
Evaluation of Muscle Oxygen Dynamics in Children’s Gait and Its Relationship with the Physiological Cost Index
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design and Subjects
2.2. Measurement Details and Methods
2.2.1. Physical Information
2.2.2. Measurement of Muscle Oxygen Dynamics
2.2.3. Physiological Cost Index
2.3. Statistical Analysis
3. Results
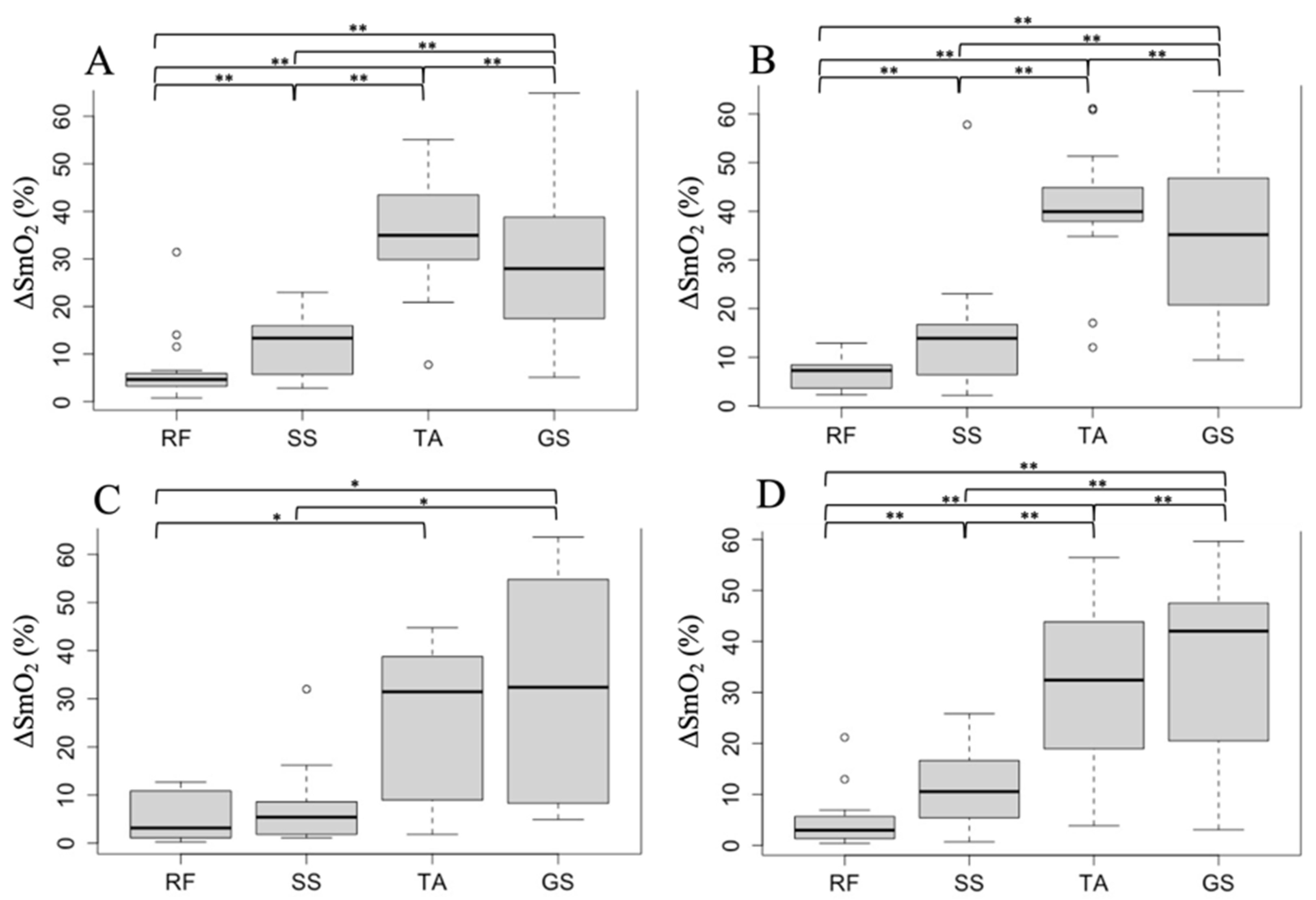
3.1. Muscle Oxygen Dynamics during Walking in Each Muscle
3.2. Association between PCI and ΔSmO2 during Walking
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Son’kin, V.; Tambovtsev, R. Energy Metabolism in Children and Adolescents. In Bioenergetics; InTechOpen: London, UK, 2012. [Google Scholar]
- Liu, J.; Yan, Y.; Xi, B.; Huang, G.; Mi, J. Skeletal Muscle Reference for Chinese Children and Adolescents. J. Cachexia Sarcopenia Muscle 2019, 10, 155–164. [Google Scholar] [CrossRef]
- Bann, D.; Wills, A.; Cooper, R.; Hardy, R.; Aihie Sayer, A.; Adams, J.; Kuh, D. Birth Weight and Growth from Infancy to Late Adolescence in Relation to Fat and Lean Mass in Early Old Age: Findings from the MRC National Survey of Health and Development. Int. J. Obes. 2014, 38, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Plasschaert, F.; Jones, K.; Forward, M. The Effect of Simulating Weight Gain on the Energy Cost of Walking in Unimpaired Children and Children with Cerebral Palsy. Arch. Phys. Med. Rehabil. 2008, 89, 2302–2308. [Google Scholar] [CrossRef]
- Bassett, D.R.; Howley, E.T. Limiting Factors for Maximum Oxygen Uptake and Determinants of Endurance Performance. Med. Sci. Sports Exerc. 2000, 32, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Takagi, S.; Murase, N.; Kime, R.; Niwayama, M.; Osada, T.; Katsumura, T. Skeletal Muscle Deoxygenation Abnormalities in Early Post-Myocardial Infarction. Med. Sci. Sports Exerc. 2014, 46, 2062–2069. [Google Scholar] [CrossRef] [PubMed]
- Takagi, S.; Murase, N.; Kime, R.; Niwayama, M.; Osada, T.; Katsumura, T. Aerobic Training Enhances Muscle Deoxygenation in Early Post-Myocardial Infarction. Eur. J. Appl. Physiol. 2016, 116, 673–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakasugi, T.; Morishita, S.; Kaida, K.; Itani, Y.; Kodama, N.; Ikegame, K.; Ogawa, H.; Domen, K. Impaired Skeletal Muscle Oxygenation Following Allogeneic Hematopoietic Stem Cell Transplantation Is Associated with Exercise Capacity. Support. Care Cancer 2018, 26, 2149–2160. [Google Scholar] [CrossRef] [PubMed]
