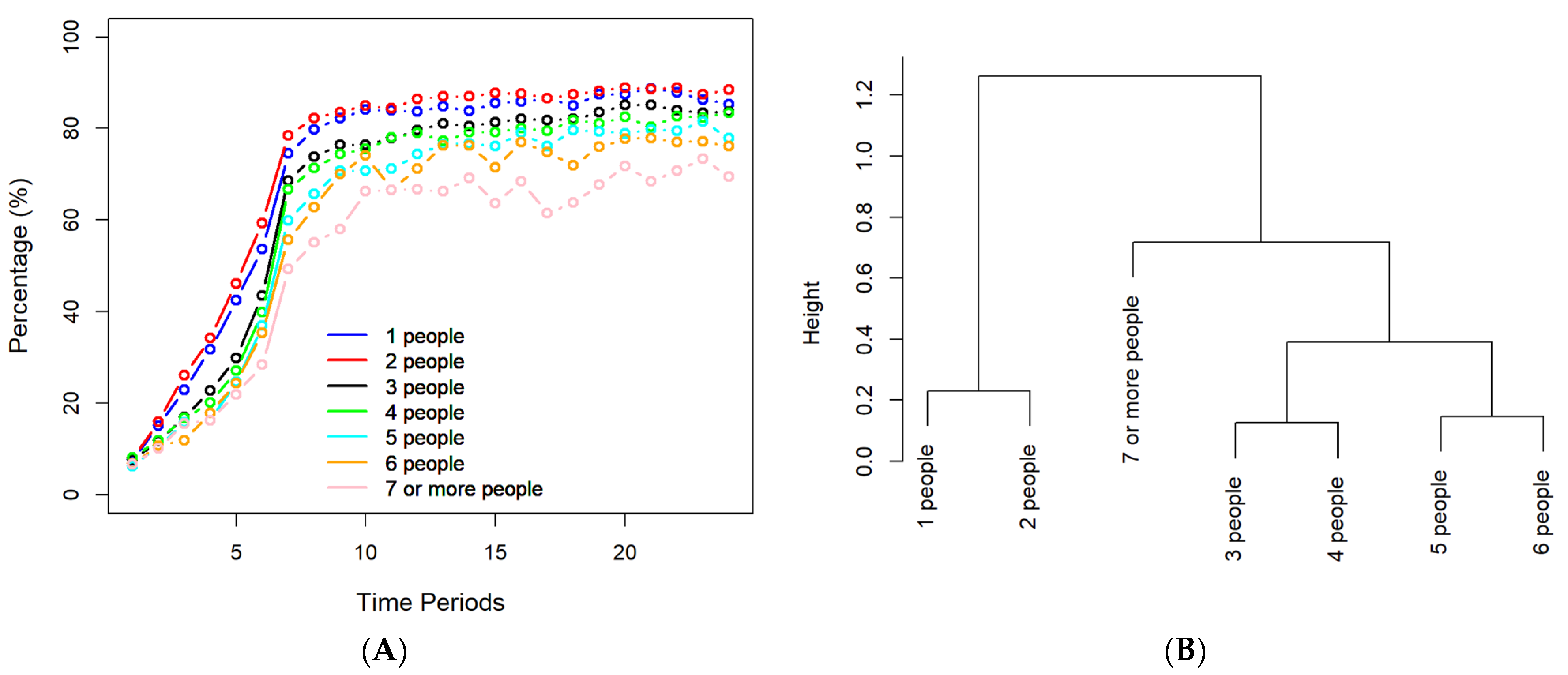
Figure 6.
(A) Historical vaccination data for participants with various marital statuses. (B) The dendrogram obtained through hierarchical clustering for groups with different marital statuses.
Figure 6.
(A) Historical vaccination data for participants with various marital statuses. (B) The dendrogram obtained through hierarchical clustering for groups with different marital statuses.
