
The Effect of Music-Based Intervention on General Cognitive and Executive Functions, and Episodic Memory in People with Mild Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of Recent Randomized Controlled Trials

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Study Outcomes
2.5. Data Extraction
2.6. Risk of Bias Assessment
2.7. Data Synthesis and Statistical Analysis
3. Results
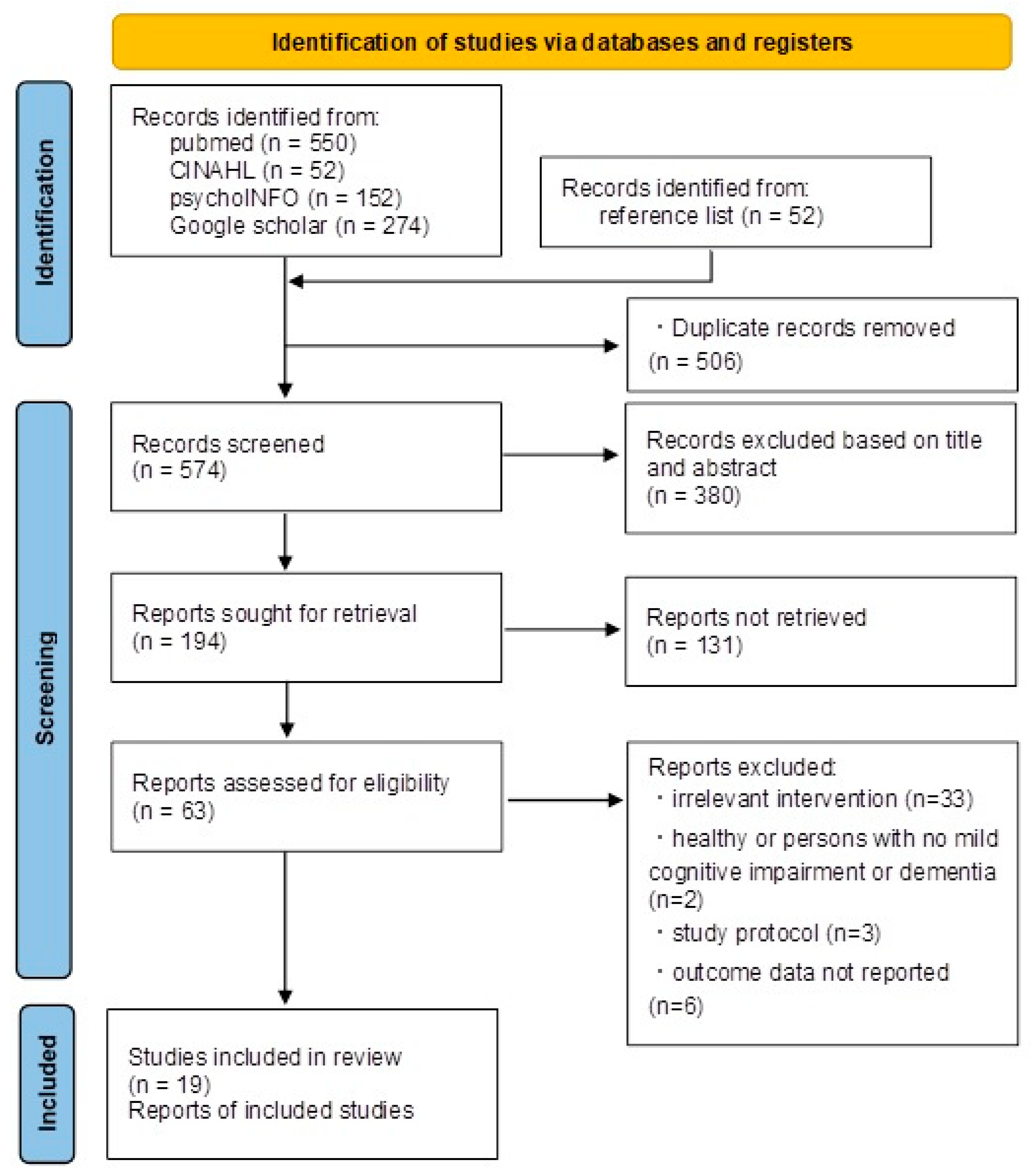
3.1. Literature Search and Study Selection
3.2. Characteristics of Included Studies
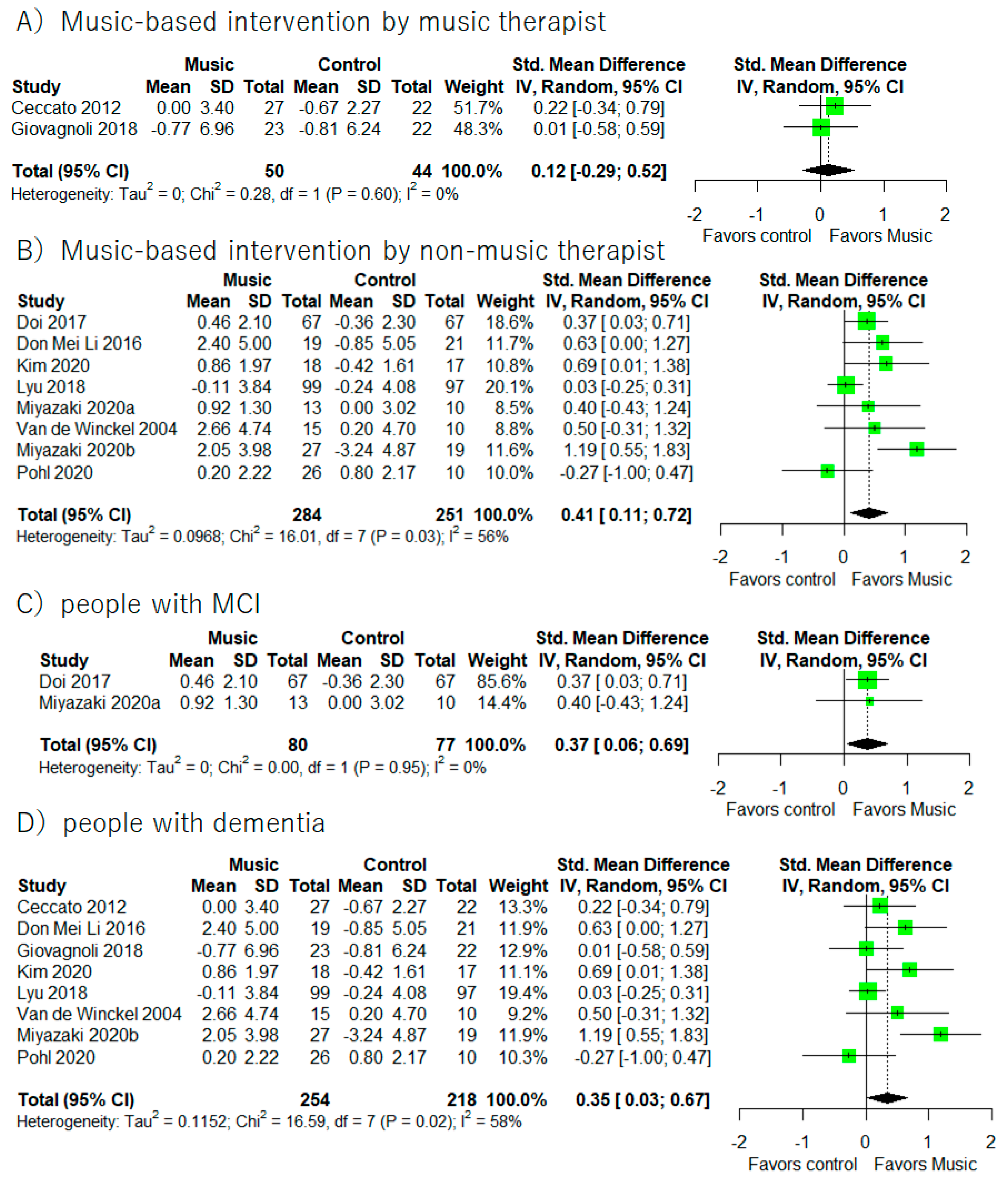
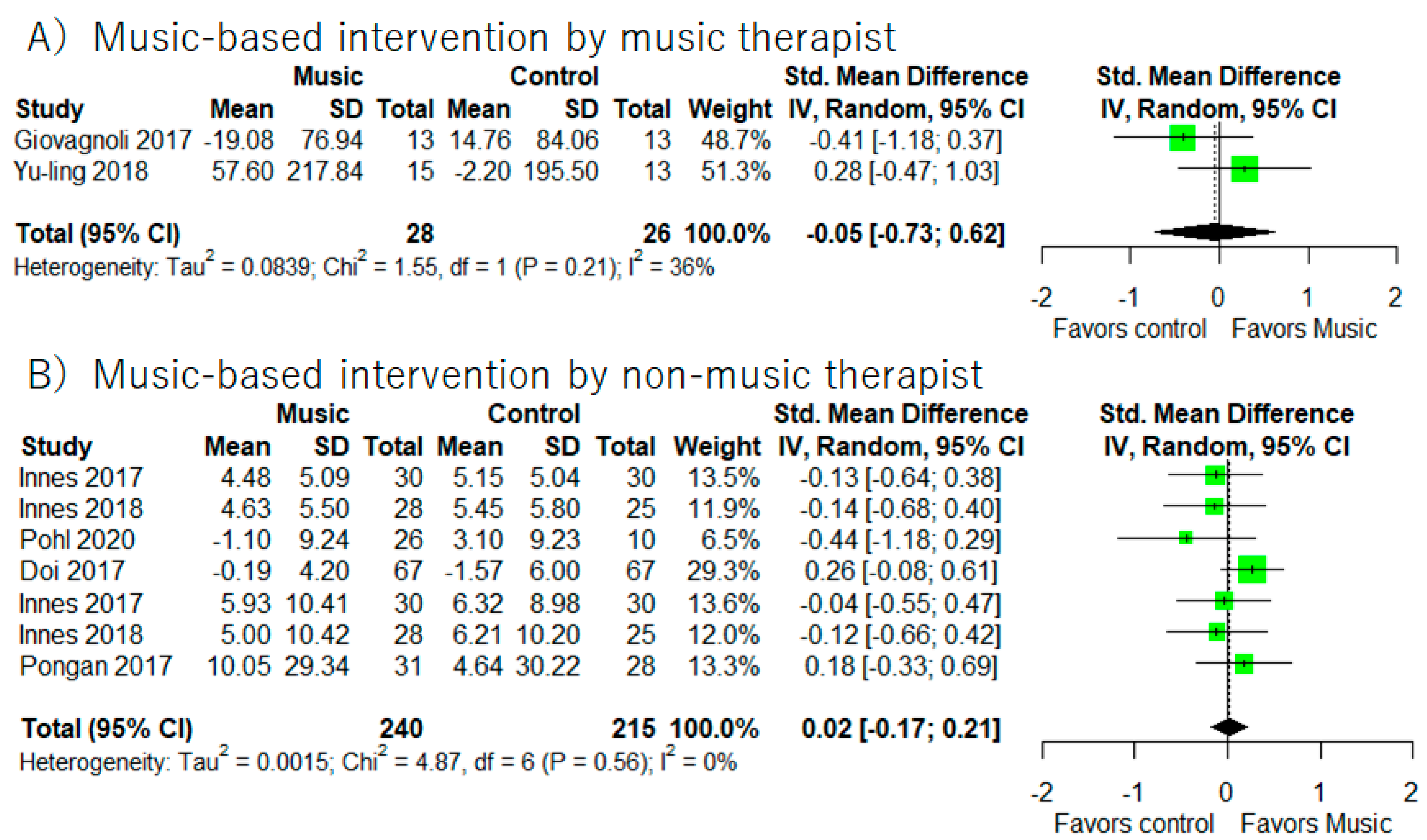
3.3. General Cognitive Function
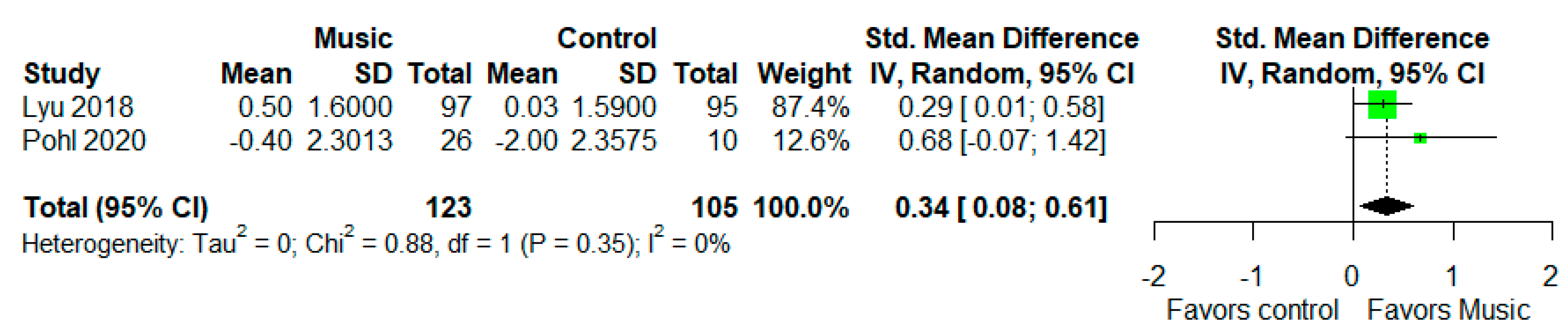
3.4. Episodic Memory
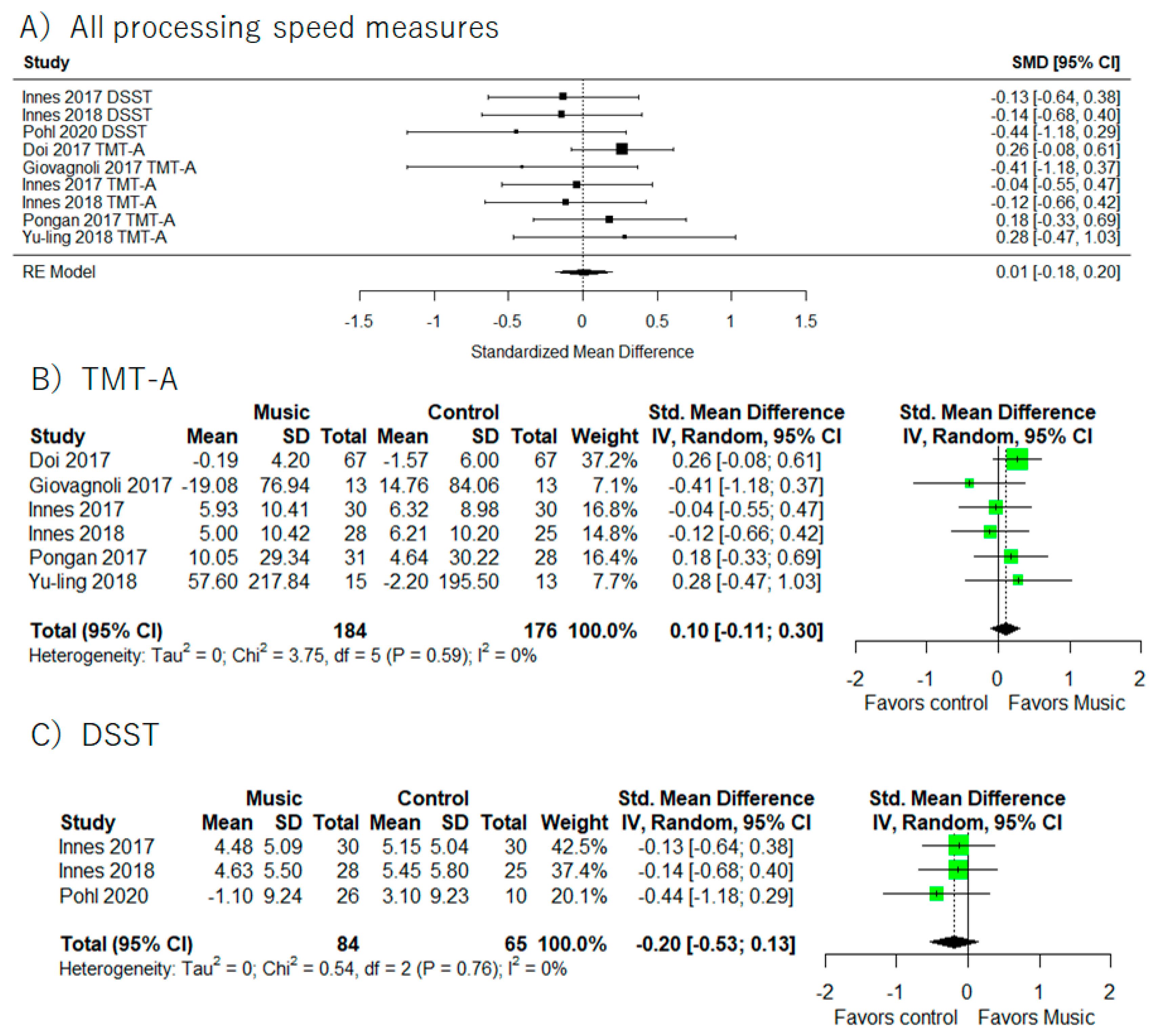
3.5. Processing Speed
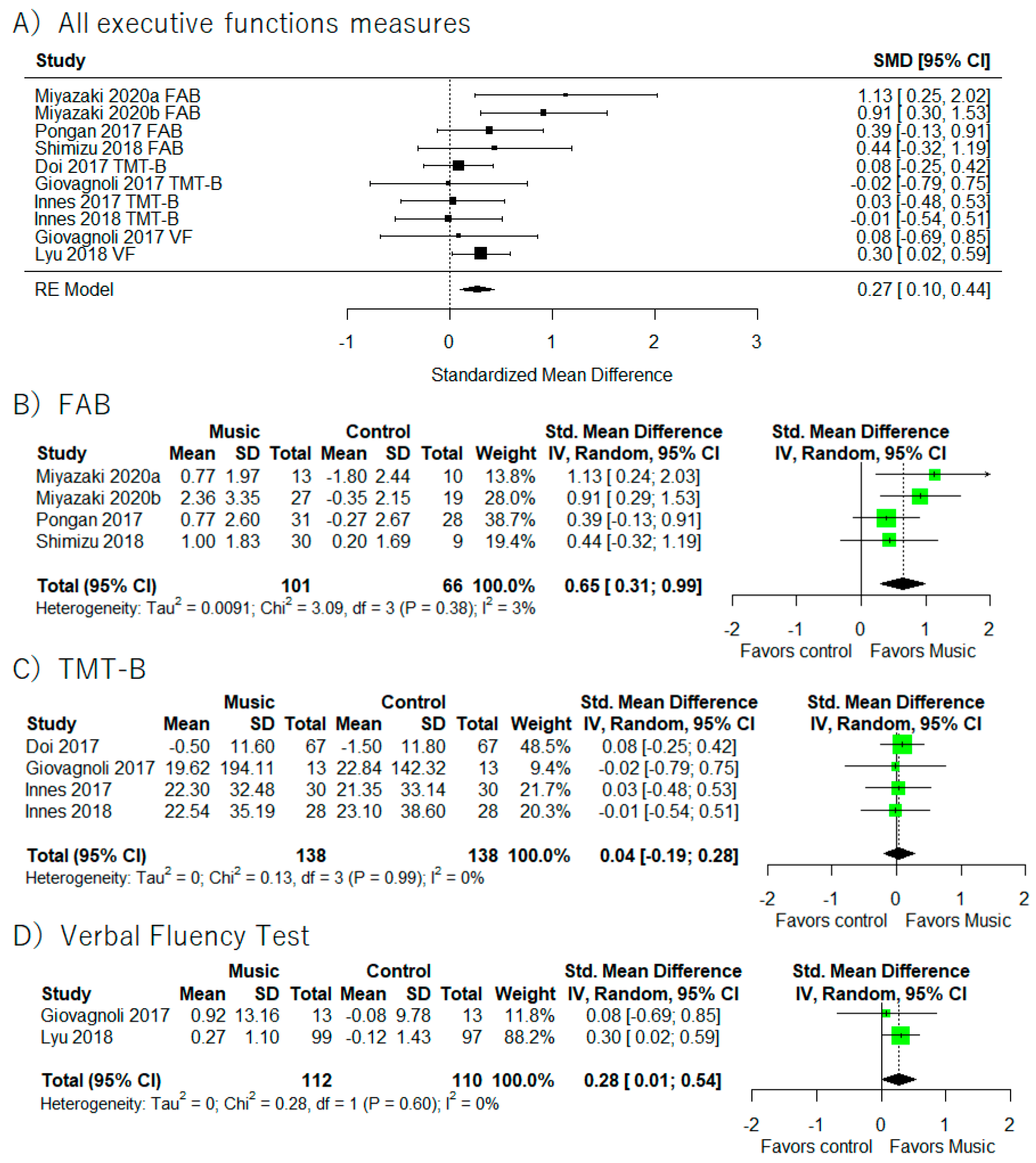
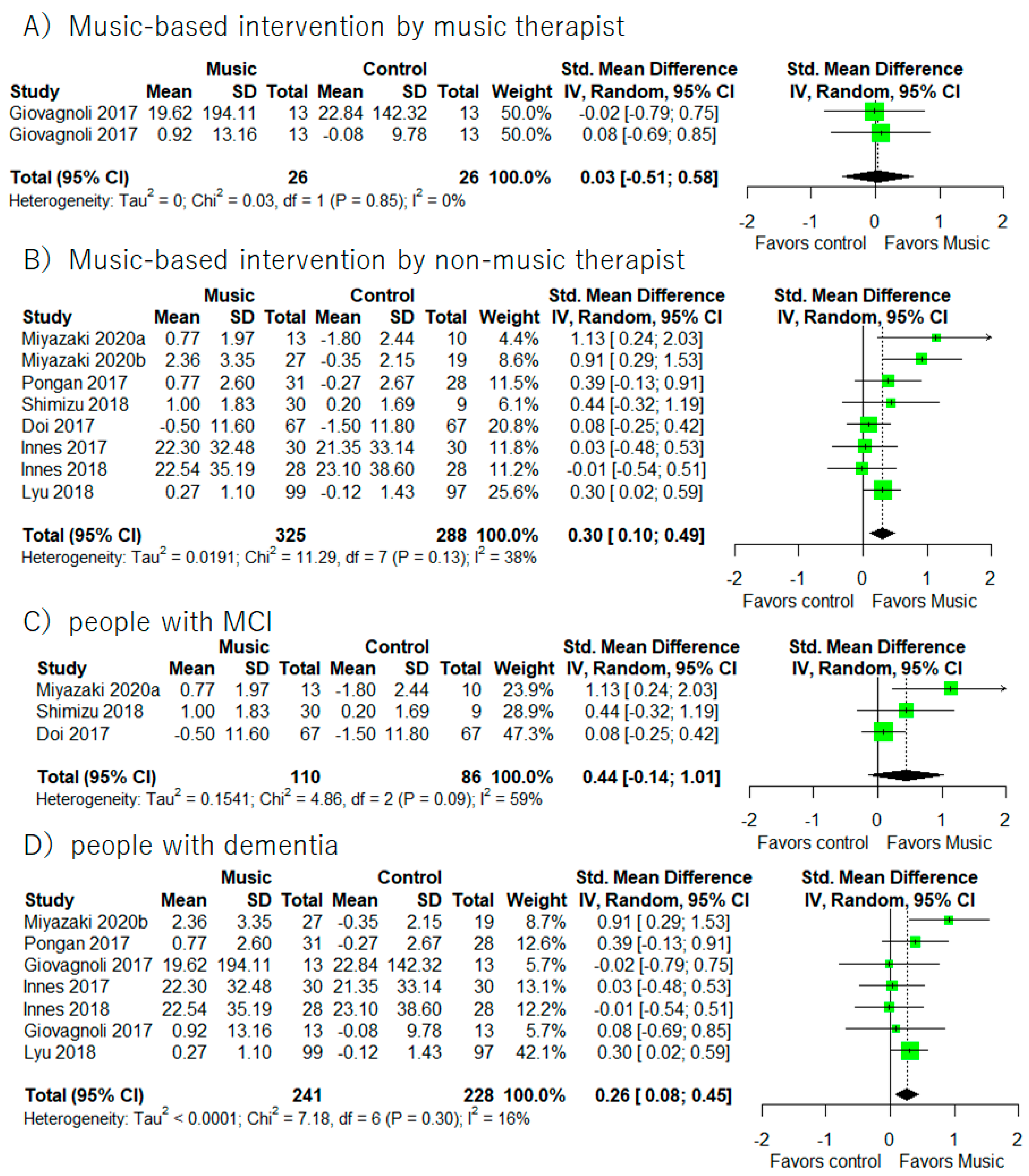
3.6. Executive Function
3.7. Working Memory/Short Term Memory/Attention
3.8. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nichols, E.; Steinmetz, J.D.; Vollset, S.E.; Fukutaki, K.; Chalek, J.; Abd-Allah, F.; Abdoli, A.; Abualhasan, A.; Abu-Gharbieh, E.; Akram, T.T.; et al. Estimation of the Global Prevalence of Dementia in 2019 and Forecasted Prevalence in 2050: An Analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef]
- Agüero-Torres, H.; Fratiglioni, L.; Guo, Z.; Viitanen, M.; Von Strauss, E.; Winblad, B. Dementia Is the Major Cause of Functional Dependence in the Elderly: 3- Year Follow-up Data from a Population-Based Study. Am. J. Public Health 1998, 88, 1452–1456. [Google Scholar] [CrossRef] [PubMed]
