Carbapenemase-Producing Raoultella Planticola: A Rare Cause of Pneumonia and Bacteremia
by
 ,
,
Jose Armando Gonzales Zamora
1,* ,
,
Monica Corzo-Pedroza
1, 
Maria Romero Alvarez
1 and
Octavio V. Martinez
2 1
Division of Infectious Diseases, Department of Medicine, Miller School of Medicine, University of Miami, Miami, FL 33136, USA
2
Department of Pathology and Microbiology, Miller School of Medicine, University of Miami, Miami, FL 33136, USA
*
Author to whom correspondence should be addressed.
Diseases 2018, 6(4), 94; https://doi.org/10.3390/diseases6040094
Submission received: 23 September 2018
/
Revised: 9 October 2018
/
Accepted: 17 October 2018
/
Published: 17 October 2018
(This article belongs to the Section Infectious Disease)
{kind=link}
{kind=link}
Abstract
:Raoultella planticola is a gram-negative bacterium of the Enterobacteriaceae family that is usually found in soil, plant and aquatic environments. It is an uncommon human pathogen and has been associated with cases of bacteremia, pneumonia, urinary tract infections, among others. Here, we present the case of an 85-year-old female that developed nosocomial pneumonia and bacteremia caused by Raoultella planticola. Pertinent microbiological studies detected carbapenemase production codified by the blaKPC gene. The patient was successfully treated with ceftazidime/avibactam and polymyxin. Our case illustrates the pathogenic potential of this organism and highlights the importance of phenotypic and genotypic assays for the appropriate identification of carbapenemase production.
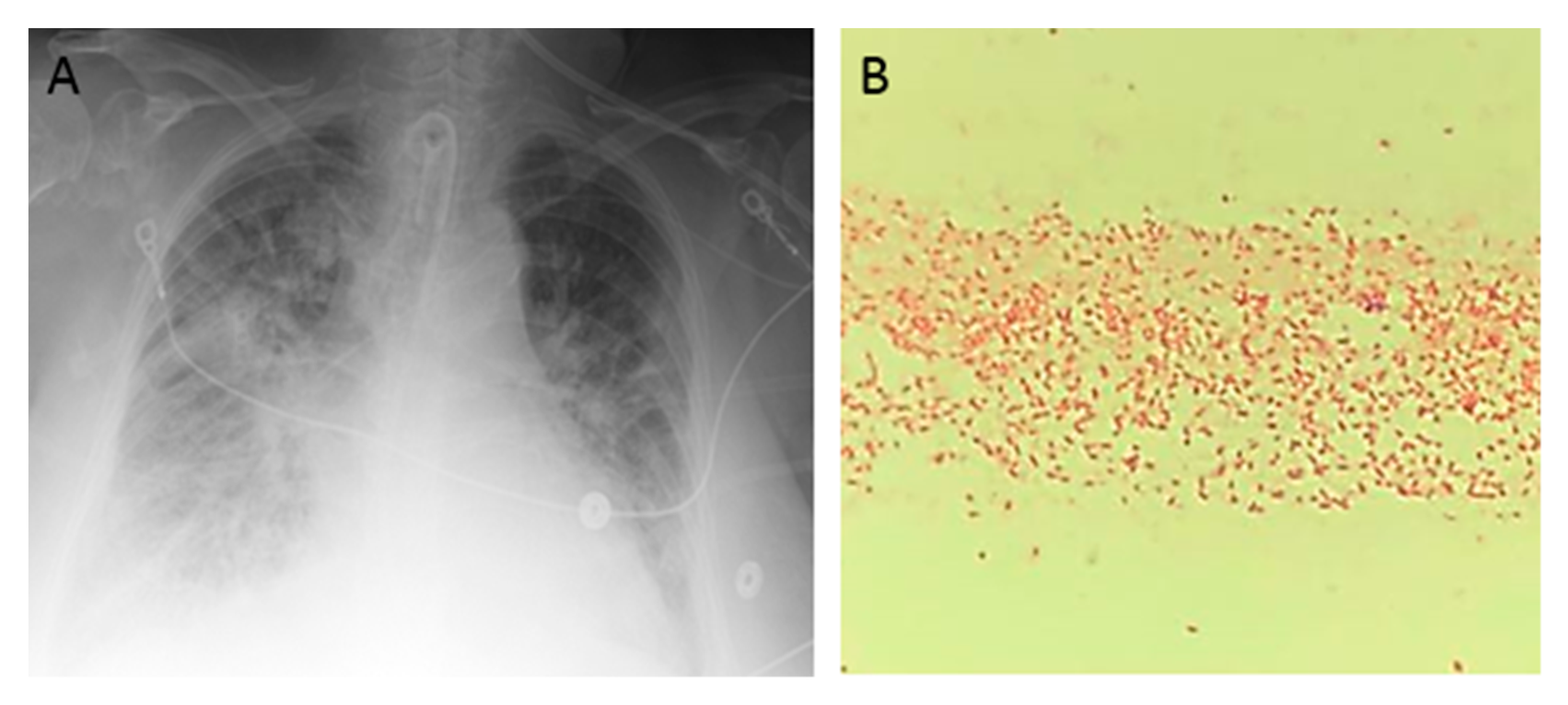
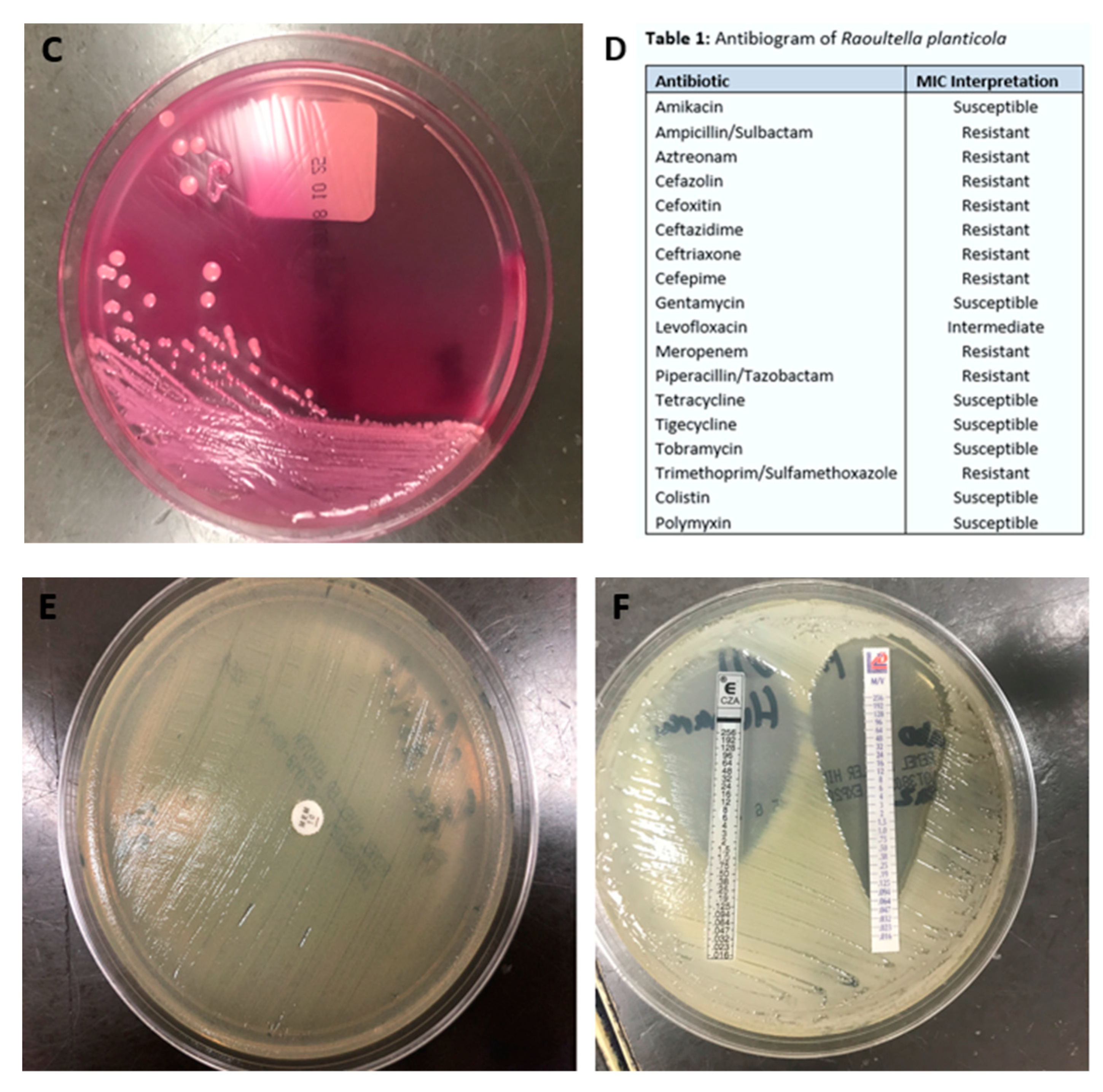
Figure 1.
