
Enhancing Joint Attention Skills in Children on the Autism Spectrum through an Augmented Reality Technology-Mediated Intervention


Abstract
:1. Introduction
1.1. Differences in JA between Non-Autistic and Autistic Children
1.2. Intervention Studies for Enhancing JA Skills in Autistic Children
1.3. Technology-Mediated Intervention Studies for Enhancing JA Skills in Autistic Children
1.4. Augmented Reality
1.5. Purpose of This Study
2. Materials and Methods
2.1. Participants
2.2. Setting and Technology Equipment
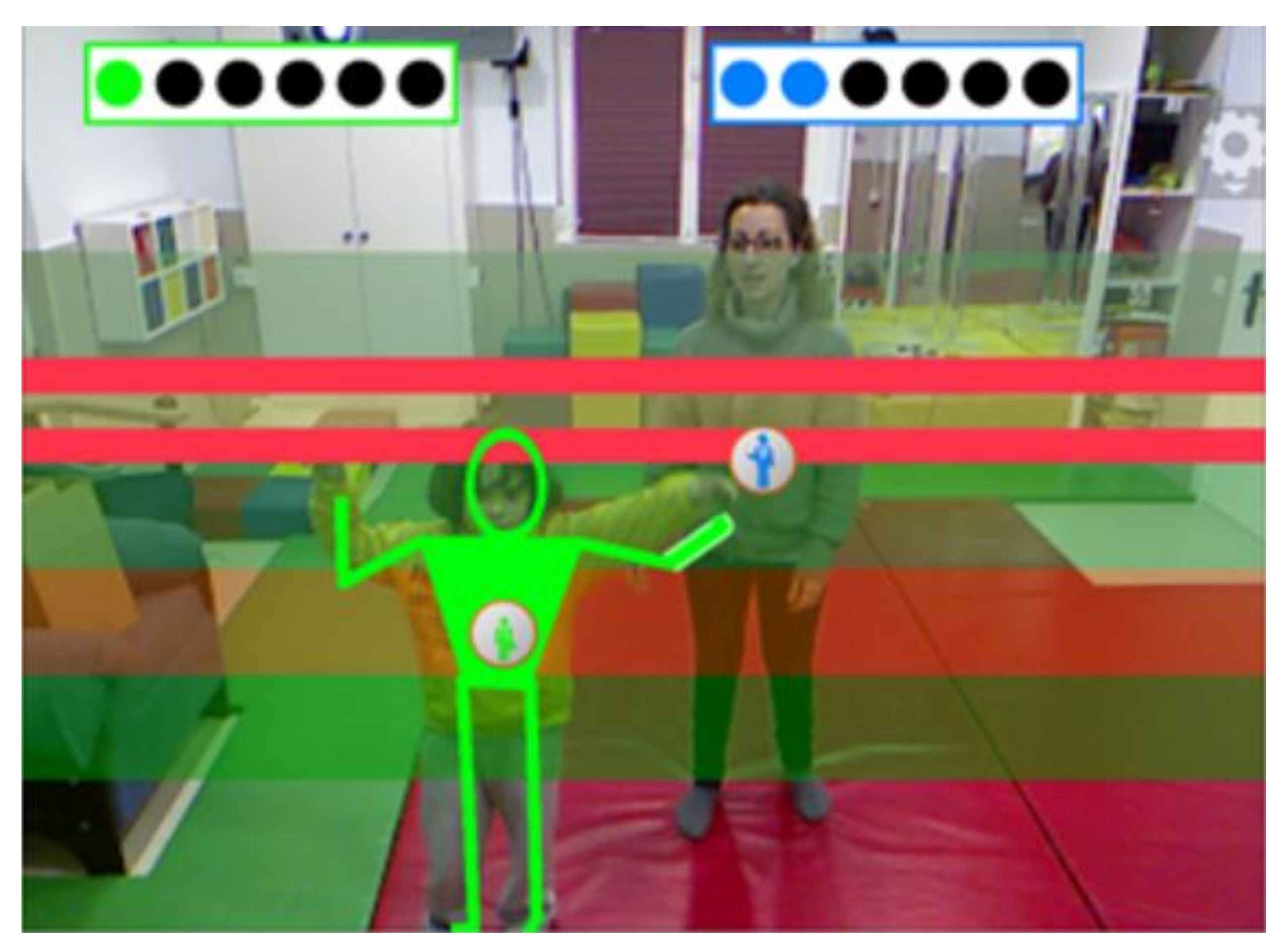
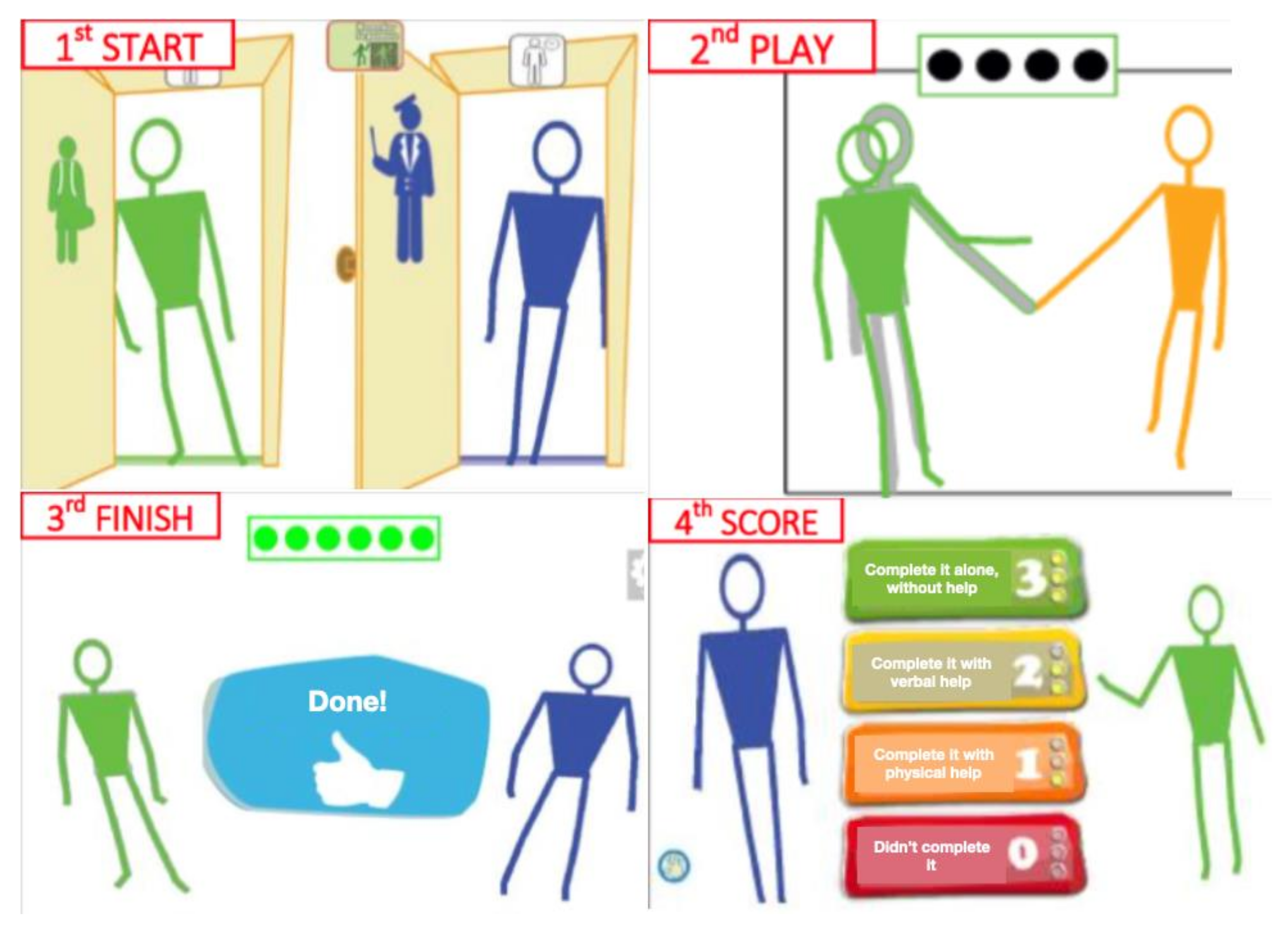
2.3. The Pictogram Room
2.4. Materials
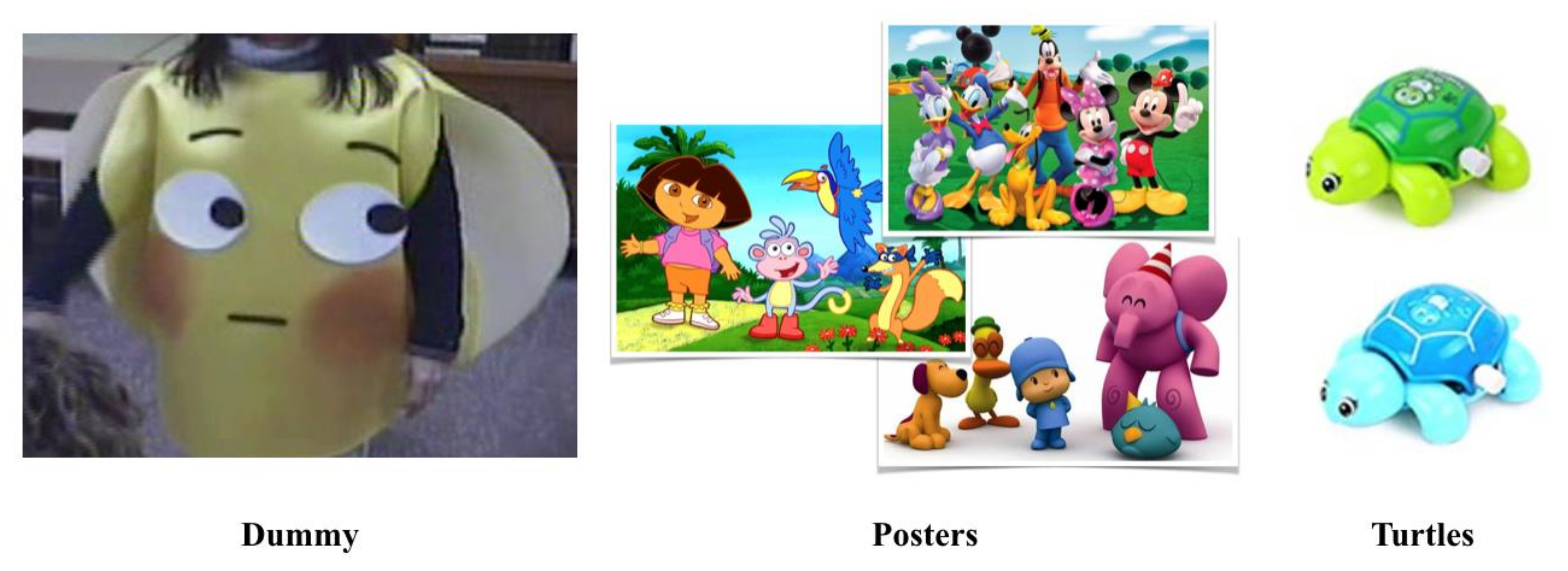
- Which poster is s/he looking at? The researcher and the child sat opposite to each other and the teacher next to or behind the child. The researcher took two posters and positioned them next to her eyes, one on the left and one on the right. Then, she moved her eyes to look at one of them and Teacher A asked: “Which poster is she looking at?”. To obtain a correct response, the child had to point to or take hold of/take away the poster the researcher was looking at. The cartoon characters of the posters were familiar to the children but their favourite ones were not used to avoid impulsive choices based on their preferences. The assessment consisted of 10 trials in which the posters position and the gaze direction were randomly altered.
- Which turtle is s/he looking at? The researcher and the child sat opposite each other and the teacher next to or behind the child. The researcher held two turtles next to her eyes, one on the left and one on the right. Then, she moved her eyes to look at one of them and Teacher A asked: “Which turtle is she looking at?”. To obtain a correct response, the child had to point to or take hold of/take away the turtle the researcher was looking at. The assessment consisted of 10 trials. On the first five trials, the turtles had the same colour (two blue or two green), and on the subsequent five trials they had different colours (one blue and one green). Two same-coloured turtles were used for ensuring that the children did not choose their favourite colour turtle but they selected the target they thought was the correct one.
- Which poster is the dummy looking at? and 4. Which turtle is the dummy looking at? The same procedure as in (1) Which poster is s/he looking at? and (2) Which turtle is s/he looking at? assessments was followed but the researcher wore the dummy costume, the objects were placed next to the dummy’s eyes and she randomly alternated the dummy’s gaze direction. The teacher was the one to ask the child “Which poster is the dummy looking at?” or “Which turtle is the dummy looking at?”.
