
Why Does Hyperuricemia Not Necessarily Induce Gout?


VIDRL and The Peter Doherty Institute, 792 Elizabeth Street, Melbourne 3000, Australia
Biomolecules 2021, 11(2), 280; https://doi.org/10.3390/biom11020280
Submission received: 5 January 2021
/
Revised: 10 February 2021
/
Accepted: 10 February 2021
/
Published: 14 February 2021
(This article belongs to the Special Issue Beyond Lipid Rafts and Caveolae: From Caveolae Compartmentalization of Signal Transduction to Medicine)
Abstract
:Hyperuricemia is a risk factor for gout. It has been well observed that a large proportion of individuals with hyperuricemia have never had a gout flare(s), while some patients with gout can have a normuricemia. This raises a puzzle of the real role of serum uric acid (SUA) in the occurrence of gout flares. As the molecule of uric acid has its dual effects in vivo with antioxidant properties as well as being an inflammatory promoter, it has been placed in a delicate position in balancing metabolisms. Gout seems to be a multifactorial metabolic disease and its pathogenesis should not rely solely on hyperuricemia or monosodium urate (MSU) crystals. This critical review aims to unfold the mechanisms of the SUA role participating in gout development. It also discusses some key elements which are prerequisites for the formation of gout in association with the current therapeutic regime. The compilation should be helpful in precisely fighting for a cure of gout clinically and pharmaceutically.
1. Introduction
Hyperuricemia has been defined as serum uric acid (SUA) >6.0 mg/dL in women; >7.0 mg/dL in men; >5.5 mg/dL in children and adolescents [1], and is an independent risk factor of a strong non-linear concentration-dependent to the incident of gout [2]. Genetic variants contribute largely to hyperuricemia [3] with 43 genes so far that have been identified in controlling SUA levels [4]. Gout, a common metabolic disorder with symptoms of localized inflammation, is caused by chronic and/or episodic deposition of monosodium urate (MSU) crystals in joints and soft tissues prompting a gouty attack/flare [5]. It has not been viewed just as an articular disease with its broad definition, but as a complex disease with interactive mechanisms of inflammatory and metabolic disorders displaying its symptoms beyond the local inflammatory consequence of MSU crystal deposition. Approximately up to 10% of adults have reported having gout [6], and 3.9% and 14.6% of the US population have gout and hyperuricemia, respectively [7].
It has been well observed and puzzled for a long time that not all hyperuricemia patients suffer from gout [8], only up to 36% of the patients develop gout [9,10], and not all gout patients have hyperuricemia [11,12]. Up to 76% of asymptomatic hyperuricemia patients could not find MSU crystal deposition [10]. This discrepancy has raised many clinical and scientific debates on the role of SUA in the development of gout and the efficacy of uric acid-lowering therapy (ULT) on the treatments of gout and other pathological conditions, despite the risk of gout increasing dramatically with increasing SUA levels in conjunction with additional factors [13]. The typical progression of gout could start from hyperuricemia without MSU crystal deposition, to crystal deposition without symptomatic gout, to acute gout flares and tophi, and to chronic gouty arthritis [14], but the correlations between gout and hyperuricemia are loose. Recent studies postulate that gout formation would be well beyond MSU crystal deposition with pathogenic mechanisms involving overproduction of chemotactic cytokines, cell proliferation and inflammation [15], and internalization of SUA induced pro-apoptotic and inflammatory effects [16].
Treatment of hyperuricemia in individuals without gout has been contentious partially due to the interrelationship between hyperuricemia and gout being not fully understood. Exploring such a mechanism, therefore, would be helpful in guiding the establishment of proper therapeutic regimes for both. This critical review aims to gather recently published literature for the elucidation of the interrelationship between hyperuricemia and gout in their pathogenesis, clinical evidence of the inflammation effects, MSU crystal formation, and therapeutic regimes, and attempts to explain why hyperuricemia does not necessarily induce gout.
2. Uric Acid and Gout
Uric acid (UA) is the end catabolic product of exogenous and endogenous purine nucleotide metabolism in humans. It exists in blood serum/plasma, cells, and tissues with steady-state conditions of its production and disposal. Its production can be found in almost all tissues, while its major disposal is via kidneys. SUA concentrations can be reflected by the intake from diet, in vivo purine metabolism, renal secretion, and intestinal degeneration [17]. In vivo, it may offer a neuroprotective advantage in the neurodegenerative Alzheimer’s disease [18], schizophrenia [19], Parkinson’s disease [20], multiple sclerosis [21], and serves as a depression biomarker [22]. SUA concentrations are linked to muscle strength and lean mass [23], although this was not shown in gastrointestinal tract cancer patients [24]. SUA may serve as a risk factor to predict poor thyroid function [25] or an indicator of malnutrition [15]. At a higher level, it activates inflammatory and oxidative mechanism action events in healthy subjects [26] and is a protective factor against the pathological decline of lung function [27] or an independent predictor for non-alcoholic fatty liver disease [28]. Abnormal SUA levels, either higher or lower, could increase the risk for mortality [29,30]. However, controversial reports have been presented: a slight increase in SUA level was an independent risk factor for all-cause and cardiovascular mortality [31,32], while another report did not find any relationship between SUA and cardiovascular disease (CVD) mortality and morbidity [33]. UA is also a potent antioxidant and an effective scavenger of singlet oxygen and free radicals [34], almost tenfold greater than other antioxidants in blood [26] or accounting for over half of the free radical scavenging activity in vivo [35]. Supplement of UA in donor blood sustains the antioxidant protection of the stored red blood cells [36]. The oxidant-antioxidant paradox of UA [37] may suggest UA could have different molecular behaviors under various pathological conditions. At the hydrophilic condition, it shows the protective effects of antioxidants [38]. Reducing SUA could decline its protective effect to radiation damage [39], and total bone mineral density [40,41] or a protective effect on bone loss in rheumatoid arthritis [42] (Figure 1).
Beyond its role in protection, over-saturated SUA together with sodium could deposit in joints, soft tissues, bones, skin, etc., as MSU crystals to form tophi and trigger gout flares with episodes of severe pain. Gout is a common and complex form of arthritis with a sudden attack(s) of pain, swelling, redness, and tenderness in the affected location(s). Tophaceous gout has been defined as classic periarticular subcutaneous tophi, disseminated intradermal tophi, an ulcerative form, and gouty panniculitis [43] and commonly appears as firm, pink nodules or fusiform swellings [44]. Without clinical intervention, tophi can become developed within affected joints and or tissues and progressively damage them. Interestingly, the prevalence of gout flares, irrespective of SUA levels, has been linked to mental disorders [45,46]. Chronic heart failure and diabetes mellitus are more strongly associated with increased MSU crystal deposition in knees and feet/ankles than gout duration [47]. As reducing SUA may not be the only way to eliminate gout flares [48], the level of SUA, in essence, should be an indicator of oxidative paradox in vivo.