- Clemmensen, F.K.; Hoffmann, K.; Siersma, V.; Sobol, N.; Beyer, N.; Andersen, B.B.; Vogel, A.; Lolk, A.; Gottrup, H.; Høgh, P.; et al. The Role of Physical and Cognitive Function in Performance of Activities of Daily Living in Patients with Mild-to-Moderate Alzheimer’s Disease—A Cross-Sectional Study. BMC Geriatr. 2020, 20, 513. [Google Scholar] [CrossRef]
- Kallio, E.L.; Öhman, H.; Hietanen, M.; Soini, H.; Strandberg, T.E.; Kautiainen, H.; Pitkälä, K.H. Effects of Cognitive Training on Cognition and Quality of Life of Older Persons with Dementia. J. Am. Geriatr. Soc. 2018, 66, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.L.; Tong, G.; Ballard, C. Treatment Combinations for Alzheimer’s Disease: Current and Future Pharmacotherapy Options. J. Alzheimer’s Dis. 2019, 67, 779–794. [Google Scholar] [CrossRef] [PubMed]
- Ito, E.; Berge, L.I.; Husebo, B.S.; Nouchi, R.; Sandvik, R.K.N.M. The Negative Impact of Psychotropic Drug Use on Quality of Life in Nursing Home Patients at Different Stages of Dementia: Cross-Sectional Analyses from the COSMOS Trial. J. Am. Med. Dir. Assoc. 2020, 21, 1623–1628. [Google Scholar] [CrossRef]
- Karssemeijer, E.G.A.; Aaronson, J.A.; Bossers, W.J.; Smits, T.; Olde Rikkert, M.G.M.; Kessels, R.P.C. Positive Effects of Combined Cognitive and Physical Exercise Training on Cognitive Function in Older Adults with Mild Cognitive Impairment or Dementia: A Meta-Analysis. Ageing Res. Rev. 2017, 40, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.T.M.; Mowszowski, L.; Naismith, S.L.; Chadwick, V.L.; Valenzuela, M.; Lampit, A. Computerized Cognitive Training in Older Adults with Mild Cognitive Impairment or Dementia: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 2017, 174, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Vink, A.; Hanser, S. Music-Based Therapeutic Interventions for People with Dementia: A Mini-Review. Medicines 2018, 5, 109. [Google Scholar] [CrossRef] [PubMed]