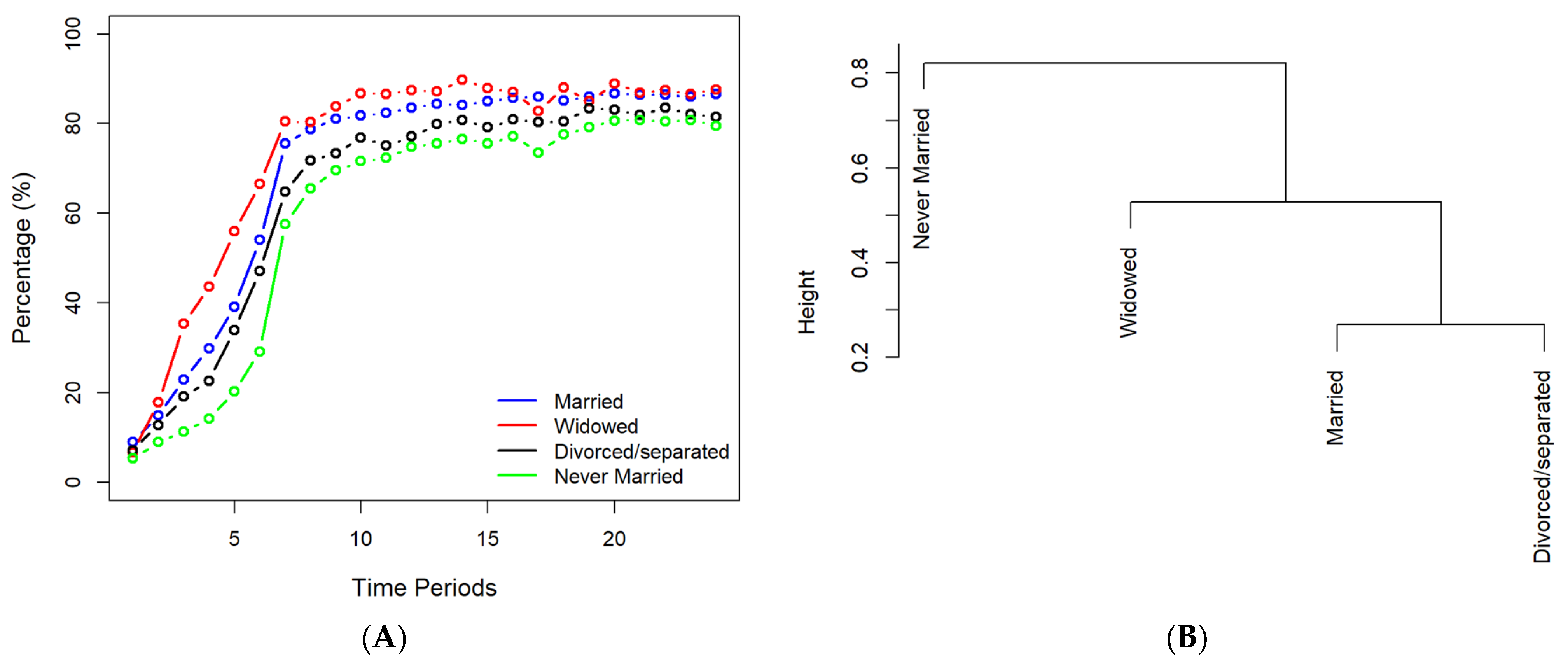
Figure 7.
(A) The historical profiles of vaccination for people with income sources from the last 7 days. (B) A dendrogram obtained through hierarchical clustering based on income resources. RegIncome: regular income sources like those used before the pandemic; Credit or Loans: credit cards or loans; Savings: money from savings or selling assets; Borrow: borrowing from friends or family; UI Benefit: unemployment insurance (UI) benefit payments; Stimulus: stimulus (economic impact) payment; Deferred: money saved from deferred or forgiven payments (to meet spending needs); SNAP: Supplemental Nutrition Assistance Program.
Figure 7.
(A) The historical profiles of vaccination for people with income sources from the last 7 days. (B) A dendrogram obtained through hierarchical clustering based on income resources. RegIncome: regular income sources like those used before the pandemic; Credit or Loans: credit cards or loans; Savings: money from savings or selling assets; Borrow: borrowing from friends or family; UI Benefit: unemployment insurance (UI) benefit payments; Stimulus: stimulus (economic impact) payment; Deferred: money saved from deferred or forgiven payments (to meet spending needs); SNAP: Supplemental Nutrition Assistance Program.
