From Workshop to E-Learning: Using Technology-Enhanced “Intermediate Concept Measures” As a Framework for Pharmacy Ethics Education and Assessment

Abstract
:1. Introduction
- (i)
- Developmental bedrock schemas, reflecting preferred decision-making schemas at an abstract level, as measured by a psychometric measure known as the Defining Issues Test (DIT) [4,7]. While the impact of educational interventions may be measured using a pre-post intervention design using the DIT as the measure [5], the discussion surrounding the measurement of the impact of professional ethics programs is beyond the scope of this paper.
- (ii)
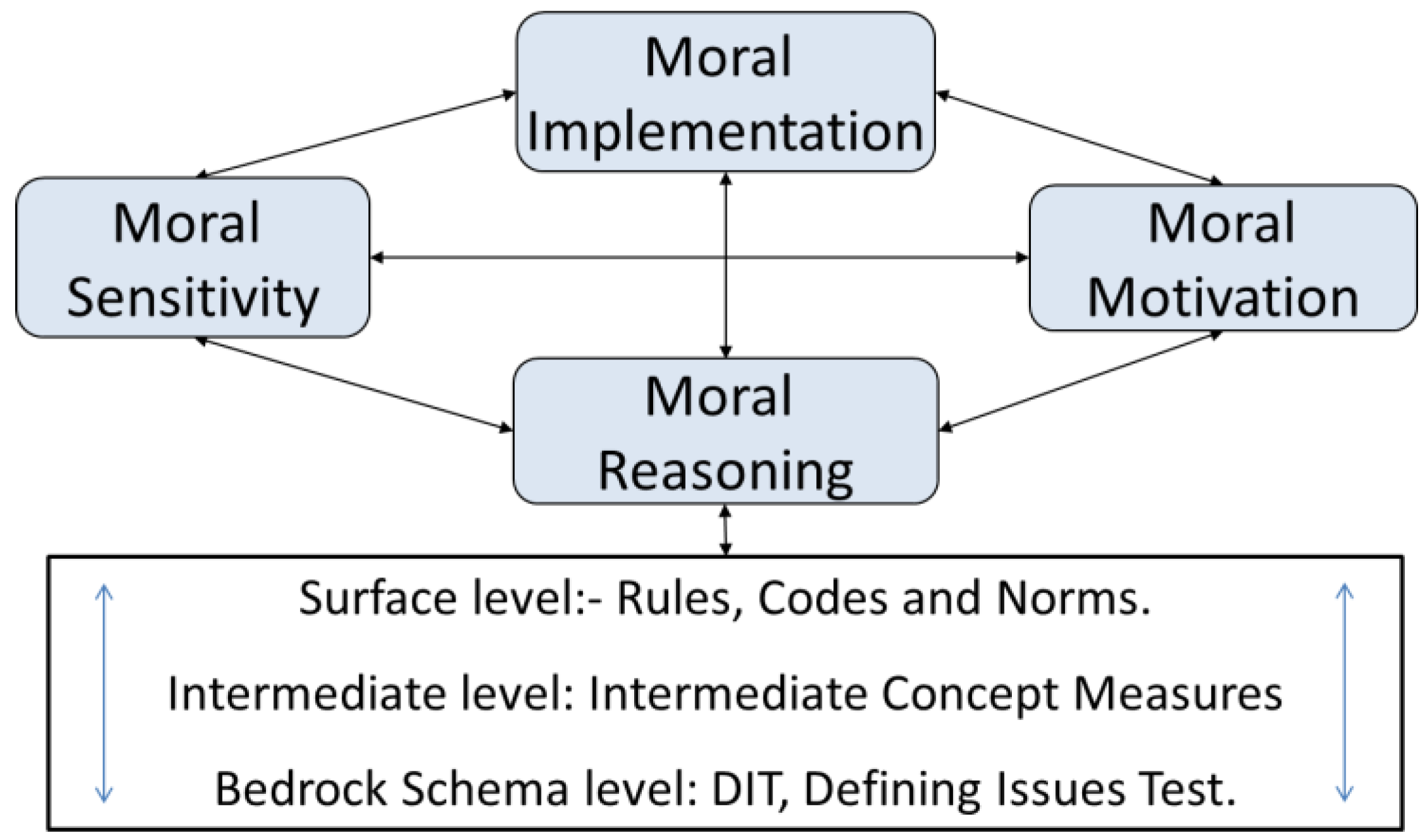
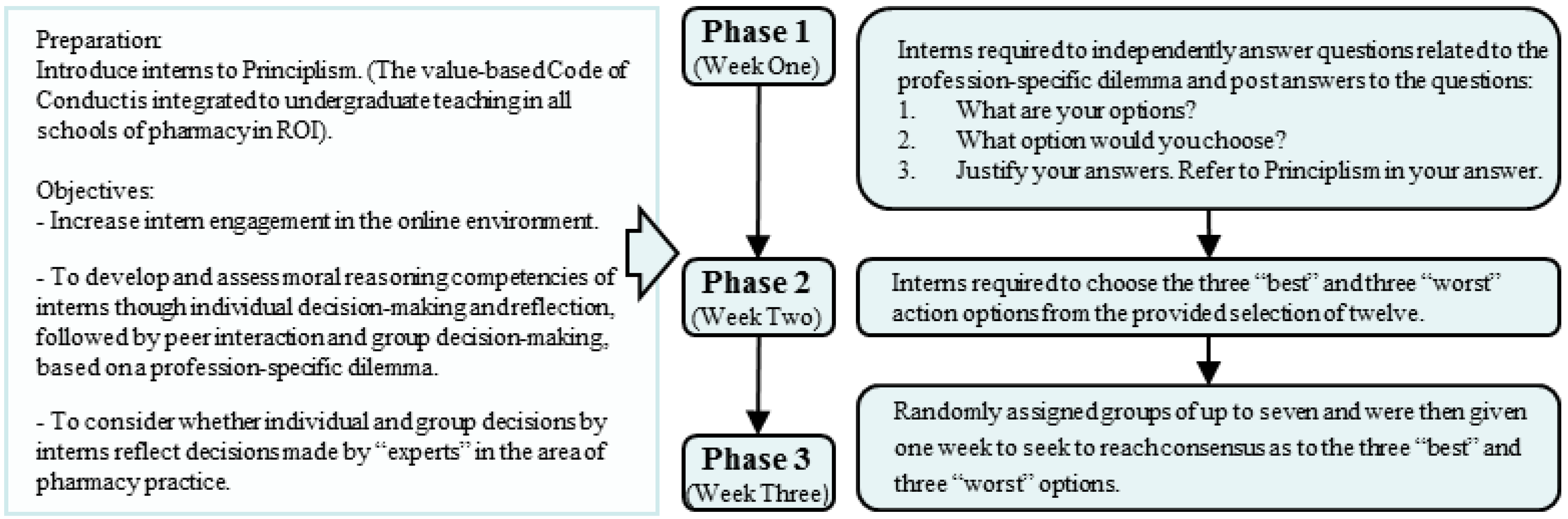
- Intermediate-level moral concepts are designed to cover a broad range of situations that require significant professional interpretation by participants in an educational intervention. Reasoning about intermediate concepts is, in part, a reflection of the individual’s preferred approach to decision-making through dilemmas. The methodology outlined in this article draws from intermediate concepts and the FCM [2], but presents a format of ICM that is used to enhance the development of moral reasoning (Figure 1) in a manner that also accommodates some demonstration and assessment of related competencies.
