Pediatric Integrative Medicine in Residency Program: Relationship between Lifestyle Behaviors and Burnout and Wellbeing Measures in First-Year Residents


 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Measures
2.2. Data Collection and Statistical Analysis
3. Results
3.1. Sample
3.2. Wellbeing Measures
3.3. Lifestyle Behaviors
3.4. Differences between Burnout Risk Groups on Wellbeing and Lifestyle Behaviors
3.5. Relationship between Lifestyle Behaviors and Wellbeing Measures
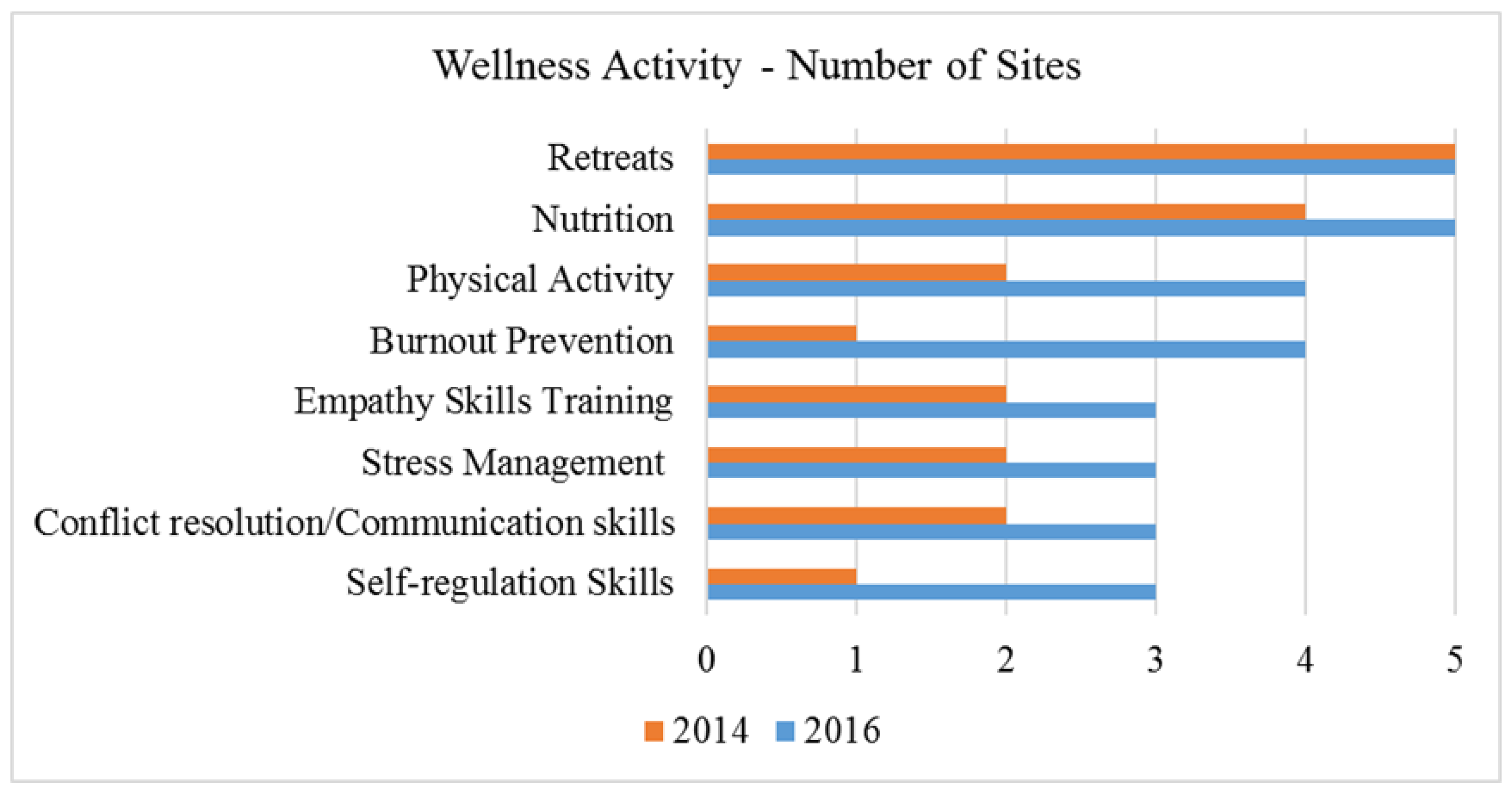
3.6. On-Site Physician Wellness Activities
4. Discussion
Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dyrbye, L.N.; West, C.P.; Satele, D.; Boone, S.; Tan, L.; Sloan, J.; Shanafelt, T.D. Burnout among US medical students, residents, and early career physicians relative to the general US population. Acad. Med. 2014, 89, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.; Shanafelt, T. A narrative review on burnout experienced by medical students and residents. Med. Educ. 2016, 50, 132–149. [Google Scholar] [CrossRef] [PubMed]
- McClafferty, H.; Brown, O.W. Physician health and wellness. Pediatrics 2014, 134, 830–835. [Google Scholar] [CrossRef] [PubMed]
- Pantaleoni, J.L.; Augustine, E.M.; Sourkes, B.M.; Bachrach, L.K. Burnout in pediatric residents over a 2-year period: A longitudinal study. Acad. Pediatr. 2014, 14, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Mahan, J.D. Burnout in pediatric residents and physicians: A call to action. Pediatrics 2017, 139, e20164233. [Google Scholar] [CrossRef] [PubMed]
- Baer, T.E.; Feraco, A.M.; Sagalowsky, S.T.; Williams, D.; Litman, H.J.; Vinci, R.J. Pediatric resident burnout and attitudes toward patients. Pediatrics 2017, 139, e20162163. [Google Scholar] [CrossRef] [PubMed]
- Jennings, M.L.; Slavin, S.J. Resident wellness matters: Optimizing resident education and wellness through the learning environment. Acad. Med. 2015, 90, 1246–1250. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; Dyrbye, L.N.; West, C.P. Addressing physician burnout: The way forward. JAMA 2017, 317, 901–902. [Google Scholar] [CrossRef] [PubMed]
- Accreditation Council for Graduate Medical Education (ACGME). Revised Common Program Requirements, Section VI, The Learning and Working Environment. Available online: https://www.acgmecommon.org/press_release (accessed on 2 March 2017).
- Accreditation Council for Graduate Medical Education (ACGME). Physician Wellbeing. Available online: http://www.acgme.org/What-We-Do/Initiatives/Physician-Well-Being (accessed on 3 February 2017).