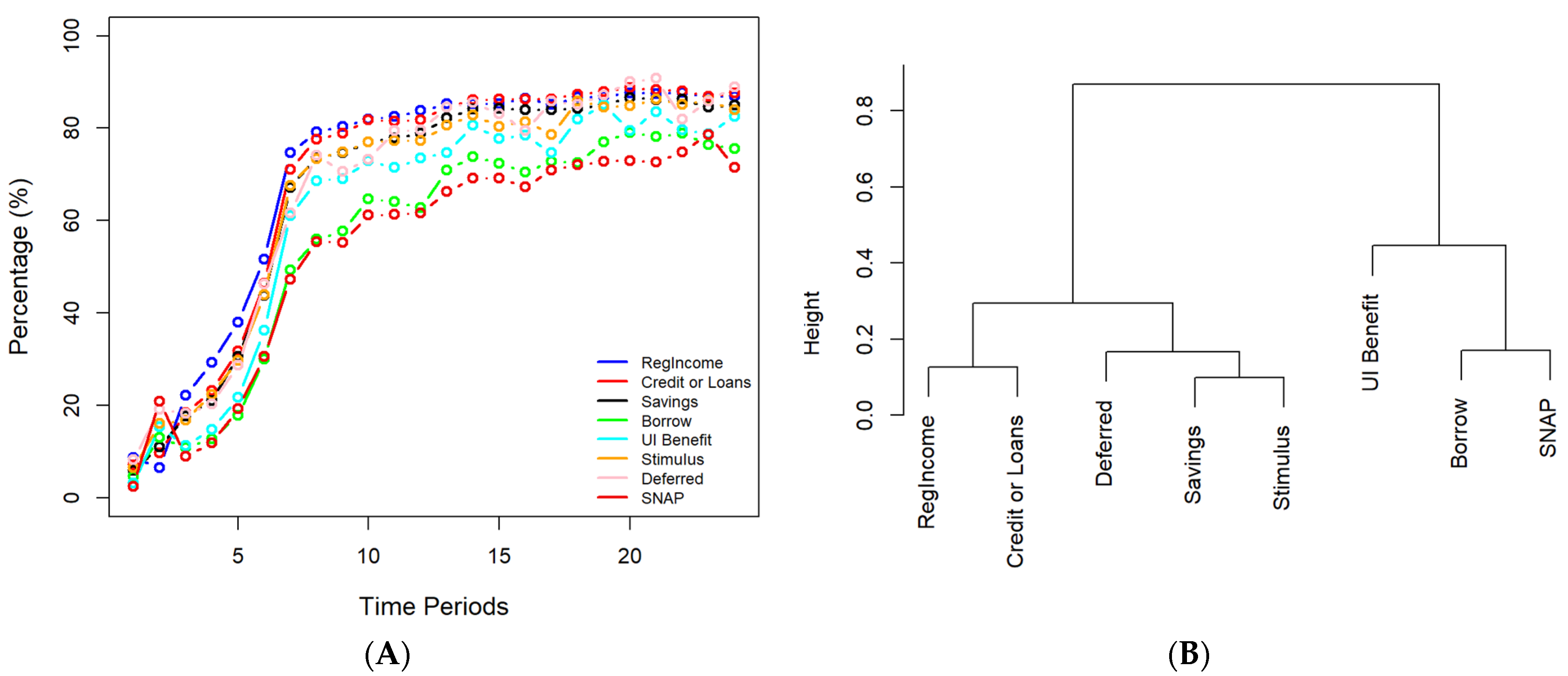
Figure 8.
(A) The historical profiles of vaccination for participants with different household incomes. (B) A dendrogram obtained through hierarchical clustering for participants with different household incomes.
Figure 8.
(A) The historical profiles of vaccination for participants with different household incomes. (B) A dendrogram obtained through hierarchical clustering for participants with different household incomes.

Figure 9.
(A) The historical profiles of vaccination for various genders. (B) The hierarchical clustering for different groups based on their gender.
Figure 9.