- (iii)
- The more concrete, or surface level, processing incorporates rules (or legislation governing the practice of pharmacy) and codes of conduct or ethics, as generally included in professional ethics programs. However, the most difficult aspect of using professional codes as a framework for decision-making is that it is difficult to recognize when the endless variables in real-life scenarios, as included in a given dilemma scenario, are actually covered by the code. Practitioners typically engage surface-level moral reasoning when it accommodates the dilemma proposed and move to intermediate-level approaches only when a satisfactory action plan is not evident from the legislation or the professional Code of Conduct (CoC).
- Upon review of a previously unseen scenario (Appendix 1: Box 1), a student is forced to declare a “position” [31] when recording online her/his reflection or “independent review” of the dilemma therein (Appendix 1: Part 1). Constructivism, which proposes that learning is an active process, wherein new information is added to “prior knowledge”, which may have been derived from personal experience, as well as formal teaching and learning [26,27,32,33], is the key learning theory employed.
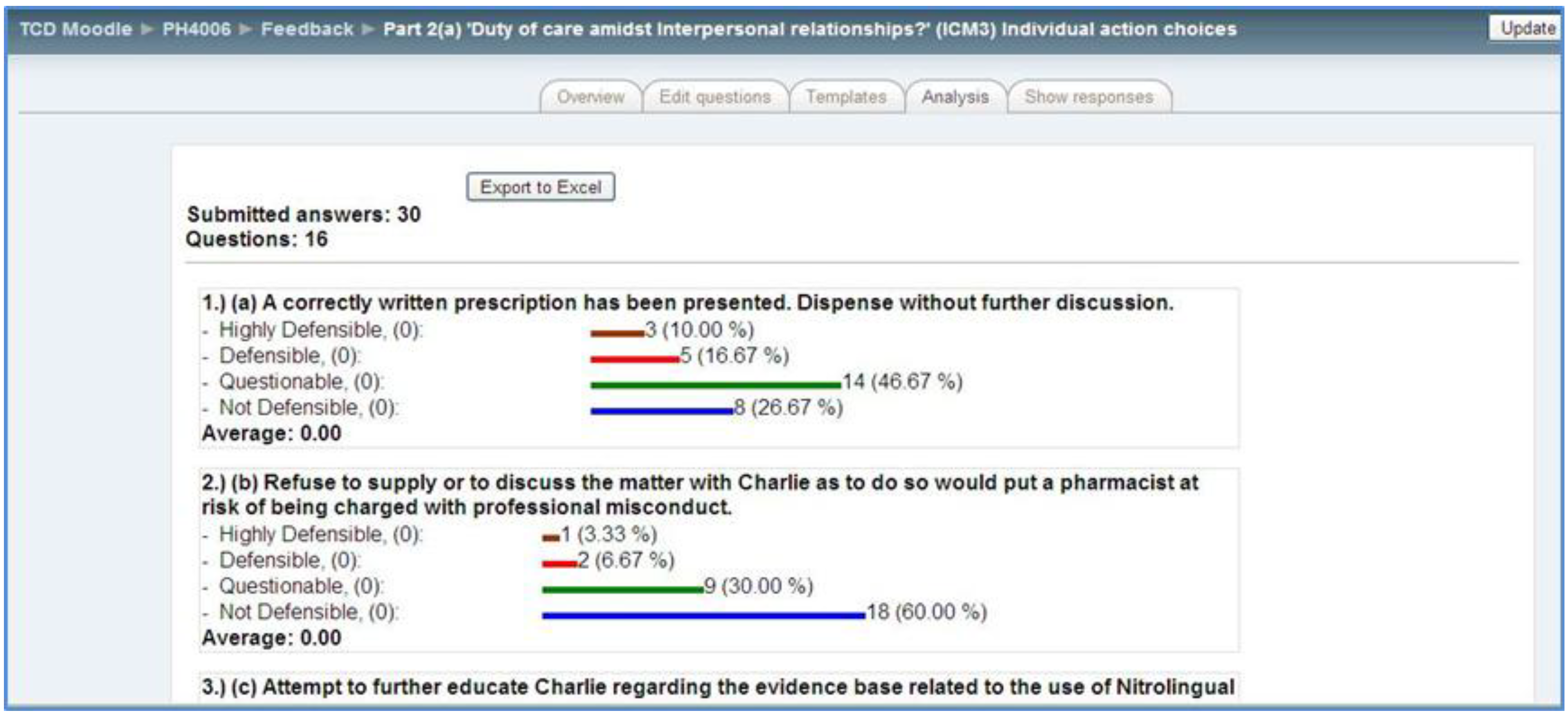
- The rating and ranking of action (Appendix 1: Part 2a) and justification options (Appendix 1: Part 2b) challenges the student to revisit the scenario, where the options posed prompt consideration of a broader range of potential professional concepts and dilemmas, while also forcing a choice between less than ideal circumstances. The discovery of “differences between expert and novice groups enables the educator to judge individual performance against a valid standard” [2] (p. 358), and the validation process grounds the ICM in the thinking and reasoning of respected practitioner and educator members of the profession, making it more likely to engage those undertaking professional ethics programs.