- McClafferty, H.; Dodds, S.; Brooks, A.J.; Brenner, M.; Brown, M.; Frazer, P.; Mark, J.; Weydert, J.; Wilcox, G.; Lebensohn, P.; Maizes, V. Pediatric integrative medicine in residency (PIMR): Description of a new online educational curriculum. Children 2015, 2, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Lebensohn, P.; Brooks, A.J.; Chen, M.K. A multi-dimensional integrative health measure to assess wellness behaviors—The Arizona lifestyle inventory. In Proceedings of the International Conference to Promote Resilience, Empathy and Well-Being in Health Care Professions (CENTILE 2017), Washington, DC, USA, 22–25 October 2017. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory, 3rd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Maslach, C.; Jackson, S.E.; Leiter, M. Maslach Burnout Inventory Manual, 4th ed.; Mind Garden Inc.: Menlo Park, CA, USA, 2016. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Pavot, W.; Diener, E. Review of the satisfaction with life scale. Psychol. Assess. 1993, 5, 164–172. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Walach, H.; Buchheld, N.; Buttenmüller, V.; Kleinknecht, N.; Schmidt, S. Measuring mindfulness—The Freiburg mindfulness inventory (FMI). Pers. Individ. Dif. 2006, 40, 1543–1555. [Google Scholar] [CrossRef]
- Davis, M.H. Measuring individual differences in empathy: Evidence for a multidimensional approach. J. Pers. Soc. Psychol. 1983, 44, 113–126. [Google Scholar] [CrossRef]
- Hojat, M.; Mangione, S.; Nasca, T.J.; Cohen, M.J.M.; Gonnella, J.S.; Erdmann, J.B.; Veloski, J.; Magee, M. The Jefferson scale of physician empathy: Development and preliminary psychometric data. Educ. Psychol. Meas. 2001, 61, 349–365. [Google Scholar] [CrossRef]
- Birks, Y.; McKendree, J.; Watt, I. Emotional intelligence and perceived stress in healthcare students: A multi-institutional, multi-professional survey. BMC Med. Educ. 2009, 9, 61. [Google Scholar] [CrossRef] [PubMed]
- Weissman, M.M.; Sholomskas, D.; Pottenger, M.; Prusoff, B.A.; Locke, B.Z. Assessing depressive symptoms in five psychiatric populations: A validation study. Am. J. Epidemiol. 1977, 106, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Lebensohn, P.; Dodds, S.; Brooks, A.J.; Cook, P.; Schneider, C.D.; Woytowicz, J.; Maizes, V. A longitudinal study of well-being, burnout and emotional intelligence in family medicine residents. In Proceedings of the International Research Congress on Integrative Medicine and Health, Miami, FL, USA, 13–16 May 2014. [Google Scholar]