2.5. Research Design
2.6. Procedures
- Pre-baseline Phase (week 1)
- Baseline Phase (weeks 2–4)
- Learning Phase (weeks 3–5)
- Intervention Phase (weeks 4–7)
- Post-intervention Phase
2.7. Data Preparation and Analysis
2.7.1. Operationalisation of the Measured Variables
2.7.2. Data Analysis
3. Results
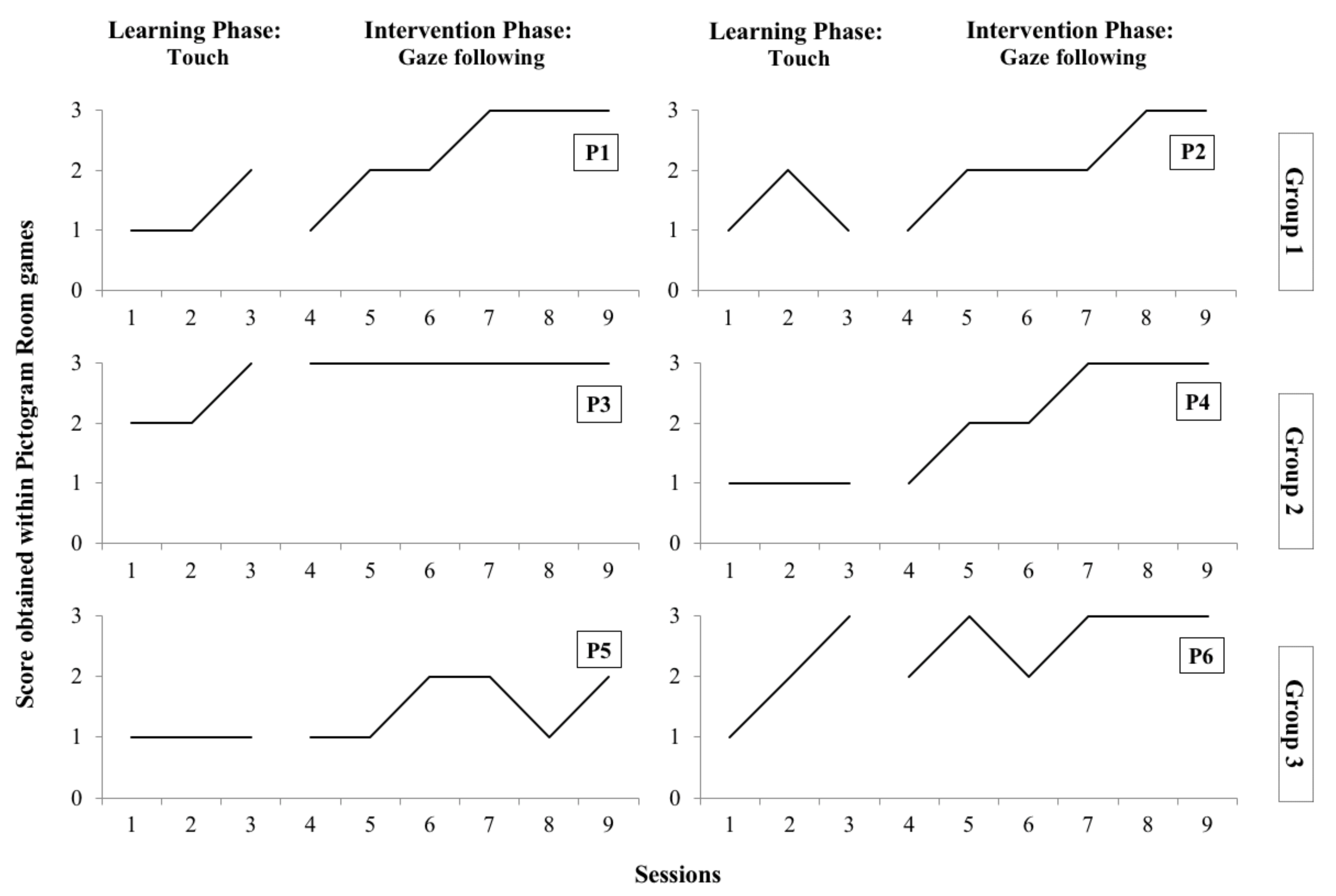
3.1. Participant Improvement within the Pictogram Room Scoring System
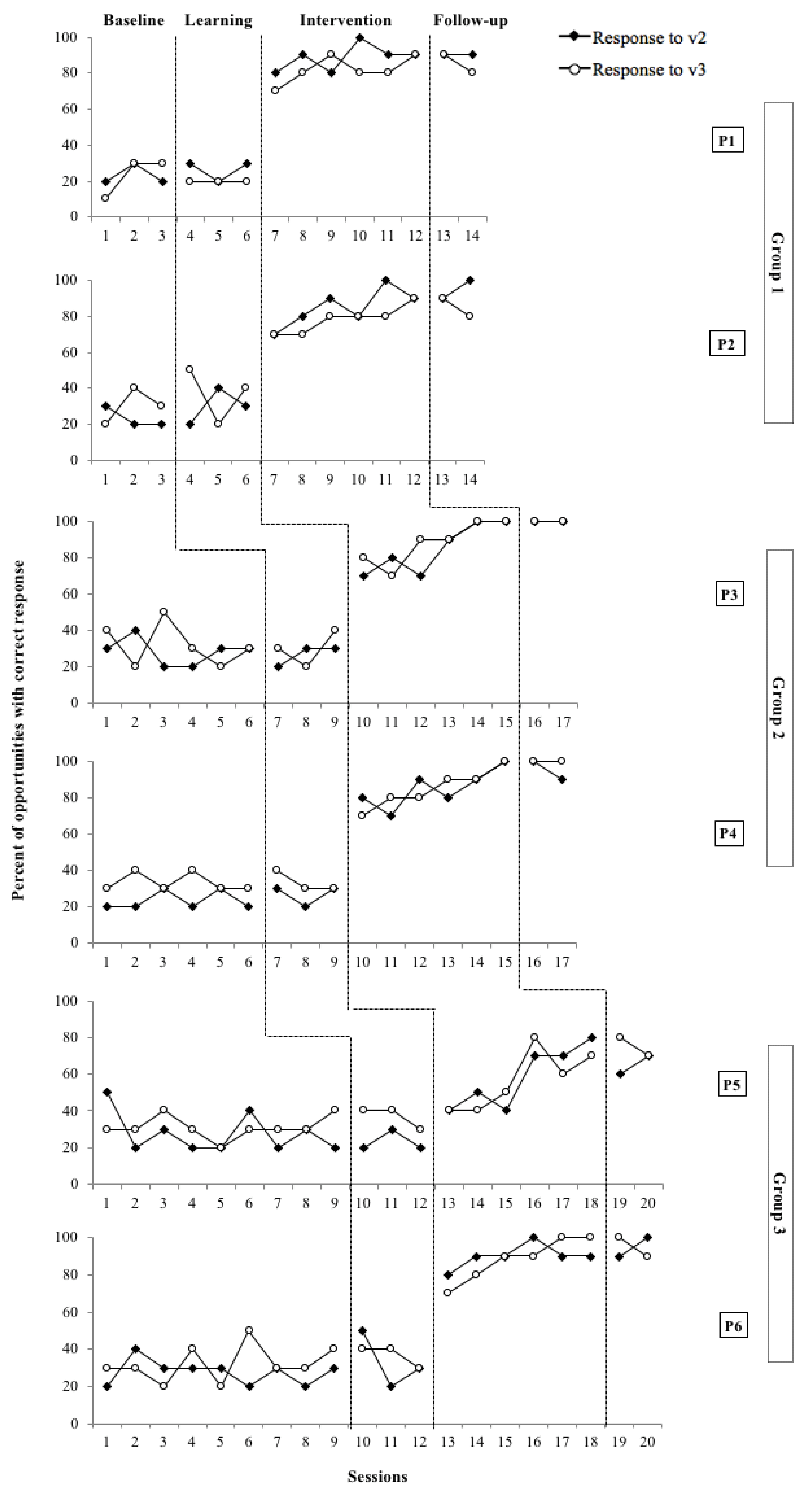
3.2. The Effectiveness of the Intervention in the Participants’ RJA Skills
3.3. Generalisation of the Participants’ RJA Skills
3.4. Research Report Rigour and Strength
4. Discussion
4.1. Findings Summary
4.2. Findings Supporting Previous Studies
4.3. Advantages of the Applied AR-TMI
- Length
- Availability and accessibility
- Ecological validity
- Designing spectrum-comprehensive intervention studies
- Engagement
4.4. Limitations
4.5. Implications for Research and Practice
4.5.1. Previous Experiences and Adaptations Using an AR System
4.5.2. The Meaning of Selecting Appropriate Materials
4.5.3. Using Other Pictogram Room Features and Taking Advantage of New Technology Developments
4.5.4. The Importance of the Setting and the Interventionists
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Charman, T.; Swettenham, J.; Baron-Cohen, S.; Cox, A.; Baird, G.; Drew, A. Infants with autism: An investigation of empathy, pretend play, joint attention, and imitation. Dev. Psychol. 1997, 33, 781–789. [Google Scholar] [CrossRef]
- Charman, T.; Swettenham, J.; Baron-Cohen, S.; Cox, A.; Baird, G.; Drew, A. An experimental investigation of social-cognitive abilities in infants with autism: Clinical implications. Infant Ment. Health J. 1998, 19, 260–275. [Google Scholar] [CrossRef]
- Mundy, P.; Gomes, A. Individual Differences in Joint Attention Skill Development in the Second Year. Infant Behav. Dev. Int. Interdiscip. J. 1998, 21, 469–482. [Google Scholar] [CrossRef]
- Mundy, P.; Newell, L. Attention, Joint Attention, and Social Cognition. Curr. Dir. Psychol. Sci. 2007, 16, 269–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, F.; Butterworth, G. Pointing and Social Awareness: Declaring and Requesting in the Second Year. J. Child Lang. 1996, 23, 307–336. [Google Scholar] [CrossRef] [PubMed]
- Mundy, P.; Crowson, M. Joint Attention and Early Social Communication: Implications for Research on Intervention with Autism. J. Autism Dev. Disord. 1997, 27, 653–676. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R.; Meltzoff, A.N. The Development of Gaze Following and Its Relation to Language. Dev. Sci. 2005, 8, 535–543. [Google Scholar] [CrossRef] [Green Version]
- Leekam, S.R.; Hunnisett, E.; Moore, C. Targets and cues: Gaze-following in children with autism. J. Child Psychol. Psychiatry 1998, 39, 951–962. [Google Scholar] [CrossRef]
- Sigman, M.; Ruskin, E. Continuity and Change in the Social Competence of Children with Autism, Down Syndrome, and Developmental Delays. Monogr. Soc. Res. Child Dev. 1999, 64, v-139. [Google Scholar]
- Frith, U.; Frith, C. The biological basis of social interaction. Curr. Dir. Psychol. Sci. 2001, 10, 151–155. [Google Scholar] [CrossRef]
- Meltzoff, A.N.; Brooks, R. “Like me” as a building block for understanding other minds: Bodily acts, attention, and intention. In Intentions and Intentionality: Foundations of Social Cognition; Malle, B.F., Moses, L.J., Baldwin, D.A., Eds.; The MIT Press: Cambridge, MA, USA, 2001; pp. 171–191. [Google Scholar]
- Tomasello, M. Joint attention as social cognition. In Joint Attention: Its Origins and Role in Development; Dunham, P.J., Moore, C., Eds.; Lawrence Erlbaum Associates: New York, NY, USA, 1995; pp. 103–130. [Google Scholar]
- Baron-Cohen, S. Mindblindness: An Essay on Autism and Theory of Mind; Bradford: Cambridge, MA, USA, 1995. [Google Scholar]
- Charman, T.; Baron-Cohen, S.; Swettenham, J.; Baird, G.; Cox, A.; Drew, A. Testing joint attention, imitation, and play as infancy precursors to language and theory of mind. Cogn. Dev. 2000, 15, 481–498. [Google Scholar] [CrossRef]
- Bakeman, R.; Adamson, L.B. Coordinating Attention to People and Objects in Mother-Infant and Peer-Infant Interaction. Child Dev. 1984, 55, 1278. [Google Scholar] [CrossRef] [Green Version]
- Butterworth, G.; Jarrett, N. What minds have in common is space: Spatial mechanisms serving joint visual attention in infancy. Br. J. Dev. Psychol. 1991, 9, 55. [Google Scholar] [CrossRef]
- Moore, C.; Corkum, V. Infant gaze following based on eye direction. Br. J. Dev. Psychol. 1998, 16, 495–503. [Google Scholar] [CrossRef]
- Morissette, P.; Ricard, M.; Décarie, T.G. Joint visual attention and pointing in infancy: A longitudinal study of comprehension. Br. J. Dev. Psychol. 1995, 13, 163–175. [Google Scholar] [CrossRef]
- Mundy, P.; Sigman, M.D.; Ungerer, J.; Sherman, T. Defining the social deficits of autism: The contribution of non-verbal communication measures. Child Psychol. Psychiatry Allied Discip. 1986, 27, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Mundy, P.; Card, J.; Fox, N. EEG correlates of the development of infant joint attention skills. Dev. Psychobiol. 2000, 36, 325–338. [Google Scholar] [CrossRef]
- Gillespie-Lynch, K.; Elias, R.; Escudero, P.; Hutman, T.; Johnson, S.P. Atypical gaze following in autism: A comparison of three potential mechanisms. J. Autism Dev. Disord. 2013, 43, 2779–2792. [Google Scholar] [CrossRef] [Green Version]
