
Untargeted Metabolomic Plasma Profiling of Emirati Dialysis Patients with Diabetes versus Non-Diabetic: A Pilot Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Design
2.3. Sample Collection and Preparation
2.4. Analytical Analysis: Liquid Chromatography-Mass Spectrometry (LC-MS/MS)
2.5. Statistical Analysis
3. Results
3.1. Clinical Data of Patients
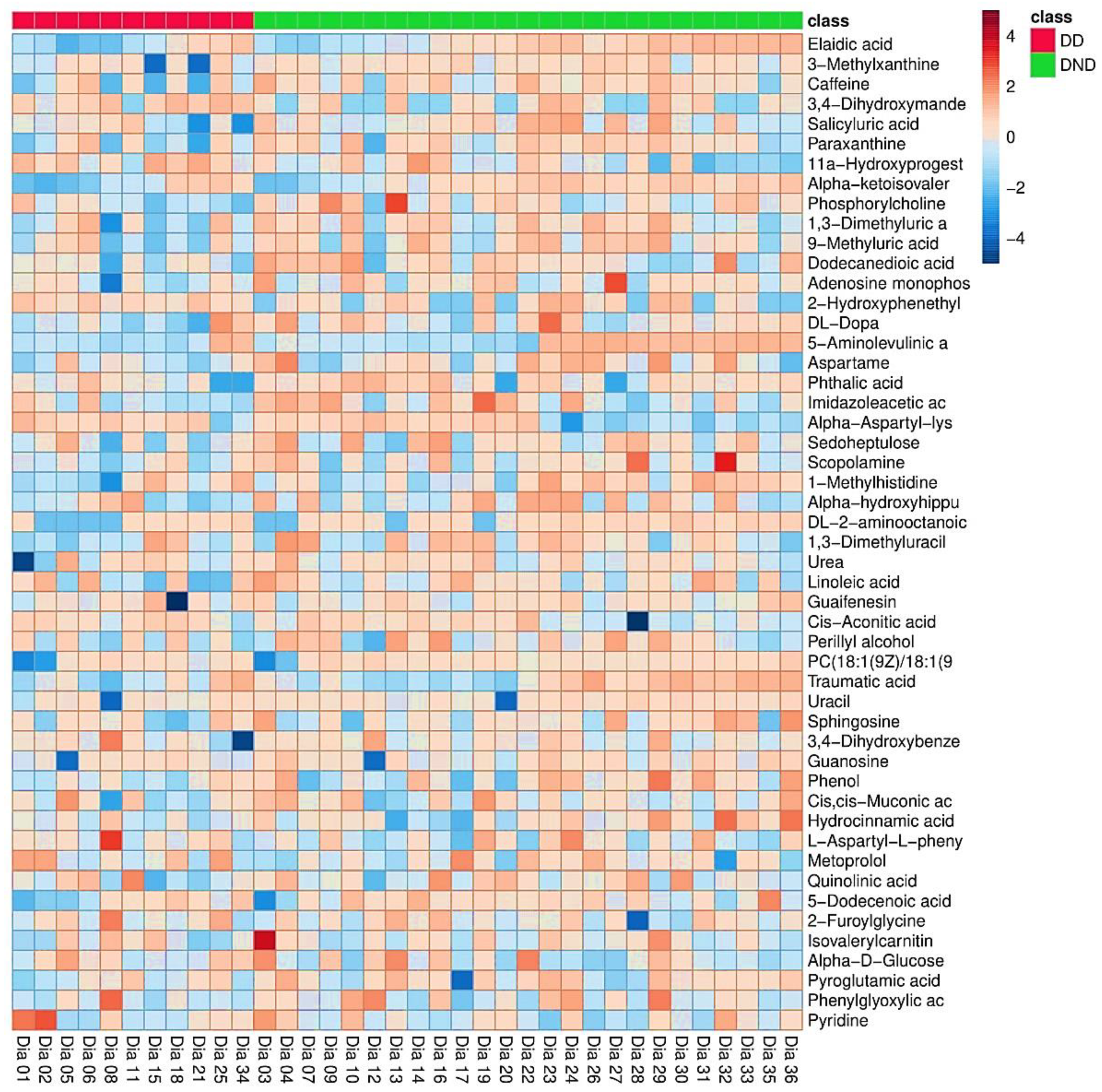
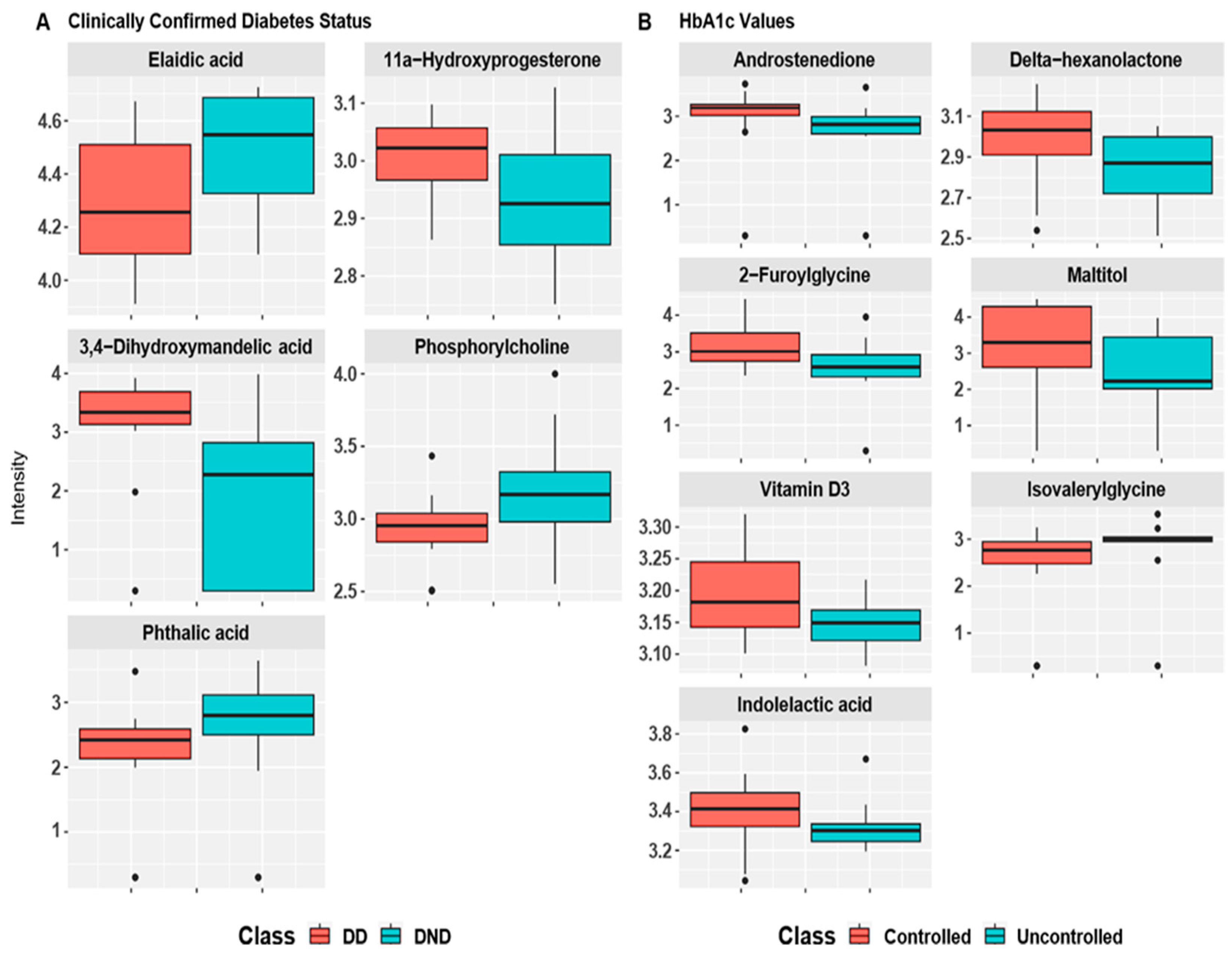
3.2. Differential Metabolite Screening
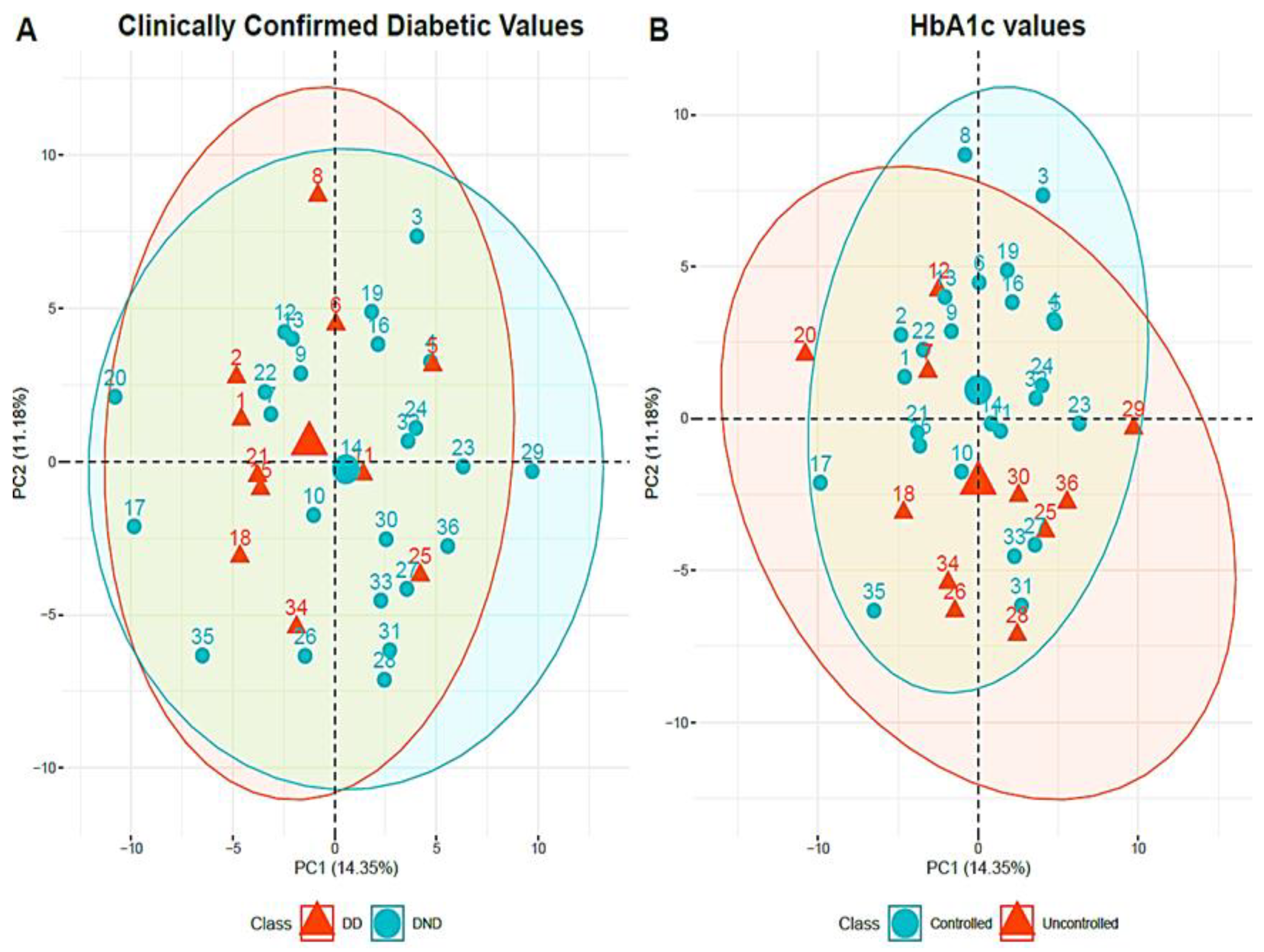
3.3. Multivariate Statistical Analysis
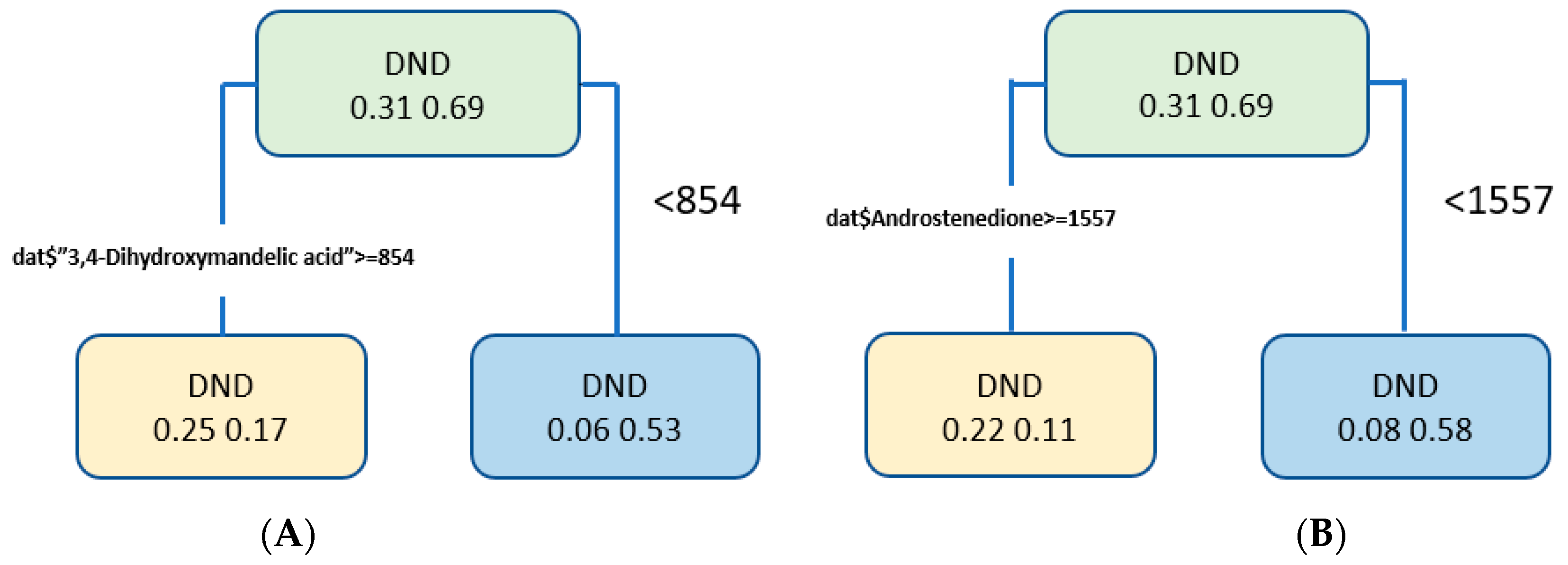
3.4. Discrepancy Metabolite Analysis
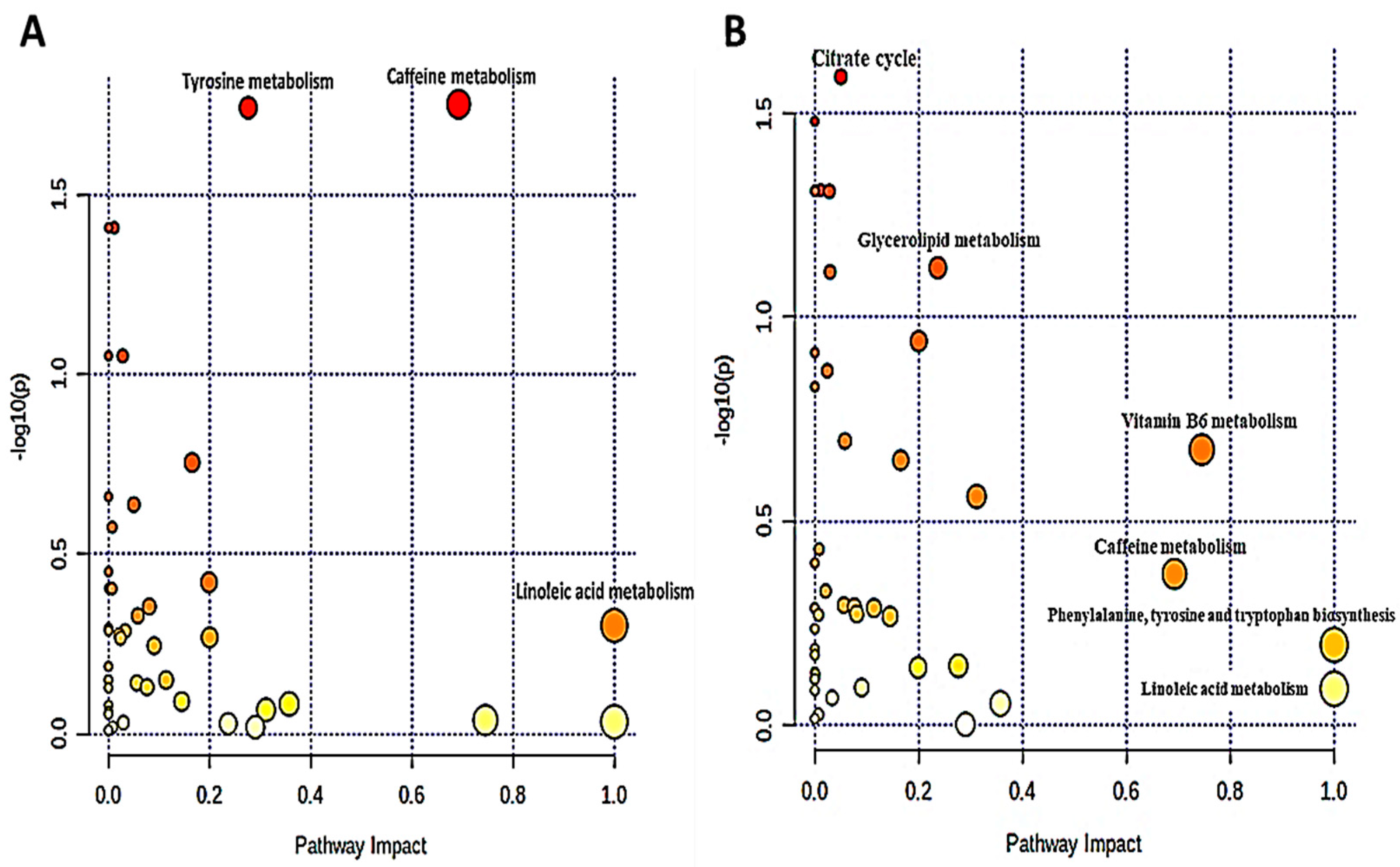
3.5. Analysis of Metabolic Pathways
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and National Diabetes Surveillance System (2016). Available online: https://www.cdc.gov/diabetes/data/index.html (accessed on 23 May 2022).
- International Diabetes. International Diabetes Federation Diabetes Atlas Ninth Edition 2019. 2019. Available online: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/159-idf-diabetes-atlas-ninth-edition-2019.html (accessed on 23 May 2022).
- Romagnani, P.; Remuzzi, G.; Glassock, R.; Levin, A.; Jager, K.J.; Tonelli, M.; Massy, Z.; Wanner, C.; Anders, H.-J. Chronic kidney disease. Nat. Rev. Dis. Primers. 2017, 3, 17088. [Google Scholar] [CrossRef] [PubMed]