(A) The historical profiles of vaccination for various genders. (B) The hierarchical clustering for different groups based on their gender.
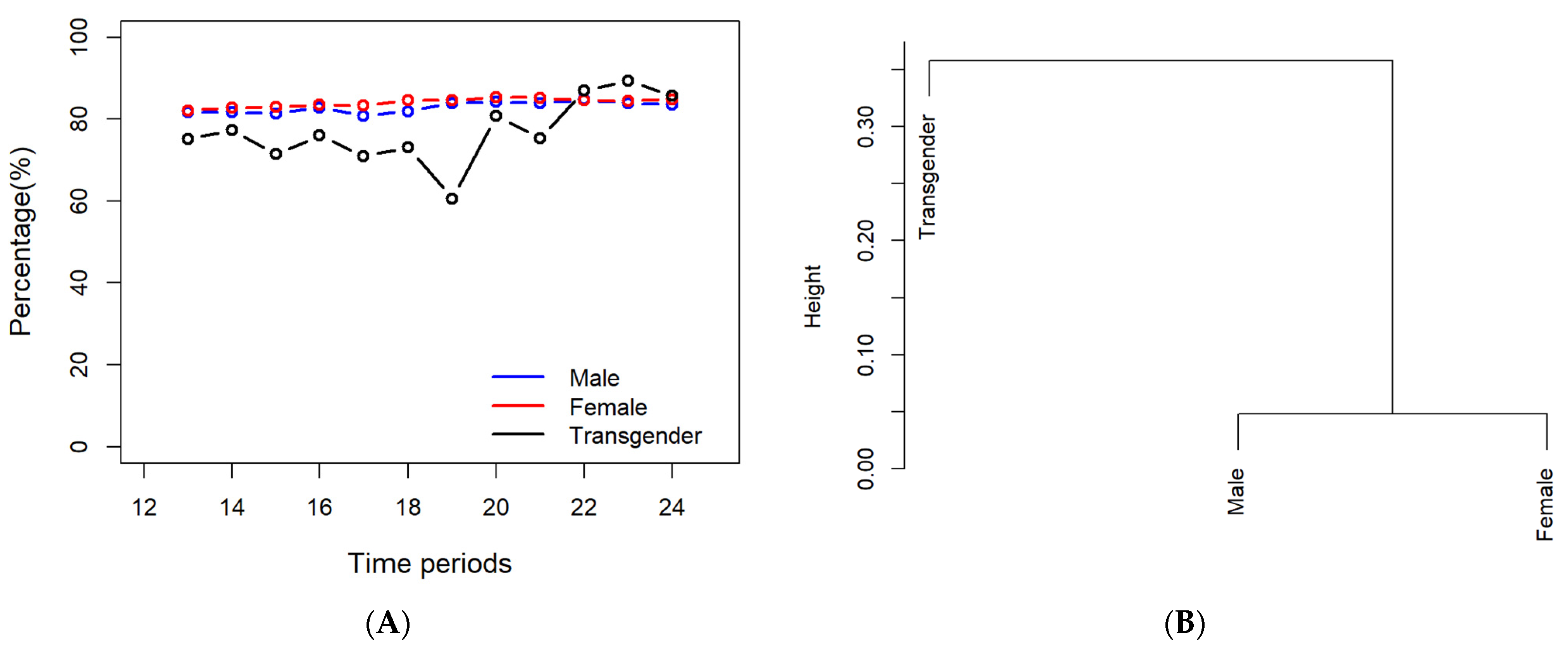
Figure 10.
(A) The historical profiles of vaccination for various genders. (B) The hierarchical clustering for different groups based on their gender.
Figure 10.
(A) The historical profiles of vaccination for various genders. (B) The hierarchical clustering for different groups based on their gender.