An 85-year-old woman presented to the hospital after sustaining burn injuries and smoke exposure from a house fire. On admission, she was tachypneic, with a respiratory rate of 20 breaths per minute. Her physical exam was significant for 2nd degree burns along the dorsal and palmar aspects of her first three fingers on the right hand and partially on the index finger and thumb of her left hand. She had 1st degree burns on the rest of her hands and both forearms, as well as on the entire face and neck. Her wounds were debrided and silvedene was applied on her hands and forearms, while bacitracin was used for her face. Shortly after admission, the patient experienced difficulty breathing, trouble swallowing, voice changes and swelling around her mouth and tongue. She was intubated for airway protection and was transferred to the intensive care unit (ICU). She was extubated 2 days later, but re-intubated after an episode of projectile vomiting and aspiration. Due to the development of fevers, blood and urine cultures were taken. She was started on cefepime 2 g every 12 h and vancomycin 15 mg/kg every 12 h for aspiration pneumonia. Blood culture grew methicillin-sensitive Staphylococcus aureus and urine culture was positive for Morganella morganii. Four days later, she developed spontaneous pneumothorax that required chest tube placement. Persistence of fever and worsening leukocytosis prompted antibiotic escalation to meropenem with continuation of vancomycin. Over the next 2 days, the patient developed acute renal failure and was started on continuous veno-venous hemodialysis. She completed 12 days of antibiotics. Over the next week, she developed a central line bloodstream infection caused by Enterococcus faecalis and ventilator associated pneumonia caused by methicillin-sensitive Staphylococcus aureus, for which she was treated with ampicillin/sulbactam for 7 days. Three days later, the patient developed a new episode of fever and worsening bilateral infiltrates in chest X-ray (A). Cultures were obtained, and gram stain from blood culture and endotracheal aspirate revealed gram-negative bacilli (B). The Mac Conckey agar demonstrated a pink color, which is characteristic of lactose-fermenting organisms (C). The patient was started empirically on cefepime 2 g every 12 h, and the central lines were removed (one of the potential sources of infection). The gram-negative rod was identified as Raoultella planticola by MALDI-TOF (matrix-assisted laser desorption ionization time of flight), and further in-vitro susceptibility testing by the Vitek® 2 system (BioMérieux, Inc., Hazelwood, MO, USA) revealed resistance to most antibiotics, except for colistin, polymyxin B, aminoglycosides, tetracycline, and tigecycline (D). We performed additional phenotypic tests and detected carbapenemase production by the Carbapenem Inactivation Method (E). Supplementary antibiotic susceptibility studies by E-test showed susceptibility to ceftazidime/avibactam (F, left side) and meropenem/vaborbactam (F, right side). Confirmation of carbapenemase production was carried out by genotypic analysis using Verigene system (Luminex Corp, Austin, TX, USA), which identified blaKPC and blaCTX-M genes. Treatment with cefepime was discontinued and the patient was started on combination therapy with ceftazidime/avibactam and polymyxin B. Follow-up blood cultures were negative and her respiratory status improved over the following days. Finally, she was transferred to a LTAC (long-term acute care) facility to complete 2 weeks of antibiotic therapy.
Figure 1.
