The Effects of Laparoscopic Sleeve Gastrectomy on the Parameters of Leptin Resistance in Obesity

 , ,
, ,
Abstract
1. Introduction
2. Subjects and Methods
2.1. Surgery
2.2. Measurement of Serum Leptin and Leptin Receptor Levels
2.3. Statistical Analysis
3. Results
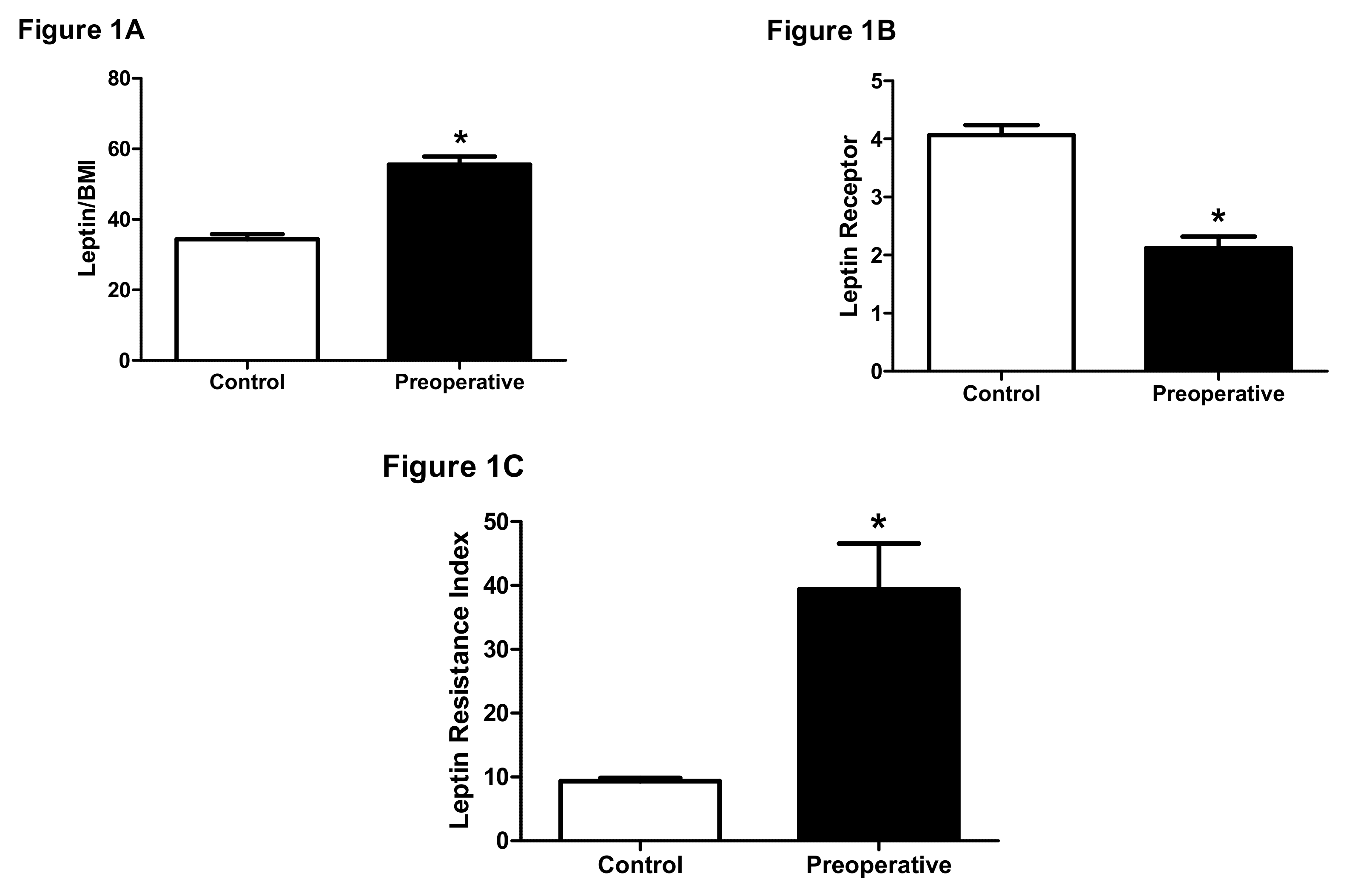
3.1. Parameters of Leptin Resistance are Different Between Normal and Obese Individuals
3.2. LSG Improves Parameters of Leptin Resistance in Obese Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rocha, V.Z.; Libby, P. Obesity, inflammation, and atherosclerosis. Nat. Rev. Cardiol. 2009, 6, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Kotsis, V.; Stabouli, S.; Papakatsika, S.; Rizos, Z.; Parati, G. Mechanisms of obesity-induced hypertension. Hypertens. Res. 2010, 33, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Golay, A.; Ybarra, J. Link between obesity and type 2 diabetes. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 649–663. [Google Scholar] [CrossRef] [PubMed]
- Leach, R.; Kalamara, E.; Shayeghi, M. The worldwide obesity epidemic. Obes. Res. 2001, 9, 228–233. [Google Scholar]
- Yang, L.; Colditz, G.A. Prevalence of Overweight and Obesity in the United States, 2007–2012. JAMA Intern. Med. 2015, 175, 1412–1413. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; El-Hamdouchi, A.; Diouf, A.; Monyeki, A.; A Somda, S. Determining the worldwide prevalence of obesity. Lancet 2018, 391, 1773–1774. [Google Scholar] [CrossRef]
- Tremmel, M.; Gerdtham, U.-G.; Nilsson, P.M.; Saha, S. Economic Burden of Obesity: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2017, 14, 435. [Google Scholar] [CrossRef]
- Malik, V.S.; Willett, W.C.; Hu, F.B. Global obesity: Trends, risk factors and policy implications. Nat. Rev. Endocrinol. 2013, 9, 13–27. [Google Scholar] [CrossRef]
- Bell, C.G.; Walley, A.J.; Froguel, P. The genetics of human obesity. Nat. Rev. Genet. 2005, 6, 221–234. [Google Scholar] [CrossRef]
- Farooqi, I.S.; O’Rahilly, S. Genetics of Obesity in Humans. Endocr. Rev. 2006, 27, 710–718. [Google Scholar] [CrossRef]
- Krude, H.; Biebermann, H.; Schnabel, D.; Tansek, M.Z.; Theunissen, P.; Mullis, P.E.; Grüters, A. Obesity Due to Proopiomelanocortin Deficiency: Three New Cases and Treatment Trials with Thyroid Hormone and ACTH4–10. J. Clin. Endocrinol. Metab. 2003, 88, 4633–4640. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.S.; Creemers, J.W.; Ohagi, S.; Raffin-Sanson, M.-L.; Sanders, L.; Montague, C.T.; Hutton, J.C.; O’Rahilly, S. Obesity and impaired prohormone processing associated with mutations in the human prohormone convertase 1 gene. Nat. Genet. 1997, 16, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Proença, R.; Maffei, M.; Barone, M.; Leopold, L.; Friedman, J.M. Positional cloning of the mouse obese gene and its human homologue. Nature 1994, 372, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Lindström, P. The Physiology of Obese-Hyperglycemic Mice [ob/ob Mice]. Sci. World J. 2007, 7, 666–685. [Google Scholar] [CrossRef] [PubMed]