- Part 3 of the process randomly allocates students to groups of five to seven members, who, having committed to individual choices regarding the rating and ranking of action and justification options offered, must agree and make a group decision regarding the ranking process within a defined time frame. This inevitably involves constructivism in the form of negotiation and active discussion, debate and persuasion, as the group seeks to complete the task by the deadline imposed. Peer debate forces deeper reflection on the decisions made.
2. Technology-Enhanced Learning: Blended Learning in Pharmacy Ethics Education
- (i)
- Undergraduate level: a blended learning approach aligned with a series of workshops, each student generally having online access during the workshop(s).
- (a)
- ICM Part 1.
- (b)
- ICM Part 2: Rate and rank the action and justification options (Appendix 1).
- (c)
- ICM Part 3: group work.
- (ii)
- Post graduate MPharm: online learning while interns undertake a 12-month placement under the direction of a tutor at a location in the Republic of Ireland (ROI).

3. Summary
- The examples outlined all relate to the ROI and cultural/legal variations, including legislation specific to the medication(s) referred to in the scenario, must be considered before deciding whether these might be generalizable to other jurisdictions.
- Profession-specific intermediate concepts central to other professions may differ from those for pharmacy and need to be considered in order to write appropriate ICMs for educational initiatives other than for pharmacy or for multidisciplinary group work.
- The technology itself raises concerns: (1) Assessment strategies need to evolve to manage the risk of plagiarism and impersonation. (2) Technology creates a different communicative space, with a permanent record of all interactions. Educators have a responsibility to seek to protect these incoming students from naivety in this regard. (3) The VLE must be adapted to accommodate the automation of teaching and learning where viable. Reservations regarding reduction in group size derive at least partly from the time pressures (on tutors/academics moderating and/or assessing group work) associated with those changes. (4) Strict cut-off times mean that there will inevitably be late-comers, and the accommodation of these participants, essential where assessment is involved, can be challenging [39]. (5) It can be challenging to accommodate “repeat” assessments for individuals when the focus is on group work.