- Baird, A.; Samson, S. Music and Dementia. Prog. Brain Res. 2015, 2017, 207–235. [Google Scholar] [CrossRef]
- Sihvonen, A.J.; Särkämö, T.; Leo, V.; Tervaniemi, M.; Altenmüller, E.; Soinila, S. Music-Based Interventions in Neurological Rehabilitation. Lancet Neurol. 2017, 16, 648–660. [Google Scholar] [CrossRef]
- Martorell, A.J.; Paulson, A.L.; Suk, H.J.; Abdurrob, F.; Drummond, G.T.; Guan, W.; Young, J.Z.; Kim, D.N.W.; Kritskiy, O.; Barker, S.J.; et al. Multi-Sensory Gamma Stimulation Ameliorates Alzheimer’s-Associated Pathology and Improves Cognition. Cell 2019, 177, 256–271.e22. [Google Scholar] [CrossRef] [PubMed]
- Clements-Cortes, A.; Bartel, L. Are We Doing More than We Know? Possible Mechanisms of Response to Music Therapy. Front. Med. 2018, 5, 255. [Google Scholar] [CrossRef] [PubMed]
- Bradt, J.; Dileo, C. Music Interventions for Mechanically Ventilated Patients. Cochrane Database Syst. Rev. 2014, 12, CD006902. [Google Scholar] [CrossRef] [PubMed]
- Munro, S.; Mount, B. Music Therapy in Palliative Care. Can. Med. Assoc. J. 1978, 119, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.D.; Mittelman, M.S. Music Therapy: A Nonpharmacological Approach to the Care of Agitation and Depressive Symptoms for Nursing Home Residents with Dementia. Dementia 2017, 16, 689–710. [Google Scholar] [CrossRef]