- Kutsuzawa, T.; Shioya, S.; Kurita, D.; Haida, M.; Yamabayashi, H. Effects of Age on Muscle Energy Metabolism and Oxygenation in the Forearm Muscles. Med. Sci. Sports Exerc. 2001, 33, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Shiavi, R.; Green, N.; McFadyen, B.; Frazer, M.; Chen, J. Normative Childhood EMG Gait Patterns. J. Orthop. Res. 1987, 5, 283–295. [Google Scholar] [CrossRef]
- Granata, K.P.; Padua, D.A.; Abel, M.F. Repeatability of Surface EMG during Gait in Children. Gait Posture 2005, 22, 346–350. [Google Scholar] [CrossRef]
- Berger, W.; Quintern, J.; Dietz, V. Stance and Gait Perturbations in Children: Developmental Aspects of Compensatory Mechanisms. Electroencephalogr. Clin. Neurophysiol. 1985, 61, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Berger, W.; Quintern, J.; Dietz, V. Afferent and Efferent Control of Stance and Gait: Developmental Changes in Children. Electroencephalogr. Clin. Neurophysiol. 1987, 66, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Callewaert, M.; Boone, J.; Celie, B.; de Clercq, D.; Bourgois, J. Quadriceps Muscle Fatigue in Trained and Untrained Boys. Int. J. Sports Med. 2013, 34, 14–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen-Jones, Z.; Perrochon, A.; Hermand, E.; Ponthier, L.; Fourcade, L.; Borel, B. Evolution of Muscular Oxygenation during a Walking Test in Preterm Children. J. Pediatr. 2020, 227, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Green, H.J. Mechanisms of Muscle Fatigue in Intense Exercise. J. Sports Sci. 1997, 15, 247–256. [Google Scholar] [CrossRef]
- Berg, A.; Kim, S.; Keul, J. Skeletal Muscle Enzyme Activities in Healthy Young Subjects*. Int. J. Sports Med. 1986, 7, 236–239. [Google Scholar] [CrossRef]
- Eriksson, B.O.; Gollnick, P.D.; Saltin, B. Muscle Metabolism and Enzyme Activities after Training in Boys 11-13 Years Old. Acta Physiol. Scand. 1973, 87, 485–497. [Google Scholar] [CrossRef]
- Kaczor, J.J.; Ziolkowski, W.; Popinigis, J.; Tarnopolsky, M.A. Anaerobic and Aerobic Enzyme Activities in Human Skeletal Muscle from Children and Adults. Pediatr. Res. 2005, 57, 331–335. [Google Scholar] [CrossRef] [Green Version]
- IJzerman, M.J.; Nene, A.V. Feasibility of the Physiological Cost Index as an Outcome Measure for the Assessment of Energy Expenditure during Walking. Arch Phys. Med. Rehabil. 2002, 83, 1777–1782. [Google Scholar] [CrossRef]