- Bellini, L.M.; Shea, J.A. Mood change and empathy decline persist during three years of internal medicine training. Acad. Med. 2005, 80, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Goebert, D.; Thompson, D.; Takeshita, J.; Beach, C.; Bryson, P.; Ephgrave, K.; Kent, A.; Kunkel, M.; Schechter, J.; Tate, J. Depressive symptoms in medical students and residents: A multischool study. Acad. Med. 2009, 84, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.-M.; Zhang, J.; Steck, S.E.; Cohen, M.J.M.; Gonnella, J.S.; Erdmann, J.B.; Veloski, J.; Magee, M. Obesity mediates the association between Mediterranean diet consumption and insulin resistance and inflammation in US Adults. J. Nutr. 2017, 147, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Chao, A.M.; Jastreboff, A.M.; White, M.A.; Grilo, C.M.; Sinha, R. Stress, cortisol, and other appetite-related hormones: Prospective prediction of 6-month changes in food cravings and weight. Obesity 2017, 25, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Razzoli, M.; Pearson, C.; Crow, S.; Bartolomucci, A. Stress, overeating, and obesity: Insights from human studies and preclinical models. Neurosci. Biobehav. Rev. 2017, 76, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Moutier, C.; Durning, S.J.; Massie, F.S., Jr.; Power, D.V.; Eacker, A.; Harper, W.; Thomas, M.R.; Satele, D.; Sloan, J.A.; Shanafelt, T.D. The problems program directors inherit: Medical student distress at the time of graduation. Med. Teach. 2011, 33, 756–758. [Google Scholar] [CrossRef] [PubMed]
- Daneshvar, F.; Weinreich, M.; Daneshvar, D.; Sperling, M.; Salmane, C.; Yacoub, H.; Gabriels, J.; McGinn, T.; Smith, M.C. Cardiorespiratory fitness in internal medicine residents: Are future physicians becoming deconditioned? J. Grad. Med. Educ. 2017, 9, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.S.; Williams, C.D.; Cronk, N.J.; Kruse, R.L.; Ringdahl, E.N.; Koopman, R.J. Understanding the exercise habits of residents and attending physicians: A mixed methodology study. Fam. Med. 2015, 47, 118–123. [Google Scholar] [PubMed]
- Dyrbye, L.N.; Satele, D.; Shanafelt, T.D. Healthy exercise habits are associated with lower risk of burnout and higher quality of life among US medical students. Acad. Med. 2017, 92, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.M.; Odo, N.U.; Duran, A.M.; Pereira, A.G.; Mandel, J.H. Burnout and physical activity in Minnesota internal medicine resident physicians. J. Grad. Med. Educ. 2014, 6, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Frank, E.; Tong, E.; Lobelo, F.; Carrera, J.; Duperly, J. Physical activity levels and counseling practices of US medical students. Med. Sci. Sports Exerc. 2008, 40, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Leventer-Roberts, M.; Zonfrillo, M.R.; Yu, S.; Dziura, J.D.; Spiro, D.M. Overweight physicians during residency: A cross-sectional and longitudinal study. J. Grad. Med. Educ. 2013, 5, 405–411. [Google Scholar] [CrossRef] [PubMed][Green Version]