- Tsoi, K.K.F.; Chan, J.Y.C.; Ng, Y.-M.; Lee, M.M.Y.; Kwok, T.C.Y.; Wong, S.Y.S. Receptive Music Therapy Is More Effective than Interactive Music Therapy to Relieve Behavioral and Psychological Symptoms of Dementia: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2018, 19, 568–576.e3. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Morales, C.; Calero, R.; Moreno-Morales, P.; Pintado, C. Music Therapy in the Treatment of Dementia: A Systematic Review and Meta-Analysis. Front. Med. 2020, 7, 160. [Google Scholar] [CrossRef]
- Fusar-Poli, L.; Bieleninik, Ł.; Brondino, N.; Chen, X.J.; Gold, C. The Effect of Music Therapy on Cognitive Functions in Patients with Dementia: A Systematic Review and Meta-Analysis. Aging Ment. Health 2018, 22, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- van der Steen, J.T.; Smaling, H.J.; van der Wouden, J.C.; Bruinsma, M.S.; Scholten, R.J.; Vink, A.C. Music-Based Therapeutic Interventions for People with Dementia. Cochrane Database Syst. Rev. 2018, 7, CD003477. [Google Scholar] [CrossRef]
- Harvey, P.D. Domains of Cognition and Their Assessment. Dialogues Clin. Neurosci. 2019, 21, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.C.; Chang, C.C.; Huang, C.W.; Nouchi, R.; Cheng, C.H. Gut Microbiota in Patients with Alzheimer’s Disease Spectrum: A Systematic Review and Meta-Analysis. Aging 2022, 14, 477–496. [Google Scholar] [CrossRef] [PubMed]
- Sakaki, K.; Nouchi, R.; Matsuzaki, Y.; Saito, T.; Dinet, J.; Kawashima, R. Benefits of VR Physical Exercise on Cognition in Older Adults with and without Mild Cognitive Decline: A Systematic Review of Randomized Controlled Trials. Healthcare 2021, 9, 883. [Google Scholar] [CrossRef]