- Feedback from the students [39] highlights that the tutors must pay particular attention to netiquette guidelines that prompt timely engagement by all group members, so that those engaging in the early stages do not become prematurely disheartened with the online team work process.
- The potential for the FCM to be used as an overarching approach to professional ethics education in pharmacy, wherein all four components would be specifically targeted.
- The establishment of a multisite collaborative investigation of the use of these methodologies in undergraduate pharmacy education.
- The adaptation of the teaching and assessment techniques outlined in this article to continuing professional development initiatives for practicing pharmacists.
- The review of how these methodologies might be adapted to incorporate interprofessional and interdisciplinary learning through the use of multidisciplinary online groups.
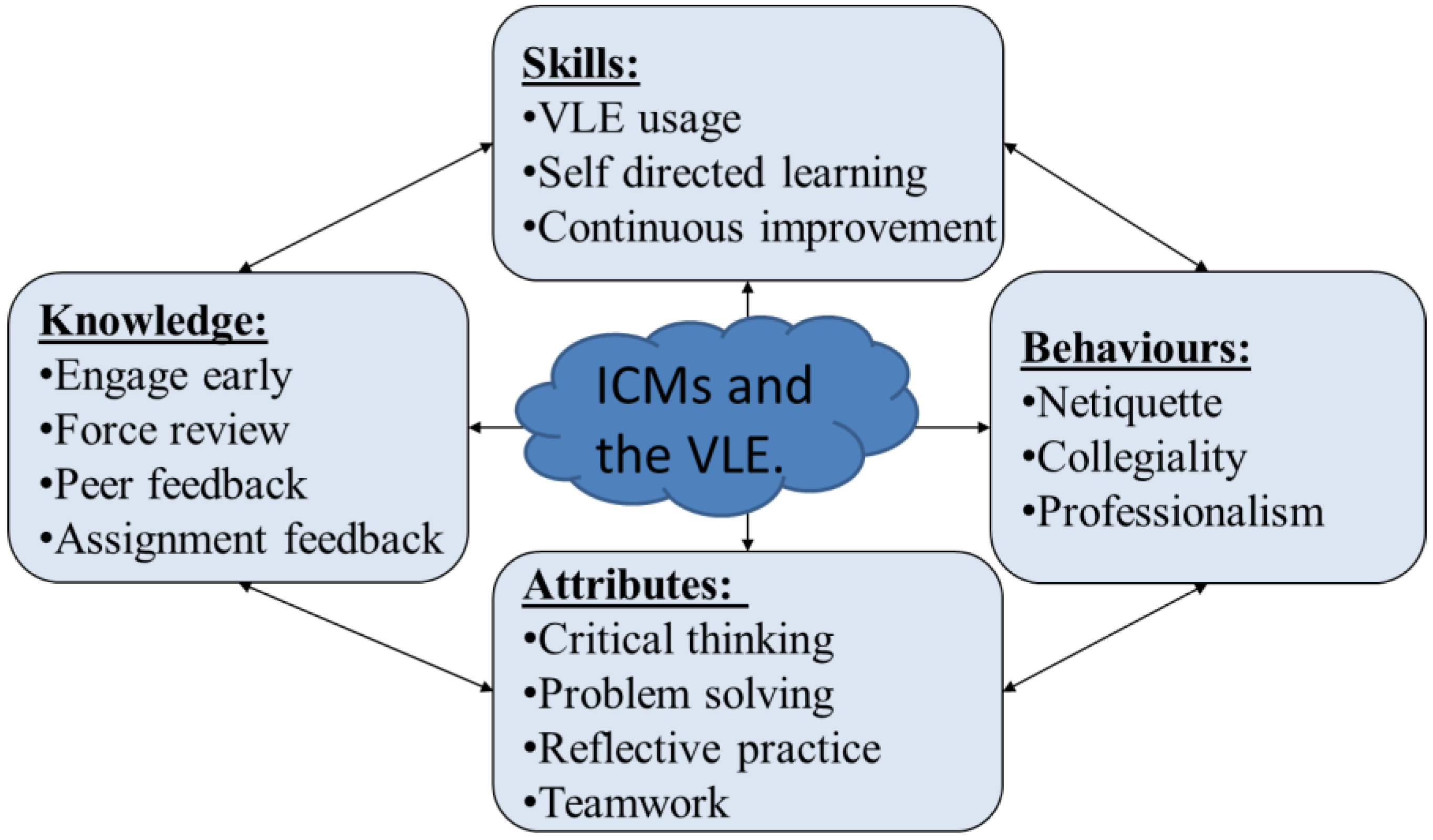
- The use of the VLE in online and blended learning programs merits further review as a means of supporting teaching and assessment methodologies aligned with competency-based assessment, such as those currently being introduced for pharmacy programs in the ROI [19]. The approaches used have the potential to support assessment challenges surrounding professional attributes, i.e., in order to assess competencies, the related behaviors must first be demonstrated in a manner that can be externally observed. The use of the online environment facilitates the demonstration of professional attributes, such as teamwork, in a manner that can be observed and assessed, even where resources (e.g., tutor time) are relatively restricted.
Acknowledgments
Author Contributions
Appendix 1
- (1)
- Nitrolingual spray contains glyceryl trinitrate 0.4 mg per metered dose, generally prescribed in cases of angina. It is sprayed under the tongue.
- (2)
- Solpadeine soluble contains paracetamol 500 mg, codeine phosphate 8 mg and caffeine 30 mg per tablet. If supplied (ROI), it must be sold by the pharmacist, having satisfied him/herself that it is in the patient’s best interests to do so.
- (1)
- What do you think is/are the main ethical concepts in this scenario?
- (2)
- What should pharmacist Celine do in this situation?
- (3)
- Justify your decision (as to what pharmacist Celine should do.).
- (4)
- What other action options might be taken?
- (5)
- How might other pharmacists justify these other action options?
- (a)
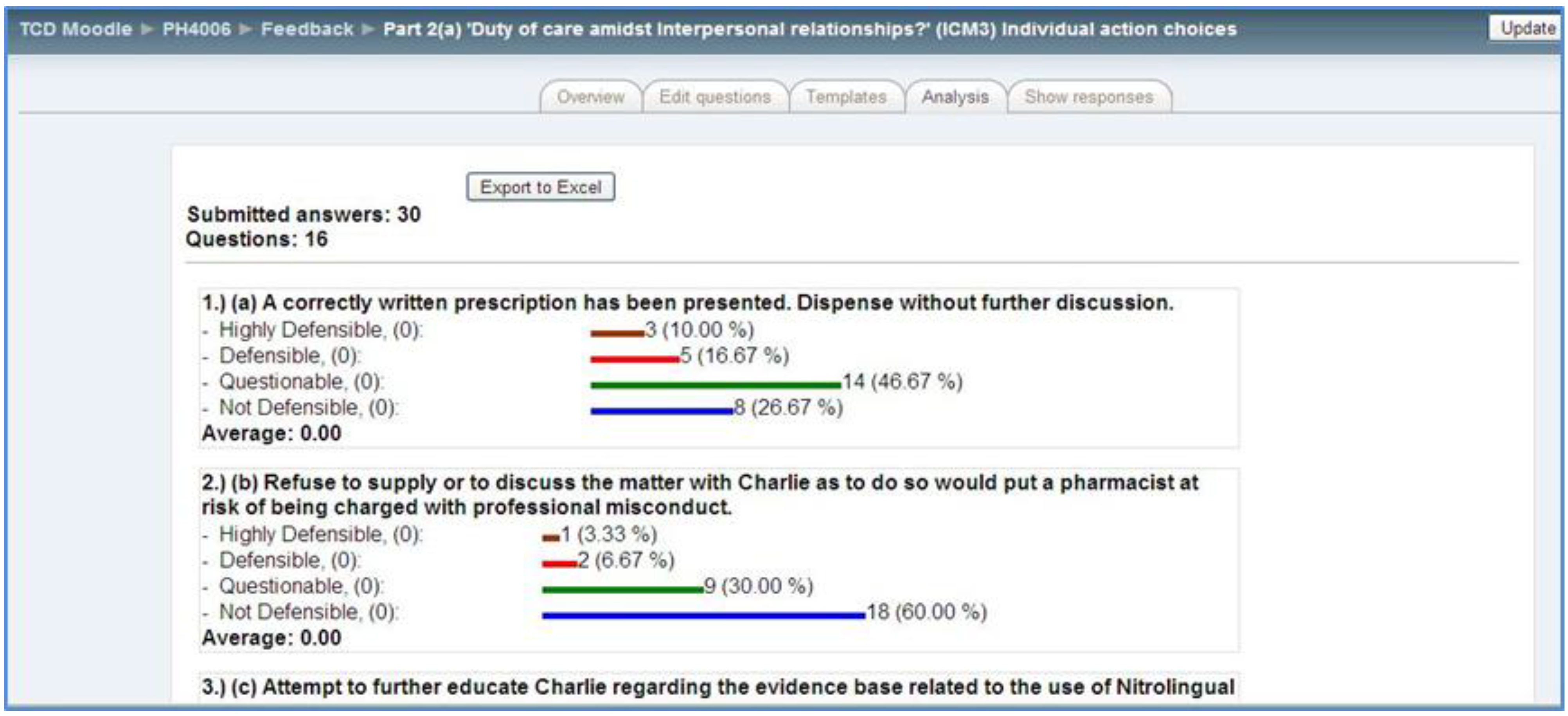
- HD D Q ND: A correctly written prescription has been presented. Dispense without further discussion.