- El Nahas, A.M.; Bello, A.K. Chronic kidney disease: The global challenge. Lancet 2005, 365, 331–340. [Google Scholar] [CrossRef]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic kidney disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Saran, R.; Robinson, B.; Abbott, K.C. United States Renal Data System: 2016 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2017, 69, A4. [Google Scholar] [CrossRef]
- Niewczas, M.A.; Mathew, A.V.; Croall, S.; Byun, J.; Major, M.; Sabisetti, V.S.; Smiles, A.; Bonventre, J.V.; Pennathur, S.; Krolewski, A.S. Circulating Modified Metabolites and a Risk of ESRD in Patients with Type 1 Diabetes and Chronic Kidney Disease. Diabetes Care 2017, 40, 383–390. [Google Scholar] [CrossRef] [Green Version]
- Guthoff, M.; Wagner, R.; Vosseler, D.; Peter, A.; Nadalin, S.; Häring, H.-U.; Fritsche, A.; Heyne, N. Impact of end-stage renal disease on glucose metabolism—a matched cohort analysis. Nephrol. Dial. Transplant. 2017, 32, 670–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deger, S.M.; Ellis, C.D.; Bian, A.; Shintani, A.; Ikizler, T.; Hung, A.M. Obesity, diabetes and survival in maintenance hemodialysis patients. Ren. Fail. 2014, 36, 546–551. [Google Scholar] [CrossRef] [Green Version]
- Vijayan, M.; Radhakrishnan, S.; Abraham, G.; Mathew, M.; Sampathkumar, K.; Mancha, N.P. Diabetic kidney disease patients on hemodialysis: A retrospective survival analysis across different socioeconomic groups. Clin. Kidney J. 2016, 9, 833–838. [Google Scholar] [CrossRef] [Green Version]
- Abe, M.; Hamano, T.; Hoshino, J.; Wada, A.; Nakai, S.; Inaba, M.; Masakane, I. SP431IS There a “Burnt-Out Diabetes” Phenomenon In Patients On Hemodialysis? Nephrol. Dial. Transplant. 2017, 32, iii268. [Google Scholar] [CrossRef]
