

Association between Diabetes and Levels of Micronutrients in Qatar—A Case–Control Study
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Design, Population, and Setting
2.2. Data Collection
2.3. Diabetes Measurements
2.4. Micro- and Macroelements and Vitamin Measurements
2.5. Ethics and Informed Consent
2.6. Data Analysis
3. Results
3.1. Characteristics of Participants by Diabetes Status
3.2. Comparison of Characteristics by Controlled Diabetes Status
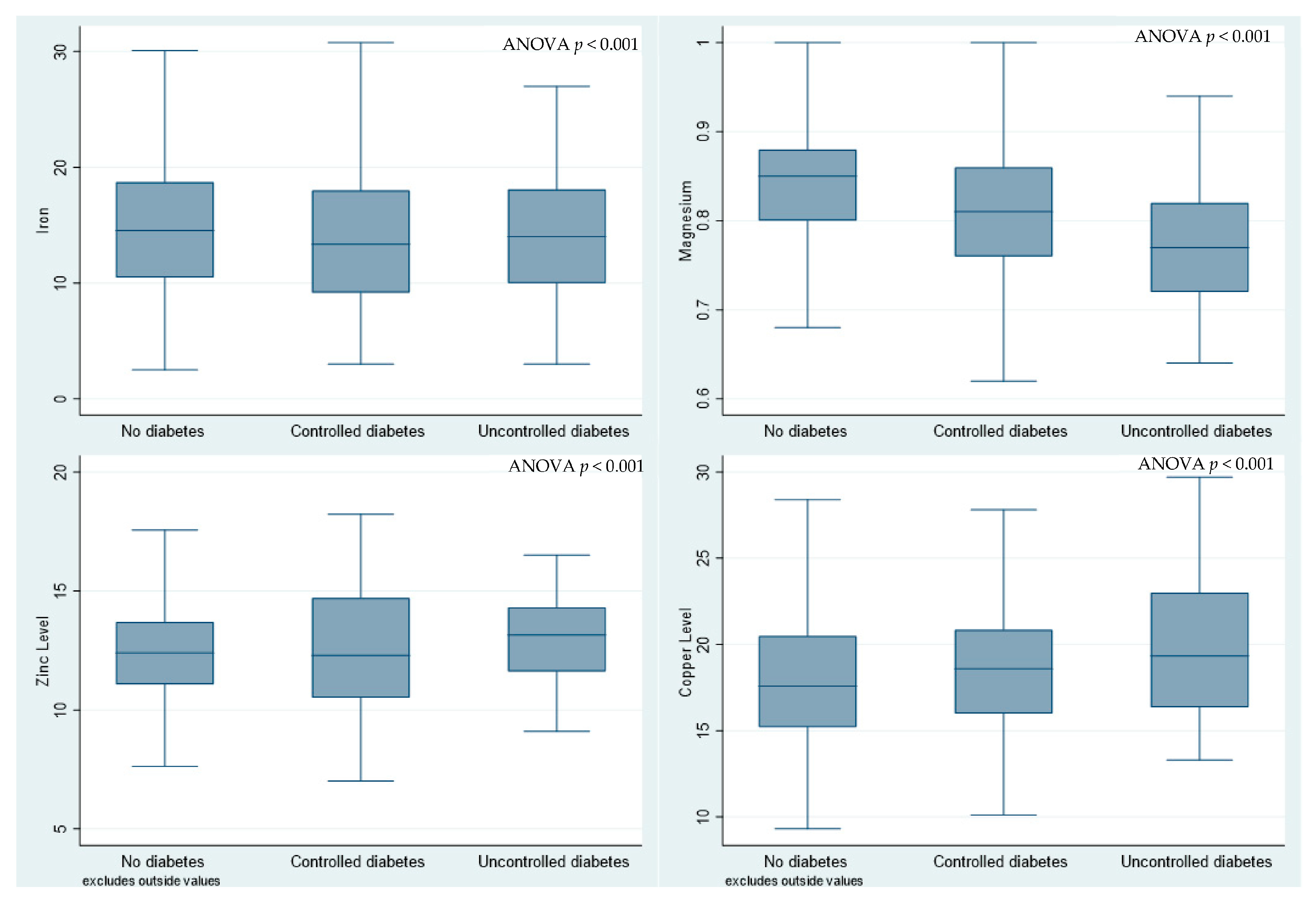
3.3. Comparison of Micronutrient Levels between Participants with and without Diabetes
3.4. Association between Diabetes and Micronutrients—Multivariable Logistic Regression
3.5. Association between Micronutrients and Controlled Diabetes—Multivariable Multinomial Logistic Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Magliano, D.J.; Boyko, E.J. IDF Diabetes Atlas 10th Edition Scientific Committee. IDF Diabetes Atlas; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Wang, H.; Li, N.; Chivese, T.; Werfalli, M.; Sun, H.; Yuen, L.; Hoegfeldt, C.A.; Elise Powe, C.; Immanuel, J.; Karuranga, S.; et al. IDF Diabetes Atlas: Estimation of Global and Regional Gestational Diabetes Mellitus Prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabetes Res. Clin. Pract. 2022, 183, 109050. [Google Scholar] [CrossRef] [PubMed]
- Chivese, T.; Hoegfeldt, C.A.; Werfalli, M.; Yuen, L.; Sun, H.; Karuranga, S.; Li, N.; Gupta, A.; Immanuel, J.; Divakar, H.; et al. IDF Diabetes Atlas: The prevalence of pre-existing diabetes in pregnancy—A systematic reviewand meta-analysis of studies published during 2010–2020. Diabetes Res. Clin. Pract. 2022, 183, 109049. [Google Scholar] [CrossRef] [PubMed]
- Chivese, T.; Werfalli, M.M.; Magodoro, I.; Chinhoyi, R.L.; Kengne, A.P.; Norris, S.A.; Levitt, N.S. Prevalence of type 2 diabetes mellitus in women of childbearing age in Africa during 2000–2016: A systematic review and meta-analysis. BMJ Open 2019, 9, e024345. [Google Scholar] [CrossRef]
- Taylor, R.; Al-Mrabeh, A.; Sattar, N. Understanding the mechanisms of reversal of type 2 diabetes. Lancet. Diabetes Endocrinol. 2019, 7, 726–736. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.B.; le Roux, C.W.; Rubino, F.; Zimmet, P. Bariatric surgery for type 2 diabetes. Lancet 2012, 379, 2300–2311. [Google Scholar] [CrossRef] [PubMed]
- Sanjeevi, N.; Freeland-Graves, J.; Beretvas, S.N.; Sachdev, P.K. Trace element status in type 2 diabetes: A meta-analysis. J. Clin. Diagn. Res. 2018, 12, OE01–OE08. [Google Scholar] [CrossRef]