- Nouchi, R.; Suiko, T.; Kimura, E.; Takenaka, H.; Murakoshi, M.; Uchiyama, A.; Aono, M.; Kawashima, R. Effects of Lutein and Astaxanthin Intake on the Improvement of Cognitive Functions among Healthy Adults: A Systematic Review of Randomized Controlled Trials. Nutrients 2020, 12, 617. [Google Scholar] [CrossRef] [PubMed]
- Yagi, A.; Nouchi, R.; Butler, L.; Kawashima, R. Lutein Has a Positive Impact on Brain Health in Healthy Older Adults: A Systematic Review of Randomized Controlled Trials and Cohort Studies. Nutrients 2021, 13, 1746. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Panisset, M.; Roudier, M.; Saxton, J.; Boller, F. Severe Impairment Battery. A Neuropsychological Test for Severely Demented Patients. Arch. Neurol. 1994, 51, 41–45. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Rey, A. L’examen Psychologique Dans Le Cas d’encephalopathie Traumatique. Arch. De Psychol. 1941, 28, 286–340. [Google Scholar]
- Green, P. Green’s Word Memory Test for Microsoft Windows: User’s Manual; Green’s Publishing: Edmonton, AB, Canada, 2005. [Google Scholar]
- Reitan, R.M. Validity of the Trail Making Test as an Indicator of Organic Brain Damage. Percept. Mot. Ski. 1958, 8, 271–276. [Google Scholar] [CrossRef]
- McLeod, D.R.; Griffiths, R.R.; Bigelow, G.E.; Yingling, J. An Automated Version of the Digit Symbol Substitution Test (DSST). Behav. Res. Methods Instrum. 1982, 14, 463–466. [Google Scholar] [CrossRef]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal Assessment Battery at Bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Chapter 10: Analysing Data and Undertaking Meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons, Ltd: Hoboken, NJ, USA, 2022; pp. 241–284. Available online: www.training.cochrane.org/handbook (accessed on 10 June 2022).