- Mundy, P.; Sigman, M.; Kasari, C. Joint attention, developmental level, and symptom presentation in autism. Dev. Psychopathol. 1994, 6, 389–401. [Google Scholar] [CrossRef]
- Nation, K.; Penny, S. Sensitivity to eye gaze in autism: Is it normal? Is it automatic? Is it social? Dev. Psychopathol. 2008, 20, 79–97. [Google Scholar] [CrossRef]
- Carpenter, M.; Pennington, B.E.; Rogers, S.J. Interrelations among social-cognitive skills in young children with autism. J Autism Dev. Disord. 2002, 32, 91–106. [Google Scholar] [CrossRef] [PubMed]
- Dawson, G.; Meltzoff, A.N.; Osterling, J.; Rinaldi, J.; Brown, E. Children with autism fail to orient to naturally occurring social stimuli. J. Autism Dev. Disord. 1998, 28, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Paparella, T.; Goods, K.S.; Freeman, S.; Kasari, C. The emergence of nonverbal joint attention and requesting skills in young children with autism. J. Commun. Disord. 2011, 44, 569–583. [Google Scholar] [CrossRef]
- Charman, T. Why is joint attention a pivotal skill in autism? In Autism: Mind and Brain; Frith, U., Hill, E., Eds.; Oxford University Press: New York, NY, USA, 2003; pp. 67–87. [Google Scholar]
- Dawson, G.; Toth, K.; Abbott, R.; Osterling, J.; Munson, J.; Estes, A.; Liaw, J. Early Social Attention Impairments in Autism: Social Orienting, Joint Attention, and Attention to Distress. Dev. Psychol. 2004, 40, 271–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales, M.; Mundy, P.; Delgado, C.E.F.; Yale, M.; Messinger, D.; Neal, R.; Schwartz, H.K. Responding to Joint Attention across the 6- through 24-Month Age Period and Early Language Acquisition. J. Appl. Dev. Psychol. 2000, 21, 283–298. [Google Scholar] [CrossRef]
- Gangi, D.N.; Ibañez, L.V.; Messinger, D.S. Joint attention initiation with and without positive affect: Risk group differences and associations with ASD symptoms. J. Autism Dev. Disord. 2014, 44, 1414–1424. [Google Scholar] [CrossRef] [Green Version]
- Mundy, P.C. Autism and Joint Attention: Development, Neuroscience, and Clinical Fundamentals; Guilford Press: New York, NY, USA, 2016; Chapter xviii; 350p. [Google Scholar]
- Whalen, C.; Schreibman, L.; Ingersoll, B. The Collateral Effects of Joint Attention Training on Social Initiations, Positive Affect, Imitation, and Spontaneous Speech for Young Children with Autism. J. Autism Dev. Disord. 2006, 36, 655–664. [Google Scholar] [CrossRef]
- Isaksen, J.; Holth, P. An operant approach to teaching joint attention skills to children with autism. Behav. Interv. 2009, 24, 215–236. [Google Scholar] [CrossRef]
- Martins, M.P.; Harris, S.L. Teaching Children with Autism to Respond to Joint Attention Initiations. Child Fam. Behav. Ther. 2006, 28, 51–68. [Google Scholar] [CrossRef]
- Taylor, B.A.; Hoch, H. Teaching children with autism to respond to and initiate bids for joint attention. J. Appl. Behav. Anal. 2008, 41, 377–391. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.S.; Kasari, C.; Freeman, S.; Paparella, T. The acquisition and generalization of joint attention and symbolic play skills in young children with autism. Res. Pract. Pers. Sev. Disabil. 2007, 32, 101–109. [Google Scholar] [CrossRef]
- Zercher, C.; Hunt, P.; Schuler, A.; Webster, J. Increasing Joint Attention, Play and Language through Peer Supported Play. Autism 2001, 5, 374–398. [Google Scholar] [CrossRef]
- Jones, E.A.; Carr, E.G.; Feeley, K.M. Multiple Effects of Joint Attention Intervention for Children with Autism. Behav. Modif. 2006, 30, 782–834. [Google Scholar] [CrossRef] [PubMed]
- Whalen, C.; Schreibman, L. Joint attention training for children with autism using behavior modification procedures. J. Child Psychol. Psychiatry 2003, 44, 456–468. [Google Scholar] [CrossRef]
- Jones, E.A. Establishing response and stimulus classes for initiating joint attention in children with Autism. Res. Autism Spectr. Disord. 2009, 3, 375–389. [Google Scholar] [CrossRef]
- Rocha, M.L.; Schreibman, L.; Stahmer, A.C. Effectiveness of training parents to teach joint attention in children with autism. J. Early Interv. 2007, 29, 154–172. [Google Scholar] [CrossRef]
- Vismara, L.A.; Lyons, G.L. Using perseverative interests to elicit joint attention behaviors in young children with autism: Theoretical and clinical implications for understanding motivation. J. Posit. Behav. Interv. 2007, 9, 214–228. [Google Scholar] [CrossRef]
- Ferraioli, S.J.; Harris, S.L. Teaching Joint Attention to Children with Autism Through A Sibling-Mediated Behavioral Intervention. Behav. Interv. 2011, 26, 261. [Google Scholar] [CrossRef]
- Pierce, K.; Schreibman, L. Increasing complex social behaviors in children with autism: Effects of peer-implemented pivotal response training. J. Appl. Behav. Anal. 1995, 28, 285–295. [Google Scholar] [CrossRef]
- Ingersoll, B.; Schreibman, L. Teaching Reciprocal Imitation Skills to Young Children with Autism Using a Naturalistic Behavioral Approach: Effects on Language, Pretend Play, and Joint Attention. J. Autism Dev. Disord. 2006, 36, 487–505. [Google Scholar] [CrossRef] [PubMed]
- Ingersoll, B. Effect of a focused imitation intervention on social functioning in children with autism. J. Autism Dev. Disord. 2012, 42, 1768–1773. [Google Scholar] [CrossRef] [Green Version]