- Pazirandeh, S.; Burns, D.; Griffin, U. Overview of Dietary Trace Elements; UpToDate: Waltham, MA, USA, 2020. [Google Scholar]
- Siddiqui, K.; Bawazeer, N.; Joy, S.S. Variation in macro and trace elements in progression of type 2 diabetes. Sci. World J. 2014, 2014, 461591. [Google Scholar] [CrossRef]
- Takaya, J.; Higashino, H.; Kobayashi, Y. Intracellular magnesium and insulin resistance. Magnes. Res. 2004, 17, 126–136. [Google Scholar]
- Von Hurst, P.R.; Stonehouse, W.; Coad, J. Vitamin D supplementation reduces insulin resistance in South Asian women living in New Zealand who are insulin resistant and vitamin D deficient—A randomised, placebo-controlled trial. Br. J. Nutr. 2010, 103, 549–555. [Google Scholar] [CrossRef]
- Valdés-Ramos, R.; Guadarrama-López, A.L.; Martínez-Carrillo, B.E.; Benítez-Arciniega, A.D. Vitamins and type 2 diabetes mellitus. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 54–63. [Google Scholar] [CrossRef]
- Akbari, M.; Tabrizi, R.; Lankarani, K.B.; Heydari, S.T.; Karamali, M.; Kashanian, M.; Keneshlou, F.; Niknam, K.; Kolahdooz, F.; Asemi, Z. The Effects of Folate Supplementation on Diabetes Biomarkers Among Patients with Metabolic Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Horm. Metab. Res. 2018, 50, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Xun, P.; Bae, J.C.; Kim, J.H.; Kim, D.J.; Yang, K.; He, K. Circulating calcium levels and the risk of type 2 diabetes: A systematic review and meta-analysis. Br. J. Nutr. 2019, 122, 376–387. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.V.; Schooling, C.M.; Zhao, J.X. The effects of folate supplementation on glucose metabolism and risk of type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Ann. Epidemiol. 2018, 28, 249–257.e241. [Google Scholar] [CrossRef] [PubMed]
- Zainel, A.A.L.; Qotba, H.; Al Nuaimi, A.; Syed, M. Vitamin D status among adults (18–65 years old) attending primary healthcare centres in Qatar: A cross-sectional analysis of the Electronic Medical Records for the year 2017. BMJ Open 2019, 9, e029334. [Google Scholar] [CrossRef]
- Al Thani, A.; Fthenou, E.; Paparrodopoulos, S.; Al Marri, A.; Shi, Z.; Qafoud, F.; Afifi, N. Qatar Biobank Cohort Study: Study Design and First Results. Am. J. Epidemiol. 2019, 188, 1420–1433. [Google Scholar] [CrossRef]
