Metabolites Associated with Vigor to Frailty Among Community-Dwelling Older Black Men

Abstract
:1. Introduction
2. Results
2.1. Characteristics of 287 Health ABC Black Men by Tertiles of SAVE Scores
2.2. Metabolites Correlated with SAVE scores
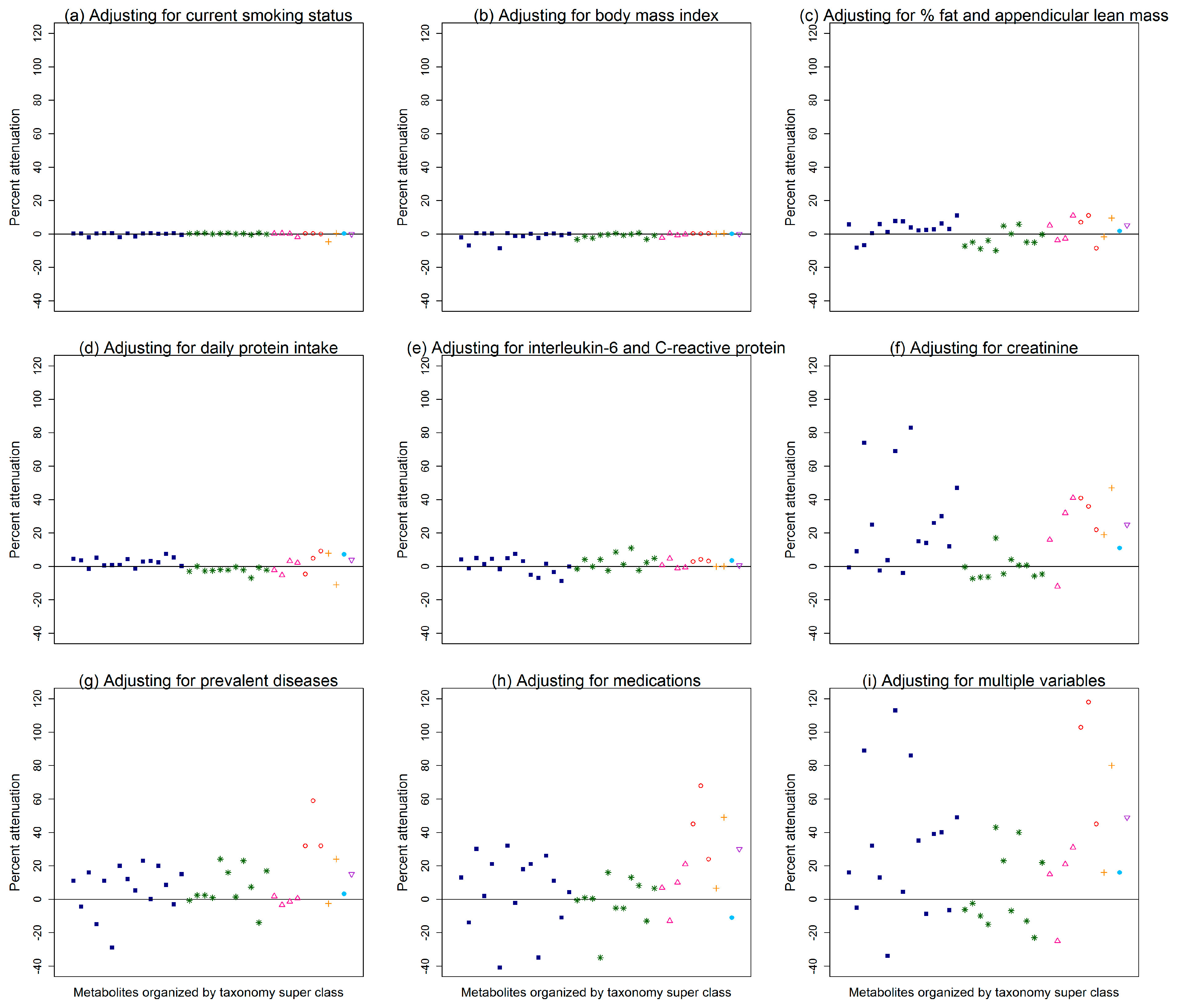
2.3. Attenuation of the Association between Metabolites and SAVE Scores after Additional Adjustments
2.4. Pathway Analysis
3. Discussion
4. Materials and Methods
4.1. The Health, Aging, and Body Composition (Health ABC) Study
4.2. Metabolites
4.3. Scale of Aging Vigor in Epidemiology (SAVE)
Health ABC Black Men with Information on Metabolites and the SAVE
4.4. Potential Confounders or Mediators of Metabolites and SAVE Scores
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bandeen-Roche, K.; Seplaki, C.L.; Huang, J.; Buta, B.; Kalyani, R.R.; Varadhan, R.; Xue, Q.L.; Walston, J.D.; Kasper, J.D. Frailty in older adults: A nationally representative profile in the United States. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, S.A.; Wershof Schwartz, A.; Karunananthan, S.; Bergman, H.; Clarfield, A.M. The identification of frailty: A systematic literature review. J. Am. Geriatr. Soc. 2011, 59, 2129–2138. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Graham, J.E.; Mogilner, A.J.; Rockwood, K. Frailty, fitness and late-life mortality in relation to chronological and biological age. BMC Geriatr. 2002, 2, 1. [Google Scholar] [CrossRef]
- Sanders, J.L.; Boudreau, R.M.; Fried, L.P.; Walston, J.D.; Harris, T.B.; Newman, A.B. Measurement of organ structure and function enhances understanding of the physiological basis of frailty: The Cardiovascular Health Study. J. Am. Geriatr. Soc. 2011, 59, 1581–1588. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.L.; Singh, J.; Minster, R.L.; Walston, J.D.; Matteini, A.M.; Christensen, K.; Mayeux, R.; Borecki, I.B.; Perls, T.; Newman, A.B. Association between mortality and heritability of the scale of aging vigor in epidemiology. J. Am. Geriatr. Soc. 2016, 64, 1679–1683. [Google Scholar] [CrossRef] [PubMed]
- Murphy, R.A.; Moore, S.C.; Playdon, M.; Meirelles, O.; Newman, A.B.; Milijkovic, I.; Kritchevsky, S.B.; Schwartz, A.; Goodpaster, B.H.; Sampson, J.; et al. Metabolites associated with lean mass and adiposity in older black men. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1352–1359. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D.S.; Tzur, D.; Knox, C.; Eisner, R.; Guo, A.C.; Young, N.; Cheng, D.; Jewell, K.; Arndt, D.; Sawhney, S. HMDB: The human metabolome database. Nucleic Acids Res. 2007, 35, D521–D526. [Google Scholar] [CrossRef] [PubMed]