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Verghese, J.; Makizako, H.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Suzuki, T.; Shimada, H. Effects of Cognitive Leisure Activity on Cognition in Mild Cognitive Impairment: Results of a Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2017, 18, 686–691. [Google Scholar] [CrossRef]
- Miyazaki, A.; Mori, H. Frequent Karaoke Training Improves Frontal Executive Cognitive Skills, Tongue Pressure, and Respiratory Function in Elderly People: Pilot Study from a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 12–14. [Google Scholar] [CrossRef]
- Shimizu, N.; Umemura, T.; Matsunaga, M.; Hirai, T. Effects of Movement Music Therapy with a Percussion Instrument on Physical and Frontal Lobe Function in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Trial. Aging Ment. Health 2018, 22, 1614–1626. [Google Scholar] [CrossRef] [PubMed]
- Giovagnoli, A.R.; Manfredi, V.; Parente, A.; Schifano, L.; Oliveri, S.; Avanzini, G. Cognitive Training in Alzheimer’s Disease: A Controlled Randomized Study. Neurol. Sci. 2017, 38, 1485–1493. [Google Scholar] [CrossRef] [PubMed]
- Mahendran, R.; Gandhi, M.; Moorakonda, R.B.; Wong, J.; Kanchi, M.M.; Fam, J.; Rawtaer, I.; Kumar, A.P.; Feng, L.; Kua, E.H. Art Therapy Is Associated with Sustained Improvement in Cognitive Function in the Elderly with Mild Neurocognitive Disorder: Findings from a Pilot Randomized Controlled Trial for Art Therapy and Music Reminiscence Activity versus Usual Care. Trials 2018, 19, 615. [Google Scholar] [CrossRef] [PubMed]
- Pongan, E.; Tillmann, B.; Leveque, Y.; Trombert, B.; Getenet, J.C.; Auguste, N.; Dauphinot, V.; el Haouari, H.; Navez, M.; Dorey, J.-M.; et al. Can Musical or Painting Interventions Improve Chronic Pain, Mood, Quality of Life, and Cognition in Patients with Mild Alzheimer’s Disease? Evidence from a Randomized Controlled Trial. J. Alzheimer’s Dis. 2017, 60, 663–677. [Google Scholar] [CrossRef] [PubMed]
- Innes, K.E.; Selfe, T.K.; Brundage, K.; Montgomery, C.; Wen, S.; Kandati, S.; Bowles, H.; Khalsa, D.S.; Huysmans, Z. Effects of Meditation and Music-Listening on Blood Biomarkers of Cellular Aging and Alzheimer’s Disease in Adults with Subjective Cognitive Decline: An Exploratory Randomized Clinical Trial. J. Alzheimer’s Dis. 2018, 66, 947–970. [Google Scholar] [CrossRef]
- Kim, D. The Effects of a Recollection-Based Occupational Therapy Program of Alzheimer’s Disease: A Randomized Controlled Trial. Occup. Ther. Int. 2020, 2020, 6305727. [Google Scholar] [CrossRef] [PubMed]
- Yu-ling, C.; Yu-Cheng, P. Musical Dual-Task Training in Patients with Mild-to- Moderate Dementia: A Randomized Controlled Trial. Neuropsychiatr. Dis. Treat. 2018, 14, 1381–1393. [Google Scholar]
- Lyu, J.; Zhang, J.; Mu, H.; Li, W.; Champ, M.; Xiong, Q.; Gao, T.; Xie, L.; Jin, W.; Yang, W.; et al. The Effects of Music Therapy on Cognition, Psychiatric Symptoms, and Activities of Daily Living in Patients with Alzheimer’s Disease. J. Alzheimer’s Dis. 2018, 64, 1347–1358. [Google Scholar] [CrossRef]
- Miyazaki, A.; Okuyama, T.; Mori, H.; Sato, K.; Ichiki, M.; Nouchi, R. Drum Communication Program Intervention in Older Adults With Cognitive Impairment and Dementia at Nursing Home: Preliminary Evidence From Pilot Randomized Controlled Trial. Front. Aging Neurosci. 2020, 12, 142. [Google Scholar] [CrossRef]
- Giovagnoli, A.R.; Manfredi, V.; Schifano, L.; Paterlini, C.; Parente, A.; Tagliavini, F. Combining Drug and Music Therapy in Patients with Moderate Alzheimer’s Disease: A Randomized Study. Neurol. Sci. 2018, 39, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Narme, P.; Clément, S.; Ehrlé, N.; Schiaratura, L.; Vachez, S.; Courtaigne, B.; Munsch, F.; Samson, S. Efficacy of Musical Interventions in Dementia: Evidence from a Randomized Controlled Trial. J. Alzheimer’s Dis. 2014, 38, 359–369. [Google Scholar] [CrossRef] [PubMed]
- van de Winckel, A.; Feys, H.; de Weerdt, W.; Dom, R. Cognitive and Behavioural Effects of Music-Based Exercises in Patients with Dementia. Clin. Rehabil. 2004, 18, 253–260. [Google Scholar] [CrossRef]
- Ceccato, E.; Vigato, G.; Bonetto, C.; Bevilacqua, A.; Pizziolo, P.; Crociani, S.; Zanfretta, E.; Pollini, L.; Caneva, P.A.; Baldin, L.; et al. STAM Protocol in Dementia: A Multicenter, Single-Blind, Randomized, and Controlled Trial. Am. J. Alzheimer’s Dis. Other Dement. 2012, 27, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Li, D.M.; Li, X.X. The Effect of Folk Recreation Program in Improving Symptoms: A Study of Chinese Elder Dementia Patients. Int. J. Geriatr. Psychiatry 2017, 32, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Li, D.; Xu, H.; Hu, Z. Effect of Traditional Opera on Older Adults with Dementia. Geriatr. Nurs. 2020, 41, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Innes, K.E.; Selfe, T.K.; Khalsa, D.S.; Kandati, S. Meditation and Music Improve Memory and Cognitive Function in Adults with Subjective Cognitive Decline: A Pilot Randomized Controlled Trial. J. Alzheimer’s Dis. 2017, 56, 899–916. [Google Scholar] [CrossRef] [PubMed]
- Pohl, P.; Wressle, E.; Lundin, F.; Enthoven, P.; Dizdar, N. Group-Based Music Intervention in Parkinson’s Disease—Findings from a Mixed-Methods Study. Clin. Rehabil. 2020, 34, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Raglio, A.; Bellandi, D.; Baiardi, P.; Gianotti, M.; Ubezio, M.C.; Zanacchi, E.; Granieri, E.; Imbriani, M.; Stramba-Badiale, M. Effect of Active Music Therapy and Individualized Listening to Music on Dementia: A Multicenter Randomized Controlled Trial. J. Am. Geriatr. Soc. 2015, 63, 1534–1539. [Google Scholar] [CrossRef]