- Kershaw, E.E.; Flier, J.S. Adipose Tissue as an Endocrine Organ. J. Clin. Endocrinol. Metab. 2004, 89, 2548–2556. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Joseph, F. Adipose Tissue and Adipokines: The Association with and Application of Adipokines in Obesity. Science 2014, 2014, 328592. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.L.; DePaoli, A.M.; Lee, J.H.; Mantzoros, C.S. Leptin Hormonal Kinetics in the Fed State: Effects of Adiposity, Age, and Gender on Endogenous Leptin Production and Clearance Rates. J. Clin. Endocrinol. Metab. 2004, 89, 2672–2677. [Google Scholar] [CrossRef]
- Klok, M.D.; Jakobsdottir, S.; Drent, M.L. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: A review. Obes. Rev. 2007, 8, 21–34. [Google Scholar] [CrossRef]
- Havel, P.J. Role of adipose tissue in body-weight regulation: Mechanisms regulating leptin production and energy balance. Proc. Nutr. Soc. 2000, 59, 359–371. [Google Scholar] [CrossRef]
- Clément, K.; Vaisse, C.; Lahlou, N.; Cabrol, S.; Pelloux, V.; Cassuto, D.; Gourmelen, M.; Dina, C.; Chambaz, J.; Lacorte, J.-M.; et al. A mutation in the human leptin receptor gene causes obesity and pituitary dysfunction. Nature 1998, 392, 398–401. [Google Scholar] [CrossRef]
- Funcke, J.-B.; Von Schnurbein, J.; Lennerz, B.; Lahr, G.; Debatin, K.-M.; Fischer-Posovszky, P.; Wabitsch, M. Monogenic forms of childhood obesity due to mutations in the leptin gene. Mol. Cell. Pediatr. 2014, 1, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Maffei, M.; Halaas, J.; Ravussin, E.; Pratley, R.; Lee, G.; Zhang, Y.; Fei, H.; Kim, S.; Lallone, R.; Ranganathan, S.; et al. Leptin levels in human and rodent: Measurement of plasma leptin and ob RNA in obese and weight-reduced subjects. Nat. Med. 1995, 1, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Considine, R.V.; Sinha, M.K.; Kriauciunas, A.; Nyce, M.R.; Ohannesian, J.P.; Marco, C.C.; McKee, L.J.; Bauer, T.L.; Heiman, M.L.; Stephens, T.W.; et al. Serum Immunoreactive-Leptin Concentrations in Normal-Weight and Obese Humans. N. Engl. J. Med. 1996, 334, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Webb, V.L.; Moran, C.H.; Bailer, B.A. Lifestyle modification for obesity: New developments in diet, physical activity, and behavior therapy. Circulation 2012, 125, 1157–1170. [Google Scholar] [CrossRef] [PubMed]
- Apolzan, J.W.; Venditti, E.M.; Edelstein, S.L.; Knowler, W.C.; Dabelea, D.; Boyko, E.J.; Pi-Sunyer, X.; Kalyani, R.R.; Franks, P.W.; Srikanthan, P.; et al. Long-Term Weight Loss With Metformin or Lifestyle Intervention in the Diabetes Prevention Program Outcomes Study. Ann. Intern. Med. 2019, 170, 682–690. [Google Scholar] [CrossRef]