- Lustgarten, M.S.; Price, L.L.; Chale, A.; Phillips, E.M.; Fielding, R.A. Branched chain amino acids are associated with muscle mass in functionally limited older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Fazelzadeh, P.; Hangelbroek, R.W.; Tieland, M.; de Groot, L.C.; Verdijk, L.B.; van Loon, L.J.; Smilde, A.K.; Alves, R.D.; Vervoort, J.; Müller, M.; et al. The muscle metabolome differs between healthy and frail older adults. J. Proteome Res. 2016, 15, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Pérez, D.; Sánchez-Flores, M.; Maseda, A.; Lorenzo-López, L.; Millán-Calenti, J.C.; Strasser, B.; Gostner, J.M.; Fuchs, D.; Pásaro, E.; Valdiglesias, V.; et al. Frailty status in older adults is related to alterations in indoleamine 2, 3-dioxygenase 1 and guanosine triphosphate cyclohydrolase I enzymatic pathways. J. Am. Med. Dir. Assoc. 2017, 18, 1049–1057. [Google Scholar] [CrossRef]
- Cheng, S.; Shah, S.H.; Corwin, E.J.; Fiehn, O.; Fitzgerald, R.L.; Gerszten, R.E.; Illig, T.; Rhee, E.P.; Srinivas, P.R.; Wang, T.J.; et al. Potential impact and study considerations of metabolomics in cardiovascular health and disease: A scientific statement from the American Heart Association. Circ. Cardiovasc. Genet. 2017, 10, e000032. [Google Scholar] [CrossRef] [PubMed]
- Newgard, C.B.; An, J.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Lien, L.F.; Haqq, A.M.; Shah, S.H.; Arlotto, M.; Slentz, C.A.; et al. A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab. 2009, 9, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Larson, M.G.; Vasan, R.S.; Cheng, S.; Rhee, E.P.; McCabe, E.; Lewis, G.D.; Fox, C.S.; Jacques, P.F.; Fernandez, C.; et al. Metabolite profiles and the risk of developing diabetes. Nat. Med. 2011, 17, 448–453. [Google Scholar] [CrossRef] [Green Version]
- Murphy, R.A.; Moore, S.; Playdon, M.; Kritchevsky, S.; Newman, A.B.; Satterfield, S.; Ayonayon, H.; Clish, C.; Gerszten, R.; Harris, T.B. Metabolites associated with risk of developing mobility disability in the Health, Aging and Body Composition Study. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Yeri, A.; Murphy, R.A.; Marron, M.M.; Clish, C.; Harris, T.B.; Lewis, G.D.; Newman, A.B.; Murthy, V.L.; Shah, R.V. Metabolite profiles of healthy aging index are associated with cardiovascular disease in African Americans: the Health, Aging, and Body Composition Study. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Cynober, L.A. Plasma amino acid levels with a note on membrane transport: characteristics, regulation, and metabolic significance. Nutrition 2002, 18, 761–766. [Google Scholar] [CrossRef]