3. Distinct Reaction and Priming Pathways of Inflammation by SUA and MSU
The major symptom of a gout flare is the MSU crystal-induced sterile inflammation with UA controversially being an intrinsic inhibitor of MSU crystal-induced tissue inflammation [49] and a direct promoter in inflammation in vivo [50]. Hyperuricemia could induce an activated status of inflammation [51] or autoinflammation [52]. It could instigate inflammation by stimulating the production of inflammatory factors such as interleukin-6, interleukin-1(beta), tumor necrosis factor-alpha and CRP [53], or enhancing reactive oxygen species [54], or initiating systemic inflammation via the nuclear factor (NF)-κB signaling pathway [55], or direct proinflammatory effects on macrophages [56]. Intra-articular injection of MSU-induced inflammatory arthritis could result from UA injection [57]. Although both SUA and MSU crystals can stimulate immune responses, different pathways have been demonstrated between them from epigenetic regulation, inflammasome activation to transcriptional control [58], and the immune reactions created by them are different inactivation and priming [59] through various proinflammatory pathways [60] involve in circulating monocytes and/or resident macrophages. UA released from dying cells during inflammation reactions could prime new monocytes and precipitate onto MSU crystals leading to more inflammation and tissue damage. Co-existing gout with hyperuricemia usually leads to higher systemic inflammation [61] and often with inflammatory psoriasis arthritis [62]. MSU deposition causes the major symptoms of inflammation and deterioration of the affected tissues with SUA playing a crucial role in a gout flare. This may support the notion that patients with both hyperuricemia and gout induce a high systemic inflammation with the greatest mortality risk [61]. Moreover, asymptomatic hyperuricemia patients usually display less potency of inflammation with a lower number of NKG2D+ (activating receptors of simulation of cytotoxicity) NK cells [63]. It could be speculated that under hyperuricemia condition the UA paradox interrelationship of the contradictory dual effects of inflammation [49,50] results from SUA “neutralizing” the inflammation produced oxygen species to protect tissue damages. It has also been discovered that some lipids from diet or alcohol consumption could directly trigger gout flares by activation of NALP-3 inflammasome through binding to toll-like receptors [64] or alteration of glucose and apolipoprotein metabolism [65], respectively. In conjunction with the aforementioned evidence, it may be postulated that although hyperuricemia could stimulate the formation of SUA crystals and prime immune responses in the promotion of gout flares, it goes along with different pathways of inflammation in contrast to that of MSU crystals (details have been reviewed on this topic [58]). Therefore, hyperuricemia may not be the only determinant of a gout flare or flares especially in the form of inflammation and can be present even without crystal formation in some patients [3]. Indeed, the differentiation in inflammation pathways may lay the foundation for elucidating the importance of eliminating any inflammation factors other than hyperuricemia during a gout flare.
4. Factors Affecting MSU Crystal Deposition Other Than Hyperuricemia
It has been found that only about half of those with SUA concentrations of ≥10 mg/dL developed clinically evident gout during a 15-year period [2]. Despite hyperuricemia playing a critical role in the formation of MSU crystals, other factors affecting MSU crystallization in tissues to induce gout flare are also involved including but not limited to temperature, pH, ion concentrations, proteins, and various connective tissue conditions as well as secondary nucleation formation [66]. Additionally, white blood cell count (WBC) in synovial envirofluid is also significantly associated with the formation of MSU crystals [67], even though it is still been unresolved whether WBC induces MSU crystal formation or vice versa. Reducing blood lipid levels with a lipid-lowering agent(s) could concurrently reduce SUA level [68], suggesting a decline of the hydrophobic environment could enhance the solubility of SUA to be easily excreted by the kidney instead of forming MSU. Furthermore, hyperlipidemia is more commonly seen in patients with gout in comparison with asymptomatic individuals with HDL-C being a protective predictor of SUA levels [69].
In spite of hyperuricemia, it has been established that pre-biological fiber damage could be a prerequisite for MSU crystal deposition [70]. In the predominated crystal-rich areas of gouty tophi, new crystals add on the already formed crystals to form secondary nucleation which puts pressure on surrounding cells and causes tissue damage [71]. Osteoarthritis could alter the cartilage surface to precede MSU crystal formation happening at collagen-rich sites of damaged and exposed tissues [72], and surgical tissue damage could also induce gout flare [73]. The altered composition of microbiomes could then contribute to gout formation possibly due to stone or crystal growth in vivo [74]. All of that evidence may suggest that the formation of MSU crystals to induce a gout flare usually has an abnormal environment caused by a pathological condition(s) in addition to hyperuricemia.
5. The Causes of Hyperuricemia Irrelevant to Gout
An increase in UA concentration that exceeds the normal range might not be exclusively linked to gout flares [75] as many factors causing hyperuricemia are not relevant or significant to gout formation. Certain foods, status, or medicines could induce hyperuricemia. Under renal dis-function or cell damage, SUA could be suddenly increased by changing renal function to cause hyperuricemia [76]. Drugs such as diuretics (thiazide), anticonvulsants (valproate and phenobarbital), cyclosporine, theophylline, and pyrazinamide have been reported to increase SUA levels [77] in addition to favipiravir (an antiviral drug) [78]. Emotional stress [79], fasting [75], or dehydration [80] caused by physical activity can also increase the concentration of SUA. Although occasionally an acute gout flare may be linked with the medication(s) or condition(s), the enhanced SUA should be only temporarily sustained and a gout flare is considered unlikely to occur if a longer duration and higher dose treatment are avoided [81]. This may match with the fact that most gout patients do not know the trigger(s) of their gout flares [82]. Contrarily, a sudden reduction of SUA may also trigger a gout flare through the dissolution of MSU fallen off from tophi [83]. Allopurinol, a ULT medicine, has not shown any efficacy in the prevention of a first gout flare in patients with asymptomatic hyperuricemia [84]. Fundamentally, SUA level is associated with physical capacity and muscle strength in healthy subjects [23,24] and may only be a biological marker of non-gout conditions such as cardiovascular damage but is not a risk factor for its development [51]. Controversially, pseudo-gout, which is caused by calcium pyrophosphate deposition (CPPD), could have the same inflammatory symptoms as gout without hyperuricemia [85].
Gout can be self-resolvable with symptoms disappearing within days or weeks when hyperuricemia might still be sustained. Therefore, the symptoms might not be paralleled with a reduction in SUA level. The immunoreaction generated anti-UA antibody could also prevent or reduce inflammation conditions to release gout flare symptoms [62]. Under hyperuricemia, apoA-I elevation [86] or neutrophil-derived microvesicles [87] may play a role in the spontaneous resolution of acute gout arthritis.
The increased SUA after fasting for a long term may not induce any gout flares [75], plausibly as fasting could reduce the signaling pathway of the mammalian target of rapamycin (mTOR). The declined mTOR pathway could concomitantly inhibit cell growth, enhance autophagy and decrease activation of the NF-κB pathway as well as oxidative stress [88], thus reducing inflammatory processes and preventing a gout attack. All of those may be indicative that many elements inducing hyperuricemia could be irrelevant or insignificant to a gout flare. This may also at least partially explain the existence of asymptomatic hyperuricemia. However, longitudinal studies would be useful to understand the evolution of hyperuricemia and gout further and highlight the need for different treatment strategies [89].