- Wolfe, B.M.; Kvach, E.; Eckel, R.H. Treatment of Obesity: Weight Loss and Bariatric Surgery. Circ. Res. 2016, 118, 1844–1855. [Google Scholar] [CrossRef]
- Albaugh, V.L.; Flynn, C.R.; Tamboli, R.A.; Abumrad, N.N. Recent advances in metabolic and bariatric surgery. F1000Research 2016, 5, 978. [Google Scholar] [CrossRef] [PubMed]
- Ganiyu, A.B.; Mabuza, L.H.; Malete, N.H.; Govender, I.; Ogunbanjo, G.A. Non-adherence to diet and exercise recommendations amongst patients with type 2 diabetes mellitus attending Extension II Clinic in Botswana. Afr. J. Prim. Health Care Fam. Med. 2013, 5, 457. [Google Scholar] [CrossRef]
- Rodgers, R.J.; Tschöp, M.H.; Wilding, J.P.H. Anti-obesity drugs: Past, present and future. Dis. Models Mech. 2012, 5, 621–626. [Google Scholar] [CrossRef]
- Maciejewski, M.L.; Arterburn, D.E.; van Scoyoc, L.; Smith, V.A.; Yancy, W.S.; Weidenbacher, H.J.; Livingston, E.H.; Olsen, M.K. Bariatric Surgery and Long-term Durability of Weight Loss. JAMA Surg. 2016, 151, 1046–1055. [Google Scholar] [CrossRef]
- Ulker, İ.; Yildiran, H. The effects of bariatric surgery on gut microbiota in patients with obesity: A review of the literature. Biosci. Microbiota Food Health 2019, 38, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Berthoud, H.-R.; Shin, A.C.; Zheng, H. Obesity surgery and gut-brain communication. Physiol. Behav. 2011, 105, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Quercia, I.; Dutia, R.; Kotler, D.P.; Belsley, S.; Laferrere, B. Gastrointestinal changes after bariatric surgery. Diabetes Metab. 2014, 40, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Al Maskari, M.Y.; A Alnaqdy, A. Correlation between Serum Leptin Levels, Body Mass Index and Obesity in Omanis. Sultan Qaboos Univ. Med. J. [SQUMJ] 2006, 6, 27–31. [Google Scholar] [PubMed]
- Bakari, A. Relationship between leptin and indices of obesity among apparently healthy adults in Kano, Northwestern Nigeria. Int. J. Med. Sci. Public Health 2015, 4, 1–10. [Google Scholar] [CrossRef]
- Sáinz, N.; Barrenetxe, J.; Moreno-Aliaga, M.J.; Martínez, J.A. Leptin resistance and diet-induced obesity: Central and peripheral actions of leptin. Metabolism 2015, 64, 35–46. [Google Scholar] [CrossRef]
- Villanueva, E.C.; Myers, M.G., Jr. Leptin receptor signaling and the regulation of mammalian physiology. Int. J. Obes. 2008, 32 (Suppl. 7), 8–12. [Google Scholar] [CrossRef]
- Pories, W.J.; Swanson, M.S.; Macdonald, K.G.; Long, S.B.; Morris, P.G.; Brown, B.M.; Barakat, H.A.; Deramon, R.A.; Israel, G.; Dolezal, J.M.; et al. Who Would Have Thought It? An Operation Proves to Be the Most Effective Therapy for Adult-Onset Diabetes Mellitus. Ann. Surg. 1995, 222, 339–352. [Google Scholar] [CrossRef]