- McKenna, K.M.; Hashimoto, D.A.; Maguire, M.S.; Bynum, W.E. The missing link: Connection is the key to resilience in medical education. Acad. Med. 2016, 91, 1197–1199. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Erwin, P.J.; Shanafelt, T.D. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet 2016, 388, 2272–2281. [Google Scholar] [CrossRef]
- Panagioti, M.; Panagopoulou, E.; Bower, P. Controlled interventions to reduce burnout in physicians: A systematic review and meta-analysis. JAMA Intern. Med. 2017, 177, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.; Goh, J.; Sinsky, C. The business case for investing in physician well-being. JAMA Intern. Med. 2017, 177, 1826–1832. [Google Scholar] [CrossRef] [PubMed]
- Heinen, I.; Bullinger, M.; Kocalevent, R.D. Perceived stress in first year medical students—associations with personal resources and emotional distress. BMC Med. Educ. 2017, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.; McBride, R.B.; Hosford, C.C.; Halaas, G. Resilience among medical students: The role of coping style and social support. Teach. Learn. Med. 2016, 28, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Ward, S.; Outram, S. Medicine: In need of culture change. Intern. Med. J. 2016, 46, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Howe, A.; Smajdor, A.; Stockl, A. Towards an understanding of resilience and its relevance to medical training. Med. Educ. 2012, 46, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Frank, E.; Rothenberg, R.; Lewis, C.; Belodoff, B.F. Correlates of physicians’ prevention-related practices. Findings from the Women Physicians’ Health Study. Arch. Fam. Med. 2000, 9, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Frank, E.; Breyan, J.; Elon, L. Physician disclosure of healthy personal behaviors improves credibility and ability to motivate. Arch. Fam. Med. 2000, 9, 287–290. [Google Scholar] [CrossRef] [PubMed]
- McClafferty, H.; Ricker, M.; Brooks, A.J.; Lebensohn, P. Cracking the nut: Wellbeing in training, increasing resilience in both individuals & across healthcare organizations. In Proceedings of the International Conference to Promote Resilience, Empathy and Well-Being in Health Care Professions (CENTILE 2017), Washington, DC, USA, 22–25 October 2017. [Google Scholar]


{kind=link}
| Dimension | Measure | Description |
|---|---|---|
| Perceived stress | Perceived Stress Scale (PSS) [13] | 10 items; scores 0–40 |
| Depression symptoms | Center for Epidemiologic Studies—Depression Scale (CES-D) [14] | 20 items; scores range from 0–60; score of 16 or higher indicates clinical syndrome |
| Burnout | Maslach Burnout Inventory (MBI) [15,16] | 22 items; 3 subscales emotional exhaustion (EE), depersonalization (DEP), personal accomplishment (PA) |