- Al Kuwari, H.; Al Thani, A.; Al Marri, A.; Al Kaabi, A.; Abderrahim, H.; Afifi, N.; Qafoud, F.; Chan, Q.; Tzoulaki, I.; Downey, P.; et al. The Qatar Biobank: Background and methods. BMC Public Health 2015, 15, 1208. [Google Scholar] [CrossRef]
- 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S15–S33. [CrossRef]
- UpToDate. Laboratory Test Normal Reference Ranges in Adults; UpToDate: Waltham, MA, USA, 2020. [Google Scholar]
- World Medical Association General Assembly. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Int. Bioethique = Int. J. Bioeth. 2004, 15, 124–129. [Google Scholar]
- Si Hassen, W.; Castetbon, K.; Cardon, P.; Enaux, C.; Nicolaou, M.; Lien, N.; Terragni, L.; Holdsworth, M.; Stronks, K.; Hercberg, S.; et al. Socioeconomic Indicators Are Independently Associated with Nutrient Intake in French Adults: A DEDIPAC Study. Nutrients 2016, 8, 158. [Google Scholar] [CrossRef]
- Rabi, D.M.; Edwards, A.L.; Southern, D.A.; Svenson, L.W.; Sargious, P.M.; Norton, P.; Larsen, E.T.; Ghali, W.A. Association of socio-economic status with diabetes prevalence and utilization of diabetes care services. BMC Health Serv. Res. 2006, 6, 124. [Google Scholar] [CrossRef]
- Alberg, A. The influence of cigarette smoking on circulating concentrations of antioxidant micronutrients. Toxicology 2002, 180, 121–137. [Google Scholar] [CrossRef] [PubMed]
- Farid, S.M. Trace mineral status related to levels of glycated hemoglobin of type 2 diabetic subjects in Jeddah, Saudi Arabia. Med. J. Islam. World Acad. Sci. 2013, 21, 47–56. [Google Scholar] [CrossRef]
- Dong, J.Y.; Xun, P.; He, K.; Qin, L.Q. Magnesium intake and risk of type 2 diabetes: Meta-analysis of prospective cohort studies. Diabetes Care 2011, 34, 2116–2122. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendía, L.E.; Sahebkar, A.; Rodríguez-Morán, M.; Guerrero-Romero, F. A systematic review and meta-analysis of randomized controlled trials on the effects of magnesium supplementation on insulin sensitivity and glucose control. Pharmacol. Res. 2016, 111, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Pham, P.C.; Pham, P.M.; Pham, S.V.; Miller, J.M.; Pham, P.T. Hypomagnesemia in patients with type 2 diabetes. Clin. J. Am. Soc. Nephrol. 2007, 2, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Gommers, L.M.; Hoenderop, J.G.; Bindels, R.J.; de Baaij, J.H. Hypomagnesemia in Type 2 Diabetes: A Vicious Circle? Diabetes 2016, 65, 3–13. [Google Scholar] [CrossRef]