- Khalaf, K.I.; Taegtmeyer, H. Clues from bariatric surgery: Reversing insulin resistance to heal the heart. Curr. Diabetes Rep. 2013, 13, 245–251. [Google Scholar] [CrossRef]
- Carvalheira, J.B.; Torsoni, M.A.; Ueno, M.; Amaral, M.E.; Araújo, E.P.; Velloso, L.A.; Gontijo, J.A.; Saad, M.J. Cross-Talk between the Insulin and Leptin Signaling Systems in Rat Hypothalamus. Obes. Res. 2005, 13, 48–57. [Google Scholar] [CrossRef]
- Morrison, C.D.; Huypens, P.; Stewart, L.K.; Gettys, T.W. Implications of crosstalk between leptin and insulin signaling during the development of diet-induced obesity. Biochim. Biophys. Acta 2009, 1792, 409–416. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Cases | |||
|---|---|---|---|
| Controls | Preoperative | Postoperative | |
| Number | 75 | 38 | |
| Age (Mean ± SD) | 23.05 ± 2.44 | 37.26 ± 11.29 | |
| Gender Male (%) Female (%) | 45 (60) 30 (40) | 10 (26) 28 (74) | |
| Comorbidity Diabetes Mellitus (%) Hypothyroidism (%) | 0 (0) 0 (0) | 7 (18) 5 (13) | |
| BMI (Mean ± SD) | 22.43 ± 0.56 | 43.00 ± 0.73 | 30.82 ± 0.73 |
| Cases | |||
|---|---|---|---|
| Controls | Preoperative | Postoperative | |
| Serum leptin concentrations (pg/mL) | |||
| Minimum | 219.0 | 1196 | 905.0 |
| Median | 764.0 | 2294 | 1282 |
| Maximum | 1701 | 3314 | 1942 |
| Mean | 772.7 | 2369 | 1306 |
| Std. Deviation | 291.5 | 566.3 | 292.6 |
| Std. Error | 33.67 | 91.86 | 47.47 |
| Serum leptin receptor concentrations (ng/mL) | |||
| Minimum | 1.600 | 0.3000 | 2.200 |
| Median | 4.000 | 2.050 | 2.900 |
| Maximum | 8.300 | 5.900 | 3.900 |
| Mean | 4.063 | 2.121 | 2.942 |
| Std. Deviation | 1.531 | 1.213 | 0.4494 |
| Std. Error | 0.1767 | 0.1968 | 0.07290 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazahreh, T.S.; Alfaqih, M.; Saadeh, R.; Al-Zoubi, N.A.; Hatamleh, M.; Alqudah, A.; Aleshawi, A.J.; Alzoubi, A. The Effects of Laparoscopic Sleeve Gastrectomy on the Parameters of Leptin Resistance in Obesity. Biomolecules 2019, 9, 533. https://doi.org/10.3390/biom9100533
Mazahreh TS, Alfaqih M, Saadeh R, Al-Zoubi NA, Hatamleh M, Alqudah A, Aleshawi AJ, Alzoubi A. The Effects of Laparoscopic Sleeve Gastrectomy on the Parameters of Leptin Resistance in Obesity. Biomolecules. 2019; 9(10):533. https://doi.org/10.3390/biom9100533
Chicago/Turabian StyleMazahreh, Tagleb S., Mahmoud Alfaqih, Rami Saadeh, Nabil A. Al-Zoubi, Moad Hatamleh, Ahmad Alqudah, Abdelwahab J. Aleshawi, and Abdallah Alzoubi. 2019. "The Effects of Laparoscopic Sleeve Gastrectomy on the Parameters of Leptin Resistance in Obesity" Biomolecules 9, no. 10: 533. https://doi.org/10.3390/biom9100533
APA StyleMazahreh, T. S., Alfaqih, M., Saadeh, R., Al-Zoubi, N. A., Hatamleh, M., Alqudah, A., Aleshawi, A. J., & Alzoubi, A. (2019). The Effects of Laparoscopic Sleeve Gastrectomy on the Parameters of Leptin Resistance in Obesity. Biomolecules, 9(10), 533. https://doi.org/10.3390/biom9100533