6. Therapeutic Regimes for Treatments of Hyperuricemia and Gout
The traditional treatment for gout flares has been well established for the improvement of quality of life (Table 1), although treatment with ULT alone may not be optimal for patients [90]. The current recommendation is to additionally employ anti-inflammatory therapy [91] to reduce pathologic MSU deposition [92]. Commencing ULT alone during an acute gout flare has neither significant efficacy on localized pain, recurrent flares, or adverse effects [48] nor been associated with the risk of gout flare [93], or able to ameliorate gout associated diabetes incidence or reverse beta-cell apoptosis with significance [94] or improvement of kidney function [95]. Given the recent safety concerns, gradually up-titrated allopurinol remains the first-line ULT [96] together with concomitant colchicine or nonsteroidal anti-inflammatory drugs for enhancement of efficacy [97]. Adversely, treatment of hyperuricemia has raised attention besides gout, and current debates on whether asymptomatic hyperuricemia should be treated are still ongoing [2,98,99]. This may partially be due to both low and high SUA levels being associated with increased all-cause and cause-specific mortality with a U-shaped association [100,101]. Adventitious reduction of SUA with fenofibrate could not mediate the cardioprotective effect [68]. It may be legitimate that reducing SUA may not rapidly be able to eliminate the local inflammation that occurred upon a gout flare. Alternatively, targeting MSU crystals could be more useful and efficient in controlling gout flares. Furthermore, as some comorbidities such as chronic heart failure and diabetes mellitus are less influenced by SUA levels [47], UTL would not be favorable to them. In spite of UA infusion improving endothelial function [102], quickly lowering SUA could induce an acute gout flare [82], cardiovascular events [103], nerve dysfunction [104], the risk of all-cause death in hemodialysis [61], vertebral fracture [105], or heart failure in patients [106]. Additionally, it has been reported that in patients with gout SUA is usually lower during acute gouty attacks than during intercritical periods [11] possibly due to the slow systemic inflammatory response. Recent evidence demonstrated that SUA was increased 3 months after starting treatment with TNFis (TNF inhibitors) in inhibition of inflammation [107] with the pathogenesis remaining unknown.
Traditional Chinese medicine treats gout with efficacy and the fundamental strategy seems to target specifically restorations of metabolisms and immunity as well as inhibition of inflammation and peripheral nerve sensation [108]. This may support the notion that gout is a systematic disease of metabolism, any symptom targeted therapy may not be the optimal strategy for a cure. Hopefully, more pathogenic evidence on the interrelationship between gout and hyperuricemia may facilitate a unified guideline globally. Fortunately, lifestyle intervention significantly decreases the MSU deposit burden and intensive training and supervision of patients with gout have resulted in very low numbers of patients not reaching treatment targets [109].
7. Conclusions
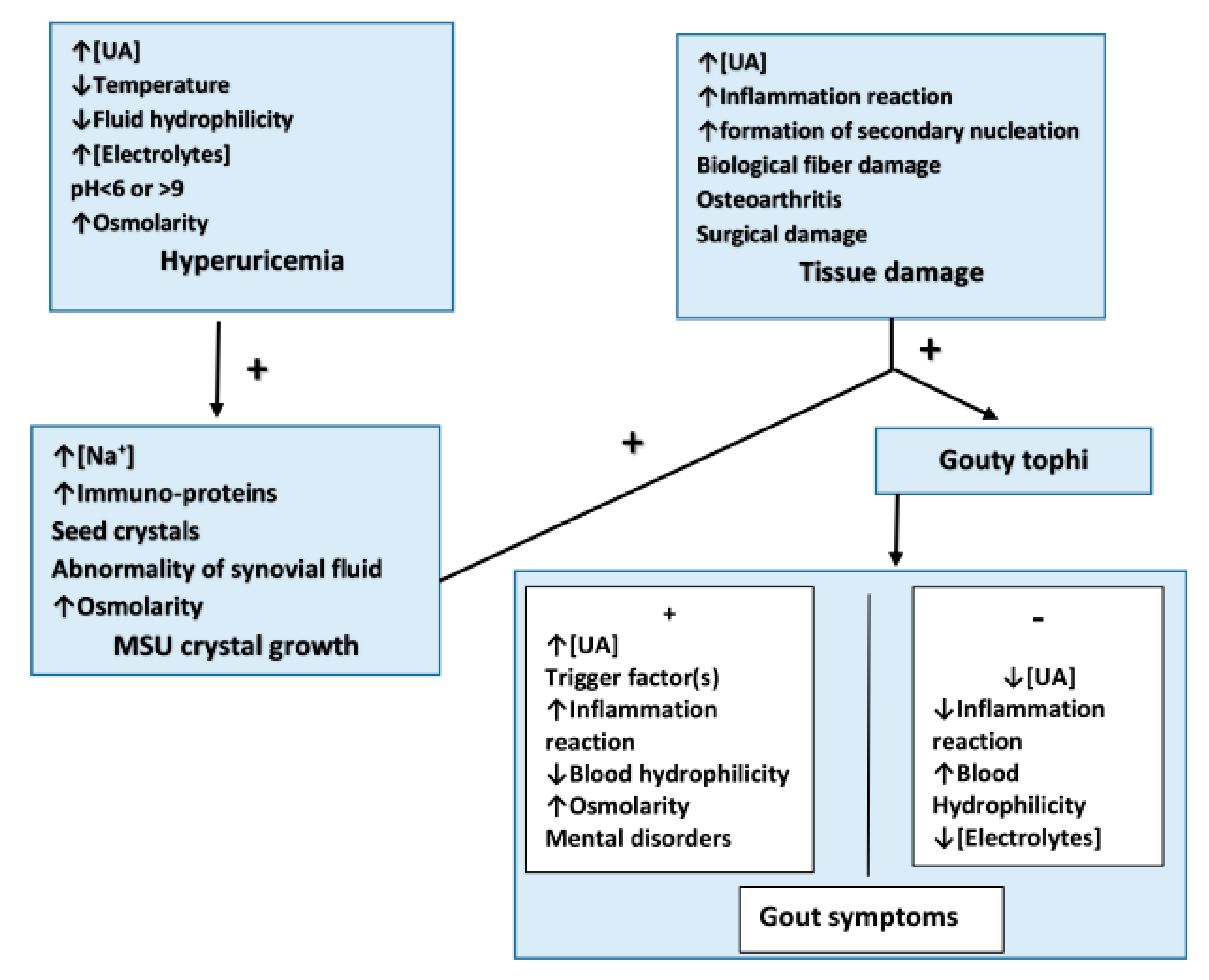
Hyperuricemia is a main, but not the only risk factor for gout flares. Recent publications suggest gout formation would be well beyond hyperuricemia in MSU crystal deposition with pathogenic mechanisms involving an activation of various inflammation pathways with UA and MSU, the critical conditions of secondary SUA deposition, and the degree of intact surrounding tissue(s). The differentiation may explain the existence of asymptomatic hyperuricemia with the UA nature of the anti-oxidative stress, gout symptom self-resolution, and some passive increase of SUA irrelevant to gout. Hyperuricemia could only be accompanied by the aforementioned factor(s) to instigate a gout flare (Figure 2). The pathogenesis between hyperuricemia and gout may support the current notion that ULT together with other therapy(s) are recommended in gout patients but controversial in asymptomatic hyperuricemia individuals, and facilitate a unified therapeutic guideline globally for both.