| Life satisfaction | Satisfaction with Life Scale (SWLS) [17,18] | 5 items; higher total scores indicate greater life satisfaction |
| Affect | Positive and Negative Affect Scale (PANAS) [19] | 20 items; 2 subscales positive affect (POS), negative affect (NEG); higher score more positive, more negative affect |
| Mindfulness | Freiberg Mindfulness Inventory (FMI) [20] | 14 items, higher score more mindful |
| Emotional Intelligence | Interpersonal Reactivity Index (IRI) [21] | 21 items; 3 subscales perspective taking (PT), empathic concern (EC), personal distress (PD); higher scores greater perspective taking, empathic concern, personal distress |
| Empathy a | Jefferson Empathy Scale (JES) [22] | 20 items, higher score greater empathy |
| Lifestyle Behaviors | Arizona Lifestyle Inventory [12] | 35 items measuring frequency of diet/nutrition, exercise, mind-body/spiritual practices, social support activities, sleep, hobbies, alcohol consumption behaviors |
| Wellbeing Measures | N | n | Mean (SD)/% Yes | Range | Norm Data |
|---|---|---|---|---|---|
| Perceived stress | 190 | 16.0 (5.9) | 2–31 | 11.9–14.7 1 | |
| CES-D depression | 190 | 12.9 (9.2) | 0–42 | ||
| Non-depressed | 132 | 69.5% | <16 non-depressed | ||
| Clinical depression risk | 58 | 30.5% | ≥16 | ||
| MBI—Emotional exhaustion | 203 | 18.1 (9.0) | 0–54 | 19–26 average | |
| Low emotional exhaustion | 112 | 55.2% | |||
| Moderate emotional exhaustion | 50 | 24.6% | |||
| High emotional exhaustion | 41 | 20.2% | |||
| MBI—Depersonalization | 203 | 7.4 (4.9) | 0–30 | 6–9 average | |
| Low depersonalization | 85 | 41.9% | |||
| Moderate depersonalization | 54 | 26.6% | |||
| High depersonalization | 64 | 31.5% | |||
| MBI—Burnout risk group | |||||
| Low risk | 70 | 34.5% | |||
| Moderate risk | 102 | 50.2% | |||
| High risk | 31 | 15.3% | |||
| MBI—Personal accomplishment | 203 | 29.5 (6.3) | 12–48 | 39–34 average | |
| Satisfaction with life | 203 | 26.4 (5.8) | 5–35 | 26–30 satisfied | |
| PANAS Positive | 174 | 35.2 (6.4) | 10–50 | 35.3 2 | |
| PANAS Negative | 174 | 20.6 (6.0) | 10–42 | 19.6 3 | |
| Mindfulness | 191 | 35.4 (7.1) | 16–54 | 34.52 3, 31.17 4 | |
| IRI Empathic concern | 190 | 21.5 (4.0) | 11–28 | 22.2 5 | |
| IRI Personal distress | 190 | 10.4 (4.9) | 0–25 | 8.9 5 | |
| IRI Perspective taking | 189 | 18.3 (4.3) | 2–28 | 20.6 5 | |
| Jefferson empathy | 174 | 110.7 (14.2) | 79–140 | 118 6 |
| Domain/Items | N | n | Mean/% | SD | Range |
|---|---|---|---|---|---|
| Diet/Nutrition | |||||
| 5 Servings fruits & vegetables | 203 | 3.3 | 2.2 | 0–7 | |
| Eat calcium rich foods | 203 | 4.9 | 2.0 | 0–7 | |
| Eat breakfast | 200 | 5.7 | 1.9 | 0–7 | |
| Eat home cooked dinner | 203 | 4.2 | 2.0 | 0–7 | |