- Rogers, S.J.; Dawson, G. Early Start Denver Model for Young Children with Autism: Promoting Language, Learning, and Engagement; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Rogers, S.J.; Hayden, D.; Hepburn, S.; Charlifue-Smith, R.; Hall, T.; Hayes, A. Teaching young nonverbal children with autism useful speech: A pilot study of the Denver model and PROMPT interventions. J. Autism Dev. Disord. 2006, 36, 1007–1024. [Google Scholar] [CrossRef] [Green Version]
- Vismara, L.A.; Rogers, S.J. The Early Start Denver model: A case study of an innovative practice. J. Early Interv. 2008, 31, 91–108. [Google Scholar] [CrossRef]
- Vismara, L.A.; Colombi, C.; Rogers, S.J. Can one hour per week of therapy lead to lasting changes in young children with autism? Autism 2009, 13, 93–115. [Google Scholar] [CrossRef]
- Schertz, H.H.; Odom, S.L. Promoting joint attention in toddlers with autism: A parent-mediated developmental model. J. Autism Dev. Disord. 2007, 37, 1562–1575. [Google Scholar] [CrossRef] [PubMed]
- Schertz, H.H.; Odom, S.L.; Baggett, K.M.; Sideris, J.H. Effects of Joint Attention Mediated Learning for toddlers with autism spectrum disorders: An initial randomized controlled study. Early Child. Res. Q. 2013, 28, 249–258. [Google Scholar] [CrossRef]
- Kasari, C.; Gulsrud, A.C.; Shire, S.Y.; Strawbridge, C. The JASPER Model for Children with Autism: Promoting Joint Attention, Symbolic Play, Engagement, and Regulation; Guilford Publications: New York, NY, USA, 2021. [Google Scholar]
- Gulsrud, A.C.; Hellemann, G.S.; Freeman, S.F.N.; Kasari, C. Two to ten years: Developmental trajectories of joint attention in children with ASD who received targeted social communication interventions. Autism Res. 2014, 7, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Kasari, C.; Freeman, S.; Paparella, T. Joint attention and symbolic play in young children with autism: A randomized controlled intervention study. J. Child Psychol. Psychiatry Allied Discip. 2006, 47, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Kasari, C.; Gulsrud, A.; Freeman, S.; Paparella, T.; Hellemann, G. Longitudinal follow-up of children with autism receiving targeted interventions on joint attention and play. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 487–495. [Google Scholar] [CrossRef] [Green Version]
- Lawton, K.; Kasari, C. Teacher-implemented joint attention intervention: Pilot randomized controlled study for preschoolers with autism. J. Consult. Clin. Psychol. 2012, 80, 687–693. [Google Scholar] [CrossRef]
- Kasari, C.; Gulsrud, A.; Paparella, T.; Hellemann, G.; Berry, K. Randomized comparative efficacy study of parent-mediated interventions for toddlers with autism. J. Consult. Clin. Psychol. 2015, 83, 554–563. [Google Scholar] [CrossRef]
- Kasari, C.; Gulsrud, A.C.; Wong, C.; Kwon, S.; Locke, J. Randomized Controlled Caregiver Mediated Joint Engagement Intervention for Toddlers with Autism. J. Autism Dev. Disord. 2010, 40, 1045–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasari, C.; Lawton, K.; Shih, W.; Barker, T.V.; Landa, R.; Lord, C.; Orlich, F.; King, B.; Wetherby, A.; Senturk, D. Caregiver-mediated intervention for low-resourced preschoolers with autism: An RCT. Pediatrics 2014, 134, e72–e79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasari, C.; Paparella, T.; Freeman, S.; Jahromi, L.B. Language outcome in autism: Randomized comparison of joint attention and play interventions. J. Consult. Clin. Psychol. 2008, 76, 125–137. [Google Scholar] [CrossRef]
- Kasari, C.; Kaiser, A.; Goods, K.; Nietfeld, J.; Mathy, P.; Landa, R.; Murphy, S.; Almirall, D. Communication interventions for minimally verbal children with autism: A sequential multiple assignment randomized trial. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 635–646. [Google Scholar] [CrossRef] [Green Version]
- Shih, W.; Shire, S.; Chang, Y.; Kasari, C. Joint engagement is a potential mechanism leading to increased initiations of joint attention and downstream effects on language: JASPER early intervention for children with ASD. J. Child Psychol. Psychiatry 2021, 62, 1228–1235. [Google Scholar] [CrossRef]
- Cheng, Y.; Huang, R. Using virtual reality environment to improve joint attention associated with pervasive developmental disorder. Res. Dev. Disabil. 2012, 33, 2141–2152. [Google Scholar] [CrossRef] [PubMed]
- Goodrich, M.A.; Colton, M.; Brinton, B.; Fujiki, M.; Atherton, J.A.; Robinson, L.; Ricks, D.; Maxfield, M.H.; Acerson, A. Incorporating a Robot into an Autism Therapy Team. IEEE Intell. Syst. 2012, 27, 52–59. [Google Scholar] [CrossRef]
- Costa, S.; Lehmann, H.; Dautenhahn, K.; Robins, B.; Soares, F. Using a Humanoid Robot to Elicit Body Awareness and Appropriate Physical Interaction in Children with Autism. Int. J. Soc. Robot. 2015, 7, 265–278. [Google Scholar] [CrossRef] [Green Version]
- Tapus, A.; Peca, A.; Aly, A.; Pop, C.; Jisa, L.; Pintea, S.; Rusu, A.S.; David, D.O. Children with autism social engagement in interaction with Nao, an imitative robot: A series of single case experiments. Interact. Stud. Soc. Behav. Commun. Biol. Artif. Syst. 2012, 13, 315–347. [Google Scholar] [CrossRef]
- Warren, Z.E.; Zheng, Z.; Swanson, A.R.; Bekele, E.; Zhang, L.; Crittendon, J.A.; Weitlauf, A.F.; Sarkar, N. Can Robotic Interaction Improve Joint Attention Skills? J. Autism Dev. Disord. 2015, 45, 3726–3734. [Google Scholar] [CrossRef] [Green Version]
- Sani-Bozkurt, S.; Bozkus-Genc, G. Social Robots for Joint Attention Development in Autism Spectrum Disorder: A Systematic Review. Int. J. Disabil. Dev. Educ. 2021; 1–19, ahead-of-print. [Google Scholar] [CrossRef]