An 85-year-old woman presented to the hospital after sustaining burn injuries and smoke exposure from a house fire. On admission, she was tachypneic, with a respiratory rate of 20 breaths per minute. Her physical exam was significant for 2nd degree burns along the dorsal and palmar aspects of her first three fingers on the right hand and partially on the index finger and thumb of her left hand. She had 1st degree burns on the rest of her hands and both forearms, as well as on the entire face and neck. Her wounds were debrided and silvedene was applied on her hands and forearms, while bacitracin was used for her face. Shortly after admission, the patient experienced difficulty breathing, trouble swallowing, voice changes and swelling around her mouth and tongue. She was intubated for airway protection and was transferred to the intensive care unit (ICU). She was extubated 2 days later, but re-intubated after an episode of projectile vomiting and aspiration. Due to the development of fevers, blood and urine cultures were taken. She was started on cefepime 2 g every 12 h and vancomycin 15 mg/kg every 12 h for aspiration pneumonia. Blood culture grew methicillin-sensitive Staphylococcus aureus and urine culture was positive for Morganella morganii. Four days later, she developed spontaneous pneumothorax that required chest tube placement. Persistence of fever and worsening leukocytosis prompted antibiotic escalation to meropenem with continuation of vancomycin. Over the next 2 days, the patient developed acute renal failure and was started on continuous veno-venous hemodialysis. She completed 12 days of antibiotics. Over the next week, she developed a central line bloodstream infection caused by Enterococcus faecalis and ventilator associated pneumonia caused by methicillin-sensitive Staphylococcus aureus, for which she was treated with ampicillin/sulbactam for 7 days. Three days later, the patient developed a new episode of fever and worsening bilateral infiltrates in chest X-ray (A). Cultures were obtained, and gram stain from blood culture and endotracheal aspirate revealed gram-negative bacilli (B). The Mac Conckey agar demonstrated a pink color, which is characteristic of lactose-fermenting organisms (C). The patient was started empirically on cefepime 2 g every 12 h, and the central lines were removed (one of the potential sources of infection). The gram-negative rod was identified as Raoultella planticola by MALDI-TOF (matrix-assisted laser desorption ionization time of flight), and further in-vitro susceptibility testing by the Vitek® 2 system (BioMérieux, Inc., Hazelwood, MO, USA) revealed resistance to most antibiotics, except for colistin, polymyxin B, aminoglycosides, tetracycline, and tigecycline (D). We performed additional phenotypic tests and detected carbapenemase production by the Carbapenem Inactivation Method (E). Supplementary antibiotic susceptibility studies by E-test showed susceptibility to ceftazidime/avibactam (F, left side) and meropenem/vaborbactam (F, right side). Confirmation of carbapenemase production was carried out by genotypic analysis using Verigene system (Luminex Corp, Austin, TX, USA), which identified blaKPC and blaCTX-M genes. Treatment with cefepime was discontinued and the patient was started on combination therapy with ceftazidime/avibactam and polymyxin B. Follow-up blood cultures were negative and her respiratory status improved over the following days. Finally, she was transferred to a LTAC (long-term acute care) facility to complete 2 weeks of antibiotic therapy.