| Drank caffeinated beverages * | 203 | 5.6 | 2.2 | 0–7 | |
| Sugary fluid drinks average day * | 202 | 0.6 | 0.9 | 0–5 | |
| 0 | 122 | 60.4% | |||
| 1 | 61 | 30.2% | |||
| 2 | 8 | 3.9% | |||
| 3 | 9 | 4.5% | |||
| 4 | 1 | 0.5% | |||
| 5 or more | 1 | 0.5% | |||
| Servings high fiber average day | 203 | 2.1 | 1.3 | 0–5 | |
| 0 | 15 | 7.4% | |||
| 1 | 51 | 25.1% | |||
| 2 | 67 | 33.0% | |||
| 3 | 43 | 21.2% | |||
| 4 | 14 | 6.9% | |||
| 5 or more | 13 | 6.4% | |||
| Vegetarian | 188 | 0.07 | 0.25 | 0–1 | |
| Yes | 13 | 6.9% | |||
| Exercise | |||||
| Vigorous physical activity ≥ 10 min | 202 | 1.6 | 1.8 | 0–7 | |
| Moderate physical activity ≥ 10 min | 202 | 2.0 | 2.0 | 0–7 | |
| Moderate physical activity ≥ 30 min | 187 | ||||
| None | 28 | 15.0% | |||
| 1–2 days | 78 | 41.7% | |||
| 3–4 days | 53 | 28.3% | |||
| 5–6 days | 21 | 11.2% | |||
| Everyday | 7 | 3.7% | |||
| Percent sedentary average day * | 198 | ||||
| Less than 5% | 4 | 2.0% | |||
| 6–10% | 8 | 4.0% | |||
| 11–20% | 12 | 6.1% | |||
| 21–30% | 19 | 9.6% | |||
| 31–40% | 25 | 12.6% | |||
| 41–50% | 36 | 18.2% | |||
| 51–60% | 29 | 14.6% | |||
| 61–70% | 31 | 15.7% | |||
| 71–80% | 25 | 12.6% | |||
| 81–90% | 9 | 4.5% | |||
| 91–100% | 0 | 0% | |||
| Mind-Body/Spiritual Practices | |||||
| Activity to relax or manage stress | 202 | 3.3 | 2.4 | 0–7 | |
| Prayer | 202 | 2.3 | 2.8 | 0–7 | |
| Spiritual ritual non-prayer | 202 | 0.6 | 1.7 | 0–7 | |
| Personal reflection | 201 | 1.5 | 2.2 | 0–7 | |
| Breathing for stress reduction | 202 | 0.5 | 1.3 | 0–7 | |
| Progressive muscle relaxation | 191 | 0.2 | 0.8 | 0–7 | |
| Social Support Activities | |||||
| Spend time family/friends | 203 | 4.8 | 2.3 | 0–7 | |
| Receive healthy touch | 203 | 4.4 | 2.6 | 0–7 | |
| Socialize with friends | 202 | 2.1 | 1.6 | 0–7 | |
| Sense of belonging groups | 203 | ||||
| Yes | 150 | 73.9% | |||
| Not sure | 20 | 9.9% | |||
| No | 33 | 16.3% | |||
| Number groups belong | 203 | 1.9 | 1.2 | 0–6 | |
| Sleep | |||||
| Get 7–9 h of sleep | 203 | 3.4 | 2.2 | 0–7 | |
| Wake feeling rested | 201 | 3.0 | 2.1 | 0–7 | |
| Trouble staying asleep * | 201 | 1.4 | 2.0 | 0–7 | |
| Hobbies | 202 | 2.1 | 2.3 | 0–7 | |
| Number of Alcohol Drinks | 200 | 2.8 | 3.0 | 0–15 | |
| Work | |||||
| Enjoy work * | 203 | 4.6 | 1.9 | 0–7 | |
| Feel overwhelmed by work | 203 | 2.6 | 2.2 | 0–7 |
| Wellbeing Measures | Total N * | Low Risk n = 70 | Moderate Risk n = 102 | High Risk n = 31 | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |||
| Perceived Stress | 190 | 12.6 a,c | 5.1 | 16.4 b | 4.9 | 22.7 | 4.4 | <0.001 |
| CES-D Total | 190 | 8.1 a,c | 5.7 | 12.6 b | 8.0 | 25.2 | 8.3 | <0.001 |
| Satisfaction with Life | 203 | 27.9 a | 4.3 | 27.0 b | 5.3 | 21.1 | 7.4 | <0.001 |