- Lee, K. Augmented Reality in Education and Training. TechTrends 2012, 56, 13–21. [Google Scholar] [CrossRef]
- Herrera, G.; Jordan, R.; Vera, L. Agency and presence: A common dependence on subjectivity? Presence-Teleoper. Virtual Environ. 2006, 15, 539–552. [Google Scholar] [CrossRef]
- Parsons, S. Authenticity in Virtual Reality for assessment and intervention in autism: A conceptual review. Educ. Res. Rev. 2016, 19, 138–157. [Google Scholar] [CrossRef] [Green Version]
- Herrera, G.; Jordan, R.; Gimeno, J. Exploring the advantages of augmented reality for intervention in asd. In Proceedings of the 2nd World Autism Congress & Exhibition, Autism Safari, Cape Town, South Africa, 30 October–2 November 2006; pp. 91–110. [Google Scholar]
- Kientz, J.A.; Hayes, G.R.; Goodwin, M.S.; Gelsomini, M.; Abowd, G.D. Interactive Technologies and Autism, 2nd ed.; Synthesis Lectures on Assistive, Rehabilitative, and Health-Preserving Technologies; Morgan & Claypool Publishers: San Rafael, CA, USA, 2020; p. i-229. [Google Scholar]
- Bai, Z.; Blackwell, A.F.; Coulouris, G. Using Augmented Reality to Elicit Pretend Play for Children with Autism. IEEE Trans. Vis. Comput. Graph. 2015, 21, 598–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharya, A.; Gelsomini, M.; Pérez-Fuster, P.; Abowd, G.D.; Rozga, A. Designing motion-based activities to engage students with autism in classroom settings. In Proceedings of the 14th International Conference on Interaction Design and Children, Aarhus, Denmark, 17–20 June 2014; ACM: New York, NY, USA, 2015; pp. 69–78. [Google Scholar]
- Escobedo, L.; Nguyen, D.H.; Boyd, L.; Hirano, S.; Rangel, A.; Garcia-Rosas, D.; Tentori, M.; Hayes, G. MOSOCO: A mobile assistive tool to support children with autism practicing social skills in real-life situations. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Austin, TX, USA, 5–10 May 2012; ACM: New York, NY, USA, 2012; pp. 2589–2598. [Google Scholar]
- Escobedo, L.; Tentori, M.; Quintana, E.; Favela, J.; Garcia-Rosas, D. Using Augmented Reality to Help Children with Autism Stay Focused. MPRV 2014, 13, 38–46. [Google Scholar] [CrossRef]
- Liu, R.; Salisbury, J.P.; Vahabzadeh, A.; Sahin, N.T. Feasibility of an Autism-Focused Augmented Reality Smartglasses System for Social Communication and Behavioral Coaching. Front. Pediatrics 2017, 5, 145. [Google Scholar] [CrossRef] [Green Version]
- Marto, A.; Almeida, H.A.; Gonçalves, A. Using Augmented Reality in Patients with Autism: A Systematic Review. In VipIMAGE 2019; Springer International Publishing: Cham, Switzerland, 2019; pp. 454–463. [Google Scholar]
- Casas, X.; Herrera, G.; Coma, I.; Fernández, M. A Kinect-based Augmented Reality System for Individuals with Autism Spectrum Disorders. In Proceedings of the International Conference on Computer Graphics Theory and Applications (GRAPP), Rome, Italy, 24–26 February 2012; SciTePress Digital Library: Setúbal, Portugal, 2012; pp. 440–446. [Google Scholar]
- Herrera, G.; Casas, X.; Sevilla, J.; Rosa, L.; Pardo, C.; Plaza, J.; Jordan, R.; Le Groux, S. Pictogram Room: Natural Interaction Technologies to Aid in the Development of Children with Autism. Annu. Clin. Health Psychol. 2012, 8, 39–44. [Google Scholar]
- Nadel, J.; Poli, G. Evaluating and training body knowledge in autism via Kinect and Pictogram Room. Enfance 2018, 1, 51–64. [Google Scholar] [CrossRef]
- Mademtzi, M. The use of a Kinect-based technology within the school environment to enhance sensory-motor skills of children with autism. Ph.D. Thesis, University of Birmingham, Birmingham, UK, 2016. [Google Scholar]
- Reichow, B.; Volkmar, F.R.; Cicchetti, D.V. Development of the Evaluative Method for Evaluating and Determining Evidence-Based Practices in Autism. J. Autism Dev. Disord. 2008, 38, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Gilliam, J.E. Gilliam Autism Rating Scale, 2nd ed.; (GARS-2); Western Psychological Services: Torrance, CA, USA, 2006. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5); American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Mesibov, G.B.; Shea, V.; Schopler, E. The TEACCH Approach to Autism Spectrum Disorders; Springer Science + Business Media: New York, NY, USA, 2005; p. 211-vii, 211. [Google Scholar]
- Bondy, A.S.; Frost, L.A. The picture exchange communication system. Focus Autistic Behav. 1994, 9, 1–19. [Google Scholar] [CrossRef]
- Rutter, M.; Bailey, A.; Lord, C. The Social Communication Questionnaire (SCQ); Western Psychological Services: Torrance, CA, USA, 2003. [Google Scholar]
- Roid, G.H.; Miller, L.J. Leiter International Performance Scale, Revised (Leiter-R); Stoelting Co.: Wood Dale, IL, USA, 1997. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S.L. Autism Diagnostic Observation Schedule, 2nd ed.; (ADOS-2); Western Psychological Services: Los Angeles, CA, USA, 2012. [Google Scholar]
- Mundy, P.; Delgado, C.; Block, J.; Venezia, M.; Hogan, A.; Seibert, J. Early Social Communication Scales (ESCS); University of Miami: Coral Gables, FL, USA, 2003. [Google Scholar]
- Kazdin, A.E. Single-case experimental designs in clinical research and practice. New Dir. Methodol. Soc. Behav. Sci. 1982, 13, 33–47. [Google Scholar]
- Leppink, J. Bridging research and practice in health professions education: Single case designs. Asia Pac. Sch. 2022, 7, 109–111. [Google Scholar] [CrossRef]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Parker, R.I.; Hagan-Burke, S.; Vannest, K. Percentage of All Non-Overlapping Data (PAND): An Alternative to PND. J. Spec. Educ. 2007, 40, 194–204. [Google Scholar] [CrossRef] [Green Version]