- Fu, S.; Li, F.; Zhou, J.; Liu, Z. The Relationship Between Body Iron Status, Iron Intake And Gestational Diabetes: A Systematic Review and Meta-Analysis. Medicine 2016, 95, e2383. [Google Scholar] [CrossRef]
- Al-Maroof, R.A.; Al-Sharbatti, S.S. Serum zinc levels in diabetic patients and effect of zinc supplementation on glycemic control of type 2 diabetics. Saudi Med. J. 2006, 27, 344–350. [Google Scholar]
- Simon, S.F.; Taylor, C.G. Dietary zinc supplementation attenuates hyperglycemia in db/db mice. Exp. Biol. Med. 2001, 226, 43–51. [Google Scholar] [CrossRef]
- Chen, M.D.; Liou, S.J.; Lin, P.Y.; Yang, V.C.; Alexander, P.S.; Lin, W.H. Effects of zinc supplementation on the plasma glucose level and insulin activity in genetically obese (ob/ob) mice. Biol. Trace Elem. Res. 1998, 61, 303–311. [Google Scholar] [CrossRef]
- Cruz, K.J.; de Oliveira, A.R.; Marreiro Ddo, N. Antioxidant role of zinc in diabetes mellitus. World J. Diabetes 2015, 6, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Jayawardena, R.; Ranasinghe, P.; Galappatthy, P.; Malkanthi, R.; Constantine, G.; Katulanda, P. Effects of zinc supplementation on diabetes mellitus: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2012, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Carulli, L.; Rondinella, S.; Lombardini, S.; Canedi, I.; Loria, P.; Carulli, N. Diabetes, genetics and ethnicity. Aliment. Pharmacol. Ther. 2005, 22, 16–19. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | No Diabetes | Controlled Diabetes | Uncontrolled Diabetes | p-Value |
|---|---|---|---|---|
| N | 744 | 229 | 145 | |
| Age in years, mean (SD) | 40.3 (9.9) | 43.8 (9.0) | 45.3 (9.9) | <0.001 |
| Sex, n (%) | ||||
| Female | 404 (54.3%) | 128 (55.9%) | 71 (49.0%) | 0.40 |
| Male | 340 (45.7%) | 101 (44.1%) | 74 (51.0%) | |
| Nationalty, n (%) | ||||
| Non-Qatari | 107 (14.4%) | 31 (13.5%) | 24 (16.6%) | 0.71 |
| Qatari | 637 (85.6%) | 198 (86.5%) | 121 (83.4%) | |
| Education, n (%) | ||||
| Primary school | 465 (62.7%) | 87 (38.0%) | 98 (68.1%) | <0.001 |
| Secondary/high school | 127 (17.1%) | 53 (23.1%) | 14 (9.7%) | |
| Tertiary education | 150 (20.2%) | 89 (38.9%) | 32 (22.2%) | |
| Employment status | ||||
| Employed | 531 (71.4%) | 168 (73.4%) | 91 (62.8%) | 0.069 |
| Monthly salary (QAR) | ||||
| <10,000 | 134 (19.3%) | 36 (16.7%) | 37 (28.0%) | 0.12 |
| 10–20,000 | 168 (24.2%) | 51 (23.7%) | 30 (22.7%) | |
| >20,000 | 393 (56.5%) | 128 (59.5%) | 65 (49.2%) | |