| PANAS Positive | 174 | 38.0 a,c | 4.5 | 35.4 b | 6.4 | 28.6 | 4.6 | <0.001 |
| PANAS Negative | 174 | 17.5 a,c | 4.6 | 20.5 b | 5.2 | 27.8 | 4.9 | <0.001 |
| FMI Mindfulness | 191 | 37.6 a | 6.9 | 35.1 b | 7.1 | 31.6 | 6.4 | 0.001 |
| IRI Empathic Concern | 190 | 22.8 a,c | 3.7 | 21.2 | 3.9 | 19.7 | 3.9 | 0.001 |
| IRI Perspective Taking | 189 | 19.5 a | 4.1 | 18.2 b | 3.8 | 15.5 | 5.2 | <0.001 |
| IRI Personal Distress | 190 | 9.3 a | 4.7 | 10.4 | 4.8 | 12.7 | 4.7 | 0.006 |
| Jefferson Empathy | 174 | 115.8 a,c | 13.0 | 110.6 b | 13.2 | 99.2 | 14.1 | <0.001 |
| Lifestyle Behaviors | ||||||||
| Diet/Nutrition | 203 | 0.084 | 0.51 | 0.043 b | 0.40 | −0.20 | 0.62 | 0.048 |
| Exercise d | 203 | 0.045 | 0.7 | 0.053 | 0.7 | −0.25 | 0.6 | 0.095 |
| Mind-body/Spiritual Practices | 203 | 1.6 | 1.2 | 1.4 | 1.0 | 1.1 | 1.1 | 0.13 |
| Social Support Activities d | 203 | 0.018 a | 0.7 | 0.075 b | 0.6 | −0.30 | 0.7 | 0.012 |
| Sleep | 203 | 4.4 a | 1.5 | 4.1 b | 1.4 | 2.9 | 1.3 | <0.001 |
| Hobbies | 202 | 2.3 | 2.6 | 2.0 | 2.1 | 1.8 | 2.1 | 0.56 |
| Alcohol drinks | 200 | 2.5 | 2.7 | 3.2 | 2.9 | 2.5 | 3.6 | 0.32 |
| Work Stress | 203 | 1.7 a,c | 1.1 | 2.6 b | 1.5 | 4.2 | 1.6 | <0.001 |
| Wellbeing Measure | Model Adjusted R2 | Model p-Value | β | t | p-Value |
|---|---|---|---|---|---|
| Perceived stress | 0.39 | <0.001 | |||
| Work stress | 0.50 | 7.95 | <0.001 | ||
| Exercise | −0.19 | −3.35 | 0.001 | ||
| Sleep | −0.16 | −2.45 | 0.015 | ||
| CES-D Total | 0.49 | <0.001 | |||
| Work | 0.47 | 7.80 | <0.001 | ||
| Sleep | −0.23 | −3.93 | <0.001 | ||
| Social | −0.18 | −3.14 | 0.002 | ||
| Exercise | −0.13 | −2.38 | 0.018 | ||
| MBI emotional exhaustion | 0.40 | <0.001 | |||
| Work stress | 0.56 | 9.52 | <0.001 | ||
| Sleep | −0.17 | −2.94 | 0.004 | ||
| MBI Depersonalization | 0.16 | <0.001 | |||
| Work stress | 0.34 | 5.21 | <0.001 | ||
| Diet | −0.20 | −3.09 | 0.002 | ||
| MBI personal accomplishment | 0.18 | <0.001 | |||
| Work Stress | −0.34 | −5.32 | <0.001 | ||
| Exercise | 0.23 | 3.64 | <0.001 | ||
| Satisfaction with life b | 0.26 | <0.001 | |||
| Work stress | −0.36 | −5.65 | <0.001 | ||
| Social | 0.21 | 3.29 | 0.001 | ||
| Diet | 0.16 | 2.60 | 0.010 | ||
| PANAS positive | 0.31 | <0.001 | |||
| Work stress | −0.46 | −7.29 | <0.001 | ||
| Exercise | 0.27 | 4.25 | <0.001 | ||
| PANAS negative | 0.26 | <0.001 | |||
| Work stress | 0.37 | 5.05 | <0.001 | ||
| Exercise | −0.17 | −2.64 | 0.009 | ||
| Sleep | −0.17 | −2.34 | 0.021 | ||
| Mindfulness | 0.20 | <0.001 | |||
| Work stress | −0.27 | −3.95 | <0.001 | ||
| Exercise | 0.25 | 3.66 | <0.001 | ||
| Social | 0.15 | 2.18 | 0.031 | ||
| Hobbies | −0.16 | −2.27 | 0.024 | ||
| Mind-body | 0.14 | 2.01 | 0.046 | ||