- Rhee, C.M.; Leung, A.M.; Kovesdy, C.P.; Lynch, K.E.; Brent, G.A.; Kalantar-Zadeh, K. Updates on the Management of Diabetes in Dialysis Patients. Semin. Dial. 2014, 27, 135–145. [Google Scholar] [CrossRef] [Green Version]
- Kalantar-Zadeh, K.; Derose, S.F.; Nicholas, S.; Benner, D.; Sharma, K.; Kovesdy, C.P. Burnt-Out Diabetes: Impact of Chronic Kidney Disease Progression on the Natural Course of Diabetes Mellitus. J. Ren. Nutr. 2009, 19, 33–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovesdy, C.P.; Park, J.C.; Kalantar-Zadeh, K. Glycemic Control and Burnt-Out Diabetes in ESRD. Semin. Dial. 2010, 23, 148–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovesdy, C.P.; Sharma, K.; Kalantar-Zadeh, K. Glycemic Control in Diabetic CKD Patients: Where Do We Stand? Am. J. Kidney Dis. 2008, 52, 766–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Lertdumrongluk, P.; Molnar, M.Z.; Kovesdy, C.P.; Kalantar-Zadeh, K. Glycemic Control in Diabetic Dialysis Patients and the Burnt-Out Diabetes Phenomenon. Curr. Diabetes Rep. 2012, 12, 432–439. [Google Scholar] [CrossRef]
- Colhoun, H.M.; Marcovecchio, M.L. Biomarkers of diabetic kidney disease. Diabetologia 2018, 61, 996–1011. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Zuo, J.-J.; Dong, S.-S.; Lan, Y.; Wu, C.-W.; Mao, G.-Y.; Zheng, C. Identification of Potential Serum Metabolic Biomarkers of Diabetic Kidney Disease: A Widely Targeted Metabolomics Study. J. Diabetes Res. 2020, 2020, 3049098. [Google Scholar] [CrossRef] [Green Version]