Key taking home messages: 1. The role of serum uric acid (SUA) should, above and beyond, be an exclusive indicator of a gout flare. 2. Hyperuricemia would not be the only risk factor of a gout flare due to many irrelevant elements between them. 3. Monosodium urate (MSU) deposition requires a pathology environment with damaged bio-fiber integrity other than hyperuricemia.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kasper, D.; Hauser, S.; Longo, D.; Jameson, J.L.; Loscalzo, J. Harrison’s Principles of Internal Medicine, 19th ed.; Mcgraw-Hill: New York, NY, USA, 2015. [Google Scholar]
- Brucato, A.; Cianci, F.; Carnovale, C. Management of Hyperuricemia in Asymptomatic Patients: A Critical Appraisal. Eur. J. Intern. Med. 2020, 74, 8–17. [Google Scholar] [CrossRef]
- Zhang, Q.; Gong, H.; Lin, C.; Liu, Q.; Baima, Y.; Wang, Y.; Lin, J. The prevalence of gout and hyperuricemia in middle-aged and elderly people in Tibet Autonomous Region, China: A preliminary study. Medicine 2020, 99, e18542. [Google Scholar] [CrossRef]
- Boocock, J.; Leask, M.; Okada, Y.; Matsuo, H.; Kawamura, Y.; Shi, Y.; Li, C.; Mount, D.B.; Mandal, A.K.; Wang, W.; et al. Genomic dissection of 43 serum urate-associated loci provides multiple insights into molecular mechanisms of urate control. Hum. Mol. Genet. 2020, 29, 923–943. [Google Scholar] [CrossRef] [PubMed]
- Towiwat, P.; Chhana, A.; Dalbeth, N. The Anatomical Pathology of Gout: A Systematic Literature Review. BMC Musculoskelet. Disord. 2019, 20, 140. [Google Scholar] [CrossRef]
- Kuo, C.F.; Grainge, M.J.; Zhang, W.; Doherty, M. Global epidemiology of gout: Prevalence, incidence and risk factors. Nat. Rev. Rheumatol. 2015, 11, 649–662. [Google Scholar] [CrossRef]
- Singh, G.; Lingala, B.; Mithal, A. Gout and hyperuricaemia in the USA: Prevalence and trends. Rheumatology 2019, 58, 2177–2180. [Google Scholar] [CrossRef]
- Bardin, T.; Richette, P. Definition of hyperuricemia and gouty conditions. Curr. Opin. Rheumatol. 2014, 26, 186–191. [Google Scholar] [CrossRef]
- Lin, K.C.; Lin, H.Y.; Chou, P. The interaction between uric acid level and other risk factors on the development of gout among asymptomatic hyperuricemic men in a prospective study. J. Rheumatol. 2000, 27, 1501–1505. [Google Scholar] [PubMed]
- Dalbeth, N.; House, M.E.; Aati, O.; Tan, P.; Franklin, C.; Horne, A.; Gamble, G.D.; Stamp, L.K.; Doyle, A.J.; McQueen, F.M. Urate crystal deposition in asymptomatic hyperuricaemia and symptomatic gout: A dual energy CT study. Ann. Rheum. Dis. 2015, 74, 908–911. [Google Scholar] [CrossRef]
- Schlesinger, N.; Norquist, J.M.; Watson, D.J. Serum urate during acute gout. J. Rheumatol. 2009, 36, 1287–1289. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kwon, O.C.; Oh, J.S.; Kim, Y.G.; Lee, C.K.; Yoo, B.; Hong, S. Clinical features and recurrent attack in gout patients according to serum urate levels during an acute attack. Korean J. Intern. Med. 2020, 35, 240–248. [Google Scholar] [CrossRef]
- Singh, A.J.; Reddy, S.G.; Kundukulam, J. Risk factors for gout and prevention: A systematic review of the literature. Curr. Opin. Rheumatol. 2011, 23, 192–202. [Google Scholar] [CrossRef] [Green Version]
- Dalbeth, N.; Stamp, L. Hyperuricaemia and gout: Time for a new staging system? Ann. Rheum. Dis. 2014, 73, 1598–1600. [Google Scholar] [CrossRef]
- Bonino, B.; Leoncini, G.; Russo, E.; Pontremoli, R.; Viazzi, F. Uric acid in CKD: Has the jury come to the verdict? J. Nephrol. 2020, 33, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Verzola, D.; Ratto, E.; Villaggio, B.; Parodi, E.L.; Pontremoli, R.; Garibotto, G.; Viazzi, F. Uric acid promotes apoptosis in human proximal tubule cells by oxidative stress and the activation of NADPH oxidase NOX 4. PLoS ONE 2014, 9, e115210. [Google Scholar] [CrossRef]
- Rahimi-Sakak, F.; Maroofi, M.; Rahmani, J.; Bellissimo, N.; Hekmatdoost, A. Serum uric acid and risk of cardiovascular mortality: A systematic review and dose-response meta-analysis of cohort studies of over a million participants. BMC Cardiovasc. Disord. 2019, 19, 218. [Google Scholar] [CrossRef] [Green Version]
- Spitsin, S.; Koprowski, H. Role of uric acid in Alzheimer’s disease. J. Alzheimers Dis. 2010, 19, 1337–1338. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; You, Y.; Yu, L.; Yao, L.; Lu, H.; Zhou, X.; Wu, S.; Chen, L.; Chen, Y.; Zhao, X. Uric acid levels in subjects with schizophrenia: A systematic review and meta-analysis. Psychiatry Res. 2020, 292, 113305. [Google Scholar] [CrossRef]
- Ellmore, T.M.; Suescun, J.; Castriotta, R.J.; Schiess, M.C. A Study of the Relationship Between Uric Acid and Substantia Nigra Brain Connectivity in Patients with REM Sleep Behavior Disorder and Parkinson’s Disease. Front. Neurol. 2020, 11, 815. [Google Scholar] [CrossRef]
- Rentzos, M.; Nikolaou, C.; Anagnostouli, M.; Rombos, A.; Tsakanikas, K.; Economou, M.; Dimitrakopoulos, A.; Karouli, M.; Vassilopoulos, D. Serum uric acid and multiple sclerosis. Clin. Neurol. Neurosurg. 2006, 108, 527–531. [Google Scholar] [CrossRef]
- Meng, X.; Huang, X.; Deng, W.; Li, J.; Li, T. Serum uric acid a depression biomarker. PLoS ONE 2020, 15, e0229626. [Google Scholar] [CrossRef] [PubMed]
- Floriano, J.P.; Nahas, P.C.; de Branco, F.M.S.; Dos Reis, A.S.; Rossato, L.T.; Santos, H.O.; Limirio, L.S.; Ferreira-Filho, S.R.; de Oliveira, E.P. Serum Uric Acid Is Positively Associated with Muscle Mass and Strength, but Not with Functional Capacity, in Kidney Transplant Patients. Nutrients 2020, 12, 2390. [Google Scholar] [CrossRef]
- Trindade, D.B.; de Araujo, V.A.; Franco, E.P.; Fernandes, R.C.; Carvalho, A.; Pimentel, G.D. Serum uric acid concentration is not associated with handgrip strength, lean body mass or survival in gastrointestinal cancer patients. Clin. Nutr. ESPEN 2020, 37, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.J.; Qian, X.W.; Zhang, X.; Han, L.; Zheng, Y.Q.; Wu, T.; Qin, G.Y.; Ye, Z.B.; Xiao, J. Association of serum uric acid with thyroid function in health check-up participants. Chin. Med. J. 2020, 133, 1409–1414. [Google Scholar] [CrossRef]