- Reichow, B. Development, Procedures, and Application of the Evaluative Method for Determining Evidence-Based Practices in Autism. In Evidence-Based Practices and Treatments for Children with Autism; Reichow, B., Doehring, P., Cicchetti, D.V., Volkmar, F.R., Eds.; Springer Science + Business Media: Boston, MA, USA, 2011; pp. 25–39. [Google Scholar]
- Hume, K.; Odom, S. Effects of an Individual Work System on the Independent Functioning of Students with Autism. J. Autism Dev. Disord. 2007, 37, 1166–1180. [Google Scholar] [CrossRef]
- Kossyvaki, L.; Jones, G.; Guldberg, K. The effect of adult interactive style on the spontaneous communication of young children with autism at school. Br. J. Spec. Educ. 2012, 39, 173–184. [Google Scholar] [CrossRef]
- Jordan, R.; Powell, S. Understanding and Teaching Children with Autism; John Wiley & Sons: West Sussex, UK, 1995. [Google Scholar]
- Jackson, L. Freaks, Geeks and Asperger Syndrome: A User Guide to Adolescence; Jessica Kingsley Publishers: London, UK, 2002; 217p. [Google Scholar]
- Jordan, R. Autistic Spectrum Disorders: An Introductory Handbook for Practitioners; David Fulton Publishers: London, UK, 1999. [Google Scholar]
- Nowell, S.W.; Watson, L.R.; Faldowski, R.A.; Baranek, G.T. An initial psychometric evaluation of the joint attention protocol. J. Autism Dev. Disord. 2018, 48, 1932–1944. [Google Scholar] [CrossRef] [PubMed]
- Russell, J. Agency: Its Role in Mental Development; Erlbaum (UK) Taylor & Francis: Oxford, UK, 1996; Chapter x; 326p. [Google Scholar]
- Hobson, R.P. Autism and the Development of Mind; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1993; Chapter x; 246p. [Google Scholar]
- Newbutt, N. Representations of the self in classroom virtual worlds: An autism perspective. In Game-Based Learning: Challenges and Opportunities; Felicia, P., Ed.; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2014; pp. 165–192. [Google Scholar]
- Dawson, G.; Webb, S.J.; McPartland, J. Understanding the Nature of Face Processing Impairment in Autism: Insights from Behavioral and Electrophysiological Studies. Dev. Neuropsychol. 2005, 27, 403–424. [Google Scholar] [CrossRef]
- Nie, G.; Ullal, A.; Zheng, Z.; Swanson, A.R.; Weitlauf, A.S.; Warren, Z.E.; Sarkar, N. An Immersive Computer-Mediated Caregiver-Child Interaction System for Young Children with Autism Spectrum Disorder. TNSRE 2021, 29, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Chong, E.; Chanda, K.; Ye, Z.; Southerland, A.; Ruiz, N.; Jones, R.M.; Rozga, A.; Rehg, J.M. Detecting Gaze Towards Eyes in Natural Social Interactions and Its Use in Child Assessment. In Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies; ACM: New York, NY, USA, 2017; pp. 43:1–43:20. [Google Scholar]
- Ambrose, D.; MacKenzie, D.E.; Ghanouni, P.; Neyedli, H.F. Investigating joint attention in a guided interaction between a child with ASD and therapists: A pilot eye-tracking study. Br. J. Occup. Ther. 2021, 84, 637–646. [Google Scholar] [CrossRef]
- Bogdashina, O. Sensory Perceptual Issues in Autism and Asperger Syndrome: Different Sensory Experiences—Different Perceptual Worlds; Jessica Kingsley Publishers: London, UK, 2003; p. 217. [Google Scholar]
- Schaaf, R.C.; Toth-Cohen, S.; Johnson, S.L.; Outten, G.; Benevides, T.W. The everyday routines of families of children with autism: Examining the impact of sensory processing difficulties on the family. Autism 2011, 15, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Leppink, J.; Pérez-Fuster, P. What is science without replication? Perspect. Med. Educ. 2016, 5, 320–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association Ethical Principles for Medical Research Involving Human Subjects. Clin. Rev. Educ. 2013, 310, 2191–2194. Available online: https://www.wma.net/wp-content/uploads/2016/11/DoH-Oct2013-JAMA.pdf (accessed on 13 January 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant’s Code | Sex | Chronological Age (Years, Months) | DSM-5 (Diagnosis) | GARS-2 | SCQ | Leiter-R (IQ) |
|---|---|---|---|---|---|---|
| P1 | Male | 7, 10 | Autism (Level 3) with intellectual and language impairment | 111 | 15 | 63 |
| P2 | Female | 8, 6 | Autism (Level 3) with intellectual and language impairment | - | 28 | 52 |
| P3 | Male | 6, 7 | Autism (Level 2) with intellectual and language impairment | 81 | 13 | 80 |
| P4 | Male | 5, 1 | Autism (Level 3) with intellectual and language impairment | 96 | 18 | 70 |
| P5 | Male | 5, 5 | Autism (Level 3) with intellectual and language impairment, with ADHD | 98 | 31 | 54 |
| P6 | Male | 3, 6 | Autism (Level 3) with intellectual and language impairment | 87 | 12 | 77 |
| Assessment Tool | Purpose | Forms/Items Used | Scores |
|---|---|---|---|
| The Social Communication Questionnaire (SCQ; [90]) | To confirm the participants’ autism diagnoses and severity levels 1 | The current form of this scale, which focuses on behaviours observed during the most recent three months of a child’s life. | ≥15, highly suggestive of autism |
| The Leiter International Performance Scale, Revised [91] | To get the participants’ intelligence quotient (IQ) scores | The brief version of this non-verbal test, which consists of two main broad areas: Visualisation and Reasoning. | IQ < 85, suggests a below-average cognitive ability; IQ < 70, is highly suggestive of intellectual disability (ID) |