- Dincer, N.; Dagel, T.; Afsar, B.; Covic, A.; Ortiz, A.; Kanbay, M. The effect of chronic kidney disease on lipid metabolism. Int. Urol. Nephrol. 2018, 51, 265–277. [Google Scholar] [CrossRef]
- Eid, S.; Sas, K.M.; Abcouwer, S.F.; Feldman, E.L.; Gardner, T.W.; Pennathur, S.; Fort, P.E. New insights into the mechanisms of diabetic complications: Role of lipids and lipid metabolism. Diabetologia 2019, 62, 1539–1549. [Google Scholar] [CrossRef] [Green Version]
- Darshi, M.; Van Espen, B.; Sharma, K. Metabolomics in Diabetic Kidney Disease: Unraveling the Biochemistry of a Silent Killer. Am. J. Nephrol. 2016, 44, 92–103. [Google Scholar] [CrossRef]
- Sharma, K.; Karl, B.; Mathew, A.V.; Gangoiti, J.A.; Wassel, C.L.; Saito, R.; Pu, M.; Sharma, S.; You, Y.-H.; Wang, L.; et al. Metabolomics Reveals Signature of Mitochondrial Dysfunction in Diabetic Kidney Disease. J. Am. Soc. Nephrol. 2013, 24, 1901–1912. [Google Scholar] [CrossRef]
- Roberts, L.D.; Souza, A.L.; Gerszten, R.E.; Clish, C.B. Targeted metabolomics. Curr. Protoc. Mol. Biol. 2012, 98, 30–32. [Google Scholar]
- Klassen, A.; Faccio, A.T.; Canuto, G.A.B.; Cruz, P.L.R.; Ribeiro, H.; Tavares, M.F.M.; Sussulini, A. Metabolomics: Definitions and significance in systems biology. In Metabolomics: From Fundamentals to Clinical Applications; Springer: Berlin/Heidelberg, Germany, 2017; pp. 3–17. [Google Scholar]
- Rhee, E.P. Metabolomics and renal disease. Curr. Opin. Nephrol. Hypertens. 2015, 24, 371. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-J.; Liao, W.-L.; Chang, C.-T.; Lin, Y.-N.; Tsai, F.-J. Identification of Urinary Metabolite Biomarkers of Type 2 Diabetes Nephropathy Using an Untargeted Metabolomic Approach. J. Proteome Res. 2018, 17, 3997–4007. [Google Scholar] [CrossRef]