- Kahl, S.; Roden, M. Amino acids—lifesaver or killer in patients with diabetes? Nat. Rev. Endocrinol. 2018, 14, 449–451. [Google Scholar] [CrossRef]
- Volpi, E.; Campbell, W.W.; Dwyer, J.T.; Johnson, M.A.; Jensen, G.L.; Morley, J.E.; Wolfe, R.R. Is the optimal level of protein intake for older adults greater than the recommended dietary allowance? J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 677–681. [Google Scholar] [CrossRef]
- Deer, R.R.; Volpi, E. Protein Requirements in Critically Ill Older Adults. Nutrients 2018, 10, 378. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Newman, A.B.; Haggerty, C.L.; Goodpaster, B.; Harris, T.; Kritchevsky, S.; Nevitt, M.; Miles, T.P.; Visser, M. Strength and muscle quality in a well-functioning cohort of older adults: the Health, Aging and Body Composition study. J. Am. Geriatr. Soc. 2003, 51, 323–330. [Google Scholar] [CrossRef]
- Townsend, M.K.; Clish, C.B.; Kraft, P.; Wu, C.; Souza, A.L.; Deik, A.A.; Tworoger, S.S.; Wolpin, B.M. Reproducibility of metabolomic profiles among men and women in 2 large cohort studies. Clin. Chem. 2013, 59, 1657–1667. [Google Scholar] [CrossRef]
- Paynter, N.P.; Balasubramanian, R.; Giulianini, F.; Wang, D.D.; Tinker, L.F.; Gopal, S.; Deik, A.A.; Bullock, K.; Pierce, K.A.; Scott, J.; et al. Metabolic predictors of incident coronary heart disease in women. Circulation 2018, 137, 841–853. [Google Scholar] [CrossRef]
- Diniz, B.S.; Sibille, E.; Ding, Y.; Tseng, G.; Aizenstein, H.J.; Lotrich, F.; Becker, J.T.; Lopez, O.L.; Lotze, M.T.; Klunk, W.E.; et al. Plasma biosignature and brain pathology related to persistent cognitive impairment in late-life depression. Mol. Psychiatry. 2015, 20, 594–601. [Google Scholar] [CrossRef]
- Houston, D.K.; Nicklas, B.J.; Ding, J.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Lee, J.S.; Sahyoun, N.R.; Visser, M.; Kritchevsky, S.B. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: the Health, Aging, and Body Composition (Health ABC) Study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Xia, J.; Wishart, D.S. Using metaboanalyst 3.0 for comprehensive metabolomics data analysis. Curr. Protoc. Bioinform. 2016, 55, 14.10. 11–14.10. 91. [Google Scholar] [CrossRef]