| HbA1c%, median (IQR) | 5.2 (5.0, 5.4) | 6.0 (5.5, 6.4) | 7.8 (7.4, 8.9) | <0.001 |
| BMI, kg/m2, mean (SD) | 29.8 (5.6) | 31.2 (5.2) | 31.9 (5.7) | <0.001 |
| Waist-to-hip ratio, mean (SD) | 0.8 (0.1) | 0.9 (0.1) | 0.9 (0.1) | <0.001 |
| Lipid profile | ||||
| Cholesterol Total, mmol/L, median (IQR) | 5.0 (4.4, 5.6) | 5.0 (4.3, 5.5) | 5.0 (4.3, 5.7) | 0.58 |
| HDL-Cholesterol, mmol/L, median (IQR) | 1.4 (1.1, 1.6) | 1.2 (1.0, 1.5) | 1.2 (1.0, 1.5) | <0.001 |
| Triglyceride, mmol/L, median (IQR) | 1.1 (0.8, 1.5) | 1.4 (1.0, 1.9) | 1.5 (1.0, 2.2) | <0.001 |
| LDL-Cholesterol Calc, mmol/L, median (IQR) | 3.0 (2.5, 3.5) | 3.0 (2.4, 3.5) | 2.9 (2.3, 3.5) | 0.24 |
| Dyslipidemia (yes), n (%) | 249 (33.5%) | 101 (44.1%) | 67 (46.2%) | <0.001 |
| Systolic BP, mmHg, mean (SD) | 112.4 (13.3) | 117.9 (14.3) | 124.1 (17.5) | <0.001 |
| Diastolic BP, mmHg, mean (SD) | 67.4 (10.2) | 70.5 (10.3) | 74.0 (11.7) | <0.001 |
| Hypertension (yes), n (%) | 128 (29.0%) | 28 (41.2%) | 46 (54.1%) | <0.001 |
| DM family history (yes), n (%) | 195 (32.8%) | 108 (65.9%) | 75 (70.8%) | <0.001 |
| Smoking statues, n (%) | ||||
| Non-smoker | 27 (3.7%) | 11 (5.0%) | 4 (3.0%) | 0.60 |
| Current smoker | 677 (92.0%) | 198 (90.8%) | 120 (90.2%) | |
| Ex-smoker | 32 (4.3%) | 9 (4.1%) | 9 (6.8%) | |
| Multivitamin supplements, n (%) | 239 (38.9%) | 94 (51.1%) | 45 (45.0%) | 0.011 |
| Factor | Level | No Diabetes | Diabetes | p-Value | Controlled Diabetes | Uncontrolled Diabetes | p-Value |
|---|---|---|---|---|---|---|---|
| N | 744 | 374 | 229 | 145 | |||
| Iron, median (IQR) | 14.6 (10.5, 18.7) | 13.6 (9.7, 18.0) | 0.036 | 13.4 (9.2, 18.0) | 14.0 (10.0, 18.1) | 0.110 | |
| Categorised iron, n (%) | Normal | 603 (81.0%) | 295 (78.9%) | 0.390 | 178 (77.7%) | 117 (80.7%) | 0.540 |
| Low | 141 (19.0%) | 79 (21.1%) | 51 (22.3%) | 28 (19.3%) | |||
| Magnesium (Mg), median (IQR) | 0.8 (0.8, 0.9) | 0.8 (0.8, 0.8) | <0.001 | 0.8 (0.8, 0.9) | 0.8 (0.7, 0.8) | <0.001 | |
| Categorized magnesium, n (%) | Normal | 578 (77.7%) | 191 (51.1%) | <0.001 | 136 (59.4%) | 55 (37.9%) | <0.001 |
| Low | 166 (22.3%) | 183 (48.9%) | 93 (40.6%) | 90 (62.1%) | |||
| Zinc level, median (IQR) | 12.4 (11.1, 13.7) | 12.7 (11.1, 14.4) | 0.290 | 12.3 (10.5, 14.7) | 13.1 (11.6, 14.3) | 0.270 | |
| Categorised zinc, n (%) | Normal | 260 (85.8%) | 46 (82.1%) | 0.480 | 21 (75.0%) | 25 (89.3%) | 0.250 |
| Low | 43 (14.2%) | 10 (17.9%) | 7 (25.0%) | 3 (10.7%) | |||