- Tang, X.; You, J.; Liu, D.; Xia, M.; He, L.; Liu, H. 5-Hydroxyhexanoic Acid Predicts Early Renal Functional Decline in Type 2 Diabetes Patients with Microalbuminuria. Kidney Blood Press. Res. 2019, 44, 245–263. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D.S.; Knox, C.; Guo, A.C.; Eisner, R.; Young, N.; Gautam, B.; Hau, D.D.; Psychogios, N.; Dong, E.; Bouatra, S.; et al. HMDB: A knowledgebase for the human metabolome. Nucleic Acids Res. 2008, 37, D603–D610. [Google Scholar] [CrossRef]
- R: A Language and Environment for Statistical Computing; Reference Index. Available online: https://www.r-project.org/ (accessed on 23 May 2022).
- Chong, J.; Soufan, O.; Li, C.; Caraus, I.; Li, S.; Bourque, G.; Wishart, D.S.; Xia, J. MetaboAnalyst 4.0: Towards more transparent and integrative metabolomics analysis. Nucleic Acids Res. 2018, 46, W486–W494. [Google Scholar] [CrossRef] [Green Version]
- Van Eeckhaut, A.; Lanckmans, K.; Sarre, S.; Smolders, I.; Michotte, Y. Validation of bioanalytical LC–MS/MS assays: Evaluation of matrix effects. J. Chromatogr. B 2009, 877, 2198–2207. [Google Scholar] [CrossRef]
- Gentile, M.A.; Nantermet, P.V.; Vogel, R.L.; Phillips, R.; Holder, D.; Hodor, P.; Cheng, C.; Dai, H.; Freedman, L.P.; Ray, W.J. Androgen-mediated improvement of body composition and muscle function involves a novel early transcriptional program including IGF1, mechano growth factor, and induction of β-catenin. J. Mol. Endocrinol. 2010, 44, 55. [Google Scholar] [CrossRef] [Green Version]