- Tariq, M.A.; Shamim, S.A.; Rana, K.F.; Saeed, A.; Malik, B.H. Serum Uric Acid—Risk Factor for Acute Ischemic Stroke and Poor Outcomes. Cureus 2019, 11, e6007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujikawa, H.; Sakamoto, Y.; Masuda, N.; Oniki, K.; Kamei, S.; Nohara, H.; Nakashima, R.; Maruta, K.; Kawakami, T.; Eto, Y.; et al. Higher Blood Uric Acid in Female Humans and Mice as a Protective Factor against Pathophysiological Decline of Lung Function. Antioxidants 2020, 9, 387. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Li, J.; Chen, C.; Zhang, K.; Cao, L.; Wang, X.; Ma, J.; Feng, S.; Li, W.D. Higher Serum Uric Acid Level Predicts Non-alcoholic Fatty Liver Disease: A 4-Year Prospective Cohort Study. Front. Endocrinol. 2020, 11, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, C.F.; See, L.C.; Yu, K.H.; Chou, I.J.; Chiou, M.J.; Luo, S.F. Significance of serum uric acid levels on the risk of all-cause and cardiovascular mortality. Rheumatology 2013, 52, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seet, R.C.; Kasiman, K.; Gruber, J.; Tang, S.Y.; Wong, M.C.; Chang, H.M.; Chan, Y.H.; Halliwell, B.; Chen, C.P. Is uric acid protective or deleterious in acute ischemic stroke? A prospective cohort study. Atherosclerosis 2010, 209, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Konta, T.; Ichikawa, K.; Kawasaki, R.; Fujimoto, S.; Iseki, K.; Moriyama, T.; Yamagata, K.; Tsuruya, K.; Narita, I.; Kondo, M.; et al. Association between serum uric acid levels and mortality: A nationwide community-based cohort study. Sci. Rep. 2020, 10, 6066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tai, S.; Li, X.; Zhu, Z.; Tang, L.; Yang, H.; Fu, L.; Hu, X.; Fang, Z.; Zhou, S. Hyperuricemia is a Risk Factor for One-Year Overall Survival in Elderly Female Patients with Acute Coronary Syndrome. Cardiovasc. Ther. 2020, 2020, 2615147. [Google Scholar] [CrossRef] [PubMed]
- Sieminska, E.; Sobczak, P.; Skibinska, N.; Sikora, J. The differential role of uric acid—The purpose or cause of cardiovascular diseases? Med. Hypotheses 2020, 142, 109791. [Google Scholar] [CrossRef] [PubMed]
- Ames, B.N.; Cathcart, R.; Schwiers, E.; Hochstein, P. Uric acid provides an antioxidant defense in humans against oxidant- and radical-caused aging and cancer: A hypothesis. Proc. Natl. Acad. Sci. USA 1981, 78, 6858–6862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowman, G.L.; Shannon, J.; Frei, B.; Kaye, J.A.; Quinn, J.F. Uric acid as a CNS antioxidant. J. Alzheimers Dis. 2010, 19, 1331–1336. [Google Scholar] [CrossRef] [Green Version]
- Bardyn, M.; Chen, J.; Dussiot, M.; Crettaz, D.; Schmid, L.; Langst, E.; Amireault, P.; Tissot, J.D.; Jolicoeur, M.; Prudent, M. Restoration of Physiological Levels of Uric Acid and Ascorbic Acid Reroutes the Metabolism of Stored Red Blood Cells. Metabolites 2020, 10, 226. [Google Scholar] [CrossRef] [PubMed]
- Sautin, Y.Y.; Johnson, R.J. Uric acid: The oxidant-antioxidant paradox. Nucleosides Nucleotides Nucleic Acids 2008, 27, 608–619. [Google Scholar] [CrossRef] [Green Version]
- Stewart, J.D.; Langlois, V.; Noone, D. Hyperuricemia and Hypertension: Links and Risks. Integr. Blood Press. Control 2019, 12, 43–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paithankar, J.G.; Kudva, A.K.; Raghu, S.V.; Patil, R.K. Radioprotective role of uric acid: Evidence from studies in Drosophila and human dermal fibroblast cells. Mol. Biol. Rep. 2020, 47, 2427–2436. [Google Scholar] [CrossRef]
- Pan, K.; Yao, X.; Liu, M.; Zhu, Z. Association of Serum Uric Acid Status with Bone Mineral Density in Adolescents Aged 12–19 Years. Front. Med. 2020, 7, 255. [Google Scholar] [CrossRef]
- Yao, X.; Chen, L.; Xu, H.; Zhu, Z. The Association between Serum Uric Acid and Bone Mineral Density in Older Adults. Int. J. Endocrinol. 2020, 2020, 3082318. [Google Scholar] [CrossRef]
- Lee, H.N.; Kim, A.; Kim, Y.; Kim, G.T.; Sohn, D.H.; Lee, S.G. Higher serum uric acid levels are associated with reduced risk of hip osteoporosis in postmenopausal women with rheumatoid arthritis. Medicine 2020, 99, e20633. [Google Scholar] [CrossRef]
- Aguayo, R.S.; Baradad, M.; Soria, X.; Abal, L.; Sanmartin, V.; Egido, R.; Gallel, P.; Casanova, J.M.; Marti, R.M. Unilateral milia-type intradermal tophi associated with underlying urate subcutaneous deposition: An uncommon cutaneous presentation of gout. Clin. Exp. Dermatol. 2013, 38, 622–625. [Google Scholar] [CrossRef]
- Pradhan, S.; Sinha, R.; Sharma, P.; Sinha, U. Atypical Cutaneous Presentation of Chronic Tophaceous Gout: A Case Report. Indian Dermatol. Online J. 2020, 11, 235–238. [Google Scholar] [PubMed]
- Howren, A.; Bowie, D.; Choi, H.K.; Rai, S.K.; De Vera, M.A. Epidemiology of depression and anxiety in gout: A systematic review and metaanalysis. J. Rheumatol. 2020, 48, 129–137. [Google Scholar] [CrossRef]
- Zhou, Q.; Shao, Y.C.; Gan, Z.Q.; Fang, L.S. Lower vitamin D levels are associated with depression in patients with gout. Neuropsychiatr. Dis. Treat. 2019, 15, 227–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascart, T.; Ramon, A.; Ottaviani, S.; Legrand, J.; Ducoulombier, V.; Houvenagel, E.; Norberciak, L.; Richette, P.; Becce, F.; Ornetti, P. Association of Specific Comorbidities with Monosodium Urate Crystal Deposition in Urate-Lowering Therapy-Naive Gout Patients: A Cross-Sectional Dual-Energy Computed Tomography Study. J. Clin. Med. 2020, 9, 1295. [Google Scholar] [CrossRef]
- Sun, R.; Lu, J.; Li, H.; Cheng, X.; Xin, Y.; Li, C. Evaluation of Febuxostat Initiation During an Acute Gout Attack: A Prospective, Randomized Clinical Trial. Jt. Bone Spine 2020, 87, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Honarpisheh, M.; Li, C.; Sellmayr, M.; Lindenmeyer, M.; Bohland, C.; Romagnani, P.; Anders, H.J.; Steiger, S. Soluble Uric Acid Is an Intrinsic Negative Regulator of Monocyte Activation in Monosodium Urate Crystal-Induced Tissue Inflammation. J. Immunol. 2020, 205, 789–800. [Google Scholar] [CrossRef]