{kind=link}
| Mean (Standard Deviation) or Frequency (Percent) | SAVE Tertiles | Overall p-Value, Pairwise Comparisons | ||
|---|---|---|---|---|
| Vigorous (T1) n = 73 | Average (T2) n = 105 | Frail (T3) n =1 09 | ||
| SAVE scores | 2.4 (0.7) Range: 0–3 | 4.5 (0.5) Range: 4–5 | 7.0 (1.1) Range: 6–10 | - |
| Age | 74 (3) | 75 (3) | 75 (3) | 0.006, T1 < T2, T3 |
| Pittsburgh site | 34 (47%) | 56 (53%) | 63 (58%) | 0.33 |
| More than high school education | 28 (38%) | 24 (23%) | 28 (26%) | 0.06 |
| Current smoker at baseline | 9 (12%) | 22 (21%) | 21 (19%) | 0.31 |
| Body mass index (kg/m2) | 27 (4) | 27 (4) | 27 (5) | 0.82 |
| Dietary intake: | ||||
| Total calories (Kcal/day) | 2329 (1111) | 2199 (1022) | 2095 (1038) | 0.35 |
| Protein intake (g/day) | 81 (44) | 75 (37) | 73 (39) | 0.41 |
| Percent of daily calories from protein | 14 (3) | 14 (3) | 14 (3) | 0.82 |
| Daily protein intake per body weight (g/kg) | 1.0 (0.6) | 0.97 (0.5) | 0.94 (0.5) | 0.71 |
| Fat intake (g/day) | 92 (51) | 87 (49) | 81 (48) | 0.30 |
| Percent of daily calories from fat | 35 (6) | 35 (8) | 34 (8) | 0.57 |
| Body composition: | ||||
| Appendicular lean mass (kg/m2) | 8.4 (1) | 8.3 (1) | 8.3 (1) | 0.68 |
| Percent fat | 28 (5) | 28 (5) | 28 (6) | 0.92 |
| Inflammation markers: | ||||
| Interleukin-6 (pg/mL) | 4.2 (5.9) Median = 2.5 | 3.2 (2.2) Median = 2.4 | 4.2 (3.4) Median = 3.0 | 0.05 |
| C-reactive protein (ug/mL) | 5.4 (8.9) Median = 2.8 | 5.3 (9.7) Median = 2.1 | 8.4 (16) Median = 3.9 | 0.05 |
| Markers of kidney disease at baseline: | ||||
| Creatinine (mg/dL) | 1.2 (0.2) Median = 1.2 | 1.2 (0.3) Median = 1.2 | 1.3 (0.4) Median = 1.2 | 0.04 |
| Cystatin C (mg/L) | 1.0 (0.2) Median = 0.96 | 1.0 (0.3) Median = 1.0 | 1.1 (0.3) Median = 1.1 | 0.05 |
| Glomerular filtration rate | 77 (17) | 75 (19) | 70 (19) | 0.03, T1 > T3 |
| Prevalent disease at baseline: | ||||
| Cardiovascular disease | 11 (15%) | 36 (34%) | 39 (36%) | 0.006, T1 < T2, T3 |
| Hypertension | 34 (47%) | 65 (62%) | 67 (61%) | 0.08 |
| Diabetes | 8 (11%) | 18 (17%) | 37 (34%) | 0.0004, T1, T2 < T3 |
| Cancer | 10 (14%) | 11 (10%) | 11 (10%) | 0.72 |
| Peripheral artery disease | 2 (3%) | 7 (7%) | 9 (8%) | 0.32 |
| Osteoarthritis | 2 (3%) | 9 (9%) | 11 (10%) | 0.17 |
| Depression | 4 (5%) | 5 (5%) | 8 (7%) | 0.71 |
| Pulmonary disease | 7 (10%) | 8 (8%) | 21 (19%) | 0.02, T2<T3 |