- Mate, K.E.; Pond, C.D.; Magin, P.J.; Goode, S.M.; McElduff, P.; Stocks, N.P. Diagnosis and Disclosure of a Memory Problem Is Associated with Quality of Life in Community Based Older Australians with Dementia. Int. Psychogeriatr. 2012, 24, 1962–1971. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Marra, C.A.; Najafzadeh, M.; Liu-Ambrose, T. The Independent Contribution of Executive Functions to Health Related Quality of Life in Older Women. BMC Geriatr. 2010, 10, 16. [Google Scholar] [CrossRef]
- Stites, S.D.; Harkins, K.; Rubright, J.D.; Karlawish, J. Relationships Between Cognitive Complaints and Quality of Life in Older Adults With Mild Cognitive Impairment, Mild Alzheimer Disease Dementia, and Normal Cognition. Alzheimer Dis. Assoc. Disord. 2018, 32, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.M.; Cho, Y.S.; Park, S.; Lee, B.H.; Sohn, B.K.; Choi, C.H.; Choi, J.S.; Jeong, H.Y.; Cho, S.J.; Lee, J.H.; et al. Montreal Cognitive Assessment Reflects Cognitive Reserve. BMC Geriatr. 2018, 18, 261. [Google Scholar] [CrossRef]
- Siqueira, G.S.A.; Hagemann, P.D.M.S.; Coelho, D.D.S.; Santos, F.H.D.; Bertolucci, P.H.F.; Heyn, P.C. Can MoCA and MMSE Be Interchangeable Cognitive Screening Tools? A Systematic Review. Gerontologist 2019, 59, E743–E763. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gallego, M.; Gómez-Gallego, J.C.; Gallego-Mellado, M.; García-García, J. Comparative Efficacy of Active Group Music Intervention versus Group Music Listening in Alzheimer’s Disease. Int. J. Environ. Res. Public Health 2021, 18, 8067. [Google Scholar] [CrossRef] [PubMed]
- Fernaeus, S.E.; Östberg, P.; Wahlund, L.O.; Hellström, Å. Memory Factors in Rey AVLT: Implications for Early Staging of Cognitive Decline. Scand. J. Psychol. 2014, 55, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Cai, J.; An, L.; Hui, F.; Ren, T.; Ma, H.; Zhao, Q. Does Music Therapy Enhance Behavioral and Cognitive Function in Elderly Dementia Patients? A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2017, 35, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Alnajjar, F.; Khalid, S.; Vogan, A.A.; Shimoda, S.; Nouchi, R.; Kawashima, R. Emerging Cognitive Intervention Technologies to Meet the Needs of an Aging Population: A Systematic Review. Front. Aging Neurosci. 2019, 11, 291. [Google Scholar] [CrossRef]
- Kawata, N.Y.S.; Nouchi, R.; Oba, K.; Matsuzaki, Y.; Kawashima, R. Auditory Cognitive Training Improves Brain Plasticity in Healthy Older Adults: Evidence From a Randomized Controlled Trial. Front. Aging Neurosci. 2022, 14, 826672. [Google Scholar] [CrossRef]
- Nouchi, R.; Hu, Q.; Saito, T.; Kawata, N.Y.d.S.; Nouchi, H.; Kawashima, R. Brain Training and Sulforaphane Intake Interventions Separately Improve Cognitive Performance in Healthy Older Adults, Whereas a Combination of These Interventions Does Not Have More Beneficial Effects: Evidence from a Randomized Controlled Trial. Nutrients 2021, 13, 352. [Google Scholar] [CrossRef] [PubMed]
- Nouchi, R.; Nouchi, H.; Dinet, J.; Kawashima, R. Cognitive Training with Neurofeedback Using NIRS Improved Cognitive Functions in Young Adults: Evidence from a Randomized Controlled Trial. Brain Sci. 2021, 12, 5. [Google Scholar] [CrossRef] [PubMed]
- Hung, L.; Van, E.A.; Zee, D.; Bernardo-Filho, M.; Da, D.; De, C.; Caputo, S.; Campbell, E.A.; Kantor, J.; Kantorová, L.; et al. Tactile Low Frequency Vibration in Dementia Management: A Scoping Review. Front. Psychol. 2022, 1, 854794. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study and Year | Country | Recruitment Site | No. of Participants | Mean Age | Female | Severity of Dementia | Type of Music-Based Intervention | Control Type | Intervention Period | Intervention Frequency | Time for Each Intervention | Study Outcomes | Quality Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ceccato 2012 [55] | Italy | Support center | 51 | 86.3 | 40 (78.4%) | Non-specific | STAM (music with movement, clapping hands) | Control | 12 weeks | Twice a week | 40 min | MMSE | 10 |
| Yu-ling 2018 [49] | USA | Dementia outpatient unit at a medical center | 28 | 77.3 | 14 (50%) | Mild to moderate | Musical dual task (sing or play instrument while walking) | Control | 8 weeks | Once a week | 60 min | MMSE, TMT-A | 12 |
| Doi 2017 [41] | Japan | National center for geriatrics and gerontology | 201 | 76 | 104 (51.7%) | MCI | Play instrument (percussion) | Dance, control | 40 weeks | Once a week | 60 min | MMSE, TMT-A, TMT-B, Story and word memory | 11 |
| Don Mei Li 2016 [56] | China | Long term care facility | 40 | 82.4 | 28 (70%) | Non-specific | Folk recreation (singing) | Control | 16 weeks | 3 times a week | 40–50 min | TMT-A | 8 |
| Giovagnoli 2017 [44] | Italy | One nursing center | 39 | 73.6 | 24 (61.5%) | Mild to moderate | Play instrument | Active control (cognitive training, neuroeducation) | 12 weeks | Twice a week | 45 min | TMT, DSST | 9 |
| Giovagnoli 2018 [52] | Italy | One center | 45 | 73.2 | 31 (68.9%) | Non-specific | Music (playing music) and drugs | Drugs only | 24 weeks | Twice a week | 40 min | SBI, MMSE | 13 |
| Innes 2017 [58] | USA | Community | 60 | 60.6 | 56 (93.3%) | Non-specific | Listening to music | Meditation | 12 weeks | Daily | 12 min | TMT-A, TMT-B, DSST, | 12 |
| Innes 2018 [47] | USA | Community | 53 | 60 | 46 (86.8%) | Non-specific | Listening to music | Meditation | 12 weeks | Daily | 30–45 min | TMT-A, TMT-B | 11 |
| Kim 2020 [48] | Korea | Adult day care center | 35 | 79.3 | 26 (74.3%) | Mild AD | Recollection based occupational music-based intervention (singing, listening) | Control | 24 weeks | 5 sessions a week | 60 min | MMSE | 9 |