| Copper level, median (IQR) | 17.6 (15.2, 20.5) | 18.6 (16.3, 21.8) | 0.099 | 18.6 (16.0, 20.9) | 19.4 (16.4, 23.0) | 0.200 | |
| Categorized copper level, n (%) | Normal | 216 (71.3%) | 45 (80.4%) | 0.160 | 22 (78.6%) | 23 (82.1%) | 0.360 |
| Low | 87 (28.7%) | 11 (19.6%) | 6 (21.4%) | 5 (17.9%) | |||
| Folate, median (IQR) | 21.3 (16.0, 26.5) | 23.5 (17.4, 28.7) | <0.001 | 23.5 (17.0, 28.5) | 23.4 (18.2, 29.1) | 0.295 | |
| Categorised folate, n (%) | Normal | 744 (100.0%) | 372 (100.0%) | 228 (100.0%) | 144 (100.0%) | ||
| Vitamin B12, median (IQR) | 243.0 (194.0, 326.0) | 239.0 (186.0, 324.5) | 0.710 | 224.0 (176.0, 299.0) | 263.0 (206.0, 371.5) | 0.014 | |
| Categorised vitamin B12, n (%) | Normal | 678 (91.3%) | 338 (90.9%) | 0.830 | 203 (89.0%) | 135 (93.8%) | 0.290 |
| Low | 65 (8.7%) | 34 (9.1%) | 25 (11.0%) | 9 (6.3%) |
| All Diabetes | Controlled Diabetes | Uncontrolled Diabetes | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Micronutrient | OR | p-Value | 95%CI | OR | p-Value | 95%CI | OR | p-Value | 95%CI |
| Mg | 3.32 | 0.000 | 2.47–4.47 | 2.47 | 0.000 | 1.75–3.48 | 5.57 | 0.000 | 3.65–8.52 |
| Fe | 1.49 | 0.034 | 1.03–2.16 | 1.38 | 0.141 | 0.90–2.11 | 1.75 | 0.047 | 1.01–3.03 |
| Zn | 1.49 | 0.336 | 0.66–3.34 | 2.47 | 0.063 | 0.95–6.41 | 0.62 | 0.531 | 0.14–2.77 |
| Cu | 0.68 | 0.382 | 0.28–1.62 | 1.17 | 0.784 | 0.38–3.59 | 0.35 | 0.125 | 0.09–1.34 |
| Vitamin B12 | 1.17 | 0.508 | 0.74–1.84 | 1.37 | 0.231 | 0.82–2.27 | 0.84 | 0.641 | 0.40–1.76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soliman, N.; Almishal, R.; Elsayed, B.; Ahmed, A.; Al-Amri, S.; Al-Kuwari, A.; Al-Muhannadi, S.; Nadeer, M.; Chivese, T. Association between Diabetes and Levels of Micronutrients in Qatar—A Case–Control Study. Biomedicines 2023, 11, 3045. https://doi.org/10.3390/biomedicines11113045
Soliman N, Almishal R, Elsayed B, Ahmed A, Al-Amri S, Al-Kuwari A, Al-Muhannadi S, Nadeer M, Chivese T. Association between Diabetes and Levels of Micronutrients in Qatar—A Case–Control Study. Biomedicines. 2023; 11(11):3045. https://doi.org/10.3390/biomedicines11113045
Chicago/Turabian StyleSoliman, Nada, Ruba Almishal, Basant Elsayed, Ayaaz Ahmed, Sara Al-Amri, Aisha Al-Kuwari, Shaikha Al-Muhannadi, Muhammed Nadeer, and Tawanda Chivese. 2023. "Association between Diabetes and Levels of Micronutrients in Qatar—A Case–Control Study" Biomedicines 11, no. 11: 3045. https://doi.org/10.3390/biomedicines11113045