- Graham, R.C.; Smith, N.M.; White, C.M. The Reliability and Validity of the Physiological Cost Index in Healthy Subjects While Walking on 2 Different Tracks. Arch Phys. Med. Rehabil. 2005, 86, 2041–2046. [Google Scholar] [CrossRef]
- Tofts, L.J.; Stanley, C.S.; Barnett, T.G.; Logan, J.G. Knee Joint Function and the Energy Cost of Level Walking in Soccer Players. Br. J. Sports Med. 1998, 32, 130–133. [Google Scholar] [CrossRef] [Green Version]
- Tuan, S.-H.; Chen, G.-B.; Chen, C.-H.; Chen, Y.-J.; Liou, I.-H.; Su, Y.-T.; Lin, K.-L. Comparison of Peak Oxygen Consumption During Exercise Testing Between Sexes Among Children and Adolescents in Taiwan. Front. Pediatr. 2021, 9, 657551. [Google Scholar] [CrossRef]
- Cooper, D.M.; Leu, S.-Y.; Taylor-Lucas, C.; Lu, K.; Galassetti, P.; Radom-Aizik, S. Cardiopulmonary Exercise Testing in Children and Adolescents with High Body Mass Index. Pediatr. Exerc. Sci. 2016, 28, 98–108. [Google Scholar] [CrossRef] [Green Version]
- Rusek, W.; Leszczak, J.; Baran, J.; Adamczyk, M.; Weres, A.; Baran, R.; Inglot, G.; Czenczek-Lewandowska, E.; Porada, S.; Pop, T. Role of Body Mass Category in the Development of Faulty Postures in School-Age Children from a Rural Area in South-Eastern Poland: A Cross-Sectional Study. BMJ Open 2019, 9, e030610. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Sugiura, H.; Ito, Y.; Noritake, K.; Ochi, N. Relationship between the Skeletal Muscle Mass Index and Physical Activity of Japanese Children: A Cross-Sectional, Observational Study. PLoS ONE 2021, 16, e0251025. [Google Scholar] [CrossRef]
- Seiyama, A.; Hazeki, O.; Tamura, M. Noninvasive Quantitative Analysis of Blood Oxygenation in Rat Skeletal Muscle. J. Biochem. 1988, 103, 419–424. [Google Scholar] [CrossRef]
- Chance, B.; Dait, M.T.; Zhang, C.; Hamaoka, T.; Hagerman, F. Recovery from Exercise-Induced Desaturation in the Quadriceps Muscles of Elite Competitive Rowers. Am. J. Physiol. 1992, 262, C766–C775. [Google Scholar] [CrossRef]
- Craig, J.C.; Broxterman, R.M.; Wilcox, S.L.; Chen, C.; Barstow, T.J. Effect of Adipose Tissue Thickness, Muscle Site, and Sex on near-Infrared Spectroscopy Derived Total-[Hemoglobin-Myoglobin]. J. Appl. Physiol. 2017, 123, 1571–1578. [Google Scholar] [CrossRef]
- Crum, E.M.; O’Connor, W.J.; van Loo, L.; Valckx, M.; Stannard, S.R. Validity and Reliability of the Moxy Oxygen Monitor during Incremental Cycling Exercise. Eur. J. Sport Sci. 2017, 17, 1037–1043. [Google Scholar] [CrossRef]