| Lyu 2018 [50] | China | Geriatric hospital | 298 | 69.7 | 173 (58.1%) | Mild to severe AD | Singing | Lyric reading, control | 12 weeks | Twice a day, twice a week | 30–40 min, | Verbal fluency, AVLT, MMSE. | 10 |
| Mahendran 2018 [45] | Singapore | Community living | 68 | 71.1 | 38 (55.9%) | Mild neurocognitive decline | Music reminiscence (listening) | Art therapy, control | 12 weeks | Once a week | 65 min (including 15 min break) | AVLT | 11 |
| Miyazaki 2020a [42] | Japan | Residential care facilities | 26 | 81.5 | 20 (76.9%) | MCI | Singing (karaoke) | Active control | 12 weeks | Once a week | 120 min | MoCA, FAB | 12 |
| Miyazaki 2020b [51] | Japan | Nursing home | 46 | 87 | 40 (87.0%) | Non-specific | Play instrument (Drum) | Control | 12 weeks | Twice a week | 30 min | MMSE, FAB | 9 |
| Narme 2013 [53] | France | Nursing home | 37 | 87.1 | 32 (86.5%) | Alzheimer’s with mixed dementia | Play instrument (Percussion) | Cooking | 4 weeks | Twice a week | 60 min | SBI | 8 |
| Pohl 2020 [59] | Sweden | Community dwelling individuals diagnosed with PD | 46 | 70 | 32 (69.6%) | PD | Training with music based intervention | Control | 12 weeks | Twice a week | 60 min | MoCA, PDQ39 | 11 |
| Pongan 2017 [46] | France | University hospital | 59 | 79.5 | 39 (66.1%) | Mild Alzheimer’s disease | Singing | Painting | 12 weeks | Once a week | 120 min | TMT-A, FAB, | 13 |
| Raglio 2015 [60] | Italy | Nursing home and day care centers | 120 | 81.7 | 94 (78.3%) | Moderate to severe dementia | Active music therapy, listening to music | Control | 10 weeks | Twice a week | 30 min | MMSE | 11 |
| Shimizu 2018 [43] | Japan | Community dwelling individuals participating in the dementia care class | 45 | 74.6 | 38 (84.4%) | MCI | Music with movement | Active control (movement without music) | 12 weeks | Once a week | 60 min | FAB | 10 |
| Van de Winckel 2002 [54] | Belgium | Public hospital | 25 | 81.7 | 25 (100%) | Non-specific | Exercise with music | Active control (one to one conversation) | 12 weeks | Once a day | 30 min | MMSE, ADS 6 | 9 |
| Total | 1024 |
| Outcome | Test | Number of Studies | Number of Studies Compared with Control Group | Number of Studies Compared with Active Control Group |
|---|---|---|---|---|
| General cognitive function | MMSE | 8 | 5 | 3 |
| MoCA | 2 | 1 | 1 | |
| Episodic memory | AVLT | 2 | 2 | 2 |
| Working memory | 0 | - | - | |
| Short-term memory | 1 | - | - | |
| Attention | 0 | - | - | |
| Processing speed | TMT-A | 6 | 2 | 6 |
| DSST | 1 | 0 | 1 | |
| Executive function | Verbal fluency | 2 | 2 | 2 |
| TMT-B | 4 | 0 | 4 | |
| FAB | 5 | 2 | 3 |
| Lead Author, Year, Country | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ceccato 2012 [55] | Y | Y | Y | Y | ? | ? | Y | Y | N | Y | Y | Y | Y | N | 10 |
| Yu-ling 2018 [49] | Y | Y | N | Y | Y | ? | Y | Y | Y | Y | Y | Y | Y | Y | 12 |
| Doi 2017 [41] | Y | Y | Y | Y | Y | ? | Y | Y | Y | Y | Y | N | Y | N | 11 |
| Don Mei Li 2016 [56] | Y | Y | Y | Y | ? | ? | Y | Y | N | N | Y | N | Y | N | 8 |
| Giovagnoli 2017 [44] | Y | Y | Y | Y | ? | N | ? | Y | N | Y | Y | Y | Y | N | 9 |
| Giovagnoli 2018 [52] | Y | Y | Y | Y | Y | ? | Y | Y | Y | Y | Y | Y | Y | Y | 13 |
| Innes 2017 [58] | Y | Y | Y | Y | ? | Y | Y | Y | Y | Y | Y | Y | Y | N | 12 |
| Innes 2018 [47] | Y | Y | Y | Y | Y | ? | Y | Y | N | Y | Y | Y | Y | N | 11 |
| Kim 2020 [48] | Y | Y | Y | Y | ? | ? | Y | Y | N | N | Y | Y | Y | N | 9 |
| Lyu 2018 [50] | Y | Y | Y | Y | Y | N | N | Y | N | Y | Y | Y | Y | N | 10 |
| Mahendran 2018 [45] | Y | Y | Y | Y | ? | N | Y | Y | Y | N | Y | Y | Y | Y | 11 |
| Miyazaki 2020a [42] | Y | Y | Y | Y | Y | Y | Y | ? | N | Y | Y | Y | Y | Y | 12 |
| Miyazaki 2020b [51] | Y | N | Y | Y | N | N | N | Y | N | Y | Y | Y | Y | Y | 9 |
| Narme 2013 [53] | Y | Y | Y | Y | ? | ? | ? | Y | N | N | Y | Y | Y | N | 8 |
| Pohl 2020 [59] | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | Y | Y | Y | 11 |
| Pongan 2017 [46] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | ? | 13 |
| Raglio 2015 [60] | Y | Y | Y | Y | ? | ? | Y | Y | Y | Y | Y | Y | Y | N | 11 |
| Shimizu 2018 [43] | Y | Y | Y | Y | N | ? | Y | Y | N | Y | Y | Y | Y | N | 10 |
| Van de Winckel 2002 [54] | Y | Y | Y | Y | ? | ? | Y | Y | N | N | Y | Y | Y | N | 9 |
| Total score across studies | 19 | 18 | 18 | 19 | 7 | 3 | 15 | 18 | 7 | 14 | 19 | 17 | 19 | 6 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, E.; Nouchi, R.; Dinet, J.; Cheng, C.-H.; Husebø, B.S. The Effect of Music-Based Intervention on General Cognitive and Executive Functions, and Episodic Memory in People with Mild Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of Recent Randomized Controlled Trials. Healthcare 2022, 10, 1462. https://doi.org/10.3390/healthcare10081462
Ito E, Nouchi R, Dinet J, Cheng C-H, Husebø BS. The Effect of Music-Based Intervention on General Cognitive and Executive Functions, and Episodic Memory in People with Mild Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of Recent Randomized Controlled Trials. Healthcare. 2022; 10(8):1462. https://doi.org/10.3390/healthcare10081462
Chicago/Turabian StyleIto, Erika, Rui Nouchi, Jerome Dinet, Chia-Hsiung Cheng, and Bettina Sandgathe Husebø. 2022. "The Effect of Music-Based Intervention on General Cognitive and Executive Functions, and Episodic Memory in People with Mild Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of Recent Randomized Controlled Trials" Healthcare 10, no. 8: 1462. https://doi.org/10.3390/healthcare10081462