- (b)
- HD D Q ND: Refuse to supply or to discuss the matter with Charlie, as to do so would put a pharmacist at risk of being charged with professional misconduct.
- (c)
- HD D Q ND: Attempt to further educate Charlie regarding the evidence base related to the use of Nitrolingual spray for angina and the use of codeine-containing products and give him contact details for the Irish Heart Foundation.
- (d)
- HD D Q ND: Supply one each of Nitrolingual spray and Solpadeine Soluble tablets.
- (e)
- HD D Q ND: Actively encourage Charlie to return to his GP or specialist and offer to phone him/her, the next morning, on behalf of Charlie.
- (f)
- HD D Q ND: Tell Charlie his right to do whatever he chooses is respected, but that continued use of the Nitrolingual spray, and providing Solpadeine, rather than paracetamol, will be more likely to do harm than good, so it would be against the professional Code of Conduct to supply them to him.
- (g)
- HD D Q ND: Report Charlie to the statutory body governing the profession.
- (h)
- HD D Q ND: Having confirmed that there is a very small amount of spray in one canister, tell Charlie that his self-prescribing of treatment for angina is of concern and that he needs to visit his medical advisor before any further supplies would be dispensed. Offer to supply paracetamol.
- (i)
- HD D Q ND: Having confirmed that there is a very small amount of spray in one canister, tell Charlie that neither product is in stock.
- (j)
- HD D Q ND: Phone Charlie’s GP or medical adviser to advise him/her of their colleague’s behavior.
- (k)
- HD D Q ND: Contact the pharmacist that dispensed the Nitrolingual spray on the previous occasion for further information, as you remember that she is the member of the staff with the most interest and expertise in matters related to heart disease.
- (l)
- HD D Q ND: Highlight to Charlie that his excess use of Nitrolingual spray may indicate the worsening of his underlying condition, that self-prescribing by doctors can indicate that they are not taking appropriate care of themselves and that to not insist on getting a prescription from his GP or cardiologist before supplying could put him at significant risk. You also offer to supply paracetamol.
| Select the three most preferred action options: | Select the three least preferred action options: |
| Most preferred action option ____ | Least preferred action option ____ |
| Second most preferred action option ____ | Second least preferred action option ____ |
| Third most preferred action option ____ | Third least preferred action option ____ |
- (a)
- G M S L N The pharmacist’s colleagues will not approve of her refusal to dispense a prescription written by a consultant.
- (b)
- G M S L N The practice of pharmacists subordinating their decision-making to the demands of other healthcare professionals in matters related to the supply of medicines should be resisted.
- (c)
- G M S L N The pharmacist is responsible for judging the scientific merit of a medicine, so must refuse to supply where questions arise.
- (d)
- G M S L N The supply of medicines as per written on the prescription in these circumstances could lead to a pharmacist being charged with professional misconduct, being called before the Statutory Body’s “Fitness-to-practice” committee and potentially struck off the professional register.
- (e)
- G M S L N The pharmacist should not let the patient control decisions to supply medicines under the pharmacist’s control.
- (f)
- G M S L N It is the pharmacist’s professional duty to alert the Statutory Body to the doctor’s behavior.
- (g)
- G M S L N Where a patient does not appear to understand the risks he may face if he continues to use particular medicines when he is not under medical supervision, it is the pharmacist’s professional responsibility to try to ensure he is informed.
- (h)
- G M S L N Pharmacists ought to accommodate patients who are in urgent need of prescription medicines, especially where they have been previously dispensed at the pharmacy, as they risk unnecessarily upsetting regular customers of the pharmacy by being inflexible.
- (i)
- G M S L N The patient does not appear to understand the gravity of the healthcare situation he faces or the implications of failing to access specialist advice.
- (j)
- G M S L N If the patient is adamant about a decision and has been properly educated and warned of the consequences, then the pharmacist should not interfere.
- (k)
- G M S L N In the long run, it is better to give up a little professional rigor than to have the doctor complain about what he considers to be unreasonable behavior.
- (l)
- G M S L N The pharmacist’s primary concern should be the welfare of the patient, and this permits him/her to breach confidentiality.