- Sathyapalan, T.; Dickerson, E.H.; Maguiness, S.M.; Robinson, J.; Dakroury, Y.H.Z.; Atkin, S.L. Androstenedione and testosterone levels correlate with in vitro fertilization rates in insulin-resistant women. BMJ Open Diabetes Res. Care 2017, 5, e000387. [Google Scholar] [CrossRef] [Green Version]
- Ganguly, P.K.; Dhalla, K.S.; Innes, I.R.; Beamish, E.R. Altered norepinephrine turnover and metabolism in diabetic cardiomyopathy. Circ. Res. 1986, 59, 684–693. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Zelnick, L.R.; Hoofnagle, A.N.; Chen, Y.; De Boer, I.H.; Himmelfarb, J.; Kestenbaum, B. Differences in proximal tubular solute clearance across common etiologies of chronic kidney disease. Nephrol. Dial. Transplant. 2019, 35, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Al-Badr, W.; Martin, K.J. Vitamin D and kidney disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1555–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dash, N.R.; Al Bataineh, M.T. Metagenomic Analysis of the Gut Microbiome Reveals Enrichment of Menaquinones (Vitamin K2) Pathway in Diabetes Mellitus. Diabetes Metab. J. 2021, 45, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Hocher, B.; Adamski, J. Metabolomics for clinical use and research in chronic kidney disease. Nat. Rev. Nephrol. 2017, 13, 269–284. [Google Scholar] [CrossRef]
- Yang, S.; Han, Y.; Liu, J.; Song, P.; Xu, X.; Zhao, L.; Hu, C.; Xiao, L.; Liu, F.; Zhang, H.; et al. Mitochondria: A Novel Therapeutic Target in Diabetic Nephropathy. Curr. Med. Chem. 2017, 24, 3185–3202. [Google Scholar] [CrossRef]