| IRI empathic concern c | 0.06 | 0.001 | |||
| Gender | 0.20 | 2.77 | 0.006 | ||
| Social | 0.17 | 2.41 | 0.017 | ||
| IRI perspective taking | 0.064 | 0.001 | |||
| Work stress | −0.20 | −2.76 | 0.006 | ||
| Exercise | 0.18 | 2.47 | 0.014 | ||
| IRI Personal distress | 0.078 | <0.001 | |||
| Exercise | −0.21 | −2.94 | 0.004 | ||
| Work stress | 0.20 | 2.78 | 0.006 | ||
| Hobbies | −0.15 | −1.97 | 0.050 | ||
| Jefferson empathy c | 0.17 | <0.001 | |||
| Gender | 0.29 | 4.11 | <0.001 | ||
| Exercise | 0.26 | 3.72 | <0.001 | ||
| Work stress | −0.17 | −2.47 | 0.009 |
| Lifestyle Behavior | PSS | CES-D | MBI-EE | MBI-DEP | MBI-PA | SWLS | PANAS Positive | PANAS Negative | FMI | IRI EC | IRI PT | IRI PD | JES |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Work Stress | ↑ | ↑ | ↑ | ↑ | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | ↑ | ↓ | |
| Exercise | ↓ | ↓ | ↑ | ↑ | ↓ | ↑ | ↑ | ↓ | ↑ | ||||
| Social Support | ↓ | ↑ | ↑ | ↑ | |||||||||
| Sleep | ↓ | ↓ | ↓ | ↓ | |||||||||
| Diet/Nutrition | ↓ | ↑ | |||||||||||
| Hobbies | ↓ | ↓ | |||||||||||
| Gender | ↑ | ↑ | |||||||||||
| Mind-body/Spiritual | ↓ | ||||||||||||
| Alcohol drinks |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McClafferty, H.; Brooks, A.J.; Chen, M.-K.; Brenner, M.; Brown, M.; Esparham, A.; Gerstbacher, D.; Golianu, B.; Mark, J.; Weydert, J.; et al. Pediatric Integrative Medicine in Residency Program: Relationship between Lifestyle Behaviors and Burnout and Wellbeing Measures in First-Year Residents. Children 2018, 5, 54. https://doi.org/10.3390/children5040054
McClafferty H, Brooks AJ, Chen M-K, Brenner M, Brown M, Esparham A, Gerstbacher D, Golianu B, Mark J, Weydert J, et al. Pediatric Integrative Medicine in Residency Program: Relationship between Lifestyle Behaviors and Burnout and Wellbeing Measures in First-Year Residents. Children. 2018; 5(4):54. https://doi.org/10.3390/children5040054
Chicago/Turabian StyleMcClafferty, Hilary, Audrey J. Brooks, Mei-Kuang Chen, Michelle Brenner, Melanie Brown, Anna Esparham, Dana Gerstbacher, Brenda Golianu, John Mark, Joy Weydert, and et al. 2018. "Pediatric Integrative Medicine in Residency Program: Relationship between Lifestyle Behaviors and Burnout and Wellbeing Measures in First-Year Residents" Children 5, no. 4: 54. https://doi.org/10.3390/children5040054
APA StyleMcClafferty, H., Brooks, A. J., Chen, M.-K., Brenner, M., Brown, M., Esparham, A., Gerstbacher, D., Golianu, B., Mark, J., Weydert, J., Yeh, A. M., & Maizes, V. (2018). Pediatric Integrative Medicine in Residency Program: Relationship between Lifestyle Behaviors and Burnout and Wellbeing Measures in First-Year Residents. Children, 5(4), 54. https://doi.org/10.3390/children5040054