| Select the three most preferred justification: | Select the three least preferred justifications: |
| Most preferred justification option ____ | Least preferred justification option ____ |
| Second most preferred justification ____ | Second least preferred justification____ |
| Third most preferred justification ____ | Third least preferred justification ____ |
Appendix 2

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ph4006: V2:11/8/2012CR | Rubric ICM Part 1: Emphasis on individual constructivism and critical and integrative thinking | Total % | ||||
|---|---|---|---|---|---|---|
| Student name | ||||||
| Criteria | Excellent I: 70%–100% | Very good II.I: 60%–69% | Good II.2: 50%–59% | Fair III: 40%–49% | Weak F: Below 39% | |
| Ethical concepts in the scenario and what leads to a dilemma | Comprehensive and accurate coverage of the concepts in the scenario and the dilemma itself and clear linkage with values in the CoC, principlism, relevant legislation and issues of consent and confidentiality as appropriate. | Accurate and well informed regarding concepts in the scenario and the dilemma itself and links with CoC or frameworks for decision-making with some omissions or errors. | Generally accurate with respect to identification of concepts with some omissions or errors. Poor linkage with CoC, principlism or legislation as appropriate. | Does not directly address the concepts, the dilemma or link with CoC, principlism or legislation as appropriate. | Does not address the concepts in the dilemma. | |
| Engages with the analysis of the scenario and the process of reasoning through a dilemma in a constructive manner | Actively seeks to reflect, identifies the ethical dilemma and reasons towards a reasonable action option in a justifiable manner. | Seeks to reflect, identifies the ethical dilemma and to reason towards a reasonable action option in a justifiable manner. | Generally seeks to increase understanding and reason towards a reasonable action option without specifically justifying the choice made. | States own opinions and choices rather than seeking to explain a reasoned action option. | No evidence of trying to develop a reasoned approach to choosing an action option. | |
| Participation in the process of critical review in a professional manner | Netiquette (online etiquette) evident at all times. Answers all 5 questions and offers a critical analysis of the scenario and introduces a different interpretation to an existing idea. | Netiquette (online etiquette) evident most of the time. Answers all 5 questions and offers some analysis of the scenario and introduces personal interpretation to an existing idea. | Netiquette (online etiquette) evident, but some risk of breaches. Answers all 5 questions and offers some analysis of the scenario or introduces personal interpretation to an existing idea. | Netiquette (online etiquette) breached but later amended. Contributes to all 5 questions, generally relating answers to questions posed. | Netiquette (online etiquette) guidelines breached. Omits some questions and/or does not answer the questions posed. | |
| Makes and justifies decisions in a manner that reflects the statutory Code of Conduct for pharmacists and pharmacy and medicines law. | Makes decisions that reflect the values in the CoC, relevant legislation and issues of consent and confidentiality as appropriate. Demonstrates understanding of how poor professional decision-making might arise and how pharmacists might try to justify same. | Makes decisions that reflect the CoC, relevant legislation and/or issues of consent and confidentiality with some omissions or errors. Demonstrates understanding of how poor professional decision-making might arise or how pharmacists might try to justify same. | Makes decisions that poorly reflect the CoC, relevant legislation and/or issues of consent and confidentiality. States examples of alternate decisions that might be taken without specifying how pharmacists might try to justify same. | Makes decisions that do not reflect the CoC, relevant legislation and/or issues of consent and confidentiality. Gives one example of an alternate decision that might be taken but does not clarify how a pharmacist might try to justify same. | Makes decisions that contradict the CoC, relevant legislation and/or issues of consent and confidentiality. Examples of alternate actions and/or justifications are not plausible in the context of pharmacy practice. | |
| Expression. (Note: spelling and grammar not penalized.) | 50–100 words. Expresses ideas clearly, concisely and cogently, in logical fashion. | 100–150 words. Ideas are readily understood and reasonably organized. | 150––00 words. Ideas are readily understood, but shows signs of disorganization. | Over 200 words. Only an occasional idea surfaces clearly. | Over 250 words. Writing is largely unintelligible. | |
| Feedback: | ||||||
| Overall Grade: | ||||||
| Acknowledgement | Trinity College Dublin (TCD) Guidelines on Awarding Grades for Essays and Examinations [40]. Dublin City University (DCU) Using marking schemes/rubrics—DCU [41]. | |||||
| Prepared by: | Cicely Roche MPSI, School of Pharmacy, TCD: 11 August 2012 | V2: PH4006 | ||||
Appendix 3
| Ph4006: V2:11/8/2012CR | Rubric ICM Part 3: Emphasis on social constructivism | Total % | ||||
|---|---|---|---|---|---|---|
| Student name | ||||||
| Criteria | Excellent I: 70%–100% | Very good II.I: 60%–69% | Good II.2: 50%–59% | Fair III: 40%–49% | Weak F: Below 39% | |
| Criteria | Excellent I: 70%–100% | Very good II.I: 60%–69% | Good II.2: 50%–59% | Fair III: 40%–49% | Weak F: Below 39% | |
| Engages with the opinions of others; negotiates towards consensus. | Engages well with the opinions of others and furthers this by expressing examples of his/her own opinion. Actively seeks to reflect, demonstrates empathy and seeks to reason towards group consensus. Demonstrates influencing and negotiation skills to resolve potential conflicts or if conflict arises. | Engages well but with some omissions. Seeks to reflect, to demonstrate empathy and to reason towards group consensus when others lead. Demonstrates influencing or negotiation skills to resolve conflict if it arises. | Generally engages with some missed opportunities to engage. Generally seeks to increase understanding and reason towards group consensus with occasional lapses. Recognizes the conflict but does not actively help to resolve it. | Does not directly address the opinions of other students. Restates own opinions and choices rather than engage with other’s opinions. Restates own opinions and choices if conflict arises. | No evidence of engagement with other students. No evidence of engagement with other students’ opinions. Avoids conflict if it arises. | |