- McManus, C.J.; Collison, J.; Cooper, C.E. Performance Comparison of the MOXY and PortaMon Near-Infrared Spectroscopy Muscle Oximeters at Rest and during Exercise. J. Biomed Opt. 2018, 23, 1. [Google Scholar] [CrossRef]
- Shibuya, K.; Tanaka, J. Skeletal Muscle Oxygenation during Incremental Exercise. Arch Physiol. Biochem. 2003, 111, 475–478. [Google Scholar] [CrossRef]
- Komiyama, T.; Onozuka, A.; Miyata, T.; Shigematsu, H. Oxygen Saturation Measurement of Calf Muscle During Exercise in Intermittent Claudication. Eur. J. Vasc. Endovasc. Surg. 2002, 23, 388–392. [Google Scholar] [CrossRef] [Green Version]
- Whyte, E.; Peni, A.; Marzolini, S.; Thomas, S. Muscle Oxygenation between the Paretic and Nonparetic Leg Measured during Arterial Occlusion and Exercise in Chronic Stroke. Can. J. Cardiol. 2021, 37, S116–S117. [Google Scholar] [CrossRef]
- Wilkinson, T.J.; White, A.E.M.; Nixon, D.G.D.; Gould, D.W.; Watson, E.L.; Smith, A.C. Characterising Skeletal Muscle Haemoglobin Saturation during Exercise Using Near-Infrared Spectroscopy in Chronic Kidney Disease. Clin. Exp. Nephrol. 2019, 23, 32–42. [Google Scholar] [CrossRef] [Green Version]
- Vieira, T.M.; Botter, A. The Accurate Assessment of Muscle Excitation Requires the Detection of Multiple Surface Electromyograms. Exerc. Sport Sci. Rev. 2021, 49, 23–34. [Google Scholar] [CrossRef]
- Butler, P.; Engelbrecht, M.; Major, R.E.; Tait, J.H.; Stallard, J.; Patrick, J.H. Physiological Cost Index of Walking for Normal Children and Its Use as an Indicator of Physical Handicap. Dev. Med. Child Neurol. 1984, 26, 607–612. [Google Scholar] [CrossRef]
- Brooks, D.; Parsons, J.; Hunter, J.P.; Devlin, M.; Walker, J. The 2-Minute Walk Test as a Measure of Functional Improvement in Persons with Lower Limb Amputation. Arch Phys. Med. Rehabil. 2001, 82, 1478–1483. [Google Scholar] [CrossRef]
- Pin, T.W.; Choi, H.L. Reliability, Validity, and Norms of the 2-Min Walk Test in Children with and without Neuromuscular Disorders Aged 6–12. Disabil. Rehabil. 2018, 40, 1266–1272. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Anderson, F.C.; Pandy, M.G. Individual Muscle Contributions to Support in Normal Walking. Gait Posture 2003, 17, 159–169. [Google Scholar] [CrossRef]
- Assaiante, C.; Woollacott, M.; Amblard, B. Development of Postural Adjustment during Gait Initiation: Kinematic and EMG Analysis. J. Mot. Behav. 2000, 32, 211–226. [Google Scholar] [CrossRef]