- Forbes, J.M.; Thorburn, D.R. Mitochondrial dysfunction in diabetic kidney disease. Nat. Rev. Nephrol. 2018, 14, 291–312. [Google Scholar] [CrossRef]
- Wei, P.Z.; Szeto, C.C. Mitochondrial dysfunction in diabetic kidney disease. Clin. Chim. Acta 2019, 496, 108–116. [Google Scholar] [CrossRef]
- Li, L.; Wang, C.; Yang, H.; Liu, S.; Lu, Y.; Fu, P.; Liu, J. Metabolomics reveal mitochondrial and fatty acid metabolism disorders that contribute to the development of DKD in T2DM patients. Mol. BioSyst. 2017, 13, 2392–2400. [Google Scholar] [CrossRef]
- Dos Santos, A.L.T.; Duarte, C.K.; Santos, M.; Zoldan, M.; Almeida, J.C.; Gross, J.L.; Azevedo, M.J.; Lichtenstein, A.H.; Zelmanovitz, T. Low linolenic and linoleic acid consumption are associated with chronic kidney disease in patients with type 2 diabetes. PLoS ONE 2018, 13, e0195249. [Google Scholar] [CrossRef] [Green Version]
- Sha, Q.; Lyu, J.; Zhao, M.; Li, H.; Guo, M.; Sun, Q. Multi-Omics Analysis of Diabetic Nephropathy Reveals Potential New Mechanisms and Drug Targets. Front. Genet. 2020, 11, 1605. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | -Log(p) | Impact | Compounds | Pathway | |
|---|---|---|---|---|---|
| Clinically confirmed diabetic status | Linoleic acid metabolism | 0.30064 | 1.0 | Linoleic acid, Glycerophosphocholine | hsa00591 |
| Caffeine metabolism | 1.7512 | 0.69231 | Paraxanthine, Caffeine | map00232 | |
| Tyrosine metabolism | 1.7414 | 0.27636 | 3,4-Dihydroxymandelic acid, 3,4-Dihydroxyphenylglycol, 3,4-Dihydroxybenzeneacetic acid, DL-Dopa, L-Tyrosine | map00350 | |