- Jung, S.W.; Kim, S.M.; Kim, Y.G.; Lee, S.H.; Moon, J.Y. Uric acid and inflammation in kidney disease. Am. J. Physiol. Renal. Physiol. 2020, 318, F1327–F1340. [Google Scholar] [CrossRef] [PubMed]
- Cortese, F.; Giordano, P.; Scicchitano, P.; Faienza, M.F.; De Pergola, G.; Calculli, G.; Meliota, G. Uric acid in metabolic and cerebrovascular disorders: A review. Curr. Vasc. Pharmacol. 2019, 18, 610–618. [Google Scholar] [CrossRef]
- Temmoku, J.; Fujita, Y.; Matsuoka, N.; Urano, T.; Furuya, M.Y.; Asano, T.; Sato, S.; Matsumoto, H.; Watanabe, H.; Kozuru, H.; et al. Uric acid-mediated inflammasome activation in IL-6 primed innate immune cells is regulated by baricitinib. Mod. Rheumatol. 2021, 31, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Kirilmaz, B.; Asgun, F.; Alioglu, E.; Ercan, E.; Tengiz, I.; Turk, U.; Saygi, S.; Ozerkan, F. High inflammatory activity related to the number of metabolic syndrome components. J. Clin. Hypertens. 2010, 12, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.A.; Sanchez-Lozada, L.G.; Johnson, R.J.; Kang, D.H. Oxidative stress with an activation of the renin-angiotensin system in human vascular endothelial cells as a novel mechanism of uric acid-induced endothelial dysfunction. J. Hypertens. 2010, 28, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Spiga, R.; Marini, M.A.; Mancuso, E.; Di Fatta, C.; Fuoco, A.; Perticone, F.; Andreozzi, F.; Mannino, G.C.; Sesti, G. Uric Acid Is Associated with Inflammatory Biomarkers and Induces Inflammation Via Activating the NF-kappaB Signaling Pathway in HepG2 Cells. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1241–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Reyes, C.P.; Manjarrez-Reyna, A.N.; Mendez-Garcia, L.A.; Aguayo-Guerrero, J.A.; Aguirre-Sierra, B.; Villalobos-Molina, R.; Lopez-Vidal, Y.; Bobadilla, K.; Escobedo, G. Uric Acid Has Direct Proinflammatory Effects on Human Macrophages by Increasing Proinflammatory Mediators and Bacterial Phagocytosis Probably via URAT1. Biomolecules 2020, 10, 576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarty, D.J., Jr. Mechanisms of the crystal deposition diseases--gout and pseudogout. Ann. Intern. Med. 1973, 78, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Cabau, G.; Crisan, T.O.; Kluck, V.; Popp, R.A.; Joosten, L.A.B. Urate-induced immune programming: Consequences for gouty arthritis and hyperuricemia. Immunol. Rev. 2020, 294, 92–105. [Google Scholar] [CrossRef] [Green Version]
- Alberts, B.M.; Bruce, C.; Basnayake, K.; Ghezzi, P.; Davies, K.A.; Mullen, L.M. Secretion of IL-1beta From Monocytes in Gout Is Redox Independent. Front. Immunol. 2019, 10, 70. [Google Scholar] [CrossRef] [Green Version]
- Joosten, L.A.B.; Crisan, T.O.; Bjornstad, P.; Johnson, R.J. Asymptomatic hyperuricaemia: A silent activator of the innate immune system. Nat. Rev. Rheumatol. 2020, 16, 75–86. [Google Scholar] [CrossRef]
- Li, S.; Cui, L.; Cheng, J.; Shu, R.; Chen, S.; Nguyen, U.S.; Misra, D.; Wu, S.; Gao, X. Repeated measurements of serum urate and mortality: A prospective cohort study of 152,358 individuals over 8 years of follow-up. Arthritis Res. Ther. 2020, 22, 84. [Google Scholar] [CrossRef] [Green Version]
- Felten, R.; Duret, P.M.; Gottenberg, J.E.; Spielmann, L.; Messer, L. At the crossroads of gout and psoriatic arthritis: “psout”. Clin. Rheumatol. 2020, 39, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Jiang, Y.; Wang, Y.; Qu, X.; Li, L.; Lou, X.; Guo, H.; Liu, Y. Male asymptomatic hyperuricemia patients display a lower number of NKG2D+ NK cells before and after a low-purine diet. Medicine 2018, 97, e13668. [Google Scholar] [CrossRef] [PubMed]
- Joosten, L.A.; Netea, M.G.; Mylona, E.; Koenders, M.I.; Malireddi, R.K.; Oosting, M.; Stienstra, R.; van de Veerdonk, F.L.; Stalenhoef, A.F.; Giamarellos-Bourboulis, E.J.; et al. Engagement of fatty acids with Toll-like receptor 2 drives interleukin-1beta production via the ASC/caspase 1 pathway in monosodium urate monohydrate crystal-induced gouty arthritis. Arthritis Rheum. 2010, 62, 3237–3248. [Google Scholar] [CrossRef]
- Rasheed, H.; Stamp, L.K.; Dalbeth, N.; Merriman, T.R. Interaction of the GCKR and A1CF loci with alcohol consumption to influence the risk of gout. Arthritis Res. Ther. 2017, 19, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chhana, A.; Lee, G.; Dalbeth, N. Factors influencing the crystallization of monosodium urate: A systematic literature review. BMC Musculoskelet. Disord. 2015, 16, 296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aliste-Fernandez, M.; San-Jose, P.; Aguadero, V. White blood cell count and total protein concentration to predict the absence of microcrystals in synovial fluid. Clin. Biochem. 2020, 83, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.Y.; Waldman, B.; O’Connell, R.; Sullivan, D.R.; Scott, R.S.; Aryal, N.; Gebski, V.; Marschner, I.; Taskinen, M.R.; Simes, J.R.; et al. Uric acid predicts long-term cardiovascular risk in type 2 diabetes but does not mediate the benefits of fenofibrate: The FIELD study. Diabetes Obes. Metab. 2020, 22, 1388–1396. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Jiang, Y.; Huang, Y.; Song, W.; Li, X.; Ou, J.; Wei, Q.; Gu, J. The comparison of dyslipidemia and serum uric acid in patients with gout and asymptomatic hyperuricemia: A cross-sectional study. Lipids Health Dis. 2020, 19, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascual, E.; Addadi, L.; Andres, M.; Sivera, F. Mechanisms of crystal formation in gout-a structural approach. Nat. Rev. Rheumatol. 2015, 11, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Martillo, M.A.; Nazzal, L.; Crittenden, D.B. The crystallization of monosodium urate. Curr. Rheumatol. Rep. 2014, 16, 400. [Google Scholar] [CrossRef]