- Jungmann, P.M.; Pfirrmann, C.; Federau, C. Characterization of Lower Limb Muscle Activation Patterns during Walking and Running with Intravoxel Incoherent Motion (IVIM) MR Perfusion Imaging. Magn. Reason. Imaging 2019, 63, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Oi, N.; Iwaya, T.; Itoh, M.; Yamaguchi, K.; Tobimatsu, Y.; Fujimoto, T. FDG-PET Imaging of Lower Extremity Muscular Activity during Level Walking. J. Orthop. Sci. 2003, 8, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Kolk, S.; Klawer, E.M.E.; Schepers, J.; Weerdesteyn, V.; Visser, E.P.; Verdonschot, N. Muscle Activity during Walking Measured Using 3D MRI Segmentations and [18F]-Fluorodeoxyglucose in Combination with Positron Emission Tomography. Med. Sci. Sports Exerc. 2015, 47, 1896–1905. [Google Scholar] [CrossRef]
- Van Beekvelt, M.C.; Colier, W.N.; Wevers, R.A.; Van Engelen, B.G. Performance of Near-Infrared Spectroscopy in Measuring Local O(2) Consumption and Blood Flow in Skeletal Muscle. J. Appl. Physiol. 2001, 90, 511–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neptune, R.R.; Sasaki, K.; Kautz, S.A. The Effect of Walking Speed on Muscle Function and Mechanical Energetics. Gait Posture 2008, 28, 135–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGowan, C.P.; Neptune, R.R.; Clark, D.J.; Kautz, S.A. Modular Control of Human Walking: Adaptations to Altered Mechanical Demands. J. Biomech. 2010, 43, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Otsuki, R.; Matsumoto, H.; Ueki, M.; Uehara, K.; Nozawa, N.; Osaki, M.; Hagino, H. Automated Stride Assistance Device Improved the Gait Parameters and Energy Cost during Walking of Healthy Middle-Aged Females but Not Those of Young Controls. J. Phys. Ther. Sci. 2016, 28, 3361–3366. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| YA Boys (n = 18) | OA Boys (n = 10) | YA Girls (n = 18) | OA Girls (n = 13) | |
|---|---|---|---|---|
| Age (years) | 6.3 ± 0.4 | 9.0 ± 0.6 | 6.5 ± 0.5 | 8.5 ± 0.6 |
| Height (cm) | 119.1 ± 5.1 | 134.0 ± 5.9 | 118.1 ± 4.5 | 129.3 ± 6.6 |
| body weight (kg) | 21.3 ± 4.2 | 27.8 ± 5.2 | 22.2 ± 3.4 | 25.9 ± 3.7 |
| BMI (kg/m2) | 14.9 ± 2.3 | 15.3 ± 1.7 | 15.8 ± 1.6 | 15.3 ± 0.8 |
| Body fat (%) | 10.2 ± 7.3 | 10.1 ± 4.7 | 15.0 ± 4.6 | 13.3 ± 3.0 |
| SMI (kg/m2) | 5.3 ± 0.4 | 5.6 ± 0.4 | 5.3 ± 0.3 | 5.4 ± 0.2 |
| 2 MWD (m) | 119.7 ± 14.5 | 129.1 ± 22.7 | 113.6 ± 10.5 | 122.9 ± 13.9 |