Raoultella planticola is a non-motile, aerobic, encapsulated, gram-negative bacterium that belongs to the Enterobacteriaceae family [1]. It is usually found in soil, plant and aquatic environments. Cases of human infections by this organism has been described sporadically, mainly causing bacteremia, pneumonia, cholangitis, retroperitoneal abscess, among others [2]. The growing utilization of automated identification systems has allowed the identification of more infections caused by Raoultella, a pathogen once classified as Klebsiella given its biochemical similarities [2]. The majority of the patients affected by this pathogen have certain degree of immunosuppression (malignancies, recent chemotherapy or post-transplant) or have a history of prolonged ICU hospitalization or recent trauma. In the present case, our patient developed pneumonia and bacteremia secondary to Raoultella after 40 days of ICU stay. Initial reports have described Raoultella as a low virulence pathogen, in which treatment with cephalosporins and carbapenems usually leads to excellent outcomes [1]. However, this perception has changed in recent years with the more frequent isolation of multidrug-resistant organisms with the capability of carbapenemase production. In a recent review, Xu et al. described the emergence of strains of Raoultella planticola with carbapenemase-producing genes, such as blaKPC, blaIMP, and blaNDM [3]. A total of six cases were reported in this review that included patients with pneumonia and bacteremia, whom prognosis was mostly fatal (4/6 deaths). Since then, four more cases of carbapenemase-producing Raoultella planticola have been reported in the literature, three of them carrying the blaOXA gene and one isolate with blaNDM [2,4]. The current availability of appropriate microbiological studies for the identification of carbapenemase production has facilitated the evaluation and treatment of patients that carry these isolates. Many phenotypic assays have been developed, of which the Carbapenem Inactivation Method is recognized as one of the most accurate, with a sensitivity of 91% and a specificity of 99% [5]. A huge progress has also taken place in genotypic assays, with several commercial methods that allow precise identification of carbapenemase producing genes. In our case, we used the Verigene system (Luminex Corp, Austin, TX, USA), that detects the five most common genes that codify carbapenemases. The treatment of these infections is very challenging, with more studies favoring combination therapy [6]. We opted for the use of ceftazidime/avibactam and polymyxin, obtaining very good outcomes. Our case illustrates the pathogenic potential of Raoultella planticola and highlights the importance of phenotypic and genotypic tests for the appropriate identification of carbapenem-resistant strains.
Author Contributions
J.A.G.Z., M.C.-P., and M.R.A. were involved in direct patient care; O.V.M. performed microbiological tests; J.A.G.Z. wrote the manuscript. All the authors have critically discussed, read and approved the final manuscript.
Funding
This research received no external funding.
Acknowledgments
The APC was sponsored by MDPI.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chun, S.; Yun, J.W.; Huh, H.J.; Lee, N.Y. Low virulence? Clinical characteristics of Raoultella planticola bacteremia. Infection 2014, 42, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Demiray, T.; Koroglu, M.; Ozbek, A.; Altindis, M. A rare cause of infection, Raoultella planticola: Emerging threat and new reservoir for carbapenem resistance. Infection 2016, 44, 713–717. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Xie, W.; Fu, Y.; Zhou, H.; Zhou, J. Nosocomial pneumonia caused by carbapenem-resistant Raoultella planticola: A case report and literature review. Infection 2015, 43, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Pan, Z.; Liu, R.; Zhang, P.; Zhou, H.; Fu, Y.; Zhou, J. Combination of Tigecycline and Levofloxacin for Successful Treatment of Nosocomial Pneumonia Caused by New Delhi Metallo-β-Lactamase-1-Producing Raoultella planticola. Microb. Drug Resist. 2017, 23, 127–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamma, P.D.; Opene, B.N.; Gluck, A.; Chambers, K.K.; Carroll, K.C.; Simner, P.J. Comparison of 11 Phenotypic Assays for Accurate Detection of Carbapenemase-Producing Enterobacteriaceae. J. Clin. Microbiol. 2017, 55, 1046–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritzenwanker, M.; Imirzalioglu, C.; Herold, S.; Wagenlehner, F.M.; Zimmer, K.P.; Chakraborty, T. Treatment Options for Carbapenem- Resistant Gram-Negative Infections. Dtsch. Arztebl. Int. 2018, 115, 345–352. [Google Scholar] [PubMed]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Gonzales Zamora, J.A.; Corzo-Pedroza, M.; Romero Alvarez, M.; Martinez, O.V. Carbapenemase-Producing Raoultella Planticola: A Rare Cause of Pneumonia and Bacteremia. Diseases 2018, 6, 94. https://doi.org/10.3390/diseases6040094
AMA Style
Gonzales Zamora JA, Corzo-Pedroza M, Romero Alvarez M, Martinez OV. Carbapenemase-Producing Raoultella Planticola: A Rare Cause of Pneumonia and Bacteremia. Diseases. 2018; 6(4):94. https://doi.org/10.3390/diseases6040094
Chicago/Turabian StyleGonzales Zamora, Jose Armando, Monica Corzo-Pedroza, Maria Romero Alvarez, and Octavio V. Martinez. 2018. "Carbapenemase-Producing Raoultella Planticola: A Rare Cause of Pneumonia and Bacteremia" Diseases 6, no. 4: 94. https://doi.org/10.3390/diseases6040094
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.