| Latest HbA1c values | Citrate cycle | 1.5898 | 0.05003 | Cis-Aconitic acid | hsa00020 |
| Glycerolipid metabolism | 1.1213 | 0.23676 | Glycerol | hsa00561 | |
| Vitamin B6 metabolism | 0.67539 | 0.68759 | Pyridoxal 5′-phosphate, Pyridoxal, 4-Pyridoxic acid | hsa00750 | |
| Linoleic acid metabolism | 0.08917 | 1.0 | Linoleic acid, Glycerophosphocholine | hsa00591 | |
| Caffeine metabolism | 0.37079 | 0.69231 | Paraxanthine, Caffeine | hsa00232 | |
| Phenylalanine, tyrosine, and tryptophan biosynthesis | 0.19682 | 1 | L-Phenylalanine, L-Tyrosine, | hsa00400 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banimfreg, B.H.; Alshraideh, H.; Shamayleh, A.; Guella, A.; Semreen, M.H.; Al Bataineh, M.T.; Soares, N.C. Untargeted Metabolomic Plasma Profiling of Emirati Dialysis Patients with Diabetes versus Non-Diabetic: A Pilot Study. Biomolecules 2022, 12, 962. https://doi.org/10.3390/biom12070962
Banimfreg BH, Alshraideh H, Shamayleh A, Guella A, Semreen MH, Al Bataineh MT, Soares NC. Untargeted Metabolomic Plasma Profiling of Emirati Dialysis Patients with Diabetes versus Non-Diabetic: A Pilot Study. Biomolecules. 2022; 12(7):962. https://doi.org/10.3390/biom12070962
Chicago/Turabian StyleBanimfreg, Bayan Hassan, Hussam Alshraideh, Abdulrahim Shamayleh, Adnane Guella, Mohammad Harb Semreen, Mohammad Tahseen Al Bataineh, and Nelson C. Soares. 2022. "Untargeted Metabolomic Plasma Profiling of Emirati Dialysis Patients with Diabetes versus Non-Diabetic: A Pilot Study" Biomolecules 12, no. 7: 962. https://doi.org/10.3390/biom12070962