| Content: Use of sources. | Comprehensive and accurate coverage of the concepts in the dilemma. Clarifies queries that arise in the forum. Always references sources correctly. | Accurate and well informed regarding concepts in the dilemma. References are correct but not integrated with the argument. | Generally accurate with some omissions or errors. References are correct but rarely used. | Does not directly address the concepts for discussion. References are frequently incorrect. | Does not address the concepts in the dilemma. Does not reference sources. | |
| Participation in the process in a respectful manner. | Netiquette evident at all times. Timely contributions and evidence of reflective “listening” on a consistent basis. | Netiquette evident most of the time. Timely contributions and evidence of reflective “listening” most of the time. | Netiquette evident, but some risk of breached. Participation is spotty; picks and chooses topics to get involved in; rare evidence of reflective “listening”. | Netiquette breached but later apologizes. Student rarely participates freely; makes short remarks that have some limited relevance. | Netiquette guidelines breached. Student rarely participates freely; has not made the requisite number of posts (3). | |
| Review of Part A of ICM (and inclusion, in order of preference, of most and least preferred action options). | 125–175 words. Evidence of engagement with rubric Part A is excellent and grade category proposed for all categories. Includes all “most and least” preferred options and order of preference is clear to reader. | 175–200 words. Evidence of engagement with all rubric Part A is present and grade category proposed for all categories. Includes all of “most and least” preferred options but order is unclear. | 200–250 words. Evidence of engagement with rubric Part A is patchy; grades proposed for some categories. Includes majority of “most and least” preferred options. | Over 250 words.Evidence of engagement with rubric Part A is vague and grade not/incompletely proposed. Includes some of “most and least” preferred options. | Over 300 words.Evidence of engagement with rubric Part A is not included. Does not include “most and least” preferred options. | |
| Feedback: | ||||||
| Overall Grade: | ||||||
| Acknowledgement | Trinity College Dublin (TCD) Guidelines on Awarding Grades for Essays and Examinations [40]. Dublin City University (DCU) Using marking schemes/rubrics—DCU [41]. | |||||
| Prepared by: | Cicely Roche MPSI, School of Pharmacy, Trinity College Dublin 11 August 2012 | V2: PH4006 | ||||
Conflicts of Interest
References
- Thoma, S.J.; Bebeau, M.J.; Bolland, A. The role of moral judgment in context—Specific professional decision making. In Getting Involved: Global Citizenship Development and Sources of Moral Values; Sense Publishers: Amsterdam, The Netherlands, 2008; pp. 147–160. [Google Scholar]
- Bebeau, M.J.; Thoma, S.J. “Intermediate” concepts and the connection to moral education. Educ. Psycol. Rev. 1999, 11, 343–360. [Google Scholar] [CrossRef]
- Bebeau, M.J. The defining issues test and the four component model: Contributions to professional education. J. Moral Educ. 2002, 31, 271–291. [Google Scholar] [CrossRef]
- Rest, J.; Narvaez, D.; Bebeau, M.J.; Thoma, S.J. Post-conventional Moral Thinking: A Neo-Kohlbergian Approach; Erlbaum: Mahwah, NJ, USA, 1999. [Google Scholar]
- Rest, J.R.; Narvaez, D. Moral Development in the Professions: Psychology and Applied Ethics; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1994. [Google Scholar]
- Bebeau, M.J.; Monson, V.E. Guided by theory, grounded in evidence: A way forward for professional ethics education. In Handbook on Moral and Character Education; Nucci, L., Narvaez, D., Eds.; Routledge: New York, NY, USA, 2008. [Google Scholar]
- Thoma, S.J.; Mahwah, N.J. Research on the defining issues test. In Handbook of Moral Development; Killen, M., Smetana, J.G., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2006; pp. 67–92. [Google Scholar]
- Roche, C.; Kelliher, F. Giving “best advice”: Proposing a framework of community pharmacist professional judgement formation. Pharmacy 2014, 2, 1–12. [Google Scholar]
- Chaar, B. Decisions, decisions: Ethical dilemmas in practice (or how to pass the “Red Face Test”). Aust. Pharm. 2006, 25, 444–449. [Google Scholar]
- Chaar, B. Legislative change in Australian pharmacy—History in the making. Aust. Pharm. 2010, 29, 198–199. [Google Scholar]
- Roche, C.; Kelliher, F. Exploring the patient consent process in community pharmacy practice. J. Bus. Ethics 2009, 86, 91–99. [Google Scholar] [CrossRef]
- Cooper, R.J.; Bissell, P.; Wingfield, J. “Islands” and the “Doctor’s Tool”: The ethical significance of isolation and subordination in UK community pharmacy. Health 2009, 13, 297–316. [Google Scholar]
- Cooper, R.J.; Bissell, P.; Wingfield, J. Ethical decision-making, passivity and pharmacy. J. Med. Ethics. 2008, 34, 441–445. [Google Scholar] [CrossRef]
- Cooper, R.J.; Bissell, P.; Wingfield, J. Ethical, religious and factual beliefs about the supply of emergency hormonal contraception by UK community pharmacists. J. Fam. Plan. Reprod. Health Care 2008, 34, 47–50. [Google Scholar] [CrossRef]
- Cooper, R.J.; Bissell, P.; Wingfield, J. Dilemmas in dispensing, problems in practice? Ethical issues and law in UK community pharmacy. Clin. Ethics 2007, 2, 1–6. [Google Scholar] [CrossRef]
- Benson, A.; Cribb, A.; Barber, N. Understanding pharmacists’ values: A qualitative study of ideals and dilemmas in UK pharmacy practice. Soc. Sci. Med. 2009, 68, 2223–2230. [Google Scholar] [CrossRef]
- Latif, D.A. The relationship between pharmacists’ tenure in the community setting and moral reasoning. J. Bus. Ethics 2001, 31, 131–141. [Google Scholar] [CrossRef]
- Latif, D.A. Cognitive moral development and pharmacy education. Amer. J. Pharm. Educ. 2000, 64, 451–454. [Google Scholar]
- Pharmaceutical Society of Ireland (PSI). Core Competency Framework for Pharmacists. 2009. Available online: http://www.thepsi.ie/gns/home.aspx (accessed on 31 December 2013).
- Wingfield, J.; Bissell, P.; Anderson, C. The Scope of pharmacy ethics—An evaluation of the international research literature, 1990–2002. Soc. Sci. Med. 2004, 58, 2383–2396. [Google Scholar] [CrossRef]
- Roche, C. Ethical and legal issues in healthcare: Residential care: Pharmacist dilemmas and issue of “covert” medication. Iran. Pharm. J. 2010, 87, pp. 203–204. Available online: http://www.thepsi.ie/tns/publications/irish-pharmacy-journal/ethics-articles.aspx (accessed on 31 December 2013).