| The Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; [92]) | To measure the participants’ RJA skills | The RJA item of module 1 and the corresponding toy (i.e., remote-controlled toy animal). | Following the ADOS-2 scoring system for this item, scores ranged from 0 (the child used the orientation of the evaluator’s eyes as a cue to look towards the target, without the need for pointing) to 3 (the child did not orient to the object even when the object was activated) |
| The Early Social Communication Scales (ESCS; [93]) | To measure the participants’ RJA skills | The RJA module includes an assessment in which the child sits in a chair in front of the evaluator. Four posters are placed on four different points related to the child’s position: left or right (L/R RJA), and back left or back right (Behind RJA). The evaluator looks at one of the posters and the child should respond by turning his/her head and looking in the same direction as the evaluator. In this study, six trials for L/R RJA and six trials for Behind RJA were performed with each child during each assessment session. | The coefficient between the number of trials in which the child presented RJA and the total number of trials |
| Phases of the Study | Groups (1–3) | Weeks (1–12) | Sessions (1–9) | Assessments | Pictogram Room Games |
|---|---|---|---|---|---|
| Pre-baseline Phase | |||||
| One-off assessments | 1–3 | 1 | 1 | SCQ, Leiter-R | |
| Pre-assessments | 1–3 | 1 | 1 | ADOS-2, ESCS, Which poster is s/he looking at? Which turtle is s/he looking at? | |
| Baseline Phase | 1 | 2 | 3 | Which poster is the dummy looking at? Which turtle is the dummy looking at? | |
| 2 | 2–3 | 6 | |||
| 3 | 2–4 | 9 | |||
| Learning Phase | 1 | 3 | 3 | Which poster is the dummy looking at? Which turtle is the dummy looking at? | Touch |
| 2 | 4 | 3 | |||
| 3 | 5 | 3 | |||
| Intervention Phase | 1 | 4–5 | 6 | Which poster is the dummy looking at? Which turtle is the dummy looking at? | Gaze following |
| 2 | 5–6 | 6 | |||
| 3 | 6–7 | 6 | |||
| Post-intervention Phase | |||||
| Post-assessments | 1–3 | 8 | 1 | ADOS-2, ESCS, Which poster is s/he looking at? Which turtle is s/he looking at? | |
| Follow-up assessments | 1–3 | 12 | 2 | Which poster is the dummy looking at? Which turtle is the dummy looking at? Which poster is s/he looking at? Which turtle is s/he looking at? |
| Variable | Assessment Tool | Assessment Unit | Scoring System | Scoring System Description |
|---|---|---|---|---|
| v1 | Pictogram Room games | General performance | 0–3 | 0 = player did not complete the level game 3 = player completed the level game on his/her own |
| v2 | Which poster is the dummy looking at? | Percentage of correct responses | 0–100% | 0% = 0 correct responses in 10 trials 100% = 10 correct responses in 10 trials |
| v3 | Which turtle is the dummy looking at? | Percentage of correct responses | 0–100% | 0% = 0 correct responses in 10 trials 100% = 10 correct responses in 10 trials |
| v4 | Which poster is s/he looking at? | The proportion of correct responses | 0–1 | 0 = 0 correct responses in 10 trials 1 = 10 correct responses in 10 trials |
| v5 | Which turtle is s/he looking at? | The proportion of correct responses | 0–1 | 0 = 0 correct responses in 10 trials 1 = 10 correct responses in 10 trials |
| v6 | ESCS | L/R RJA Behind RJA | 0–1 | 0 = 0 correct responses in 6 trials 1 = 6 correct responses in 6 trials |
| v7 | ADOS-2 | RJA | 0–3 | 0 = the lowest RJA level 3 = the highest RJA level |
| Participant | V4 | V5 | V6: ESCS | V7: ADOS-2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Poster | Turtle | L/R RJA | Behind RJA | ||||||||||
| Pre | Post | F-Up | Pre | Post | F-Up | Pre | Post | Pre | Post | Pre | Post | ||
| Group 1 | P1 | 0.30 | 00.90 | 0.90 | 0.30 | 1 | 1 | 0.17 | 0.83 | 0 | 0.67 | 2 | 2 |
| P2 | 0.30 | 1 | 1 | 0.20 | 1 | 1 | 0.33 | 0.83 | 0.17 | 0.67 | 2 | 1 | |
| Group 2 | P3 | 0.30 | 1 | 1 | 0.30 | 1 | 1 | 0.67 | 1 | 0.50 | 1 | 1 | 0 |
| P4 | 0.20 | 1 | 0.90 | 0.30 | 0.90 | 0.90 | 0.50 | 0.83 | 0.17 | 0.83 | 2 | 2 | |
| Group 3 | P5 | 0.40 | 0.80 | 0.90 | 0.20 | 0.80 | 0.70 | 0.17 | 0.67 | 0 | 0.33 | 3 | 3 |
| P6 | 0.30 | 1 | 1 | 0.20 | 1 | 1 | 0.33 | 1 | 0.33 | 0.83 | 2 | 1 | |
| IOA | 1 | 1 | 0.97 | 0.92 | |||||||||
| Kappa | 1 | 1 | 0.94 | 0.88 | |||||||||
| Rigour Rating | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Primary Quality Indicators | Secondary Quality Indicators | ||||||||||
| PART | IV | DV | BSLN | VIS AN | EXP CON | IOA | KAP | FID | BR | G/M | SV |
| H | H | H | H | H | H | Y | Y | N | Y | Y | Y |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Fuster, P.; Herrera, G.; Kossyvaki, L.; Ferrer, A. Enhancing Joint Attention Skills in Children on the Autism Spectrum through an Augmented Reality Technology-Mediated Intervention. Children 2022, 9, 258. https://doi.org/10.3390/children9020258
Pérez-Fuster P, Herrera G, Kossyvaki L, Ferrer A. Enhancing Joint Attention Skills in Children on the Autism Spectrum through an Augmented Reality Technology-Mediated Intervention. Children. 2022; 9(2):258. https://doi.org/10.3390/children9020258
Chicago/Turabian StylePérez-Fuster, Patricia, Gerardo Herrera, Lila Kossyvaki, and Antonio Ferrer. 2022. "Enhancing Joint Attention Skills in Children on the Autism Spectrum through an Augmented Reality Technology-Mediated Intervention" Children 9, no. 2: 258. https://doi.org/10.3390/children9020258