| Kidney disease | 1 (1%) | 2 (2%) | 0 | 0.36 |
| Medication use: | ||||
| Total number of prescription medications | 2.2 (2) | 3.0 (3) | 4.0 (4) | 0.0003, T1,T2 < T3 |
| Antihypertensive medications | 35 (48%) | 64 (61%) | 74 (68%) | 0.03, T1 < T3 |
| Antilipemic medications | 14 (19%) | 11 (10%) | 17 (16%) | 0.25 |
| Medications for diabetes: | 5 (7%) | 17 (16%) | 36 (33%) | <0.0001, T1, T2 < T3 |
| Insulin | 0 | 2 (2%) | 10 (9%) | 0.004, T1, T2 < T3 |
| Oral hypoglycemic | 5 (7%) | 15 (14%) | 28 (26%) | 0.003, T1, T2 < T3 |
| Medications for prostate disease | 10 (14%) | 14 (13%) | 19 (17%) | 0.83, P = 0.66 |
| Medications for pulmonary diseases | 5 (7%) | 2 (2%) | 13 (12%) | 0.02, T2 < T3 |
| Spasmolytics (theophylline and others) | 0 | 1 (1%) | 5 (5%) | 0.09 |
| Anti-inflammatory | 24 (33%) | 43 (41%) | 52 (49%) | 0.09 |
| Log-Transformed and Standardized Metabolites | Human Metabolome Database ID Number | Human Metabolome Database Taxonomy Sub Class | Continuous SAVE Scores, Adjusting for Age and Study Site (N = 287) | Continuous SAVE Scores, Adjusting for Multiple Variables 1 (n = 257) | ||
|---|---|---|---|---|---|---|
| Correlation, p-Value | False Discovery Rate | Correlation, p-Value | Percent Attenuation 2 | |||
| Glucuronate | HMDB00127 | Carbohydrates/carbohydrate conjugates | 0.21, p = 0.0003 | 0.08 | 0.12, p = 0.07 | 49% |
| Tryptophan | HMDB00929 | Indolyl carboxylic acids/derivatives | −0.21, p = 0.0005 | 0.08 | −0.18, p = 0.005 | 15% |
| Methionine | HMDB00696 | Amino acids/peptides/analogues | −0.19, p = 0.001 | 0.15 | −0.13, p = 0.04 | 16% |
| N-carbamoyl-beta-alanine | HMDB00026 | Ureas | 0.17, p = 0.004 | 0.22 | 0.13, p = 0.045 | 39% |
| Tyrosine | HMDB00158 | Amino acids/peptides/analogues | −0.17, p = 0.004 | 0.22 | −0.16, p = 0.01 | −5% |
| Isocitrate | HMDB00193 | Tricarboxylic acids and derivatives | 0.17, p = 0.004 | 0.22 | 0.11, p = 0.08 | 40% |
| Creatinine | HMDB00562 | Amino acids/peptides/analogues | 0.16, p = 0.008 | 0.27 | 0.02, p = 0.79 | 89% |
| C4-OH carnitine | HMDB13127 | Beta hydroxy acids/derivatives | 0.16, p = 0.009 | 0.27 | 0.10, p = 0.14 | 34% |
| C14:0 SM | HMDB12097 | Phosphosphingolipids | −0.15, p = 0.009 | 0.27 | −0.14, p = 0.03 | −6% |
| Cystathionine | HMDB00099 | Amino acids/peptides/analogues | 0.15, p = 0.009 | 0.27 | 0.11, p = 0.09 | 32% |
| Hydroxyphenylacetate | HMDB00020 | 1-hydroxy-2-unsubstituted benzenoids | 0.15, p = 0.01 | 0.27 | −0.004, p = 0.95 | 103% |