| YA Boys | |||||
|---|---|---|---|---|---|
| RF | SS | TA | GS | p-Value | |
| Baseline (%) | 65.9 [60.7–70.7] | 61.2 [55.3–72.1] | 48.8 [46.4–52.2] | 54.9 [51.8–60.2] | - |
| Minimum (%) | 58.9 [57.2–63.0] | 50.9 [47.1–55.7] | 12.7 [7.8–22.0] | 23.8 [15.9–41.2] | - |
| ΔSmO2 (%) | 4.6 [3.3–5.9] | 13.3 [6.3–15.7] | 34.9 [29.9–43.2] | 27.9 [17.5–18.0] | <0.001 |
| OA Boys | |||||
| RF | SS | TA | GS | p-Value | |
| Baseline (%) | 64.3 [59.1–75.7] | 56.0 [52.0–60.1] | 51.2 [48.9–53.6] | 58.8 [49.7–62.3] | - |
| Minimum (%) | 63.5 [53.0–71.6] | 48.8 [43.9–53.3] | 23.5 [11.2–34.7] | 23.1 [7.3–41.4] | - |
| ΔSmO2 (%) | 3.1 [1.1–10.0] | 5.4 [1.9–8.4] | 31.4 [10.3–37.7] | 32.3 [12.9–50.9] | 0.001 |
| YA Girls | |||||
| RF | SS | TA | GS | p-Value | |
| Baseline (%) | 73.9 [61.4–81.6] | 67.6 [62.6–75.7] | 53.4 [47.1–67.6] | 52.5 [50.7–60.3] | - |
| Minimum (%) | 65.8 [57.8–74.2] | 52.6 [47.8–60.2] | 12.1 [6.0–27.6] | 17.1 [13.5–31.9] | - |
| ΔSmO2 (%) | 7.2 [3.7–8.2] | 13.8 [6.7–16.5] | 39.9 [38.1–44.0] | 35.1 [21.4–46.5] | <0.001 |
| OA Girls | |||||
| RF | SS | TA | GS | p-Value | |
| Baseline (%) | 66.8 [65.6–72.7] | 65.3 [57.7–71.4] | 52.3 [47.8–58.1] | 55.7 [49.1–59.3] | - |
| Minimum (%) | 62.2 [59.8–67.8] | 52.4 [42.9–59.5] | 16.0 [7.4–35.0] | 12.2 [6.9–32.7] | - |
| ΔSmO2 (%) | 2.9 [1.3–5.6] | 10.5 [5.4–16.6] | 32.4 [18.9–43.8] | 42.0 [20.5–47.5] | <0.001 |
| YA Boys (n = 18) | OA Boys (n = 10) | YA Girls (n = 18) | OA Girls (n = 13) | |
|---|---|---|---|---|
| PCI (beats/m) | 0.45 ± 0.16 | 0.23 ± 0.14 | 0.46 ± 0.17 | 0.43 ± 0.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shirai, Y.; Ito, T.; Ito, Y.; Matsunaga, N.; Noritake, K.; Ochi, N.; Sugiura, H. Evaluation of Muscle Oxygen Dynamics in Children’s Gait and Its Relationship with the Physiological Cost Index. Healthcare 2023, 11, 221. https://doi.org/10.3390/healthcare11020221
Shirai Y, Ito T, Ito Y, Matsunaga N, Noritake K, Ochi N, Sugiura H. Evaluation of Muscle Oxygen Dynamics in Children’s Gait and Its Relationship with the Physiological Cost Index. Healthcare. 2023; 11(2):221. https://doi.org/10.3390/healthcare11020221
Chicago/Turabian StyleShirai, Yuya, Tadashi Ito, Yuji Ito, Naomichi Matsunaga, Koji Noritake, Nobuhiko Ochi, and Hideshi Sugiura. 2023. "Evaluation of Muscle Oxygen Dynamics in Children’s Gait and Its Relationship with the Physiological Cost Index" Healthcare 11, no. 2: 221. https://doi.org/10.3390/healthcare11020221