- Pritzker, K.P.; Gay, S.; Jimenez, S.A.; Ostergaard, K.; Pelletier, J.P.; Revell, P.A.; Salter, D.; van den Berg, W.B. Osteoarthritis cartilage histopathology: Grading and staging. Osteoarthr. Cartil. 2006, 14, 13–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dang, N.L.H.; Kim, J.K.; Lee, K.B. Crystal-Induced Arthritis After Total Ankle Arthroplasty. J. Am. Podiatr. Med. Assoc. 2019, 109, 159–161. [Google Scholar] [CrossRef]
- Ning, Y.; Yang, G.; Chen, Y.; Zhao, X.; Qian, H.; Liu, Y.; Chen, S.; Shi, G. Characteristics of the Urinary Microbiome from Patients With Gout: A Prospective Study. Front. Endocrinol. 2020, 11, 272. [Google Scholar] [CrossRef] [PubMed]
- Wilhelmi de Toledo, F.; Grundler, F.; Goutzourelas, N.; Tekos, F.; Vassi, E.; Mesnage, R.; Kouretas, D. Influence of Long-Term Fasting on Blood Redox Status in Humans. Antioxidants 2020, 9, 496. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Xie, J.; Li, Z.; Field, C.; Block, C.; Taylor, T. Effect of Uric Acid Control on Serum Creatinine. J. Clin. Rheumatol. 2019, 25, 279–283. [Google Scholar] [CrossRef]
- Kubota, M. Hyperuricemia in Children and Adolescents: Present Knowledge and Future Directions. J. Nutr. Metab. 2019, 2019, 3480718. [Google Scholar] [CrossRef]
- Mishima, E.; Anzai, N.; Miyazaki, M.; Ab. Uric Acid Elevation by Favipiravir, an Antiviral Drug. Tohoku J. Exp. Med. 2020, 251, 87–90. [Google Scholar] [CrossRef]
- Batandier, C.; Poyot, T.; Marissal-Arvy, N.; Couturier, K.; Canini, F.; Roussel, A.M.; Hininger-Favier, I. Acute emotional stress and high fat/high fructose diet modulate brain oxidative damage through NrF2 and uric acid in rats. Nutr. Res. 2020, 79, 23–34. [Google Scholar] [CrossRef]
- Yoo, I.H.; Kim, W.; Cho, J.; Kim, H.; Lim, B.C.; Hwang, H.; Chae, J.H.; Choi, J.; Kim, K.J. Erratum to: Elevated Serum Uric Acid in Benign Convulsions with Mild Gastroenteritis in Children. J. Clin. Neurol. 2020, 16, 181. [Google Scholar] [CrossRef]
- Hase, R.; Kurata, R.; Ishida, K.; Kurita, T.; Muranaka, E.; Mito, H. Acute Gouty Arthritis During Favipiravir Treatment for Coronavirus Disease 2019: A Case Report. Intern. Med. 2020, 59, 2327–2329. [Google Scholar] [CrossRef]
- Abhishek, A.; Valdes, A.M.; Jenkins, W.; Zhang, W.; Doherty, M. Triggers of acute attacks of gout, does age of gout onset matter? A primary care based cross-sectional study. PLoS ONE 2017, 12, e0186096. [Google Scholar] [CrossRef] [PubMed]
- Flynn, T.J.; Cadzow, M.; Dalbeth, N.; Jones, P.B.; Stamp, L.K.; Hindmarsh, J.H.; Todd, A.S.; Walker, R.J.; Topless, R.; Merriman, T.R. Positive association of tomato consumption with serum urate: Support for tomato consumption as an anecdotal trigger of gout flares. BMC Musculoskelet. Disord. 2015, 16, 196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazard, A.; Bourrion, B.; Dechaine, F.; Fournier, L.; Francois, M. Lack of evidence for allopurinol for the prevention of a first gout attack in asymptomatic hyperuricemia: A systematic review. Eur. J. Clin. Pharmacol. 2020, 76, 897–899. [Google Scholar] [CrossRef]
- Zamora, A.E.; Naik, R. Calcium Pyrophosphate Deposition Disease. Available online: https://www.statpearls.com/ArticleLibrary/viewarticle/27935 (accessed on 31 December 2020).
- Chiang, S.L.; Ou, T.T.; Wu, Y.J.; Tu, H.P.; Lu, C.Y.; Huang, C.M.; Kuo, T.M.; Wang, T.N.; Chou, C.H.; Ko, Y.C. Increased level of MSU crystal-bound protein apolipoprotein A-I in acute gouty arthritis. Scand. J. Rheumatol. 2014, 43, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Cumpelik, A.; Ankli, B.; Zecher, D.; Schifferli, J.A. Neutrophil microvesicles resolve gout by inhibiting C5a-mediated priming of the inflammasome. Ann. Rheum. Dis. 2016, 75, 1236–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwangbo, D.S.; Lee, H.Y.; Abozaid, L.S.; Min, K.J. Mechanisms of Lifespan Regulation by Calorie Restriction and Intermittent Fasting in Model Organisms. Nutrients 2020, 12, 1194. [Google Scholar] [CrossRef] [PubMed]
- Filippou, G.; Scanu, A.; Adinolfi, A.; Picerno, V.; Toscano, C.; Bortoluzzi, A.; Frediani, B.; Govoni, M.; Punzi, L.; Scire, C.A. The two faces of the same medal... or maybe not? Comparing osteoarthritis and calcium pyrophosphate deposition disease: A laboratory and ultrasonographic study. Clin. Exp. Rheumatol. 2020, 39, 66–72. [Google Scholar] [PubMed]
- Chen, H.H.; Hsieh, M.C.; Ho, C.W.; Chen, C.C.; Hsu, S.P.; Chang, S.S.; Lin, C.L.; Kao, C.H. Increased the risk of heart failure and comorbidities in patients with gout treatment: A population-based cohort study. Ann. Transl. Med. 2020, 8, 462. [Google Scholar] [CrossRef]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; Gelber, A.C.; Harrold, L.R.; Khanna, D.; King, C.; et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Rheumatol. 2020, 72, 879–895. [Google Scholar] [CrossRef]
- Ellmann, H.; Bayat, S.; Araujo, E.; Manger, B.; Kleyer, A.; Cavallaro, A.; Lell, M.; Schenker, H.; Simon, D.; Tascilar, K.; et al. Effects of Conventional Uric Acid-Lowering Therapy on Monosodium Urate Crystal Deposits. Arthritis Rheumatol. 2020, 72, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Tang, Y.; Wang, M.; Wang, D.; Li, Q. The clinical efficacy of urate-lowering therapy in acute gout: A meta-analysis of randomized controlled trials. Clin. Rheumatol. 2020, 40, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Li, Y.; Li, L.; Kong, Y.; Shi, T.; Xiao, H.; Cao, S.; Zhu, H.; Li, Z.; Zhou, Y. Alterations of Serum Uric Acid Level and Gut Microbiota After Roux-en-Y Gastric Bypass and Sleeve Gastrectomy in a Hyperuricemic Rat Model. Obes. Surg. 2020, 30, 1799–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badv Badve, S.V.; Pascoe, E.M.; Tiku, A.; Boudville, N.; Brown, F.G.; Cass, A.; Clarke, P.; Dalbeth, N.; Day, R.O.; de Zoysa, J.R.; et al. Effects of Allopurinol on the Progression of Chronic Kidney Disease. N. Engl. J. Med. 2020, 382, 2504–2513. [Google Scholar] [CrossRef]