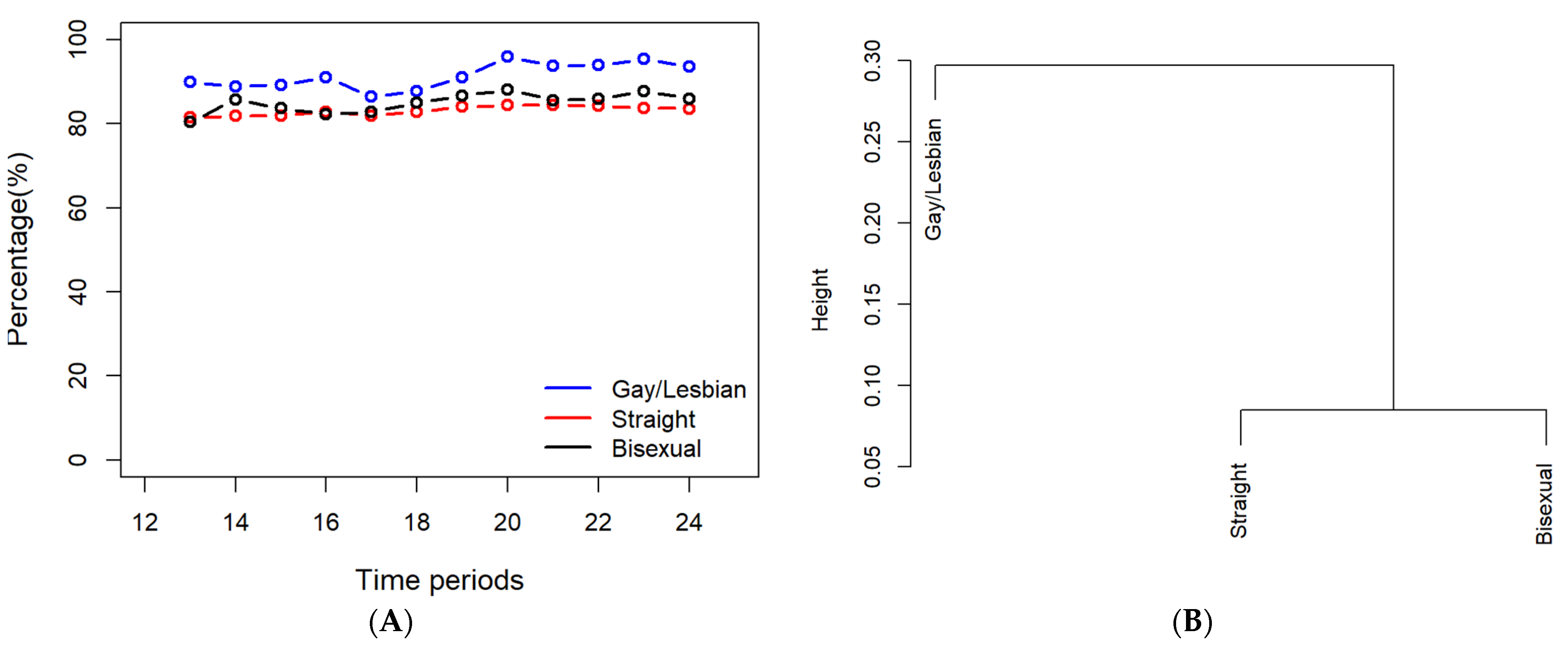
Figure 11.
The historical data for the numbers of non-vaccination cases due to the nine reasons listed in the survey.
Figure 11.
The historical data for the numbers of non-vaccination cases due to the nine reasons listed in the survey.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chen, J.; Chen, A.; Shi, Y.; Chen, K.; Zhao, K.H.; Xu, M.; He, R.; Huang, Z. A Systematic Investigation of American Vaccination Preference via Historical Data. Processes 2022, 10, 1665. https://doi.org/10.3390/pr10081665
AMA Style
Chen J, Chen A, Shi Y, Chen K, Zhao KH, Xu M, He R, Huang Z. A Systematic Investigation of American Vaccination Preference via Historical Data. Processes. 2022; 10(8):1665. https://doi.org/10.3390/pr10081665
Chicago/Turabian StyleChen, Jason, Angie Chen, Youran Shi, Kathryn Chen, Kevin Han Zhao, Morwen Xu, Ricky He, and Zuyi Huang. 2022. "A Systematic Investigation of American Vaccination Preference via Historical Data" Processes 10, no. 8: 1665. https://doi.org/10.3390/pr10081665
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.