| Putrescine | HMDB01414 | Amines | 0.15, p = 0.01 | 0.27 | 0.11, p = 0.09 | 16% |
| 1-methylnicotinamide | HMDB00699 | Pyridinecarboxylic acids/derivatives | −0.15, p = 0.01 | 0.27 | −0.18, p = 0.004 | −25% |
| Asparagine | HMDB00168 | Amino acids/peptides/analogues | −0.15, p = 0.01 | 0.27 | −0.12, p = 0.07 | 13% |
| Leucine | HMDB00687 | Amino acids/peptides/analogues | −0.14, p = 0.02 | 0.35 | −0.19, p = 0.003 | −34% |
| 5-aminolevulinic acid | HMDB01149 | Amino acids/peptides/analogues | 0.14, p = 0.02 | 0.36 | −0.02, p = 0.81 | 113% |
| Inosine | HMDB00195 | Not available | 0.14, p = 0.02 | 0.39 | 0.12, p = 0.06 | 16% |
| Histidine | HMDB00177 | Amino acids/peptides/analogues | −0.13, p = 0.03 | 0.39 | −0.12, p = 0.07 | 4% |
| C34:3 PE plasmalogen | HMDB11343 | Glycerophosphoethanolamines | −0.13, p = 0.03 | 0.39 | −0.08, p = 0.21 | −15% |
| Symmetric dimethylarginine (SDMA) | HMDB03334 | Amino acids/peptides/analogues | 0.13, p = 0.03 | 0.39 | 0.02, p = 0.77 | 86% |
| C24:1 ceramide (d18:1) | HMDB04953 | Ceramides | 0.13, p = 0.03 | 0.39 | 0.12, p = 0.06 | −7% |
| C36:4 PE | HMDB08937 | Glycerophosphoethanolamines | 0.13, p = 0.03 | 0.39 | 0.07, p = 0.31 | 43% |
| Urate | HMDB00289 | Purines/purine derivatives | 0.13, p = 0.03 | 0.39 | 0.11, p = 0.09 | 21% |
| C18:2 CE | HMDB00610 | Steroid esters | −0.13, p = 0.03 | 0.39 | −0.09, p = 0.17 | 22% |
| Trimethylamine-N-oxide | HMDB00925 | Aminoxides | 0.13, p = 0.03 | 0.39 | 0.02, p = 0.73 | 80% |
| 2-hydroxyglutarate | HMDB00694 | Short-chain hydroxy acids/derivatives | 0.13, p = 0.03 | 0.39 | 0.07, p = 0.29 | 49% |
| C24:0 SM | HMDB11697 | Phosphosphingolipids | −0.13, p = 0.03 | 0.39 | −0.13, p = 0.049 | −3% |
| Fumarate | HMDB00134 | Dicarboxylic acids/derivatives | 0.13, p = 0.03 | 0.39 | 0.19, p = 0.002 | −7% |
| C22:0 SM | HMDB12103 | Phosphosphingolipids | −0.13, p = 0.03 | 0.39 | −0.15, p = 0.02 | −10% |
| C20:5 LPC | HMDB10397 | Glycerophosphocholines | −0.12, p = 0.04 | 0.39 | −0.06, p = 0.36 | 40% |
| Salicylurate | HMDB00840 | Benzoic acids/derivatives | 0.12, p = 0.04 | 0.41 | −0.02, p = 0.75 | 118% |
| Homogentisate | HMDB00130 | Phenylacetic acids | 0.12, p = 0.04 | 0.41 | 0.08, p = 0.19 | 45% |
| Glycodeoxycholate | HMDB00631 | Bile acids, alcohols and derivatives | −0.12, p = 0.04 | 0.42 | −0.13, p = 0.045 | −13% |
| Malate | HMDB00156 | Beta hydroxy acids and derivatives | 0.12, p = 0.04 | 0.42 | 0.16, p = 0.01 | −9% |