- Abhishek, A. Debates in gout management. Curr. Opin. Rheumato.l 2020, 32, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Day, R.; Nguyen, A.; Graham, G.; Aung, E.; Coleshill, M.; Stocker, S. Better outcomes for patients with gout. Inflammopharmacology 2020, 28, 1395–1400. [Google Scholar] [CrossRef]
- Jonsson, H.; Aspelund, T.; Eiriksdottir, G.; Harris, T.B.; Launer, L.J.; Gudnason, V. Hyperuricemia is associated with intermittent hand joint pain in a cross sectional study of elderly females: The AGES-Reykjavik Study. PLoS ONE 2019, 14, e0221474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yip, K.; Cohen, R.E.; Pillinger, M.H. Asymptomatic hyperuricemia: Is it really asymptomatic? Curr. Opin. Rheumatol. 2020, 32, 71–79. [Google Scholar] [CrossRef]
- Hu, L.; Hu, G.; Xu, B.P.; Zhu, L.; Zhou, W.; Wang, T.; Bao, H.; Cheng, X. U-Shaped Association of Serum Uric Acid with All-Cause and Cause-Specific Mortality in US Adults: A Cohort Study. J. Clin. Endocrinol. Metab. 2020, 105, e597–e609. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Furuhashi, M.; Tanaka, M.; Numata, K.; Hisasue, T.; Hanawa, N.; Koyama, M.; Osanami, A.; Higashiura, Y.; Inyaku, M.; et al. U-shaped relationship between serum uric acid level and decline in renal function during a 10-year period in female subjects: BOREAS-CKD2. Hypertens. Res. 2021, 44, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Waring, W.S.; McKnight, J.A.; Webb, D.J.; Maxwell, S.R. Uric acid restores endothelial function in patients with type 1 diabetes and regular smokers. Diabetes 2006, 55, 3127–3132. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Ye, Z.C.; Li, C.M.; Zhao, W.B.; Tang, H.; Liu, X.; Peng, H.; Lou, T.Q. Low serum uric acid levels increase the risk of all-cause death and cardiovascular death in hemodialysis patients. Ren. Fail. 2020, 42, 315–322. [Google Scholar] [CrossRef]
- Jiang, T.N.; Li, Y.F.; Huo, L.L.; Zhang, Q.; Wang, L.Y.; Zhao, C.L.; Liu, L.G. Association between serum uric acid and large-nerve fiber dysfunction in type 2 diabetes: A cross-sectional study. Chin. Med. J. 2019, 132, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Iki, M.; Yura, A.; Fujita, Y.; Kouda, K.; Tachiki, T.; Tamaki, J.; Sato, Y.; Moon, J.S.; Hamada, M.; Kajita, E.; et al. Relationships between serum uric acid concentrations, uric acid lowering medications, and vertebral fracture in community-dwelling elderly Japanese men: Fujiwara-kyo Osteoporosis Risk in Men (FORMEN) Cohort Study. Bone 2020, 139, 115519. [Google Scholar] [CrossRef]
- Kanbay, M.; Afsar, B.; Siriopol, D.; Dincer, N.; Erden, N.; Yilmaz, O.; Sag, A.A.; Kuwabara, M.; Cherney, D.; Rossignol, P.; et al. Effect of Uric Acid-Lowering Agents on Cardiovascular Outcome in Patients With Heart Failure: A Systematic Review and Meta-Analysis of Clinical Studies. Angiology 2020, 71, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Hasikova, L.; Pavlikova, M.; Hulejova, H.; Kozlik, P.; Kalikova, K.; Mahajan, A.; Herrmann, M.; Stiburkova, B.; Zavada, J. Serum uric acid increases in patients with systemic autoimmune rheumatic diseases after 3 months of treatment with TNF inhibitors. Rheumatol. Int. 2019, 39, 1749–1757. [Google Scholar] [CrossRef] [PubMed]
- Chi, X.; Zhang, H.; Zhang, S.; Ma, K. Chinese herbal medicine for gout: A review of the clinical evidence and pharmacological mechanisms. Chin. Med. 2020, 15, 17. [Google Scholar] [CrossRef] [Green Version]
- Loffler, W.; Fairbanks, L. Refractory Gout—Does It Exist? Nucleosides Nucleotides Nucleic Acids 2020, 39, 1410–1423. [Google Scholar] [CrossRef]
Figure 1.
Summary of the pathophysiologic roles of uric acid in humans as identified in the review.

Figure 2.
A summary of the prerequisite from hyperuricemia to gout flare. UA is involved in the pathogenesis of hyperuricemia and gout formation. Hyperuricemia could only be accompanied by the aforementioned factor(s) to instigate a gout flare. + Favorable; − Adverse; UA: uric acid.
Figure 2.
A summary of the prerequisite from hyperuricemia to gout flare. UA is involved in the pathogenesis of hyperuricemia and gout formation. Hyperuricemia could only be accompanied by the aforementioned factor(s) to instigate a gout flare. + Favorable; − Adverse; UA: uric acid.


{kind=link}
{kind=link}
Table 1.
Common medications for the treatments of hyperuricemia and gout flares.
| Drug | Brand Name(s) | Action Mechanism | Therapeutic Function |
|---|---|---|---|
| Allopurinol | Aloprim, Zyloprim | Xanthine oxidase inhibitor. | Reduces uric acid production. |
| Febuxostat | Ulonic | Xanthine oxidase inhibitor. | Reduces uric acid production. |
| Lesinurad | Zurampic | URATI inhibitor. | Helps your body get rid of uric acid when you pee. |
| Colchicine | Colcrys, Mitigare | Blocker of mitotic cells in metaphase. | Reduces inflammation. |
| Indomethacin | Indocin, Tivorbex | Inhibitor of the synthesis of prostaglandins. | Relieves the NSAID pain. |
| Probenecid | Probalan | Inhibition of a renal tubular transporter. | Helps the kidneys excrete uric acid from your body. |
| Losartan | Cozaar | Inhibition of urate/anion transport in kidneys. | Reduces uric acid levels. |
| Corticosteroids | Orapred, Prelone, etc. | Suppressor of the multiple inflammatory genes. | Fights with inflammation. |
| Fenofibrate | Antara, Fenoglide, Lipofen, Lofibra, TriCor, Triglide | Increase of uric acid solubility. | Reduces uric acid levels. |
| Pegloticase | Krystexxa | Recombinant urate oxidase. | Breaks down uric acid. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zhang, W.-Z. Why Does Hyperuricemia Not Necessarily Induce Gout? Biomolecules 2021, 11, 280. https://doi.org/10.3390/biom11020280
AMA Style
Zhang W-Z. Why Does Hyperuricemia Not Necessarily Induce Gout? Biomolecules. 2021; 11(2):280. https://doi.org/10.3390/biom11020280
Chicago/Turabian StyleZhang, Wei-Zheng. 2021. "Why Does Hyperuricemia Not Necessarily Induce Gout?" Biomolecules 11, no. 2: 280. https://doi.org/10.3390/biom11020280
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.