- Sanghavi, N. Pharmacy in a new age commercial environment. Pharm. J. 1995, 255, 615–618. [Google Scholar]
- Szeinbach, S.L.; Barnes, J.H.; Summers, K.L.; Benjamin, B.F., III. The changing retail environment: Its influence on professionalism in chain and independently owned pharmacies. J. Appl. Bus. Res. 1994, 11, 5–15. [Google Scholar]
- Swisher, L.L.; van Kessel, G.; Jones, M.; Beckstead, J.; Edwards, I. Evaluating moral reasoning outcomes in physical therapy ethics education: Stage, schema, phase and type. Phys. Ther. Rev. 2012, 17, 167–175. [Google Scholar] [CrossRef]
- Jones, D. A novel approach to business ethics training: Improving moral reasoning in just a few weeks. J. Bus. Ethics 2008, 88, 367–379. [Google Scholar] [CrossRef]
- Treleaven, L.; Voola, R. Integrating the development of graduate attributes through constructive alignment. J. Market. Educ. 2009, 30, 160–173. [Google Scholar] [CrossRef]
- Biggs, J. Constructing learning by aligning teaching: Constructive alignmen. In Teaching for Quality Learning at University, 2nd ed.; SRHE and Open University Press: Berkshire, UK, 2004; pp. 11–33. [Google Scholar]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics; Oxford University Press: New York, NY, USA, 2009. [Google Scholar]
- Pharmaceutical Society of Ireland (PSI). Code of Conduct for Pharmacists. Available online: http://www.thepsi.ie/gns/home.aspx (accessed on 31 December 2013).
- Wingfield, J.; Badcott, D. Pharmacy Ethics and Decision Making; Pharmaceutical Press: London, UK, 2007. [Google Scholar]
- Hew, K.F.; Cheung, W.S. Student facilitators’ habits of mind and their influences on higher-levelknowledge construction occurrences in online discussions: A case study. Innov. Educ. Teach. Intern. 2011, 48, 275–285. [Google Scholar] [CrossRef]
- Sthapornnanon, N.; Sakulbumrungsil, R.; Theeraroungchaisri, A.; Watcharadamrongkun, S. Social constructivist learning environment in an online professional practice course. In Am. J. Pharm. Educ.; 2009; 73, pp. 1–11. Available online: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2690880/ (accessed on 25 April 2014). [Google Scholar]
- Huball, H.; Burt, H. An integrated approach to developing and implementing learning centred curricula. Int. J. Acad. Dev. 2004, 1, 51–65. [Google Scholar] [CrossRef]
- Hrastinski, S. A theory of online learning as online participation. Comput. Educ. 2009, 52, 78–82. [Google Scholar] [CrossRef]
- Feinberg, Jonathan. WordleTM. Available online: http://www.wordle.net/ (accessed on 25 April 2014).
- Roche, C. Technology Enhanced Pharmacy Education: Using the Virtual Learning Environment to Support the Development of Professional Attributes. Poster Presentation. In Proceedings of the International Pharmaceutical Federation (FIP) 73rd World Congress, Amsterdam, Netherlands, 3–8 October 2012.
- Roche, C.; Gallagher, P. Developing moral reasoning skills in the virtual learning environment (VLE). Poster Presentation. In Proceedings of the Association for Medical Education in Europe (AMEE) Annual Conference, Glasgow, Scotland, 4–8 September 2010.
- Roche, C.; Gallagher, P. Technology Enhanced Development of Moral Reasoning Competencies in Pharmacist Interns: Stimulating Their Engagement in Dilemma Review and Resolution in the Online Environment. Oral Presentation. In Proceedings of the International Pharmaceutical Federation (FIP) 73rd World Congress, Amsterdam, Netherlands, 3–8 October 2012.
- Roche, C. Formative Assessment for “Graduate Attributes”: Technology-Enhanced Learning in the First Semester. Proceedings of the Edulearn12 Conference Proceedings, Barcelona, Spain, 1–3 July 2012; Available online: http://library.iated.org/view/ROCHE2012FOR (accessed on 23 February 2014).
- Trinity College Dublin School of Pharmacy and Pharmaceutical Sciences (B.Sc.Pharm) Degree Course Student Handbook 2012–2013. Available online: http://pharmacy.tcd.ie/assets/pdf/Student%20Handbook%20%202012%2013%20FINAL.pdf (accessed on 25 April 2014).
- Dublin City University. Using marking schemes/rubrics—DCU. 2014. Available online: http://pharmacy.tcd.ie/assets/pdf/Student%20Handbook%20%202012%2013%20FINAL.pdf (accessed on 25 April 2014).
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Roche, C.; Thoma, S.; Wingfield, J. From Workshop to E-Learning: Using Technology-Enhanced “Intermediate Concept Measures” As a Framework for Pharmacy Ethics Education and Assessment. Pharmacy 2014, 2, 137-160. https://doi.org/10.3390/pharmacy2020137
Roche C, Thoma S, Wingfield J. From Workshop to E-Learning: Using Technology-Enhanced “Intermediate Concept Measures” As a Framework for Pharmacy Ethics Education and Assessment. Pharmacy. 2014; 2(2):137-160. https://doi.org/10.3390/pharmacy2020137
Chicago/Turabian StyleRoche, Cicely, Steve Thoma, and Joy Wingfield. 2014. "From Workshop to E-Learning: Using Technology-Enhanced “Intermediate Concept Measures” As a Framework for Pharmacy Ethics Education and Assessment" Pharmacy 2, no. 2: 137-160. https://doi.org/10.3390/pharmacy2020137
APA StyleRoche, C., Thoma, S., & Wingfield, J. (2014). From Workshop to E-Learning: Using Technology-Enhanced “Intermediate Concept Measures” As a Framework for Pharmacy Ethics Education and Assessment. Pharmacy, 2(2), 137-160. https://doi.org/10.3390/pharmacy2020137