| 5-hydroxytryptophan | HMDB00472 | Tryptamines and derivatives | −0.12, p = 0.04 | 0.42 | −0.10, p = 0.13 | 31% |
| C54:10 TAG | ---- | Triradylcglycerols | −0.12, p = 0.046 | 0.43 | −0.16, p = 0.01 | −23% |
| C44:13 PE plasmalogen | ---- | Glycerophosphoethanolamines | −0.12, p = 0.049 | 0.44 | −0.07, p = 0.29 | 23% |
| Pathways | Match Status | Fisher’s Exact Test p-Value | False Discovery Rate | Impact Score |
|---|---|---|---|---|
| Nitrogen metabolism | 5/39 | 0.00009 | 0.007 | 0.008 |
| Aminoacyl-tRNA biosynthesis | 6/75 | 0.0002 | 0.01 | 0 |
| Citric acid cycle | 3/20 | 0.002 | 0.05 | 0.12 |
| Tyrosine metabolism | 4/76 | 0.013 | 0.27 | 0.15 |
| Phenylalanine metabolism | 3/45 | 0.02 | 0.28 | 0 |
| Glycine, serine and threonine metabolism | 3/48 | 0.02 | 0.28 | 0 |
| Alanine, aspartate and glutamate metabolism | 2/24 | 0.03 | 0.37 | 0.05 |
| Sphingolipid metabolism | 2/25 | 0.04 | 0.37 | 0.30 |
| Phenylalanine, tyrosine and tryptophan biosynthesis | 2/27 | 0.04 | 0.37 | 0.007 |
| beta-Alanine metabolism | 2/28 | 0.05 | 0.37 | 0.04 |
| Five Items Used to Calculate the SAVE: | Best Tertile = 0 | Mid Tertile = 1 | Worst Tertile = 2 |
|---|---|---|---|
| 1. Weight change (kg) | >0.68 | <−1.36 to ≤0.68 | ≤−1.36 |
| 2. Physical activity 1 (kcal/kg/week) | ≥43 | >11 to <43 | ≤11 |
| 3. 20 m walk time (sec)** | ≤16 | >16 to ≤18 | >18 |
| 4. Grip strength (kg): | |||
| BMI < 24 | >38 | >32 to ≤38 | ≤32 |
| BMI ≥ 24 | >41 | >35 to ≤41 | ≤35 |
| 5. Usual energy level | 8 to 10 | 6 to 7 | 0 to 5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marron, M.M.; Harris, T.B.; Boudreau, R.M.; Clish, C.B.; Moore, S.C.; Murphy, R.A.; Murthy, V.L.; Sanders, J.L.; Shah, R.V.; Tseng, G.C.; et al. Metabolites Associated with Vigor to Frailty Among Community-Dwelling Older Black Men. Metabolites 2019, 9, 83. https://doi.org/10.3390/metabo9050083
Marron MM, Harris TB, Boudreau RM, Clish CB, Moore SC, Murphy RA, Murthy VL, Sanders JL, Shah RV, Tseng GC, et al. Metabolites Associated with Vigor to Frailty Among Community-Dwelling Older Black Men. Metabolites. 2019; 9(5):83. https://doi.org/10.3390/metabo9050083
Chicago/Turabian StyleMarron, Megan M., Tamara B. Harris, Robert M. Boudreau, Clary B. Clish, Steven C. Moore, Rachel A. Murphy, Venkatesh L. Murthy, Jason L. Sanders, Ravi V. Shah, George C. Tseng, and et al. 2019. "Metabolites Associated with Vigor to Frailty Among Community-Dwelling Older Black Men" Metabolites 9, no. 5: 83. https://doi.org/10.3390/metabo9050083